
Women’s Empowerment and Health Care Seeking Behavior in...
12
1 Women’s Empowerment and Health Care Seeking Behavior in Bangladesh: Measurement and Model Fitting of Empowerment Abstract The aim of the present study is to estimate the women empowerment index value in Bangladesh. Since women's empowerment is a matter of basic human rights which has during the last decade become a panacea for Third World development. For this purpose BDHS 2007 data have been used which reveals that empowerment level of women increases up to age group 30-34. Moreover, a mathematical model has been fitted to the mean score of women empowerment index which shows that women empowerment index follows a quadratic polynomial model. However, the role of women’s decision-making in reproductive health cannot be overemphasized. In this study, different dimensions of women’s decision-making autonomy and their relationship to maternal and child health- care are examined. The study shows that most autonomy indicators are important predictors of maternal and child health-care utilization although the strength and statistical significance vary by health-care utilization outcome and in some cases significance is lost when socio-economic indicators are held constant. Introduction Since women constitute nearly half of the population of a developing country Bangladesh, they can become a great resource in the development process if they are properly mobilized and organized. Like many other developing countries it needs poverty alleviation and empowering women as well. Since, the empowerment of women is an essential precondition for the elimination of world poverty and the upholding of human rights, empowerment and autonomy are essential for the achievement of sustainable development. The full participation and partnership of both women and men are required in productive and reproductive life, including shared responsibilities for the care and nurturing of children and maintaining the household. Hashemi and Schuler (1993) hypothesized that “the process of empowerment should weaken the systematic basis of women’s subordination”. They identify six hierarchy of domains in which women have traditionally been subordinated such as sense of self and vision of a future, mobility and visibility, economic security, status of decision-making power within the household, ability to interact effectively in the public sphere, and participating in non-family groups. In the same year, Young (1993) stated that, empowerment enables women “to take control of their own lives, set their own agenda, organize to help each other and make demands on the state for support and on the society itself for change”. Empowerment is a complete change of the processes and structures responsible for women’s inferior status in the society. Malhotra et al. (2003) tried to provide a methodology to measure women empowerment. He explained many ways in which empowerment can be measured with six dimensions: economic, socio-cultural, familial-interpersonal, legal, political and psychological. A number of studies have shown that women may be empowered in one area of life while not in others (Malhotra et al., 2003; Kishore and Gupta, 2004; Hashemi et al. 1996), while Williamson (1983) and Jejeebhoy and Sathar (2001) have studied women empowerment in different countries with special emphasis on demographic determinants. Mahendra (2004) have studied the impact of economic participation and health and education on empowerment. Some researchers have attempted to measure the women empowerment with a variety of determinants and dimensions by different methods and techniques (Amin et al., 1998; Pradhan, 2003; Kishore and Gupta, 2004; Kabeer, 2005; Schüler, 2006; Klasen, 2006). They have also developed separate indices with different variables in their studies. Moreover the World Economic Forum’s Gender Gap Index (GGI) also uses a broad range of dimensions and indicators (Lopez- Claros and Zahidi, 2005 and Klasen, 2006). Roy TK, Niranjan S (2004) in their study “Indicator’s of women’s empowerment” found that there exists a regional divide in the level of women’s empowerment. Recently, women’s autonomy and its association with reproductive health and behavior have emerged as a focal point of investigations and interventions around the world. Particularly, since the Cairo International Conference on Population and Development in 1994, ICPD (United Nation, 1994),
Transcript of Women’s Empowerment and Health Care Seeking Behavior in...

1
Women’s Empowerment and Health Care Seeking Behavior in Bangladesh:
Measurement and Model Fitting of Empowerment
Abstract
The aim of the present study is to estimate the women empowerment index value in Bangladesh. Since women's
empowerment is a matter of basic human rights which has during the last decade become a panacea for Third
World development. For this purpose BDHS 2007 data have been used which reveals that empowerment level of
women increases up to age group 30-34. Moreover, a mathematical model has been fitted to the mean score of
women empowerment index which shows that women empowerment index follows a quadratic polynomial model.
However, the role of women’s decision-making in reproductive health cannot be overemphasized. In this study,
different dimensions of women’s decision-making autonomy and their relationship to maternal and child health-
care are examined. The study shows that most autonomy indicators are important predictors of maternal and child
health-care utilization although the strength and statistical significance vary by health-care utilization outcome and
in some cases significance is lost when socio-economic indicators are held constant.
