What’s with this venous blood gas stuff
41
Click here to load reader
-
Upload
anthony-rossi-md -
Category
Documents
-
view
147 -
download
2
description
Use of goal directed therapy to improve outcomes in patients after congenital heart surgery.
Transcript of What’s with this venous blood gas stuff

Goal Oriented Therapy after Goal Oriented Therapy after Congenital Heart SurgeryCongenital Heart Surgery
ororWhat’s with this Venous Blood What’s with this Venous Blood
Gas Stuff?Gas Stuff?Anthony Rossi, MD
Director, Cardiac Intensive Care ProgramMiami Children’s Hospital
Miami, FL USA

BackgroundBackground• Monitoring oxygen delivery in the critically ill Monitoring oxygen delivery in the critically ill
pts after congenital heart surgery and pts after congenital heart surgery and developing treatment plans to optimize developing treatment plans to optimize oxygen delivery , is a logical approach to pt oxygen delivery , is a logical approach to pt management and has been shown to improve management and has been shown to improve outcome in a wide spectrum of critical illnessoutcome in a wide spectrum of critical illness
• Critically ill pts achieving a normal or Critically ill pts achieving a normal or supernormal level of oxygen delivery have supernormal level of oxygen delivery have lower mortality, less end organ damage, lower mortality, less end organ damage, lower morbidity and shorter hospital stayslower morbidity and shorter hospital stays

Oxygen Delivery=Oxygen Delivery=DODO22
• DODO22=Cardiac Index x Arterial Oxygen =Cardiac Index x Arterial Oxygen
Content (CaOContent (CaO2)2)

Indirect Indicators of Systemic DOIndirect Indicators of Systemic DO22
• pHpH
• HCOHCO33
• BEBE
• SVOSVO22 (AVO2, OER) (AVO2, OER)
• COCO2 2 (SvCO (SvCO22-SaCO-SaCO22))
• lactatelactate

Common Cardiac Surgical Common Cardiac Surgical ProceduresProcedures
• Arterial switch operationArterial switch operation• Repair of tetralogy of FallotRepair of tetralogy of Fallot• VSD closureVSD closure• ASD closureASD closure• AVC repairAVC repair• Rastelli operationRastelli operation• Norwood operationNorwood operation• Bi-GlennBi-Glenn• FontanFontan• Repair IAARepair IAA• BTSBTS• Central shuntCentral shunt• RossRoss• MV replacementMV replacement• AV replacementAV replacement• Aortic ValvotomyAortic Valvotomy• KonnoKonno• Ross-KonnoRoss-Konno• Repair TAPVCRepair TAPVC• Repair coarctationRepair coarctation• Repair DORVRepair DORV• SenningSenning• MustardMustard• Double switchDouble switch

Single Goal of PO CareSingle Goal of PO Care
• Maintain optimal tissue oxygen deliveryMaintain optimal tissue oxygen delivery

Goal of Post-Op CareGoal of Post-Op Care• Maintain Optimal Tissue OxygenationMaintain Optimal Tissue Oxygenation
– globalglobal
– regionalregional• splanchnic - the correction of splanchnic - the correction of
unrecognized perfusion defects seems unrecognized perfusion defects seems to be a desirable addition to the to be a desirable addition to the standard clinical management of standard clinical management of critically ill patients with regard to critically ill patients with regard to preservation of organ function*preservation of organ function*
• coronarycoronary* J.-L. Vincent. Intensive Care Med (1996) 22:3* J.-L. Vincent. Intensive Care Med (1996) 22:3

Determinants of Tissue Determinants of Tissue OxygenationOxygenation
• C.O.C.O.
• HbHb
• SaOSaO22
• OO22 Demands (oxygen consumption: VO Demands (oxygen consumption: VO22))

• HR, BP, central filling pressuresHR, BP, central filling pressures• perfusionperfusion
– cap refillcap refill– extremity tempextremity temp
• urine outputurine output• arterial blood gas (pH, bicarb, BE)arterial blood gas (pH, bicarb, BE)• blood lactateblood lactate
Hemodynamic MonitoringHemodynamic Monitoring: All mechanisms of : All mechanisms of hemodynamic monitoring are used to hemodynamic monitoring are used to estimateestimate the the relationship of oxygen delivery to oxygen consumption. This relationship of oxygen delivery to oxygen consumption. This relationship might be considered an indicator of relationship might be considered an indicator of cardiovascular well-being. Traditional hemodynamic cardiovascular well-being. Traditional hemodynamic parameters include:parameters include:

