





Languages
Pages
Legal


Nephrolithiasis & Neoplasm
Clinical Medicine IPA-522Spring 2009

Types of Urology Lectures
Infectious diseases / bacterial infections
”….itis”, STD's
bugs and drugs
Everything else
calculus
neoplasms
prostate disease

Objectives
Describe the ROS associated with a GU complaint
Describe the key symptoms associated GU complaints
Describe the presentation, evaluation and treatments of renal calculus
Describe the presentation, evaluation and treatment options associated with kidney, bladder, testis and prostate cancer

Review of Systems
Frequency day and night
Urgency
Hesitancy
Force of stream
Incontinence pad use
Hematuria gross or microscopic
Pain with urination
Previous history GU surgery, UTIs, STDs,
kidney stones
Family h/o cancer
PSA status
LMP
Sexual complaints

Key Symptoms
Dysuria
Pain
Hematuria

Dysuria
Related to acute inflammation of the bladder, urethra, or prostate
The first symptom suggesting urinary infection originating from a stone, contaminant, prostate
Described as a “burning” while voiding with discomfort located in the urethra
Often associated with frequency and urgency
Don’t forget STD’s

Pain
Two types Local
which is felt in or near the involved organ
Referred originates in a diseased organ but is felt elsewhere
Kidney Prostate
Ureter Testicular
Bladder Epididymal
Bone / leg

Hematuria
Creates a wide variety of diagnostic possibilities
Differential diagnosis may include:
Infection
Renal calculus
Cancer
Trauma
Renal parenchymal disease

Hematuria
Hematuria without other symptoms must be regarded as a tumor of the bladder or kidney until proved otherwise.

Hematuria
High power field (HPF)
0 - 3 RBC/HPF accepted as normal
> than 3 requires
follow-up studies
UA
C&S
Cytology

Hematuria

Hematuria
Changing the focus causes RBC’s to appear as black circles

Hematuria timing
Partial
initial
suggests an anterior urethral lesion
terminal
suggests posterior urethral, trigone, or
bladder neck lesion
Total
present throughout urination

Topics to Cover
Nephrolithiasis
renal and ureteral calculus
Neoplasms
kidney, bladder, prostate, testis

Nephrolithiasis
Occur throughout the urinary tract
pain, infection, obstruction
Incidence
typical age range between 30 - 50 years
sex: male predominance
race: rare in African Americans
geographics: “stone belts” and developed countries
recurrences are common: 50% in 5 years
Caused by saturation and crystallization of stone-forming
salts in the urine

Etiology
Varies with different types of stones
calcium stones
hypercalciuria (50% of stone formers)
Idiopathic (95%) or 1 hyperparathyroidism (5%)
uric acid stones
volume depletion, acidic urine
struvite stones
form in high urinary pH (Proteus spp.)
cystine stones
Defect in the renal tubular absorption of cystine

Types of Calculus
Calcium 75 - 85% radiopaque
Uric acid 5 - 8% radiolucent
Cystine 1% radiolucent
Struvite 10 - 15% radiopaque
McPhee, 2003, p. 468

Etiology
Varies with different types of stones
calcium stones
hypercalciuria (50% of stone formers)
Idiopathic (95%) or 1 hyperparathyroidism (5%)
uric acid stones
volume depletion, acidic urine
struvite stones
form in high urinary pH (Proteus spp.)
cystine stones
Defect in the renal tubular absorption of cystine

Radiography
Radiopaque
applies to substances that absorb x-rays
representative areas appear white on the exposed
x-ray film
Radiolucent
applies to substances that penetrate x-rays
representative areas appear dark or black on the film

Radiography

Types of Calculus
Calcium 75 - 85% radiopaque
Uric acid 5 - 8% radiolucent
Cystine 1% radiolucent
Struvite 10 - 15% radiopaque
McPhee, 2003, p. 468

Presentation
Asymptomatic patients
Symptomatic / acute presentations
back pain or flank pain that waxes and wanes
pain can radiate to the groin, testicles, labia
hematuria
nausea/vomiting
dysuria

Flank Pain

Pertinent Labs and Studies
Urinalysis
Urine culture
Plain film of the abdomen
KUB
identifies radiopaque stones only (85%)
Renal U/S
Intravenous pyelogram (IVP)
CT (Spiral or Helical)

Urinalysis
Dipstick
Microscopic

IVP
A series of contrast films of the kidneys, ureters, and bladder taken at timed intervals after the IV injection of an iodine containing contrast medium.
A plain film of the abdomen is taken initially.
Serial films taken at 5, 15, 30, 60, 180 minutes.