Introduction
Since women constitute nearly half of the population of a developing country Bangladesh, they can become a great resource in the development process if they are properly mobilized and organized. Like many other developing countries it needs poverty alleviation and empowering women as well. Since, the empowerment of women is an essential precondition for the elimination of world poverty and the upholding of human rights, empowerment and autonomy are essential for the achievement of sustainable development. The full participation and partnership of both women and men are required in productive and reproductive life, including shared responsibilities for the care and nurturing of children and maintaining the household. Hashemi and Schuler (1993) hypothesized that “the process of empowerment should weaken the systematic basis of women’s subordination”. They identify six hierarchy of domains in which women have traditionally been subordinated such as sense of self and vision of a future, mobility and visibility, economic security, status of decision-making power within the household, ability to interact effectively in the public sphere, and participating in non-family groups. In the same year, Young (1993) stated that, empowerment enables women “to take control of their own lives, set their own agenda, organize to help each other and make demands on the state for support and on the society itself for change”. Empowerment is a complete change of the processes and structures responsible for women’s inferior status in the society. Malhotra et al. (2003) tried to provide a methodology to measure women empowerment. He explained many ways in which empowerment can be measured with six dimensions: economic, socio-cultural, familial-interpersonal, legal, political and psychological. A number of studies have shown that women may be empowered in one area of life while not in others (Malhotra et al., 2003; Kishore and Gupta, 2004; Hashemi et al. 1996), while Williamson (1983) and Jejeebhoy and Sathar (2001) have studied women empowerment in different countries with special emphasis on demographic determinants. Mahendra (2004) have studied the impact of economic participation and health and education on empowerment. Some researchers have attempted to measure the women empowerment with a variety of determinants and dimensions by different methods and techniques (Amin et al., 1998; Pradhan, 2003; Kishore and Gupta, 2004; Kabeer, 2005; Schüler, 2006; Klasen, 2006). They have also developed separate indices with different variables in their studies. Moreover the World Economic Forum’s Gender Gap Index (GGI) also uses a broad range of dimensions and indicators (Lopez-Claros and Zahidi, 2005 and Klasen, 2006). Roy TK, Niranjan S (2004) in their study “Indicator’s of women’s empowerment” found that there exists a regional divide in the level of women’s empowerment. Recently, women’s autonomy and its association with reproductive health and behavior have emerged as a focal point of investigations and interventions around the world. Particularly, since the Cairo International Conference on Population and Development in 1994, ICPD (United Nation, 1994),
2
women’s role has been a priority area not only for sustainable development, but also in reproductive health. At the ICPD, a general consensus was reached to ameliorate women’s status, along with the related goals of improving women’s reproductive health and securing their reproductive rights, which represents a paradigm shift that emphasizes the reproductive autonomy of individuals. Following the ICPD, there has been a number of recent studies that examine women’s autonomy and relationship with reproductive health and health outcomes (e.g. Kishor 2000, 2005; Bloom et al., 2001; IUSSP, 1997). Most of these studies found relationship between various aspects of autonomy and reproductive health and behavior, but there are many complexities and contradictory findings among them, with different aspects of autonomy showing unexpected relationships with reproductive health and preferences in difference settings and under different research designs. For example, lower fertility desire was observed among women with higher level of autonomy in Bangladesh (Balk 1994) and in many regions of India (Jejeebhoy 1991), and lower fertility was found to be associated with women’s greater autonomy in Malaysia, the Philippines and Thailand (Tfaily 2004). Women’s reproductive health care seeking behavior was found to be associated positively with freedom of movement and decision-making power in South India, but these effects were reduced when confounding factors were taken into account (Bhatia and Cleland, 1995). A study by Kishor (2000) found women’s autonomy to be an important explanatory factor in child survival and child health in Egypt along with other bio-demographic and socio-economic factors. Using DHS data from Zimbabwe, Becker (1997) examined the relationship between women’s role in household decision-making and the extend of prenatal care and contraceptive use and found a strong association with prenatal care, but not with contraceptive use. The scenario of women empowerment and women’s maternal and child health care seeking behavior is not good in Bangladesh. Again, form the above discussion, we found that, increased empowerment of women is likely to increase their ability to seek out and use health services to better meet their own reproductive health goals, including the goal of safe motherhood and also in child health care seeking behavior. So, it could be an nice research issue to determine the overall empowerment scenario of Bangladesh by estimating women empowerment index value, investigating the various factors that effect women’s empowerment in Bangladesh and how women’s decision making autonomy effect their maternal and child health care seeking behavior. So the specific objectives of the study are as follows:
1. To measure the WEI score by some selected background characteristics. 2. To build up a mathematical model to WEI score. 3. To examine determinants of different dimensions of women’s decision-making autonomy
and their relationship to maternal and child health-care seeking behavior. Data In this study we use BDHS, 2007 data and all ever-married women age 10-49 in the selected households were eligible respondents. A total of 11,178 eligible women age 15-49 were identified and 10,996 were interviewed (the number of ever-married women age 10-14 was very low, and thus this group had to be excluded from the analysis). Variables of the study In this study we have tried to determine the determinant of women empowerment in the domestic sphere using the dimensions in accordance with Mason and Smith (2003). The particular aspects or dimensions of domestic empowerment we take are: 1. Women's economic decision making autonomy. 2. Their household decision making autonomy. 3. Their physical freedom of movement. These are considered as dependent variables. Detail description of each dimension are given in table one. To analyze women’s maternal and child health-care seeking behavior the dependent variables are- 1) Antenatal care during pregnancy as measured by the frequency of visits, 2) Delivery care 3) Postnatal Care and 4) Child immunization status

3
The median number of ANC visits, in Bangladesh, among women who received antenatal care is 3.1. So, here antenatal care is measured by whether the mother visited medical facility at least three times(as the median number of ANC visits, in Bangladesh is 3.1) during pregnancy of her last child. According to World Health Organization (WHO) delivery should be done by proper medical attention and in a hygienic environment. We used a binary variable to model delivery care, reflecting whether the last birth was born at a medical facility (hospital or clinic) versus at home, regardless of attended (trained or any other person). The postnatal care is assessed by women who had delivered a child had received a health check after the delivery by trained person versus any other persons, regardless the time after delivery health provider was used. To model immunization status of the last child, we used a binary variable reflecting whether the child has received all the necessary vaccinations (full immunization) or not. According to World Health Organization (WHO) a child is considered to be fully vaccinated if it has received a dose of BCG vaccine (against tuberculosis), three doses of DPT (a vaccine to immunize against diphtheria, pertussis and tetanus) three doses of polio immunization, and a measles vaccination by 12 months of age. Demographic Variables Age of respondent, age at last birth, age at first marriage, age differences between spouses, birth order, number of family members, number of living children. Socio-economic Characteristics Division, place of residence, respondent’s educational level, respondent’s working status, partner’s educational level, partner’s working status, wealth index, religion, watching television. Methodology Linear Logistic Regression Analysis Logistic regression models were first fitted to investigate factors predicting the likelihood of involvement of women in decision making autonomies. Subsequently, we fitted two separate logistic regression models for each of the outcome variables of our study to investigate the effect of women’s autonomy on maternal and child health care seeking behavior. The first of these latter models includes women’s autonomy indicators only, while the second model adds all the background characteristics. Then on the basis of odds ratio and their p-value decided which variables are significant.
