




Languages
Pages
Legal


Treatment Track
Preventing Opioid Overdose Deaths: Practical Skills for Clinicians
Presenters:
• Brian Manns, PharmD, Health Policy Fellow, Policy Research Analysis and Development Office, CDC
• Roger Weiss, MD, Professor of Psychiatry, Harvard Medical School, and Chief, Division of Alcohol and Drug Abuse, McLean Hospital
• Udi E. Ghitza, PhD, Health Science Administrator, NIDA
• Cynthia Campbell, PhD, Research Scientist, Division of Research, Kaiser Permanente, Northern California
Moderator: CDR Christopher M. Jones, PharmD, MPH, Senior Advisor, Office of Public Health Strategy and Analysis, Office of the Commissioner, FDA, and Member, Rx Summit National Advisory Board

Disclosures
• Brian Manns, PharmD; Udi E. Ghitza, PhD; and Christopher M. Jones, PharmD, MPH, have disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce healthcare goods and services.
• Roger Weiss, MD – Consulting Fees: Reckitt-Benckiser
• Cynthia Campbell, PhD – Contracted Research: Purdue Pharma

Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition

Learning Objectives
1. Explain the epidemiology of the opioid overdose crisis.
2. Describe treatment options clinicians can use to curtail opioid overdose deaths.
3. Advocate directions for advancing research and clinical practice on prevention of opioid overdose deaths.

Preventing Opioid Overdose Deaths: Practical Skills for Clinicians
Brian J. Manns, PharmD
Health Policy Fellow
Centers for Disease Control and Prevention

Disclosure Statement
Brian Manns, PharmD, has disclosed no relevant, real, or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.


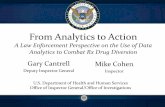
Dramatic Increase in Overdose Deaths Related to Opioid Pain Relievers
CDC, National Center for Health Statistics, National Vital Statistics System
4,030 opioid deaths in 1999
16,235 opioid deaths in 2013
Increase in heroin deaths
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Prescription Opioids
Heroin
Cocaine

Prescription Drug Monitoring Programs (PDMPs)
Source: Alliance of States with Prescription Monitoring Programs
Status of PDMPS – December 20142013

PDMP Characteristics and Provider Utilization
• PDMP registration rate ~35% 1
• 20 states require providers to register with the PDMP 2
• 22 states mandate provider usage of PDMP 2
– Variation across mandatory use situations • In all or nearly all cases when a controlled substance (CS) is
prescribed• Initially/periodically when a CS is prescribed• Only under select circumstances
– Mandatory use requirements have increased enrollment and use, impacted CS prescribing, and reduced multiple provider episodes 3
1. Prescription Drug Monitoring Program Interoperability Standards: A Report to Congress. September 2013. Available at: http://www.healthit.gov/sites/default/files/fdasia1141report_final.pdf2. NAMSDL. Recent Legislative and Regulatory Trends in Prescription Monitoring Programs. Available at: http://www.namsdl.org/library/D651C2DC-B73E-DC6A-C450A4863CC1F73C/3. Prescription Drug Monitoring Program Center of Excellence at Brandeis. Mandating PDMP participation by medical providers: current status and experience in selected states. Available at: http://www.pdmpexcellence.org/sites/all/pdfs/COE_briefing_mandates_2nd_rev.pdf

PDMP Monitoring of Controlled Substances
PA will begin collecting data on all schedules of substances on June 30, 2015
CS Collected States/Territories Number
Schedule II only PA 1
Schedules II-IVAZ, CA, FL, IA, KS, ME, NV, NH, OR, RI, SC, VT, VA, WV, WY
15
Schedules II-V
AL, AK, AR, CO, CT, DE, DC, GA, GU, HI, ID, IL, IN, KY, LA, MD, MA, MI, MN, MS, MT, NE, NJ, NM, NY, NC, ND, OH, OK, SD, TN, TX, UT, WA, WI
35

