





Languages
Pages
Legal


1
APPROACH TO THE PATIENT OF PLEURAL EFFUSION
Presented by :Dr. Vidhu MittalJunior Resident
Deptt. of Chest and TB

2
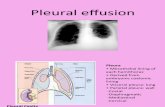
PLEURAL SPACEIntroduction
The pleural space is a potential space around the lungs, bounded by two membranes, the visceral pleura covering the lung and the parietal pleura covering the chest wall and the diaphragm.
Blood Supply of Pleura
The parietal pleura is supplied by intercostal arteries.
The visceral pleura is exclusively supplied by the bronchial circulation which drains into the pulmonary veins.

3
Lymphatic Drainage
The visceral pleura has extensive lymphatics but they do not connect to the pleural space. The parietal pleura lymphatics connect to the pleural space via stomata, holes of 8-10 m in diameter.
From stoma liquid drains into
Lacunae Spider like submessothelial collecting lymphatics infracostal lymphatics
Systemic Venous System Thoracic Duct Parasternal &
Periaortic Nodes

4
In a normal pleural space, fluid enters and exists at a constant, equal rate because of the ongoing filtration of a small amount of low protein liquid in normal microvessels. Near the end of the 19th Century, Starling and Tubby hypothesized that the exchange of microvascular fluid and solutes was governed by the balance between the hydrostatic pressure, osmotic pressure and membrance permeability and they devised the starling equation :
QF = LP x A [(PCAP-PPL ) - D (piCAP-piPL)]
QF = Fluid movement
LP = Filtration Coefficient
A = Surface area of the pleura
D = Reflection coefficient for protein movement across the pleura (PL)
P = Hydrostatic pressure of the pulm. capillary bed. (CAP).
Pi= Oncotic pressure of pleural space.

5
This equation formed the basis for understanding fluid accumulation in the pleural space, where the hydrostatic forces that filter water out of the vessel are balanced by osmotic forces that reabsorb water back into the vessel. In the pleura, reabsorption is facilitated by the extensive lymphatic system on the diaghram and mediastinal surfaces of the parietal pleura.
Normal Characteristics of Pleural Space/Fluid
Major Consideration are given to :-
(a) Volume of pleural fluid
(b) Thickness of Pleural Space
(c) Cellular Components
(d) Physiochemical Factors

6
(a) Volume :- Normally, the volume of fluid in the right and left pleural spaces is quite similar expressed/kg of bodymass, the total pleural fluid volume in normal non-smoking humans in 0.260.1 ml/kg.
(b) Thickness of space :- The normal pleural space is 18-20 m in width, although it widens at its most dependent areas.
(c) Cellular components :- In the pleural space WBC count has been reported to be 1700 cells/mm3 and the mean RBC count of 700 cells/mm3 and approx. 75% of the cells are macrophages and 25% are lymphocytes, with mesothelial cells, neutrophils and eosinophils accounting for <2% each.

7
(d) Physiochemical Factors :-
Protein : A small amount of protein is normally present in pleural fluid and is similar to serum fluid except for former contain more of LMW albumin.
HCO3 Bicarbonate conc. is increased by 20-25% relative to that in
plasma.
NA+ reduced by 3% to 5%
Cl- reduced by 6% to 9%
Concentration of K+ and glucose in the pleural fluid & plasma appears to be nearly identical.
Pathophysiology :- For pleural liquid to accumulate to form an effusion it is likely that both the entry rate of liquid must increase and the exit rate must decrease.

8
If only the entry rate increased it would require a sustained rate more than 30 times normal to exceed the reserve lymphatic removal capacity; if the exit rate decreased it would take more than a month at the normal entry rate at 12ml/day to produce an effusion detectable by chest radiograph.
Increased entry rate Decreased exist of liquidMay result from ed filtration May result from interferenceacross systemic or pulm. capillaries with lymphatic function (e.g.)
• Obst. of parietal pleura stomata. • Inhibition of lymphatic contractility • Infiltration of draining parasternal
lympha nodes. • Elevation of systemic venous
pressure into which the lymph drains.

9
HOW TO APPROACH : (1) Clinical Signs and Symptoms :- Common symptoms of patients with effusion are pleuritic chest pain, cough and dyspnoea and it appears that the three symptoms are due to different causes.
(a) Pleuritic chest pain :- it is derived from inflammation of the parietal pleura. Some patients with pleural effusions experience a dull aching chest pain rather than pleuritic chest pain which suggests patient has pleural malignancy.

