1 Session 3 Design and Analysis of Trials of Therapist Treatments Chris Roberts University of...
74
1 Session 3 Design and Analysis of Trials of Therapist Treatments Chris Roberts University of Manchester Email: [email protected] Methodology Research Group Research funded by: MRC Methodology Grants G0600555 G0900678, G0800606, G0802418 MHRN Methodology Research Group
-
Upload
jesse-matthews -
Category
Documents
-
view
213 -
download
0
Transcript of 1 Session 3 Design and Analysis of Trials of Therapist Treatments Chris Roberts University of...

1
Session 3Design and Analysis of Trials of Therapist Treatments
Chris RobertsUniversity of ManchesterEmail: [email protected]
Methodology Research Group
Research funded by:MRC Methodology Grants G0600555
G0900678, G0800606, G0802418MHRN Methodology Research Group

2
Intervention Trials with clustering
• Cluster randomised trials• Health professional activities - therapist trials• Group therapies/ group administered treatments trials
In all three types of trial patients can be considered to be in clusters.
Clusters may be:• Experimental units define by randomisation.• Observational units related to the delivery of treatment.

3
Overview of presentation
• Cluster randomised trials – Design – Analysis –Sample Size – Advantage & Disadvantages
• Therapist and Group Therapy Trials– Design – Analysis -
In all three types of trial patients can be considered to be in clusters.
Clusters may be:• Experimental units define by randomisation.• Observational units related to the delivery of treatment.
4
Cluster Randomised Trials (CRTs)
5
Cluster Randomised Trials
Interventions are randomised to groups of patients (clusters) rather than to patients individually.
In mental health CRTs are typically used to test:
•IMPLEMENTATION of new procedures where the intervention applies to complete clinical units.
•PROFESSIONAL BEHAVIOUR CHANGE where the intervention involves training of health professionals.
For these types of intervention once the intervention has taken place it is difficult if not impossible for patients to receive the comparator without changing clinical unit or health professional.

6
Mental Health Cluster Randomised Trials
ExampleSystematic assessments of need and care planning in severe mental illness Priebe et al BJP, (2007) 191: 420-426. Aims To test a computer-mediated intervention structuring patient–clinician dialogue (DIALOG). Methods 134 key workers (clusters) were allocated to DIALOG or treatment as usual.507 people with schizophrenia or related disorders were included.Outcome MeasuresPrimary outcome was subjective quality of life, and secondary outcomes were unmet needs and treatment satisfaction.

7
Illustration of Cluster Randomised Trials
Clus1
P11 P12 P13
Clus2
P21 P22 P23
Clus3
P31 P32 P33
Intervention A
Clus4
P41 P42 P43
Clus5
P51 P52 P53
clus6
P61 P62 P63
Intervention B
CLUSTER
PATIENT
Intervention A
CLUSTER
PATIENT
Intervention B
Schematic Unit Diagram
Classification Diagram
8
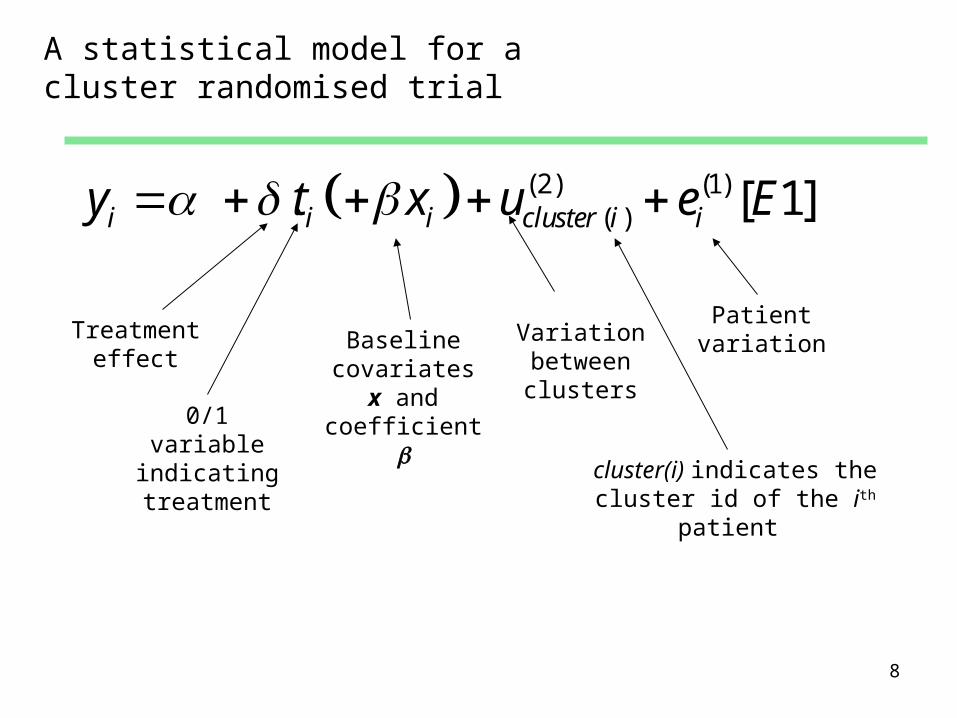
A statistical model for a cluster randomised trial
Treatment effect
Baseline covariates x
and coefficient
Variation between clusters
Patient variation
(2) (1)( ). [ 1]i i i cluster i iy t x u e E
0/1 variable indicating treatment cluster(i) indicates the
cluster id of the ith
patient
9
Methods of statistical analysis
Summary measure analysis
Use each cluster as the unit of analysis.Obtain an average for each cluster then compare treatments use a t-
test applied to the cluster averages.
Modelling Methods
Maximum Likelihood (ML)REstrict Maximum Likelihood (REML)
Generalised Estimating Equation (GEE)Survey Estimators (SVY in Stata)
10
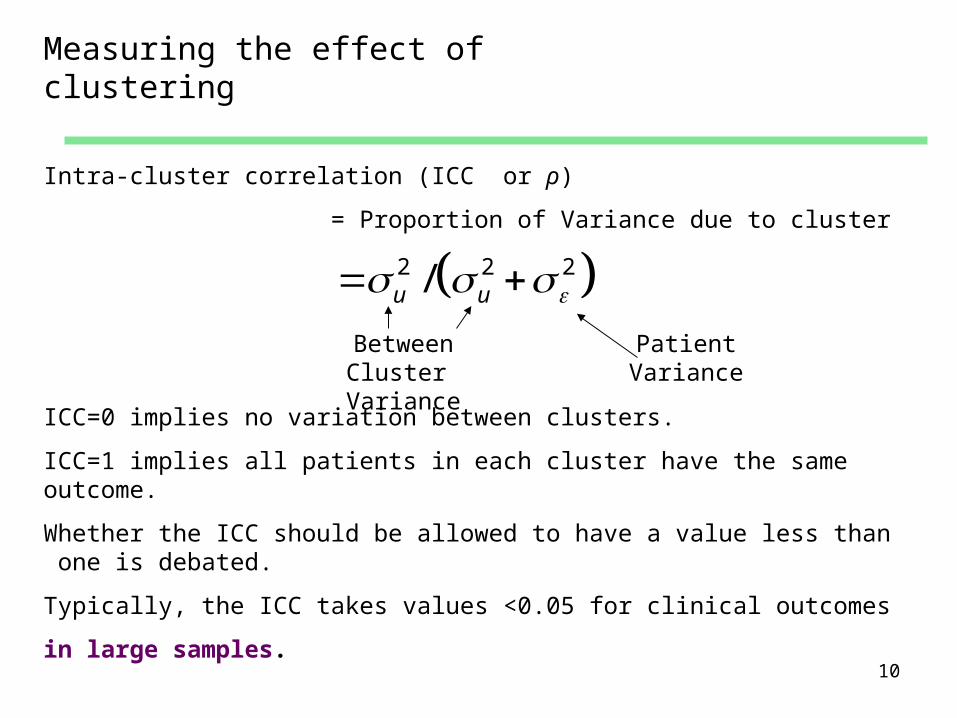
Measuring the effect of clustering
2 2 2/u u Between Cluster
VariancePatient
Variance
Intra-cluster correlation (ICC or ρ)
= Proportion of Variance due to cluster
ICC=0 implies no variation between clusters.
ICC=1 implies all patients in each cluster have the same outcome.
Whether the ICC should be allowed to have a value less than one is debated.
Typically, the ICC takes values <0.05 for clinical outcomes
in large samples.