Measuring Women Empowerment In previous section we mentioned that in this study we have tried to measure women empowerment index value using the dimensions in accordance with Mason and Smith (2003). The particular aspects or dimensions of domestic empowerment we take are:
1. Women's economic decision making autonomy. 2. Their household decision making autonomy. 3. Their physical freedom of movement.
The detailed description of these three dimensions with their relevant indicators is given in table 1. Then the index of each dimension was constructed where minimum and maximum values were chosen for each underlying indicator. Performance in each indicator is expressed as the minimum and maximum value between 0 and 1 in accordance with the construction method of the Human Development Index (UNDP, 2005) as follows:
Where, , Min , Max and are respectively the actual, minimum, maximum and
dimension index.
The Women Empowerment Index (WEI) is then computed by averaging these three indices.
4
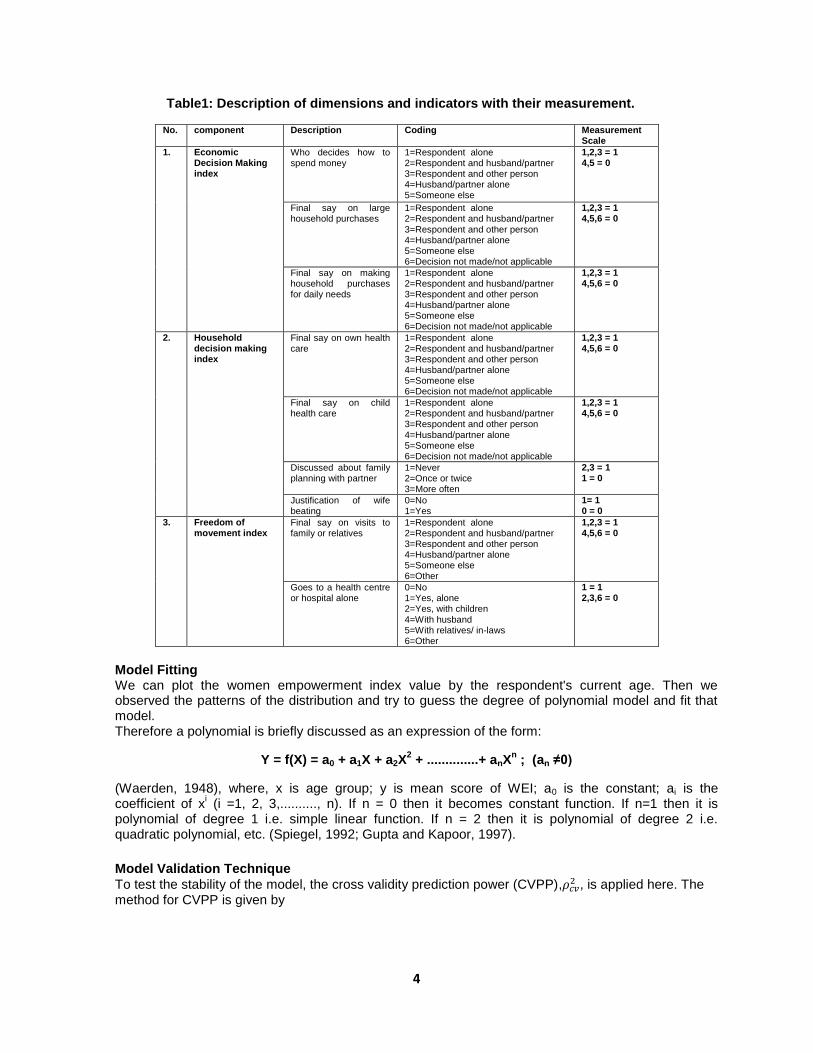
Table1: Description of dimensions and indicators with their measurement.
No. component Description Coding Measurement Scale
1. Economic Decision Making index
Who decides how to spend money
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else
1,2,3 = 1 4,5 = 0
Final say on large household purchases
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else 6=Decision not made/not applicable
1,2,3 = 1 4,5,6 = 0
Final say on making household purchases for daily needs
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else 6=Decision not made/not applicable
1,2,3 = 1 4,5,6 = 0
2. Household decision making index
Final say on own health care
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else 6=Decision not made/not applicable
1,2,3 = 1 4,5,6 = 0
Final say on child health care
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else 6=Decision not made/not applicable
1,2,3 = 1 4,5,6 = 0
Discussed about family planning with partner
1=Never 2=Once or twice 3=More often
2,3 = 1 1 = 0
Justification of wife beating
0=No 1=Yes
1= 1 0 = 0
3. Freedom of movement index
Final say on visits to family or relatives
1=Respondent alone 2=Respondent and husband/partner 3=Respondent and other person 4=Husband/partner alone 5=Someone else 6=Other
1,2,3 = 1 4,5,6 = 0
Goes to a health centre or hospital alone
0=No 1=Yes, alone 2=Yes, with children 4=With husband 5=With relatives/ in-laws 6=Other
1 = 1 2,3,6 = 0
Model Fitting We can plot the women empowerment index value by the respondent's current age. Then we observed the patterns of the distribution and try to guess the degree of polynomial model and fit that model. Therefore a polynomial is briefly discussed as an expression of the form:
Y = f(X) = a0 + a1X + a2X2 + ..............+ anX
n ; (an ≠0)
(Waerden, 1948), where, x is age group; y is mean score of WEI; a0 is the constant; ai is the coefficient of x
i (i =1, 2, 3,.........., n). If n = 0 then it becomes constant function. If n=1 then it is
polynomial of degree 1 i.e. simple linear function. If n = 2 then it is polynomial of degree 2 i.e. quadratic polynomial, etc. (Spiegel, 1992; Gupta and Kapoor, 1997).
