What Is the Optimal Place for Heart Failure Treatment and Care: Home or Hospital?
5
SELF-CARE AND HEALTH OUTCOMES (T JAARSMA, SECTION EDITOR) What Is the Optimal Place for Heart Failure Treatment and Care: Home or Hospital? Simon Stewart Published online: 25 June 2013 # Springer Science+Business Media New York 2013 Abstract This article examines the role of home versus hospital clinic-based management of heart failure to achieve the best outcomes for affected individuals and their carer/families. It also considers the role of remote manage- ment strategies. Overall, the evidence in favor of home-based strategies is quite compelling. However, persistently high levels of heart-failure-related morbidity and mortality, com- bined with inconsistent application of key components of care, mandate greater efforts to develop more standardized and cost-effective forms of heart failure support services. Keywords Heart failure . Disease management programs . Home-based . Specialist outpatient clinics Introduction In a timely reminder of an enduring epidemic of heart failure (HF) within our aging populations, the American Heart Association has estimated that by 2030 there will be >8 million people with HF and that total related expenditure will be $70 billion ($160 billion if one accounts for all costs of treating such patients) [1•] These data mirror U.K.-based estimates of a rising number of HF cases [2] and increasing costs [3] in the 21st century. Recently, published data from Sweden clearly support the supposition that the major cost component of health-care expenditure related to HF is hos- pital care—predominantly, inpatient care [4]. Moreover, it is very clear that HF, particularly when combined with acute myocardial infarction, one of its major drivers, rivals and even dwarfs in some cases the major forms of cancer (in both men and women) in respect to total number of hospital admissions, subsequent case fatalities, and life-years lost as a consequence [4]. This article articulates the reasons why home is probably best for HF care and support, while firmly stressing the caveat that the hospital remains the best place for advanced and specialist support of acute clinical instability (including most forms of acute decompensated HF), and the role of “hospital in the home” strategies in replacing acute hospital care of patients with acute HF being still in an evolutionary stage (at least from a global perspective). Historical Development of HF Management Programs to Reduce Morbidity and Prolong Survival Predominantly nurse-led, but still multidisciplinary, HF management programs (MPs) applied in different settings now form part of the gold standard management of the syndrome as advocated by such influential bodies as the European Society of Cardiology [5]. Following the publica- tion of seminal randomized controlled trials undertaken in the 1990s [6–9], meta-analyses confirmed the benefits of HF-MPs in reducing readmission rates, improving quality of life, reducing costs, and prolonging survival, relative to usual care [10]. A more detailed analysis of some of the key trials con- tributing to the literature demonstrated that a face-to-face approach applied within a multidisciplinary framework ap- pears to be a nonnegotiable component of HF-MP applica- tion wherever possible [11]. More recently, the role of brain natriuretic peptide (BNP) monitoring in detecting clinical instability and/or the need for treatment up-titration of treat- ment (particularly in relatively younger individuals—i.e., those <75 years of age) has been the subject of increasing debate [12, 13]. Regardless of the specific form of HF-MP to be applied, translation into practice is often imperfect, due to selective S. Stewart (*) NHMRC Centre of Research Excellence to Reduce Inequality in Heart Disease & Head, Preventative Health, Baker IDI Heart and Diabetes Institute, PO Box 6492, St Kilda Rd Central, Melbourne, Victoria 8008, Australia e-mail: [email protected] Curr Heart Fail Rep (2013) 10:227–231 DOI 10.1007/s11897-013-0144-x
-
Upload
simon-stewart -
Category
Documents
-
view
212 -
download
0
Transcript of What Is the Optimal Place for Heart Failure Treatment and Care: Home or Hospital?

SELF-CARE AND HEALTH OUTCOMES (T JAARSMA, SECTION EDITOR)
What Is the Optimal Place for Heart Failure Treatmentand Care: Home or Hospital?