Systemic Venous Oxygen Saturation Systemic Venous Oxygen Saturation (SvO(SvO22) Monitoring: ) Monitoring:
• defines the relationship of DOdefines the relationship of DO22/VO/VO22
• estimate oxygen delivery (AVOestimate oxygen delivery (AVO22 difference, OER: oxygen extraction difference, OER: oxygen extraction ratio)ratio)
• estimate cardiac output trendsestimate cardiac output trends• estimate Qp/Qs in single ventricle ptsestimate Qp/Qs in single ventricle pts
– SaOSaO22 poor indicator of Qp/Qs (low SvO poor indicator of Qp/Qs (low SvO22 will decrease SaOwill decrease SaO22 in face of large Qp/Qs) in face of large Qp/Qs)

Causes of Low SVOCauses of Low SVO22
• SVOSVO22 = SaO = SaO22 – (VO – (VO22/Q x Hb x 13)/Q x Hb x 13)
– HypoxemiaHypoxemia– Increased metabolic rateIncreased metabolic rate– Low cardiac outputLow cardiac output– anemiaanemia
1
1 2
2
3
3 4
4

OER: Oxygen Extraction RatioOER: Oxygen Extraction Ratio• OER = OOER = O22 consumption/O consumption/O22 delivery delivery
• OER = OER = OO22 Sat art - O Sat art - O22 Sat sys ven Sat sys ven
OO22 Sat art Sat art
• normal relationship of 5/1 DOnormal relationship of 5/1 DO22/VO/VO22
• normal OER = 0.2normal OER = 0.2• Omega is the reciprocal of the OER (normal value is Omega is the reciprocal of the OER (normal value is
5)5)• higher omega and lower OER are associated with an higher omega and lower OER are associated with an
improved relationship of DOimproved relationship of DO22 to VO to VO22..

Relation of DORelation of DO22 to VO to VO22: Under normal conditions, the cardiovascular : Under normal conditions, the cardiovascular
system delivers approximately 5 times as much oxygen as the body uses. system delivers approximately 5 times as much oxygen as the body uses. This would be reflected by an SvOThis would be reflected by an SvO22 of 80%, an A-VO of 80%, an A-VO22 difference of 20 or an difference of 20 or an
oxygen extraction ratio (OER) of 0.2. As oxygen delivery (DOoxygen extraction ratio (OER) of 0.2. As oxygen delivery (DO22) decreases, ) decreases,
SvOSvO22 decreases, the A-VO decreases, the A-VO22 difference increases and the OER increases. difference increases and the OER increases.
Oxygen consumption (VOOxygen consumption (VO22) should not be affected by DO) should not be affected by DO22. At the . At the critical critical
point of DOpoint of DO22, further decreases in DO, further decreases in DO22 are associated with a pathologic are associated with a pathologic
decrease in VOdecrease in VO22. This pathologic relationship is associated with increased . This pathologic relationship is associated with increased
lactate production.lactate production.
DODO22
VOVO22
critical point of DOcritical point of DO22
(VO(VO22 , lactate ) , lactate )
0.2 OER0.2 OER0.50.5**
** Decreasing CV ReserveDecreasing CV Reserve

Relation of DORelation of DO22 to VO to VO22: The graph now shows how decreasing cardiac : The graph now shows how decreasing cardiac
output (or more appropriately DOoutput (or more appropriately DO22) is associated with an SvO) is associated with an SvO22 which drops which drops
from 80 to 50 while the AVOfrom 80 to 50 while the AVO22 difference increases from 20 to 50. This difference increases from 20 to 50. This
graphic demonstration of the pathologic relationship of VOgraphic demonstration of the pathologic relationship of VO22 to DO to DO22 will look will look
somewhat different under various pathologic conditions, such as sepsis. somewhat different under various pathologic conditions, such as sepsis. The principles are similar however. Also, remember that the SvOThe principles are similar however. Also, remember that the SvO22 is the is the
sumsum of all systemic venous return. Lactate elevation does not correlate of all systemic venous return. Lactate elevation does not correlate
precisely with SVOprecisely with SVO22..
VOVO22
critical point of DOcritical point of DO22
(VO(VO22 , lactate ) , lactate )
SVOSVO22=80=80
AVOAVO22=20=20SVOSVO22=50=50
AVOAVO22=50=50
**
** Decreasing CV ReserveDecreasing CV ReserveExcellent COExcellent COBad COBad CO