Model Validation Technique
To test the stability of the model, the cross validity prediction power (CVPP), , is applied here. The
method for CVPP is given by

5
Where n is the number of cases, k is the number of predictors in the model and the cross-validated, R2
is the correlation between observed and predicted values of the dependent variable. The shrinkage of the model is the absolute value of the difference between ρ
2cv and R
2. Moreover, the stability of R
2 of
the model is equal to (1- shrinkage) (Stevens, 1996).
Analysis and results: Determinants of women’s autonomy Before we examine the link between autonomy and utilization of maternal health care, it is instructive to look first at the relationship between socio-economic characteristics and women’s autonomy. From the logistic regression analysis we can say that Respondent’s age showed significant effect for all of the indicators of economic decision making autonomy. Age of respondent also showed significant effect on household decision making autonomy and freedom of movement autonomy. Economic, household and freedom of movement autonomy increases with increases of respondent’s age and then decline after a certain age.
Regional impact is also present for decision making autonomy of women. For making large and daily household purchase women of Khulna and Dhaka have higher autonomy respectively than other divisions. The highest freedom of movement is found in women of RajshahiPlace of residence also has vital impact on women’s decision making autonomy. Rural women are less likely to have decision making autonomy than urban women.
Number of living children also showed significant impact on women’s economic decision making autonomy. For large household purchase and about spending money, decision making autonomy decreases with increase of number of living children. For household decision making autonomy number of living children showed significant impact on child health care and discussing about family planning and for freedom of movement autonomy number of living children showed significant impact on visiting health care centre/hospital alone.
Wealth index also plays important role on final say on making household purchases for daily needs. Richest women discussed about family planning 70 percent more than that of poorest women. Wealth index is found to be significant for visiting family members/relatives.
From our findings, we can summarize that, women with the higher the education level have more decision making autonomy than women with less or no education women. Watching television plays significant role on decision making autonomy; watchers have more decision making autonomy than non-watchers. Measurement and model fitting of empowerment Here, we compute empowerment index value for 7 separate background characteristics, respondent’s current age, age at first marriage, age differences between spouses, place of residence, wealth index, education level and partner’s education level. Table 1 present the empowerment index for each of the indicator. Empowerment index values by respondent’s age are summarized in table 2. From the values we found that, women’s empowerment increases up to a certain age of women, and then it starts to fall. Empowerment is found to be the lowest at age group 15 to 19, increase up to age group 30 to 34, where it picks the highest value, then decreases again in the next age groups. The mean score of WEI is highest for very rich group and the score is 0.7147614 for them. It also shows the higher empowerment of middle women than rich class women.

6
Early marriage usually leads to early motherhood and young women are often threatened by death due to pregnancy-related causes. From table we observed that the women who marry earlier (<15 years) are less empowered than those who marry at older ages (after 20 years). Conclusions can be drawn from these findings that, early marriages for women result in dropping out of school and losing opportunities for economic activities and thereafter less empowerment. The result expresses that the women having little age gap with the husband are more empowered than other women.
From Table we observe that the educational qualification, both for husband and wife affects women empowerment significantly. We can say that, the women who are in higher education are more empowered than other education groups and also this is same for the women whose husbands have higher education (0.72823). Conclusions can be drawn here that more education contributes to the fundamental process of women's empowerment.
We observed that urban women are more empowered than rural women. This pattern is caused for lack of education, working opportunity in rural areas compare to urban area.
Table 2: Mean score of WEI by age Variable age
Mean score of WEI
Variable(Wealth Index)
Mean score of WEI
15-19 20-24 25-29 30-34 35-39 40-44 45-49
0.6010281 0.6448049 0.6724105 0.6974624 0.6892113 0.6652153 0.6242266
Very poor Poor middle Rich Very Rich
0.6577539 0.6572734 0.6624416 0.6590373 0.7147614
Age at first marriage Age differences between spouses
<15 15-16 17-19 20+
0.66167 0.66457 0.67063 0.73090
Little (Up to 5 years) Moderate(6-10 years) Big (>10 years)
0.67826 0.66704 0.65909
Education Partner’s education
No education Primary education
Secondary education Higher education
0.6511814 0.6563191 0.6881850 0.7504623
No education Primary education Secondary education Higher education
0.66131 0.65924 0.66040 0.72823
place of residence
Urban Rural
0.7167680 0.6532087
To fit a specific mathematical model to WEI score, we plotted the mean score of WEI by age groups which showed that (figure 4.3) mean score of WEI can be distributed by polynomial model for different ages. From the figure we can say that the distribution of mean score of WEI for different age group is more than one degree polynomial. So we first fit a two degree polynomial model to WEI score and the results of the fitted model are discussed in the table 3.