11
Sample Size and Power for a Cluster Randomised Trial
As well as effect size, test size () and s.d., power depends on:• number of clusters (n)• numbers of patients per cluster (m) • intra-cluster correlation coefficient (ρ)
Design Effect (DE) = Ratio of the number of subjects required where there is clustering to the number required assuming no clustering.
Assuming clusters are of equal size
1 ( 1)m DE
Cluster size (m) ICC (ρ)
12
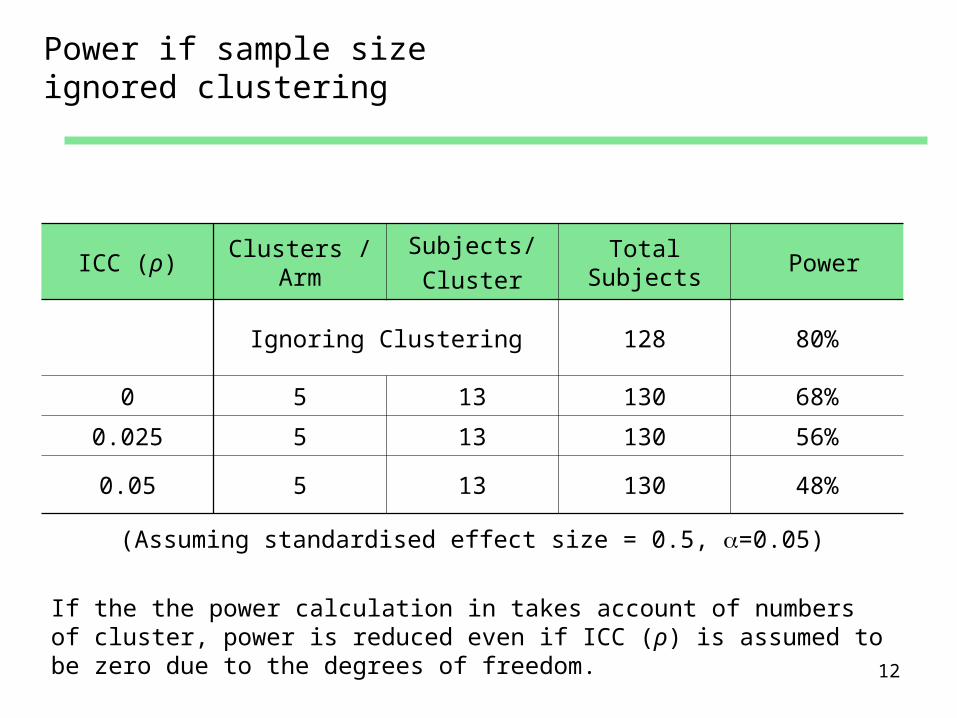
Power if sample size ignored clustering
ICC (ρ)Clusters
/ArmSubjects/Cluster
Total Subjects
Power
Ignoring Clustering 128 80%
0 5 13 130 68%
0.025 5 13 130 56%
0.05 5 13 130 48%
(Assuming standardised effect size = 0.5, =0.05)
If the the power calculation in takes account of numbers of cluster, power is reduced even if ICC (ρ) is assumed to be zero due to the degrees of freedom.

13
ICC (ρ)Clusters /
ArmSubjects/Cluster
Total Subjects
Power 1/ρ
Ignoring Clustering 128 80% -
0 5 18 180 81% -
0.025 5 30 300 80% 40
0.05 5 130 1300 80% 20
(Assuming standardised effect size = 0.5, =0.05)
Numbers of subjects required increases substantial as ICC increases particularly once it exceeds 1/ρ.
Increasing the number of Subjects/Cluster

14
Increasing number of clusters/arm
ICC (ρ)Clusters
/ArmSubjects/Cluster
Total Subjects
Power
Ignoring Clustering 128 80%
0 7 13 182 86%
0.025 8 13 208 83%
0.05 9 13 234 80%
(Assuming standardised effect size = 0.5, =0.05)
Required numbers of subjects more feasible.

15
Advantages of Cluster Randomised Trial
• No contamination between the interventions being compared.
• External validity as intervention can be made to correspond more closely to Usual Care as patients not being individually randomised.
• Administrative and logistic convenience.• Acceptability to health service staff as less disruptive than
individual patient randomisation.• Potential for greater recruitment of patients and groups.• Patient consent may be simpler.

16
Disadvantages of Cluster Randomised Trial
Any two patients within the same cluster are likely to be more similar than two patients from different clusters due to:•Characteristics of patients in a cluster.•Patient interaction within a cluster.•Measured and unmeasured characteristics of health care delivery of a cluster.
This effect is called clustering or more formally intra-cluster correlation.
Valid statistical methods need to take account of the implications of intra-cluster correlation. This requires:•More complex methods of statistical analysis.•A larger sample size of patients is required to achieve the same power and precision as the corresponding individually randomised trial.
Internal validity depends on the selection of patients being independent of randomisation.

17
Summary: Cluster RCTs
Use of cluster randomisation may have advantages including external validity but:
• Precision is reduced.• Validity depends on patient recruitment being
independent of the cluster randomisation.

18
Therapist and Group Administered Treatments Trials

19
Therapist Variation and Clinical Trials
Outcome for patients treated by the same therapist may be more similar than outcomes for patients treated by different therapists due to Therapist characteristics such as:
•Experience•Training•Competence•Empathy
Patients can be considered to be clustered by therapist.
This variation has implications for the Precisions and Validity of psycho-therapy trials.
20
Consort Guidance for Non-pharmacological Trials
A recently published extension of the Consort Guidelines for Non-pharmacological Treatment Trials has drawn attention to the issue.
They recommend that trial of Non-pharmacological Treatment reports how clustering by care-provider has been considered in relation to:
•Selection of care providers.•Sample size calculation.•Allocation of care providers to each trial arm.•Statistical analysis of outcome.
21
Type of Comparisons involving Care Providers
TechniquesDifferent treatment methods delivered by the same care provider.Face-2-Face and Telephone delivered CBT therapy for patients with OCD.Different surgical methods.
Care Provider CharacteristicsComparison of nurse practitioners and general practitioners in primary care.
Packages
Different techniques and different characteristics combined.CBT delivered by a clinical psychologist with Non-directive counselling delivered by a counsellor.
22
Group Administered Treatments
• Examples: Group CBT, Substance misuse, Anger management
• Outcome may be more similar for subjects in the same class or group as patients may interact and this may be a component of the treatment.
• The clustering effect of group deliver only applies to group therapy arm if trial patients are randomised individually.
• Groups may be closed, open, or rolling.
• Where groups are closed, each therapy group can be considered as a cluster.