Demographics
• Men
• 35-54 year olds
• Whites
• American Indians/Alaska Natives
Risk Factors for Overdose
Socioeconomics and Geography
• Medicaid
• Rural
Clinical Characteristics
• Chronic pain
• Substance abuse
• Mental health
• Nonmedical use
• Multiple prescriptions
• Multiple prescribers
• High daily dosage

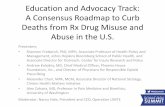
Overdose Risk Highest Among Small Percentage of Patients at High Dosage, Group Health, 1997-2005
11.44
3.73
8.87
0
10
20
30
40
50
60
70
80
90
100
0
1
2
3
4
5
6
7
8
9
10
1-19 20-49 50-99 100+
% P
ati
en
t Y
ea
rs
Ris
k (
Od
ds
Ra
tio
)
Opioid dosage (MME/d)
Dunn et al, Opioid prescriptions for chronic pain and overdose. Ann Int Med 2010;152:85-92.

PDMP Value to Clinical Care
• Identifying patients at highest risk for overdose
– Elevated Morphine Milligram Equivalence Dose
– Polypharmacy
– Concurrent/Overlapping Prescription
• Potential Drug Interactions
– Substance Use Disorder
• Promote conversation or referral to treatment
• Protect patient from serious or fatal harm
– Opportunity for tapering and avoiding withdrawal

Examples of PDMP Added Value
• Identification of high risk use
– Baumblatt (2014) used Tennessee PDMP data to identify risk factors accounting for 55% of overdose deaths
– Katz (2009) used Massachusetts PDMP data to identify pharmacy and prescriber visit patterns

Practical Steps for Providers When Accessing the PDMP to Reduce Risk
• High number of scripts, providers, pharmacies – Discuss concerns when suspecting SUD
• Consider criteria for SUD and referral to treatment– SAMHSA Buprenorphine Physician and Treatment Locator
(http://buprenorphine.samhsa.gov/bwns_locator/)
– Communicate concerns for patient safety if not seeing an improvement in function
– Use MME to assess risk for overdose– Address potential drug interactions
• Educate patients about risks • Avoid a medication plan that includes potentially dangerous
combinations (e.g. benzodiazepines and opioids)
– Avoid abrupt discontinuation of opioids or benzodiazepines

CDC PDMP Activities
• PEHRIIE – PDMP Electronic Health Record Integration and Interoperability Expansion Project
• PBSS – Prescription Behavior Surveillance System
• Prescription Drug Overdose: Boost for State Prevention
• Prevention for States Program

PEHRIIE
• Cooperative Agreement – SAMHSA and CDC
• Improve prescribing and dispensing practices
– Integration of PDMP data into EHRs and other health information technology (pharmacy systems)
– Interoperability of PDMPs across state lines.

PBSS
• 11 states currently provide data to PBSS
• PBSS indicators over time and by demographic and controlled substance drug categories
– Patient-Level Behavior
– Prescriber-Level Behavior
– Dispenser-Level Behavior

Prevention BOOST
• Maximizing PDMPs– Expanding interstate data sharing between PDMPs
across state borders
– Refining proactive PDMP reports to identify and address inappropriate prescribing patterns
– Shortening the PDMP reporting interval to make PDMP data more timely and useful
– Leveraging PDMPs as public health surveillance systems to better understand what drives overdose deaths

Prevention for States
• More intense effort to enhance and maximize PDMPs
– Streamline and simplify PDMP registration process
– Data sharing between PDMPs and EHRs
– Support proactive reporting and data analysis
– Move toward a real-time PDMP

Thank You
The findings and conclusions in this report are those of the author and do not necessarily
represent the views of the Centers for Disease Control and Prevention.
Brian J. Manns - - [email protected]

Treatment of Prescription Opioid Dependence
Roger D. Weiss, MDHarvard Medical School
McLean Hospital, Belmont, MANew England Consortium Node, NIDA Clinical Trials
Network

Disclosure
Roger D. Weiss, MD wishes to disclose that he has consulted to Reckitt-Benckiser. He will present this content in a fair and balanced
manner.

