Heart failure 3 new - WordPress.com · 2012. 11. 6. · “Heart Failure” vs. “Congestive Heart...
53
1 Heart failure Tamás Fenyvesi MD 3rd Department of Medicine
Transcript of Heart failure 3 new - WordPress.com · 2012. 11. 6. · “Heart Failure” vs. “Congestive Heart...

1
Heart failure
Tamás Fenyvesi MD3rd Department of Medicine

2
Circulatory failure
Heart
Insufficient oxygen and nutrient supply to the tissues,and cells+ insufficient removal of the metabolic endproducts
causes:cardiac extracardiac
1.decreased venous return2.increased vascular capacity3.decreased oxyhemoglobin

3
Heart failure:the heart is unable to pump sufficient blood , provided the
venous return is normal
mechanical myocardial1. pressure overload 1. ischaemic heart disease
AS, hypertension diffuse or segmental2. volume overload 2. myocardial disease
valvular regurg.,shunts
3. insufficient fillingmitral or tricuspid
stenosis4. Pericardial disease

4
Classifications of impaired ventricular fuction
1. Forward failure vs backward failure2. Left heart failure vs right heart failure3. Systolic vs diastolic dysfunction4. Acute vs chronic5. Low output vs high output

5
“Backward” failure
James Hope 18321. ventricular volume and pressure2. atrial volume and pressure behind the failing ventricle3. atrial contraction4. venous pressure 5. capillary pressure6. transsudation into the interstitial tissue7. extracellular fluid volume

6
“Forward failure”Sir James Mackenzie 1913
decreased cardiac output:kidneys sodium retention
(RAS activation)liver dysfunctionmuscular weakness, fatiguebrain confusion

7
„left” or „right” heart failure
This is implicitly „backward failure”congestion behind the originally failing ventricle
left ventricle pulmonary congestion,pulm edema
right ventricle liver and peripheralcongestion oedema etc

8
Acute heart failure
The sudden development of the syndromeno time for compensatory mechanisms to activate
massive myocardial infarctionheart block with very slow ventricular rate< 35/mintachyarrhythmia with very rapid rate > 180/minrupture of a valveocclusion of a large segment of pulmonary artery
sudden reduction of cardiac output

9
stroke volume
symp PRA
catechol vasoconstr AII
prostaglandin bradykinin vasopressin aldosteronedilate dilate constr constr
constrictor > dilatator

10
Low-output vs high-output failure
1. Low output is the typical: most of the heart diseasesimpaired peripheral circulation, cold, pale or cyanotic extremities
2. High output: cardiac output is high before the developmentof failure
anaemia, hyperthyroidismAV shunts, Paget’s disease, Beriberi (B1 vit defic)gravidityhot, hyperemic extremities

11
Compensatory mechanismsExtracardiac cardiacpreload
afterloadnatriuresis
volume decomp atrial dilat vasodilat
vasoconstr cardiac output ANP
RASsymp,ADH
RBF GFR FFsodium retention

12

13

14

15

16
ACC Heart Failure GuidelinesSlide Deck
Based on the ACC/AHA 2005 Guideline Update
for the Diagnosis and Management of Chronic Heart Failure in the Adult
January 2006

17
Definition of Heart Failure
HF is a complex clinical syndrome that canresult from any structural or functionalcardiac disorder that impairs the ability ofthe ventricle to fill with or eject blood.

18
“Heart Failure” vs. “Congestive Heart Failure”
Because not all patients have volume overload atthe time of initial or subsequent evaluation, theterm “heart failure” is preferred over the older term “congestive heart failure.”

19
Causes of HF in Western World
For a substantial proportion of patients, causes are:
1. Coronary artery disease
2. Hypertension
3. Dilated cardiomyopathy

20
Class I —No limitation: Ordinary physical activity does notcause undue fatigue, dyspnea, or palpitation.
Class II —Slight limitation of physical activity:Such patients are comfortable at rest.Ordinary physical activity results in fatigue, palpitation dyspnea, or angina.
Class III —Marked limitation of physical activity:Although patients are comfortable at rest, less than ordinary activity will lead to symptoms.
Class IV —Inability to carry on any physical activity without discomfort: Symptoms of congestivefailure are present even at rest. With any physical activity, increased discomfort isexperienced.
NYHA Classification of HF

21
Stages of Heart Failure
At Risk for Heart Failure:
STAGE A High risk for developing HF
STAGE B Asymptomatic LV dysfunction
Heart Failure:
STAGE C Past or current symptoms of HF
STAGE D End-stage HF

22
Stage A
Patients at High Risk for Developing Heart Failure

23
Stage B
Patients with Asymptomatic LV Dysfunction

24
Stage C
Patients with Past or CurrentSymptoms of Heart Failure

25
Stage D
Patients with Refractory End -Stage HF

26
Stage D Therapy
Options for end-of-life care should be discussed with the patient and family when severe symptoms in patients with refractory end-stage HF persist despite application of all recommended therapies.
Discussion of Options for End-of-Life Care
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

27

28

29
Stages of Heart Failure
COMPLEMENT, DO NOT REPLACE NYHA CLASSES
• NYHA Classes - shift back/forth in individual patient (in response to Rx and/or progression of disease)
• Stages - progress in one direction due to cardiac remodeling

30
Differential Diagnosis in Patient with HF and Normal LVEF with Symptoms
• Incorrect diagnosis of HF• Inaccurate measurement of
LVEF• Primary valvular disease• Restrictive (infiltrative)
cardiomyopathies• Amyloidosis, sarcoidosis,
hemochromatosis• Pericardial constriction• Episodic or reversible LV
systolic dysfunction• Severe hypertension,
myocardial ischemia
• HF associated with high metabolic demand (high-output states)
• Anemia, thyrotoxicosis, arteriovenous fistulae
• Chronic pulmonary disease with right HF
• Pulmonary hypertension associated with pulmonary vascular disorders
• Atrial myxoma• Diastolic dysfunction of
uncertain origin• Obesity

