1 NCLEX RN Preparation Program Respiratory Disorders Module 5, Part 3 of 3.
82
1 NCLEX RN Preparation Program Respiratory Disorders Module 5, Part 3 of 3
-
Upload
katy-maull -
Category
Documents
-
view
216 -
download
1
Transcript of 1 NCLEX RN Preparation Program Respiratory Disorders Module 5, Part 3 of 3.

1
NCLEX RN Preparation Program
Respiratory Disorders
Module 5, Part 3 of 3

2
Chronic Airflow Limitation
Emphysema
+
Chronic Bronchitis
=
COPD
Chronic Obstructive Pulmonary Disease
Photo Source: National Heart, Lung and Blood Institute (NHLBI http://www.nhlbi.nih.gov/health/dci/Diseases/Copd/Copd_WhatIs.html

3
Emphysema
Loss of lung elasticity
Hyperinflation
Air trapped in lungs
Alveoli over-stretched bullae

4
Chronic Bronchitis
Recurrent inflammation Vasodilation, Congestion, Edema, Spasm
Excessive thick mucus blocks air flow Hypoxemia, CO2 retained
5
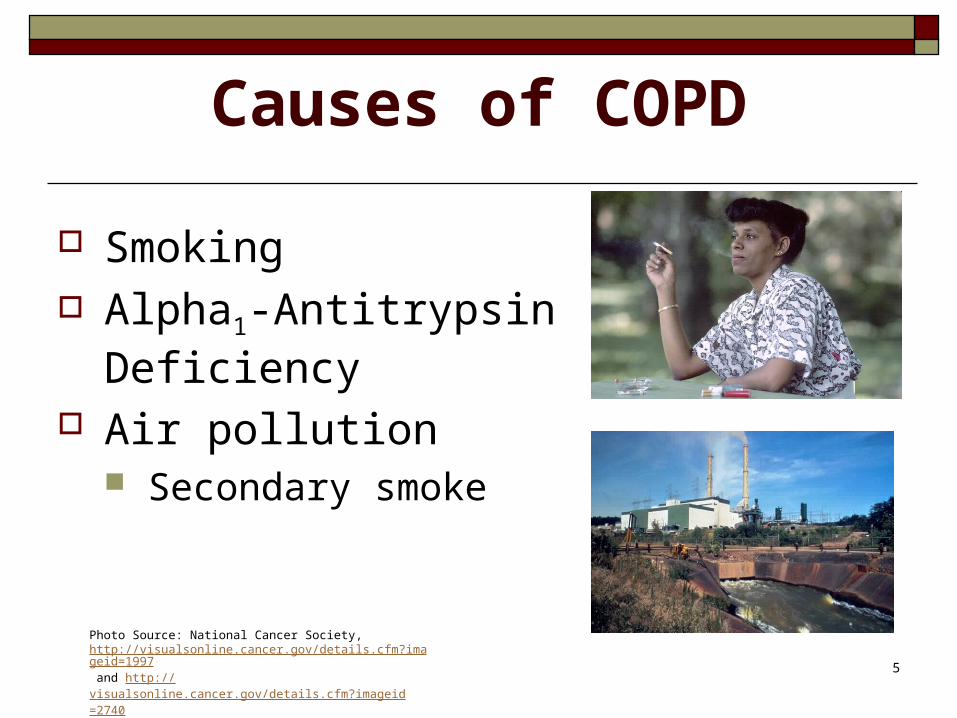
Causes of COPD
Smoking Alpha1-Antitrypsin
Deficiency Air pollution
Secondary smoke
Photo Source: National Cancer Society, http://visualsonline.cancer.gov/details.cfm?imageid=1997 and http://visualsonline.cancer.gov/details.cfm?imageid=2740

6
Signs of COPD
General Breathing Sputum Sounds Skin Finger tips

7
Assess
* LOC* Airway status and breathing* Pulses* RR, depth* BP, Heart Rate* SpO 2 level on room air* Color, temperature & capillary refill

