12 lead EKG interpretation part 2
7
LAST MONTH, I described the components of the 12-lead electro- cardiogram (ECG) and how to rec- ognize a normal ECG. In this arti- cle, I’ll explain some advanced techniques that you can use to interpret common ECG abnormali- ties: bundle-branch blocks, myocardial infarction (MI), and common dysrhythmias. Bundle-branch blocks: Obstruction in the conduction Probably the most common ECG abnormality you’ll encounter is a bundle-branch block, which appears on the ECG as a wider- than-normal QRS complex (more than 0.12 second in duration). As you know, the cardiac impulse, originating in the sinoatrial (SA) node, normally travels through the bundle of His into the right and left bundle branches in the sep- tum. The two bundle branches ter- minate in the Purkinje fibers. When the impulse reaches them, ventricular depolarization begins. Normally the impulse is deliv- ered to myocardial cells on both sides of the heart simultaneously, so depolarization begins at the same time on both sides of the heart. The result is a very fast, syn- chronous contraction of the ventri- cles. On ECG, the normal QRS complex duration from two intact bundle branches is 0.12 second or less (three or fewer small squares of the ECG paper). A bundle-branch block occurs when one of the two bundle branches can’t conduct the cardiac impulse to the myocardial cells. The most common cause of chron- ic bundle-branch block is ischemic heart disease. When an artery sup- plying the bundle branch narrows, the flow of oxygenated blood is reduced and the bundle branch can’t conduct impulses normally. A common cause of acute bundle-branch block is acute MI. If the MI involves the ventricular septum, one of the bundle branch- es may become infarcted, leading to a loss of conduction. Although uncommon, physical injury of a bundle branch during an invasive procedure such as cardiac cathe- terization or heart surgery also may produce a bundle-branch block. 1 • In a right bundle-branch block (RBBB), impulse conduction to the right ventricle is blocked. The cardiac impulse is conducted only to the left side of the heart where left ventricular depolarization 36 Nursing2006, Volume 36, Number 12 www.nursing2006.com Learn to recognize bundle-branch blocks, myocardial infarction, and common dysrhythmias. BY GUY GOLDICH, RN, CCRN, MSN 12-lead ECG Understanding the part II Lead V 1 showing RBBB
Transcript of 12 lead EKG interpretation part 2

LAST MONTH, I described thecomponents of the 12-lead electro-cardiogram (ECG) and how to rec-ognize a normal ECG. In this arti-cle, I’ll explain some advancedtechniques that you can use tointerpret common ECG abnormali-ties: bundle-branch blocks,myocardial infarction (MI), andcommon dysrhythmias.
Bundle-branch blocks:Obstruction in the conductionProbably the most common ECGabnormality you’ll encounter is abundle-branch block, whichappears on the ECG as a wider-than-normal QRS complex (morethan 0.12 second in duration). Asyou know, the cardiac impulse,originating in the sinoatrial (SA)node, normally travels through thebundle of His into the right andleft bundle branches in the sep-tum. The two bundle branches ter-minate in the Purkinje fibers.
When the impulse reaches them,ventricular depolarization begins.
Normally the impulse is deliv-ered to myocardial cells on bothsides of the heart simultaneously,so depolarization begins at thesame time on both sides of theheart. The result is a very fast, syn-chronous contraction of the ventri-cles. On ECG, the normal QRScomplex duration from two intactbundle branches is 0.12 second orless (three or fewer small squaresof the ECG paper).
A bundle-branch block occurswhen one of the two bundlebranches can’t conduct the cardiacimpulse to the myocardial cells.The most common cause of chron-ic bundle-branch block is ischemicheart disease. When an artery sup-plying the bundle branch narrows,the flow of oxygenated blood isreduced and the bundle branchcan’t conduct impulses normally.