Overdose prevention
• Effective treatment is the best way to prevent overdoses
• Most studies of opioid dependence treatment have focused on heroin addicts in methadone maintenance treatment
• It is not clear the degree to which this applies to those with prescription opioid dependencereceiving office-based buprenorphinetreatment

Prescription Opioid Addiction Treatment Study (POATS)
• Compared treatments for prescription opioid dependence, using
– buprenorphine-naloxone (bup-nx) of varying durations
– counseling of varying intensities
• Conducted as part of National Institute on Drug Abuse Clinical Trials Network (NIDA CTN)
• 10 participating sites across the U.S.
• Largest study ever conducted for prescription opioid dependence (N=653)
Weiss RD et al. Arch Gen Psychiatry. 2011;68(12):1238-1246

POATS study questions
• Does adding individual drug counseling to bup-nx+SMM improve outcome? – May be a proxy for drug abuse treatment program
vs. office-based opioid treatment, using bup-nx
• What length of bup-nx is best for these patients? – 1-month taper?
– 3 months, then taper?
– Longer-term maintenance?

Key eligibility criteria
• DSM-IV dx of opioid dependence, not just physical dependence
• ≥20 days opioid use in past 30 days
• Additional SUDs eligible if not requiring immediate medical treatment
• Non-psychotic, psychiatrically stable
• Minimal or no heroin use (never dependent or injected, <5 d in past 30

Phase 1, up to 12 weeks

Phase 2, 24 weeks

POATS Main Trial Results

Successful outcome, Phase 1 (N=653)
Phase 1 successful outcome criteria
• ≤4 days opioid use per month
• No positive urine screens for opioids on 2 consecutive wks
• No other formal substance abuse treatment
• No injection of opioids
• No more than 1 missing urine sample during the 12 weeks
SMM + ODC SMM p
6% 7% .36
Weiss RD et al. Arch Gen Psychiatry. 2011;68(12):1238-1246

Successful outcome, Phase 2 (n=360)
Phase 2 successful outcome criteria
• Abstinent for ≥3 of final 4 weeks (including final week) of bup-nx stabilization (urine-confirmed self-report)
SMM +ODC
SMM p
Week 12
(end of stabilization)52% 47% .3
Weiss RD et al. Arch Gen Psychiatry. 2011;68(12):1238-1246

Phase 2: Successful outcome at end of taper & at follow-up
SMM +ODC
SMM Overall p
Week 16
(end of taper)28% 24% 26% .4
Week 24
(8 wks post-taper)10% 7% 9% .2
Weiss RD et al. Arch Gen Psychiatry. 2011;68(12):1238-1246

POATS Recent Findings

Patient characteristics associated with buprenorphine/naloxone treatment outcome for Rx opioid dependence
Dreifuss et al., DAD, 2013

Significant baseline predictors by outcome: Bivariate analysis (N=360)
0
10
20
30
40
50
60
70
80
90
100
Self-help* Other priortreatment*
Route of usenot as
prescribed**
OxyContinused most in
past 30days**
%
of
pa
tie
nts
Fail
Success
*p<.05, **p<.01

Significant predictors by outcome (cont’d)
Patient characteristics
at baseline
Failure
(n=183)
Successful
(n=177)Sociodemographics
Age, mean (sd)** 31 (9) 34 (10)
Opioid use history
Used heroin* 32% 20%
1st source* Medical Rx 49% 62%
Dealer 14 6
1st reason for use* To relieve pain 60 70
To get high 33 24
Other diagnoses
Major depression** Past year 14 26
Lifetime 27 41
*p<.05, **p<.01

Logistic Regression Model for Predictors of Success (N=360)
Baseline variables Odds ratio
Age, for every +10 years 1.28*
Lifetime major depression 1.82*
Prior opioid use disorder treatment .62*
Lifetime route of use other than oral or
sublingual .51^
^p<.052, *p<.05
39

