X-ray Diffraction Analysis Of Central Asian Vesical Calculi
15
Henry Ford Hospital Medical Journal Volume 12 | Number 2 Article 4 6-1964 X-ray Diffraction Analysis Of Central Asian Vesical Calculi Jonathan Parsons Follow this and additional works at: hps://scholarlycommons.henryford.com/hmedjournal Part of the Life Sciences Commons , Medical Specialties Commons , and the Public Health Commons is Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons. For more information, please contact [email protected]. Recommended Citation Parsons, Jonathan (1964) "X-ray Diffraction Analysis Of Central Asian Vesical Calculi," Henry Ford Hospital Medical Bulletin : Vol. 12 : No. 2 , 187-200. Available at: hps://scholarlycommons.henryford.com/hmedjournal/vol12/iss2/4
Transcript of X-ray Diffraction Analysis Of Central Asian Vesical Calculi

Henry Ford Hospital Medical Journal
Volume 12 | Number 2 Article 4
6-1964
X-ray Diffraction Analysis Of Central Asian VesicalCalculiJonathan Parsons
Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal
Part of the Life Sciences Commons, Medical Specialties Commons, and the Public HealthCommons
This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in HenryFord Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons. For more information, please [email protected].
Recommended CitationParsons, Jonathan (1964) "X-ray Diffraction Analysis Of Central Asian Vesical Calculi," Henry Ford Hospital Medical Bulletin : Vol. 12 :No. 2 , 187-200.Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol12/iss2/4

Henry Ford Hosp. Med. Bull. Vol. 12, June, 1964
X-RAY DIFFRACTION ANALYSIS OF CENTRAL ASIAN VESICAL CALCULI
JONATHAN PARSONS*
I T WAS THROUGH A CONVERSATION with a visiting urologist, during a medical meeting at this hospital, that an unusual opportunity presented itself to analyze renal calculi from one of the most remote areas of the world. The author was told that Dr. Carl Friedericks, a medical missionary on furlough from Nepal Asia, desired to have studies made upon a small group of calculi, coming from the stone-bearing area of Asia which includes portions of India and Assam as well as Nepal. The analysis of urinary calculi by the x-ray diffraction powder method has been a regular service of the Edsel B. Ford Institute for Medical Research for about 12 years. The chance to analyze and report on these unusual calculi was readily accepted.
Nepal is an independent state, located in the heart of the Himalayan mountains, on the northeast border of India and sandwiched between the subcontinent and communist-dominated Tibet. Until 1954 its people, enslaved by superstition and ignorance, were trying to make a living by farming, using implements and methods which had not changed for centuries. At mid-century a great enlightenment for the country occurred. The powerful Rana family of prime ministers was overthrown by Tribhuvan and at the latter's untimely death, his son Mahendra Bir Birkram Shah Deva became King.
King Mahendra, a man of great heart and action, readily accepted the challenge to strive to remove the archaic and tyrannical rule of the past. He invited the Christian Church, with its medical missionaries, to enter this isolated country, where for centuries any influence from the outside world has been excluded. A United Church Mission was established consisting of 58 christian workers from eight countries, encouraged by grants of land and buildings.
After the establishment of a medical welfare center at Bhatgaon and a hospital at Katmandu, Dr. Carl Friedericks established a medical clinic and hospital at Tansen, three days journey by foot over mountainous trails from Katmandu. In 1959 over 16,000 out-patients visited this hospital, many traveling miles over these tortuous trails bearing their infirmities.'
*Edsel B. Ford Institute for Medical Research.
187