A common cause of acute
bundle-branch block is acute MI.If the MI involves the ventricularseptum, one of the bundle branch-es may become infarcted, leadingto a loss of conduction. Althoughuncommon, physical injury of abundle branch during an invasiveprocedure such as cardiac cathe-terization or heart surgery also mayproduce a bundle-branch block.1
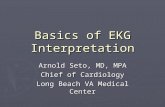
• In a right bundle-branch block(RBBB), impulse conduction tothe right ventricle is blocked. Thecardiac impulse is conducted onlyto the left side of the heart whereleft ventricular depolarization
36 Nursing2006, Volume 36, Number 12 www.nursing2006.com
Learn to recognize bundle-branch blocks, myocardial infarction, and common dysrhythmias.BY GUY GOLDICH, RN, CCRN, MSN
12-leadECG
Understanding the
part II
Lead V1 showing RBBB

begins. The right side of the heartdepolarizes only in response to thecell-to-cell wave of depolarizationthat travels from the left side of theheart. This cell-to-cell depolariza-tion is much slower than the nor-mal synchronous depolarization;that’s why the QRS complex is sig-nificantly wider than normal.
Examine lead V1 to identify anRBBB. In lead V1, the normal QRScomplex consists of a small Rwave, then a large S wave. As yourecall, lead V1 looks at the rightside of the heart. A small vectororiginating in the septum towardV1 creates a small upward R wave,then the predominant mean QRSvector creates the large S wave asthe mean QRS vector flows awayfrom lead V1.
In RBBB, the path of the meanQRS vector is changed due to left-to-right slow conduction; lead V1now records a delayed R waveapproaching it, resulting in a posi-
tive R wave. So the key identifier ofRBBB in lead V1 is a QRS complexwider than 0.12 second with adelayed (longer than 0.07 second)positive main R wave. Some RBBBsmay display a triphasic waveform(“rabbit ears”) consisting of a smallr wave, downward S wave, and asecond, larger R wave.2
• In a left bundle-branch block(LBBB), electrical impulses don’treach the left side of the heartnormally, so once again, synchro-nous depolarization of the ventri-cles doesn’t occur. Depolarizationbegins in the right side of the
heart and travels in a right-to-leftdirection via slow cell-to-celldepolarization. Lead V1 recordsthe mean QRS vector directedaway from its positive lead,resulting in a wide downwardcomplex. Because the mean vec-tor takes a relatively longer timeto cross to the left side of theheart, the QRS complex is widerthan 0.12 second. The key to rec-ognizing an LBBB is a wide,downward S wave or rS wave inleads V1 and V2.
Recognizing an MIOne of the most critical functionsof the 12-lead ECG is to determinewhether a patient is experiencingan acute MI. A series of predictableECG changes that occur during anMI help you identify it quickly andinitiate appropriate treatment.
Among one of the earliestchanges in the ECG tracing is anelevation of the ST segment, indi-
www.nursing2006.com Nursing2006, December 37
2.5ANCC/AACN
CONTACT HOURS
Lead V1 showing LBBB

cating reversible myocardial injury(see Understanding ST-segment ele-vation). In a normal ECG, the STsegment is level with the tracing’sbaseline. When myocardial cellssustain injury from MI, depolariza-tion is impaired, resulting in ST-segment elevation in the leadsmonitoring the affected areas of theheart. An ST-segment-elevation MI(STEMI), the most serious type ofMI, is associated with more com-plications and a higher risk ofdeath.3
The leads with ST-segment ele-vations identify the area of myocar-dial injury, so you can determinethe region of the heart affected byknowing which area is monitoredby which ECG lead. Let’s look atsome examples. • Because leads II, III, and aVF allmonitor the inferior (or bottom)wall of the heart from slightly dif-ferent directions, they’re usually
described as the inferior leads. Thisarea of the heart is perfused by theright coronary artery. A patientwith a STEMI involving the inferi-or wall of the heart will have ele-vated ST segments in leads II, III,and aVF (see Inferior-wall STEMI).• Another common infarct leadpattern occurs when an MIinvolves the intraventricular sep-tum, which is perfused by the leftanterior descending (LAD) coro-nary artery. In a septal MI, theleads monitoring the septum’selectrical activity will display ele-vated ST segments. Precordial (orchest) leads V1 and V2, which are
located on the anterior chest walldirectly over the septum, mostaccurately monitor the septum’selectrical activity. (These leadsalso are known as the septalleads.) The patient experiencing aseptal MI will have ST-segmentelevations in leads V1 and V2.• Directly to the left of the septalarea of the heart is the largefrontal or anterior wall of theheart, which is also perfused bythe LAD coronary artery. As themost muscular and powerfulpumping wall of the heart, theanterior wall is responsible for alarge proportion of cardiac output.Anatomically, leads V3 and V4 arelocated directly above the anteriorwall of the heart and monitor itselectrical activity. An anterior-wallSTEMI will cause the ST segmentsin these leads to be elevated (seeAnterior-wall STEMI).• The lateral wall of the heart, per-fused by the left circumflex artery,
38 Nursing2006, Volume 36, Number 12 www.nursing2006.com
Inferior-wall STEMILead II
Lead III
Lead aVF
Anterior-wall STEMILead V3
Lead V4
Understanding ST-segment elevation
Impaired depolarizationsecondary to myocardialinjury causes ST-segmentelevation in the leadsmonitoring the injuredareas of the heart.