10
(2) Second symptoms for pleural effusion is dry, non-productive. The exact mechanism for cough is not clear.
(3) Third symptom is dyspnoea. Pleural effusion acts as a space occupying process in the thoracic cavity and therefore reduces all the subdivisions of lung volumes.
Physical Examination :-
Inspection : While inspecting it is important to examine the relative sizes of the hemithoraces and the intercostal spaces.
(a) If the pleural pressure is increased on the side of the effusion, that hemithorax will be larger and usual concavity of ICSs will be blunted or even convex.
(b) Whereas if the pleural pressure on the side of effusion is decreased (as with obstruction of major bronchus or a trapped lung). The ipsilateral hemithorax will be smaller and the normal concavity of ICS will be exaggerated.
(c) In addition with inspiratory efforts, the intercostal spaces retract.

11
Palpation :
(a) Is useful for delineating the extent of effusion in areas where pleural fluid separates the lung from the chest wall, tactile fremetus is absent or accentuated.
(b) With a thin rim of fluid, the percussion note may still be resonant, but the TF is diminished.
(c) Palpation may also reveal that the cardiac point of maximum impulse is shifted to one side or the other.
Percussion :- The percussion not over a pleural effusion is dull or flat. The dullness is maximum at the lung bases where the thickness of the fluid is greatest.

12
Auscultation :-
Auscultation over the pleural fluid characteristically reveals decreased or absent breath sounds.
• Near the superior border of the fluid, however, breath sounds may be accentuated and take on a bronchial characteristic.
• Auscultation may also reveal a pleural rub. pleural rubs often appear as pleural effusions diminish in size, either spontaneously or as a result of treatment because the pleural fluid is no longer present between the roughened pleural surfaces.
• Obviously the chest is not the only structure that should be examined when evaluating a patient with a pleural effusion, clues to the origin of the effusion are often present elsewhere.

13
1 CHF Cardiomegaly, neck vein distension or peripheral edema.
2 Rheumatoid or Lupus erythematosis
Signs of joint disease or subcut. nodules.
3 Metastatic Disease • Enlarged nontender nodular liver.• Hypertrophic osteo arthropathy.
4 Subdiaphragmatis Process
• Abdominal Tenderness
5 Cirrhosis & hepatothorax
• Tense Ascitis
6 Lymphoma, sacrodosis
• Lymphadenopathy

14
Separation of Exudates from Transudates
A diagnostic thoracocentesis should be performed on nearly every patient with free pleural fluid that measures >10mm on the decubitus radiograph.
If the patient has obvious CHF, consideration can be given to postponing the thoracentosis until the heart failure is treated.
Thoracacentesis procedure :-
• Is a safe procedure and may be much safer when guided by USG but due to cost and inaccessibility USG is accompanied in high risk cases only.
• Because of the small bore of the needle required, it can be safely performed in patients with coagulopathies and thrombocytopenia.

15
Descriptions of Technique emphasizes on :• Proper positioning of the patient.
• Identification of the area of decreased tactile fremitus.
• Adequate local anaesthesia of parietal pleura as well as skin.
• The needle should run over the top of the rib to avoid the neurovascular bundle that travels in the middle of the intercostal space from the spine for approx. 5-6 inches before taking its safer position beneath the upper rib. Thus one should avoid thoracocentesis medial to midclavicular line.
• Complication from thoracocentesis include :-
• Pneumothorax (2-6%)
• hemothorax (1%)

16
The risk for pneumothorax is higher in patients.
• With prior radiotherapy to the chest.
• Multiple prior thoracocentesis
• Use of vaccum bottles.
• The first question that should be answered with the diagnostic thoracoceatesis is whether the patient has a transudative or an exudative pleural effusion.
1) Light's Criteria :-
(a) Pleural fluid protein-to-serum protein ratio > 0.5
(b) Pleural fluid LDH - to - serum LDH > 0.6.
(c) Pleural fluid LDH > 2/3 of the upper normal limit for serum.

17
But this criteria may misidentify a transudative effusion as an exudative effusion in as many as 25% of cases. If a patient appears to have a transudative effusion clinically, additional tests can be assessed to verify its transudative etiology.
(a) If the difference between the protein conc. of serum and the pleura exceeds 3.1 gm/dl the patient in all probability has a tranudative effusion.
(b) If pleural concentrations of N-terminal brain natruretic peptide (NT-BNP) are >1300 pg/ml the patient likely has a transudate from a cardiac cause.