AVOAVO22 difference vs. OER difference vs. OER
• AVOAVO22 diff of 25 in pt with SaO diff of 25 in pt with SaO22 100% 100%
– OER = 25/100 = 0.25OER = 25/100 = 0.25
– DODO22/VO/VO22 = 4/1 ( = 4/1 (normalnormal))
• AVOAVO22 diff of 25 in pt with SaO diff of 25 in pt with SaO22 65% 65%
– OER = 25/65 = 0.38OER = 25/65 = 0.38
– DODO22/VO/VO22 = 2.5/1 ( = 2.5/1 (2/1 = critical point of DO2/1 = critical point of DO22!!))
– This pt is living on the edge!This pt is living on the edge!

Rossi, Seiden, Gross, et al. Annals Thorac Surg. 1999Rossi, Seiden, Gross, et al. Annals Thorac Surg. 1999
0
0.1
0.2
0.3
0.4
0.5
0.6
Admit 6 hours 12hours
18hours
24hours
time after admission to CICU
OE
R Survivors
Non Survivors
*
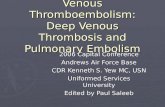
OER in Infants following Heart SurgeryOER in Infants following Heart Surgery: This study showed that in infants : This study showed that in infants undergoing congenital heart surgery, survivors and nonsurvivors had similar undergoing congenital heart surgery, survivors and nonsurvivors had similar OER, or indices of cardiovascular well-being, on admission to the CICU and OER, or indices of cardiovascular well-being, on admission to the CICU and at 24 hrs after admission. At 6 hours after admission, nonsurvivors showed a at 24 hrs after admission. At 6 hours after admission, nonsurvivors showed a severe derangement in the DOsevere derangement in the DO22/VO/VO2 2 (either decreased DO(either decreased DO22 or increased or increased
VOVO22). It was presumed that the oxygen debt in these patients was so great ). It was presumed that the oxygen debt in these patients was so great
at 6 hours, that improvement in DOat 6 hours, that improvement in DO22 thereafter was not associated with thereafter was not associated with
survival.survival.

Base Excess
-15 -10 -5 0 5 10 15
Ser
um
Lac
tate
0
5
10
15
20
25
2.2
Base Excess vs Blood LactateBase Excess vs Blood Lactate
r2 = 0.27
elevated lactateelevated lactate+ base excess+ base excess
elevated lactateelevated lactate- base excess- base excess
normal lactatenormal lactate+ base excess+ base excess
normal lactatenormal lactate- base excess- base excess
2.2
lact
ate
10
5 10-10 -5Base excess
The base excess does not predict blood lactate levels. Pts with a positive base excess can have severe hyperlactatemia.

Lactate Monitoring after CHSLactate Monitoring after CHS: A number of studies have shown : A number of studies have shown the predictive value of blood lactate levels after CHS. the predictive value of blood lactate levels after CHS.
Infants after cardiac surgeryInfants after cardiac surgery• Initial lactate > 7mmol/l - mortality 55%Initial lactate > 7mmol/l - mortality 55%• Maximum lactate > 9mmol/l - mortality 86% (Chefitz et al. 1997)Maximum lactate > 9mmol/l - mortality 86% (Chefitz et al. 1997)
Children after cardiac surgeryChildren after cardiac surgery
Initial lactate > 4.2 mmol/l - mortality 100%Initial lactate > 4.2 mmol/l - mortality 100%(Siegel et al.1996) (Siegel et al.1996) Initial lactate > 4.5 mmol/l - mortality 79%Initial lactate > 4.5 mmol/l - mortality 79%(Hatherhill et al.1997)(Hatherhill et al.1997)
Serial Lactate Measurements Predict Outcomes after CHSSerial Lactate Measurements Predict Outcomes after CHS Charpie et al. 2000Charpie et al. 2000

Speculation: In the summer of 2001, the cardiac surgical program began to wonder…..
• If lactate is useful in predicting outcomes in pts after If lactate is useful in predicting outcomes in pts after CHS could lactate be used as a target goal for medical CHS could lactate be used as a target goal for medical management in this pt population?management in this pt population?
• Can GDT be applied to pts after CHS?Can GDT be applied to pts after CHS?

