


Languages
Pages
Legal


1
New Frontiers and Pivotal Clinical Advances for the
Pathoimmunobiology of Atopic Dermatitis
The Translational Path in Atopic Dermatitis and the Implications for Dermatology Practice
A Year 2016‐2017 Science‐to‐Practice Update for the Dermatological Specialist
PROFESSOR EMMA GUTTMAN, MD, PhD – Program ChairProfessor and Vice Chair, Dermatology
Director, Center for Excellence in Eczema and Laboratory for Inflammatory Skin DiseasesIcahn School of Medicine at Mount Sinai Medical Center

2
CME‐certified symposium jointly provided by Advancing Knowledge in Healthcare (AKH) and CMEducation Resources, LLC
Commercial Support: Supported by an independent educational grant from Sanofi Genzyme and Regeneron Pharmaceuticals
Faculty disclosures: Listed in program materials
This CME activity may include discussions of off‐label or unapproved uses of specific agents
Welcome and Program Overview
We Request That You…
►PLEASE FILL OUT
QUESTION AND ANSWER (Q&A) CARDS as program proceeds so we can collect them and discuss during the Q&A session
COURSE SURVEY: Please hand all survey forms to staff at the desk outside following the program
CME CREDIT can be received by completing the online evaluation/claimed credit form atwww.akhcme.com/aderm (listed in your program materials)

3
Continue Learning With UsEnduring Materials from This Symposium
• This entire program will be available as a CME Clinical Excellence WebCAST on multiple clinical websites, including www.BiologicsCAST.com
• PowerPoint slides from today’s program will be available for download
• Clinical questions about atopic dermatitis management may be submitted to www.iQandA‐CME.com
Distinguished Program Faculty
PROFESSOR EMMA GUTTMAN, MD, PhDProfessor and Vice Chair, DermatologyDirector, Center for Excellence in Eczema and Laboratory for Inflammatory Skin DiseasesIcahn School of Medicine at Mount Sinai Medical Center New York, NY
PROFESSOR MARK LEBWOHL, MD Sol and Clara Kest Professor and ChairmanKimberly and Eric J. Waldman Department of DermatologyIcahn School of Medicine at Mount SinaiNew York, NY
PROFESSOR LISA A. BECK, MDProfessor, Department of Dermatology and Medicine (Allergy/Immunology and Rheumatology) University of Rochester Medical Center School of Medicine and Dentistry Rochester, NY

4
New Frontiers and Pivotal Clinical Advances for the
Pathoimmunobiology of Atopic Dermatitis
The Translational Path in Atopic Dermatitis and the Implications for Dermatology Practice
PROFESSOR EMMA GUTTMAN, MD, PhD – Program ChairProfessor and Vice Chair, Dermatology
Director, Center for Excellence in Eczema and Laboratory for Inflammatory Skin DiseasesIcahn School of Medicine at Mount Sinai Medical Center
A Year 2016‐2017 Science‐to‐Practice Update for the Dermatological Specialist

5
Translational Revolution in AD
In the last decade there is a real revolution in atopic dermatitis research with rapid therapeutic development, further amplifying our current disease understanding
These therapeutic developments are giving our AD patients hope for a better future and quality of life
This symposium will present current data on disease pathogenesis, the unmet need and the emerging systemic nature of AD, suggesting the need for systemic treatments for patients with severe AD
It will also present data on disease control using systemic treatments
Translational Revolution in AD

6
Overview
Overview of Therapeutic Advances in AD (Dr Mark Lebwohl)
Evolving Pathogenic Concepts On Atopic Dermatitis (AD) and Its Systemic Nature with Implications for Targeted Therapeutics (Dr. Emma Guttman‐Yassky)
Review of Published Clinical Trials and How This is Likely to Change Our Approach to the Treatment of AD (Dr. Lisa Beck)
Summary, future directions, questions (all)

7
Therapeutic Advances inAtopic Dermatitis
A Year 2016‐2017 Mechanism‐to‐Practice UpdateFocused on Biologic Therapies
Professor Mark Lebwohl, MD Sol and Clara Kest Professor
and ChairmanKimberly and Eric J. Waldman Department of Dermatology
Icahn School of Medicine at Mount Sinai
Mount Sinai Gets Dollars From:
► Amgen
► Anacor
► Boehringer Ingleheim
► Celgene
► Lilly
► Janssen Biotech
► Kadmon
►LEO Pharmaceuticals
► Medimmune
► Novartis
► Pfizer
► Sun Pharmaceuticals
► Valeant

8
Optimist: Glass is half fullPessimist: Glass is half emptyRealist: Glass is half full and half empty
The Clinical Dilemma in AD
► No universally accepted biomarker to define disease stages, severity or clinical success
► >20 instruments to assess disease severity in clinical trials that differ in items and domains they include and most have not been sufficiently validated● Treatment effects cannot be readily compared and meta‐analyses
are difficult
● Impacts evidence‐based management
Unmet need for effective therapy of moderate and severe atopic dermatitis

9
IL-17AIL-17FIL-17R
IL-12
Antimicrobial peptidesIL-1βIL-6
TNF-αS100
CXCL8CXCL9
CXCL10CXCL11CCL20
ActivationNatural
killer T cell
Keratinocyte
Myeloiddendritic cell
Plasmacytoid dendritic cell
Macrophage
IL-1βIL-6
TNF-αTNF-αINF-γ
INF-γ
Th1 cell
Th17 cell
TNF-αINF-γ
Keratinocyte
TNF-α
Adaptive immunity
Innate immunityInnate immunity
IL-20
Adapted from: Nestle F, et al, NEJM 2009; 501.
Pathogenesis of PsoriasisMechanism of Alefacept
Th22 cell
IL-22
IL-20
IL-23
IL-17AIL-17FIL-17R
IL-12
Antimicrobial peptidesIL-1βIL-6
TNF-αS100
CXCL8CXCL9
CXCL10CXCL11CCL20
ActivationNatural
killer T cell
Keratinocyte
Myeloiddendritic cell
Plasmacytoid dendritic cell
Macrophage
IL-1βIL-6
TNF-αTNF-αINF-γ
INF-γ
Th1 cell
Th17 cell
TNF-αINF-γ
Keratinocyte
TNF-α
Adaptive immunity
Innate immunityInnate immunity
IL-20
Adapted from: Nestle F, et al, NEJM 2009; 501.
Mechanism of Cyclosporine
Th22 cell
IL-22
IL-20
IL-23

10
IL-17AIL-17FIL-17R
IL-12
Antimicrobial peptidesIL-1βIL-6
TNF-αS100
CXCL8CXCL9
CXCL10CXCL11CCL20
ActivationNatural
killer T cell
Keratinocyte
Myeloiddendritic cell
Plasmacytoid dendritic cell
Macrophage
IL-1βIL-6
TNF-αTNF-αINF-γ
INF-γ
Th1 cell
Th17 cell
TNF-αINF-γ
Keratinocyte
TNF-α
Adaptive immunity
Innate immunityInnate immunity
IL-20
Adapted from: Nestle F, et al, NEJM 2009; 501.
Mechanism of TNF Blockers
Th22 cell
IL-22
IL-20
IL-23
IL-17AIL-17FIL-17R
IL-12
Antimicrobial peptidesIL-1βIL-6
TNF-αS100
CXCL8CXCL9CXCL10CXCL11CCL20
ActivationNatural
killer T cell
Keratinocyte
Myeloiddendritic cell
Plasmacytoid dendritic cell
Macrophage
IL-1βIL-6
TNF-αTNF-αINF-γ
INF-γ
Th1 cell
Th17 cell
TNF-αINF-γ
Keratinocyte
TNF-α
Adaptive immunity
Innate immunityInnate immunity
IL-20
Adapted from: Nestle F, et al, NEJM 2009; 501.
Mechanism of Secukinumab, Ixekizumab, Brodalumab
Th22 cell
IL-22
IL-20
IL-23
SecukinumabIxekizumab
Brodalumab

11

12

13

14

15

16
Inborn errors of human IL‐17 immunity underlie chronic mucocutaneous candidiasis.
Puel A, et al. Allergy Clin Immunol. 2012;12:616‐22.

