






Languages
Pages
Legal


1
7” Casing Drop Incident
DrillSafe Forum - June 2nd 2011
Nick Muecke
Vermilion Oil & Gas Australia

2
Cazaux
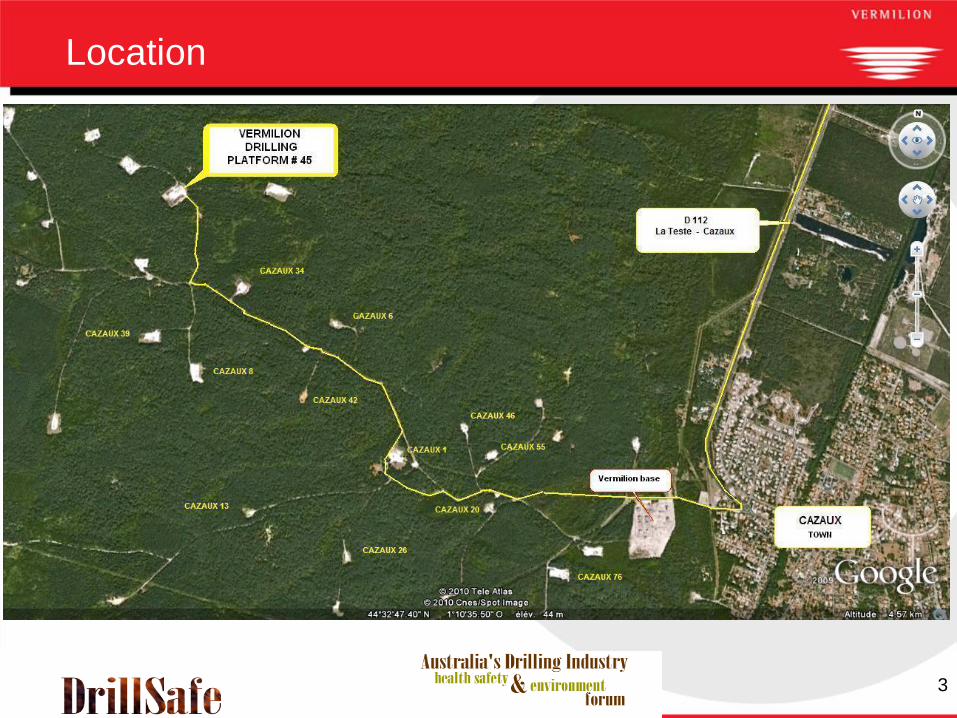
Location
3
Location
4
8 ½” hole drilled to 3497m MD (3275m TV)
Hole stability, torque and drag issues and rig
related problems
Hole logged
Rigged up and ran 7” casing to 2521m where
it held up (20 hours of operations)
Attempted to work through (6 hrs of ops)
POH laying down casing joints in singles
Background to Incident

