







Languages
Pages
Legal


ContentsPreface 3
Introduction 3
Appendix C of the UK Vision Strategy 2013Adult UK sight loss pathway

Guidance notes 4
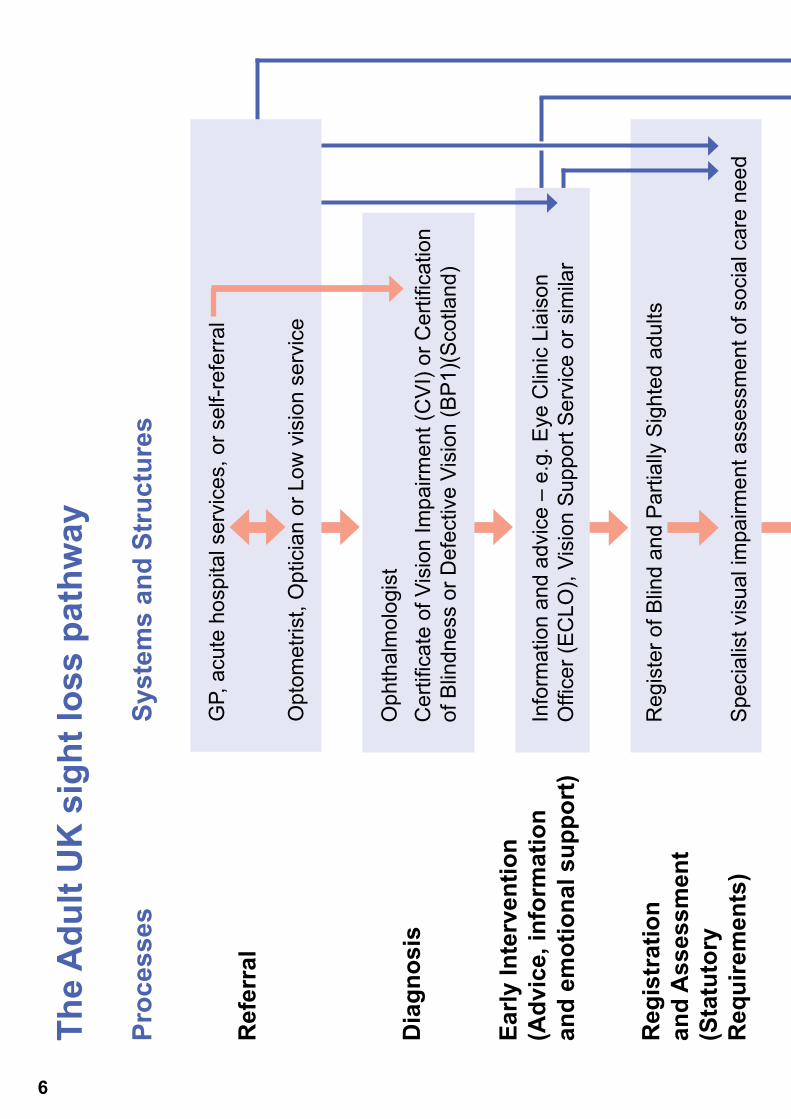
The Adult UK sight loss pathway 6
Framework of the Adult UK sight loss pathway for achieving independent living outcomes 8

Preface The Adult UK sight loss pathway offers commissioners and practitioners a unique tool to enable people with sight loss to get the right support at the right time and from the right person. It clarifies the pathway across health and social care and so enables better partnership working and a smooth transition for the person with sight loss.This pathway has been approved by the Strategic Advisory Group of the UK Vision Strategy and we urge local authorities, GPs, Optometrists, Ophthalmologists and all eye health professionals to work together to implement it fully.
IntroductionThe Adult UK sight loss pathway is a process map describing how the principles of best-practice can be applied to service delivery for adults with sight loss so that they can enjoy:
• Early interventions to address their presenting needs, as a right.
• Visual impairment rehabilitation as an early intervention, delivered by specialist, qualified professionals.
• Interventions that help them maximise their functional vision.
• Community Care Assessment of eligibility for adult social care, only if they still have un-met needs after receiving early intervention services.
This document explains the Adult UK sight loss pathway and the framework of skills required to deliver it.Delivering the Adult UK sight loss pathway contributes to achieving ‘Seeing it my way’ outcomes for blind and partially sighted people. These outcomes underpin the UK Vision Strategy, uniting the sector to ensure that every person who experiences sight loss can benefit from improved eye health and eye care services. The Seeing it my way outcomes are:1: That I understand my eye condition and the registration process.2: That I have someone to talk to.3: That I can look after myself, my health, my home and my family.4: That I receive statutory benefits and information and support that I need.5: That I can make the best use of the sight I have.6: That I can access information making the most of the advantages that technology
brings.7: That I can get out and about.8: That I have the tools, skills and confidence to communicate.9: That I have equal access to education and life long learning.10: That I can work and volunteer.
3