17
Immunity to infection in IL‐17‐deficient mice and humans. Cypowyj S, Picard C, Maródi L, et alEur J Immunol. 2012;42:2246‐2254
Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin‐17 immunity. Puel A, Cypowyj S, Bustamante J, et al.Science. 2011;332(6025):65‐68.
TSLP
Gittler JK…and Guttman-Yassky E. J Allergy Clin Immunol Sep 2012

18

19
TSLP
Gittler JK…and Guttman‐Yassky E. J Allergy Clin Immunol Sep 2012Mechanism of cyclosporine

20

21
Cyclosporine
►Nephrotoxicity
►Hypertension
►Hypomagnesemia, Hyperkalemia
►Hyperlipidemia
►Drug interactions
►Hypertrichosis
► Lymphoproliferative disease
► “Sexual Frenzy”
TSLP
Gittler JK…and Guttman-Yassky E. J Allergy Clin Immunol Sep 2012Mechanism of Dupilumab

22
Th2 Cytokine (IL‐4/IL‐13) Effects on the Epidermis in AD
Inhibit terminal differentiation of KCs (IL‐4, IL‐13, IL‐31/Th2)
Inhibit lipid synthesis (Th2 cytokines/IL‐4, IL‐13, IL‐31)
Inhibit synthesis of antimicrobial peptides (Th2/IL‐4, IL‐13, IL‐33 cytokines)
Promote staph aureus binding and colonization (IL‐4, IL‐13)
Augment TSLP secretion by KCs (Th2 cytokines/IL‐4, IL‐13)
Sa et al. J Immunol 2007
Nograles KE. Br J Dermatol 2008
Guttman‐Yassky E. J Immunol 2008
Kim BE et al. Clin Immunol 2008;126:332‐7
Howell MD et al. J Invest Dermatol 2008;128:2248‐58
Cornelissen C et al. J Allergy Clin Immunol 2012;129(2):426‐33
DansoMO. JID July 2014
Th2 cytokines could link the barrier and immune defects in AD
IL‐4 Transgenic Mice Demonstrate Atopic Inflammatory Skin Disease Spontaneously
TgNon‐Tg4 mos
Tg 8 months
Tg 8 months Tg 8 months
Chan LS, et al. J Invest Dermatol 2001;117:977‐83

23
Dupilumab Blocks Signaling Through the IL‐4/IL‐13 Receptor/Ligand System
Type I Receptor
IgE responses, Th2 –mediated inflammation, reduced antimicrobial
peptides
Type II Receptor
Reduced skin barrier function, increased Th2 responses
Dupilumab in persistent asthma with elevated eosinophil levels.
Wenzel S, et al. N Engl J Med. 2013 May 21. [Epub ahead of print]

24
Dupilumab treatment in adults with moderate‐to‐severe atopic dermatitis.
Beck LA, Thaçi D, Hamilton JD, Graham NM, Bieber T, Rocklin R, Ming JE, Ren H, Kao R, Simpson E, Ardeleanu M, Weinstein SP, Pirozzi G, Guttman‐Yassky E, Suárez‐Fariñas M, Hager MD, Stahl N, Yancopoulos GD, Radin AR
N Engl J Med. 2014;371:130‐9.

25
Evolving Pathogenic Concepts On Atopic Dermatitis (AD) and Its Systemic Nature with Implications for
Targeted Therapeutics
PROFESSOR EMMA GUTTMAN, MD, PhD – Program ChairProfessor and Vice Chair, Dermatology
Director, Center for Excellence in Eczema and Laboratory for Inflammatory Skin DiseasesIcahn School of Medicine at Mount Sinai Medical Center
A Year 2016‐2017 Science‐to‐Practice Update for the Dermatological Specialist
Speaker Disclosures
Research support, consulting or lecture fees on atopic dermatitis from Regeneron, Sanofi, Merck, Stiefel/GSK, Pfizer, Genentech, Bristol‐Myers Squibb, Galderma, Celgene, Leo Pharma, Janssen, Medimmune, Dermira, Anacor, AnaptysBio, Glenmark, Novartis, Celsus, Abbvie, Sun Pharma, Mitsubishi Tanabe, Vitae, Almirall
No patents, ownership, or financial gain from any atopic dermatitis drug

26
Atopic Dermatitis
Most common inflammatory skin disease (3‐7% of adults and 15‐25% of children)
~ 1/3 of AD patients have moderate‐to severe disease
Large unmet need for safe and effective therapeutics in both adults and children

27
Barrier Defects in AD (and Clinical Correlations)
Lichenification: Epidermal hyperplasia characterizes chronic lesional AD skin
Terminal Differentiation, Tight Junction, and Lipid Defects
Guttman‐Yassky, et al J Allergy Clin Immunol 2009
De Benedetto A et al JACI 2011; 127: 773‐786
N NL LS
N NL LS

28
A
B
C
D
E
Non-lesional Acute Chronic
CD3
CD11c
CD83
CD1a
! "#$ %
! &' $ %
0
20
40
60
80
100
120
140
*
*
Cel
ls/m
m
CD3
0
100
200
300
**
**
CD11c
0
100
200
300
400
**
****
CD83
0
50
100
150
200
250
*
*
CD1a
0
10
20
30
40
*
*
Acute and even more chronic AD are associated with large T cell and dendritic cell infiltrates
AD Skin Lesions are Invariably Characterized by Immune Activation
Gittler JK…and Guttman‐Yassky E J Allergy Clin Immunol 2012
Non‐lesionalAcute ADChronic AD
0
2
4
6
8
10
1
4
16
64
256
1024
IL−4
IL−5
IL−10
IL−13
IL−31
IL−33
CC
L17
CC
L18
CC
L22
CCL5
CC
L26
CC
L13
CC
L11
*
**
**
*
*** **
**
**
*
*
Non‐lesionalAcute ADChronic AD
IL‐4Th2
IL‐5Th2
IL‐10Th2
IL‐13Th2
IL‐31Th2
IL‐33Th2
CCL17Th2
CCL18Th2
CCL22Th2
CCL5Th2
CCL26Th2
CCL13Th2
CCL11Th2
ln(exp
ression/hARP)
Expression/hARP
ln(exp
ression/hARP)
IL‐22Th22
S100A7Th22
S100A8Th22
S100A9Th22
2 7 8 9
*
*** *
*** **** **
0
2
4
6
8
10
Th2
Th22
AD Lesions are Accompanied by Th2/Th22 Cytokine Activation
Gittler JK…and Guttman‐Yassky E J Allergy Clin Immunol 2012
S100A7
S100A8
Non‐lesional Acute Chronic

29
Two Proposed Mechanistic Hypotheses for AD
“Outside‐in” ‐ AD is a disease of fixed (genetic) epidermal barrier defects, that may trigger abnormal keratinocyte hyperplasia and secondary immune activation
Supported by the FLG gene mutation in 10‐40% of AD patients
Palmer CAN, et al Nat Genet 2006; 48: 441‐446.
“Inside‐out”‐ The abnormal epidermal phenotype in lesional AD skin is driven by increased expression of cytokines produced by distinct T‐cell subsets
The Th2 Cytokines IL‐4 and IL‐13 Downregulate Epidermal Differentiation Proteins In Vitro
Howell MD et al. J Invest Derm 2008;128:2248–2258; Kim BE et al. Clin Immunol 2008;126:332–337.
Filaggrin Loricrin Involucrin