ST-segment elevation
ST-segment elevation
Almost 4 mm

Tissue damage after MI
is located to the left of the anteriorwall and follows the curve of theleft lateral chest wall. Relativelymuscular, it also contributes sig-nificantly to the heart’s pumpingability. The ECG lead pattern thatmonitors the lateral wall’s electri-cal activity is more complexbecause the lateral wall is moni-tored by a combination of precor-dial (chest) leads and frontal(limb) leads.
Chest leads V5 and V6 are locat-ed on the left lateral chest walland monitor electrical activity bylooking down at the lateral heartwall. Leads I and aVL also moni-tor the lateral wall’s electrical ac-tivity. A patient with a lateral-wallSTEMI will have ST-segment ele-vations in leads I, aVL, V5, and V6.
Although patients can have MIsaffecting a single heart wall, suchas a discrete septal MI or anterior-wall MI, the area of infarction mayinvolve more than one area of theheart. In such a case, ST-segment
elevations appearin the leads moni-toring all of theinvolved areas. Forexample, if theinfarction extendsinto both the sep-tum and the ante-rior wall, the ST-segment elevationswould appear in
leads V1, V2, V3, and V4. The areasinvolved in the MI are reflected bythe descriptive name; in this case,an anterioseptal MI. For informa-tion on how MI affects heart mus-cle, see Tissue damage after MI.
Identifying common dysrhythmiasNow let’s examine some commonECG rhythm abnormalities youmay encounter in your practice,keeping in mind that you alwaystreat the patient, not the rhythm.When you find an abnormalrhythm or a rhythm change, assessyour patient and document levelof consciousness, vital signs, chestpain, shortness of breath, andother signs and symptoms associ-ated with thedysrhythmia.By using yourassessmentskills, nursingjudgment, andknowledge of
ECGs, you can determine the levelof urgency of the situation.• Sinus bradycardia is a sinusrhythm slower than the lowernormal sinus rate of 60 beats/minute. The P waves, QRS com-plexes, and T waves are all nor-mal. Sinus bradycardia is com-monly caused by ischemic heartdisease that causes the SA nodeto malfunction. Sinus bradycardiacan also be caused by acute MIand some types of medications,such as beta-blockers. Well-conditioned athletes may havenormal resting heart rates slowerthan 60 beats/minute. Assessyour patient for hemodynamicstability if he has a new or pro-found sinus bradycardia. Contactthe health care provider if yourpatient is symptomatic. Signs andsymptoms that may accompanysinus bradycardia include hypo-tension, lethargy, fatigue, chestpain, and difficulty breathing. Beprepared to transfer your patientto the intensive care unit (ICU)for a temporary pacemaker.• Sinus tachycardia is a sinusrhythm that’s faster than the
www.nursing2006.com Nursing2006, December 39
Sinus bradycardia
Sinus tachycardia
Ischemic zone
Area of injury
Area of necrosis
After an MI, the heart muscle has three zones of damage.Necrotic tissue dies from lack of blood flow. Injured cells mayrecover and ischemic cells can be saved if the area is reper-fused promptly.