23
Care Providers and Trial Designs

24
Trial Designs for Therapist Treatment
• Nested (Therapist) Design also called Hierarchical (Therapist) Design.
• Partially Nested (Therapist) Design.
• Crossed (Therapist) Design also called a Stratified (Therapist) Design.
25
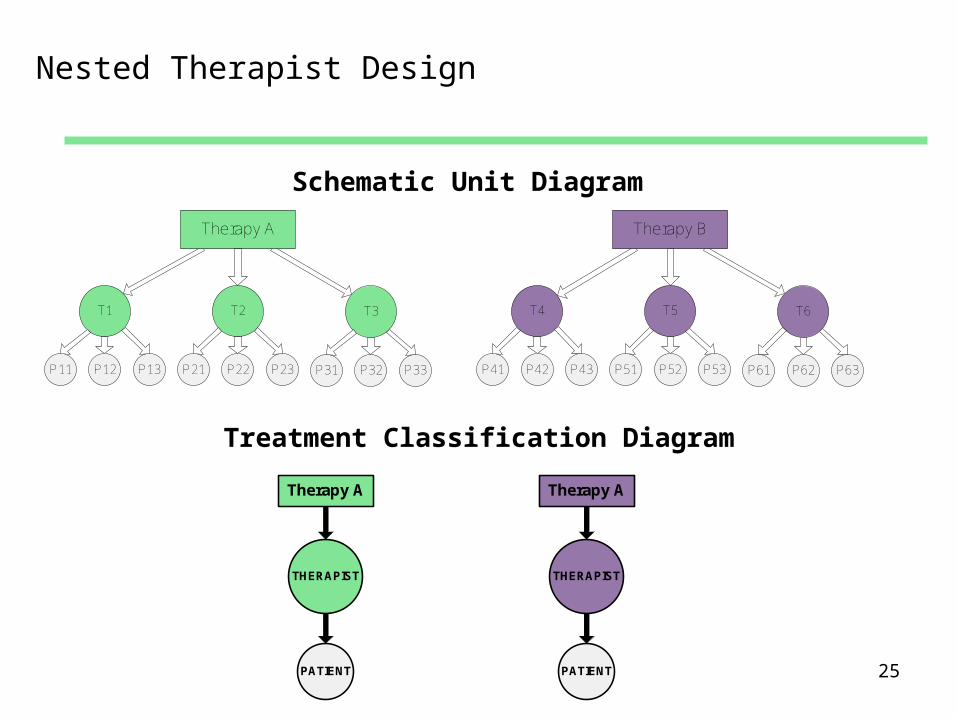
Nested Therapist Design
Schematic Unit Diagram
THERAPIST
PATIENT
Therapy A
THERAPIST
PATIENT
Therapy A
Treatment Classification Diagram
T1
P11 P12 P13
T2
P21 P22 P23
T3
P31 P32 P33
Therapy A
T4
P41 P42 P43
T5
P51 P52 P53
T6
P61 P62 P63
Therapy B
26
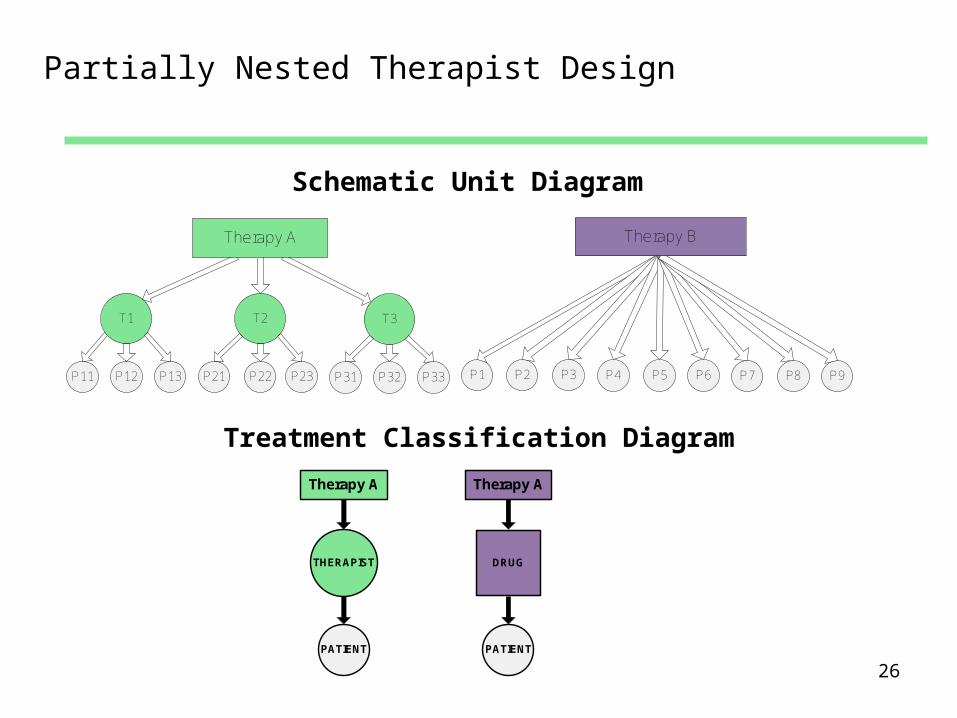
Partially Nested Therapist Design
THERAPIST
PATIENT
Therapy A
PATIENT
Therapy A
DRUG
Schematic Unit Diagram
Treatment Classification Diagram
P1 P2 P3 P4 P5 P6 P7 P8 P9
Therapy B
T1
P11 P12 P13
T2
P21 P22 P23
T3
P31 P32 P33
Therapy A