PARSONS
It has been reported by Butt' that 70 per cent of vesical calculi from India are composed of urates and oxalates. Cauiy in 1931 cited a report of Thomson stating that, while treating 2,967 cases of urinary calculi in India, five cases of renal calcuU and 2,962 cases of vesical calculi were found. He also contrasted the latter low incidence of renal to vesical calculi in India with his own finding of a ratio of three renal to one vesical in the St. Louis region of the United States.
Although the occurrence of vesical calculus disease in this country seems to be prominently associated with the age range between 60 and 70̂ '', the age of vesical neck obstruction, Price= in 1945 reported that in the Shantung Province of North China, 74 per cent of the cases of vesical calculi were from children 5-15 years of age with only 7 per cent coming from the age group over 25 years.
Reports from this country indicate that only 7 to 12 per cent of the cases
of vesical calculus disease occur among the female sex''''. Dr. Friederick reports the
occurrence of vesical calculi among females in Nepal to be practically non-existant.
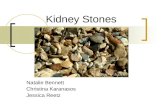
The six bladder calcuh (Figure 1), sent to our laboratory for analysis, represent a wide age range coming from various caste groups within the area. A colleague of Dr. Friederick's writes, "We have had enough stones recently to pebble a beach of which the six included are a representative selection." It is noted that there is an older, almost aboriginal group of people which makes up a large part of the population and which is not represented here because this Magar group or caste didn't present many calculi. Dr. Friederick comments that the reason for the latter fact may be well be a subject for further study. He asks, "Can one imagine those poor people traveling many miles over rough trails in that misery and how glad we are to be there to relieve their pain?"
CASE REPORTS
CASE 1. (L. B.) — This 66-yer-old male farmer, living in a village 38 miles from Tansen, is a member of the Kshetri Caste. His symptoms were a burning micturition for three years with obstructed flow and haematuria. Upon sounding a stone was revealed which was removed by operaticn (10-27-59). The stone appeared to be of mixed composition 48 x 35 mm. in size and weighing 42.3 gms. There were no complications. The catheter was removed on the fourth day and the patient was discharged on the eighth day.
CASE 2. (G. S.) — This 76-year-old male farmer is a member of the Khati Caste, living in a village about 50 miles from Tansen. His symptoms were obstructed urine for seven to eight years prior to operation. He had purulent or blood-stained discharge in urine. He had his own catheter which he passed frequently. The prostate was enlarged which made sounding not possible. The bladder mucous membrane was very granular and unhealthy. Lithotomy and prostatectomy were performed (11-21-59) revealing a large stone, 47 x 40 mm. in size and weighing 45.6 gms. and an enormous prostrate. At the time that this report was written (11-28-59) the patient was still in the hospital but was "doing well."
CASE 3. (C. K.) — This young farmer, 15-years-old and Hving in a village 10 miles from Tansen, is a member of the Bechium Caste. He had dysuria since infancy which had become worse for the month prior to operation. He had severe burning micturition and passed his urine, filled with pus and blood, in spurts. He was an emaciated and very small, sick-looking boy. Only calculus disease was found. An operation was performed on (8-8-59) producing a large stone measuring 52 x 40 mm. and weighing 61.0 gms. The bladder mucous membrane was very unhealthy. The catheter was kept in for eight days because of perivesical infection. His discharge occurred on the 18th day.
188

VESICAL CALCULI
CASE 4. (P. N.) — A 25-year-old man was a farmer belonging to the Brahman Caste and living in a village three miles from Tansen. His symptoms were a fever, dysuria and blood and pus in urine for 25 days previous to surgery, which took place on (10-24-59). An irregular stone 35 x 28 mm. in size and weighing 18.2 gms. was removed with no complications. The catheter was removed on the fourth day and he was discharged on the 15th day.
CASE 5. (N. M.) — This 84-year-old male farmer belonged to the Thakuri Caste and lived in a village 30 miles from Tansen. He had difficulty in micturition for six months, producing a very poor stream. There was no haematuria nor enlargement of prostate. The stone was revealed by sounding. An operation was performed on (8-4-59), two stones being removed whose size were 35 x 27 mm. and 36 x 23 mm. and weighing 14.2 and 12.6 gms. respectively. This very old man was up on the second day with catheter in. The latter was removed on the fourth day. There were no complications but burning micturition did not clear up for some time. He was discharged on the 17th day.
CASE 6. (D. B.) — A 21/2-year-old boy, son of a blacksmith belonging to the Sunar Caste, lived in a village six miles from Tansen. After having had urinary obstructions for six months, a stone was revealed present by sounding. An operation performed on (11-14-59) produced a small stone 17 x 12 mm. in size and weighing 1.8 gms. The catheter was not kept in and urine was readily passed from beginning of recovery. The child was discharged on the ninth postoperative day.
ANALYSIS BY X-RAY DIFFRACTION The method and results of the application of x-ray diffraction to the analysis of
600 urinary calculi was described by Prien and Frondel (1947)'. Parsons and Eurs' (1959) reported the application of x-ray diffraction to the analysis of inorganic pathological crystals found in tissue. In the present study an x-ray generator and Debye-Scherrer powder cameras similar to those described by Prien et. al. were used. After fracturing each calculus, a few milligrams of powder were picked from each of the differently appearing areas. When each minute pile of powder had been reduced to about 200 mesh size, using micro mortar and pestle methods, the powder was introduced into Lindemann glass capillary mounts. These mounts, consisting of the specimen powder supended in glass capillaries 0.01 mm. in wall thickness and 0.2 mm. in diameter, were placed in the powder camera and bathed for two hours by nickel filtered copper x-radiation generated at 35 K V and 20 ma. A complete description of the x-ray diffraction powder technique is found elsewhere' ".
X-ray diffraction powder analysis results in a film or chart record which is characteristic of a specific material in a manner similar to the way fingerprints are characteristic of a particular individual. A file of diffraction patterns thus can be used as a method of analysis, just as a file of fingerprints can be used as a method of personal identification.
RESULTS
The fractured calculi from the six cases described are shown in Figures 2-7 with arrows indicating the regions from which samplings were taken for x-ray powder analysis. The x-ray diffraction findings are indicated in the captions for the above figures. The following four constituents were found to be present:
(1) calcium oxalate monohydrate (CaC204*H20)
(2) uric acid (C5H4N4O3)
(3) magnesium ammonium phosphate hexahydrate (Mg NH4P04-6H20)
(4) ammonium acid urate (NH4C5H3O3N4)
189

