
WHO-EDM Report-Eng
24
ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES ESSENTIAL DRUGS AND MEDICINES Annual Report Essential Drugs and Medicines Policy 2003
Transcript of WHO-EDM Report-Eng
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ESES
SEN
TIAL D
RUG
S
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ESES
SEN
TIAL D
RUG
S
AND
MED
ICIN
ES
ESSE
NTIA
L DRU
GS
AND
MED
ICIN
ES
Annual Report
Essential Drugs and Medicines Policy 2003
WHO-EDM Report-Eng 27/10/04 2:58 pm Page c
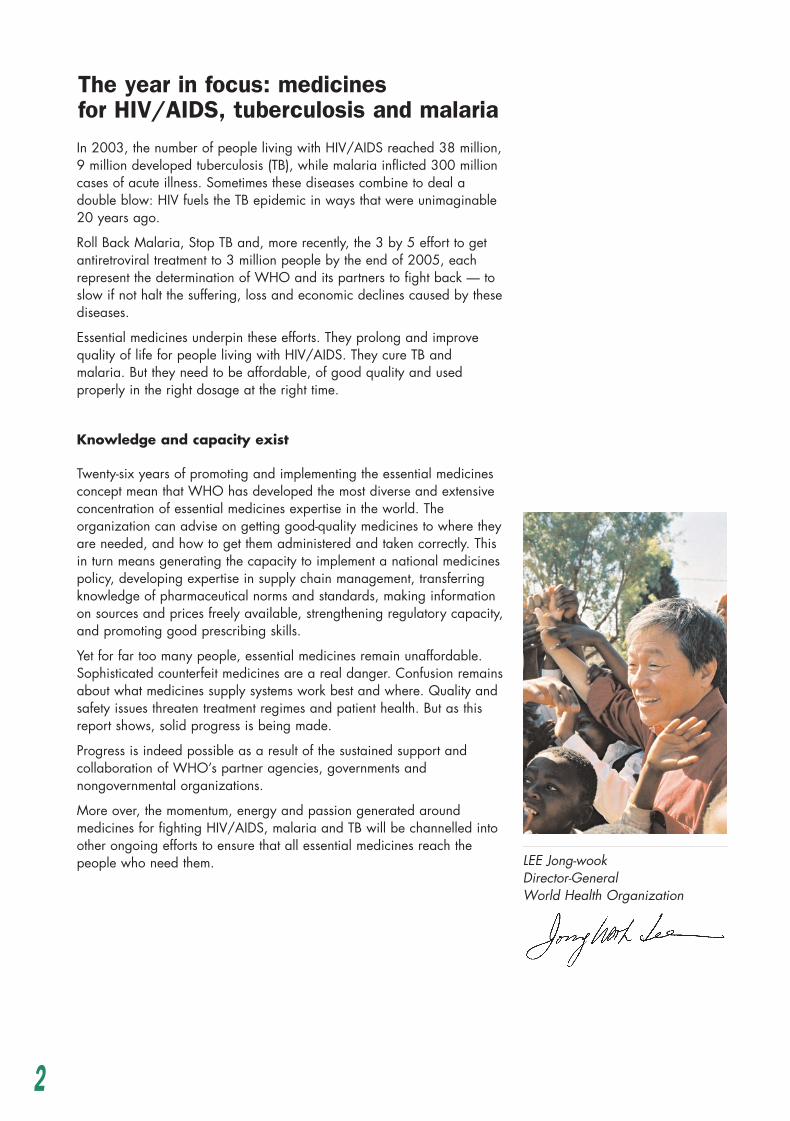
In 2003, the number of people living with HIV/AIDS reached 38 million,9 million developed tuberculosis (TB), while malaria inflicted 300 millioncases of acute illness. Sometimes these diseases combine to deal adouble blow: HIV fuels the TB epidemic in ways that were unimaginable20 years ago.
Roll Back Malaria, Stop TB and, more recently, the 3 by 5 effort to getantiretroviral treatment to 3 million people by the end of 2005, eachrepresent the determination of WHO and its partners to fight back — toslow if not halt the suffering, loss and economic declines caused by thesediseases.
Essential medicines underpin these efforts. They prolong and improvequality of life for people living with HIV/AIDS. They cure TB andmalaria. But they need to be affordable, of good quality and usedproperly in the right dosage at the right time.
Knowledge and capacity exist
Twenty-six years of promoting and implementing the essential medicinesconcept mean that WHO has developed the most diverse and extensiveconcentration of essential medicines expertise in the world. Theorganization can advise on getting good-quality medicines to where theyare needed, and how to get them administered and taken correctly. Thisin turn means generating the capacity to implement a national medicinespolicy, developing expertise in supply chain management, transferringknowledge of pharmaceutical norms and standards, making informationon sources and prices freely available, strengthening regulatory capacity,and promoting good prescribing skills.
Yet for far too many people, essential medicines remain unaffordable.Sophisticated counterfeit medicines are a real danger. Confusion remainsabout what medicines supply systems work best and where. Quality andsafety issues threaten treatment regimes and patient health. But as thisreport shows, solid progress is being made.
Progress is indeed possible as a result of the sustained support andcollaboration of WHO’s partner agencies, governments andnongovernmental organizations.
More over, the momentum, energy and passion generated aroundmedicines for fighting HIV/AIDS, malaria and TB will be channelled intoother ongoing efforts to ensure that all essential medicines reach thepeople who need them.
The year in focus: medicines for HIV/AIDS, tuberculosis and malaria
LEE Jong-wookDirector-GeneralWorld Health Organization
2
WHO-EDM Report-Eng 27/10/04 2:58 pm Page 2

Policy
WHO is pioneering a ”hierarchi-cal” approach to monitoring medi-cines policy impacts at countrylevel. Level I consists of a struc-tured national pharmaceutical situation questionnaire and Level IIconsists of a systematic survey ofhealth facilities and pharmacies.By moving from the general to theparticular, the potential for makingeffective medicines policy deci-sions is increased.
In 2003, 145 countries completedthe national pharmaceuticalsituation questionnaire. Thequestionnaire can be rapidly andeasily completed with informationcollected mostly from healthministries and departments, and medicines regulatoryauthorities. Analysis of the 2003questionnaire results has indicatedwhich countries would benefitmost from increased WHOsupport for medicines activities.
Are countries implementingand updating their nationalmedicines policies?
Questionnaire results showed thatcountries that have updated theirnational medicines policy (NMP)within the previous 10 yearsincreased from 49 in 1999 to 57 in 2003, and that 16 countriessucceeded in moving from a draftNMP document in 1999, to anofficial NMP in 2003. But ninecountries have still not managed toturn their draft NMP documents intoofficial NMP documents. Imple-mentation is progressing, though —whereas only 40% of countries haddeveloped an NMP implementationplan in 1999, this figure hadincreased to 52% by 2003.
How do we know if NMP imple-mentation is effective? By monitor-ing levels of access to medicines,
and how rationally those medi-cines are being procured, paid forand used. Questionnaire resultshave given both cause for opti-mism, and a strong indication thatgreater efforts must be made bycountries and their internationalpartners to enhance medicinesimpact for public health.
Where are we in terms of access?
WHO is tracking the number ofcountries where more than 50%
A valuable resource for health professionals, policy-makers andresearchers, this publication guidesreaders through the process of developing, implementing andmonitoring a national drug policy
Country-specific data boost monitoring impact
Strategies to improve access tomedicines include: publicfinancing; generic procurement;health insurance; and appropriateprocurement and medicinesmanagement schemes. Datacollected showed that Eritrea,Mongolia and Sudan have allincreased per capita publicmedicines expenditure to morethan US$ 2.00, while in Bahamasand Belize, the increase wassubstantially higher. Fourteencountries that had not stipulatedgeneric substitution in privatepharmacies by 1999 had done soby 2003, while Benin, Guinea,Rwanda and Samoa haveadopted public health insuranceschemes that reimburse medicinesexpenditure. A further 11countries now limit publicprocurement to medicines on theiressential medicines lists. Theseinclude three countries in theAmericas and three countries inAfrica.
Rational to what extent?
Standard treatment guidelines,essential medicines lists (EMLs) andmedicines information centres, eachcontribute significantly to ensuringthat medicines are used to besteffect, both therapeutically andfinancially. In 1999, only 23countries reported having updatedtheir standard treatment guidelineswithin the previous five years, but by 2003 this figure had risen to31. And while in 1999 only 35 countries reported havingmedicines information centres thatprovided medicines informationboth to prescribers and dispensers,a further seven countries hadestablished such an informationcentre by 2003. Still, the figuressuggest that greater effort needs tobe put into encouraging many othercountries to make available the
of the population has previouslybeen reported as having no regularaccess to medicines. Questionnaireresults showed that 11 of thecountries surveyed (seven of whichare in Africa) that reported lessthan 50% regular access in 1999,now report more than 50% access.However, five countries reportedregular access as having declinedfrom more than 50% in 1999 toless than 50% in 2003.
3
WHO-EDM Report-Eng 27/10/04 2:58 pm Page 3