27
Crossed Therapist Design
THERAPIST
PATIENT
Therapy A
PATIENT
Therapy B
THERAPIST
CROSSED
P11 P12
A
P13 P14
B
P21 P22
A
P23 P24
B
P31 P32
A
P33 P34
B
P41 P42
A
P43 P44
B
T1 T2 T3 T4
Schematic Unit Diagram
Treatment Classification Diagram
28
Crossed Therapist Design
Same health professional delivers both interventions.
Example: Treatment delivered face-to-face or by phone
Similar to:
• Multi-centre study: Therapist Centre/Study• Meta-analysis: Therapist Study• Crossover cluster randomised trial: Therapist Cluster• Matched pairs cluster randomised: Therapist Matched pair
Treatment effect can be estimated within therapists
See Appendix for details of regarding analysis and sample size.
29
Statistical Analyses for Nested and Partially Nested Designs
• Statistical analysis of Nested and Partially nested designs are similar to cluster randomised trials.
• There is nevertheless added complexity due to the cluster being defined by treatment rather pre-specified for the purpose of randomisation.
30
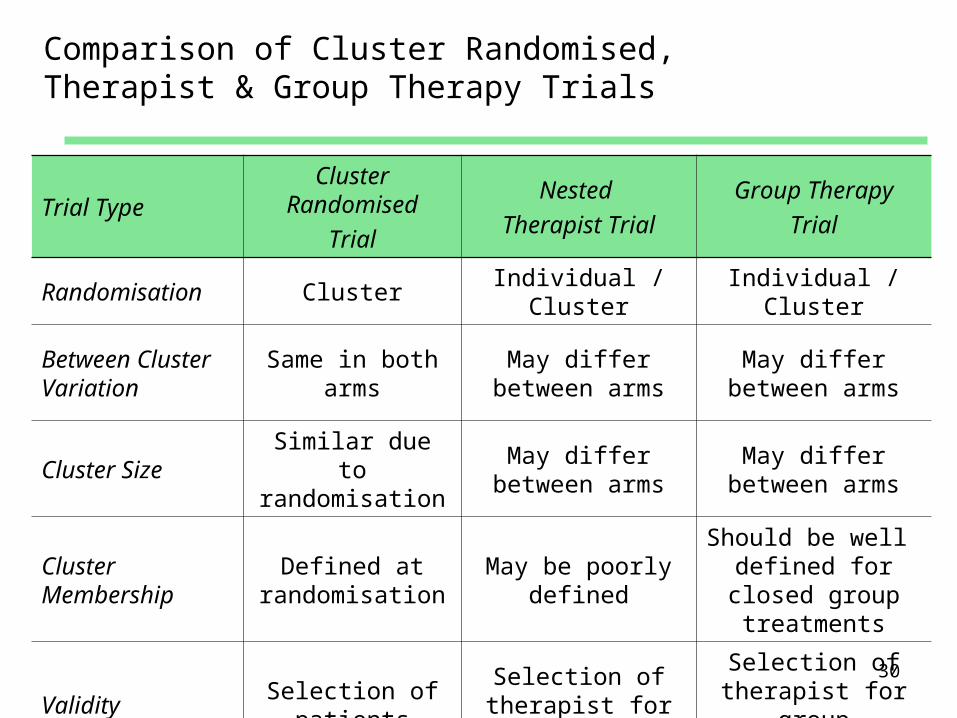
Comparison of Cluster Randomised, Therapist & Group Therapy Trials
Trial TypeCluster
RandomisedTrial
Nested Therapist Trial
Group TherapyTrial
Randomisation ClusterIndividual /
ClusterIndividual /
Cluster
Between Cluster Variation
Same in both arms
May differ between arms
May differ between arms
Cluster SizeSimilar due to randomisation
May differ between arms
May differ between arms
Cluster Membership
Defined at randomisation
May be poorly defined
Should be well defined for closed group treatments
ValiditySelection of
patients
Selection of therapist for treatments
Selection of therapist for
group treatments
31
Care Providers and Statistical Analysis
32
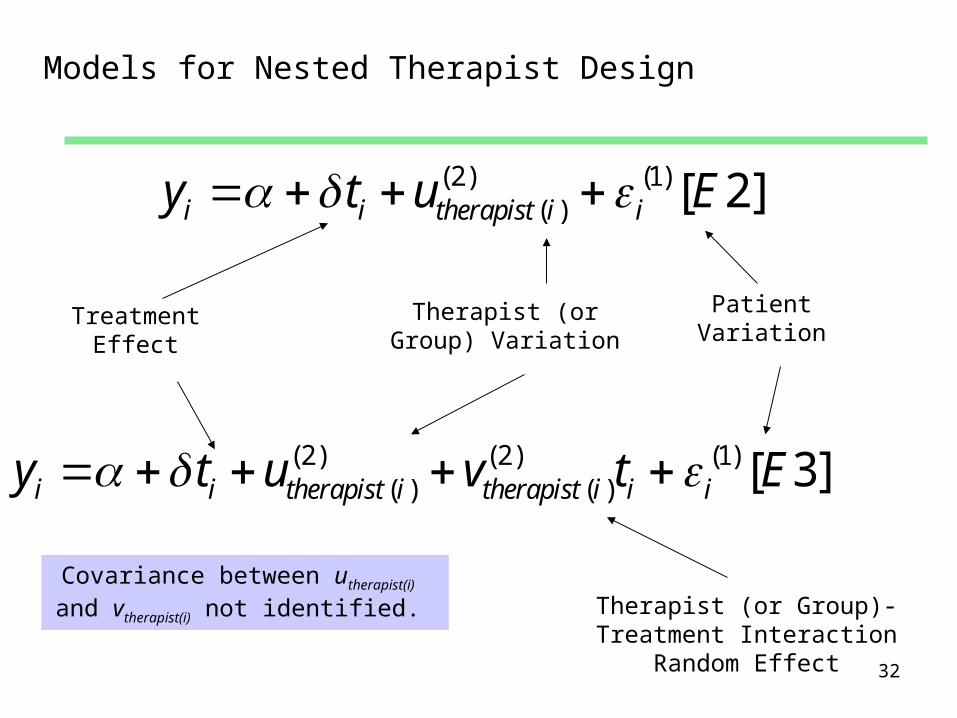
Models for Nested Therapist Design
Treatment Effect
Therapist (or Group) Variation
Patient Variation
(2) (1)( ) [ 2]i i therapist i iy t u E
Therapist (or Group)-Treatment Interaction
Random Effect
(2) (2) (1)( ) ( ) [ 3]i i therapist i therapist i i iy t u v t E
Covariance between utherapist(i) and vtherapist(i) not identified.

33
Level Heteroscedasticity in a Nested Therapist Design
In cluster randomised trial between arm heteroscedasticity generally ignored and not important
Treatment Effect Therapist or Group
VariationPatient
Variation
Heteroscedasticity in patient variation between treatments (level 1) may bias estimates of therapist variances (level 2) if cluster size differ.
(2) (2) (1) (1)( ) ( ) [ 4]i i therapist i therapist i i i i iy t u v t t E

34
Level Heteroscedasticity in a Nested Therapist Design (Alternative Parameterization)
In cluster randomised trial between arm heteroscedasticity generally ignored and not important
Treatment Effect Therapist or Group
VariationPatient
Variation
Heteroscedasticity in patient variation between treatments (level 1) may bias estimates of therapist variances (level 2) if cluster size differ.
(2) (2) (1) (1)1, ( ) 2, ( ) 1, 2,. 1 . 1 . [ 5]i i therapist i i therapist i i i i i iy t u t u t t t E

35
Intra-cluster Correlation for Therapist (ρ)
2 2 2/u u
Therapist Variance
Patient Variance
ICC (ρ)= Proportion of Variance due to Therapist
2 2 2 2 2 22 u v u v
ICC for second treatment where differential clustering is considered is
36
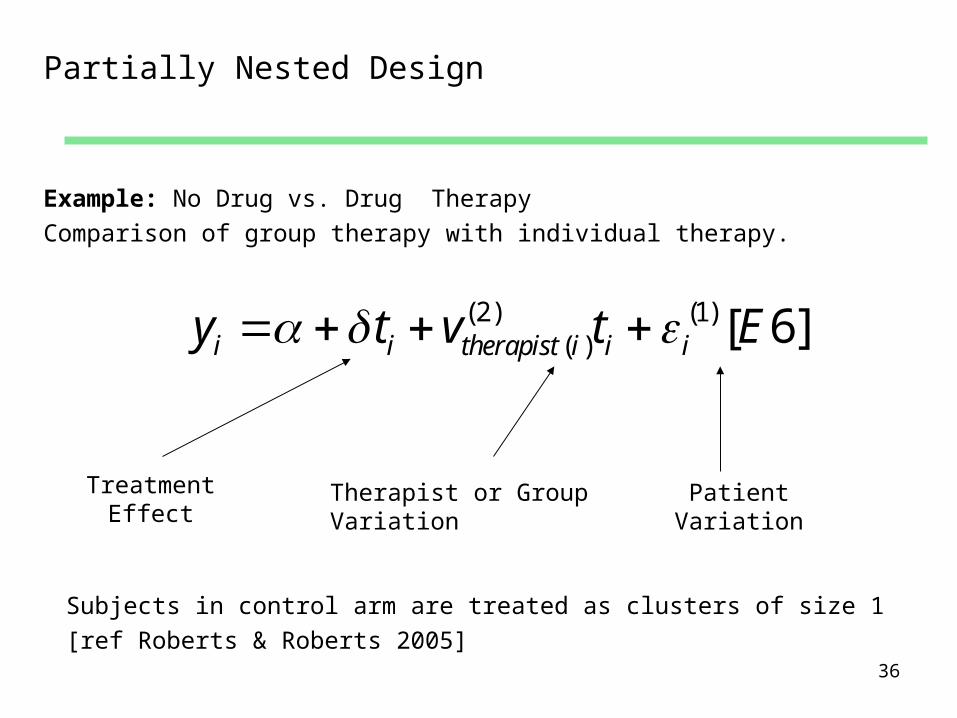
Partially Nested Design
Subjects in control arm are treated as clusters of size 1[ref Roberts & Roberts 2005]
Treatment Effect
Therapist or Group Variation
Patient Variation
Example: No Drug vs. Drug TherapyComparison of group therapy with individual therapy.
(2) (1)( ) [ 6]i i therapist i i iy t v t E