Who benefits from additional drug counseling among Rx opioid
dependent pts receiving bup-nx and standard medical management?
Weiss et al., DAD, 2014

Key study questions
Do subgroups of Rx opioid dependent patients benefit from more intensive treatment, i.e., drug counseling in addition to bup-nx and standard medical management?
Compared patients with• More severe problems• Greater attendance at treatment sessions, i.e.
adherence• The interaction of the two

Did drug counseling improve outcomes in more severe patients?
Illness severity operationalized as• ASI drug composite score (mean=.34)• Heroin use (26%)• Chronic pain (41%)
RESULTSHeroin users were half as likely to have successful outcomes, but this was not related to being randomized to drug counseling.
The remaining severity measures were not associated with outcome.

Adequate attendance/adherence to treatment
Sessions offered during 12-week Phase 2• Medical management (360): 17• Drug counseling (180): 18 (plus 17 MM)
Adequate adherence set a priori at ≥60% of both MM + drug counseling sessions offered:74% of patients met this criterion
RESULTSAmong patients with adequate attendance/adherence (n=266), treatment assignment was not related to outcome.

Did patients with more severe problems have better outcomes if assigned to drug counseling?
(n=266 with adequate adherence)
Interaction between heroin & treatment p=.03

Interpretation of results
• Heroin users were as likely to succeed as non-heroin users if they were randomized to drug counseling and went (i.e., were adherent).
• Adherent heroin users assigned to SMM alone were half as likely to succeed as all other adherent Rx opioid patients.

Implications
Perhaps there are clinically meaningful subgroupsof patients with prescription opioid dependence• Older • Depressed • Initiated use for pain
vs. • Younger, more “recreational” users, including
heroin users• Latter group may require and benefit from more
intensive counseling (if they attend)

Does early response to buprenorphine-naloxone predict
treatment outcome in prescription opioid dependence?
McDermott et al., J Clin Psychiatry, 2015

Research questions
1) Is it possible to tell early in treatment whether a prescription opioid dependent patient will have a successful bup-nxoutcome?
2) How early can bup-nx treatment response be evaluated accurately?

Methods
Positive predictive value = the degree to which initial opioid abstinence predicted final successful outcome at the end of bup-nxstabilization.
Negative predictive value = the degree to which initial opioid use predicted final unsuccessful outcome at the end of bup-nx stabilization.

Predicting abstinence at end of tx(weeks 9-12)
Initial abstinence
and final
abstinence, n
Initial abstinence
and final lack of
abstinence, n
Positive
Predictive Value,
%
Week 1 101 107 49%Weeks 1-2 88 70 56Weeks 1-3 73 54 57Weeks 1-4 68 45 60

Predicting use in weeks 9-12
Initial use and final lack
of abstinence, n
Initial use and final
abstinence, n
Negative
Predictive Value,
%
Week 1 122 30 80%Wks 1-2 89 6 94Wks 1-3 72 3 96Wks 1-4 58 2 97

Acknowledgements
McLean CTN-0030 research team, with
3 World Series trophies
Our home base: Proctor House, McLean Hospital

Acknowledgements, cont’d
• Investigators, clinicians, & patients at the 10 study sites
• Jennifer Potter, Ph.D., M.P.H. and Walter Ling, M.D.
• CCTN, CCC, and DSC-1 staff
• NIDA Grants U10DA15831 & K24DA022288

54Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Session - Preventing Opioid Overdose Deaths: Practical Skills for Clinicians
Udi E. Ghitza, Ph.D.Health Scientist AdministratorNational Institute on Drug Abuse (NIDA)
April 7, 2015

55Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Disclosure statement
Udi E. Ghitza, Ph.D. has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
The opinions in this presentation are those of Udi E. Ghitza, Ph.D. and do not represent the official position of the U.S. government.

56Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Learning objectives of session
1. Explain epidemiology of the opioid overdose crisis.
2. Describe treatment options clinicians can use to curtail opioid overdose deaths.
3. Advocate directions for advancing research and clinical practice on prevention of opioid overdose deaths.
This talk’s focus: New treatment option for opiate use disorders, treatment as a potential means of curtailing opioid overdose deaths

57Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Rates of prescription painkiller sales, deaths and substance abuse treatment admissions (1999-2010)

58Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Specific Illicit Drug Dependence or Abuse in the Past Year among Persons Aged 12 or Older: 2013
Reference: Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2013
National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: SAMHSA, 2014.

59Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Relapse rates for opiate use are high despite available medication-assisted treatment options
Prescription pain relievers that are full μ-opioid receptor agonists are same class of drugs as heroin.
FDA-approved medication-assisted treatments (MAT) for opiate use disorders:
Buprenorphine/naloxoneMethadoneNaltrexone
MAT are adjuncts to evidence-based psychosocial treatments
However, discharges from MAT programs and relapse rates remain high.
Reference: Substance Abuse and Mental Health Services Administration (SAMHSA). Treatment Episode Data Set (TEDS):
2011. Discharges from Substance Abuse Treatment Services. Chapter 8. Rockville, MD: SAMHSA, 2014.

60Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Clonidine maintenance prolongs opioid abstinence anddecouples stress from craving: a randomized controlled trial (RCT) with ecological momentary assessment
• Placebo-controlled RCT testing effectiveness of clonidine (alpha-2 adrenergic receptor agonist) added to buprenorphine to reduce lapses to and extend abstinence from opiate use in opiate-use-disorders patients
• 118 participants who maintained opiate abstinence during weeks 5-6 were continued on buprenorphine and randomized to clonidine (n=61) or placebo (n=57) for 14 weeks.
• Urine was tested thrice weekly.
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

61Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Clonidine maintenance prolongs opioid abstinence and decouples stress from craving: a randomized controlled trial (RCT) with ecological momentary assessment
• Clonidine plus buprenorphine produced longest duration of consecutive days of abstinence from opiates during intervention, versus placebo + buprenorphine (34.8±3.7 days versus 25.5±2.7 days, P<0.05, Effect size: d=0.38).
• Clonidine group also took longer to lapse (hazard ratio:0.67, 95% CI=0.45-1.00, P<0.05).
• Ecological momentary assessment showed daily-life stress was decoupled from opiate craving in the clonidine group (interaction F(3,257)=8.8, P<0.01).
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

62Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
The effect of clonidine on longest periodof opioid abstinence
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

63Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
The effect of clonidine on time to opioid lapse
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

64Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Conclusions
• Clonidine may be useful off-label in treating opiate use disorders, not just to reduce withdrawal signs, but also as an adjunct maintenance treatment that increases duration of opiate abstinence and delays lapses
• Even in absence of withdrawal, it decouples stress from craving
• Participants in the clonidine group were not more likely to report an adverse event compared with placebo. Therefore, the doses of clonidine used appear to be safe and well tolerated in this population.
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

65Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Clinical Implications
• Clonidine may effectively work off-label as a maintenance medication and adjunct to buprenorphine to enhance prevention of lapses to opiate use and prolong abstinence.
• This is a major new use for a readily available old drug.
• Clinicians have more options in their toolbox to prevent lapses to opiate use and enhance abstinence in opiate-dependent patients.
Reference: Kowalczyk, Phillips, Jobes, Kennedy, Ghitza…Preston (2015) The American Journal of Psychiatry (in press)

66Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Acknowledgments
• Kenzie L. Preston Ph.D., NIDA Intramural Research Program (IRP)
• William J. Kowalczyk Ph.D., NIDA IRP
• Karran A. Phillips M.D., NIDA IRP
• Michelle J. Jobes Ph.D., NIDA IRP
• Ashley P. Kennedy Ph.D., National Institute of Mental Health (NIMH)
• Daniel A. Agage M.D., NIDA IRP
• John P. Schmittner M.D., Spectrum Health System
• David H. Epstein Ph.D., NIDA IRP

67Opiate use disorders treatment:
Importance of effective relapse-
prevention medications
Udi E. Ghitza, Ph.D.
Health Scientist Administrator
National Institute on Drug Abuse (NIDA)
Thank you!