18
Differentiating Among Various Exudative Pleural Effusions :-
Once it has been determined that the patient has an exudative pleural effusion attempt is made to find out the cause.
The various tests done that can eb done are :-
(1) Appearance of pleural fluid :-
The gross appearance and the odor of the pleural fluid is to be noted.

19
Cause Fluid Appearance / Odor• Pseudochylothorax & Chycothorax• Urinothorax• Anaerobic empyema• Chylothorax• Aspergillus infection• Empyema• Amebic liver abscess• Esophageal rupture• Trauma/pul embolism/ malignancy, benign asbestor related, pneumonia or after MI syndrome.
Milky white
Ammonical urinePutridBile stainedBlackTurbidAnchovy BrownFood particlesBlood stained

20
PLEURAL FLUID IS BLOODY
Hematocrit of pleural fluid
>50% of peripheral blood 1-50% <1%
Hemothorax Malignant Pleural No clinical
Disease/Pulm. Significance
Chest tube embolus/trauma
induced

21
PLEURAL FLUID IS TURBID OR MILKY
Centrifugation
Turbidity clears Turbidity Persists
In due to cells or debris in Chylothorax or
pleural fluid Pseudochylothorax

22
Results of Fluid Analysis
Pseudochylothorax Chylothorax
• TG level
• Cholesterol level
• Cholesteral crystals
•Chylomicrons
• <50 mg/dl
• >200 mg/dl
• Yes, common
• No
• Disease process is usually chronic & pleural surfaces are thickened
> 110 mg/dl< 200 mg/dlNo YesDisease process is usually acute 2 pleural surfaces not thickened.

23
Pleural Fluid Protein :-
It is generally not useful in the differential diagnosis of exudative pleural effusion as these tends to be elevated to a comparable degree with all exudative pleural effusion.
However :-
To label it exudative effusion protein > 2.9 gm/dl
If protein is >5g/dl likelihood of tuberculous pleurisy is increased.

24
Pleural Fluid LDH :
Whereas pleural liquid protein and LDH arise from filtration from serum and thus serves as indication of vascular premeability LDH as an intracellular enzyme, may also indicate the degree of cell turnover and/or the degree of inflammation within the pleural space. The pleural fluid LDH level is increased to a comparable degree inpatients with all categories of exudative pleural effusion.
• However, pleural fluid LDH level should be measured everytime thoracocentesis is performed.

25
Pleural Fluid Glucose :-
A low glucose concentration probably indicate the co-existence of two abnormalities : a thickened, infilterated pleura leading to an impaired diffusion of glucose into the pleural space plus increased metabolic activity leading to increased glucose utilization within the pleural space.
• Demonstration of pleural fluid glucose <60mg/dl narrows the diagnostic possibilities to 7.
• Parapneumonic effusion Malignant Effusion
TuberculousRheumatoid ParagonimiasisChurg - Strauss - Syndrome

26
If a patient with parapneumonic effusion has a pleural fluid glucose <40mg/dl tube thoracostomy is considered.
Pleural Fluid White Cell Count and Differential :-
Pleural liquid that is submitted for white cell count and differential should be sent in a tube with an anticoagulant to prevent the cells from clumping.
The differential cell count on the pleural fluid is much more useful than the white cell count itself. The normal pleural space contains predominnalty macrophages (75%)
lymphocytes (23%)

27
For pleural fluid differential count, cells are partitioned into :-
• Polymorphonuclear leukocytes.
• Eosinophils
• Small lymphocytes
• Mesothelial cells and
Other mononuclear cells.
Pleural effusion due to an acute disease contain predominantly polymorphonuclear leucocytes.
Due to chronic diseae predominanlty mononuclear cells.

28
Pleural fluid eosinophilia :-
• Most commonly due to air or blood in the pleural space.
• Can also be due to drugs like nitrofurantoin or dantrolene.
• Small lymphocytes when >50% of WBC's in an exudative pleural effusion indicates that patient may either has a malignant or a tuberculous pleural effusion. Hence, the presence of pleural fluid lymphocytosis should alert the physician to consider needle biopsy of pleural for diagnosis.