Table3: Information of model fitting Model Age
groups (n)
k R2 ρ
2cv Shrinkage Parameter Significant
probability (p)
(A) 7 3 0.988 0.931 0.057 a0 0.000
a1 0.000
a2 0.000
7
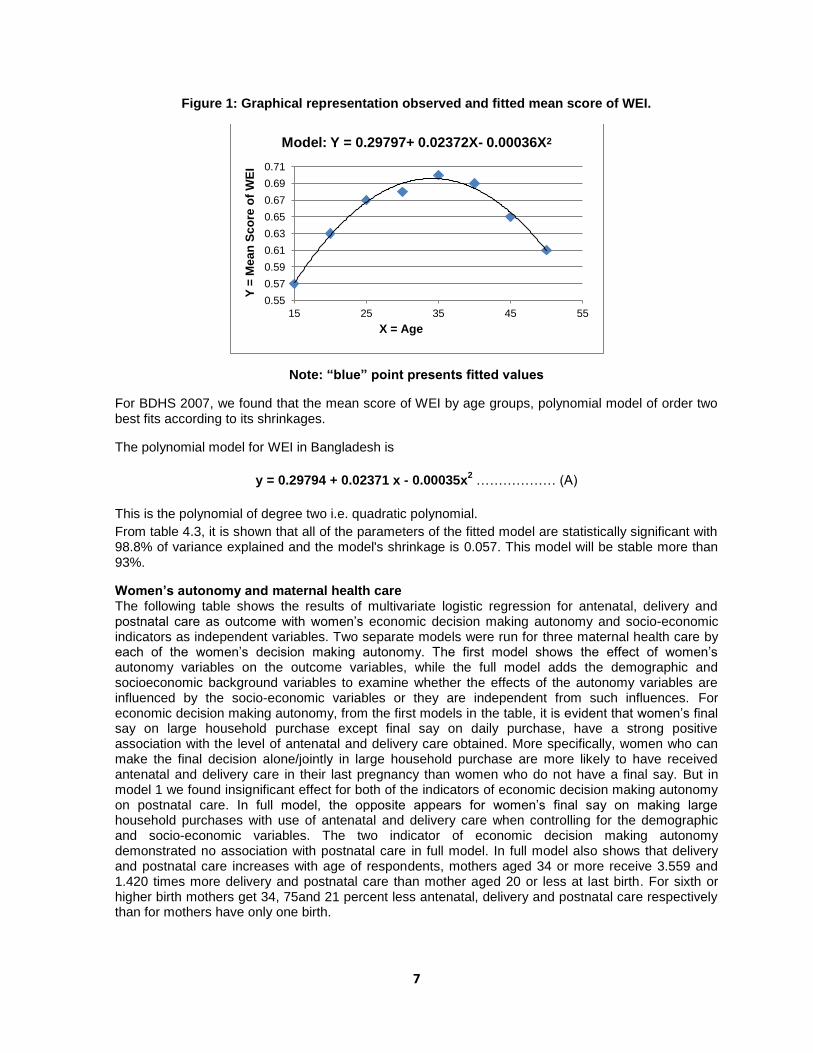
Figure 1: Graphical representation observed and fitted mean score of WEI.
Note: “blue” point presents fitted values
For BDHS 2007, we found that the mean score of WEI by age groups, polynomial model of order two best fits according to its shrinkages.
The polynomial model for WEI in Bangladesh is
y = 0.29794 + 0.02371 x - 0.00035x
2 ……………… (A)
This is the polynomial of degree two i.e. quadratic polynomial.
From table 4.3, it is shown that all of the parameters of the fitted model are statistically significant with 98.8% of variance explained and the model's shrinkage is 0.057. This model will be stable more than 93%.
Women’s autonomy and maternal health care The following table shows the results of multivariate logistic regression for antenatal, delivery and postnatal care as outcome with women’s economic decision making autonomy and socio-economic indicators as independent variables. Two separate models were run for three maternal health care by each of the women’s decision making autonomy. The first model shows the effect of women’s autonomy variables on the outcome variables, while the full model adds the demographic and socioeconomic background variables to examine whether the effects of the autonomy variables are influenced by the socio-economic variables or they are independent from such influences. For economic decision making autonomy, from the first models in the table, it is evident that women’s final say on large household purchase except final say on daily purchase, have a strong positive association with the level of antenatal and delivery care obtained. More specifically, women who can make the final decision alone/jointly in large household purchase are more likely to have received antenatal and delivery care in their last pregnancy than women who do not have a final say. But in model 1 we found insignificant effect for both of the indicators of economic decision making autonomy on postnatal care. In full model, the opposite appears for women’s final say on making large household purchases with use of antenatal and delivery care when controlling for the demographic and socio-economic variables. The two indicator of economic decision making autonomy demonstrated no association with postnatal care in full model. In full model also shows that delivery and postnatal care increases with age of respondents, mothers aged 34 or more receive 3.559 and 1.420 times more delivery and postnatal care than mother aged 20 or less at last birth. For sixth or higher birth mothers get 34, 75and 21 percent less antenatal, delivery and postnatal care respectively than for mothers have only one birth.