37
Heteroscedasticity and the Partially Nested Design
Failure to take account of heteroscedasticity can bias estimates of therapist variation and can effect test size
[ref Roberts & Roberts 2005]
Treatment Effect
Therapist or Group Variation
Patient Variation
Example: No Drug vs. Drug TherapyComparison of group therapy with individual therapy.
(2) (1) (1)( ) [ 7]i i therapist i i i i iy t v t t E

38
Crossed Design
2 2 2/ 2v v
Variance of treatment with therapist interaction
(vtherapist(i) )
Pooled Variance of patient within
treatment
How should clustering effect be considered in a crossed design?
(2) (2) (1)( ) ( ) [ 3]i i i i therapist i therapist i i iy t x u v t E
Loss of precision and design effect depends on variance of vtherapist(i) but not utherapist(i) . A parameter for sample size calculation could be

39
Crossed Design (Alternative parameterization)
2 2 2/q q q
Variance of treatment with therapist interaction
(qtreat(i) )
Pooled Variance of patient within
treatment
Three level model with patients nested in treatments nested in therapist
(3) (2) (1)( ) ( ) [ 8]i i i i therapist i treat i iy t x p q E
qtreat(i) is the variation between treatments within therapist
Loss of precision and design effect depends on variance of qtreat(i) but not ptherapist(i) .
40
Internal and External Validity

41
Internal Validity and Therapist Variation
Randomisations Possible in Trials of Therapeutic Approaches
PATIENTS
NESTED DESIGN
THERAPISTS
TREATMENTS
• Random allocation of treatment to therapist to prevent confounding of therapist characteristics with the treatment effect. Example: Schnurr et al.
• Random allocation of Therapist to Patient to would prevent confounding of therapist variation with patient characteristics. Example: Schnurr et al.
42
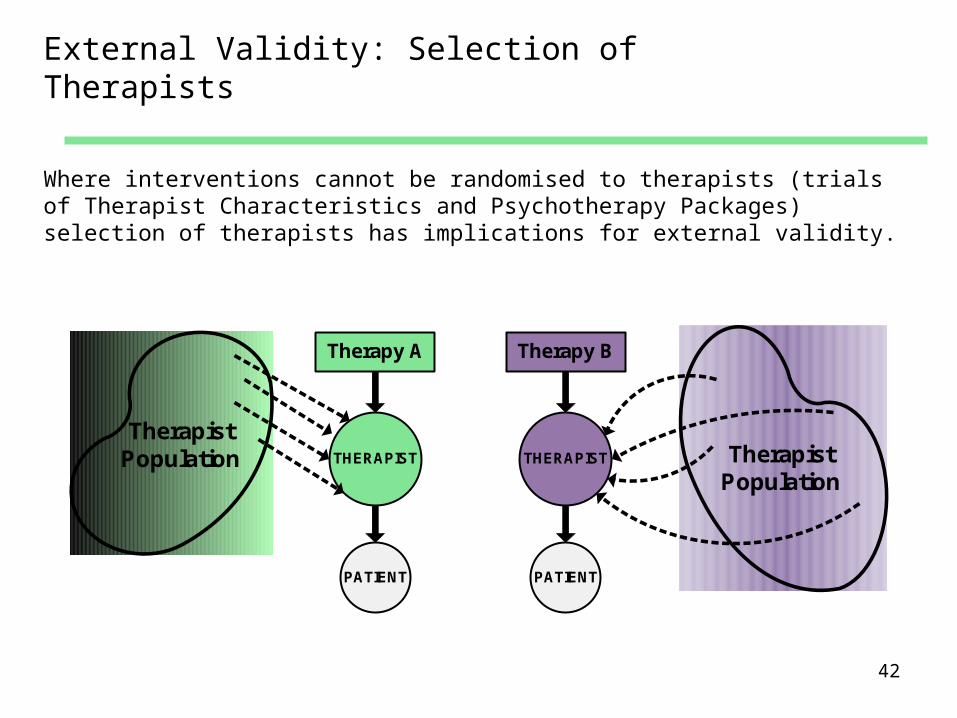
External Validity: Selection of Therapists
Where interventions cannot be randomised to therapists (trials of Therapist Characteristics and Psychotherapy Packages) selection of therapists has implications for external validity.
THERAPIST
PATIENT
Therapy A
THERAPIST
PATIENT
Therapy B
TherapistPopulation Therapist
Population
43
External Validity of Therapist
Particularly for trials of Therapist Characteristics and Psychotherapy Packages selection of therapist has implications for external validity.
Need to consider how representative trial therapists are of non-trial therapists.
Just as for patients in any trial inclusion and exclusion criteria are need for therapist.
Recruiting therapists directly from clinical practice using broad eligibility criteria might be more representative
but this could also increase the intra-cluster correlation.

44
External Validity: Therapists and Patient characteristics
T1
P11 P12 P13
T2
P21 P22 P23
T3
P31 P32 P33
Therapy A
T4
P41 P42 P43
T5
P51 P52 P53
T6
P61 P62 P63
Therapy B
Randomisation of treatment to patients balances patients characteristics across arms.
Since it is rare to be able to randomise to therapists to patients, therapist variation may be confounded by patient characteristics.
Two possibilities for analysis are:• Estimating the ICC by therapist for patient baseline characteristics.• The effect of baseline covariates on the ICC for therapist for the
outcome measures.