PARSONS
The x-ray diffraction powder patterns for the compounds found in the analysis of the calculi discussed in this paper are shown in Figure 8. Patterns 1, 2, 4, and 5 are pure constituent patterns; patterns 3 and 6 are patterns for the frequently occurring combinations of constituents. The diameter of each arc in these patterns is a function of the distance between one set of parallel planes of atoms in that particular crystalline compound. The varying darknesses of these different arcs depend upon the relative number of atoms in the various existing atom planes and the diffracting efficiency of the type of atom involved. Tabular data for the latter interplanar distances and relative intensities of diffraction arcs are given in Table I for the constituent patterns involved in this report.
URINARY CALCULI FROM MICHIGAN: Since 1950, 880 urinary calculi coming from the Detroit, Michigan region of the United States have been analyzed in this laboratory using the x-ray diffraction powder method. Table I I shows the number and percentage of these general urinary tract stones of the various constituent types. In this table the word "mixed" implies the presence of a minor amount of one or more of the other listed components.
DISCUSSION
Whereas the usual types of calculi analyzed in this laboratory and reported in Table I I come from all parts of the urinary tract the particular group of calculi from Nepal are bladder stones. Dr. Friedericks states that kidney stones are quite uncommon in that part of Asia and that from 18,000 patients he can recall only 10 cases involving renal calculi. They have removed hundreds of vesical calculi, however, and have usually but not always found an obvious cause of urinary retention" such as prostatic hypertrophy. In such cases the stone could quite conceivably be a result of retention and concentration of urine. Dr. Friederick continues to comment, "We have found that if the cause of the retention is not removed, stones can quickly recur in the cases of the older men. On the other hand in the cases of the larger group of children, no obvious strictures or other causes of urinary retention have been found. Treatment of them has consisted merely of removing the stones. In children these stones rarely recur. It is in the cases of children that the etiology is most puzzling. Why do the vesical calculi appear in the first place and why do they not recur if we do nothing specific about their basic cause?"
In considering the group of patients seen in the Nepal clinic a few factors have been observed. First, the formation of bladder stones .seems to be limited almost entirely to the male sex. Dr. Friedericks being able to recall treating only one woman personally from the thousands who have visited his hospital. Secondly, this condition seems to involve chiefly men and boys at extremes of age. In the third place, there is a preponderance of cases among the Aryan groups in that part of Asia.
A bit more information about Nepal from Dr. Friedericks correspondence with the author may be pertinent to this report. The probable aboriginal groups are gone. The oldest residents in the Polpa district are the Magars. These are a Mongoloid people speaking a Burmo-Chinese language, with their own customs and practicing a form of
190