30
Gittler JK…and Guttman‐Yassky E, JACI 2012
A Paradigm Shift in The Pathogenesis of AD….
Staph
Is the pediatric AD phenotype similar to adults?
Paradigm‐shifting AD discoveries have been based on adult biomarkers, reflecting decades of disease activity
But, 85% of AD cases begin before 5yo
We thus (collaboratively with Amy Paller’s group) aimed to:
Determine differences and similarities between early onset AD in children and chronic AD in adults with similar disease activity
We assessed blood and skin samples from 20 AD children<5yrs, within 6 month of disease onset, as well as 14 age‐matched controls
Pediatric vs Adult AD

31
0
10
20
30(%)
p=0.36p=0.88
* p=0.044 *** p<0.001
control AD control AD
children adults
0
1
2
3
4
5
(%)
p=0.38p=0.35
p=0.13 * p=0.028
control AD control AD
children adults
0
10
20
30
40
(%)
** p=0.0056p=0.92
p=0.69 *** p<0.001
control AD control AD
children adults
0
2
4
6
8
10
(%)** p=0.0021
*** p<0.001
p=0.91 * p=0.042
control AD control AD
children adults
IL‐13+CLA+ IL‐13+CLA‐
CD4+ T‐cells
CD8+ T‐cells
Comparable Th2 activation in both pediatric and adult AD
In pediatric AD the Th2 imbalance is confined to skin homing/CLA+ T‐cells and does not extend to CD8+ T‐cells
In adults, Th2 activation extends into systemic/CLA‐ T‐cells and CD8+ T‐cells
Early AD Already Shows Strong Th2 Skewing in Blood
No Th1, Th22, Th17 or Th9 subset expansion was seen in
blood of AD children
Czarnowicki T…, Paller AS* and Guttman‐Yassky* E. JACI 2015
Pediatric AD Exhibits Profound Epidermal Hyperplasia
Bruner PM*, Esaki H*, ….. Paller AS* and Guttman‐Yassky*. JACI September 2016.

32
Th2 Cytokines are Greatly Increased in Skin at Disease Initiation
Bruner PM*, Esaki H*, ….. Paller AS* and Guttman‐Yassky*. JACI September 2016.
Continuous Filaggrin Expression Characterizes Pediatric AD
Bruner PM*, Esaki H*, ….. Paller AS* and Guttman‐Yassky*. JACI September 2016.

33
There is early and potent Th2 activation in blood and skin of AD children, establishing the systemic nature of new onset disease
Pediatric non‐lesional skin is already hyperplastic, accompanied by significant inflammation and activated cytokines to levels often higher than in adults, possibly reflecting “true” AD initiation
FLG deficiency of adult AD is missing in early AD challenging the notion of filaggrin as central for disease elicitation and instigator of the atopic march
Conclusions
Can the Atopic March can be prevented by appropriate immune manipulations (using broad or specific T‐cell targeting) once the skin phenotype has developed?

34
A prediction of the immune model is that immune suppression will reverse the epidermal pathology
The hypothesis can be rejected if immune suppression is achieved but the epidermal phenotype persists
Test of this hypothesis is our study with dupilumab, a specific immune antagonist
Testing the Immune Hypothesis of AD
Dupilumab, a Fully Human IL‐4Rα mAb, Potently Inhibits Both IL‐4 and IL‐13 Signaling
4 week study with weekly injections of dupilumab 75mg, 150 mg, 300 mg and placebo
A total of 67 patients, 18 participated in the biopsy study
Type I Receptor
B cells, T cells, Monocytes, Eosinophils, Fibroblasts
Type II Receptor
Epithelial cells, Smooth muscle cells, Fibroblasts, Monocytes, Activated B cells

35
18.8
0
37.5
27.3
54.552.4
71.4
0
10
20
30
40
50
60
70
80
90
100
% Responders
2 40
Study Week
Placebo (n=16)
Dupilimab 75 mg (n=8)
Dupilimab 150 mg (n=22)
Dupilimab 300 mg (n=21)
*
*
*p<0.05; †p=0.003
*
†
Beck L….Guttman‐Yassky E et al, NEJM 2014
No differences in responses were seen between AD patients based on IgE or FLG mutation status
Dupilumab Response Rates
Dupilumab Significantly Reduced Epidermal Hyperplasia After Only Four Weeks of Treatment
Significant decreases in the expression of genes related to hyperplasia also by arrays (K16, Mki67)
K16K16
p=0.0026p=0.12
p=0.57
10
5
Dupilumab300mg
Dupilumab150mg
Placebo
Time
PrePost
Iog 2
(Exp
ression/hARP)
p=0.023
p=0.241
0.565
4
–4
Dupilumab300mg
Dupilumab150mg
Placebo
FCH (Post vs Pre)
0.122
0.003
2
–8
0
–16
–2
–32
Hamilton J…..and Guttman‐Yassly E. JACI Dec 2014

36
Dupilumab Suppressed Inflammatory Pathways Beyond Th2
Placebo DPL_300DPL_150Down Up
Marked reductions in expression of:
Th2 chemokines (CCL17, CCL18, CCL13, CCL22, CCL26)
S100As (S100A8/9/12)
IL‐23/IL‐17 genes (elafin, IL‐23p19 and p40, IL‐17A)
hyperplasia related genes (K16, Mki67)
One possibility is through the inhibition of IL‐4 induced differentiation of dendritic cells
Hamilton J…..and Guttman‐Yassly E. JACI Dec 2014
FCH (Post vs. Pre)
In vitro studies in KCs suggest that the Th2 cytokines (IL‐4, IL‐13, and IL‐31) inhibit differentiation genes
In vivo, IL‐4R blockade increases expression of LOR and FLG mRNAs, but the magnitude of the effect is small at 4 weeks; may also be confounded by reversal of epidermal hyperplasia
Trend for Increased Expression of Barrier Function Genes (LOR, FLG) with Dupilumab Treatment
FLG/K16 LOR/K16
Dupilumab300mg
Dupilumab150mg
PlaceboDupilumab300mg
Dupilumab150mg
Placebo

37
Dupilumab Improved the AD Transcriptome in a Dose‐Dependent Manner
Drug Effect = Transcriptome‐specific changes with p<0.05 and FCH>2
PrePre Pre
PlaceboDupilumab 150mg
Dupilumab 300mg
PostPost Post
Placebo Dupilumab150mg
Dupilumab300mg
Avg % Improvement
‐21.5+24.7
+52
EASI
Time Point
Hamilton J…..and Guttman‐Yassly E. JACI Dec 2014
Dupilumab Impacts Both the Inflammation and the Barrier Dysfunction of AD
Type 2 Immune Response
Chronic StageAcute StageInitiation
Skin Barrier DysfunctionEnvironmental Factors/Allergens
Innate Immune Response
Dupilumab
dupilumab
This establishes IL‐4 and IL‐13 as pathogenic cytokines in AD and cements AD as a reversible, immune‐driven disease, like psoriasis
Noda S et al. J Allergy Clin Immunol 2015;135:324–336.