Simon Stewart
Published online: 25 June 2013# Springer Science+Business Media New York 2013
Abstract This article examines the role of home versushospital clinic-based management of heart failure toachieve the best outcomes for affected individuals and theircarer/families. It also considers the role of remote manage-ment strategies. Overall, the evidence in favor of home-basedstrategies is quite compelling. However, persistently highlevels of heart-failure-related morbidity and mortality, com-binedwith inconsistent application of key components of care,mandate greater efforts to develop more standardized andcost-effective forms of heart failure support services.
Keywords Heart failure . Disease management programs .
Home-based . Specialist outpatient clinics
Introduction
In a timely reminder of an enduring epidemic of heart failure(HF) within our aging populations, the American HeartAssociation has estimated that by 2030 there will be >8million people with HF and that total related expenditurewill be $70 billion ($160 billion if one accounts for all costsof treating such patients) [1•] These data mirror U.K.-basedestimates of a rising number of HF cases [2] and increasingcosts [3] in the 21st century. Recently, published data fromSweden clearly support the supposition that the major costcomponent of health-care expenditure related to HF is hos-pital care—predominantly, inpatient care [4]. Moreover, it isvery clear that HF, particularly when combined with acutemyocardial infarction, one of its major drivers, rivals andeven dwarfs in some cases the major forms of cancer (in both
men and women) in respect to total number of hospitaladmissions, subsequent case fatalities, and life-years lost asa consequence [4]. This article articulates the reasons whyhome is probably best for HF care and support, while firmlystressing the caveat that the hospital remains the best placefor advanced and specialist support of acute clinical instability(including most forms of acute decompensated HF), and therole of “hospital in the home” strategies in replacing acutehospital care of patients with acute HF being still in anevolutionary stage (at least from a global perspective).
Historical Development of HF Management Programsto Reduce Morbidity and Prolong Survival
Predominantly nurse-led, but still multidisciplinary, HFmanagement programs (MPs) applied in different settingsnow form part of the gold standard management of thesyndrome as advocated by such influential bodies as theEuropean Society of Cardiology [5]. Following the publica-tion of seminal randomized controlled trials undertaken inthe 1990s [6–9], meta-analyses confirmed the benefits ofHF-MPs in reducing readmission rates, improving qualityof life, reducing costs, and prolonging survival, relative tousual care [10].
A more detailed analysis of some of the key trials con-tributing to the literature demonstrated that a face-to-faceapproach applied within a multidisciplinary framework ap-pears to be a nonnegotiable component of HF-MP applica-tion wherever possible [11]. More recently, the role of brainnatriuretic peptide (BNP) monitoring in detecting clinicalinstability and/or the need for treatment up-titration of treat-ment (particularly in relatively younger individuals—i.e.,those <75 years of age) has been the subject of increasingdebate [12, 13].
Regardless of the specific form of HF-MP to be applied,translation into practice is often imperfect, due to selective
S. Stewart (*)NHMRC Centre of Research Excellence to Reduce Inequalityin Heart Disease & Head, Preventative Health, Baker IDI Heart andDiabetes Institute, PO Box 6492, St Kilda Rd Central, Melbourne,Victoria 8008, Australiae-mail: [email protected]
Curr Heart Fail Rep (2013) 10:227–231DOI 10.1007/s11897-013-0144-x

application of key components integral to effective HF man-agement [14]. Moreover, debate about the best approach toHF management continues [15]. As such, there is increasingawareness of the need for rigorous pragmatic trials of differ-ent forms of HF-MP to determine the most cost-effectivemodality and, indeed, the components of management (asshown in Table 1) needed to address persistently high levelsof HF-related morbidity and mortality.
It is important to note that the notion of merely providingsupport to the patient during an acute hospitalization toensure that he or she is fully prepared to optimally managehis or her HF posthospitalization has long disappeared fromthe lexicon of HF-MPs for the following reasons:
& HF patients (like most patients) are typically under se-vere physiological and psychological stress that impairstheir ability to comprehend and understand complexinstructions.
& Levels of cognitive impairment and depression are usu-ally high.
& Management of acute versus chronic forms of HF ismarkedly different.
& Most HF admissions involve a complex set of circum-stances and conditions that are difficult to unravel in theacute care setting.