Addressing the Prescription Opioid Crisis in Health Systems: Role of EHRs and RegistriesPreventing Opioid Overdose Deaths: Practical Skills for Clinicians
Cynthia Campbell, PhD, Constance Weisner, DrPHKaiser Permanente Division of Research
Drug and Alcohol Research Team
National Rx Drug Abuse Summit, Atlanta, GA
April 7, 2015

Disclosures
• Cynthia Campbell, PhD – Contracted Research: Purdue Pharma

Overview• What we know from studying a health plan
– Long-term opioid use – patient characteristics
– Substance abuse, depression, adverse events
• Clinical implications
– EHR-supported registries
• What goes into an EHR
• How this informs clinical tools and registries
• Clinician Query Tool

Prescription Opioid Problem: Context for Health Care Systems

Integrated health care delivery system (medical, psychiatry & AOD services)
3.6 + million members (45% of market share, diversity increasing with ACA)
Longitudinal data & long membership enrollment
Harmonized data with 18 health plans

Pain and Opioids: Challenges in a Health System
• Complex patients, high utilizers
• Health systems very interested• Chronic pain programs
• Purchasers very interested
• Highlighted SU as a problem• Identifying misuse

Trends in Prescription Opioid Use in Health Systems: Substance Abuse History

0%
10%
20%
30%
40%
50%
60%
1997
1998
1999
2000
2001
2002
2003
2004
2005
Prevalence of Long-Term Opioid Use by Substance Use Diagnosis (diagnosis in prior 2 years)
Prevalence
long-term
opioid use
No Drug or Alcohol (including Opioid)
diagnosis
Kaiser N California Group Health
Supported by NIDA Grant R01 DA022557
Weisner CM, Campbell CI, Ray GT, Saunders K, Merrill JO, Banta-Green C, Sullivan MD, Silverberg MJ, Mertens JR, Boudreau D, Von Korff M. Trends in prescribed opioid therapy for non-cancer pain for individuals with prior substance use disorders. Pain 2009;145(3):287-293.

0%
10%
20%
30%
40%
50%
60%
1997
1998
1999
2000
2001
2002
2003
2004
2005
Prevalence of Long-Term Opioid Use by Substance Use Diagnosis (diagnosis in prior 2 years)
Prevalence
long-term
opioid use
Drug or Alcohol Diagnosis
No Drug or Alcohol (including Opioid)
diagnosis
Kaiser N California Group Health

0%
10%
20%
30%
40%
50%
60%
1997
1998
1999
2000
2001
2002
2003
2004
2005
Prevalence
long-term
opioid use
Opioid Disorder Diagnosis
Drug or Alcohol Diagnosis
No Drug or Alcohol (including Opioid)
diagnosis
Prevalence of Long-Term Opioid Use by Substance Use Diagnosis (diagnosis in prior 2 years)
Kaiser N California Group Health

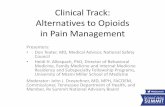
Prevalence of Long-Term Opioid Use by Depression Dx in Prior 2 Years, 1997-2005
Kaiser N California (solid lines) & Group Health (dashed lines)
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
1997
1998
1999
2000
2001
2002
2003
2004
2005
Prevalence (%)
of long-term
opioid use
Depression Dx
No Depression Dx
Braden J, Sullivan MD, Ray GT, Saunders K, Merrill J, Silverberg MJ, Rutter CM, Weisner C, Banta-Green,
Campbell CI, Von Korff M, et al. (2009). Trends in Long-term Opioid Therapy for Non-Cancer Pain among Persons
with a History of Depression. General Hospital Psychiatry. 31(6):564-70