upper normal sinus rate of 100beats/minute. Sinus tachycardiacan produce heart rates of 100 to150 beats/minute. At faster rates,the heart’s myocardial oxygendemand increases, and a patientwith preexisting heart diseasemay experience chest pain orother cardiac symptoms. Sinustachycardia usually is related to aphysiologic cause, such as fever,infection, pain, physical exertion,anxiety, hypoxia, or shock. If youcan identify and treat the cause,the heart rate will usuallydecrease. To manage sinus tachy-cardia with an unknown cause,the health care provider mayorder a beta-blocker such asmetoprolol or atenolol.4
• Atrial fibrillation (AF), one ofthe most common dysrhythmias
you’ll see in practice, has two pre-dominant characteristics: an irreg-ularly irregular heart rhythm andno meaningful P waves. Normally,after passive ventricular filling,the atria contract regularly andeject their load of blood into theventricles (atrial kick). In AF, atri-al kick is lost. Instead of contract-ing normally, the atria quiver dueto random and chaotic depolariza-tion of atrial cells. The randomatrial depolarization is alsoresponsible for the irregular ven-tricular rate, which can vary from40 to 180 beats/minute. Atrial fi-brillation has many causes, includ-ing atrial enlargement from chron-ic obstructive pulmonary disease
or other lung disease, thyroid dis-ease, ischemic heart disease, acuteMI, stress or fatigue, and excessiveuse of caffeine, alcohol, or ciga-rettes.
You may firstencounter AF dur-ing a routine vitalsigns check. If yourpatient has a newirregular heart rate,or has an abnormal-ly fast or slow heart rate, obtain anorder for a 12-lead ECG. Look foran irregularly irregular rhythm andf waves, the two hallmarks of AF.Perform a thorough physicalassessment because patients canrapidly become hemodynamicallyunstable or develop worseningheart failure. If your patient hasunstable or symptomatic AF,
administer supple-mental oxygen andestablish or main-tain intravenous(I.V.) access beforetransferring him tothe ICU or teleme-
try unit for treatment with I.V. dil-tiazem or a beta-blocker.
If the patient is stable, the healthcare provider may order variousoral medications to control or con-vert AF, such as digoxin, diltiazem,amiodarone, or metoprolol.
All patients with AF lastingmore than 48 hours are at high riskfor thrombus forma-tion because of irreg-ular blood flow inthe atria. If releasedinto the circulation,these thrombi cancause arterialobstruction resulting in life-threatening complications such asstroke. As ordered, administer I.V.
heparin and start the patient onoral warfarin to prevent thrombusformation.5
• Premature ventricular con-tractions (PVCs) are character-
ized by a wide, abnormal QRScomplex because conduction isthrough the ventricular tissue andnot the His-Purkinje system.Look for a QRS greater than 0.12second that appears large, abnor-mal, and premature (occurringbefore the next sinus beat).Caused by irritable ventriculartissue that depolarizes early andunpredictably, PVCs can be trig-gered by heart failure, electrolyteimbalances, stimulants such ascaffeine, hypoxia, acute MI,mitral valve prolapse, thyroid dis-ease, and injury or infarct of themyocardial tissue. Rare or isolatedPVCs seldom require aggressivetreatment. However, if you noticethat the frequency of PVCs isincreasing, or if you see newgroups or “runs” of PVCs, contactthe health care provider for fur-ther evaluation.• Ventricular tachycardia (VT)is a very rapid (100 to 250 beats/
minute) series of wide-complexventricular depolarizations. Inthis dysrhythmia, abnormal ven-
40 Nursing2006, Volume 36, Number 12 www.nursing2006.com
Isolated PVCs
Atrial fibrillation
Ventricular tachycardia

tricular tissue rapidly depolarizes,taking rhythm control away fromthe sinus node. Along with therapid rate, VT is characterized bywide, bizarre QRS complexes usu-ally followed by large T waves inthe opposite direction of themajor QRS deflection.
If your patient is unconscious,apneic, and pulseless, call a codeand start cardiopulmonary resus-citation. If your patient has apulse and is awake, treat this situ-ation as a medical emergency. Callfor the physician stat (and therapid response team, if your facil-ity has one), bring a crash cartwith a monitor/defibrillator to thebedside, and prepare to transferthe patient to the ICU.
Summing upLike any new skill, interpreting12-lead ECGs takes practice andcommitment. Make a habit ofreviewing your patients’ ECGsroutinely. Seek guidance from col-leagues experienced in ECGinterpretation, such as senior staffnurses, clinical nurse specialists,and clinical nurse-educators.Many physicians will also behappy to review an ECG with youif they know you’re interested inlearning to spot problems early.