0.55
0.57
0.59
0.61
0.63
0.65
0.67
0.69
0.71
15 25 35 45 55
Y =
Me
an
Sc
ore
of
WE
I
X = Age
Model: Y = 0.29797+ 0.02372X- 0.00036X2

8
Table 4: Determinants of maternal health care utilization
Variable name
Antenatal care Delivery care Postnatal care
Model with
autonomy only
(Model 1)
Full model
(Model2)
Model with
autonomy only
(Model 1)
Full model
(Model2)
Model with
autonomy only
(Model 1)
Full model
(Model2)
Final say on large household purchase
Husband/others(ref) Respondent alone/jointly
1.207**
1.072
1.272**
1.097
1.088
0.890
Final say on making household purchase for daily needs
Husband/others(ref) Respondent alone/jointly
1.069
1.139
0.849*
0.770**
0.928
1.041
Mother’s age at birth <20(ref) 20-33 34-
1.115 1.015
1.664*** 3.559***
1.410*** 1.420
Birth order 1(ref) 2-3 4-5 6-
0.775*** 0.660*** 0.660*
0.461*** 0.368*** 0.249***
0.731*** 0.651*** 0.794
No. of family members 1-4(ref)
5-7 8-
0.911 0.981
0.700*** 0.826
1.008 0.938
Division Barisal(ref) Chittagong
Dhaka Khulna
Rajshahi Sylhet
0.844 0 .688** 1.132 1.657*** 0.785
1.154 1.681** 1.932**
1.023 1.157
1.175 0.778
1.326 0.720*
1.038
Residence Urban(ref)
Rural
0.531***
0.702***
1.069
Religion Muslim(ref) Non-muslim
1.28**
1.791***
1.097
Wealth index Very poor(ref)
Poor middle Rich
Very Rich
0.947 1.176 1.412** 2.544**
0.738 0.840 1.186 2.029***
1.293* 1.194
1.428** 1.389*
Mother’s education No education(ref)
Primary Secondary
Higher
1.367*** 2.408*** 4.310***
1.572** 3.062*** 4.642***
1.310** 1.664*** 2.386***
Mother’s working status Not working(ref)
Working
0.983
0.850
1.036
Partner’s education No education(ref)
Primary Secondary
Higher
1.160 1.430*** 1.986***
1.006 1.338* 2.185***
0.856 0.850 1.078
Partner’s working status Not working(ref)
Working
0.527***
1.255
0.910
Watch TV No(ref)
Yes
1.409***
1.224
1.069

9
Antenatal care No (ref)
Inadequate Adequate
1.801*** 6.131***
1.850*** 2.696***
Delivery care No(ref)
Yes
-
-
45.670***
Note: Reference level denoted by (ref); ***p<0.01, **p<0.05, *p<0.1
Regional impact is highest for Rajshahi division for antenatal care. Regional impact is also found to be significant for receiving delivery and postnatal care. Again, rural women receive antenatal and delivery care 0.531 and 0.702 times less likely than that of urban women. Wealth index is important too; the richest women get 2.544 and 2.029 times more antenatal and delivery care than the poorest women. Mother’s education plays vital role on antenatal and delivery care, higher educated women receives almost 4 times more antenatal and delivery care and 2.386 times more postnatal care than that of non-educated mothers. Mother exposed to television watching receive 40 and 22.4 percent more antenatal and delivery care than that of non-exposed mothers. Mother who receives adequate antenatal care gets 2.696 times more postnatal care than receiving no antenatal care. Receiving delivery care also has significant effect on postnatal care. For household decision making autonomy, in model 1, we found strong association with the level of three maternal health care obtained for all of the indicators of household decision making autonomy(except final say on child health care on postnatal care.). More specifically, women who can make the final decision alone/jointly in final say on own health care, final say on child health care and discussed about family planning with partner (last 3 months) are more likely to receive three maternal health care in their last pregnancy than women who do not have a final say. Women who think that wife beating is justified are less likely to have received antenatal, delivery and postnatal care than the women who think wife beating is not justified. In full model final say on child health care still demonstrates a strong and positive association with use of antenatal care when controlling for the socio-economic variables, the opposite appears for other three indicators of household decision making autonomy. Respondent alone/jointly decision maker on child health care receive 24 percent more antenatal care than husband/others take final decision on child health care. For delivery care (in full model), we found insignificant effect for all of the indicators of household decision making autonomy and for postnatal care discussed about family planning with partner has significant effect. In full model also shows that delivery and postnatal care increases with age of respondents, mothers aged 34 or more receive 3.559 times more delivery care than mother aged 20 or less at last birth and mothers aged 20-33 years receive 1.350 times more postnatal care than mother aged 20 or less . Antenatal, delivery and postnatal care receiving decreases with higher birth order for mothers. For sixth or higher birth mothers get 38 and 73 percent less antenatal and delivery care respectively than for mothers have only one birth. For postnatal care mother with 4-5 birth receive 34 percent less postnatal care than the mothers have only one birth. Regional impact is also found to be significant for receiving antenatal and delivery care; it is highest for Rajshahi and Khulna division respectively. Again, rural women receive antenatal and delivery care 0.536 and 0.721 times less likely respectively than that of urban women. Wealth index is important too; the richest women get 2.601 and 2.203 times more antenatal and delivery care respectively than the poorest women. Mother’s education plays vital role on antenatal care, higher educated women receives almost 4 times more antenatal and delivery care than that of non-educated mothers. For postnatal care, higher educated women receive 2.360 times more postnatal care than that of non-educated mothers. Mother exposed to television watching receive approximately 42 percent more antenatal care than that of non-exposed mothers. Mothers receiving antenatal care adequately receive 6.508 and 2.723 times more delivery and postnatal care than mothers don’t receiving antenatal care. Receiving delivery care also has significant effect on postnatal care. Women who receive delivery care are more likely to receive postnatal care. For freedom of movement autonomy, in model 1, we found significant effect for both of the indicators on antenatal care but we found significant effect for final say on visit to family/relatives on delivery and postnatal care. In full model, both of the indicators of freedom of movement autonomy still demonstrate a strong and positive association with use of antenatal care and goes to a health

10