Most effective forms of HF management, therefore, whilenot ignoring the importance of ensuring that the HF patient isclinically stable at the point of discharge, are applied in thepostdischarge setting. Each of the potential modes of HF-MPdelivery has strengths and weaknesses. However, it could beargued that home-based programs of care offer notable ad-vantages, as compared with all other current alternatives,noting that none are mutually exclusive but that funded pro-grams tend to favor one form of delivery over the other (evenif there are potentially important differences in outcome).
Such potential advantages of a home-based program includethe following:
& It represents a face-to-face form of HF-MP.& By its very nature, it represents a more holistic (rather
than HF-specific) form of management.& Visiting patients and carers in the home alters the typical
dynamics of the health-care team and patient interaction,empowering the latter to take more control.
& Patients and carers spend most of their time at home, andit is there that the positive and negative factors likely toinfluence health behaviors and outcomes will be foundand best understood.
A recent review of HF management in the home byJaarsma and colleagues [16] assessed 70 relevant researchreports according to five key components of care: (1) involve-ment of a multidisciplinary team, (2) continuity of care andapplication of care plans accordingly (3) optimized treatmentaccording to expert guidelines, (4) application of educationalcounseling for patients and their family/caregivers, and (5)provision for increased accessibility to care. Perhaps disap-pointingly, they found that just under one third (20 studies,29 %) applied all five components of care [16].
The Which Heart Failure Intervention Is MostCost-Effective and Consumer Friendly in ReducingHospital Care (WHICH?) Multicenter, Randomized Trial
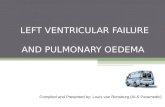
It is for the above reasons that we postulated that there wereimportant differences between clinic and home-based HF-MPs in respect to cost of health care and consumer preferenceswhile implementing a comprehensive range of interventionsthat comply with the full list identified by Jaarsma [16] in bothgroups, in addition to the type of nonpharmacological man-agement components advocated by the European Society ofCardiology [17•]. The WHICH? trial [18] was a prospective,multicenter randomized control trial with blinded endpointadjudication comprising 280 hospitalized patients with chronicHF (73 % male, 71±14 years of age and 73 % with LVEF≤45 %) randomized to outreach, home-based intervention(HBI) or outpatient specialized HF clinic-based intervention(CBI). As was reported in the primary outcome report [19••],102/143 (71 %) HBI versus 104/137 (76 %) CBI patientsexperienced the primary endpoint of all-cause hospitalizationor death (adjusted HR 0.97; 95 % CI 0.73–1.30; p=.861)during 12- to 18-month follow-up, comprising fewer deathsin the HBI group (31 [21.7 %] vs. 38 [27.7 %]: adjusted HR0.75, 95 % CI 0.45–1.23; p=.252) and similar proportionshospitalized [18]. However, HBI patients had fewer days ofhospitalization overall, the pattern clearly demonstrating thatthere were fewer “high-cost” and clinically unstable patients inthe HBI group (see Fig. 1). Consequently, total cost of