38
EASI‐75 Response in Phase III: Change from Baseline
† Censored analysis.
0
10
20
30
40
50
60
70
80
0 1 2 4 6 8 12 160
10
20
30
40
50
60
70
80
0 1 2 4 6 8 12 16
51.3*†
11.9†14.7†
44.2*†
52.5*†48.1*†
*P < 0.0001 vs placebo *P < 0.0001 vs placebo
Week Week
Patients (%)
SOLO 1 SOLO 2
Dupilumab 300 mg qw (censored)Dupilumab 300 mg qw (uncensored)
Dupilumab 300 mg q2w (censored)Dupilumab 300 mg q2w (uncensored)
Placebo qw (censored) Placebo qw (uncensored)
Pre‐Treatment Pictures (My Own Patient in Phase 2B)

39
Post‐Treatment Pictures
Pre Treatment Pictures (My Own Patient in Phase 3)

40
Post Treatment Pictures
What Features of AD May beExplained by Other Cytokines Effects
(IL‐22, and IL‐23/IL‐17)?

41
IL‐22 Promotes Hyperplasia and Impairs Terminal Differentiation
Nograles KE et al, British Journal of Dermatology, 2008
Full thickness skin rafts (epidermis + fibroblasts/dermis)
*S100As FCH S100A7 psoriasin 458.87Terminal DifferentiationLOR Loricrin 0.084FLG Filaggrin 0.032CALML5 Calmodulin 5 0.326KRT1 keartin 1 0.022KRT10 keratin 10 0.499
Genes up/down‐regulated by IL‐22 in keratinocytes
Targeting Th22/IL‐22 in AD
Since IL‐22 is involved in the epidermal hyperplasia and barrier defects in AD, we hypothesized that anti IL‐22 treatment might prove to be effective in chronic AD patients
We are conducting an NIH/NIAMS‐funded trial with an anti IL‐22 antibody (ILV‐094) in 60 moderate‐to‐severe AD patients (study completed, analyses in process)

42
3 months Post ILV‐094
Pre ILV‐094/anti IL‐22
What is the Potential Significance of IL‐23/IL‐17 to AD Lesions?
Th17
Induction of S100As& EpidermalHyperplasia
Zheng et al. Nature 445: 648, 2007
Antimicrobiials and S100as FCH DEFB4 defensin, beta 4 238.549S100A7 psoriasin 189.381S100A12 S100 calcium binding protein A12 30.707Cytokines and Chemokines FCH IL8 interleukin 8 14.529CCL20 chemokine (C-C motif) ligand 20 28.306CXCL1 chemokine (C-X-C motif) ligand 1 (me 7.688CXCL2 chemokine (C-X-C motif) ligand 2 6.006CXCL3 chemokine (C-X-C motif) ligand 3 3.812Terminal DifferentiationLOR Loricrin 0.163
IL‐17 induces S100As and impairs differentiation in KCs
Th22
IL‐23
IL‐22 dependent
Nograles KE et al, BJD 2008 Sa et al. J Immunol 2007
IL‐22
IL‐17

43
Pre Ustekinumab
Shroff A, and Guttman‐Yassky E. JAAD case reports January 2015
A Case Report of Successful Treatment of Refractory AD with High Dose Ustekinumab
Post Ustekinumab
Ustekinumab
Secukinumab
ILV-094
Tezepelumab
GBR 830
Dupilumab
Nemolizumab BMS-981164
Tralokinumab Lebrikizumab
JAK inhibitors
Apremilast
Other Pathways/Targets Under Investigation
Noda S, Krueger JG, and Guttman-Yassky E.J Allergy Clin Immunol 2015

44
Summary….It is Not That Simple….
The AD phenotype cannot be explained by a single cytokine pathway like psoriasis
It is currently unclear how many immune axes need to be targeted and to what extent to fully reverse the pathogenic disease phenotype
Clinical trials with IL‐17/IL‐23, IL‐22, and IL‐4/IL‐13 antagonists (coupled with mechanistic studies) are needed to determine the relative contribution of each axis to AD in different AD phenotypes and in different parts of the world
AD Emerging As A Systemic Disease

45
What is the Level of Systemic Immune Activation in AD vs Psoriasis (and Controls)?
Both atopic dermatitis (AD) and psoriasis are characterized by T‐cell activation in skin, but their comparable systemic T‐cell activation has been unclear
We recently evaluated T‐cell activation markers (ICOS and HLA‐DR) in central (Tcm/CCR7+CD45RO+) and effector memory (CCR7‐CD45RO+) skin homing (cutaneous lymphocyte antigen/CLA+) and CLA‐ subsets from psoriasis, AD and controls
Czarnowicki T…..Krueger JG, and Guttman‐Yassky E. JACI 2015
Compared with psoriasis, AD is characterized by increased levels of T‐cell activation (ICOS/HLA‐DR) among central and effector CD4+ and CD8+ CLA+ and CLA‐ memory subsets (p<0.01)
AD is Characterized by Excess Systemic T‐cell Activation Compared to Psoriasis
Czarnowicki T…. and Guttman‐Yassky E. JACI April 2015

46
Ungar B…Guttman‐Yassky E. J Invest Dermatol Nov 2016 (Epub ahead of print)
Systemic Cytokine Activation in AD
Serum cytokines levels were shown to be increased in AD patients compared to controls and correlated with disease activity (SCORAD)
IL‐22 CCL17 IL‐13 CCL22 CCL13 CCL2 IFNγ CXCL10 CCL4 CCL11 CCL26 CCL3
FCH (log 2)
‐3
‐2
‐1
0
1
2
3
4
5
…post CsA treatment …
Modifiable risk factors?
Ungar B…Guttman‐Yassky E. J Invest Dermatol Nov 2016 (Epub ahead of print)
IL‐22 CCL17 IL‐13 CCL22 CCL13 CCL2 IFNγ CXCL10 CCL4 CCL11 CCL26 CCL3
‐4.0
‐3.5
‐3.0
‐2.5
‐2.0
‐1.5
‐1.0
‐0.5
0.0
0.5
FCH (log 2)

47
AD and Cardiovascular Risk Factors
Higher odds of:
Smoking at least 100 cigarettes
Current smoker
Started smoking at younger age
Drinking >12 alcoholic beverages/yr
Greater odds of drinking
Higher BMI, esp. >35
Hypertension
Pre‐diabetes, high cholesterol
Especially with increased fatigue, sleep issues
Silverberg and Greenland. JACI 2015;135:721
Atopic Dermatitis and Cardiac Disease
National Health Interview Survey 2010 and 2012
1 year history of AD associated with:
● Coronary artery disease ‐‐ Stroke
● Angina ‐‐ Myocardial infarction
● Congestive heart failure ‐‐ Peripheral vascular disease
Silverberg J. Allergy 2015

48
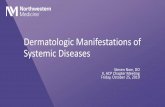
Hjuler KF et al.: Am J Med. 2015 Dec;128(12):1325‐34
Increased Coronary Calcifications in Severe Psoriasis and AD
Percentage of
Analyzab
le segm
ents
Cardiac computedtomographyangiography (CCTA) showed plaques in 48.1% of AD patients vs. 38.3% in psoriasis and 21,2% in controls)
► Chronic inflammation accelerates atherosclerosis due to repetitive vascular injury/endothelial cell activation
–impaired vascular relaxation
–increased leukocyte adhesion
–increased endothelial permeability
–generation of a pro‐thrombotic state
Systemic inflammation and CVD
Steyers CM & Miller FJ: Int J Mol Sci. 2014 Jun 25;15(7):11324‐49Signorelli SS et al.: Int J Mol Med. 2014 Apr;33(4):777‐83

49
Abnormal Cytokine Profile Already Exists in Non‐Lesional AD Skin (Unlike Psoriasis)
Suárez‐Fariñas M…Guttman E. J Allergy Clin Immunol 2011;127:954‐964.
Th2
NormalAD nonlesional AD lesionalTh22
Nonlesional skin expression of Th2 and Th22 markers IL‐13, IL‐22, CCL22, and CCL18 showed high correlation with disease activity
Expression of terminal differentiation genes (EREG, PPL, and LOR) in nonlesional skin showed an inverse correlation with SCORAD
The Nonlesional Phenotype is Influenced by Disease Severity (SCORAD)
ANL AL
Suárez‐Fariñas M…Guttman‐Yassky E. J Allergy Clin Immunol 2011;127:954‐964. Down Up