Opioid overdoses (fatal and non-fatal)
• Higher dosage levels related to higher likelihood of overdose– Patients with highest dose (100 mg/d+) had highest risk (HR=8.9, 95% CI 4.0-
20) compared with patients receiving 1 to 20 mg/d
• Those with highest dose compared with lowest:
– Male, substance abuse , current smokers, depression, higher Charlson comorbidity scores
Dunn KM, Saunders KW, Rutter CM, Banta-Green CJ, Merrill JO, Sullivan MD, Weisner CM, Silverberg MJ, Campbell CI, Psaty BM, Von Korff M. (2010). Opioid prescriptions for chronic pain and overdose. Annals of Internal Medicine. 152(2):85-92
Controlled for age, sex, smoking, depression diagnosis, substance abuse diagnosis, index
pain diagnosis, and chronic disease comorbidity adjustors

Electronic health record and opioid registries: Clinical implications

What is a registry?
• Continually refreshed database on a group of people meeting certain criteria
• Provides up-to-date information (e.g. clinical characteristics, health care utilization, medication use)

Example: Prescription Opioid Registry
• Proof-of-concept project with NIDA to explore use of EHR
• Looking across four years (2010-2014)
• Creating daily records of opioid use as well as episodes of use with varying criteria
• Data elements include:– Pharmacy data: new and long term prescription opioid users, opioid
misuse, overdose and poisoning, mortality, other adverse events (e.g. fractures).
– Demographics, socioeconomic, comorbidities
– Health services use
• Can refresh periodically to make a “living” registry

Registry Development
Health System/Clinical
EncountersEHR Registries

Health System Encounters
Primary Care Specialty
(Substance use, Mental
Health)
Hospital
Health IT
Pharmacy
Laboratory

Integration of Substance Use
Specialty Care
Primary Care
Screen and treat in PC
(if moderate problem,
continue monitoring)
Specialty care if needed
Back to primary care for
monitoring
Bodenheimer T, Wagner E, Grumback K. Improving primary care for patients with chronic illness. JAMA .
2002; 288:1775-1779.
Von Korff M, Gruman J, Schaefer J, Curry SJ, Wagner E. Collaborative management of chronic illness.
Ann Intern Med. 1997; 127(12):1097-1102.
Chi FW, Parthasarathy S, Mertens JR, Weisner C. (2011) Continuing care and long-term substance use
outcomes in managed care: initial evidence for a primary care based model. Psychiatr Serv.
2011;62(10):1194–1200.






How Does A Registry Develop?
Health System/Clinical
EncountersEHR Registries

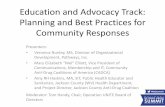
Transforming Healthcare Data Into Usable Information
92
Utilization
Research Database
Data Span: 1960 – Current
REG+ (Legacy ED & Clinic encounters)
Diagnosis Procedures
Pharmacy Lab Results Lab Notes
EnrollmentDemographic
sECG
ProvidersRehabilitatio
nVitals
Enrollment
SSA Death
CA Death
Cancer/SEERCause of
deathCensus
DiabetesMellitus
IP Clinical Warehouse
KidneyDisease
OSCR (Legacy ED & Clinic Diagnoses & Procs)
AOMS (Referrals for Contracted Non-KP Care)
CATS (Non-KP Emergency Claims)
eConsult (Referrals within KP)
ADT (Legacy Hospital Diagnoses & Procedures)
KITS (Immunization)
LURS (Inpatient & Outpatient Labs)
CPM (Facilities)
PATDEM (Patient Demographic Features)
TRRS (Radiology Reports)
FRSS (Provider Info)
PARRS (KP Appointments)
CAMMOLOT/COPS (Legacy Chemotherapy)
TraceMaster (ECGs)
CoPath (Pathology)
KP.Org
KP HealthConnect (Clarity)
Mortality
Cancer Registry
RPGEHAd-hoc SAS Data Sets
KP CESR Virtual Data Warehouse
FDA Mini-Sentinel Common Data Model
Web Application
Oracle 11G
14TB
KP Virtual Data Warehouse (VDW)