With practice and experience,ECG interpretation will become avaluable nursing tool, helping youto recognize problems promptlyand provide even better patientcare.‹›
REFERENCES1. Kinney M, et al. (eds). AACN Clinical ReferenceGuide to Critical Care Nursing, 4th edition. St.Louis, Mo., Mosby, Inc., 1998.
2. Conover MB. Understanding Electrocardiogra-phy, 8th edition. St. Louis, Mo., Mosby, Inc., 2002.
3. Huszar RJ. Basic Dysrhythmias: Interpretation &Management, 3rd edition. St. Louis, Mo., Mosby,Inc., 2002.
4. Urden LD, et al. Thelan’s Critical Care Nursing:Diagnosis and Management, 5th edition. St. Louis,Mo., Mosby, Inc., 2005.
5. American Heart Association. (2005). Atrial fibrillation. Retrieved August 21, 2005, fromhttp://www.americanheart.org/presenter.jhtml?identifier=1596.
RESOURCEDubin D. Rapid Interpretation of EKGs, 6th edi-tion. Tampa, Fla., Cover Publishing, 2000.
Guy Goldich is assistant nurse-manager of the car-diac intensive care unit at Abington (Pa.) MemorialHospital and an adjunct faculty member at the hos-pital’s Dixon School of Nursing.
The author has disclosed that he has no significantrelationship with or financial interest in any commer-cial companies that pertain to this educational activity.
www.nursing2006.com Nursing2006, December 41
Earn CE credit online: Go to http://www.nursingcenter.com/CE/nursing and receive a certificate within minutes.
INSTRUCTIONS
Understanding the 12-lead ECG, part IITEST INSTRUCTIONS• To take the test online, go to our secure Web site at http://www.nursingcenter.com/ce/nursing.• On the print form, record your answers in the test answer sectionof the CE enrollment form on page 42. Each question has only onecorrect answer. You may make copies of these forms.• Complete the registration information and course evaluation.Mail the completed form and registration fee of $22.95 to:Lippincott Williams & Wilkins, CE Group, 2710 YorktowneBlvd., Brick, NJ 08723. We will mail your certificate in 4 to 6weeks. For faster service, include a fax number and we will faxyour certificate within 2 business days of receiving your enroll-ment form. • You will receive your CE certificate of earned contact hours and ananswer key to review your results. There is no minimum passing grade.• Registration deadline is December 31, 2008.
DISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published by
Lippincott Williams & Wilkins together and deduct $0.95 from theprice of each test.• We also offer CE accounts for hospitals and other health carefacilities on nursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATIONLippincott Williams & Wilkins, the publisher of Nursing2006, willaward 2.5 contact hours for this continuing nursing education activ-ity. Lippincott Williams & Wilkins is accredited as a provider of con-tinuing nursing education by the American Nurses CredentialingCenter’s Commission on Accreditation. This activity is also providerapproved by the California Board of Registered Nursing, ProviderNumber CEP 11749 for 2.5 contact hours. Lippincott Williams &Wilkins is also an approved provider by the American Associationof Critical-Care Nurses (AACN 00012278, CERP Category A),Alabama #ABNP0114, Florida #FBN2454, and Iowa #75.Lippincott Williams & Wilkins home study activities are classifiedfor Texas nursing continuing education requirements as Type 1.Your certificate is valid in all states.

1. A bundle-branch block occurs whenone of two bundle branches can’t conductcardiac impulses to thea. atria. c. myocardial cells.b. bundle of His. d. atrioventricular node.
2. The most common cause of a chronicbundle-branch block isa. ischemic heart disease.b. an acute MI.c. an acute coronary syndrome.d. trauma to one of the bundle branches.