50
Integrated Disease Severity Biomarker Models Highlight Systemic Immune Activation
LS NL
●●
●
●
●
●
●
●
●
●
●
● ●
●
●
●
●
●
●
●
●
● ●
●
r=0.63 p<0.01
-MX1, S100A12, S100A9, -PPL, IL17A
●●
●
●
●
●
●
●
●
●
●
●●
●
●
●
●
●
●
●
●
●●
●
r=0.73 p<0.01
-PPL, CD11c, CD3, IL13, E.Thickness
●
●
●
●
●
●●
●●
●
●●
●
●
●
●
●●
●
r=0.8 p<0.01
LS + NL + Serum
Ungar B…Guttman‐Yassky E.: J Invest Dermatol Nov 2016 (Epub ahead of print)
50 60 70 80
μScore
50 60 70 80 90
μScore
50 60 70 80
μScore
SCORAD
50
70
90
110
‐MX1, S100A12, S100A9, ‐PPL, IL17A
60
80
100SC
ORAD
‐PPL, CD11c, CD3, IL13, E. Thickness
r=0.73 p<0.01
100
80
60
40
SCORAD
r=0.8 p<0.01
EOS (serum), CCL11 (serum), S100A12 (LS), IL13 (NL), E. Thickness (NL)
AD Emerges as a Systemic Disease
1) High grade systemic immune activation in AD (T‐cells, B‐cells, circulating
cytokines) Czarnowicki T….Guttman‐Yassky E JACI 2015; Czarnowicki T… Guttman‐Yassky E JACI 2016; Ungar
B…..Guttman‐Yassky E J Invest Dermatol 2016.
2) Allergy, Asthma, and the Atopic March
3) Cardiovascular and other co‐morbidities
While Asthma and other comorbidities involve ~30% of AD patients, ALL moderate to severe AD patients are associated with systemic immune abnormalities (might be the common denominator that drives 2‐3)

51
Therapeutic Implications
The high level systemic immune activation in AD is reflected in the wide immune abnormalities seen in the NL AD skin (compared to psoriasis in which NL is closer to normal skin)
This emphasizes the need for systemic treatment approaches for patients with moderate‐to‐severe AD

52
A Review of Landmark Clinical Trials in Atopic Dermatitis
How Will the Data Change Our Approach to Treating Atopic Dermatitis?
A Year 2016‐2017 Science‐to‐Practice Update for the Dermatological Specialist
LISA A. BECK, MDProfessor, Department of Dermatology and Medicine (Allergy/Immunology and Rheumatology)
University of Rochester Medical Center School of Medicine and Dentistry
Rochester, NY
Speaker Disclosures
• Abbvie – AD clinical trials / Consultant• Array Biopharma ‐ Consultant• Celgene, Inc. – Consultant• Hoffman‐ LaRoche ‐ Consultant• Genentech, Inc. ‐ Urticaria clinical trials / consultant• Janssen – Consultant• Novartis – Consultant• Regeneron, Inc. ‐ AD Clinical trials / consultant• Unilever ‐ Consultant• Pfizer & Medtronics ‐ Stock

53
Skin BarrierDefects
Th2AdaptiveImmunity
Itch
MicrobiomeDysbiosis
GeneralInflammation
10,000
1,000
100
10
1Hay fever
Total serum IgE(IU/m
L)
AD is the Most Type 2 Polarized Allergic DiseaseSerum IgE Values
Perennialrhinitis
Asthma Atopic Dermatitis

54
AD is the Most Type 2 Polarized Allergic Disease Serum TARC (CCL17)
AD is the Most Type 2 Polarized Allergic Disease Serum TARC (CCL17)
(J Allergy Clin Immunol. 2004;113:334.)
Asthma Asthma&
AR
AR HealthyControls
AD AD&
Asthma
AD&
AR
ADAAAR
Th2‐Mediated EffectsTh2‐Mediated Effects
Plasma Cell
IgE
Allergens
Itch
Scratch
TH2
IL-4 IL-5IL-13
Eosinophil
B Cell
Skin Barrier Function(↓FLG, LOR, IVL, TJ proteins)
Innate Immune Receptors(↓TLR1, TLR2, TLR6)
Anti-Microbial Peptides(↓HBD3, LL-37, S100s)
Epithelium
FLG=filaggrin; HBD3=human beta-defensin 3; IVL=involucrin; LL-37=cathelicidin;LOR=loricrin;TJ=tight junction; S100s=S100 calcium binding proteins; TLR 1, 2, 6=Toll-like receptor 1, 2, 6.Modified from Janeway CA et al. Immunobiology. 2008.
Dysbiosis
EpidermalThickening

55
SystemicTh2 Targeted
Therapies in ≥ Ph2 Development
SystemicTh2 Targeted
Therapies in ≥ Ph2 Development
Wang & Beck Am J Clin Dermatol. 2016 Oct;17:425
Dupilumab (anti‐IL‐4Rα) Blocks the IL‐4/IL‐13 Receptor/Ligand System
Type I Receptor
B cells, T cells, Monocytes, Eosinophils, Fibroblasts
Type II Receptor
Epithelial cells, Smooth muscle cells, Fibroblasts, Monocytes, Activated B
cells
IL‐4R, IL‐4 receptor‐alpha; IL‐13R, IL‐13 receptor‐alpha; JAK1, Janus kinase type 1; JAK3, Janus kinase type 3; STAT6, signal transducer and activator of transcription 6; TYK2, tyrosine kinase type 2; c, common cytokine receptor gamma chain.
• Dupilumab: a fully human mAb directed against IL‐4Rα subunit
• Blocks IL‐4 and IL‐13 intracellular signaling
• Efficacy in patients with moderate‐to‐severe asthma and increased IgE
(Wenzel et al. NEJM 2013;268:2455)

56
Five DBPC Trials of Dupilumabfor Atopic Dermatitis in US,
Europe, and Japan
Five DBPC Trials of Dupilumab for Atopic Dermatitis in US, Europe, and Japan

57
Baseline Demographics
Characteristic
4‐Wk Monotherapy
Placebo (n=16)
Dupilumab(n=51)
Age – yr 37.4±4.3 42.6±1.9
Male sex – no. (%) 11 (69) 28 (55)
White race – no. (%) 13 (81) 39 (76)
Body mass index 25.7±1.5 26.6±0.9
EASI score 22.8±3.0 30.0±2.0
Investigator’s global assessment score
3.6±0.2 2.8±0.1
Body‐surface area affected ‐ % 40.3±6.5 51.4±3.5
5‐D pruritus score 16.9±1.0 19.3±0.5
Pruritus numerical rating scale 5.98±0.5 6.0±0.2
(Beck et.al., N Engl J Med. 2014;371:130.)
Keratin 16
Molecular Changes in the Atopic Dermatitis Transcriptome in Studies M4A and M4B

58
Two 4‐week monotherapy placebo‐controlled dose‐finding studies (Europe and US)
4‐week trial monotherapy vs. placebo + topical steroids allowed ad lib C4
16‐week monotherapy placebo‐controlled (US, Europe, Japan)
12‐week monotherapy placebo‐controlled (Europe)
Five DBPC Trials of Dupilumab for Atopic Dermatitis in US, Europe, and Japan
Characteristic (Day 29)
4‐Wk Combination Therapy
Placebo and Topical Glucocorticoids
(n=10)
Dupilumab and Topical
Glucocorticoids (n=21)
EASI‐50 ‐ no. of patients (%) 5 (50%) 21 (100%)
EASI‐75 ‐ no. of patient (%) 4 (40%) 13 (62%)
Change in Pruritus NRS ‐ % ‐24.7 ± 15.0 ‐70.7 ± 4.7
IGA 0‐1 ‐ no. of patients (%) 3 (30%) 11 (52%)
Change in IGA ‐ % ‐30.6 ± 12.3 ‐52.5 ± 4.7
Change in EASI ‐% ‐52.5 ± 12.5 ‐75.6 ± 2.9
Beck L, Thaci D, Hamilton JD, et al. (2014) N Engl J Med 371: 130‐139
Efficacy Endpoints