canter/hospital alone has significant effect on delivery care when controlling for the demographic and socio-economic variables. But both the indicators show insignificant association with receiving postnatal care in full model. Women who can make the final decision alone/jointly in freedom of movement autonomy are more likely to have received antenatal, delivery and postnatal care in their last pregnancy than women who do not have a final say. Delivery care increases with age of respondents, mothers aged 34 or more receive 3.514 times more delivery care than mother aged 20 or less at last birth. Antenatal, delivery and postnatal care receiving decreases with higher birth order for mothers. For sixth or higher birth mothers get 35, 75 and 22 percent less antenatal, delivery and postnatal care respectively than for mothers have only one birth. Regional impact is also found to be significant for receiving antenatal and postnatal care; it is highest in Rajshahi division for both antenatal and postnatal care. Again, rural women receive antenatal and delivery care 0.541 and 0.697 times less likely than that of urban women. Wealth index is important too; the richest women get 2.572 and 2.002 times more antenatal and delivery care than the poorest women. Mother’s education plays vital role on antenatal care, higher educated women receives 4.208, 4.737 and 2.343 times more antenatal, delivery and postnatal care than that of non-educated mothers. Mother exposed to television watching receive 37.1 and 24.5 percent more antenatal and delivery care than that of non-exposed mothers. Mothers receiving antenatal care adequately receive 2.667 and 6.161 times more delivery and postnatal care than mothers don’t receiving antenatal care. Receiving delivery care also has significant effect on postnatal care. Women’s autonomy and immunization status of last child For child health care we also apply two separate logistic regression model as previous analysis, in which the dichotomy of whether the child has received all the necessary immunizations versus not received all immunizations is the dependent variable. For economic decision making autonomy in the first model, we found insignificant association of women’s final say in both of the autonomy indicators with seeking child immunization. In full model both indicators shows insignificant association with seeking child immunization when controlling for the demographic and socio-economic variables. Division, place of residence, mother’s education level has significant effect on child immunization. Among all divisions, the children of Rajshahi are found to be most immunized than all other divisions. Rural children are found to be 36% less immunized than that of urban children. Again, the children of higher educated mother are found to be 3.591 times more immunized than that of children of non-educated mothers.
For household decision making autonomy, children of women who have the final say (either alone or jointly with partner/others) in decision on child health care, discussing about family planning with partners and who disagrees wife beating are more likely to receive all the necessary vaccinations (in model 1). In full model, only decision final say on child health care still retained its significance, the effects of decisions on discussing about family planning with partners and wife beating justification disappear when controlling for the demographic and socio-economic variables. Mothers having final say in child health care are 1.6 times more likely to have immunized children than that of others. Regarding the demographic and socio-economic indicators division and mother’s education are found to be significant differential of child immunization. The children of Khulna are found to be most immunized. Children of higher educated mother are found to be approximately 3 times more likely to be immunized than that of non-educated mothers. For freedom of movement autonomy we found that final say on visit family/relatives has significant effect on child immunization on model 1. In full model we found that final say on visit family/relatives, division, place of residence and mothers education have significant impact on child immunization. For freedom of movement autonomy, children of Chittagong are found to be highest immunized than that of all other divisions. Rural children are found to be 36 percent less immunized than that of urban children. Higher educated mother are found to be more aware about children health condition, these children are found to be 3.53 times more immunized than that of others.

11
Conclusion This study was aimed to measure women empowerment index value in Bangladesh. Women’s autonomies are also examined and whether there is a link between women’s autonomy and utilization of maternal and child health care and how such relationships, if any, depend on demographic and socio-economic factors are also found.
We have explained empowerment from different angles. From this study we can say that economic, household and freedom of movement decision making autonomy increases as they are older, becoming more educated, and involving in different occupation. With increase in women’s decision making autonomies, the women become more empowered. We estimate the women empowerment index value in Bangladesh. On the basis of our analysis (WEI score), we can say that overall empowerment scenario is not satisfactory in Bangladesh. Older women have more independence and empowerment than younger women because they have more experience with life, a better understanding of how to get what they want or need, a closer relationship with the husband. Moreover, a mathematical model has been fitted to the mean score of women empowerment index by age which shows that women empowerment index follows a quadratic polynomial model. The most important result from our analyses on health-seeking behavior during pregnancy is that several demographic and socio-economic characteristics, particularly division, residence, wealth index, mother’s and husband’s education and watching television have association with seeking health care, implying that these variables have direct effects on the use of antenatal health care facilities. For care during delivery several demographic and socio-economic characteristics, such as mother’s age at last birth, birth order, number of family members, division, residence, wealth index, mother’s and husband’s education and watching television have association with seeking health care. For postnatal care mother’s age at last birth, birth order, division, wealth index, mother’s education, antenatal care and care during delivery have association with seeking health care. And for child immunized status divisions, place of residence and mother’s education have association with seeking child immunization behavior. On the other hand, the results suggest that not all dimensions of women’s autonomy are important predictors of these health outcomes. The effects of women’s autonomy varied by the health outcomes and some of them lost their significance after the socioeconomic indicators are controlled. Final say on child health care, visit to family/relatives and goes to health centre/hospital alone increases receiving antenatal care. Final say on making household purchase for daily needs has significant impact on receiving delivery care. Discussed about family planning with partners (in last 3 months) increases receiving postnatal care. The most relevant conclusion from this study is that in country like Bangladesh where women’s autonomy is low, health-care seeking behaviors are more strongly affected by socio-economic factors - like education, residence and employment. But, the effects of some of women’s direct autonomy indices like decisions on final say on making household purchase for daily needs, final say on child health care, visit to family/relatives and goes to health centre/hospital alone and discussed about family planning with partner’s (in last 3 months) which retained their significant effects after controlling for the demographic and socio-economic factors should not be ignored in studies like the one we have carried out. Finally we can say that women having more autonomy seek more health care.