8
Is this an emergency?
Dyspnea scale 0-10 Oxygen saturation < 90% Peak flow < 300 ml

9
Diagnostic Tests
Arterial Blood Gases Oxygen Saturation Chest x-ray Labs Pulmonary Function Tests (PFTs)

10
Goal: Patent Airway
Position Secretions Mucolytics Expectoration Hydration Humidifier

11
Teach Effective Breathing Diaphragm Pursed-lips Controlled cough Orthopneic position
http://emphysemafoundation.org/pulhthex.jsp

12
Bronchospasm
Bronchodilators Cholinergic antagonists Theophyllins

13
Inflammation Infection
Inhaled steroids Systemic steroids Prevent pneumonia Influenza vaccination yearly Pneumovax q 5 years

14
Conserve Energy
Schedule activities Don’t rush Supplemental oxygen Avoid arm raises

15
Mealtime Strategies
Rest 4-6 small meals Bronchodilator ac Easy chewing Supplements Avoid gas-producing foods

16
Stepped Therapy
1. Combivent (ipratropium + albuterol)
2. Add beta2 agonist (Albuterol)
3. Add theophyllin
4. Add Prednisone

17
Control Anxiety = Dyspnea
Develop a plan Develop support network Join support group

18
Complementary/Alternatives
Ask about non-prescribed methods used
Teach relaxation techniques

19
Pneumonia
Photo Source: Centers for Disease Control, Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Pneumonia_x_ray.jpg

20
Categories
Viral Fungal Bacterial Aspiration
Photo Source: USDS, http://www.ars.usda.gov/is/graphics/photos/sep01/k9606-20.htm]

21
Classification
Causative agent (Streptococcus pneumoniae)
Anatomic location of the infection (lobar pneumonia)
By where it was acquired (community vs. hospital/nosocomial)

22
Major Organisms
Community-acquired: Streptococcus pneumoniae (gram +) Staphylococcus aureus (gram +)
Nosocomial: Staphylococcus aureus (gram +) MRSA

23
Who is at greatest risk?
Photo Source: National Camcer Society, http://visualsonline.cancer.gov/details.cfm?imageid=1994 and http://visualsonline.cancer.gov/details.cfm?imageid=2193

24
Community Prevention
PneumovaxWash handsDon’t smokeWear mask: dusty, moldy areasAvoid crowdsEat healthy dietExercise

25
Nosocomial Prevention
Prevent aspiration - How? Prevent cross-contamination Vaccinate inpatients Education Mouth care??

26
Signs & Symptoms
Fever, chills Dyspnea, RR, shallow breathing Coughing, crackles, wheezing Pleuritic pain Anorexia Hypoxemia Sputum: purulent, blood-tinged, rusty

27
Diagnosis
Sputum C&S Leukocytosis ABG’s Blood C&S Chest x-ray Oxygen saturation

28
Goal: Improve Gas Exchange
Oxygen Antibiotics Rest Incentive spirometry Raise head of bed No smoking

29
Goal: Clear Airway
Enhance cough strength Bronchodilators Rest Mucolytics Corticosteroids

30
Goal: Control Pain and Fever
Pain Fever control Adequate volume

31
Pulmonary Tuberculosis
Photo Source: Centers for Disease Control (CDC) / Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Mantoux_tuberculin_skin_test.jpg and http://commons.wikimedia.org/wiki/Image:TB_CXR.jpg

32
Tuberculosis: What is it?
Mycobacterium tuberculosis causes inflammation in upper lungs
Bacillus colonies form a lesion (tubercle) When the colonies die, they cause
necrosis & scar tissue (consumption of tissue)
Photo Source: Centers for Disease Control (CDC) / Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Mycobacterium_tuberculosis_8438_lores.jpg

33
How do I know I have it?
Cough that will not go away Feeling tired all the time Weight loss Loss of appetite Fever Coughing up blood Night sweats