VESICAL CALCULI
Hindu religion which they have adopted. Scattered throughout Nepal are the similar
ethnic groups such as Rai, Limbu, Thamung, Newar, Gurung, and Sherpa. In the
past three centuries the Aryan priestly Brahmin and warrior Kshetri migrated from
India into Nepal in sufficient strength to achieve political and religious dominance.
With them came a trickle of low-caste Negroid peoples. Thus Nepal has a great
mixture of races. The caste system has tended to maintain the purity of racial stock.
Returning to the subject of this paper, the great majority of bladder stone cases are
from these invaders from India.
It might seem possible to find marked dietary differences between these ethnic
groups which would give clues as to any dietary cause, but this is not the case. There
are more differences within any given group because of economics and geography than
there are between groups. Although the older groups eat meat so do many of the Aryans.
All of these people have a diet which is largely carbohydrates. Nearly everyone's urine
is acid in reaction.
When the results of this study, as shown in the captions to Figures 2 to 7, are
examined two rather striking differences from composition findings for stones analyzed
by the author at Edsel Ford Institute for Medical Research, are observed. First,
ammonium acid urate, which has not been found in the 880 urinary stones from the
Detroit area, was present in three of the six representative cases discussed. Table I I
indicates that the three urate stones analyzed in this laboratory since 1950 were
composed principally of sodium, acid urate and comprised only about two tenths of
one per cent of the total number of urinary tract stones. The second significant differ
ence in the results of the Asian study as compared with the stone composition range
in this country is the complete lack of finding of apatite, the complex calcium phosphate
which is present in about twenty per cent of the calculi analyzed locally. The author
hastens to state that the above two observations may not be truly represenative of the
vesical calculi from Nepal sinec the number of stones analyzed was limited.
SUMMARY
The results of x-ray diffraction powder analysis for six cases of vesical calculus
disease, from the independent state of Nepal, are reported. This small number of
representative bladder stones were taken from thousands of patients operated upon in
this remote region where this condition is endemic. X-ray diffraction powder patterns
for the resulting vesical calculus constituents together with molecular interplanar spacings
are given. For comparison purposes Table I I gives a urinary calculus composition report
for 880 stones analysed by the author and originating in the general geographical region
of Detroit, Michigan. It is noteworthy that ammonium acid urate is found in three of
the six Asian stones analyzed. The fact that no apatite (calcium phosphate) appears
as a constituent of these Asian bladder stones also may be significant. Other observations
which are made is that vesical calculus disease in Nepal is confined principally to males
at the extremes of age.
191

PARSONS
A C K N O W L E D G M E N T S
The author wishes to acknowledge the help of Dr. Carl W. Friedericks medical missionary and surgeon assigned to the United Church Mission in Nepal, f rom whom the vesical calculi and case reports were procured. His helpful communications from which direct and indirect quotations have been used for this report have contributed historical, geographical and other information pertinent to this report.
Dr. John W. Best f rom York, Pennsylvania first talked to the author about the possibility of this study. Thanks are also extended to him for his help.
The technical assistance of Sik Toon Wong from this Institute, who helped in the preparation of the illustrations and tables is greatly appreciated.
REFERENCES
1. Peters, J. T.: The high hidden kingdom of Nepal. Presbyterian Life, 13:14, 1960.
2. Butt, A. J.: Treatment of urinary lithiasis. Charles C. Thomas, Springfield, 111., 1960.
3. Caulk, J. R.: Litholapaxy; the method of preference for the removal of vesical calculi, Ann Surg. 93:891, 1931.
4. Wishard, W. N. and Nourse, M. H.: Vesical calculus with report of gigantic stone in the female
bladder, J. Urol. 63:794, 1950.
5. Price, P. B.: Experience with calculus of the bladder in North China, Arch. Surg. 50:82, 1945.
6. Twinem, F. P. and Langdon, B. B.: Surgical management of bladder stone, J. Urol. 66:201, 1951. 7. Prien, E. L. and Frondel, C : Studies in urohthiasis: I . The composition of renal calculi, J. Urol.
57:949, 1947.
8. Parsons, J. and Eurs, F. J.: X-ray diffraction analysis of crystals in pathology, Amer. J. Clin. Path. 32:405, 1959. f
^' ^'"^19^4^' ^"'^ Alexander, L. E.: X-ray diffraction procedures. John Wiley & Sons, New York,
10. Azaroff, L. V. and Buerger M. J.: The powder method in x-ray crystallography. McGraw-Hill Book Co., Inc., New York, 1958.
11. Parsons, J.: Zinc phosphate identified as a constituent of urinary calculi. Science, 118:217, 1953.
192