Table 1 Mode of delivery may differ, but the key components of heartfailure (HF) management are the same
Mode of Delivery Key Components of Care
Specialist HF clinic usually locatedin a tertiary referral institution
Clinical symptom surveillance
Physiological monitoring
Specialist HF outreach programvisiting patients in their own home
Routine reminders and contact
Patient initiated contact
Structured telephone supportvia central “call-center”
Enhance/support self-carebehaviors
Education
Automated remote monitoring usingimplanted or noninvasive devices
Diet and fluid management
Exercise therapy
Community-based/primary-caremanagement
Initiate and up-titrate therapy
Monitor treatment adherence
Combination of the above Carer support
228 Curr Heart Fail Rep (2013) 10:227–231
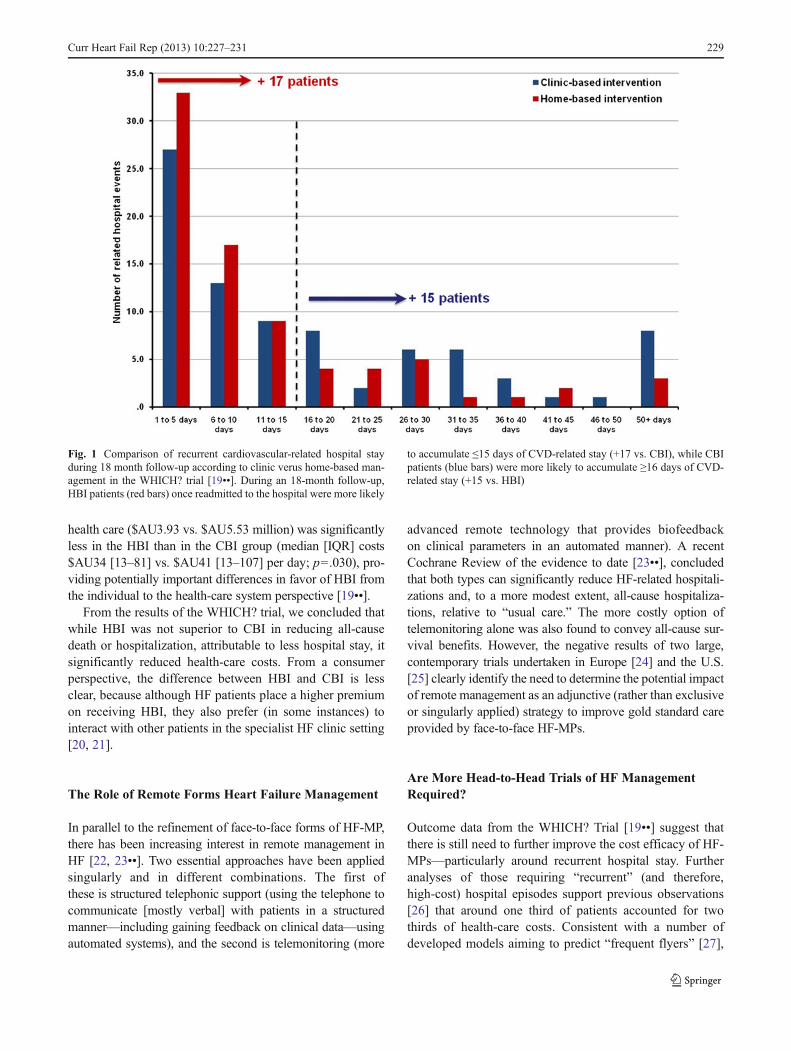
health care ($AU3.93 vs. $AU5.53 million) was significantlyless in the HBI than in the CBI group (median [IQR] costs$AU34 [13–81] vs. $AU41 [13–107] per day; p=.030), pro-viding potentially important differences in favor of HBI fromthe individual to the health-care system perspective [19••].
From the results of the WHICH? trial, we concluded thatwhile HBI was not superior to CBI in reducing all-causedeath or hospitalization, attributable to less hospital stay, itsignificantly reduced health-care costs. From a consumerperspective, the difference between HBI and CBI is lessclear, because although HF patients place a higher premiumon receiving HBI, they also prefer (in some instances) tointeract with other patients in the specialist HF clinic setting[20, 21].
The Role of Remote Forms Heart Failure Management
In parallel to the refinement of face-to-face forms of HF-MP,there has been increasing interest in remote management inHF [22, 23••]. Two essential approaches have been appliedsingularly and in different combinations. The first ofthese is structured telephonic support (using the telephone tocommunicate [mostly verbal] with patients in a structuredmanner—including gaining feedback on clinical data—usingautomated systems), and the second is telemonitoring (more
advanced remote technology that provides biofeedbackon clinical parameters in an automated manner). A recentCochrane Review of the evidence to date [23••], concludedthat both types can significantly reduce HF-related hospitali-zations and, to a more modest extent, all-cause hospitaliza-tions, relative to “usual care.” The more costly option oftelemonitoring alone was also found to convey all-cause sur-vival benefits. However, the negative results of two large,contemporary trials undertaken in Europe [24] and the U.S.[25] clearly identify the need to determine the potential impactof remote management as an adjunctive (rather than exclusiveor singularly applied) strategy to improve gold standard careprovided by face-to-face HF-MPs.