34
Diagnosis
Initial Screening – skin test Positive if >10mm induration
Chest x-ray Sputum for AFB

35
Skin Testing
Mantoux 0.1 ml PPD
48-72 hours induration
False-positive False-negative
Photo Source: Centers for Disease Control (CDC) / Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Mantoux_tuberculin_skin_test.jpg

36
Chest X-ray
To confirm positive PPD When PPD cannot be done Cavitation Caseation

37
Sputum Testing
First morning specimen 3 days Acid-fast Bacilli Tb C & S
Photo Source: Centers for Disease Control (CDC) / Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:TB_Culture.jpg

38
How is it treated?
Initial Therapy may include: Isoniazid (INH) Rifampin Pyrazinamide (PZA) Ethambutol or Streptomycin
After two months: Isoniazid Rifampin

39
Isoniazid
Precautions: Take on empty stomach, avoid antacids LFTs if liver disease
Warnings: Increases Dilantin & Tegretol levels

40
Rifampin
Precautions Body secretions turn orange May ruin contact lenses
Warnings Reduces contraceptive, methadone
effect May interact with anti-retrovirals

41
Rifapentine
Precautions Probably discolors body secretions
Warnings Decreased potency diabetes meds,
barbs, antibiotics, contraceptives

42
Ethambutol Precautions
Decreased visual acuity Decreased red-green color discrimination
Warnings Optic toxicity is dose related Increased toxicity with renal insufficiency

43
Pyrazinamide
Precautions Hepatotoxicity Nausea/vomiting Polyarthralgias Hyper-uricemia Transient rash Photo-sensitive dermatitis

44
Hospitalization
Isolate all patients with active pulmonary TB in negative-pressure rooms with high-volume air replacement and circulation
Continue isolation until combined drug treatment has been administered for 2 weeks, and three consecutive sputum smears have tested negative.

45
Transplant Recipients
Immune suppressed Donor organ with latent TB Reactivate pt’s latent infection Diagnosis difficult
Decreased PPD reaction

46
HIV positive
Increased risk: Why? Interactions with protease inhibitors Decreased CD4 cell count anergy
(impaired or absent ability to react to common antigens administered through skin) PPD testing early in HIV infection Use control to rule out anergy
?? INH prophylaxis

47
Drug Toxicity
Hx of liver disease Consuming alcohol daily Baseline + repeat LFTs Watch!
Dark urine Light stools Fatigue

48
Drug Resistance
Multi-drug resistant TB (MDRTB) Second-line drugs Increased time of treatment

49
Non-compliance
Failure of treatment Resistant bacilli Intermittent dosing? Arrest the patient?

50
Patient/Family Teaching
Prevention Phone contact Test entire family Use precautions Follow-up sputum cultures Diet

51
Acute Respiratory Failure
Dyspnea, tachycardia Progressive respiratory distress Breath sounds Mental status

52
ARDS
Aspiration Sepsis Drowning Trauma

53
Diagnostic Tests
pO2 < 60 mmHg
pCO2 > 50 mmHg
O2 saturation < 90% Chest x-ray – increasing
infiltrates to “white out”

54
Collaborative Management
Oxygen Mechanical ventilation
Photo Source: Wikimedia Commons / Public Domain image, http://commons.wikimedia.org/wiki/Image:CPR_Dummy-Air_Force.JPG

55
Intubation
Intubation tray Patient position Bed position Suction Oxygen flow meter Verify ETT placement Secure ETT
Photo Source: Centers for Disease Control (CDC) / Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Intubation.jpg

56
Mechanical Ventilation
FiO2 100%
Tidal volume (Vt) 6-7 ml/kg Rate 20-28/minute

57
Ventilators
Negative pressure Pressure cycled Time cycled Volume cycled

58
Modes of Ventilation
CMV SIMV PSV PEEP CPAP

59
Acidosis
Low pH = acidosis (normal 7.35-7.45) Low pH + low HCO3 = metabolic
acidosis (normal 21-26) Low pH + high CO2 = respiratory
acidosis (normal 35-45)