to be compared across differentyears, areas of concern to bepinpointed and progress to bemonitored.”
She notes that, ”the culture ofmonitoring is quickly gainingground. Before it was difficult tomotivate countries to doassessments and monitoring to findout whether people are accessingmedicines, where they areaccessing them, and if they aren’table to do so, why not. Butcountries increasingly understandthe benefits of collecting suchdata, and the impetus it gives tohealth policy-makers andmanagers to undertake furtherNMP development and
implementation.”Results can be both encouragingand discouraging, pointing to thedifficulties involved in tacklingmedicines issues. In thePhilippines, the cost of treatment inmany public health facilities (PHF)is lower than that available inprivate retail outlets. However,only one-third of essentialmedicines are available at all inPHFs, and are frequently out ofstock. Moreover, only 20% of thePHFs use standard treatmentguidelines and not one healthfacility had an EML. The negativeresults might be attributable todecentralization, which appearsto have slowed NMPimplementation.
Monitoring progress in the Americas
In 2003, the WHO Regional Office for theAmericas/Pan American Health Organization(AMRO/PAHO) organized a regional LevelII/systematic survey training workshop in theDominican Republic. Participant countries —Bolivia, Brazil, the Dominican Republic, El Salvador, Honduras, Nicaragua and Venezuela,and a representative of the Caribbean —developed an implementation plan for countrypharmaceutical assessment and monitoring usingLevel II indicators.
Level I monitoring had already produced someinteresting results. Analysis of the responses indicated areas in which WHO and countriesneed to focus greater effort. For example, only 11 of the 24 countries that responded indicatedthat they have a national strategy to combatantimicrobial resistance. And despite increasinguse of medicinal plants, most of the countries donot yet include medicinal plants in their national medicines lists.
But questionnaire responses revealed someencouraging signs of progress too. Procurement ofessential medicines only by the public sector hadincreased from 33% in 1999 to 50% in 2003.Several countries have increased their capacity totest the quality of medicines available on their
markets. In 1999, only 54% of officiallaboratories were involved in testing qualitycontrol, but by 2003, this figure had risen to 70%.However, the number of samples tested varieswidely from country to country, demonstrating thatthere is still a need to build national capacity torun a systematic and self-financed programme ofquality control testing as a key element of nationalmedicines quality assurance.
Medical schools increasingly include essentialmedicines in their curricula. In 1999, only 25% ofmedical schools did so. But by 2003, the figurehad grown to 41%. Drug information centres aremore widely appreciated, and both genericprescription and generic substitution haveincreased since 1999.
Commented Dr Rosario d’Alessio, AMRO/PAHO’sregional adviser for pharmaceuticals, ”Theassessments are vital not only for WHOidentification of priorities for technical assistance,but also to enable systematic documentation ofcountry-level progress and shifts in pharmaceuticalsector priorities.”
Further information:Rosario d’Alessio — [email protected]
guidance and information neededto support rational medicines use.The figures for EML updating aremore impressive: before 1999, 68 countries had updated theirnational EML within the previousfive years. By 2003, this figurehad risen to 80 countries.
Monitoring at the next level
Dr Daisy Carandang, a medicalofficer in the Department ofEssential Drugs and MedicinesPolicy at WHO Headquarters, has responsibility for monitoringthe impact of medicines policy.She describes how Level IImonitoring results, ”enable anational pharmaceutical situation
4
WHO-EDM Report-Eng 27/10/04 2:58 pm Page 4

Policy
In the Islamic Republic of Iran,survey data revealed thatprescribing of medicines isexcessive and that the averagenumber of medicines perprescription is high. The Ministryof Health has responded byestablishing a rational use centreto promote and monitor rationaluse of medicines.
Monitoring has highlighted manyother areas requiring improvementat national level. In Nigeria,assessment of facilities showedinadequate record-keeping,especially at primary health carelevel. Thus although 46% of keymedicines were available at
public health facilities, 7% of themhad expired. By comparison, noexpired medicines were found onthe shelves in private drug outlets.
Results also sometimes indicatewhen national medicines targetsare not being met. In Ethiopia, thenational average for availabilityof key essential medicines inhealth facilities was 70%, 85%and 91% for public healthfacilities, regional medicinesstores and private medicines retailoutlets respectively. The figures arelower than the 100% target setout in the Health SystemDevelopment Plan.
Priorities for 2004
WHO aims to furtherinstitutionalize medicines policymonitoring. It will also encourageuse of monitoring results in theplanning and implementation ofnational programmes, and ofWHO medicines activities atcountry and regional levels.
”In many ways the challengesremain the same. But theknowledge about how to tacklethem is improving. If thisknowledge was to be combinedwith political will and enoughresources to put policy intopractice, WHO could withoutdoubt achieve its medicinesobjectives,” comments Dr GuitelleBaghdadi. As programme officerin essential drugs and medicinespolicy at WHO Headquarters, shecoordinated a global processleading to the WHO MedicinesStrategy 2004–2007.
Five key working groupscomposed of WHO staff inHeadquarters, WHO regions andcountries together reviewedmedicines challenges and plannedWHO responses for addressingthem during 2004–2007. Dr Baghdadi continues, ”The newstrategy is coherent and easy tofollow. We have also includedsome new areas that were notincluded in the previous strategy(WHO Medicines Strategy2000–2003), reflecting the
evolution of the environment inwhich we work. So access toessential medicines as a humanright, the promotion of ethicalpractices in the pharmaceuticalsector, the UN prequalificationproject, our work with the GlobalFund, and the promotion ofinnovation based on public healthneeds, but especially forneglected diseases, are all nowcovered.”
The new strategy retains the samefour core objectives as theprevious strategy (policy; access;quality and safety; and rationaluse), which are divided intocomponents and expectedoutcomes, with a clear indicationof what is needed in countries toturn WHO’s vision for medicinesinto reality.
Progress in medicines work willcontinue to be tracked via a set of country progress indicators.The strategy can be accessed at:http://www.who.int/medicines/strategy/stmission.html.
A vision for essential medicines: WHO Medicines Strategy 2004–2007
Further information:Guitelle Baghdadi — [email protected]
The WHO Medicines Strategy2004–2007 provides guidingprinciples for medicines activitiesat country, regional and globallevels
5
Further information:Daisy Carandang — [email protected]; WHO pharmaceutical situationdata can be accessed at:http://mednet.who.int
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 5

• A global survey of nationalpolicy on traditional medicineand regulation of herbalmedicines was carried out to:obtain baseline information;assess the impact of the WHOTraditional Medicine Strategy todate; and identify the technicalsupport needs of MemberStates. Analyses of the surveyresults and summaries havebeen prepared for easyconsultation. This activity wassupported by Japan’s NipponFoundation. Many other newpartners are working withWHO to implement thestrategy. In 2003, they includedthe Regional Government ofLombardy, Italy and the Princeof Wales’s Foundation forIntegrated Health.
• A series of regional workshops— supported by theLuxembourg Government —was held to familiarize nationalregulatory authorities withherbal medicine quality andsafety issues, and requirementsfor registration. More than 60countries from all six WHOregions participated in theworkshops.
• WHO Guidelines on GoodAgricultural and CollectionPractices for Medicinal Plantswere published to promoteherbal medicine quality controlthrough good agriculturalpractices and sustainablecollection of medicinal plants.
• A WHO Consultation was heldin Milan, Italy in December, tofinalize the WHO Guidelinesfor Developing ConsumerInformation on Proper Use ofTraditional Medicine andComplementary/Alternative
Medicine, with support from theRegional Government ofLombardy, Italy.
• Organized largely by theWHO African Regional Office,the first African TraditionalMedicine Day was held inAugust, highlighting the roleand value of traditionalmedicine in African culture.
• The third meeting of the WHOAfrican Regional ExpertCommittee on TraditionalMedicine was held in SouthAfrica to: share countryexperience regardingtraditional medicine R&D fortreatment of HIV/AIDS,malaria, sickle cell anaemia,diabetes and hypertension;review draft guidelines forconducting clinical observation
studies of use of traditionalmedicine; review draftguidelines on researchmethodology for evaluating thequality, safety and efficacy oftraditional medicine in Africa;and review a regionalframework on intellectualproperty rights for theprotection and benefit-sharingof traditional medicineknowledge and the use ofAfrica’s biodiversity.
Further information:Xiaorui Zhang —[email protected]; [email protected] copies of the guidelinedocuments mentioned.
His Royal Highness the Prince of Wales, President of the Prince of Wales’s Foundation for Integrated Health meets Dr Xiaorui Zhang,team coordinator of the traditional medicine team at WHO Headquarters
Highlights of WHO work in traditional medicine in 2003
PHO
TO: G
eorg
e Bo
dmar
6
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 6