Guidance notes1. The following structure chart is based on the principles of good practice to promote
independence and autonomy for adults with sight loss. There is therefore an emphasis on early intervention and a clear pathway to ensure that services are well coordinated across health and social care.
2. It is a pathway for any adult who experiences sight loss, whether through a diagnosed eye condition or as a secondary factor (due to stroke, dementia or head injury for instance). Thus it is referred to as a sight loss pathway, not an eye care pathway.
3. The pathway is designed to ensure seamless transition from NHS diagnosis and interventions, through emotional support, information, reablement (visual impairment rehabilitation), maximising residual vision, and other social care supports, to full autonomy, independence, health and wellbeing.
4. The policy framework, systems, structures, and shape of services across the four countries of the UK vary considerably but the basic principles of early intervention to address presenting needs, followed by community care assessment of any outstanding needs to determine eligibility for services should always apply.
5. In practice, the pathway for people with sight loss varies considerably, not just across the four countries but also across different local authorities in the UK. The aim of this pathway is to promote a unified best practice response:
• It is not a fixed model for delivery and it is not set in stone.
• It only appears linear as a way of representing it easily. Actual practice will vary and flexibility is vital.
• People may join the pathway at different points and may be referred back to an earlier stage at any point.
• There may be several different entry points or referral routes into the pathway depending on circumstance – via Certificate of Vision Impairment (CVI) or Certification of Blindness or Defective Vision (BP1) in Scotland, specialist clinics (stroke, falls etc), GPs, Optometrists and so on.
• The pathway represents best principles but should not be seen as prescriptive.
• In the same way, the pathway does not dictate specific models for service delivery, such as Eye Clinic Liaison Officer (ECLO) because models across the country may vary whilst aiming to deliver the same outcomes.
• The final process (social care supports) ceases to follow a clear pathway because it develops according to the choices and needs of the person. Thus it is only represented as one line of the process map, although in reality it may be very complex.
4

6. The Adult UK sight loss pathway also represents the ideal process map to underpin the set of outcomes developed by blind and partially sighted people – Seeing it my way.
7. The referral mechanisms of Certificate of Vision Impairment (CVI) or Certification of Blindness or Defective Vision (BP1), Referral of a Vision Impaired Patient (RVI) and Low Vision Leaflet (LVL) are used to different degrees across the UK but the only route to registration is the Certificate of Vision Impairment (CVI), or in Scotland the Certification of Blindness or Defective Vision (BP1).
8. At any stage people may be referred or signposted on to statutory or voluntary, local or national, social care services, as appropriate to their needs.
9. The critical factor of success and effectiveness for the visual impairment assessment and rehabilitation interventions is that they should be conducted by a specialist, qualified professional. The accompanying framework clarifies what this means in practice.
10. The framework does not go into extensive detail about the tasks carried out by any professionals because it seeks to give an overview, not an exhaustive catalogue.
11. In some parts of the UK the Rehabilitation professional is required to carry out the full Community Care Assessment, although this is not usually part of this specialist role.
12. It should be noted that no comparable provisions to Part 2 of the Welfare Reform Act 2009: Disabled People Right to Control Provision of Services, have been enacted in Northern Ireland.
13. In Scotland integrated sensory services are already in place or are being developed across the country.
14. Registration in Scotland is currently under review.
5
The
Adu
lt U
K s
ight
loss
pat
hway
Proc
esse
s Sy
stem
s an
d St
ruct
ures
Ref
erra
l
Dia
gnos
is
Early
Inte
rven
tion
(Adv
ice,
info
rmat
ion
and
emot
iona
l sup
port
)
Reg
istr
atio
n an
d A
sses
smen
t(S
tatu
tory
R
equi
rem
ents
)
Early
Inte
rven
tion
(Rea
blem
ent)
Ass
essm
ent
of e
ligib
le n
eed
Soci
al c
are
supp
orts
Info
rmat
ion
and
advi
ce –
e.g
. Eye
Clin
ic L
iais
on
Offi
cer (
EC
LO),
Visi
on S
uppo
rt S
ervi
ce o
r sim
ilar
GP,
acu
te h
ospi
tal s
ervi
ces,
or s
elf-r
efer
ral
Opt
omet
rist,
Opt
icia
n or
Low
vis
ion
serv
ice
Reg
iste
r of B
lind
and
Par
tially
Sig
hted
adu
lts
S
peci
alis
t vis
ual i
mpa
irmen
t ass
essm
ent o
f soc
ial c
are
need
Oph
thal
mol
ogis
tC
ertifi
cate
of V
isio
n Im
pairm
ent (
CV
I) or
Cer
tifica
tion
of B
lindn
ess
or D
efec
tive
Visi
on (B
P1)
(Sco
tland
)
6