How Does A Registry Develop?
Health System/Clinical
EncountersEHR Registries
Data cleaning, algorithm development, QC, clinical consult

How Can Registries Be Used?• Can identify high risk patients according to various criteria• Track outcomes of interest over time
– Long term use– Poisoning/overdose, abuse/dependence, ER use
• Examine comorbidities• Family members• Correlation with other health outcomes with access to the whole
medical record, other registries• Can target certain populations for disease management
– Cancer Registry, HIV Registry, Diabetes, Preventing Heart Attack and Stroke Registry (PHASE)
• Treatment and care processes• Can identify providers of these patients for interventions• Collaborating with other health systems to create networks
– Potential for surveillance for some substances– Common Data Elements

How Clinicians Use These Data
Data Warehouse/Registries
Query Tool



VDW Query Tool Capabilities
• Web-based interface for querying• Flexible, fast• Draws from multiple data sources, including registry
data• Large-volume, longitudinal data• Basic and advanced queries• Breakdown by patient demographics and KP facility• Results delivered to browser, Excel export, or e-mail• Save, re-run and re-edit queries• As good as the user’s questions
98

Implications
• Exciting time– Integration of SU treatment with primary care
– EHRs more widely available
• More data becoming available in the EHR that can feed SUD registries
• More information available to help manage patients– Development of clinical tools
– Health IT

AOD Research at Division of ResearchPrincipal InvestigatorsCynthia Campbell, PhDLyndsay Ammon Avila, PhDDerek Satre, PhDStacy Sterling, MSW, MPHKelly Young-Wolff, PhDConnie Weisner, DrPH, LCSW
Health EconomistSujaya Parthasarathy, PhD
Senior Research AdministratorAlison Truman, MHA
Analysts/BiostaticiansFelicia Chi, MPHAndrea H Kline Simon, MSWendy Lu, MPHTom Ray, MBA
Interview SupervisorGina Smith Anderson
Project ManagerMonique Does, MPHLuisa Hamilton
Project CoordinatorsSabrina Wood, BA
Research Associates Georgina BerriosVirginia BrowningNancy CharvatMelanie JacksonElinette NicholsDiane Lott-GarciaIrene Kane
KPNC Members
KPNC Primary Care
KPNC Chemical Dependency Quality Improvement Committee
KPNC Adolescent Medicine Specialists Committee
KPNC Adolescent Chemical Dependency Coordinating Committee
KPNC Oakland Pediatrics Department
KPNC ADHD Steering Committee
KPNC Regional Mental Health and Chemical Dependency
Research Clinicians
Thekla B Ross, PsyD
Ashley Jones, PsyD
Amy Leibowitz, PsyD
Catherine Marino, PsyD
Clinical Partners
Anna Wong, PhD
Charles Wibbelsman, MD
David Pating, MD
Barry Levine, MD
Charles Moore, MD, MBA
Don Mordecai, MD
Cosette Taillac, LCSW
Murtuza Ghadiali, MD
Mason Turner, MD
Andrea Rubinstein, MD

Treatment Track
Preventing Opioid Overdose Deaths: Practical Skills for Clinicians
Presenters:
• Brian Manns, PharmD, Health Policy Fellow, Policy Research Analysis and Development Office, CDC
• Roger Weiss, MD, Professor of Psychiatry, Harvard Medical School, and Chief, Division of Alcohol and Drug Abuse, McLean Hospital
• Udi E. Ghitza, PhD, Health Science Administrator, NIDA
• Cynthia Campbell, PhD, Research Scientist, Division of Research, Kaiser Permanente, Northern California
Moderator: CDR Christopher M. Jones, PharmD, MPH, Senior Advisor, Office of Public Health Strategy and Analysis, Office of the Commissioner, FDA, and Member, Rx Summit National Advisory Board
Top Related