29
Pleural fluid cytology :-
• The first pleural fluid cytologic study is positive for malignant cells in upto 60% and is 3 separate specimens 90% of effusion due to pleural malignancy.
• The frequency of positive pleural fluid cytologic tests is depedent on the tumor type. For e.g. <25% of patients with Hodgkins disease have the positive cytology, whereas most patients with adeno carcinoma have positive cytology.

30
Other diagnostic tests for malignancy :-
Cytology may be non diagnostic either because of a problem of specificity or sensitivity.
(a) Fish fluorescent in situ hybridization with chromosome specific probes that can confirm abnormal numbers of specific chromosomes.
(b) Early findings of malignancy including DNA methylation can be detected by methylation specific PCR.
(c) Gene expression patterns can help distinguish mesothelioma and adenocarcinoma.

31
Culture & Bacteriological Stains :-
Pleural fluid should be sent for culture for bacteria, mycobacteria and fungi along with gram's stain.
The newer adjuncts are :-
(1) Detection of bacterial antigens via CIE or latex agglutination or of bacterial DNA by PCR.
(2) Antigen specific assays especially in children against most common pathogens like staphlococcus, streptococcus and H.influenza.
(3) Amplification and sequencing of bacterial 16s ribosomal RNA.

32
Other Diagnostic Tests for Pleural Fluid
Pleural Fluid pH and pCO2
The pleural fluid pH is most useful in determining whether
chest tubes should be inserted in patients with
parapneumonic effusion as a fall in pH i.e. <7.2 is an
indication for ICCT.
In general pleural fluid much a low pH also have a
low glucose hence glucose level can be used as an
alternative as measuring pH require the similar condition
of measurement as measuring arterial pH.

33
Other Diagnostic Tests for Pleural Fluid
Pleural Fluid Amylase:-
Pleural fluid amylase is elevated in patients with effusion
secondary to
esophageal perforation.
• Pancreatic disease
• Malignancy
•As first 2 are rare causes of effusion so amylase levels are usually
not done.
• Malignancy can be differentiated from pancreatic disease with
amylase isoezymes because the amylase with malignant effusion is
primarily of the salivary type.

34
Tests for collagen vascular disease:
•About 5% of patients with rheumatoid arthritis and 50% of patients
with SLE have a pleural effusion during the course of the disease or
may be the first manifestation of disease.
•Measurement of ANA litre is the best screening test for lupus pleuritis
although it is now evident that a positive pleural fluid ANA is not
specific for the diagnosis.
Rheumatoid Arthiritis :
• When a rheumatoid pleural effusion is suspected, the clinical picture
usually establishes the diagnosis but patients with rheumatoid
pleuritis have a pleural fluid RA factor titre of 1:320 and serum titre.

35
Adenosine Deaminase
• The pleural fluid ADA levels are elevated in almost all
patients with tuberculous pleuritis and remains a sensitive
marker for tuberculous pleurisy in pateints with HIV also.
• As it is a highly sensitive test it can be useful to exclude
the diagnosis of tuberculosis when the ADA level is low
(<40 U/L).

36
Interferon - (IFN-)
• Pleural fluid IFN- is elevated almost exclusively in
tuberculous effusions.
•However IFN- release assays had variable results and
have not added to the use of ADA or IFN- measurements
for the diagnosis or exclusion of active pleural
tuberculosis.

37
Molecular Techniques for diagnosis of mycobacterium tuberculosis
(a) PCR to detect specific mycobacterial DNA sequences
in clinical specimens.
(b) Nucleic acid probes to identify the organism in culture.
(c) RFLP to compare strains in epidemologic studies.
(d) Gene based susceptibility studies to screen for known
genes associated with drug resistance.

38

39
USEFUL RADIOGRAPHIC TESTS IN PATIENTS WITH SUSPECTED PLEURAL DISEASE
1) Chest Radiography:-
Two main factors influence the distribution of free fluid
in the pleural space.
(a) Fluid collects in the most dependent part of the
thoracic cavity because the lung is less dense than the
pleural fluid.
(b) Because of their, elastic recoil the lobes of the lung, if
normal, maintain their traditional shape at all stages of
collapse.

40
• If Fluid is < 75 ml, in upright position fluid first
accumulates between inferior surface of the lower lobe
and diaphragm without overflowing into the costphrenic
sinuses.
• The presence of a clinically significant amount of free
pleural fluid can be excluded if both posterior costophrenic
angles are clear.
• When there are larger amounts of pleural fluid the
lateral costophrenic angle on the PA radiograph becomes
blunted.