July 2001: The Premise
• Establish near patient testing of routine critical care lab values with rapid turn-around-time– Clinician can react quickly to changing physiologic conditions
• Establish blood lactate measurement as objective indicator of oxygen debt
• Establish clinical guidelines which are directed at normalizing blood lactate levels (thereby minimizing oxygen debt)
• The combination of the above would increase survival after congenital heart surgery

Initial Lactate > 2.2Initial Lactate > 2.2
No ChangeNo Change Increase in LactateIncrease in Lactate Decrease in LactateDecrease in Lactate
< 5< 5 > 5> 5
Repeat in 4 hrsRepeat in 4 hrs Escalate Medical RxEscalate Medical Rx
Escalate Medical RxEscalate Medical Rx
Repeat in 4 hrsRepeat in 4 hrs
Repeat in 4 hrsRepeat in 4 hrs
Repeat Q 4 HrsRepeat Q 4 Hrs
LactateLactate > > 10 10
CPSCPSLactate < 5Lactate < 5 Lactate 5-10Lactate 5-10
Escalate Medical RxEscalate Medical RxRepeat in 4 hrsRepeat in 4 hrs
Repeat q4hrs x 4
CPS = Cardiopulmonary SupportCPS = Cardiopulmonary Support
Consider
Lactate Management Protocol

MCH Goal Directed Lactate Management Strategy in Postoperative Patients
Lactate Normal or
DiminishingNo Changes

MCH Goal Directed Lactate Management Strategy in Postoperative Patients
Lactate ElevatedOr
Rising
pH normal?
pCO2 appropriate?
Hb appropriate?
CVP appropriate?
HR appropriate?
BP appropriate?
Increase Oxygen DeliveryIncrease Oxygen Delivery

Patients Undergoing CHS at MCH from 6/95-12/07
ERAERA AgeAge(Range)(Range)MedianMedian
WeightWeight(Range)(Range)MedianMedian
Total Total PtsPts
< 1 mth< 1 mth > 1 mth> 1 mth
6/95-6/95-6/016/01
(0-72 yrs)(0-72 yrs)311 d311 d
(0.5-127 kg)(0.5-127 kg)7.9 kg7.9 kg 16561656 321321 13351335
7/01-7/01-12/0712/07 (0-72 yrs)(0-72 yrs)
166 d166 dP < 0.01P < 0.01
(0.4-114 kg)(0.4-114 kg)5.8 kg5.8 kgP < 0.01P < 0.01
18101810 445445 13651365
Adapted and updated from: Point of Care Testing and Goal Directed Therapy Improve Outcomes after Congenital Heart Surgery. Rossi et al. Intensive Care Med. 2005
Adapted and updated from: Point of Care Testing and Goal Directed Therapy Improve Outcomes after Congenital Heart Surgery. Rossi et al. Intensive Care Med. 2005

Total Oxygen Debt is Related to Outcome: The concept of “lactime” was described by Bakker and colleagues in 1999. The peak lactate alone may not be the best predictor of mortality in critical illness, the total area under the curve that one spends with an elevated lactate, or in oxygen debt, may be a better predictor.
0
2
4
6
8
10
12
admit 6 hrs 12
hrs
18
hrs
24
hrs
lact
ate
Pt 1
Pt 2
“lactime” Bakker, Am J Surg 1996

In a study of lactate patterns of children after congenital heart surgery, peak lactate level correlated with mortality. Interestingly, earlier studies of critically ill adults in surgical ICUs showed that mortality was almost 100% in that population if the blood lactate level was above 10. These children routinely survived with lactate levels above 10 and occasionally survived with lactate levels greater than 20. Unpublished data from the Mt. Sinai Medical Center.
1.6
11.5
44.4
66.7
0
10
20
30
40
50
60
70
80
<5 5-10 10-20 > 20
peak lactate
% m
ort
alit
y