3. In addition to a QRS complex widerthan 0.12 second, which ECG abnormalityis a key indicator of an RBBB?a. a negative R wave in lead V1b. a positive R wave in lead V3c. a negative R wave in lead V3d. a positive main R wave in lead V1
4. Which is one of the earliest changesindicative of reversible myocardialinjury?a. QT prolongationb. Q-wave deepeningc. ST-segment elevationd. PR interval shortening
5. Which leads view the inferior wall ofthe heart?a. V1 through V6 c. I and aVLb. I, II, and III d. II, III, and aVF
6. Elevated ST segments in V1 and V2indicate which type of MI? a. anterior wall c. lateral wallb. septal wall d. inferior wall
7. Which heart wall is perfused by thecircumflex branch of the left coronaryartery?a. lateral c. anteriorb. inferior d. septal
8. A patient with ST-segment elevation in leads I, aVL, V5, and V6 may havea. an anterior-wall MI.b. an inferior-wall MI.c. a lateral-wall MI.d. a posterior-wall MI.
9. An anterioseptal MI would have STelevation in leadsa. V1 and V2 only. c. V5 and V6 only.b. V3 and V4 only. d. V1 through V4.
10. Which isn’t a possible cause of sinusbradycardia?a. atropineb. beta-blockersc. acute MId. a well-conditioned heart
11. Sinus tachycardia usually is related toa. medications.b. an MI.c. a physiologic cause.d. ischemic heart disease.
12. One hallmark of AF isa. a regularly irregular rhythm.b. a prolonged QRS complex. c. an irregularly irregular rhythm.d. a prolonged PR interval.
13. Atrial contraction just before ventric-ular contraction is calleda. atrial kick. c. synchrony.b. repolarization. d. f waves.
14. Which medication may be used totreat AF?a. lidocaine c. captoprilb. atropine d. diltiazem
15. Premature ventricular contractionsare characterized by wide, abnormal a. QRS complexes. c. P waves.b. U waves. d. T waves.
16. If your patient is in pulseless VT,which action would you take first?a. Call the rapid response team.b. Obtain a stat 12-lead ECG.c. Call a code.d. Ensure adequate vascular access.
Understanding the 12-lead ECG, part IIGENERAL PURPOSE To provide nurses with techniques to analyze common ECG abnormalities. LEARNING OBJECTIVES After reading the pre-ceding article and taking this test, you should be able to: 1. Differentiate between LBBB and RBBB. 2. Determine the relationship between leads withECG changes and areas of myocardial damage. 3. Identify common dysrhythmias.
2.5ANCC/AACN CONTACT HOURS
ENROLLMENT FORM Nursing2006, December, Understanding the 12-lead ECG, part II
A. Registration Information:
Last name ____________________________ First name ________________________ MI _____
Address _______________________________________________________________________________
City _______________________________________ State _________________ ZIP ______________
Telephone ____________________ Fax ____________________ E-mail ____________________
Registration Deadline: December 31, 2008Contact hours: 2.5 Pharmacology hours: 0.0 Fee: $22.95
q LPN q RN q CNS q NP q CRNA q CNM q other ___________________
Job title __________________________________ Specialty _________________________________
Type of facility ____________________________________ Are you certified? q Yes q No
Certified by ___________________________________________________________________________
State of license (1) __________________________ License # ___________________________
State of license (2) __________________________ License # ___________________________
q Please fax my certificate to me.q From time to time, we make our mailing list available to outside organizations to announce special offers.
Please check here if you do not wish us to release your name and address.
B. Test Answers: Darken one circle for your answer to each question.
a b c d1. m m m m2. m m m m3. m m m m4. m m m m
a b c d5. m m m m6. m m m m7. m m m m8. m m m m
a b c d9. m m m m
10. m m m m11. m m m m12. m m m m
a b c d13. m m m m14. m m m m15. m m m m16. m m m m
C. Course Evaluation*1. Did this CE activity's learning objectives relate to its general purpose? q Yes q No2. Was the journal home study format an effective way to present the material? q Yes q No3. Was the content relevant to your nursing practice? q Yes q No4. How long did it take you to complete this CE activity?___ hours___minutes5. Suggestion for future topics __________________________________________________________
D. Two Easy Ways to Pay:q Check or money order enclosed (Payable to Lippincott Williams & Wilkins)q Charge my q Mastercard q Visa q American Express
Card # _____________________________________________ Exp. date __________________
Signature _______________________________________________________________________
*In accordance with the Iowa Board of Nursing administrative rules governing grievances, a copy of your evaluation of the CE offering may be submitted directly to the Iowa Board of Nursing.N2406
$$