The
Adu
lt U
K s
ight
loss
pat
hway
Proc
esse
s Sy
stem
s an
d St
ruct
ures
Ref
erra
l
Dia
gnos
is
Early
Inte
rven
tion
(Adv
ice,
info
rmat
ion
and
emot
iona
l sup
port
)
Reg
istr
atio
n an
d A
sses
smen
t(S
tatu
tory
R
equi
rem
ents
)
Early
Inte
rven
tion
(Rea
blem
ent)
Ass
essm
ent
of e
ligib
le n
eed
Soci
al c
are
supp
orts
Visu
al Im
pairm
ent R
ehab
ilita
tion
prog
ram
me
Com
mun
ity C
are
Ass
essm
ent
E
ligib
le
Not
Elig
ible
Com
mun
ity b
ased
C
omm
unity
bas
ed
soci
al c
are
supp
orts
se
rvic
es
(sta
tuto
ry fu
ndin
g)
(no
stat
utor
y fu
ndin
g)
Inde
pend
ent l
ivin
g w
ith fu
ll ch
oice
and
con
trol
7

Fram
ewor
k of
the
Adu
lt U
K s
ight
loss
pat
hway
for a
chie
ving
in
depe
nden
t liv
ing
outc
omes
(T
his
fram
ewor
k un
derp
ins
the
outc
omes
of t
he S
eein
g it
my
way
fram
ewor
k)
Proc
esse
sPr
ofes
sion
als
invo
lved
Qua
lifica
tion
Hea
lth a
nd S
ocia
l Car
e in
terv
entio
ns
Cor
e ac
tivity
un
dert
aken
Oth
er p
ract
ition
ers
with
sp
ecia
list s
kills
for f
urth
er
inte
rven
tions
Ref
erra
l and
di
agno
sis
Oph
thal
mol
ogis
tC
ore
com
pete
nce
and
part
of s
tand
ard
qual
ifica
tion
Und
erta
ke v
isio
n an
d ey
e he
alth
scr
eeni
ng
and
asse
ssm
ent
Trea
tmen
t of e
ye
cond
ition
s
Low
vis
ion
asse
ssm
ent
Ref
erra
l
Oth
er p
rofe
ssio
nals
with
in
low
vis
ion
serv
ice
Opt
omet
rist
Orth
optis
t
Cor
e co
mpe
tenc
e an
d pa
rt of
sta
ndar
d qu
alifi
catio
n;
high
er q
ualifi
catio
n in
low
vi
sion
is a
lso
avai
labl
e;
accr
edita
tion
in W
ales
and
so
me
othe
r are
asO
phth
alm
ic N
urse
Dip
lom
a in
low
vis
ion
Dis
pens
ing
optic
ian
Cor
e co
mpe
tenc
e an
d pa
rt of
sta
ndar
d qu
alifi
catio
n;
high
er q
ualifi
catio
n in
lo
w v
isio
n av
aila
ble;
ac
cred
itatio
n in
Wal
es a
nd
som
e ot
her a
reas
8