Policy
WHO medicines advisers are nowworking in 11 WHO countryoffices in Africa. Their task is towork with ministries of health andother stakeholders to plan,implement and monitor nationalmedicines policies. Their ultimategoal is to improve access to andrational use of good-qualityessential medicines, especiallythose for treating HIV/AIDS,tuberculosis and malaria.
During 2003, the medicinesadvisers supported their respectiveministries of health in conductingbaseline surveys of thepharmaceutical sector. Throughthese surveys, national capacity inmonitoring and evaluation wasgreatly strengthened. OgoriTaylor, medicines adviser forNigeria (see box), comments that,in the case of Nigeria, thepharmaceutical sector review was
extensively referred to duringrevision of the national medicinespolicy.
In Ghana, Kenya and Uganda thebaseline surveys wereimplemented with the support ofthe Regional Collaboration forAction on Essential Medicines inAfrica. This is a programme that isjointly implemented by WHO andHealth Action International Africa(a network of civil societyorganizations). The Collaborationprovides intensified support toincrease the coordination andparticipation of ministries ofhealth, civil society and WHO inplanning, implementing, andmonitoring medicines policies andprogrammes.
As well as the baseline surveys,the Collaboration has supported anumber of activities related topricing and intellectual propertyissues. In 2003, the Collaborationand WHO medicines adviser forUganda, Joseph Serutoke (seebox), provided technical andfinancial support to the UgandaCoalition for Access to EssentialMedicines, to host a nationalstakeholder workshop on“promoting public health throughpatent legislation”.
Ogori Taylor is national programmeofficer/medicines adviser for Nigeria.In describing her role as medicinesadviser, she comments, ”Thechallenges for Nigeria’spharmaceutical sector are enormous,but I’ve been able to provide insightinto medicines management andrational use problems, especially interms of how they impact on patient
care.” She is heavily involved in access, quality and rational useissues, especially in relation to antimalarials and antiretrovirals.
Joseph Serutoke is WHO medicinesadviser for Uganda. He is a registeredpharmacist, qualified from Uganda’sMakerere University Medical Schooland with postgraduate training inHealth Systems Management andDevelopment from Galilee College,Israel and Karolinska Institute, Sweden.Having worked in public healthservices, academia and the private
sector on national medicines procurement and supply, regulation ofthe pharmacy profession, and health sector reform, he hasaccumulated a wealth of experience. Mr Serutoke comments thatWHO medicines advisers are “involved on a daily basis in excitingand challenging work, seeking and implementing innovativeapproaches and strategies, with many others, to improve access,quality and rational use of medicines in our communities.”
Medicines advisers: maximizing medicines impact atcountry level
Further information:At WHO Headquarters,Gilles Forte — [email protected];Joseph Serutoke —[email protected]; Ogori Taylor —[email protected]
7
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 7

“If you have a peptic ulcer andrequire a month’s treatment, theoriginator brand version ofranitidine will cost you theequivalent of 50 days wages inCameroon, almost 19 days of payin Armenia and 13 days in thePhilippines…If a partner andchildren get sick, then themedicines bill will rapidlydevastate a household income.”
With this truth, the new jointWHO–Health Action International(HAI) project manual MedicinePrices — a New Approach toMeasurement was launched in2003. The manual andaccompanying workbook, whichare available in Arabic, English,French and Spanish present arigorous method for datacollection and analysis, for use bygovernments, nongovernmentalorganizations and othersinterested in price information.
Applying the methodologyat country level
In addition, a series of regionalworkshops on medicine prices isbeing organized. The first of thesewas held in October 2003 inCairo. Those taking part were
split into working groups focusingon data collection (via localpharmacies) and workbook data-entry exercises. The workshopwas also a forum to share country-specific price issues.
Two members of the University ofKuwait’s Faculty of Pharmacyattended the Cairo workshop, aspreparation for a medicine pricingsurvey in Kuwait. Dr Douglas Ball,Associate Professor of PharmacyPractice, commented, ”Apart frommaking contact with otherinterested groups in the Arabic-speaking countries and learningabout their particular concernsand situations, more specificbenefits were realized. HearingDr Anita Kotwani’s experience inRajasthan, India, clarified theplanning and administrationnecessary for successfullycompleting a pricing survey. Thiswas complemented with the mockdata collection and entry exercise,which provided insight into thepractical difficulties that can beencountered. Overall, the Cairoworkshop was a rewardingexperience that helped to prepareus for conducting a medicinesurvey in Kuwait.”
Participants generally conductcountry medicine price surveysafter attending an initial workshopand then attend a secondworkshop, to consider dataanalysis and interpretation issues.Lebanon has already initiated aprice survey and other countriesare set to follow suit in 2004.
Higher prices in poorcountries
Andrew Creese, a healtheconomist working on medicinepricing at WHO Headquarterscomments, “What is clear is thatmanufacturers’ pricing policies
The Medicine Prices manual, an essential tool for collectingmedicine prices information.
Medicine prices — measuring the difference
and government pricing policiesoften result in much higher pricesin poor countries for the samedrug, and the problem is madeworse by poor people having tobuy their own medicines. Thismechanism doesn’t apportionblame. But it does give a goodmethodology for comparingprices. It also reveals hugedifferences in the price break youcan get with generics. It’s anevidence-based means ofempowering policy-makers.”
Margaret Ewen, Director of HealthAction International Europe andproject coordinator, is categoricalabout the need for governments toact regarding medicine prices,”No longer can governmentsstand idle while the poor diebecause they cannot afford medi-cines. They must implement soundpricing policies. But to do this,careful diagnosis of prices isneeded — that’s where theWHO–HAI methodology is so use-ful. It can point the way to bring-ing medicine prices down.”
The project is having otherbenefits. Ms Ewen continues, ”The WHO–HAI project has notonly produced a much-neededsurvey tool. It’s also shown thesynergistic value of WHO andcivil society working together. Wesaw this during the development ofthe methodology and, importantly,when the surveys wereundertaken. Most surveys are nowundertaken as collaborationsbetween civil society, government,WHO and academia.”
Further information:Andrew Creese —[email protected]; Marg Ewen —[email protected];email [email protected] —for a copy of the Medicine Pricesmanual.
8
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 8

AccessWhile working in Rwanda, Ruth
Evans — journalist and writer — met and interviewed two youngwomen. She writes…
The 1994 genocide in Rwandawas deliberately planned andsystematically executed, resultingin the brutal mass murder of overa million people. Rwandanwomen and young girls not onlywitnessed the torture and killing oftheir families, and destruction andlooting of their homes andproperty. They were alsosubjected to extreme and brutalforms of sexual violence, raped,deliberately infected withHIV/AIDS and mutilated. Chantalis one of them. Her family wereall killed in the genocide, and shewas raped and infected with HIV.As the sole survivor, she nowstruggles to care for five orphanedchildren, as well as her own child,conceived as a result of the rape.Ten years on, she is sometimes toosick to work or plant her shamba,
and then the children go hungry.She knows that treatment withantiretrovirals is available inRwanda for around US$ 25 amonth. But she says she cannotafford even the bus fare to theclinic, let alone the medicines.“Only God can help me,” shesays. “The genocide is still a dailyreality for women like me, onlyours is a slow death. My biggestworry is who will look after thechildren when I am dead.”
Akimana’s story is just asdistressing. When she was tenyears old, Akimana’s Hutu parentswere killed because they opposedthe genocide in Rwanda.Although she herself was shot inthe shoulder and left for dead, shesurvived. Today she looks after herfour orphaned brothers andsisters. “Getting treatment is a bigproblem,” she says. She still hasmedical complications from herwounds, including fainting attacksand heart problems. But her
greatest worry is looking after theother children. “It’s not easy to getmoney to take them to the clinicabout 10 kilometres away.Malaria is the biggest problem. Inthe rainy season, one of themmight fall sick twice a month. Itisn’t easy to get treatment and themedicines are too expensive forus to buy.”
These stories portray not only theterrible circumstances somepeople have been forced toendure as a result of civil strife.They also underscore thecontinuing gap between thepotential that essential medicinesoffer for improving andmaintaining quality of life, and thereality that for millions of peoplewho desperately need them, theyremain far beyond reach.
(Editor’s note: Chantal gave per-mission for her story to be used topublicize the plight of women whowere raped during the genocide.)
Genocide survivors at Munrire Genocide Site in Rwanda
Access denied: two personal stories
PHO
TO: U
nite
d N
atio
ns/D
PI
9
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 9