45
Could ICC for therapist be induced by unobserved confounding?
Suppose we have
• Outcome Y and unobserved confounder Z
• Suppose ICC for Z is Z
• Suppose rYZ is the correlation between Y and Z
• Induced ICC is Z rYZ2
Given that rYZ is unlikely to exceed 0.5 Z would need to be
large for an ICC of Y to be induced by unobserved confounding.
46
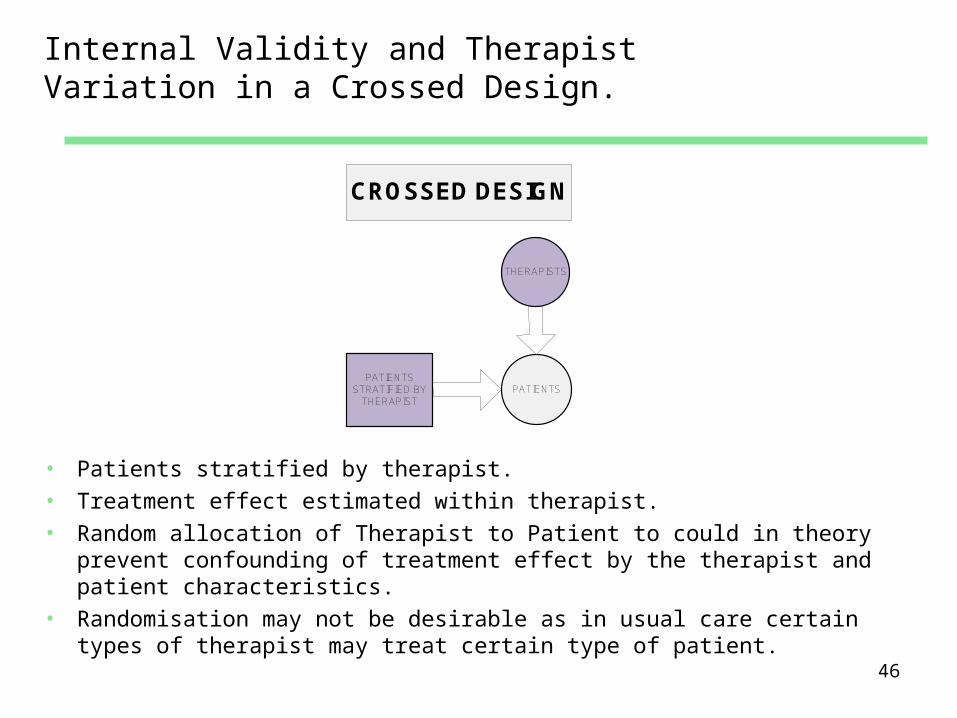
Internal Validity and Therapist Variation in a Crossed Design.
PATIENTS
THERAPISTS
PATIENTSSTRATIFIED BY
THERAPIST
CROSSED DESIGN
• Patients stratified by therapist.• Treatment effect estimated within therapist.• Random allocation of Therapist to Patient to could in theory
prevent confounding of treatment effect by the therapist and patient characteristics.
• Randomisation may not be desirable as in usual care certain types of therapist may treat certain type of patient.
47
Treatment Comparisons in Psychotherapy Trials
Therapeutic ApproachesEither Crossed Design or Nested Design.
Therapist CharacteristicsNested Design
Psychotherapy Packages combining different approaches and different characteristics
Nested Design
Whether a trial is of Therapeutic Approaches, Therapist Charactistics or a Package depends on the counter factual treatment. What would/should a patient receive if they did not receive the intervention?

48
An Example
Comparison of CBT & NDC for Depression in Primary Care
Data from Ward et al BMJ 2000;321:1383-8
49
Trial: CBT v NDC for Depression in Primary Care
Participants: 262 patients presenting with depression or mixed anxiety + depression.
Interventions: Up to 12 sessions of therapy•cognitive-behaviour therapy (12 psychologist) •non-directive counselling (14 counsellors)
Primary outcome measures: Beck Depression Inventory scores at 4 and 12 months.
Original published analysis ignored clustering by therapist.
Reanalyzed including random effect for therapist.

50
Trial: CBT v NDC for Depression in Primary Care
CLINICALPSCHOLOGIST
PATIENT
CBT
ROGERIANCOUNCELOR
PATIENT
NDC
Treatment Classification Diagram

51
Summary Stats by Treatment Arm
Cognitive Behavioural Therapy
Non-directive Counselling
Mean sd n mean sd n
AGE 35.5 12.0 134 36.1 11.8 126
Male 25% (34/134) 28% (35/126)
BDI mean sd n mean sd n
At Rand. 27.6 7.9 134 27.6 9.0 126
4 months 12.5 10.0 117 12.3 8.5 112
12 months
9.9 10.2 107 11.2 9.1 102

52
Intra-cluster Correlation of Baseline Characteristics
ICC() 95% c.i.
AGE 0.014 (0.000, 0.119)
Male 0.019 (0.000, 0.125)
BDI 0 (0.000, 0.102)
If therapists were randomised to patients, one would expected these to be zero.
53
Analysis of Outcome BDI
• Random effect models fitted using REML (STATA:xtmixed) or RIGLS (ML-WIN)
• Outcome BDI at 4 months.
• Covariates Age, Gender, BDI at baseline.
• BDI squared transformed to improve normality.
Alternative analysis not presented:
• Survey estimators (STATA:svy)
• Generalized Estimating Equations (STATA:xtgee)
• Bayesian Random Effects Models (MCMC: Winbugs/R/MLWin)
54
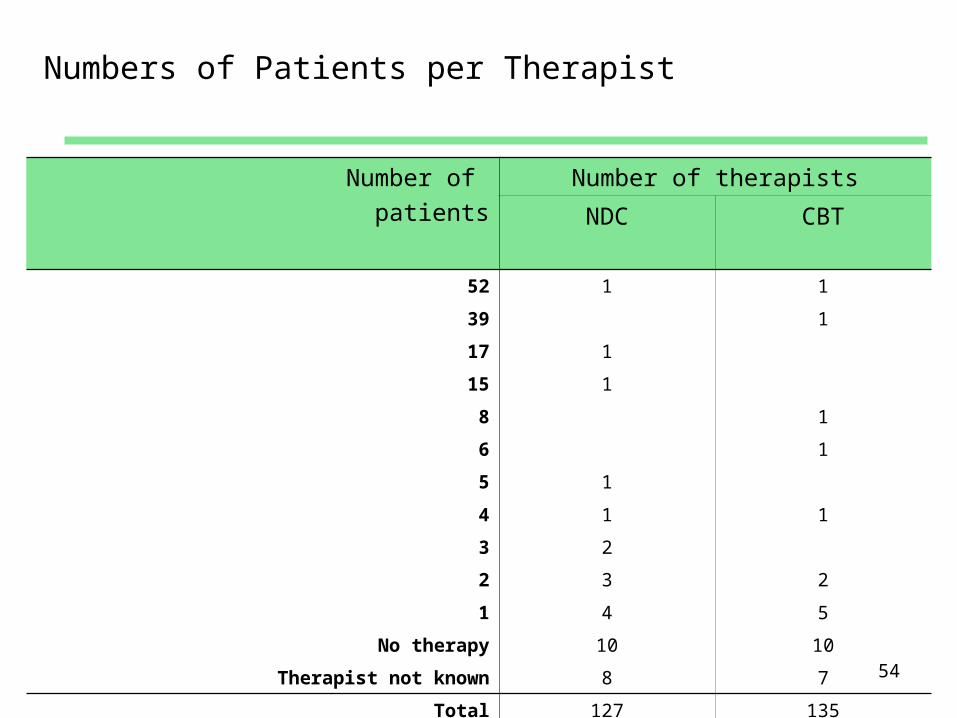
Numbers of Patients per Therapist
Number of patients
Number of therapists
NDC CBT
52 1 1
39 1
17 1
15 1
8 1
6 1
5 1
4 1 1
3 2
2 3 2
1 4 5
No therapy 10 10
Therapist not known 8 7
Total 127 135
55
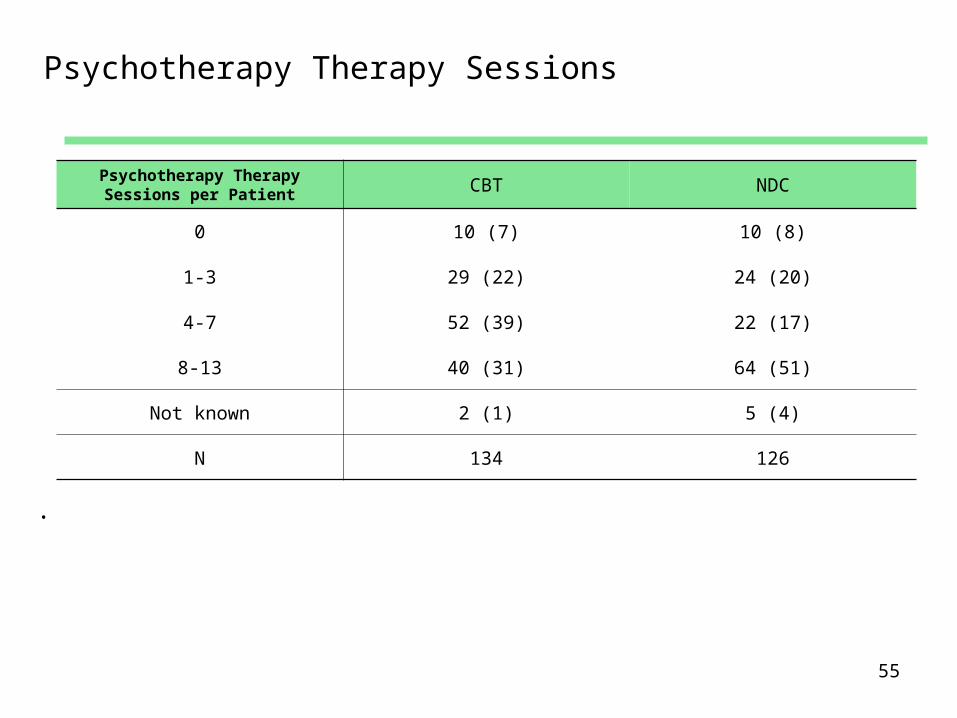
Psychotherapy Therapy Sessions
Psychotherapy Therapy Sessions per Patient CBT NDC
0 10 (7) 10 (8)
1-3 29 (22) 24 (20)
4-7 52 (39) 22 (17)
8-13 40 (31) 64 (51)
Not known 2 (1) 5 (4)
N 134 126
.
56
Missing Therapist ID
• Non-recording of Therapist ID for some patients.• Patient non-compliance.
Implications
• Treat missing values as clusters of size 1 in the analysis.• This form of analysis can be biases if compliant and non-
compliant patients have very different outcomes.• Ideally randomly allocate therapists to patient and apply ITT
using the allocated therapist ID.• Purposively assign a patient’s therapist at randomization of
patients and analyze accordingly.