Proc
esse
sPr
ofes
sion
als
invo
lved
Qua
lifica
tion
Hea
lth a
nd S
ocia
l Car
e in
terv
entio
ns
Cor
e ac
tivity
un
dert
aken
Oth
er p
ract
ition
ers
with
sp
ecia
list s
kills
for f
urth
er
inte
rven
tions
Ref
erra
l and
di
agno
sis
Oph
thal
mol
ogis
tC
ore
com
pete
nce
and
part
of s
tand
ard
qual
ifica
tion
Und
erta
ke v
isio
n an
d ey
e he
alth
scr
eeni
ng
and
asse
ssm
ent
Trea
tmen
t of e
ye
cond
ition
s
Low
vis
ion
asse
ssm
ent
Ref
erra
l
Oth
er p
rofe
ssio
nals
with
in
low
vis
ion
serv
ice
Opt
omet
rist
Orth
optis
t
Cor
e co
mpe
tenc
e an
d pa
rt of
sta
ndar
d qu
alifi
catio
n;
high
er q
ualifi
catio
n in
low
vi
sion
is a
lso
avai
labl
e;
accr
edita
tion
in W
ales
and
so
me
othe
r are
asO
phth
alm
ic N
urse
Dip
lom
a in
low
vis
ion
Dis
pens
ing
optic
ian
Cor
e co
mpe
tenc
e an
d pa
rt of
sta
ndar
d qu
alifi
catio
n;
high
er q
ualifi
catio
n in
lo
w v
isio
n av
aila
ble;
ac
cred
itatio
n in
Wal
es a
nd
som
e ot
her a
reas
Early
in
terv
entio
n (a
dvic
e an
d in
form
atio
n)
Eye
Clin
ic L
iais
on
Offi
cer (
EC
LO),
Hos
pita
l Inf
orm
atio
n O
ffice
r, Vi
sion
su
ppor
t ser
vice
or
sim
ilar
Cer
tifica
te in
Eye
Clin
ic
Sup
port
Stu
dies
Em
otio
nal s
uppo
rt
Info
rmat
ion
abou
t eye
co
nditi
on
Info
rmat
ion
abou
t si
ght l
oss
path
way
Ass
ist w
ith
certi
ficat
ion
proc
ess
Exp
lain
ben
efits
of
regi
stra
tion
Ref
erra
ls to
sta
tuto
ry
and
volu
ntar
y se
ctor
se
rvic
es
Sig
npos
ting
to lo
cal
and
natio
nal s
uppo
rt se
rvic
es
Cou
nsel
lors
Bef
riend
ers
Oth
er c
omm
unity
bas
ed
soci
al c
are
agen
cies
and
vo
lunt
ary
sect
or a
genc
ies
Ref
erra
l fr
om H
ealth
to
Soc
ial
Car
e
Reg
iste
r Offi
cer,
front
line
dut
y st
aff
Min
imum
requ
irem
ent f
or
spec
ialis
t kno
wle
dge
of
visu
al im
pairm
ent,
sigh
t los
s pa
thw
ay a
nd re
gist
ratio
n pr
oces
s
Take
refe
rral
Exp
lain
ben
efits
of
regi
stra
tion
Invi
te re
gist
ratio
n
Ref
er o
n fo
r ent
ry o
nto
regi
ster
dat
a ba
se a
nd
for v
isua
l im
pairm
ent
asse
ssm
ent o
f nee
d
9

Proc
esse
sPr
ofes
sion
als
invo
lved
Qua
lifica
tion
Hea
lth a
nd S
ocia
l Car
e in
terv
entio
ns
Cor
e ac
tivity
un
dert
aken
Oth
er p
ract
ition
ers
with
sp
ecia
list s
kills
for f
urth
er
inte
rven
tions
Reg
istr
atio
n,
asse
ssm
ent
and
early
in
terv
entio
n (r
eabl
emen
t)
Reh
abili
tatio
n O
ffice
r for
Vis
ual
Impa
irmen
t
Dip
lom
a in
vis
ual
impa
irmen
t reh
abili
tatio
n,
or e
quiv
alen
t
Visu
al im
pairm
ent
asse
ssm
ent o
f pr
esen
ting
need
–
Func
tiona
l vis
ion
and
eye
heal
th s
cree
ning
an
d a
sses
smen
t
Furth
er e
mot
iona
l su
ppor
t
Mor
e de
taile
d in
form
atio
n ab
out
eye
cond
ition
Teac
hing
cor
e or
ient
atio
n an
d m
obili
ty s
kills
and
te
chni
ques
Teac
hing
co
mm
unic
atio
n sk
ills:
• Use
of a
ssis
tive
tech
nolo
gy
• Bra
ille
Mob
ility
inte
rven
tion
(e
.g. g
uide
dog
, or
My
Gui
de s
chem
e)
Acc
ess
tech
nolo
gy tr
aine
rs
Oth
er p
rofe
ssio
nals
with
in
low
vis
ion
serv
ice
Reh
abili
tatio
n w
orke
r as
sist
ants
Occ
upat
iona
l The
rapi
st
train
ed to
wor
k w
ith p
eopl
e w
ith s
ight
loss
Dua
l sen
sory
and
com
plex
ne
eds
spec
ialis
ts (e
.g. G
uide
C
omm
unic
ator
s)
Edu
catio
n an
d lif
elon
g le
arni
ng s
peci
alis
ts
Voca
tiona
l spe
cial
ists
Com
mun
ity b
ased
sup
port
serv
ices
(e.g
. soc
ial g
roup
s)
10