WHO’s Constitution states, ”Theenjoyment of the highestattainable standard of health isone of the fundamental rights ofevery human being withoutdistinction of race, religion,political belief, economic or socialcondition.” The human right tohealth is also recognized in manyinternational and regional treaties.
The most comprehensive article onthe right to health is found in theInternational Covenant onEconomic, Social and CulturalRights (ICESCR). Article 12.2 setsout a number of steps for ensuringprogressive realization of this right,including provision of healthfacilities, goods and services.
Turning treaties into practice
By the end of 2002, 142countries had signed the Covenantand 83 countries had signedregional human rights treaties.Over 100 countries have nowincorporated the right to health in
their constitution. Ratification of aninternational human rights treatymeans that a state becomes astate party to that treaty. As such,it is obliged to meet certainobligations with respect to itspopulation. But are theseobligations enforceable inpractice?
In 2002, WHO started a study toidentify, analyse and summarizecourt cases in developingcountries that individuals orgroups had initiated against agovernment or governmentalinstitution, to secure access toessential medicines, fully or partlyon the basis of human rightstreaties signed and ratified bytheir government. Evidently, thestudy focused on those who hadwon their case and how theirexample could be used toempower other individuals andgroups to launch similarlysuccessful cases and claim thebenefits due to them.
A total of 20 cases fromArgentina, Bolivia, Colombia,Costa Rica, El Salvador, SouthAfrica and Venezuela wereidentified. Of these, seven (35%)cases had been stronglysupported by nongovernmentalorganizations. Eleven (55%) casescontested a social securityscheme. In a further six (30%)cases, the defendant was theministry of health.
The full study has not yet beenpublished, but the boxedexamples illustrate the potentialfor increasing access to essentialmedicines through legal actionbased on the state’s obligation toprovide access to essentialmedicines in part fulfilment of theright to health.
Further information:Hans Hogerzeil —[email protected]
Essential medicines and the right to health
Claiming the right to access to medicines
In El Salvador, Odir Miranda and 25 others livingwith HIV/AIDS filed a complaint in January 2000,before the Inter-American Commission on HumanRights, alleging the state’s failure to provide themwith life-saving antiretroviral (ARV) therapy. TheCommission solicited the Salvadoran State tocomply with its regional obligations and providethe treatment. The Supreme Court in El Salvador supported the claim and in 2001 issued a rulingordering the Social Security Institute to provideARV therapy. The ruling was based on the right to life and health as entrenched in the Constitutionand international treaties ratified by El Salvador.
In 2001, in South Africa, individuals and healthadvocacy nongovernmental organizations jointlychallenged the decision of the South AfricanMinistry of Health to restrict access to nevirapine,a medicine used to prevent mother-to-childtransmission of HIV. The central argument wasthat restriction of nevirapine to test sites onlyviolated the right to health, to life and to equality.The case was eventually brought before theConstitutional Court. In 2002, it ruled that therestriction on nevirapine was unconstitutional andordered the government “without delay” toensure its availability throughout the country.
10
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 10

AccessThe success of new strategies to
fight against high-burden diseasesdepends heavily on effectivemedicines supply systems. Supplyproblems must not be thebottleneck that prevents medicinesreaching those who need them.WHO is exploring options forusing the experience ofnongovernmental organizations(NGOs) to create supply systemsbased on an efficient public–private mix. One example ofWHO’s work in this area is aninnovative study on medicinessupply activities by faith-basedorganizations.
Throughout 2003, in collaborationwith the Ecumenical Pharma-ceutical Network, and withfunding from the SwedishInternational DevelopmentAgency, WHO surveyed themedicines supply practices of 16 faith-based NGOs in 11 sub-
Saharan African countries. Oneparticularly effective feature hasbeen data collection throughpaired country assessments. Stafffrom NGOs in one country havesystematically researched supplysystems in their partner countryand later hosted a return visit.
Adding value to supplysystems
Commenting on the value of thistwinning arrangement, MrsMarsha Macatta-Yambi,pharmacist at the Christian SocialServices Commission, Dar EsSalaam, Tanzania, said that,”Receiving the visit from theZambian group was a highlight,and it reinforced just one of theproject’s positive outcomes — ithas made my colleagues in otherdepartments realize theimportance of my pharmacy’swork.”
Collaborators in medicines supply (from left to right): Marlon Banda(lead investigator, Zambia); Stella Feka (Organisation catholique pour laSanté au Cameroon); Marsha Maccata-Yambi (Christian Social ServicesCommission, Tanzania); Hans Peter Bollinger (Ecumenical PharmaceuticalNetwork)
The country reviews had beencompleted by December 2003.Preliminary findings indicate thatfaith-based supply organizationsoften fill gaps left by governmentsupply systems. One issue that hasbeen highlighted is the negativeeffect of unexpected drug dona-tions on the sustainability of NGOsupply systems. In some cases,donations distributed free ofcharge, had decreased the salesof revolving drug fund mecha-nisms, leading to stock wastageand financial loss.1
Data analysis of study results iscontinuing, and WHO will dissem-inate the information gatheredand its recommendations.
Further commenting on herinvolvement in the study, MrsMacatta-Yambi said, ”My initialfeeling was one of trepidation atthe possible difficulties and extrawork, but it has been worth all theeffort — being part of the projecthas definitely added value to mywork. The study questionnairesare so well thought out and socomprehensive that the project hasgiven us greater insight into whatwe do. Also, transparency is soimportant to us and this projecthas been one way of ensuring ourtransparency.”
1 This finding underlines the importance ofcontinued adherence to the InteragencyGuidelines for Drug Donations, and acompanion volume, Guidelines for PriceDiscounts of Single-source Pharmaceuticals,the latter published by WHO in 2003.They can be obtained by [email protected].
Ensuring medicines supplies at all levels at all times
Further information:Marthe Everard —[email protected]; Sophie Logez — [email protected]
PHO
TO: W
HO
/Sop
hie
Loge
z11
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 11
Civil society has had a major rolein pushing the issue of access toantiretrovirals (ARVs) higher upthe global health agenda.Nongovernmental organizations(NGOs) such as Oxfam,Médecins Sans Frontières (MSF)and the Treatment ActionCampaign in South Africa, as wellas the media, have all activelyand repeatedly demanded thatHIV/AIDS medicines, includingARVs, be made much more widelyavailable and affordable.Concurrently, WHO is looked tofor guidance on how to ensuregood-quality and effectivemedicines.
WHO continues to develop closecollaborative relationships withmany NGOs working onHIV/AIDS issues, including MSF.“We don’t necessarily alwaysagree,” says Daniel Berman, co-director of MSF’s AccessCampaign, “but the workingrelationships we have developedwith WHO have been veryproductive. We know that some ofWHO’s most important work is
carried out under considerablepressure. One example isprequalification of medicines. It’scrucial for the countries in whichwe work, and has revolutionizedthe purchase and supply of low-cost medicines.”
In October 2003, WHO and MSFjointly published SurmountingChallenges: Procurement ofAntiretroviral Medicines in Low-and Middle-Income Countries.1
This survey of the availability anduse of ARVs in 10 countries foundsubstantial variation in access toARVs. But it distils the individualprocurement experiences of thecountries concerned and makes anumber of recommendations onhow to optimize ARV availability.
Drug price targets: could try harder
Much remains to be done,however, to get ARVs to all whoneed them. Although prices ofARVs are now much lower thanthey have ever been, MSF saysthey should come down even
further still. “WHO’s drug pricetargets lack ambition and do notreflect prices that are currentlyavailable,” claims MSF’sPresident, Morten Rostrup,referring to an announcement byan Indian drug company that isnow offering its triple therapy forUS$ 140 per patient per year.“Today, drug prices have fallenanother 50%. WHO shouldencourage this trend so thatuniversal access to AIDStreatments becomes a reality. Thefull effects of the implementationof TRIPS 2 will not become visibleuntil after 2005, when genericcompetition will become moredifficult. WHO will then need toplay an even more active role inensuring that affordable essentialmedicines become available.”
1 http://www.msf.org/source/reports/2003/09/msf-who-arvreport.pdf2 World Trade Organization Agreement on Trade-Related Aspects of Intellectual Property Rights.
WHO and Médecins Sans Frontières: productive differences
Documenting availability and use of antiretrovirals (ARVs) in 10 countries, this new publication givesrecommendations on how to optimize ARV availability
12
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 12