57
Problems caused by large variation in cluster size
• Maximum cluster size places lower limit on ICC equal to -1/(max cluster size -1).
• Variable cluster size leads to loss of power.
• Problem for GEE, survey estimators, MCMC, and ML if negative variances are allowed.
Important that numbers of patients treated by each therapist do no vary greatly
58
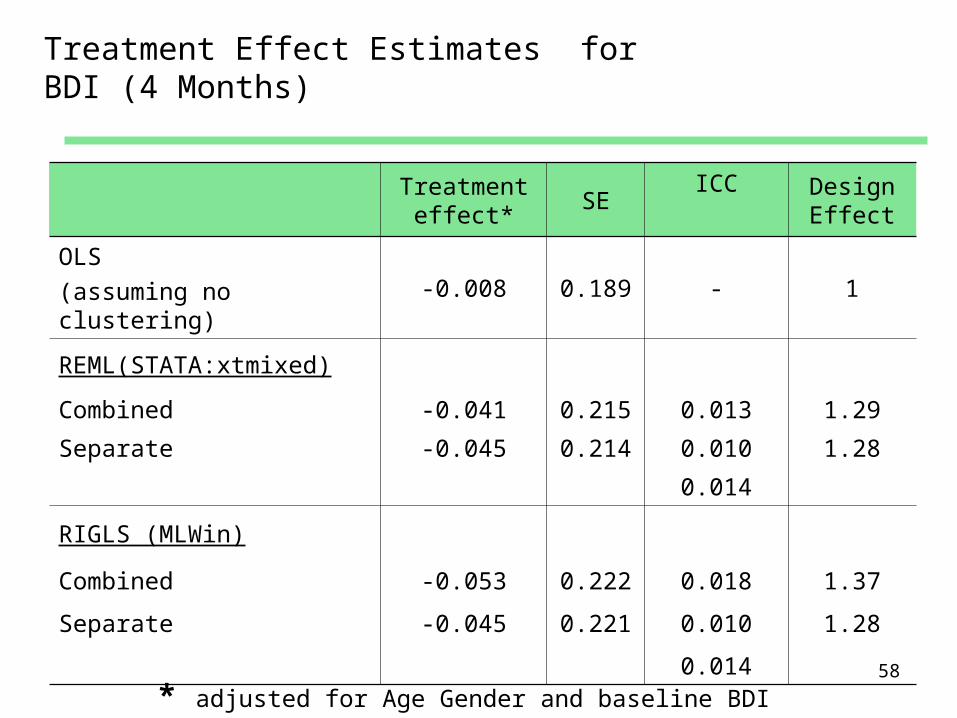
Treatment Effect Estimates for BDI (4 Months)
Treatment effect*
SEICC Design
Effect
OLS (assuming no clustering)
-0.008 0.189 - 1
REML(STATA:xtmixed)
Combined -0.041 0.215 0.013 1.29
Separate -0.045 0.214 0.010 1.28
0.014
RIGLS (MLWin)
Combined -0.053 0.222 0.018 1.37
Separate -0.045 0.221 0.010 1.28
0.014
* adjusted for Age Gender and baseline BDI

59
Treatment Effect Estimates for BDI (12 Months)
Treatment effect*
SEICC Design
Effect
OLS (assuming no clustering)
0.219 0.207 - 1
REML (STATA:xtmixed)
Combined 0.219 0.210 <0.0001 1.026
Separate 0.219 0.210 <0.0001 1.027
<0.0001
RIGLS (MLWin)
Combined 0.219 0.207 0.0 1.000
Separate 0.219 0.207 0.0 1.000
0.0
* adjusted for Age Gender and baseline BDI

60
Multiple Membership
Patient may receive of treatment from more than one therapist.
This creates a multiple-membership relationship as each patient is then clustered within two therapist.
This conflicts with the hierarchy of standard multilevel models.
Options for analysis• Define a “primary” cbt therapist (the therapist giving most sessions)
then analyze by primary therapist using hierarchical models described above
• Fit a multiple membership model.
61
Pre-testing for therapist variation
Two-stage analysis has been proposed1. Test for therapist variation. 2. Only model therapist variation if the null hypothesis is rejected.3. Otherwise do an analysis disregarding clustering.
This approach has several flaws:
• The test lacks power unless the number of therapists is large.• It is the point estimate that determines the loss of precision due
to clustering.• The analysis strategy misuses hypothesis testing as
failure to reject the null hypothesis of no therapist variation does not justify its acceptance.
62
Conclusions regarding modelling
• Pattern of clustering in therapist trials may be complex than in cluster randomised trials
• Heterogeneity of clustering needs to be consided
• Clusters due to therapist or therapy group may be poorly defined non-adherence with treatment
• Multiple membership.