Acute Stone Episode Tx
Often presents in the ER
After the HPI UA, C&S, CBC with diff, BUN, Creatinine
KUB / IVP / Spiral CT
Admission may be indicated high grade unilateral obstruction
bilateral obstruction
obstruction of a solitary kidney
severe pain not controlled by oral analgesics

Treatment
Dependant on the size of the stone

Treatment
Stones measuring < 5 mm
Most likely to pass spontaneously
“Trial of stone passage”
Drink plenty of fluids
Increase urinary output to 2L/day
Strain urine
Oral analgesics
NSAIDs or possibly narcotic (Darvocet)
Weekly follow-up, earlier if pt. develops fever

Treatment
Stones measuring 5 - 10 mm
Less likely to pass spontaneously
Elective early intervention likely
especially if infection, obstruction, or solitary kidney is present
Treat as 5mm stone
ESWL or ureteroscopy with stone extraction possible.
ESWL failure: stone burden, body habitus, impaction, stone composition

Treatment (5 – 10mm)
ureteroscopy
ESWL

Treatment
Stones measuring >10 mm Not likely to pass
Treatment will depend Symptoms of the patient
If Cystine or Uric acid stones then dissolution may be possible with alkalization (ie. Potassium citrate)
Open surgery or percutaneous endoscopic procedure may be warranted

Treatment (>10mm)

Prevention
Regular high fluid intake
Consider diet restrictions for salt and protein
Medications
Potassium citrate (Urocit-K)
Allopurinol (Zyloprim, Aloprim)

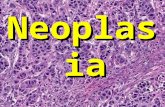
Neoplasms
Kidney
Bladder
Testis
Prostate

Renal Neoplasms
General Characteristics Cause unknown
# 9 of ten most common cancers
Male:Female ratio 2:1
Occurs most commonly in the fifth to sixth decade
RCC is the most common malignant primary renal mass in adults: 80%

Renal Tumor Presentation
Incidental / Asymptomatic presentation
50% found this way
When not found incidentally, 33% will have metastatic disease with initial presentation
Symptomatic presentation
Pain, hematuria, weight loss, flank mass
Classic triad of flank mass, hematuria, and pain occurs in 10% of patients

Evaluation
UA
Cytology
CT scan with contrast
tumor is staged with CT

Kidney Tumor Staging
2 systems
TNM (Tumor, Nodes, Metastasis)
Robson’s classification
simplified staging system but correlated poorly with prognosis

http://hopkins-gi.nts.jhu.edu/pages/latin/templates/index.cfm

Treatment
Surgery is treatment of choice Cure rate for confined local disease: 60 to 90%
RCC is relatively radioresistant
Chemotherapy trials have been disappointing
Immunotherapy trials in progress show promise

Bladder Cancer
Average age: 40 - 70 years
# 4 of ten most common cancers
3 times more common in men
3% of cancer related deaths in US
Risk Factors tobacco exposure occupational carcinogens
Rubber, dye, printing, chemical industries

Bladder Presentation
Hematuria
Gross
Microscopic

Bladder Cancer Studies
Urine for UA, C&S, cytology
IVP
Cystoscopy
TURBT

TURBT

Bladder Cancer Treatment
Stage Dependant
Superficial lesions
Resection and fulguration with f/u cystoscopy every 3 months
Treatment with BCG Decreases tumor recurrence and progression
Invasive or recurrent cancer
Radical cystectomy

BCG (Bacillus Calmette-Guerin)
Instillation into the bladder
Medication must remain for 2 hours in the bladder
Generally a series of 6 treatments
Temporary side effects
frequent urination dysuria flu-like symptoms
Possible systemic infection
BCG Sepsis Conversion to PPD positive

Bladder Cancer Treatment
Stage Dependant
Superficial lesions
Resection and fulguration with f/u cystoscopy every 3 months
Treatment with BCG
Decreases tumor recurrence and progression
Invasive or recurrent cancer
Radical cystectomy with conduit or neobladder

Ileal conduit
The most commonly
used method of
urinary diversion in
the USA

Neobladder / Pouch
A variety of neobladders exist

Neobladder / Pouch

Testicular Cancer
Most common malignancy in young men
average age at diagnosis: 32 years
Initial presentation
painless, solid testicular swelling
“heaviness” in testis
Differential diagnosis
orchitis, hydrocele, spermatocele, testicular torsion

Etiology
Cryptorchidism a condition in which a testicle is arrested at some point in
its normal descent anywhere between the renal and scrotal areas
unilateral arrest more common than bilateral arrest at birth the incidence of maldescent is 3.4% half of such testicles descend in the first month of life
Trauma is not a cause of tumor
Testis tumors do not appear to have a geneticpredisposition

Laboratory Studies
Blood work
AFP, B-HCG: will be elevated and are diagnostic for germ cell tumors
BUN and Creatinine: retroperitoneal disease can cause urinary obstruction
Radiologic studies Scrotal U/S

Treatment
Orchiectomy
with possible biopsy of the contralateral testis

Scrotal Masses
Hydrocele fluid filled mass around testicle transilluminates elective surgical repair possible
Varicocele a venous varicosity in the spermatic vein “bag of worms”, does not transilluminate, may decrease
Testicular torsion acute, tender, painful, scrotal swelling surgical emergency