Quality and Safety
“Because it works hand-in-handwith national medicines regulatoryauthorities, our prequalificationproject is proving to be one of thebest things we’ve done to helplocal producers improveantiretroviral (ARV) quality. Thefeedback they get from us hascontributed substantially to scalingup production of good-qualityARVs,” says André van Zyl, ofWHO’s Quality Assurance andSafety of Medicines team.
Partnered with UNICEF, UNAIDSand the UN Population Fund, andreceiving support from the WorldBank, the prequalification projectprovides a solid, scientificassessment of the quality of bothgeneric and patented medicines,based on internationallyharmonized standards forevaluating information on productquality and bioequivalence,inspecting manufacturing sites andundertaking quality control ofpharmaceutical production. “Theproject provides a greatopportunity for pharmaceuticalmanufacturers to prove that theassumed quality distinctionsbetween innovative drugs andmulti-source products are notvalid,” comments Mr van Zyl.
Increasing treatment options and simplifyingtreatment regimes
On World AIDS Day 2003, WHOannounced that three new genericproducts for first-line AIDS treatmenthad been added to the list ofprequalified products. The productsare fixed-dose triple-therapycombinations and will contribute tosimplifying HIV/AIDS treatmentregimes. By the end of 2003, over240 medicines for treatingHIV/AIDS had been evaluated,and more than 50 of theseproducts included in the list. Theproject now also covers medicinesfor treating tuberculosis andmalaria.
The list means that procurementagencies can choose betweenseveral manufacturers offering thesame quality product. Indeed, theGlobal Fund to Fight AIDS,Tuberculosis and Malariaconsiders the list to be vital toensuring that its funds are spenton medicines of assured quality.Mr Van Zyl points out that, “TheFund is allowing countries whoreceive funds a period of grace interms of procuring ARVs and othermedicines. But after that fundsmust be spent only on productsthat have been prequalified byWHO.” The list savesprocurement agencies time sincethey don’t have to assess thequality of products themselves.
Evaluations and inspections arecarried out by a group ofqualified external experts fromnational medicines regulatoryagencies providing support to acore team at WHO. At all stages,WHO provides feedback toencourage the manufacturer tomeet prequalification standards.
Publicly available standardsfor independent laboratories
Key also to the success of theprequalification project has beenthe issuing of pharmacopoeialmonographs to provideindependent laboratories with theinformation they need to be ableto test product quality. In 2003,draft monographs were issued forsome ARVs. Nine monographswere circulated for comments andfurther validation. Others willfollow.
Comments Dr Sabine Kopp, ascientist with the Quality andSafety: Medicines team at WHOHeadquarters, “Because ARVs arenew substances and products, nointernationally validatedmonographs are publiclyavailable for them. We arecollecting information frommanufacturers in all regions sothat we can develop tests fordetecting any impurities. Ofcourse there are commercialsensitivities, but we’ve had agood response from manymanufacturers. Hopefully othermanufacturers will come torecognize that this will contributeto not only ensuring that patientsget quality medicines, but also tofighting counterfeiting.”
Further informationon the prequalification project: André van Zyl —[email protected]
Further information onpharmacopoeial monographs: Sabine Kopp — [email protected]
Prequalification — vital to global goals for treating HIV/AIDS, malaria and tuberculosis
PHO
TO: I
rene
R L
engu
i/L’I
VC
om13
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 13

Without the right medicines, therecan be no effective treatment formalaria, and resistance toantimalarials will continue togrow. A WHO study, The Qualityof Antimalarials, published in May2003, revealed significantproblems of substandard productsin Africa.
The deeply disturbing resultsshowed that many antimalarialsfor sale in the countries studied(Gabon, Ghana, Kenya, Mali,Mozambique, Sudan andZimbabwe) often contain little orinsufficient active ingredients. Thisappears to be due to failure ofmanufacturers of antimalarials tocomply with good manufacturingpractice (GMP), and to the highprevalence of counterfeiting.
“Such results cannot be ignoredby Roll Back Malaria (RBM)partners — either at the globallevel or at the level of countryaction,” says Dr Clive Ondari,one of the report’s authors. Heaffirmed that WHO’s RBMprogramme, and others working
in malaria prevention, mustactively support nationalregulatory authorities instrengthening GMP as well asgood procurement and gooddistribution procedures.
Quality standards for manyantimalarials are now in place.However, for a number of thenewer antimalarial products, suchstandards have yet to bedeveloped. The challenge will beto get the different RBM technicalpartners (including WHO,UNICEF, USAID and the UnitedStates Pharmacopeia) to workeffectively together to improveproduction and distribution ofsafe, effective and good-qualityantimalarials.
Safety tracking of the new antimalarials
Safety issues will be critical to effective use of the newgeneration of artemisinin-basedcombination (ACT) antimalarials,now being deployed in countrieswhere resistance to chloroquine
and sulphadoxine-pyrimethamineis high.
WHO and RBM are alsodeveloping pharmacovigilancereporting programmes for the newartemisinin combinations, in a bidto avoid the quality and resistanceissues that have beset past drugresponses. Pharmacovigilanceidentifies and quantitativelyassesses the risks related to the useof medicines in an entirepopulation or in specific populationgroups. It can pinpoint problemsrelating to misuse of a medicine,poor-quality or counterfeitproduction, or safety issues notpicked up during a drug’sdevelopment and initial testing.
Dr Mary Couper, who leadspharmacovigilance activities atWHO Headquarters in Geneva,comments that, “Any new drug onthe market needs especialvigilance. No drug is completelysafe. But there are certain effectswith malaria medicines that weneed to be on the look-out forsuch as blood disorders andStevens-Johnson allergic skindisorders. This is especially truefor African countries for whichACTs represent new products andwhich have not yet developedcapacity to undertakepharmacovigilance.”
Further information on quality of antimalarials: Clive Ondari — [email protected];email [email protected] fora copy of The Quality ofAntimalarials
Further information onpharmacovigilance: Mary Couper —[email protected]
Quality antimalarials: meeting the challenge
Child being tested for malaria in the Congo
PHO
TO: W
HO
/Har
ry A
nend
en
14
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 14

Quality &
Safety
Recent headline stories in theinternational press on counterfeitmedicines touch only the tip of avery large and very dangerousiceberg. They are in part aresponse to WHO’s efforts to raiseawareness of the dangers ofcounterfeit medicines, defined asmedicines that are ”deliberatelyand fraudulently mislabelled withrespect to identity and/or source”.
Lucrative trade in counterfeitmedicines
Some agencies estimate that up to25% of all medicines in thedeveloping world are counterfeitor substandard. Counterfeitmedicines are often used —particularly in Africa and Asia —to treat life-threatening conditionssuch as HIV/AIDS, tuberculosisand malaria.
The lack of openness and poorinformation exchange on this issuemeans that fighting counterfeits isnot easy. Sometimes, of course,the information is simply notavailable, because the necessarysurveillance is not undertaken.And legitimate manufacturersworry that if concerns aboutcounterfeit medicines are publiclyhighlighted, sales of their productswill fall. So they can be reluctantto participate in campaignsagainst counterfeit medicines.Compounding these problems isthe fact that many countries find itdifficult to attract qualifiedpersonnel for regulatory positions,given that they can offer only lowsalaries. Law enforcement isanother factor — all too oftencounterfeiting of medicines isclassified merely as a tradeviolation, carrying a minorpenalty only.
Awareness campaign
In 2003, WHO intensified itsefforts to raise public andgovernment awareness of thedangers of counterfeit andsubstandard medicines, and toimprove collaboration betweenmedicines regulatory agencies andlaw enforcement agencies in thisarea. It also continued to strengthennational regulatory authorities,through training, provision ofadvice, and development ofguidelines and tools for improvingregulatory systems.
Eshetu Wondemagegnehu is aWHO technical officer, workingwith the Quality and Safety:Medicines team at WHOHeadquarters. Although herecognizes that public awarenessof counterfeit medicines isincreasing, he considers thatenhanced country-level regulation,using WHO guidelines andadvice, remains an urgent priority.“In most developing countries,there is a shortage of medicines.This encourages smuggling andcounterfeiting. What’s more, theirregulatory system is often very
Quality assurance and safety — a cure for counterfeiting
Fakes in Central and Eastern Europe and the Newly Independent States
Counterfeit medicines plague not only Asia and Africa.Following the collapse of communism, under which the statehad been the monopoly supplier and regulator of medicines,ensuring effective medicines regulation in Central and EasternEurope (CEE), and in the Newly Independent States (NIS),proved to be extremely challenging. Although many of thesecountries have now created national medicines regulatoryauthorities, regulatory ”gaps” are reflected in reports ofincreased incidence and variety of counterfeit medicines.
Accurate data on incidence of counterfeit medicines in NIS andCEE countries have yet to be collected. But we do know that inseveral countries in the Caucasus, Central Asia and South-Eastern Europe, medicines are sold on markets and from kiosks.Ministries of health in the region have limited funds forpurchasing medicines and so populations must generally covertheir health costs themselves. The temptation to buy medicinesfrom these cheap sources is therefore very strong. Unfortunately,the medicines may be not only cheaper but fake and/orsubstandard as well. Kees de Joncheere, Regional Adviser forPharmaceuticals in WHO’s European Regional Office, observesthat, ”Ministries of health in CEE and the NIS are clearly awareof this problem and very concerned about it, but they lack theresources that would enable them to tackle this issue effectively.”
Further information: Kees de Joncheere — [email protected]
15
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 15