31

32

33
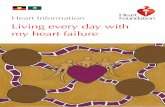
BNP - echodyspnea
BNP - echodyspnea
EKG, RTG, BNP
<100 100-500 >500 pg/ml
HF echo: LVD HF 95%unlikely COPD echo
PE
EKG, RTG, BNP
<100 100-500 >500 pg/ml
HF echo: LVD HF 95%unlikely COPD echo
PE
Maisel Rev CV Med 2003;4:S3-12Maisel Rev CV Med 2003;4:S3-12

34
Systolic vs diastolic heart failure
Implicit in the physiological definition the defect to pumpadequate volume of blood is a systolic heart failure
the abnormality may be caused by a defect ofventricular filling i.e. diastolic heart failure
slowed or incomplete ventricular relaxation possible causes:
acute or chronic ischaemiaconcentrical hypertrophyrestrictive cardiomyopathy
most clinical manifestations are combined

35
Diastolic dysfunctionFibrosis Cellular dysarray PassiveHypertrophy chamber
stiffnessAsynchrony DiastolicAbnormal loading pressureIschemia RelaxationAbnormal Ca++ flux

36
Diastolic heart failure became a centralissue of cardiology.
Diastolic heart failure is heart failure with preserved systolic functionor normal ejection fraction (HFNEF)EF>50%

37

38

39
Systole and diastole
“So that the coming together,
depends on the going apart,
the systole depends on the diastole;
the flow depends on the ebb.”
DH Lawrence

40
Symptoms of heart failure
1.dyspnea2.fatigue and weakness
hypoperfusion of the sceletal musculaturehyponatremia caused by diuretics
3.nocturiaredistribution of cardiac output at night: RBF
4.liver distensionepigastrial dyscomfort

41
General mechanisms of dyspnoe:left atrial pressure
pulmonary capillary pressure
interstitial fluid volume in the lungs
elasticity of the lung
increased work of breathing low cardiac output impaired perfusion of the respiratory
muscles fatigue sensation of dyspnoe

42
Physical signs of heart failure1
•visible dyspnoe •gray color of the face•cold extremities and acrocyanosis •decreased pulse pressure•extension of the veins (jugular) •palpable liver •symmetrical edema (pitting)
ankle-sacral-generalized•ascites•hydrothorax •rales „moist” at the end of inspiration

43
Physical signs of heart failure 2
tachycardiapulsus alternans ?
auscultation of the heartS3 gallopaccentuated P2syst murmur- tricusp regurg
cardiac cachexia

44
Pulsus alternans
this is just an interesting possibility

45
Framingham criteria for congestive heart failure
Major criteria:paroxysmal nocturnal dyspnea or orthopneaneck vein distensionralescardiomegalyacute pulmonary edemaS3 gallopincreased venous pressure > 16cm H2Ocirculation time > 25 sechepatojugular reflux

46
Framingham criteria for congestive heart failure
Minor criteria: ankle edemanight coughdyspnea on exertionhepatomegalypleural effusionvital capacity 1/3 from maximumtachycardia > 120/min
Minor or major criterion:weight loss > 4,5 kg in 5 days in
response to treatment

47
The main causes of heart failureIschaemic heart disease !!
myocardial infarction necrosisremodeling
Systemic hypertension LV hypertrophy
Valvular heart disease pressure load, ASvolume load AI
Cardiomyopathies obstructivedilatativerestrictive

48
Algoritm of diagnostic approach to HF
Suspition of HF
EKG,,RTG, BNP if available
Dg. rejected
abnormal
echocardiography
Cause,type,severity?
abnormal
therapy
additional Workup, eg.
coronarography
norm
norm

49
Epidemiology of heart failure~ 4 million pts in the USA
yearly incidence > 400.000 hospitalization 1000 000
most prevalent cause of death > 300.000Hospital mortality 30-50% / yearin the mixed population
5 years survival afterdiagnosis only 25% in men and
38% in womenyearly cost 22billion $

50
Annual incidence of heart failure per 1000 population in
Framingham
1 2 35 6
9
13
17
2831
0
5
10
15
20
25
30
35
45-54 55-64 65-74 75-84 85-94
femalemale

51
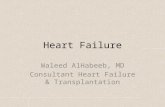
Prevalence of heart failure

52
Prevalence of HFPrevalence of HF
4,8 4,25,1
3,14,5
2,91,7 1,23 1,5
0
3
6
9
Nether.Rotter.2,1
Nether.Rotter.2,1
USAOlmsted2,2
USAOlmsted2,2
PortugalEPICA4,2
PortugalEPICA4,2
SpainAsturias4,9
SpainAsturias4,9
Den.Copen.6,4
Den.Copen.6,4
SvedenVästeras6,7
SvedenVästeras6,7
EnglandPoole7,5
EnglandPoole7,5
FinlandHelsinki8,2
FinlandHelsinki8,2
USACHS8,8
USACHS8,8
Age(years) 66-103 75-86 70-84 75 ≥50 >40 >25 >44 55-95Mean 78 - 76 75 - 60 68 63 65
Age(years) 66-103 75-86 70-84 75 ≥50 >40 >25 >44 55-95Mean 78 - 76 75 - 60 68 63 65
proportion with preserved
LV systolic function
proportion with preserved
LV systolic function
Hogg JACC 2004; 43:317Hogg JACC 2004; 43:317
Overall 2.5% in the communitySenni, Circ 1998; 98:2282
Overall 2.5% in the communitySenni, Circ 1998; 98:2282

53