41
• Lateral decubitus radiographs should be obtained in
most instances when free pleural fluid is suspected as, as
little as 5ml of pleural fluid can be demonstrated with
properly exposed decubitus radiographs.
• We can also semiquantitate the amount of pleural fluid
by measuring the distance between the inner border of the
chest wall and the inner border of the lung as when this
distance is <10mm, the amount of pleural fluid is small
and a diagnostic thoracocentesis is usually not attempted.

42

43
• Pleural fluid may become encapsulated by adhesions
anywhere between the visceral and parietal pleura or
interlobar fissures.
•When the loculation is situated between the lung and the
chest wall, there is a characteristic radiographic 'D-shaped'
loculation seen with the base of D against the chest wall and
the smooth convexity protruding inward toward the lung.
•The absence of air bronchograms helps differentiate
between a loculated pleural effusion and a parenchymal
infilterate.
•A definate diagnosis of loculated pleural effusion is best
established by USG or CT.

44
• For semiquantitation of pleural fluid Blackmore et al
demonstrated that if > 750ml of pleural fluid (is
present)
• Visible on lateral radiograph as a memories positively.
• >200 ml - menesin can be identified in the lateral
costophrenic angle of the PA radiograph.
• > 500ml - menesive observes the entire
hemidiaphragm.

45
Ultrasonography
• In context with the pleural effusion USG is useful in
following situations:
(a) Determining whether pleural fluid is present.
(b) Marking the site for appropriate thoracocentesis.
(c) Identification of pleural fluid loculation.
(d) Distinction of pleural fluid from pleural thickening.
(e) Semiquantitation of the amount of pleural fluid.

46
Ultrasonography
• A 2-5 MHz curvilinear probe allows visualization of the
deeper structures and the sector scan field allows a wider
field of view through a small acoustic window.
• The best distinguishing characteristic of pleural fluid
collection on ultrasound is that it changes its shape with
respiration.

47

48
Positioning:-
• Posterior chest - patient sitting upright
• Anterior and lateral chest - lateral decubitus position.
• If patients arm is raised above his head the distance
between the rib spaces is increased and this facilitates
scanning the patient in erect or recumbent position.

49
• Apart from the above uses one more use of USG is in ICU.
• USG helps to diagnose pleural effusion in supine patients in
ICU as many chest radiograph are taken with the patient in
the supine position and pleural effusions are often missed.
• Identification of pleural effusion in ICU patients in is
important for atleast 2 reasons:-
(a) If the patient in on ventilator removal of the fluid may
facilitate weaning.
(b) If the patient is febrile, it is important to ascertain whether
the patient has infected pleural fluid.

50
Advantages of USG over CT Scan
• Ease and speed with which examination can be done.
• Availability of portable units hence useful for bedside
examination in seriously ill patients.
• Lack of ionizing radiation.
• Low cost.
• USG is also useful to evaluate pleural effusion due to
pulmonary embolism.

51
Pleural effusion
S/o pulmonary Colour
embolism doppler of lower Positive Treat for
extremities thrombo embolism
Negative
Proceeds to lung V/Q Scan
or CT angio
Where CT angio is > sensitive and specific and can diagnose alternate
diagnosis.

52

53
Computed Tomography (CT Scan):
1. CT chest has it greatest utility in distinguishing
parenchymal and pleural abnormalities as between lung
abscess and loculated empyema.
Empyema Lung Abscess
•Cavity walls are of uniform thickness both internally and externally and adjacent lung is usually collapsed.
* Walls of the cavity are not of uniform thickness and the adjacent lung is not compressed.
• The angle of contact with the chest mall may be obtuse.
•Acute
• Most empyemas have lenticular shape and demonstrate the split pleura sign.

54

55
2. Distinguish between malignant and benign
causes in diffuse pleural disease as features
associated with malignancy are:-
(a) Circumferential pleural thickening
(b) Pleural nodules
(c) Parietal thickening >1 cm and
(d) Mediastinal pleural involvement.

56
3. When free fluid lies in posterior costophrenic
recess adjacent to the diaphragm, it may be difficult to
differentiate from ascitis. So several CT signs have been
described for differentiated pleural effusion from ascitis.
(a) Displaced crus sign:-
Pleural effusion Ascites
Displacement of diaphragmatic crus away from the spine by the fluid.
Ascites lies anterior and lateral to the crus.