59
Beck L, Thaci D, Hamilton JD, et al. (2014) N Engl J Med 371: 130‐139
TCS use
TCS Use Was About Half in Dupilumab Group
Two 4‐week monotherapy placebo‐controlled dose‐finding studies (Europe and US)
4‐week trial monotherapy vs. placebo + topical steroids allowed ad lib
16‐week monotherapy placebo‐controlled (US, Europe, Japan) M16
12‐week monotherapy placebo‐controlled (Europe)
Five DBPC Trials of Dupilumab for Atopic Dermatitis in US, Europe, and Japan

60
Five DBPC Trials of Dupilumab for Atopic Dermatitis in US, Europe, and Japan
International Dose‐Ranging, Phase 2b Study
SC dupilumab × 16 weeks in adult patients with moderate‐to‐severe AD inadequately controlled by topical medications
Primary endpoint: % change in EASI ‐ baseline to Week 16
Secondary endpoints: Changes from baseline to Week 16 in: Pruritus score; SCORAD; Proportion of patients achieving EASI‐50/75/90; Proportion of patients achieving IGA 0–1; Safety
Lancet. 2016 Jan 2;387(10013):40-52

61
Study treatment(weekly SC injection for 16 weeks after a
loading dose*)
Screening Safety follow‐up (16 weeks)
Study Design and Objective
*Loading doses: • 600 mg for 300 mg dose regimens • 400 mg for the 200 mg and 100 mg dose regimens
Dupilumab 100 mg q4w (n = 65)
Placebo (n = 61)
Dupilumab 300 mg q4w (n = 65)
Dupilumab 200 mg q2w (n = 62)
Dupilumab 300 mg q2w (n = 64)
Dupilumab 300 mg weekly (n = 63)
q4w, every 4 weeks; q2w, every 2 weeks; SC, subcutaneous.
Lancet. 2016 Jan 2;387(10013):40-52
Placebo Dupilumab
n = 61
100 mg q4w
n = 65
300 mg q4w
n = 65
200 mg q2w
n = 61
300 mg q2w
n = 64
300 mg weeklyn = 63
Age (years), mean 37 37 37 36 39 36
Male sex, % 66 52 62 59 64 68
AD duration (years), mean 31 28 27 26 29 26
BSA %, mean (SD) 51 (23.5) 49 (23.9) 51 (22.6) 51 (25.4) 53 (24.8) 48 (20.9)
SCORAD [range 0–103], mean (SD) 67 (13.6) 68 (15.0) 67 (12.3) 68 (14.0) 69 (12.6) 65 (12.2)
EASI [range 0–72], mean (SD) 33 (13.8) 32 (13.5) 29 (11.5) 33 (15.5) 34 (14.5) 30 (11.2)
Peak pruritus NRS [0–10 scale], mean (SD)
6.3 (1.8) 6.7 (1.9) 6.8 (1.9) 7.0 (2.3) 6.7 (2.1) 6.5 (1.5)
Patients with IGA score, %
IGA score = 3 52.5 52.3 56.9 50.8 53.1 50.8
IGA score = 4 47.5 47.7 43.1 49.2 46.9 49.2
Baseline Characteristics
and Clinical Symptoms
Placebo Dupilumab
n = 61
100 mg q4w
n = 65
300 mg q4w
n = 65
200 mg q2w
n = 61
300 mg q2w
n = 64
300 mg
weekly
n = 63
Age (years), mean 37 37 37 36 39 36
Male sex, % 66 52 62 59 64 68
AD duration (years), mean 31 28 27 26 29 26
BSA %, mean (SD) 51 (23.5) 49 (23.9) 51 (22.6) 51 (25.4) 53 (24.8) 48 (20.9)
SCORAD [range 0–103], mean (SD) 67 (13.6) 68 (15.0) 67 (12.3) 68 (14.0) 69 (12.6) 65 (12.2)
EASI [range 0–72], mean (SD) 33 (13.8) 32 (13.5) 29 (11.5) 33 (15.5) 34 (14.5) 30 (11.2)
Peak pruritus NRS [0–10 scale],
mean (SD)6.3 (1.8) 6.7 (1.9) 6.8 (1.9) 7.0 (2.3) 6.7 (2.1) 6.5 (1.5)
Patients with IGA score, %
IGA score = 3 52.5 52.3 56.9 50.8 53.1 50.8
IGA score = 4 47.5 47.7 43.1 49.2 46.9 49.2
Baseline Demographics and Disease Characteristics
Moderate AD, IGA = 3; Severe AD, IGA = 4; NRS, Numeric Rating Scale; SCORAD, SCORing in Atopic Dermatitis; SD, standard deviation.

62
Proportion of Patients Achieving EASI‐50/75/90 over 16 Weeks
EASI‐50 EASI‐75 EASI‐90
0
20
40
60
80
100
123
0
20
40
60
80
100
*P < 0.0001, †P < 0.001, and ‡P < 0.05 (vs placebo, Week 16)
Week
Pro
po
rtio
n o
f p
atie
nts
(%
)
*†
**
‡
****
***
‡
*
4 8 12 160 4 8 12 1600
20
40
60
80
100
4 8 12 160
Placebo Dupilumab 100 mg q4w Dupilumab 300 mg q4w
Dupilumab 200 mg q2w Dupilumab 300 mg q2w Dupilumab 300 mg weekly
EASI-50, 50% improvement in EASI score; EASI-75, 75% improvement in EASI score; EASI-90, 90% improvement in EASI score
Lancet. 2016 Jan 2;387(10013):40‐52
Mean % Change in EASI to Week 32 (All Observed Values with Censoring After Rescue Medication Use)
-100
-90
-80
-70
-60
-50
-40
-30
-20
-10
00 1 2 3 4 6 8 10 12 14 15 16 18 20 22 24 26 28 30 32
124
Placebo Dupilumab 100 mg q4w Dupilumab 300 mg q4w
Dupilumab 200 mg q2w Dupilumab 300 mg q2w Dupilumab 300 mg weekly
*Week 16, P < 0.001 vs placebo; †Week 16, P < 0.0001 vs placebo; ‡Week 32, P < 0.05 vs placebo
*
†
‡
†
††
Mea
n %
ch
ang
e fr
om
bas
elin
e
Week
End of Treatment
EASI
Lancet. 2016 Jan 2;387(10013):40‐52