weak. So medicines are easilysold over the counter withoutprescription or even on the street.In other words, we have to look atthe whole pharmaceutical supplysystem, and encouragegovernments to strengthen andreally enforce their medicinesregulation and legislation,including where, how and bywhom medicines can be sold.”
Mr Wondemagegnehu continues,“We are very concerned aboutthe persistence of counterfeits indeveloping countries. Notsurprisingly, for many of them,national policies are driven byeconomic priorities and the needto ensure safe medicines topromote public health is forgotten.Production and sale of medicinescan then take precedence overensuring the quality and safety ofmedicines. In general, I think it’s aquestion of political
commitment…if the commitment isthere it’s easy to enforceregulation.
”China is a good example ofeffective political commitment andallocation of the resources needed.In just five years it has set up anindependent regulatory authority(the State Drug Administration) anddeveloped significantly in terms ofinfrastructure and qualified humanresources. It has enacted the DrugAdministration Law with provisionsprohibiting the manufacture, saleand distribution of counterfeit andsubstandard medicines, and hasalso taken action against peopleand companies convicted ofcounterfeiting medicines.”
Joining forces to fight counterfeits
In 2003, implementation of aWHO multi-country project to
combat counterfeit medicines forthe greater Mekong sub-regioncountries (Cambodia, China, LaoPDR, Myanmar, Thailand and VietNam) continued, with supportfrom AusAID. The percentage ofcounterfeit artemisinin-basedantimalarials exceeds 50% inparts of this region. Comments DrBudiono Santoso, regionalpharmaceuticals adviser inWHO’s Western Pacific RegionalOffice, ”It’s hard to imagine whatthe final economic cost will be.The technological investment thatwill be required if these newartemisinin-based antimalarialsbecome ineffective, and yetanother antimalarial has to bedeveloped, is unthinkable.”
The project aims to improvecollaboration between thepharmaceutical sectors and lawenforcement agencies, and raisepublic awareness of counterfeitmedicines. WHO has worked withthe countries to not only developnational, cross-sectoral plans totackle counterfeits, but also toencourage collaboration,exchange of expertise andinformation-sharing between them.
A meeting in Hanoi between theMekong countries and a variety ofagencies (Interpol, ManagementSciences for Health, Aus AID,JICWELS (Japan InternationalCooperation for WelfareServices), United StatesPharmacopeia, Wellcome Trust,Australia’s Therapeutic GoodsAdministration and USAID) washeld in November. Dr Santososays that, ”It’s becomingincreasingly obvious that countriescannot fight counterfeit medicinesin isolation but must work togetherto track incidence of counterfeitsand the counterfeiters themselves,as well as encourage each otherto enforce legislation againstcounterfeit medicines.”Counterfeit medicines are increasingly headline news in both
the international and national press
CO
URT
ESY
OF:
Inte
rnat
iona
l Her
ald
Trib
une
16
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 16

Quality &
Safety
• Finalization of second series oftests for WHO ExternalAssessment for National QualityControl Laboratories, providingindependent, internationalstandards for quality-controltesting so that national quality-control laboratories canevaluate their level ofperformance of quality-controltesting of medicines.
• Development and adoption offive new and two revised Goodmanufacturing practice (GMP)texts to take account of countryrequests for more GMPguidance and of recentadvances in pharmaceuticalmanufacturing.
• Introduction to Drug UtilizationResearch published, to guidecountries on how they can useand benefit from medicinesutilization research.
• ASEAN countries agree onsingle set of technicalrequirements for medicinesevaluation, enabling bettertechnical collaboration amongASEAN member states,facilitating access to medicinesin the ASEAN region, andimprovement of the regulatorycapacity of less well resourcedASEAN member states.
• Tunisia starts publishingprescribing information for allmedicines approved by thenational medicines regulatoryauthority and granted amarketing authorization,indicating that developingcountries can make correctmedicines informationavailable, thus limiting thenegative impacts of unethicalmedicines promotion.
Further information: Lembit Rägo — [email protected]
In 2003, many long-term activitiesaimed at ensuring the quality andsafety of medicines — carried outin parallel to efforts to increaseaccess to essential medicines —were completed. Some of themare described briefly below.
• Creation of WHO AdvisoryCommittee on the Safety ofMedicinal Products, to respondto the growing number ofcountry requests for guidanceon medicines safety issues.
• First training course onpharmacovigilance for newantimalarials, which will serveas a model for similar trainingfor HIV/AIDS treatmentprogramme managers to initiatepharmacovigilance forantiretrovirals (ARVs).
• Volume 5 of the 3rd edition ofThe InternationalPharmacopoeia published,including 75 new monographsand test procedures. Thespecifications for all knownartemisinin-based antimalarialsare especially important. Theymean that vital information forimproving manufacturingquality control and helping newmanufacturers to startproducing good-qualityantimalarials, is now publiclyavailable. This will contribute toincreased competition andlowering of prices.
• Development of internationally-validated specifications forARVs used to treat HIV/AIDSinitiated, as a move towardsmaking information on qualitystandards publicly available.This will help national qualitycontrol laboratories to test thequality of products and genericmanufacturers to produce ARVsof assured quality.Poster used in Lao PDR to warn
against the dangers of counterfeitmedicines
Quality and safety achievements: 2003Dr Krisantha Weerasuriya,regional adviser in WHO’s South-East Asia Regional Office, furthercommented that almost all healthministry officials of the MekongDelta countries are now aware ofthe counterfeit medicines problemand that the next phase included,”making others, such as lawenforcement, legal and tradeofficials equally aware of it”.
The Mekong Project continues in2004, focusing on developing arapid regional alert system, post-marketing surveillance, deterrentlegislation and further advocacy.
Further information: Eshetu Wondemagegnehu — [email protected];Budiono Santoso —[email protected]; Krisantha Weerasuriya — [email protected]
17
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 17

“The Global Fund is already theworld’s largest single financier ofdrugs to fight AIDS, tuberculosis(TB) and malaria. To ensure thatthese drugs are of good qualityand safe, we rely heavily on theexpertise of WHO. We greatlyappreciate the close collaborationbetween the Global Fund andWHO’s Essential Drugs andMedicines Policy Department,”comments Professor RichardFeachem, Executive Director of theGlobal Fund to Fight AIDS,Tuberculosis and Malaria.
On World AIDS Day 2003, WHOannounced that three new genericproducts for first-line AIDStreatment had been prequalified.The products were fixed-dosetriple therapy antiretroviral (ARV)
combinations containinglamivudine, stavudine andnevirapine. Effective, simple totake as a treatment regimen andeasily administered, they are alsocost-efficient. By the end of 2003,the list of prequalified productscontained more than 50 ARVmedicines — in single-drug, two-drug and three-drug combinations.It also contained first- and second-line treatments for TB and onemedicine for malaria. By clearlyindicating what medicines cansafely be procured where, the listis both reducing the time andeffort needed for procurement,and helping to ensure that fundsfor treating the three majordiseases of poverty are usedoptimally.
Working in partnership with the Global Fund to Fight AIDS, Tuberculosis and Malaria
WHO is also collaborating withthe Global Fund to developpolicies and procedures formedicines procurement andsupply management, providingtechnical advice, analysis anddata. Global Fund procurementand supply managementguidelines now incorporate anumber of WHO pharmaceuticalnorms and standards.
Further information: Hans Hogerzeil — [email protected]
The WHO Model Formulary wasfirst launched in 2002 and thenmade available in electronicformat on the WHO medicinesweb site (http://mednet3.who.int/eml/eml_intro.asp) in 2003. Thispractical tool to assist nationaldrug selection committees has alsobeen released on CD ROM, andtranslation into Arabic, Russianand Spanish is now under way. In2004, plans will be made formaking the Model Formularyavailable on a palm computer.
The electronic versions (in bothpdf and Word formats) of theModel Formulary are especiallyuseful for countries that would liketo develop their own formulary.Rather than starting from scratch,they can now start with a full text
and adapt that to their specificneeds by omitting or adding otherinformation.
Presenting independentinformation on all 316 medicineson the WHO Model List ofEssential Medicines, the 2004edition of the Model Formularywill also incorporate updates andchanges made during the relevantExpert Committee meeting of2003. A manual describing howcountries can best adapt theModel Formulary to nationalrequirements will be madeavailable in electronic format inearly 2005.
Further information: Lalit Dwivedi — [email protected]
Easy electronic access to WHO Model Formulary
The WHO Model Formulary wasfirst launched in 2002, beforebeing made available on CDROM in 2003
18
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 18