Lactate on admission to the CICU and peak lactate correlated with Lactate on admission to the CICU and peak lactate correlated with outcome in our study. The time it took to reach the peak lactate outcome in our study. The time it took to reach the peak lactate level was also higher in nonsurvivors. So pts who die not only have level was also higher in nonsurvivors. So pts who die not only have higher levels of lactate but also take longer to peak and spend more higher levels of lactate but also take longer to peak and spend more time in “oxygen debt.”time in “oxygen debt.”
9.9
15.3
8.16.7
8.4
3.1
0
2
4
6
8
10
12
14
16
18
blo
od
lac
tate
or
tim
e in
ho
urs
NONSURVIVORS SURVIVORS
Peak lactate (mmol/l)Peak lactate (mmol/l) Time to peak lactate Time to peak lactate (hours)(hours)
P<0.001P<0.001 P<0.001
Admission lactate Admission lactate (mmol/l)(mmol/l)
N=41

Lactate Monitoring in Pts Who Survive: Individual pts who survive congenital Lactate Monitoring in Pts Who Survive: Individual pts who survive congenital heart surgery can have differing lactate curves. Pt number 1 is admitted after a heart surgery can have differing lactate curves. Pt number 1 is admitted after a high risk operation with a markedly elevated lactate that returns to baseline fairly high risk operation with a markedly elevated lactate that returns to baseline fairly rapidly with aggressive medical therapy. Pt 2 has a more delayed response to rapidly with aggressive medical therapy. Pt 2 has a more delayed response to medical therapy but ultmately improves the DOmedical therapy but ultmately improves the DO22/VO/VO22 relationship and survives. relationship and survives.
Low risk cardaic pts exhibit only mild elevations in blood lactate (pt 3).Low risk cardaic pts exhibit only mild elevations in blood lactate (pt 3).
3
2 2 21.5
5
4 4
3
2
9
7
5 5
4
0
1
2
3
4
5
6
7
8
9
10
ADMIT 6 HR 12 HR 18 HR 24 HR
PT1
PT2
PT3

0
2
4
6
8
10
0 10 20 30 40 50
hours postop
lact
ate(
mm
ol/L
)
Category 1 MeanCategory 2 MeanCategory 3 MeanCategory 4 Mean
Category 1-4 Survivors (excluding CPS patients)
n=127
Patterns of Lactate Values after Congenital Heart Surgery and Timing of Cardiopulmonary Support. Robert L. Hannan, MD * , Marion A. Ybarra, BS, Jeffrey A. White, MS, Jorge W. Ojito, CCP, Anthony F. Rossi, MD, Redmond P. Burke, MD Ann Thorac Surg 2005;80:1468-1474

y = 4E-05x3 - 0.0018x2 - 0.0197x + 2.5738
0
2
4
6
8
10
0 10 20 30 40 50
hours postop
lacta
t (m
mo
l/L
)
Category 1-4 Survivors (excluding CPS patients)
n=127
Patterns of Lactate Values after Congenital Heart Surgery and Timing of Cardiopulmonary Support. Robert L. Hannan, MD * , Marion A. Ybarra, BS, Jeffrey A. White, MS, Jorge W. Ojito, CCP, Anthony F. Rossi, MD, Redmond P. Burke, MD Ann Thorac Surg 2005;80:1468-1474

y = 0.0002x3 - 0.0176x2 + 0.3418x + 3.0448
y = 4E-05x3 - 0.0018x2 - 0.0197x + 2.5738
0
1
2
3
4
5
6
7
8
0 10 20 30 40 50
hours postop
lact
ate
(mm
ol/L
)Category 1-4Category 6
Survivors Excluding CPS Patients
Patterns of Lactate Values after Congenital Heart Surgery and Timing of Cardiopulmonary Support. Robert L. Hannan, MD * , Marion A. Ybarra, BS, Jeffrey A. White, MS, Jorge W. Ojito, CCP, Anthony F. Rossi, MD, Redmond P. Burke, MD Ann Thorac Surg 2005;80:1468-1474