Scrotal Masses
VARICOCELE HYDROCELE HYDROCELE
TRANSILLUMINATED

Prostate Cancer
The most common tumor in U.S. males: # 1 30 - 40% of men > 50 years of age have prostate
CA, although < 10% of those with prostate cancer will die from prostate cancer
Presentation is in men usually > 65 y
Risk factors: family history African American age

Screening for Prostate Cancer
Screening generally consists of an annual PSA and DRE
Methods
Digital rectal exam (DRE)
begin at age 40 years, earlier for those with family hx
Serum PSA level

DRE
70% of all
prostate cancer
originates in the
peripheral zone

DRE

PSA
Prostate specific antigen Nl value: 0 – 4 ng/dl
Relative risk assessment will likely supplant PSA
PSA is an enzyme made in the prostate gland and is found in the peripheral circulation Present in 2 forms
Bound
Free
PSA test is not diagnostic of prostate cancer

PSA – the good…
PSA has resulted in detecting more prostate cancers
Detects prostate cancers earlier
Will elevate with malignant conditions (cancer) as
well as infectious benign conditions (prostatitis)
Free PSA

PSA – the bad and the ugly
PSA test is not a foolproof test for prostate cancer A normal PSA does not rule out prostate cancer
Often used improperly Started younger than necessary
Continued later than necessary
Can be masked with patients using Finasteride up to 50%

PSA Value
Journal of the American Medical Association 2005;294:66-70

PSA Velocity
The rate of change in serum PSA
more than 0.75 ng/mL per year
the prostate cancer detection rate was 47% among men with a PSA "velocity" greater than 0.75 ng/mL per year versus 11% among men with a PSA velocity less than 0.75 ng/mL per year (Smith & Catalona, 1994)

Free PSA

Prostate Evaluation - TRUS

Prostate Tumor Staging
2 systems
TNM (Tumor, Nodes, Metastasis)
Gleason score
one of the best tools available for predicting the outcomes of men treated with radical prostatectomy or with radiation therapy
prostate cancers with Gleason scores of 8 to 10 are much more likely to recur after primary treatment than are prostate cancers with Gleason scores of 2 to 6

Tannenbaum, 1977

Treatment
Watchful Waiting
PCPT
Finasteride reduced the risk of developing prostate cancer by 25% in men 55y and older
Radical Prostatectomy
External Beam Radiation
Radioactive Seed Implant
Cryosurgery
Hormone Therapy

Watchful Waiting
One approach to managing prostate cancer
Unlike other cancers, the natural progression of prostate cancer is slow and unpredictable
Creating a difficulty in distinguishing clinically relevant disease in the patient
Active surveillance
Another option that aims to individualize therapy

Watchful Waiting
Parker, 2004
Contrasts between active surveillance and watchful waiting
Watchful waiting Active surveillance
Aim To avoid treatment To individualise treatment
Patient characteristicsAge >70 or
life expectancy <15 yrs
Fit for radical treatment
Age 50–80
Tumour characteristicsAny T stage GS ≤7
Any PSA
T1–T2 GS ≤7
Initial PSA <15
MonitoringPSA testing unimportant
No repeat biopsies
Frequent PSA testing
Repeat biopsies
Indications for treatment Symptomatic progressionShort PSADT
Upgrading on biopsy
Treatment timing Delayed Early
Treatment intent Palliative Radical

Treatment
Watchful Waiting
Radical Prostatectomy
External Beam Radiation
Radioactive Seed Implant
Cryosurgery
Hormone Therapy

Objectives
Describe the ROS associated with a GU complaint
Describe the key symptoms associated GU complaints
Describe the presentation, evaluation and treatments of renal calculus
Describe the presentation, evaluation and treatment options associated with kidney, bladder, testis and prostate cancer

References
Course TextLeibovich, B.C. et al. (2003). Current staging of renal cell carcinoma. Urologic Clinics
of North America, 30, 481-497.McPhee, S.J., Lingappa, V.R., & Ganong, W.F. (2003). Pathology of disease: An
introduction to clinical medicine (4th ed.). New York: McGraw-Hill.Parker, C. (2004). Active surveillance: towards a new paradigm in the management
of early prostate cancer. The Lancet Oncology, 5, 101-106.Smith, D.S., & Catalona, W.J. (1994). Rate of change in serum prostate specific
antigen levels as a method for prostate cancer detection. Journal of Urology, 152, 1163–1167.
Tanagho, E.A., & McAninch, J.W. (2004). Smith’s general urology (16th ed.). New York: McGraw-Hill.
Tannenbaum, M. (1977). Urologic pathology: The prostate. Philadelphia: Lea and Febiger.
Yun, E.J., Meng, M.V., & Carroll, P.R. (2004). Evaluation of the patient with hematuria. The Medical Clinics of North America, 88, 329-343.