Rational U
se
Traditional medicine vs. SARS: expert meeting backsintegrated treatment
In July 2003, WHO announcedthat it had broken the chain ofhuman-to-human transmission ofthe SARS (severe acute respiratorysyndrome) coronavirus. In anepidemic that started in Chinaand lasted a little over 12 months,more than 8400 cases of SARSwere reported in 29 countries.Within a few months of the end ofthe epidemic, it was recognizedby a meeting of experts thattraditional Chinese medicine(TCM) had helped fight the SARSbattle. Why and how was TCMintegrated with western medicine(WM) to achieve this success?
A long history of use
China has a long history oftraditional medicine use, whichoften includes herbal medicines,acupuncture or acupressure andspiritual therapies. TCM isfrequently used to meet primaryhealth care needs.
When SARS broke out, theChinese State Administration ofTraditional Chinese Medicine(SATCM) initiated clinical researchprojects on integrated TCM andWM. A total of 21 projects wereset up focusing on prevention,treatment and rehabilitation.(More than half of all SARSpatients in China were treatedwith TCM.) At the request of theChinese Government, and withfinancial support from the NipponFoundation, WHO guided SATCMon 13 clinical trials. Workingtogether, WHO and SATCM laterorganized the International ExpertMeeting on Review of Treatmentof SARS and the Integration ofTraditional Chinese Medicine withWestern Medicine. The meeting
was held in Beijing, China, inOctober 2003, and reviewed thereports of the 13 clinical trials.
Dangerous conditions
In all, 68 experts from sevencountries attended the meeting.They paid tribute to the TCMprofessionals who treated SARSpatients. They were recognized ashaving carried out vital datacollection in dangerousconditions. They are estimated tohave participated in the treatmentof SARS in 102 of the 195 SARS-specific hospitals in China.
For SARS patients, data collectedindicated that TCM couldpotentially alleviate fatigue,shortness of breath and otherclinical symptoms and enhanceimmune system functioning. The13 clinical reports indicated thatno negative side-effects on heart,liver or kidney functioning wereobserved, suggesting that TCMtreatment was safe. Moreover, fora group of early-stage SARSpatients treated only with TCM, allrecovered, without the need forcorticoids, antiviral agents orantibiotics. Additionally, no SARScases were observed amonghealth workers who had beenexposed to SARS but who hadtaken TCM for the purpose ofprevention. The meeting report (inpress) comments, “TCM is theaccumulation of thousands ofyears of experience of theChinese nation in fighting againstdiseases. Facing unknown reasonsor complicated pathologicalcauses of diseases, traditionalChinese differentiation cognitiontheory and treatment principleshave obvious advantages.”
However, the experts whoattended the meeting noted thatthe data in the reports wereinconclusive. Accordingly, theirrecommendations were to:continue follow-up of SARS cases,and observation and comparisonof the long-term effects of varioustreatments; improve clinicalresearch design; and strengthenresearch on health economics andSARS.
Further information:Xiaorui Zhang — [email protected]
Communicable Diseases Hospital,Beijing, China
PHO
TO: W
HO
/Pie
rre
Viro
t
19
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 19

20
“It was a unique and importantmeeting. By bringing together thelarge pharmaceutical companies,the generic manufacturers anddisease control experts, we wereable to get a consensus on theway forward. It was anopportunity for disease controlspecialists to say to thepharmaceutical industry — this iswhat we want. And there was aclear willingness by the industry tofocus on global public healthneeds,” comments Dr RichardLaing, of the Medicines Policy,Access and Rational Use team atWHO Headquarters. He isdescribing the meeting on fixed-dose combinations (FDCs) forHIV/AIDS, tuberculosis (TB) andmalaria, organized by WHO inDecember 2003 and supportedby the Rockefeller Foundation.Attended by WHO medicines anddisease control programmes,nongovernmental organizations,medicines regulatory agencies,and representatives of thepharmaceutical industry, themeeting brought together the fullrange of stakeholders in FDCs.
FDCs have a long history ofdevelopment and use. Thecombined contraceptive pill andthe treatment of cancer, infectiousdiseases, hypertension andneurological disorders, are well-known examples of FDC use. Infact, in the 1960s, in the USA,they accounted for over half of allpharmaceutical products and for40% of the best-selling medicines.But then followed controversy.Because there were many”irrational” combination productson the market, FDCs fell out offavour with medicines regulators.
“It became clear that FDCs shouldbe used only where combination
treatment offered a clearadvantage. Since the 1990s wehave become increasinglyconcerned about the rise ofantimicrobial resistance. Now weare also concerned about howbest to promote AIDS/TB/malariatreatment adherence. In bothareas, FDCs have obviousadvantages,” continues Dr Laing.
“Instead of asking someone totake 12 or 13 tablets a day, if heor she can just take one or two,then there is a much greaterchance of compliance. We haveseen this in TB control with use ofFDCs in DOTS1 programmes. Andwhen we consider the highinteraction of TB and AIDSinfection, it’s clear that FDCs willbecome increasingly important topublic health programmes.”
“The meeting was a key point intime. WHO was a forum for allthose people to come together, toget a synthesis of ideas. We were able to bring these differentgroups together because theyshare the same problems. Theconsensus was that FDCs are theway forward for HIV/AIDS, TB andmalaria treatment, where possible.That is the first choice. If that is notpossible, then we use blister packs,which also simplify patientadherence,” says Dr Laing.
FDCs also help streamlinemedicines supply management —theft, wastage and misuse can allbe minimized. However, thesethree- or four-drug combinationscan be difficult to produce toquality-assured standards.
The value of FDCs for 3 by 5
Commenting on the use of FDCantiretroviral (ARV) medicines
One pill to be taken 2 x daily: ground-breakingindustry–public health meeting on fixed-dose combinations
within WHO’s 3 by 5 strategy tofight HIV/AIDS, Dr VladimirLepakhin, WHO AssistantDirector-General for HealthTechnology and Pharmaceuticals,emphasizes that the ease ofcompliance and distribution wouldprove invaluable. “The 3 by 5strategy recommends simplifiedAIDS treatment regimens,” hecontinues. “These new FDCs willhelp the countries which arehardest hit by the AIDS epidemicto provide easy-to-take AIDSmedicines to the people who needthem most urgently.”
Médecins Sans Frontières iscurrently providing ARV treatmentto more than 11 000 peopleliving with HIV/AIDS in over 20countries. It is a strong advocateof triple-FDCs and comments that,“Compared to ARV drugs used asseparate products, triple-FDCshave clear advantages, such asease of use, reduced risk of drugresistance, competitive prices andthe easing of pressure on thesupply chain.”
1Directly observed treatment, short-course.
Further information:Richard Laing — [email protected]
PHO
TO: I
rene
R L
engu
i/L’I
VC
om
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 20

Rational U
se
“Until now, surveillance workaimed at understanding and tack-ling antimicrobial resistance(AMR) was carried out largely atnational level, with little local inputor feedback. The new approachbeing developed by WHO, is togather local data for localaction,” explains Dr KathleenHolloway, medical officer with thePolicy, Access and Rational Useteam at WHO Headquarters. Oneof Dr Holloway’s tasks is toencourage rational use of antibi-otics to help slow development ofAMR. But doing this demandsunderstanding of why and how itdevelops in the first place.
Dr Holloway continues, “Theproblem has been that littleevidence has so far beencollected as to which AMRinterventions are the most effectiveand feasible. Instead, attempts totackle AMR have tended to behospital-based, involving onlysurveillance by microbiologists.Samples analysis has remained atthe level of the sample (i.e.bacteria), and has been linked toneither patients nor type ofantimicrobial use. Antimicrobialsare used not just in hospitalsthough, but also widely withincommunities. So what is needed isa broad-based analysis.
“This in turn means using a multi-disciplinary approach, wherebyhealth professionals experiencedin rational use of medicines andantimicrobial resistance, work withanthropologists and sociologistsexperienced in working with com-munities. Only then can we workout the how and why of antimicro-bial use. After that, we canchoose interventions for contain-ing AMR that are likely to belocally appropriate and feasible.”
But developing countries often lackmultidisciplinary capacity. Dr Holloway has therefore assem-bled a team of researchers, and issupporting five pilot projects inIndia and South Africa, to encour-age its development. Based aroundlocal institutions, the projects arehelping experts of different disci-plines to pool their expertise to col-lect a wide variety of data on AMRand antibiotic use. The projectshave gathered one year’s worth ofdata from all levels of the healthcare system, both public and pri-vate. These data will be used toformulate local action plans.
Problems and progress
Each project experienceddifficulties in getting started,including problems in creating amultidisciplinary team, insufficientsample size of patients, logisticalproblems in collecting medicinesuse data and difficulties inperforming adequate dataanalysis. That said, at everyproject site, project participantshave found project involvement tobe an invaluable learningexperience. ”Not only are wecreating a standard method formultidisciplinary research intoAMR — suitable for use in anycountry — but we are buildingunderstanding about how to doit,” comments Dr Holloway.Initial results from all projectsshow an association between highantimicrobial use and resistance,and significant over-use ofantimicrobials in the community.Alarmingly, some resultsdemonstrate that trends inincreasing use are associated withtrends in increasing resistance.
Phase II will broaden this pro-gramme of work, so as to identifyinterventions that can most
effectively slow resistance to treat-ment for HIV/AIDS, tuberculosis(TB) and malaria. Failure to do socould threaten achievement ofMillennium Development Goal 4— to reduce child mortality —and Goal 6 — to combatHIV/AIDS, malaria and other dis-eases. AMR could also undermineglobal initiatives such as 3 by 5,Roll Back Malaria and Stop TB, aswell as national efforts to tackleinfectious diseases.
In describing the project hesupervises in Vellore, India, Dr Kurien Thomas, Professor ofMedicine at the Christian MedicalCollege, comments that workingwith WHO has, ”helped us todetermine our directions intackling AMR”. For his clinicalpharmacologist colleague, DrSujith Chandy, the WHO AMRproject has presented, “WHO —a wonderful holistic opportunity.The value of linking data on AMRand on medicines use at locallevel, of working in urban andrural areas and of bringingcolleagues from differentdisciplines within the hospital towork together on the project isproving to be a great experiencefor all involved.”
Further information:Kathleen Holloway — [email protected]
Local data for local action to fight antimicrobial resistance
Dr Kurien Thomas, a collaboratorwith WHO in gathering local datafor to tackle antimicrobialresistance
PHO
TO: W
HO
/Kat
h H
urst
21
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 21