63
Other options for dealing with therapist clustering
• Ignore it .
• Standardize treatment to remove between-therapist variation.
64
Ignore it
• It may be plausible to believe there is no clustering.
• Trials with small numbers of therapists are still justified as they can
demonstrate efficacy or potential effect.
• Generalisation will be theoretical based on the assumption of no
variation between therapist (“no therapist effect”) .
• External validity of such a trial is weaker having only a small
numbers of therapist.
65
Standardize treatment
• Treatment manuals.• Harmonisation of procedures.• Supervision and observation of treatment delivery.
Has been shown to reduce therapist variation, but not completely.
This approach may be fine for explanatory pilot trials considering efficacy or developing new treatments.
butStatistical analyses that ignore therapist variation are conditional on there being none.
This may not be acceptable where a treatment is to be rolled our across health services as the treatment may not be generalisable
Efficacy vs Effectiveness
66
References
• Roberts C. The implications of variation in outcome between health professionals for the design and analysis of randomized controlled trials. Statistics in Medicine 1999; 18(19):2605-2615.
• Hoover DR. Clinical trials of behavioural interventions with heterogeneous teaching subgroup effects. Statistics in Medicine 2002; 21(10):1351-1364.
• Schnurr PP, Friedman MJ, Lavori PW, Hsieh FY. Design of Department of Veterans Affairs Cooperative Study No. 420: Group treatment of posttraumatic stress disorder. Controlled Clinical Trials 2001; 22(1):74-88.
• Schnurr PP, Friedman MJ, Engel CC, Foa EB, Shea MT, Resick PM, James KE, Chow BK. Issues in the design of multisite clinical trials of psychotherapy: VA Cooperative Study No. 494 as an example. Contemporary Clinical Trials 2005; 26(6):626-636.
• Lee KJ, Thompson SG. Clustering by health professional in individually randomised trials. British Medical Journal 2005; 330(7483):142-144.
67
References II
• Roberts C, Roberts SA (2005) Design and analysis of clinical trials with clustering effects due to treatment Clinical Trials, 2:152-162
• Lee KJ, Thompson SG. The use of random effects models to allow for clustering in individually randomized trials. Clinical Trials 2005; 2(2):163-173.
• Moerbeek M, Wong WK. Sample size formulae for trials comparing group and individual treatments in a multilevel model. Statistics in Medicine 2008; 27(15):2850-2864.
• Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, for the CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacolgic treatment: Explanation and elaboration. Annals of Internal Medicine 2008; 148:295-309. (www.consort-statement.org)
• Walwyn, R. & Roberts, C. (2010). Therapist variation in randomised trials of psychotherapy: Implications for precision, internal and external validity. Statistical Methods in Medical Research 19:291-315.

68
References III
• Martindale C. The therapist-as-fixed-effect fallacy in psychotherapy research. Journal of Consulting & Clinical Psychology 1978; 46(6):1526-1530.
• Crits-Christoph P, Mintz J. Implications of therapist effects for the design and analysis of comparative studies of psychotherapies. Journal of Consulting & Clinical Psychology 1991; 59(1):20-26.
• Wampold BE, Serlin RC. The consequence of ignoring a nested factor on measures of effect size in analysis of variance. Psychological Methods 2000; 5(4):425-433.
• Elkin I, Falconnier L, Martinovich Z, Mahoney C. Therapist effects in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. Psychotherapy Research 2006; 16(2):144-160.

69
References IV
• Kim D-M, Wampold BE, Bolt DM. Therapist effects in psychotherapy: A random-effects modeling of the National Institute of Mental Health Treatment of Depression Collaborative Research Program data. Psychotherapy Research 2006; 16(2):161-172.
• Goodyer I, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, Breen S, Ford C, Barrett B, Leech A, Rothwell J, White L, Harrington R (), Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care with and without cognitive behaviour therapy in adolescents with major depression: randomised controlled trial. BMJ 2007 335(7611):142
• Ward E, King M, Lloyd M, Bower P, Sibbald B, Farrelly S, et al. Randomised controlled trial of non directive counselling, cognitive behaviour therapy and usual general practitioner care for patients with depression. I: Clinical effectiveness. BMJ 2000;321:1383 8.
70
APPENDIX I
SAMPLE SIZE &
POWER CALCULATION

71
SAMPLE SIZE & POWER CALCULATION
• Asymptotic approximation are available to calculate sample size for specified cluster sizes and numbers of clusters.
• Where sample size of therapist or groups is small (say <20 per group) non-asymptotic approximations can be used to calculate power for a given number of clusters, cluster size and intra-cluster correlations coefficient.
• With similar syntax to sampsi a user written STATA routine cluspower can calculates power were cluster size, numbers of clusters and the intra-cluster correlation coefficient differs between treatment arms. This can be used iteratively to calculate sample size.
Available from http://www.medicine.manchester.ac.uk/healthmethodology/
research/biostatistics/data/cluspower/ • clsampsi coming soon calculates sample sizes for given
power
72
APPENDIX II
STATA Code
73
STATA xtmixed syntax
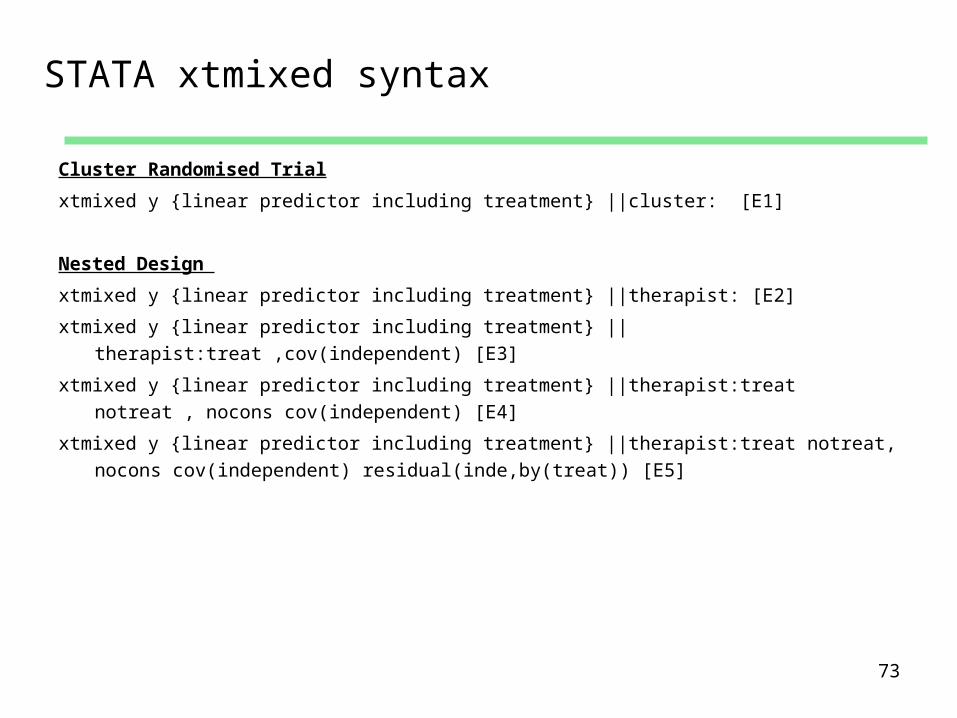
Cluster Randomised Trial
xtmixed y {linear predictor including treatment} ||cluster: [E1]
Nested Design
xtmixed y {linear predictor including treatment} ||therapist: [E2]
xtmixed y {linear predictor including treatment} ||therapist:treat ,cov(independent) [E3]
xtmixed y {linear predictor including treatment} ||therapist:treat notreat , nocons cov(independent) [E4]
xtmixed y {linear predictor including treatment} ||therapist:treat notreat, nocons cov(independent) residual(inde,by(treat)) [E5]

74
STATA xtmixed syntax
Partially Nested Design
xtmixed y {linear predictor including treatment} ||therapist:
xtmixed y {linear predictor including treatment} ||therapist:treat, nocons [E6]
xtmixed y {linear predictor including treatment} ||therapist:treat, nocons residual(inde,by(treat)) [E7]
treat and notreat are indicator variables for treatment and no treatment
Crossed Design as a 3 level model
xtmixed y {linear predictor including treatment} ||therapist:treat ,cov(unstru) [E3]
xtmixed y {linear predictor including treatment} ||therapist:||ther_treat:[E7]
which is equivalent to
xtmixed y {linear predictor including treatment} ||therapist:treat notreat , nocons cov(exch) [E4]
Note differences in random effect covariance matrix for Nested and Crossed Designs