5
The procedure to lay out pipe was as follows:
1. Break out a joint using the TDS system
2. Lift the joint using Side Door Elevator (SDE) / bails attached
to top drive
3. Push the joint over to the V-door and lower pin until its
movement is controlled by a bogey running along the
catwalk
4. Casing joint is allowed to rest at top of V-door while a soft
sling is wrapped around the box end and attached to the jib
crane;
5. Once the soft sling is safely secured to the jib, the SDE lock
pin is removed and the elevators opened;
6. The joint is then lowered down the V-door by jib crane with
pin end controlled by the catwalk bogey.
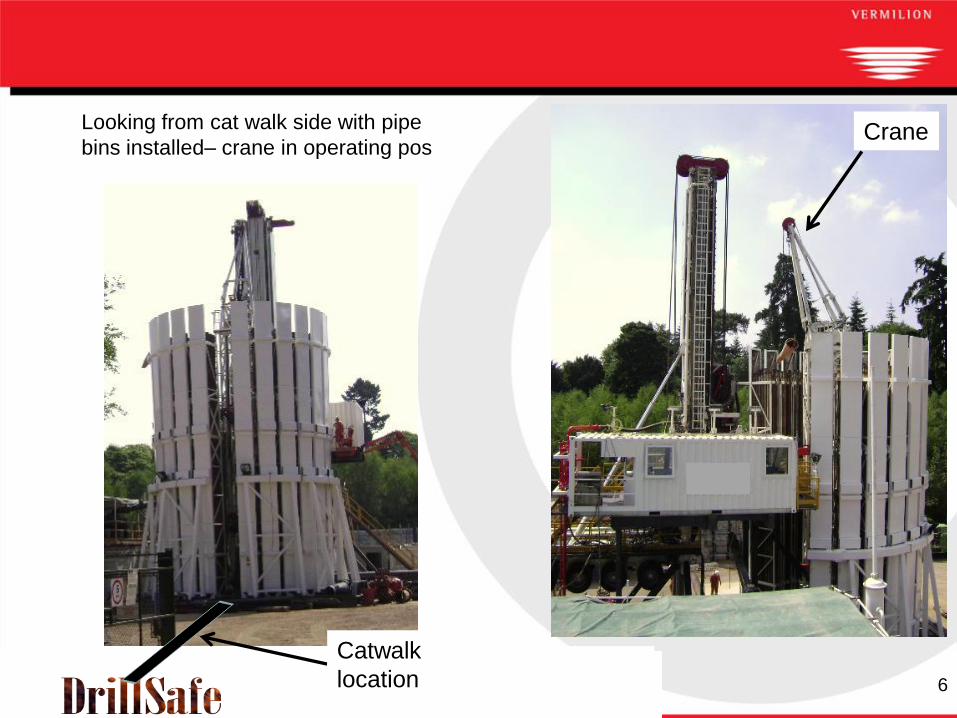
Picking Up/Laying Down Casing
6
CraneLooking from cat walk side with pipe
bins installed– crane in operating pos
Catwalk
location
7
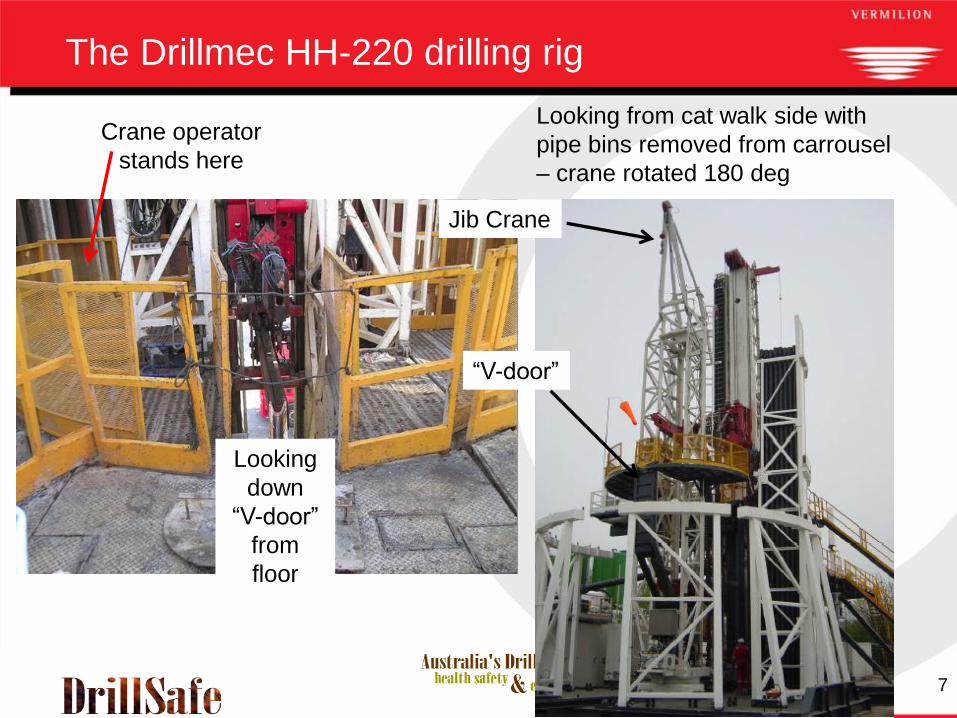
The Drillmec HH-220 drilling rig
Looking from cat walk side with
pipe bins removed from carrousel
– crane rotated 180 deg
Jib Crane
“V-door”
Looking
down
“V-door”
from
floor
Crane operator
stands here