Sources of extrabudgetary revenue received in2002–2003 (US$)
Funding sources for essentialdrugs and medicines policyactivities continue to be verydiverse. In 2002–2003, inaddition to regular budget funds— which accounted for 17% offunds available for the Departmentof Essential Drugs and MedicinesPolicy at WHO Headquarters —important extrabudgetarycontributions were received from anumber of governments (Australia,Denmark, Germany, Italy, Japan,Luxembourg, the Netherlands,Norway, Sweden, the UnitedKingdom and the USA).Extrabudgetary contributions alsocame from the RegionalGovernment of Lombardy (Italy),UNAIDS, the European MedicinesEvaluation Agency, and theNippon and RockefellerFoundations. Income was receivedtoo from fees paid bypharmaceutical manufacturers forthe assigning of InternationalNonproprietary Names (US$ 723 000). For 2004–2005,significant support is alsoanticipated from the EuropeanCommission, and the Bill andMelinda Gates Foundation.
Other human and financialsupport was leveraged byarranging co-sponsoring oftechnical meetings, includingworkshops and training seminars,contribution of technical expertiseto specific projects, and co-funding of technical publications.
Areas of experience
For the 2002–2003 biennium, the budget for essential drugs andmedicines policy activities atWHO Headquarters was US$ 34.9 million. Fundstransferred from WHOHeadquarters to supplementfunding for medicines activities incountries and regions amounted toUS$ 5.8 million. Funds were spentin line with the objectives andtargets of the WHO MedicinesStrategy 2000–2003. The largestshare of the funding supportedobjectives relating todevelopment, implementation andmonitoring of national medicinespolicies, safe use of medicines,and medicines regulation andquality assurance.
Into the future
Diversity of funding and in-kindsupport will be maintained.Indeed, it is absolutely crucialgiven the volatility of distributionof funds for health, and increasedcompetition for those funds. Lossof a source of funding could havea heavily negative impact on thedirection and implementation ofthe WHO Medicines Strategy for2004–2007.
Funding is still a concern,however. Growing countryrequirements for pharmaceuticaltechnical support — particularlyfollowing extended efforts toincrease access to medicines forHIV/AIDS, malaria andtuberculosis — mean that fundsavailable do not match need. Thusat the end of 2003, the shortfallfor the 2004–2005 biennium wascalculated at US$ 9.1 million forWHO Headquarters and US$ 6.8million for WHO regions andcountries. Should this shortfall notbe covered, a number of activitieswould have to be reduced inscope, delayed or cancelled.
Needless to say, given the need tomaximize funds for health,increased efforts are being madeto ensure timely liaison withdonors, and careful matching ofWHO and donor priorities andpolicies within the widerdevelopment context. Greaterpriority is also being given tomonitoring and evaluation ofmedicines activities at countrylevel, to help ensure that resourcesare applied where most neededand where they can be used tooptimal effect.
Further information:Jacqueline Sawyer —[email protected]
Where the money went: financial information 2002–2003
NetherlandsUnited Kingdom
NorwaySweden
DenmarkUSAID
UNAIDSAustralia
International Nonproprietary Names ProgrammeLuxembourg
ItalyJapan
European Medicines AgencyRegional Government of Lombardy (Italy)
GermanyRockefeller Foundation
Nippon FoundationNew Zealand
World BankInternational Federation of Pharmaceutical
Manufacturers AssociationsUS Pharmacopeia
Consiglio Nazionale delle Ricerche, Istituto di Ricerche sulla Popolazione e le Politiche Sociale, Rome, Italy
World Self-Medication Industry
4 654 2203 762 750
2 412 7301 806 834
1 312 941818 852800 121
735 180722 966701 341
562 788515 401
300 000239 473
201 852178 540157 80095 23881 00056 500
10 0007 656
5 650
22
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 22

Managem
ent
“People don’t want to hear howmany meetings WHO has held.They want to know whatdifference it has made. Havemedicine prices gone down? Hasavailability gone up? Are fewerunnecessary injections beinggiven? Is generic substitutionpossible? Is drug promotion beingmonitored? Are safety mechanismsin place? Is quality improving?”Dr Jonathan Quick is direct andforthright. Now, after seven yearsas head of the Department ofEssential Drugs and MedicinesPolicy at WHO Headquarters, heis returning to the USA-basedManagement Sciences for Health(MSH) — scene of his first-everstudent research project.
Dr Quick leaves a legacy: theWHO Medicines Strategy, whichwon the endorsement of all WHOMember States; the successfulmerger of the former ActionProgramme on Essential Drugsand the Division of DrugManagement and Policies; theprequalification project; and theestablishment of the GlobalMedicines Council.
“I am happy to have had theopportunity to define a singleWHO strategy for medicinesactivities. It provides a framework,with the core aims of affordability,accessibility, quality and safetyand rational use. In addition, itincorporates a practicalmonitoring programme, with eachaim underpinned by specific andmeasurable progress indicators,”says Dr Quick.
Analysing finance and public–private roles in medicines supply,he has encouraged WHOmedicines activities to focus on thebalance between knowledgecreation and implementation. Hehas also supported a modernizing
approach to the WHO Model Listof Essential Medicines, andbelieves that the Doha Declarationon the World TradeOrganization’s TRIPS1 Agreementand Public Health has moved inthe right direction, affirming mostof the points WHO tried to makein the controversial discussions of1998.
“Implementation of sensible pro-health policies in countries is nothappening anywhere to the extentit should. If we get it wrong now,it’s not just wrong for us, but forour children, and our children’schildren”, he adds.
Similar problems — diverse solutions
Dr Quick’s career began inBoston, USA. As a young medicalstudent in 1978 — with majors insociology and psychology — heembarked on an essentialmedicines research thesis. Itbecame an eight-month globalsurvey for MSH and WHO —whose Model List of EssentialMedicines was still in its infancy— and led to the definitiveManaging Drug Supply, publishedin 1981.
“The focus then was very much onthe nuts and bolts of procurement,distribution and use. I went toPeru, which had one of theearliest generics and rational useprogrammes, Guatemala becausethey had good management,Costa Rica for their social healthinsurance, and Norway, becauseof its tough logistics. Tanzaniawas on my list, also Sri Lanka,Malaysia and Papua NewGuinea. I had two weeks in eachcountry,” says Dr Quick.
1 Trade-Related Aspects of IntellectualProperty Rights.
“What struck me then — and stillstrikes me now — is how similarthe problems are and howcreatively diverse the solutions. Ithink one of the biggest barriers toprogress is just not learning fromwhat others have achieved.”
“Looking back, if you ask mewhere there has been significantand sustainable progress, it’swhere there is both strong politicalcommitment and sound technicalsupport. Although it is ironic thatmany people from the politicalculture and the technical cultureseem to miss the fact that theyneed each other to succeed,” hecontinues.
In terms of medicines, what willchallenge WHO in the nextdecade? The loss of medical andpharmacy leadership indeveloping countries, unfairfinancing of medicines and failingmanagement systems will all be critical issues according to Dr Quick.
Essentially qualified
23
Dr Jonathan Quick, who headedthe Department of Essential Drugsand Medicines Policy at WHOHeadquarters for seven years
PHO
TO: W
HO
/Pie
rre
Viro
t
WHO-EDM Report-Eng 27/10/04 2:59 pm Page 23

© World Health Organization 2004
All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, WorldHealth Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland or by emailing: [email protected]. Requests for
permission to reproduce or translate WHO publications should be emailed to: [email protected].
The designations employed and the presentation of the material in this publication do not imply the expression of any opinionwhatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its
authorities, or concerning the delimitation of its frontiers or boundaries.
The World Health Organization does not warrant that the information contained in this publication is complete and correct andshall not be liable for any damages incurred as a result of its use.
WH
O/E
DM
/2004.1
Art
Dir
ection:M
ark
Forr
est
Layout:
L’I
VCom
Sàrl
, M
org
es,
Switze
rland
WHO-EDM Report-Eng 27/10/04 2:58 pm Page b


