63
TEAEs over 32 Weeks (16 Weeks Treatment + 16 Weeks Follow Up)
125125
Placebo Dupilumab
n = 61
100 mg q4w
n = 65
300 mg q4w
n = 65
200 mg q2w
n = 61
300 mg q2w
n = 64
300 mg weeklyn = 63
All dupilumab
doses combined
n = 318Total number of TEAEs 184 249 212 207 207 256 1,131
Total number of serious TEAEs 4 7 3 3 2 1 16
Any TEAE, %* 80.3 81.5 86.2 75.4 78.1 84.1 81.1
Any serious TEAE, %* 6.6 7.7 4.6 1.6 3.1 1.6 3.8
Discontinuation due to TEAE, %* 4.9 15.4 4.6 4.9 6.3 1.6 6.6
Any infection, %* 59.0 63.1 63.1 49.2 56.3 61.9 58.8
Upper respiratory tract infection 41.0 38.5 43.1 29.5 37.5 38.1 37.4
Bacterial infections (NEC) 11.5 9.2 6.2 6.6 6.3 11.1 7.9
Herpes viral infections 1.6 12.3 6.2 9.8 7.8 4.8 8.2
Skin structures & soft tissue infections 8.2 7.7 4.6 8.2 7.8 4.8 6.6
Urinary tract infections 6.6 7.7 6.2 9.8 4.7 1.6 6.0Viral infections (NEC) 9.8 4.6 4.6 3.3 6.3 7.9 5.3
AD or eczema exacerbation, %* 19.7 24.6 18.5 14.8 21.9 19 19.8
Headache, %* 3.3 10.8 7.7 14.8 7.8 12.7 10.7
Nausea & vomiting symptoms, %* 6.6 3.1 1.5 6.6 1.6 3.2 3.1
Injection site reactions, %* 3.3 4.6 7.7 6.6 4.7 9.5 6.6
Musculoskeletal & connective tissue pain, %* 8.2 6.2 4.6 1.6 6.3 4.8 4.7
Conjunctival infections, irritations, & inflammations, %* 3.3 1.5 6.2 9.8 4.7 11.1 6.6
*%, percent of patients. NEC, not otherwise classified; TEAE, treatment-emergent adverse event.
Lancet. 2016 Jan 2;387(10013):40‐52
Dupilumab Summary
► Dupilumab (anti‐IL‐4Rα) 300 mg dosing schedules provides rapid, marked and sustained improvement in EASI, SCORAD, IGA, and BSA%, and pruritus
► Dupilumab lead to statistically superior clinical outcomes compared to the placebo group in all measures of disease activity and pruritus
► The most common TEAEs were nasopharyngitis, headache, conjunctivitis and possibly Herpes infections.

64
SOLO 1 and 2 TrialsSOLO 1 and 2 Trials
Presented at late‐breaker session at EADV Congress, 2016.
Objective: Demonstrate efficacy and assess safety of dupilumab monotherapy vs placebo in adults with moderate-to-severe AD inadequately controlled with or medically inadvisable for topical therapy
671 patients in SOLO 1 and 708 patients in SOLO 2
Objective: Demonstrate efficacy and assess safety of dupilumab monotherapy vs placebo in adults with moderate-to-severe AD inadequately controlled with or medically inadvisable for topical therapy
671 patients in SOLO 1 and 708 patients in SOLO 2
SOLO 1 & SOLO 2: Pivotal Phase 3 Studies with Identical Study Design
SOLO 1 & SOLO 2: Pivotal Phase 3 Studies with Identical Study Design
* Dupilumab, 600 mg; placebo, matching placebo. q2w, every other week; qw, weekly; R, randomization; SC, subcutaneously.
Placebo SC qw
Dupilumab 300 mg SC qw
Post-treatment options:
• Maintenance study
• Open-label extension
• Safety follow-up through Week 28
Screening Dupilumab 300 mg SC q2w
Treatment period (16 weeks)
Follow-up period (12 weeks)
Loading dose on Day 1*
Day –35 to –1 Baseline Week 28Week 16
R
GZUS.DUP.16.09.2128

65
Baseline Disease CharacteristicsBaseline Disease Characteristics
SOLO 1 SOLO 2
EventPlacebo
qw(n = 224)
Dupilumab 300 mg q2w
(n = 224)
Dupilumab 300 mg qw(n = 223)
Placeboqw
(n = 236)
Dupilumab 300 mg q2w
(n = 233)
Dupilumab 300 mg qw(n = 239)
Duration of AD, median, years 28.0 26.0 26.0 26.0 24.5 24.0
BSA affected, median, % 57.0 53.4 54.5 53.3 50.0 50.0
EASI score, median 31.8 30.4 29.8 30.5 28.6 29.0
IGA score (range 0–4), %
3 (moderate) 50.4 51.8 52.5 51.3 50.6 53.1
4 (severe) 49.1 48.2 47.5 48.7 49.4 46.9
Peak pruritus NRS, median 7.7 7.6 7.7 7.7 7.8 7.8
Total SCORAD score, median 67.0 65.1 65.9 68.9 67.8 67.4
DLQI score, median 14.0 13.0 14.0 15.0 15.0 16.0
BSA, body surface area; DLQI, Dermatology Life Quality Index; NRS, numerical rating scale; SCORAD, SCORing Atopic Dermatitis. GZUS.DUP.16.09.2128
IGA 0 or 1 and EASI‐75 ResponseIGA 0 or 1 and EASI‐75 Response
† Co-primary endpoint in EU and Japan; key secondary endpoint in other regions.
14.711.9
51.3
44.2
52.548.1
0
10
20
30
40
50
60
70
80
SOLO 1 SOLO 2
10.3 8.5
37.9 36.137.2 36.4
0
10
20
30
40
50
60
70
80
SOLO 1 SOLO 2
* * * *
* ** *
* P < 0.0001 vs placebo * P < 0.0001 vs placebo
EASI‐75† at Week 16IGA = 0 or 1 and ≥ 2 points reduction
from baseline at Week 16
Pa
tie
nts
(%
)
Dupilumab 300 mg qwDupilumab 300 mg q2wPlacebo qw
GZUS.DUP.16.09.2128

66
EASI: % Change from BaselineEASI: % Change from Baseline
LS, least squares; SE, standard error.
-80
-70
-60
-50
-40
-30
-20
-10
00 1 2 4 6 8 12 16
-80
-70
-60
-50
-40
-30
-20
-10
00 1 2 4 6 8 12 16
−37.6−30.9
−72.3*
−67.1*−72.0*
−69.1*
* P < 0.0001 vs placebo* P < 0.0001 vs placebo
SOLO 1 SOLO 2
LS
mea
n p
erce
nt
chan
ge
in E
AS
I fr
om
ba
se
lin
e (
±S
E)
WeekWeek
Dupilumab 300 mg qw (censored)Dupilumab 300 mg q2w (censored)Placebo qw (censored)
GZUS.DUP.16.09.2128
Peak Pruritus NRS: % Change from BaselinePeak Pruritus NRS: % Change from Baseline
NRS, numerical rating scale.
-80
-70
-60
-50
-40
-30
-20
-10
00 2 4 6 8 10 12 14 16
-80
-70
-60
-50
-40
-30
-20
-10
00 2 4 6 8 10 12 14 16
*
−15.4
−44.3*
−48.3*
*
* P < 0.0001 vs placebo * P < 0.0001 vs placebo
LS
mea
n p
erce
nt
chan
ge
inp
eak
pru
ritu
s N
RS
fro
m b
asel
ine
(±S
E)
WeekWeek
Dupilumab 300 mg qw (censored)Dupilumab 300 mg q2w (censored)Placebo qw (censored)
−26.1
−51.0*
−48.9*
*
*
GZUS.DUP.16.09.2128
SOLO 1 SOLO 2