Proc
esse
sPr
ofes
sion
als
invo
lved
Qua
lifica
tion
Hea
lth a
nd S
ocia
l Car
e in
terv
entio
ns
Cor
e ac
tivity
un
dert
aken
Oth
er p
ract
ition
ers
with
sp
ecia
list s
kills
for f
urth
er
inte
rven
tions
Reg
istr
atio
n,
asse
ssm
ent
and
early
in
terv
entio
n (r
eabl
emen
t)
Reh
abili
tatio
n O
ffice
r for
Vis
ual
Impa
irmen
t
Dip
lom
a in
vis
ual
impa
irmen
t reh
abili
tatio
n,
or e
quiv
alen
t
Visu
al im
pairm
ent
asse
ssm
ent o
f pr
esen
ting
need
–
Func
tiona
l vis
ion
and
eye
heal
th s
cree
ning
an
d a
sses
smen
t
Furth
er e
mot
iona
l su
ppor
t
Mor
e de
taile
d in
form
atio
n ab
out
eye
cond
ition
Teac
hing
cor
e or
ient
atio
n an
d m
obili
ty s
kills
and
te
chni
ques
Teac
hing
co
mm
unic
atio
n sk
ills:
• Use
of a
ssis
tive
tech
nolo
gy
• Bra
ille
Mob
ility
inte
rven
tion
(e
.g. g
uide
dog
, or
My
Gui
de s
chem
e)
Acc
ess
tech
nolo
gy tr
aine
rs
Oth
er p
rofe
ssio
nals
with
in
low
vis
ion
serv
ice
Reh
abili
tatio
n w
orke
r as
sist
ants
Occ
upat
iona
l The
rapi
st
train
ed to
wor
k w
ith p
eopl
e w
ith s
ight
loss
Dua
l sen
sory
and
com
plex
ne
eds
spec
ialis
ts (e
.g. G
uide
C
omm
unic
ator
s)
Edu
catio
n an
d lif
elon
g le
arni
ng s
peci
alis
ts
Voca
tiona
l spe
cial
ists
Com
mun
ity b
ased
sup
port
serv
ices
(e.g
. soc
ial g
roup
s)
Reg
istr
atio
n,
asse
ssm
ent
and
early
in
terv
entio
n (r
eabl
emen
t)
Reh
abili
tatio
n O
ffice
r for
Vis
ual
Impa
irmen
t
Dip
lom
a in
vis
ual
impa
irmen
t reh
abili
tatio
n,
or e
quiv
alen
t
Teac
hing
and
en
ablin
g in
depe
nden
t liv
ing
skill
s
Low
vis
ion
asse
ssm
ent (
poss
ibly
de
liver
ed b
y, o
r in
tand
em w
ith lo
w v
isio
n th
erap
ist,
opto
met
rist
or o
ptic
ian)
Inte
rven
tions
to
max
imis
e us
e of
re
sidu
al v
isio
n
Ref
erra
ls to
sta
tuto
ry
and
volu
ntar
y se
ctor
se
rvic
es
Sig
npos
ting
to lo
cal
and
natio
nal s
uppo
rt se
rvic
es
Ass
essm
ent
of e
ligib
le
need
Soc
ial w
orke
rs
(Not
e: T
his
proc
ess
may
in s
ome
area
s be
con
duct
ed b
y R
ehab
ilita
tion
Offi
cers
)
Soc
ial w
ork
dipl
oma
or
degr
ee, o
r equ
ival
ent
Com
mun
ity c
are
asse
ssm
ent o
f el
igib
le n
eed
Res
ourc
e al
loca
tion
Car
e m
anag
emen
t
Com
mun
ity b
ased
soc
ial
care
wor
kers
and
sup
ports
(in
clud
ing
priv
ate
and
volu
ntar
y se
ctor
soc
ial c
are
prov
ider
s)
11

V I S I O
THE RIGHT TO SIGHT
n
UK
This Adult UK sight loss pathway document has been produced by the UK Vision Strategy ‘Future of Rehabilitation’ Group, which aims to ensure that every person who experiences sight loss can benefit from the provision of early access to a nationally agreed pathway promoting independence, choice and control over their lifestyle.
www.vision2020uk.org.uk/UKVisionstrategy
Top Related