Are More Head-to-Head Trials of HF ManagementRequired?
Outcome data from the WHICH? Trial [19••] suggest thatthere is still need to further improve the cost efficacy of HF-MPs—particularly around recurrent hospital stay. Furtheranalyses of those requiring “recurrent” (and therefore,high-cost) hospital episodes support previous observations[26] that around one third of patients accounted for twothirds of health-care costs. Consistent with a number ofdeveloped models aiming to predict “frequent flyers” [27],
Fig. 1 Comparison of recurrent cardiovascular-related hospital stayduring 18 month follow-up according to clinic verus home-based man-agement in the WHICH? trial [19••]. During an 18-month follow-up,HBI patients (red bars) once readmitted to the hospital were more likely
to accumulate ≤15 days of CVD-related stay (+17 vs. CBI), while CBIpatients (blue bars) were more likely to accumulate ≥16 days of CVD-related stay (+15 vs. HBI)
Curr Heart Fail Rep (2013) 10:227–231 229

multivariate analyses showed that the independent predictorsof recurrent hospitalization were (1) older age, (2) livingalone, (3) presence of increasing comorbidity, (4) impairedfunctional status, and (5) duration of HF.
Our group is currently in the process of finalizing theprotocol of the WHICH? II trial in order to further improveHF-related outcomes by testing the cost impact of moreintensive management (with adjunctive structured telephonesupport) in selected high-risk cases. We believe that this studywill be unique and innovative because of the following:
1. The recently reported COACH study (one of the largestand most rigorous studies of its kind) undertaken byJaarsma and colleagues also compared less intensiveversus a more intensive (home-based) HF-MP, with onlymodest benefits found in the latter [28]. However, itsapplication was based on a “one-size-fits-all approach,”and the WHICH? II trial will selectively apply moreintensive care.
2. We seek to further improve outcomes in patients livingin nonmetropolitan areas (i.e., beyond the reach of tra-ditional face-to-face HF-MP) by selectively applyingadditional home visits in those being routinely managedvia structured telephone support. This study will be thefirst to apply such a hybrid approach and focus onmetropolitan and regional patients simultaneously.
3. The primary endpoint is health-care costs, reflecting theevolving need for face-to-face randomized trials focusedon cost efficiency for the best health outcomes.
4. We will consider of additional factors, such as (1) theimpact of cognitive function and patient preferences ondelivery of care, (2) use of advanced cardiac parametersin delineating risk for ongoing morbidity and prematuremortality, and (3) the frequency and duration of tailoredmanagement and its impact on health outcomes and cost.
This is undoubtedly the future for HF-MPs (i.e., morehead-to-head trials) as we seek to further improve healthoutcomes in an increasingly older and fragile patient popu-lation with HF and related concurrent conditions requiringchronic care and support. This observation is supported bythe results of the recently reported NorthStar MonitoringStudy, a multicenter randomized trial that compared (goldstandard) clinical management versus clinical managementguided by NT-proBNP monitoring. Even though the en-hanced form of management did not positively influencethe (composite) primary endpoint of death or a cardiovascu-lar admission during the 2.5-year follow-up, it addressed anextremely promising strategy for improving HF care [29]. Aswe improve the gold standard management of the syndrome,it should be expected that it will be appropriately difficult toimprove on what we have already achieved via head-to-headtrials, while still acknowledging that there is room for im-provement. On balance, while there is still ongoing debate
around the role of adjunctive BNP monitoring [12, 13, 29], itwould appear that enhancing home-based management strat-egies still represents a promising means for reducing recur-rent hospital stay and prolonging survival in those with HFdischarged from hospitals.
Conclusions
There is a simple truism that resonates whenever there is acrisis or we, as individuals, feel stressed or threatened:“Home is where the heart is.” This article could well havebeen entitled such, because there are overwhelming reasons(both objective and subjective) why HF care and supportshould be predominantly (but not exclusively) applied in thehome. As has been indicated, how this is best applied andwith what specific components of direct delivery and adjunc-tive support require further investigation.