8
Picking Up/Laying Down Casing
“V-door” & slide
down to catwalk
Looking down
“V-door” from
floor
Crane from
drill-floor
Crane operator
stands here

9
85 joints laid out over 8 ½ hrs
10 minutes from shift change @ 18:00 hrs a joint of casing
was lowered down the V-door using Side Door Elevator
(SDE) /bails attached to top drive
As the box end came to rest on the top of the V door, the
safety pin was removed from the SDE and the elevator
was opened before the sling on the casing joint was
secured to the crane
The casing joint fell in an uncontrolled manner down the
V-door, eventually coming to rest with the pin end some
9m past the end of the catwalk.
No one was hurt and no equipment was damaged
What Happened
10
Operations were stopped to allow a preliminary
investigation to be carried out
Procedure changed to ensure the sling is installed
and tension taken on the winch prior to removing
safety pin from the SDE
Safety meeting held with both crews to review
incident and highlight the dangers
Elevator was taken out of service and replaced with
backup set
Immediate Actions
11
The same procedure, the removal of the elevator safety
pin before the weight of load had been transferred via the
connected sling from the elevators to the jib crane, had
been used for the previous 89 joints without incident.
Personnel involved on the rig floor had all been with the
Contractor for at least 3 yrs and in position for at least 2
yrs and were 11 days into their 2 week hitch.
Crew had run 7” (and other sizes) numerous times, but
had never been involved with pulling casing
Incident occurred 10 minutes prior to the end of the shift.
Floor hand "operating" the elevators at the time possibly
didn't fully understand the critical function of the safety
pin and that it should not be removed prior to completing
installation of sling between casing joint and jib crane.
Investigation Findings
12
Personnel carrying out activities at ground level were all
standing in positions that would keep them safe when pipe
moving
No Task Based Risk Assessment (TBRA – the Contractor’s
equivalent to the JSA) was carried out prior to POH with casing
A TBRA was available for use as a guide
A toolbox talk was held, but did not include discussion on the
need for good communication or what should be communicated
No contractor standard operating procedure (SOP) existed for
laying down casing
Once the operation to lay down casing commenced there was
little oversight of activities by either Toolpusher or Drilling
Supervisor
Equipment inspection revealed that safety the pin cannot be
installed if the latch is not fully closed
Investigation Findings

13
Varco elevator design - latch cannot open when under load even
if safety pin is removed
Elevator has additional hole for safety pin storage during
transportation
Was the pin installed in the “transport hole”?
Investigation Findings

14
Causal Factors
The main causal factor contributing to the incident
was the removal of the elevator safety pin prior to the
weight of load being transferred from the elevators to
the jib crane via the connected sling.
Floor hand "operating" the elevators at the time
possibly didn't fully understand the critical function
of the safety pin.
Causal Factors

15
Root Causes
No TBRA conducted for operation despite none of
the crew having prior experience with this operation
No standard operating procedure in place for pulling
and laying out of casing.
Insufficient senior level supervision on the rig floor
for an unfamiliar operation
Root Causes

16
Reinforce requirement for TBRA prior to operations
or for any significant change in operation or
personnel and ensure all involved personnel
participate
Reinforce requirement for senior supervisors to
spend time “on the floor”, particularly during non-
routine operations.
Generate SOP for pulling out of hole with casing
Outcomes

17
Revise TBRA for pulling / laying down casing and
include:
Communication requirements
Order of steps associated with pulling / laying out
casing
Positions of all personnel involved including lease
hands and forklift driver
Guidance required on steps to cover pulling /
installing safety pin, connecting / disconnecting
elevators and connecting/disconnecting sling to
crane
Associated operational risks
Outcomes

18
Questions
Top Related