VESICAL CALCULI
Table la Table lb CALCIUM OXALATE URIC ACID
MONOHYDRATE (C.H.O,N.) (CaCjO^ H j O ) d ( A ) I / I i
d ( A ) I / I i 6.60 0.87 5.99 1.00 5.66 0.40 5.77 0.04 4.95 0.87 4.52 0.05 4.75 0.06 4.05 0.03 4.26 0.01 3.79 0.05 3.88 0.87 3.66 0.88 3.74 0.02 3.49 0.01 3.59 0.03 3.33 0.01 3.44 0.01 3.12 0.04 3.30 0.15 2.98 0.47 3.21 0.40 2.92 0.11 3.12 1.00 2.84 0.10 3.03 0.01 2.50 0.20 2.89 0.30 2.44 0.01 2.80 0.15 2.36 0.75 2.58 0.20 2.31 0.01 2.48 0.04 2.26 0.18 2.41 0.04 2.21 0.08 2.34 0.03 2.14 0.04 2.29 0.04 2.08 0.08 2.24 0.20 1.99 0.08 2.20 0.15 1.96 0.10 2.16 0.01 1.93 0.08 2.10 0.02 1.89 0.08 2.04 0.06 1.87 0.04 2.00 0.01 1.85 0.08 1.93 0.03 1.82 0.08 1.88 0.04 1.80 0.08 1.81 0.17 1.74 0.11 1.75 0.03 1.70 0.04 1.67 0.06 1.64 0.02 1.64 0.03 1.63 0.02 1.62 0.06
1.60 0.03
1.56 0.08
1.51 0.01
193

PARSONS
Table Ic MAGNESIUM AMMONIUM
PHOSPHATE HEXAHYDRATE (MgNH4P04.6HjO)
Table I d AMMONIUM ACID URATE
(NH^C5H303N4)
d(A) 6.24 5.91 5.64 5.39 4.61 4.26 4.14 3.47 3.30 3.17 3.04 2.92 2.81 2.69 2.51 2.35 2.25 2.18 2.14 2.06 2.02 1.96 1.93 1.88 1.85 1.80 1.76 1.74 1.72 1.69 1.66 1.60
I / I i 0.01 0.20 0.47 0.11 0.07 1.00 0.11 0.20 0.15 0.01 0.08 0.47 0.38 0.47 0.08 0.11 0.07 0.03 0.07 0.08 0.07 0.11 0.01 0.02 0.01 0.10 0.08 0.11 0.03 0.03 0.04 0.08
d(A) 9.77 8.84 5.68 5.32 4.87 4.65 4.36 3.86 3.66 3.48 3.37 3.25 3.16 3.03 2.95 2.84 2.66 2.59 2.53 2.44 2.26 2.22 2.09 2.03 1.97 1.89 1.83 1.76 1.73 1.68 1.62 1.57
0.17 0.27 0.73 0.01 0.08 0.15 0.05 0.01 0.13 1.00 0.11 0.08 0.20 0.20 0.08 0.02 0.02 0.11 0.05 0.08 0.08 0.01 0.05 0.03 0.01 0.02 0.08 0.04 0.04 0.05 0.02 0.05
194