Compliance with Ethics Guidelines
Conflict of Interest Simon Stewart declares that he has no conflict ofinterest.
Human and Animal Rights and Informed Consent This articledoes not contain any studies with human or animal subjects performedby any of the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. • Heidenreich PA, Albert NM, Allen LA, et al. Forecasting theImpact of Heart Failure in the United States: A Policy Statementfrom the American Heart Association. Circ Heart Fail publishedonline April 24, 2013; doi:10.1161/HHF.0b013e318291329a. Areminder of a sustained epidemic of heart failure in our agingpopulations that will require more cost-effective health services.
2. Stewart S, MacIntyre K, Capewell S, McMurray JJV. Heart failureand the aging population: An increasing burden in the 21stCentury? Heart. 2003;89:49–53.
3. Stewart S, Jenkins A, Buchan S, Capewell S, McGuire A, et al. Thecurrent cost of heart failure to the National Health Service in theUK. Eur J Heart Fail. 2002;4:361–71.
4. Stewart S, Ekman I, Ekman T, et al. Population impact of heartfailure and the most common forms of cancer: a study of 1 162 309hospital cases in Sweden (1988 to 2004). Circ Cardiovasc QualOutcomes. 2010;3:573–80.
5. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guidelines forthe diagnosis and treatment of acute and chronic heart failure 2012:The Task Force for the Diagnosis and Treatment of Acute andChronic Heart Failure 2012 of the European Society of Cardiology.Developed in collaboration with the Heart Failure Association (HFA)of the ESC. Eur J Heart Fail. 2012 Aug;14(8):803–69.
230 Curr Heart Fail Rep (2013) 10:227–231

6. Rich MW, Beckham V, Wittenberg C, et al. A multidisciplinaryintervention to prevent the readmission of elderly patients withcongestive heart failure. N Engl J Med. 1995;333:1190–5.
7. Stewart S, Marley JE, Horowitz JD. Effects of a multidisciplinary,home-based intervention on unplanned readmissions and survivalamong patients with chronic congestive heart failure: A randomisedcontrolled study. Lancet. 1999 Sep 25;354:1077–83.
8. Blue L, Lang E, McMurray JJ, et al. Randomised controlled trial ofspecialist nurse intervention in heart failure. BMJ. 2001;323:715–8.
9. Cline CM, Israelsson BY, Willenheimer RB, et al. Cost effectivemanagement programme for heart failure reduces hospitalisation.Heart. 1998;80:442–6.
10. McAlister FA, Stewart S, Ferrua S, et al. Multidisciplinary strate-gies for the management of heart failure patients at high risk foradmission: A systematic review of randomized trials. J Am CollCardiol. 2004;44:810–9.
11. Sochalski J, Jaarsma T, Krumholz HM, Laramee A, McMurray JJV,Rich MW, et al. What Works In Chronic Care Management: TheCase Of Heart Failure. Heal Aff. 2009;28:179–89.
12. Berger R, Moertl D, Peter S, et al. N-terminal pro-B-type natriureticpeptide-guided, intensive patient management in addition to multi-disciplinary care in chronic heart failure a 3-arm, prospective,randomized pilot study. J Am Coll Cardiol. 2010;55:645–53.
13. Maisel A, Barnard D, Jaski B, et al. Primary Results of the HABITTrial (Heart Failure Assessment With BNP in the Home). J Am CollCardiol. 2013;61:1726–35.
14. Driscoll A, Worrall-Carter L, Hare DL, et al. Evidence-basedchronic heart failure management programs: reality or myth?Qual Saf Health Care. 2009;18:450–5.
15. Clark AM, Savard LA, Thompson DR. What is the strength ofevidence for heart failure disease-management programs? J AmColl Cardiol. 2009;54:397–401.
16. Jaarsma T, Brons M, Kraai I, et al. Componenents of heart failuremanagement in home care; a literature review. Eur J CardiovNursing; published online 2013: doi:10.1177/1474515112449539.