Non Survivors (excluding CPS Patients)
0
2
4
6
8
10
12
14
16
18
20
0 10 20 30 40 50
hours postop
lact
ate
(mm
ol/
L)
Patterns of Lactate Values after Congenital Heart Surgery and Timing of Cardiopulmonary Support. Robert L. Hannan, MD * , Marion A. Ybarra, BS, Jeffrey A. White, MS, Jorge W. Ojito, CCP, Anthony F. Rossi, MD, Redmond P. Burke, MD Ann Thorac Surg 2005;80:1468-1474

Lactate Monitoring in Pts Who Die: Pt 1 exhibits a typical lactate pattern of a pt Lactate Monitoring in Pts Who Die: Pt 1 exhibits a typical lactate pattern of a pt who dies after congenital heart surgery. The lactate on admission is high and who dies after congenital heart surgery. The lactate on admission is high and despite attempts to improve the DO2/VO2 relation, lactate continues to rise. despite attempts to improve the DO2/VO2 relation, lactate continues to rise. Rarely, a pt will be admitted after surgery with a low lactate that rises despite Rarely, a pt will be admitted after surgery with a low lactate that rises despite therapy and dies. Some pts may “honeymoon” and show deterioration later therapy and dies. Some pts may “honeymoon” and show deterioration later (pt 3). (pt 3). Serial lactate monitoring is valuable even in pts who are admitted and appear clinically well.
11
8
101111
12
5
77
46
322
3
0
2
4
6
8
10
12
14
ADMIT 6 HR 12 HR 18 HR 24 HR
PT 1PT 2PT 3

Venous Blood Gas MonitoringVenous Blood Gas Monitoring• VBG monitoring allows you to calculate the a-vCOVBG monitoring allows you to calculate the a-vCO22
(the difference b/w the arterial and venous pCO(the difference b/w the arterial and venous pCO22) and ) and a-vpH (the difference b/w the arterial and venous pH) a-vpH (the difference b/w the arterial and venous pH) gradients in the critically illgradients in the critically ill
• a-vCOa-vCO22 is directly related to Cardiac Output is directly related to Cardiac Output– This difference, also known as the COThis difference, also known as the CO22 GAP, is a better GAP, is a better
indicator of cardiac output than the a-vOindicator of cardiac output than the a-vO22 difference difference
• The larger the a-vCOThe larger the a-vCO2 2 gradient, the lower the cardiac gradient, the lower the cardiac outputoutput
• pH gradient has been used to access pts in shockpH gradient has been used to access pts in shock

Effect of Cardiac Output on Effect of Cardiac Output on vCO2vCO2
CELLCELLCO2CO2
aCO2=40aCO2=40
vCO2=45vCO2=45
CELLCELLCO2CO2
aCO2=40aCO2=40
vCO2=52vCO2=52
Normal CONormal CO Low COLow CO

AVCO2, AV pH, Lactate and AVCO2, AV pH, Lactate and OER in Survivors After Heart OER in Survivors After Heart
SurgerySurgery
2
3
4
5
6
7
8
9
admit 6 hours 12 hours 18 hours 24 hours
AV
CO
2, A
VpH
, Lac
tate
0.2
0.25
0.3
0.35
0.4
0.45
OER
lactate
AVCO2
AVpH
OER

Objective Indicators of DO2 in Varying Physiologic States
VpHVpH SvO2SvO2 AVO2AVO2 O2 EFO2 EF OEROER AVCO2AVCO2 LactateLactate
Normal CONormal CO <0.05<0.05 75%75% 25%25% 44 0.250.25 <7<7 <2.2<2.2
Decreased Decreased COCO
>0.05>0.05 66%66% 33%33% 33 0.330.33 8-128-12 <2.2<2.2
Critical Critical Point of Point of DO2DO2
>0.05>0.05 50%50% 50%50% 22 0.500.50 >12>12 >2.2>2.2

VBG/ABGVBG/ABGVBGpH/CO2/SvO2
ABGpH/CO2/SaO2
A-V pH/
A-V CO2/
A-V O2
Normal 7.35/45/757.35/45/75 7.40/40/1007.40/40/100 0.05/5/250.05/5/25
Resp Acidosis
7.20/70/657.20/70/65 7.25/65/907.25/65/90 0.05/5/250.05/5/25
Low CO 7.15/70/507.15/70/50 7.30/40/1007.30/40/100 0.15/30/500.15/30/50