VESICAL CALCULI
Table I I
SUBSTANCES F O U N D I N
Pure Calcium Oxalate
Calcium Oxalate Monohydrate (CaC204'H20)
Calcium Oxalate Dihydrate (,CaCj04'2HjO)
Calcium Oxalate (mixed)
Calcium Oxalate plus Apatite
Calcium Oxalate Monohydrate -(- Apatite
Calcium Oxalate Dihydrate -(- Apatite
Calcium Oxalate (mixed) - f Apatite
Apatite (pure)
Ca,5(PO4CO30H)j(OH)j0r Ca,o(P04)4(OH)j
Magnesium Ammonium Phosphate Hexahydrate (pure)
MgNH4P04-6H20
MgNH4P04'6H20 + Apatite
MgNH4P04-6H20 -)- Apatite + Calcium Oxalate (mixed)
Uric Acid
C5N4H4O3
Pure
Mixed with others
Mixed with Uric Acid Monohydrate
Uric Acid Monohydrate (pure)
C5N4H403-Hj0
Calcium Hydrogen Phosphate Dihydrate
CaHP04-2H20
Pure
Mixed
Tricalcium Phosphate (mi::ed)
Ca3(P04)2
Cystine (pure)
SCH2CH(NH2)-COOH
Sodium Acid Urate
NaH.C5N4H203'H20
Pure
Mixed Zinc Phosphate (mixed); (Parsons, 1953) Zn(P04)2-4H20
U R I N A R Y C A L C U L I
Male Female Total 172 45 217 113 15 128 120 20 140 485=55.2%
24 13 37 16 3 19 12 8 20 76= 8.6%
53 31 84 84= 9.6%.
36 37 73 73= 8.3%
1! 3 14 14= 1.6%
11 4 !5 15= 1.7%
58 3 61 14 3 17 11 2 13 91=10.3%
11 3 14 14= 1.6%
3 1 4
6 0 6 10= 1.1%
6 2 8 8= 0.9%
3 2 5 5= 0.6%
I 0 1 1 1 2 3= 0.3% 0 2 2 2= 0.2%
628=771/2'% 198=221/2 %> 880=100%
195

PARSONS
Figure I Six representative bladder calculi from Nepal, Asia, (fractured)
Figure 2 (Case 1) A. Light Surface Crust — Magnesium Ammonium Phosphate Hexahydrate. B. Dark Surface Area — Ammonium Acid Urate and Calcium Oxalate Monohydrate. C. Intermediate Core — Calcium Oxalate Monohydrate. D. Nucleus — Calcium Oxalate Monohydrate and Uric acid. E. Outside Core — Uric Acid and Calcium Oxalate Monohydrate.
196

VESICAL CALCULI
Figure 3 (Case 2) A. Dark Surface Bump — Calcium Oxalate Monohydrate. B. Light Crust — Magnesium Ammonium Phosphate Hexahydrate. C. Nucleus — Calcium Oxalate Monohydrate and Uric Acid. D. Intermediate — Uric Acid and Calcium Oxalate Monohydrate.
Figure 4 (Case 3) A. Crust Scrapings — Uric Acid and Calcium Oxalate Monohydrate. B. Hallow Cavern. C. Nucleus — Ammonium Acid Urate D. Dark Region Outside Nucleus — Ammonium Acid Urate and Calcium Oxalate Monohydrate. E. Outer Dark Ring — Calcium Oxalate Monohydrate.
197

PARSONS
2
A. B. C.
T:*^JM , . . . 1 . . . . I . . . . *' • •• • • *•*••••-• - . .
:3:WTTITTITT]^^ '[''•: Figure 5 (Case 4)
Nucleus — Calcium Oxalate Monohydrate. White Surface Material — Magnesium Ammonium Phosphate Hexahydrate. Body Regions Outside Nucleus — Uric Acid and Calcium Oxalate Monohydrate.
Figure 6 (Case 5) A. Crust Scrapings — Ammonium Acid Urate. B. Dark Ring Outside Nucleus — Calcium Oxalate Monohydrate and Uric C. Nucleus — Uric Acid. D. Main Body — Uric Acid.
198
Acid.

VESICAL CALCULI
% • «• ; ' 1 ' •
J «1« * * 1
f'raBHIl
METRIC 1 i» • ' » . > . , 1 . * .
• -•ff I* , ! « 4 i t I f i S l t
Figure 7 (Case 6)
Entire Calculus — Calcium Oxalate Monohydrate.
Figure 8
X-ray Diffraction Powder Patterns tor calculi examined in this study. 1. Calcium Oxalate Monohydrate 2. Uric Acid. 3. Mixture of Uric Acid and Calcium Oxalate Monohydrate. 4. Magnesium Ammonium Phosphate Hexahydrate. 5. Ammonium Acid Urate. 6. Mixture of Ammonium Acid Urate and Calcium Oxalate Monohydrate.
199

PARSONS
Figure 8 200