57
(a) Interface Sign:-
(b) Diaphragm sign
(c) Bare area sign: restriction of ascitis by the coronary
ligaments from the base area of the liver indicates
ascitis.
Ascitis Pleural Effusion
If present a sharp interface between fluid and liver / spleen.
Line much less distinct.
Pleural Effusion Ascitis
Fluid present outside the diaphragm
Fluid present inside the diaphragm.

58
Magnetic Resonance Imaging
Pleural effusions generally have a long T1 and T2
values. The intensity of pleural effusion is therefore
low to extremely low on T1 weighted images.
However, at the present time MRI of chest is less
satisfactory than USG or CT in identifying the
presence of pleural fluid, major limitation being the
respiratory and cardiac motion.

59
INVASIVE TESTS IN PATIENTS WITH UNDIAGNOSED
EXUDATIVE PLEURAL EFFUSION
Three main factors which necessitates the
aggressive approach for the diagnosis in pleural
effusion :.

60
(a) Sign and symptom of the patient are not improving with
time.
(b) Serial LDH level after thoracocentesis if increases after
each aspiration.
(c) Patient himself is anxious to know the cause.
The various invasive tests that can be done
(d) Needle biopsy of pleura.
(e) Image guided pleural biopsy
(f) Bronchoscopy
(g) VATs
(h) Open biopsy of pleura.

61

62
Needle biopsy of the pleura
•Because needle biopsy of the pleura is useful mainly to
establish the diagnosis of malignant or tuberculous
pleural effusion, this procedure should be considered
when one of these diagnosis is suspected.
• Needles most commonly used are COPE needle and
ABRAMS needle.
• Procedure is usually blind or also called closed needle
biopsy.

63
• In malignant pleural disease the needle biopsy of the pleura will
be positive in 40-60% of patients. But it should be considered
only if the initial pleural fluid cytology after thoracocentesis is
non diagnostic. • It has greater utility for tuberculous pleuritis than malignancy.
The initial biopsy is positive for granulomas in 50-80% of
patients and the demonstrations of granulomas on pleural
biopsy is virtually diagnostic of tuberculous pluritis, caseous
nacrosis or acid fast bacilli need not to be demonstrated. • The greatest value of needle biopsy for a patients with
tuberculosis is obtaining material for culture for mycobacterium
tuberculosis for the determination of drug susceptibility.

64
Complications
• Pneumothorax : in about 1% of pleural biopsies.
• Hemothorax can result if an intercostal artery or vein is in
advertantly biopsied.
IMAGE GUIDED PLEURAL BIOPSY
Situations in which the pleural effusion is small or there is
loculation or pleural thickening without an effusion, CT image
guided pleural biopsy is an excellent choice.

65
BRONCHOSCOPY
If the patient of undiagnosed pleural effusion has associated
parenchymal lesion or hemoptysis, fibreoptic bronchoscopy will
provide diagnosis in nearly 75% of patients and in <10% time in
patients with no parenchymal lesion. And for confirming the
parenchymal lesions CT scan is usually done prior to bronchoscopy.
PLEUROSCOPY OF VIDEO ASSISTED THORACOSCOPIC SURGERY
(VATS)
Pleuralscopy can be performed by pulmonologist using local
anaesthesia and conscious sedation for direct visualization of
pleural services, tissue sampling and pleurodesis;

66
Thoracoscopy performed by thoracic surgeons generally referred
to as VATS utilizes general anaesthesia and single lung ventilation
by double lumen intubation and allows greater access to the
pleura and lung surface.
(1) In patients who are strong suspect for malignancy but pleural
fluid cytology or needle biopsy is inconclusive, this can make
diagnosis in over 80% of cases of malignancy including
mesothelioma.
(2) Also insufflation of talc may be carried out to control the
pleural effusion.

67
DISADVANTAGES
(1) Risks of the procedure.
(2) Need for post procedure chest tubes.
(3) Cost
OPEN BIOPSY OF THE PLEURAL
Thoracotomy with direct biopsy of the pleura provides the best
visualization of the pleural and the best biopsy specimen.
The main indication for open pleural biopsy is progressive
undiagnosed pleural disease that cannot be approached by or has
failed to be diagnosed by thoracoscopy.

68
It is important the remember that no diagnosis is established
for approximately 20% of all exudative pleural effusions and that
many resolve spontaneously, leaving no residua.

69

70
Top Related