12
References
Amin, R., Becker, S. and Byes, Abdul. (1998). NGO-Promoted Micro credit Programs and Women’s Empowerment in Rural Bangladesh: Quantitative and Qualitative Evidence, The Journal of Developing Areas, winter, 221-236. Balk D. 1994. Individual and community aspects of women’s status and fertility in rural Bangladesh. Population Studies, 48(1): 21-45. Becker S. 1997. Incorporating women’s empowerment in studies of reproductive health: an example from Zimbabwe. Paper presented in the seminar on female empowerment and demographic processes: Moving beyond Cairo. 21-24 April 1997, Lund, Sweden. Bloom S.S., Wypij D. and Das Gupta M. 2001. Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. Demography 28(1): 67-78. Bhatia J. and Cleland J. 1995b. Self-reported symptoms of gynaecological morbidity and their treatment in south India. Studies in Family Planning, 26(4): 203-216. Gupta, S. C. & Kapoor, V. K. "Fundamentals of Mathematical Statistics" RevisedEdition, Sultan Chand & Sons, Educational Publishers, New Delhi, 1997. Hashemi, Syed M. and Sidney Ruth Schuler "Defining and Studying Empowerment of Women: A Research Note from Bangladesh." JSI Working Paper No. 3. Washington DC: John Snow, Inc. 1993. Hashemi, S., Sydney, R., Schuler and Ann, R. (1996). Rural Credit programs and Women’s Empowerment in Bangladesh. World Development, 24 (4), 635-653. Jejeebhoy S.J. 1991. Women’s status and fertility: Successive cross-sectional evidence from Tamil Nadu, India. Studies in Family Planning, 22(4): 217-30. Jejeebhoy, S.and Sathar Z. (2001). Women’s Autonomy in India and Pakistan: The Influence of Religion and Region. Population and Development Review, 27(4), 687-712. Kabeer, Naila (2005). Gender Equality and Women’s Empowerment: A Critical Analysis of the Third Millennium Development Goal. Gender and Development, 13 (1), 13–24. Kishore, S. and Gupta, K. (2004). Women’s Empowerment in India and Its States: Evidence from the NFHS, Economics and Political Weekly. Kishor S. 2000. Empowerment of women in Egypt and links to the survival and health of their infants. In Presser H. and Sen G. (eds.) Women’s Empowerment and Demographic Processes: Moving Beyond Cairo. New York: Oxford University Press. ______ 2005. A Focus on Gender: Collected Papers on Gender using DHS data. Calverton, Maryland, USA: ORC Macro. Klasen, S. (2006). UNDP’s Gender-related Measures: Some Conceptual Problems and Possible Solutions, Journal of Human Development, 7 (2), 243–274. Lopez-Claros, A. and Zahidi, S. (2005). Women’s Empowerment: Measuring the Global Gender Gap, Geneva: World Economic Forum http://www.weforum.org/pdf/Global_Competitiveness_Reports/Reports/gender_gap.pdf Mahendra, S.D. (2004). Female Work Participation Using Occupational Data from NFHs Data Set, Economics and Political Weekly, February 14. Mason, Karen Oppenheim and Smith "Women's Empowerment and Social Context: Result from Five Asian Countries", 2003. Pradhan, B. (2003). Measuring empowerment: a methodological approach. Development, 46 (2), 51–57 Malhotra, A., Schüler, S. and Boender, C. (2003). Measuring women’s empowerment as a variable in international development, paper presented at the International Council for Research on Women (ICRW) Insight and Action Seminar, Washington, DC 12 November 2003. Mitra and Associates. "Bangladesh Demographic and Health Survey (BDHS-2007)" Dhaka, Bangladesh and Calverton, Maryland [USA]: National Institute of Population Research and Training, Mitra and Associates, and ORC Macro, 2007. Schüler, D. (2006). The uses and misuses of the Gender-related Development Index and Gender Empowerment Measure: a review of the literature, Journal of Human Development, 7 (2), 161– 181. Spiegel, M. R. "Theory and Problems of Statistics", Second Edition in SI Units., Schaum's Outline Series, McGraw -Hill Book Company, London, 1992. Stevens, J. "Applied Multivariate Statistics for the Social Sciences." Third Edition, Lawrence Erlbaum Associates, Inc., Publishers, New Jersey, 1996. Tareque M. I., Haque, M.M., Mostofa, M. G. and Islam, T. M, "Age, Age at Marriage, Age Difference between Spouses and Women Empowerment: Bangladesh Context" Middle East Journal of Age and Ageing, 2007; 4 (6): 8 - 14. Tfaily R. 2004. Do women with higher autonomy have lower fertility? Evidence from Malaysia, the Philippines and Thailand. Genus. LXL(2): 7-32. United Nations Development Programme (UNDP) "Human Development Report 2005, United Nations Development Programme, New York, 2005. Waerden, B.L.Van Der. "Modern Algebra", Vol. 1, ICK Ungar Publishing Co. New York, 1948. Williamson, N.E (1983). Parental Sex preference and Sex Selection. In N.G.Benette (ed) Sex Selection of Children. New York: Academic Press. Woldemicael, Gebremariam (2007). ‘Do Women with Higher Autonomy Seek More Maternal and Child Health-Care? Evidence from Ethiopia and Eritrea.’ MPIDR Working Paper, WP 2007-035, November 2007. World Health Organization. The world health report 2005: Make every mother and child count. Geneva: WHO; 2005.


