17. • Lainscak M, Blue L, Clark AL, et al. On Behalf of Committee onHeart Failure Management Network of the Heart Failure AssociationPractical Recommendations for Self-Care Management of HeartFailure. Eur J Heart Fail. 2011;13:115–26. Professional societiesare now producing expert, pragmatic guidelines for the managementof “real-world” heart failure patient populations.
18. Stewart S, Carrington MJ, Marwick T, et al. The WHICH? trial:rationale and design of a pragmatic randomized, multicentre com-parison of home- vs. clinic-based management of chronic heartfailure patients. Eur J Heart Fail. 2011;13:909–16.
19. •• Stewart S, Carrington MJ, Marwick TH, et al. Impact of HomeVersus Clinic-Based Management of Chronic Heart Failure: TheWHICH? (Which Heart Failure Intervention Is Most Cost-Effective& Consumer Friendly in Reducing Hospital Care) Multicenter,
Randomized Trial. J Am Coll Cardiol. 2012;60(14):1239–48.This is the first head-to-head trial of the two most popular formsof heart failure management, demonstrating some potentially im-portant advantages in favor of a home-based approach tomanagement.
20. Whitty JA, Carrington MJ, Stewart S, et al. Patient Preferences forthe Delivery of Disease Management in Chronic Heart Failure: AQualitative Study. J Cardiovasc Nurs. 2012;27(3):201–7.
21. Whitty JA, Stewart S, Carrington MJ, et al. Patient preferences andwillingness-to-pay for a home or clinic based program of chronicheart failure management: findings from the Which? trial. PLoSOne. 2013;8:e58347.
22. Clark RA, Inglis SC, McAlister FA, et al. Telemonitoring or struc-tured telephone support programmes for patients with chronic heartfailure: Systematic review and meta-analysis. BMJ. 2007;334:942.
23. •• Inglis SC, Clark RA, McAlister FA, et al. Which components ofheart failure programmes are effective? A systematic review andmeta-analysis of the outcomes of structured telephone support ortelemonitoring as the primary component of chronic heart failuremanagement in 8323 patients: Abridged Cochrane Review. Eur JHeart Fail. 2011;13:1028–40. This updated Cochrane Review pro-vides compelling evidence of the potential benefits of remote man-agement techniques, while suggesting that they should be appliedas an adjunctive, rather than primary, strategy in the managementof heart failure.
24. Koehler F, Winkler S, Schieber M, et al. Telemedical InterventionalMonitoring in Heart Failure (TIM-HF), a randomized, controlledintervention trial investigating the impact of telemedicine on mor-tality in ambulatory patients with heart failure: study design. Eur JHeart Fail. 2010;12:1354–62.
25. Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in pa-tients with heart failure. N Engl J Med. 2010;363:2301–9.
26. Pocock SJ, Ariti CA, McMurray JJV, et al. Predicting survival inheart failure: a risk score based on 39 372 patients from 30 studies.Eur Hear J. 2013;34:1404–13. doi:10.1093/eurheartj/ehs337.
27. Stewart S, Blue L, Walker A, et al. An economic analysis ofspecialist heart failure nurse management in the UK; can we affordnot to implement it? Eur Heart J. 2002;23:1369–78.
28. Jaarsma T, van der Wal MH, Lesman-Leegte I, et al. Effect ofmoderate or intensive disease management program on outcome inpatients with heart failure: Coordinating Study Evaluating Outcomesof Advising and Counseling in Heart Failure (COACH). Arch InternMed. 2008;168:316–24.
29. Schou M, Gustafsson F, Videbaek L, et al.; on behalf of theNorthStar Investigators. Adding serial N-terminal pro brain natri-uretic peptide measurements to optimal clinical management inoutpatients with systolic heart failure: a multicentre randomizedclinical trial (NorthStar monitoring study). Eur J Heart Fail. 2013Mar 18. [Epub ahead of print].
Curr Heart Fail Rep (2013) 10:227–231 231