ConclusionsConclusions• Optimizing DOOptimizing DO22 is a goal oriented task and it’s rewards are is a goal oriented task and it’s rewards are
rapidly appreciated. rapidly appreciated. • Goal oriented medical therapy may be directed at a number of Goal oriented medical therapy may be directed at a number of
objective parameters after congenital heart surgery, but SvOobjective parameters after congenital heart surgery, but SvO22 and blood lactate have shown the most promise.and blood lactate have shown the most promise.
• SvO2 and Lactate monitoring are complimentary techniques to SvO2 and Lactate monitoring are complimentary techniques to evaluate cardiovascular well-being.evaluate cardiovascular well-being.
• The currently available technologies allow SvO2 monitoring to The currently available technologies allow SvO2 monitoring to occur continuously and in real-time. Lactate monitoring is occur continuously and in real-time. Lactate monitoring is intermittent. intermittent.
• Small victories are critical in the psyche of all involved in the Small victories are critical in the psyche of all involved in the care of the most critically ill.care of the most critically ill.
• Objective indicators of cardiovascular well-being must be Objective indicators of cardiovascular well-being must be accurate, reproducible and available rapidly to be useful.accurate, reproducible and available rapidly to be useful.

ConclusionsConclusions• VBG (a-vCOVBG (a-vCO22 and a-vpH) and SvO and a-vpH) and SvO22 allow the clinician to rapidly assess if a new allow the clinician to rapidly assess if a new
treatment is having it’s desired effect (increasing DOtreatment is having it’s desired effect (increasing DO22 or improving DO or improving DO22 / VO / VO22).).• SvOSvO22 monitoring has been proven to save the lives of critically ill pts. monitoring has been proven to save the lives of critically ill pts.• The highest risk pts, such as those who undergo the Norwood operation seem to The highest risk pts, such as those who undergo the Norwood operation seem to
benefit most.benefit most.• Lactate monitoring tells the clinician how well the patient has been doing over an Lactate monitoring tells the clinician how well the patient has been doing over an
extended period of time, it is evidence of end-organ injury.extended period of time, it is evidence of end-organ injury.• Blood lactate levels can change very rapidly with changes in DOBlood lactate levels can change very rapidly with changes in DO22/VO/VO22. Lactate . Lactate
levels do not show significant “lag-times.” Lactate wash-out as a cause of levels do not show significant “lag-times.” Lactate wash-out as a cause of persistently elevated lactate levels probably does not occur frequently in the critically persistently elevated lactate levels probably does not occur frequently in the critically ill. A more likely reason for persistence of an elevated lactate is continued tissue ill. A more likely reason for persistence of an elevated lactate is continued tissue hypoxia. If the lactate remains high, the patient is not better!hypoxia. If the lactate remains high, the patient is not better!
• Increase in blood lactate does not necessarily mean tissue oxygenation is poor Increase in blood lactate does not necessarily mean tissue oxygenation is poor (inability to metabolize lactate appropriately occurs in liver failure), however, (inability to metabolize lactate appropriately occurs in liver failure), however, whatever the cause of hyperlactatemia, it is always associated with increased whatever the cause of hyperlactatemia, it is always associated with increased morbidity and mortality.morbidity and mortality.

Who’s Minding the Store?Who’s Minding the Store?• Subjective indicators of cardiovascular well-being Subjective indicators of cardiovascular well-being
must be complemented by objective indicatorsmust be complemented by objective indicators• Objective indicators are necessary since the level of Objective indicators are necessary since the level of
experience of the person responsible for the care of experience of the person responsible for the care of the critically ill patient after heart surgery varies the critically ill patient after heart surgery varies significantly, even within ICUs.significantly, even within ICUs.
• It has been show that even experienced clinicians It has been show that even experienced clinicians can misjudge a pts overall cardiovascular well-being can misjudge a pts overall cardiovascular well-being (blood lactate level or SvO(blood lactate level or SvO22).).
• Objective indicators must be accurate, reproducible Objective indicators must be accurate, reproducible and available rapidly to be useful.and available rapidly to be useful.