67
DLQI and POEM: Proportions of Patients Achieving Improvement ≥ 4 (MCID) from Baseline at Week 16 DLQI and POEM: Proportions of Patients Achieving Improvement ≥ 4 (MCID) from Baseline at Week 16
DLQI, Dermatology Life Quality Index; MCID, minimal clinically important difference; POEM, Patient-Oriented Eczema Measure.
30.527.6
64.1
73.1
58.462.0
0
10
20
30
40
50
60
70
80
SOLO 1 SOLO 2
26.924.4
67.671.7
63.1 64.0
0
10
20
30
40
50
60
70
80
SOLO 1 SOLO 2
** *
*
* Nominal P < 0.0001 vs placebo * Nominal P < 0.0001 vs placebo
**
**
DLQI POEMP
ati
en
ts (
%)
Dupilumab 300 mg qwDupilumab 300 mg q2wPlacebo qw
GZUS.DUP.16.09.2128
HADS‐A (Anxiety) and HADS‐D (Depression): Proportions of Patients Achieving Score < 8 at Week 16
HADS‐A (Anxiety) and HADS‐D (Depression): Proportions of Patients Achieving Score < 8 at Week 16
1. Bjelland I, et al. J Psychosom Res. 2002;52:69-77. HADS, Hospital Anxiety and Depression Scale; HADS-A, HADS Anxiety subscale; HADS-D, HADS Depression subscale.
Dupilumab 300 mg qwDupilumab 300 mg q2wPlacebo qw
12.4
6.1
41.0 39.536.3
41.2
0
10
20
30
40
50
60
70
80
SOLO 1 SOLO 2
* Nominal P < 0.0001 vs placebo† Nominal P = 0.0001 vs placebo
* † * *
Pa
tie
nts
(%
)
• Analysis conducted in patients with clinical symptoms of anxiety or depression at baseline (i.e., HADS-A or HADS-D ≥ 8)1
GZUS.DUP.16.09.2128

68
Adverse Events Reported in ≥ 5% of Patients in Any Treatment Group
Adverse Events Reported in ≥ 5% of Patients in Any Treatment Group
SOLO 1 SOLO 2
Event*Placebo
qw(n = 222)
Dupilumab 300 mg q2w
(n = 229)
Dupilumab 300 mg qw(n = 218)
Placeboqw
(n = 234)
Dupilumab 300 mg q2w
(n = 236)
Dupilumab 300 mg qw(n = 237)
Patients, n (%)
Nasopharyngitis 17 (8) 22 (10) 25 (12) 22 (9) 20 (9) 20 (8)
Conjunctivitis 2 (1) 11 (5) 7 (3) 1 (< 1) 9 (4) 9 (4)
Upper respiratory tract infection
5 (2) 6 (3) 11 (5) 5 (2) 7 (3) 9 (4)
Injection-site reaction 13 (6) 19 (8) 41 (19) 15 (6) 32 (14) 31 (13)
Atopic dermatitis 67 (30) 30 (13) 21 (10) 81 (35) 32 (14) 38 (16)
Headache 13 (6) 21 (9) 11 (5) 11 (5) 19 (8) 22 (9)
Allergic conjunctivitis 2 (1) 12 (5) 7 (3) 2 (1) 2 (1) 3 (1)
* MedDRA Preferred Term.
GZUS.DUP.16.09.2128
In the pivotal phase 3 studies the primary endpoints were met Both dose regimens of dupilumab showed clinically meaningful improvement and statistical significance versus placebo in: AD signs and symptoms (including itch/pruritus and sleep) Health‐related quality of life Symptoms of anxiety/depression
Significant improvement in itch was observed as early as Week 2 Most AEs were mild or moderate
Injection site reactions and conjunctivitis were more frequent with dupilumab Overall, there were no observed increases in infections with dupilumab
SOLO 1 & 2: Conclusions

69
TH Subsets in Atopic DermatitisTH Subsets in Atopic Dermatitis
DC=dendritic cell; AMPs= Antimicrobial peptides.Hamid Q et al. J Clin Invest. 1994 Aug;94(2):870-876.Werfel T et al. J Invest Dermatol. 1996 Dec;107(6):871-876.Gittler JK et al. J Allergy Clin Immunol. 2012 Dec;130(6):1344-1354.
Non-lesional
Dermal DC
LangerhansCell
TH17
TH2
Antigens
Onset of Hyperplasia/ RegenerativeEpidermal Growth
Acute stage
TH22TH2
Disrupted Barrier
IL-22
IL-31 IL-4IL-13
AMPs (HBD3, LL-37)
Itch Scratch Lichenification
TH22
TH2
Intensification ofCytokine Effects
Chronic stage
TH1
Systemic Anti‐Cytokine Therapies in Development for ADSystemic Anti‐Cytokine Therapies in Development for AD
Blocking Th17 or Th1/Th17 pathways
Blocking Th2 pathway
Blocking Th22 pathway
Blocking a pruritogen
Wang & Beck Am J Clin Dermatol. 2016 Oct;17:425

70
OC459 – Phase 2
Skin BarrierDefects
Th2AdaptiveImmunity
Itch
MicrobiomeDysbiosis
GeneralInflammation

71
Other Systemic Rxs
Wang & Beck Am J Clin Dermatol. 2016;17:425
Name of Agent Route Mechanism Phase Clinical Trials ID
Omalizumab SC Anti‐IgE mAb 2 NCT02300701
Ligelizumab SC Anti‐IgE mAb 2 NCT01552629
MEDI4212 SC/IV Anti‐IgE mAb 1 NCT01544348
XmAb7195 IV Anti‐IgE mAb 1b NCT02148744
Apremilast Oral PDE‐4 inhibitor 2 NCT02087943
AQ‐1125 POSHIP1 activator
(small molecule)
2 NCT02324972
DS106/DS107 PO/TopicalDGLA‐bioactive
lipid2
Paller et al., JAAD. 2016;75:494
• Two Phase III, RDBPC study (>1400) mild‐to‐moderate AD (> 2yrs of age) randomized 2:1 to crisaborole or vehicle
• Primary endpoint: SGA score at day 29 of clear (0)/almost clear (1) with 2‐grade or greater improvement from baseline
• Improvement in Itch was earlier in crisaborole‐treated pts.
• TEAE were infrequent and mild

72
JAK Kinase InhibitorsJAK Kinase Inhibitors
(Nat Rev Drug Discov. 2016;15:35-50Am J Clin Dermatol. 2016 Oct;17:425J Am Acad Dermatol 2015;73:395)
ABT-494 PO JAK 1 inhibitor(small molecule)
2b NCT02925117
Oral JAK 1 and 3 inhibitor
(BJD. 2016; 175:902BJD. 2016;175:86)
• 4 wk, Phase IIa, RDBPC study 69 adults with mild‐to‐moderate AD
• randomized 1:1 to 2% tofacitinib or vehicle ointment twice daily
• Primary endpoint: % change of EASI from baseline (LS Means 81.7% Tofavs 28.9% Veh)
• Improvement in Itch• No safety signals
EASI50
EASI75

73
Skin BarrierDefects
Th2AdaptiveImmunity
Itch
MicrobiomeDysbiosis
GeneralInflammation
The Itch that RashesThe Itch that Rashes
Systemic & Topical Anti‐Itch Rxs
Wang & Beck Am J Clin Dermatol. 2016 Oct;17:425

74
Skin BarrierDefects
Th2AdaptiveImmunity
Itch
MicrobiomeDysbiosis
Wang & Beck Am J Clin Dermatol. 2016 Oct;17:425
Systemic & Topical Barrier Repair RxsSystemic & Topical Barrier Repair Rxs

75
Conclusions
► Last FDA‐approved therapy for AD was 15 yrs ago.
► Many new topical and systemic Rxs are in the pipeline for AD treatment.The only ones that have reported Phase 3 data are:
Dupilumab – biologic targeting IL‐4Ralpha chain (moderate‐severe AD)
Crisaborole – topical PDE4 inhibitor
A major focus is on inhibiting components of the Type 2 (Th2) pathway:• DPL is effective at reducing the signs, symptoms and S. aureus levels (?barrier)
Whether there are AD endotypes that might respond better to Th17 or Th22 antagonists is currently being explored.
A number of more general anti‐inflammatory therapies show great promise (PDE4 inhibitors, JAK inhibitors, H4R inhibitors)
Top Related