60
Alkalosis
High pH = alkalosis High pH + high HCO3 = metabolic
alkalosis High pH + low CO2 = respiratory
alkalosis

61
Ventilator Alarms
High pressure Low inspiratory pressure High respiratory rate Low exhaled volume

62
Monitor Physiological Response
Breath sounds Breathing pattern Skin color Secretions Oxygen saturation ABGs, daily chest x-ray

63
Monitor Psychological Response
Anxiety Communication Anticipate questions/needs

64
Manage the Ventilator
Correct settings? Alarms on? Maintain humidity Monitor inline temperature ETT placement, cuff Tubing adjustments

65
Prevent Complications
Barotrauma Stress ulcers Infection: Ventilator-assisted
pneumonia (VAP) Ventilator dependence Pressure necrosis

66
Weaning from Ventilator
Awake, rested Muscle strength Heart rhythm Breath sounds ABGs Pulmonary function tests

67
Weaning Methods
SIMV CPAP Pressure Support

68
Extubation
Explain procedure Prepare: nasal cannula, towel, Chux Hyper-oxygenate Suction Deflate pilot balloon Suction Pull tube No talking!

69
Pneumothorax
Signs and Symptoms Pleuritic chest pain SOB Tachypnea Tachycardia Asymmetrical chest wall
movement Decreased breath sounds Cyanosis Photo Source: Colorado State University,
http://www.cvmbs.colostate.edu/clinsci/wing/trauma/tension.htm

70
Tension Pneumothorax
Photo Source: Lippincott, Williams, & Wilkins Connection Image Bank, http://connection.lww.com/products/smeltzer9e/imagebank.asp
71
Tension Pneumothorax
Signs and Symptoms Tracheal deviation Distended neck veins Hypotension Compensatory tachycardia
& tachypnea Decreased cardiac outputMust be treated promptly

72
Hemothorax
Signs and Symptoms In addition to those seen with
pneumothorax: Subcutaneous Emphysema
(crepitus) Percussion dullness over
area of hemothorax
Photo Source: http://www.chgranby.qc.ca/trauma_formation_drain.htm

73
Nursing Care of the Chest Tube
Maintain closed system Assess, kinks, water seal, drainage
Maintain patency occlusive dressing, tubing, suction
Photo Source: Wikimedia Commons, GNU license, http://commons.wikimedia.org/wiki/Image:Chest_drain_-_bedside_with_fluids.jpg

74
Nursing Care of the Patient
Oxygen Vital signs Chest wall movement, trachea, neck
veins Position Watch for distress

75
Pulmonary Embolus
DVT Air Fat Catheter
Photo Source: National Heart, Lung and Blood Institute (NHLBI),

76
Signs/Symptoms
Classic triad Common: dyspnea, tachypnea,
pleuritic pain Pleuritic chest pain + dyspnea +
predisposing factor

77
Diagnosis
ABGs Chest x-ray V/Q scan Spiral CT Pulmonary angiogram
Photo Source: CDC/Wikimedia Commons, http://commons.wikimedia.org/wiki/Image:Pneumonia_x-ray.jpg

78
Prevention
Early ambulation Hydration Anti-embolic stockings Sequential pumps Avoid lower extremity punctures Aspirate clotted IVs SQ heparin or LMWH

79
Emergency Measures
Oxygen HOB up Support Stat ABGs, chest x-ray Prepare for code blue

80
Collaborative Management
Continue oxygen Bed rest Heparin drip Coumadin Thrombolytics? Embolectomy, umbrella filter

81
Teach
Bleeding precautions Avoid immobility Avoid dehydration Avoid aspirin products

82
Photo Acknowledgement:Unless noted otherwise, all photos and clip art contained in this module were obtained from the 2003 Microsoft Office Clip Art Gallery.