
Webinar pv use case 23 march2016
48
1 Pharmacovigilance and the role of Scientific Literature – Challenges and Solutions Presented by: Joyce de Langen, pharmacist Sr Solution Manager Pharmacovigilance, Elsevier Life Sciences Date: 23 rd of March 2016
-
Upload
ann-marie-roche -
Category
Health & Medicine
-
view
1.159 -
download
0
Transcript of Webinar pv use case 23 march2016

1
Pharmacovigilance and the role
of Scientific Literature –
Challenges and Solutions
Presented by: Joyce de Langen, pharmacist
Sr Solution Manager Pharmacovigilance,
Elsevier Life Sciences
Date: 23rd of March 2016

2
Take Home Message
• Scientific and medical literature is a relevant source of adverse drug
reactions
• Literature screening for single adverse drug reactions does have
impact on patient safety and the life cycle of a drug
• MAHs are facing a number of challenges with regard to literature
management for pharmacovigilance
• Software solutions for literature management improve patient safety,
increase efficiency in literature management, and improve regulatory
compliance

3
Pharmacovigilance
• Science and activities relating to the detection, assessment,
understanding and prevention of adverse drug reactions (ADRs) or
any other medicine-related problem
• Pharmacovigilance is a science and activity that improves patients’
safety and public health
• Traditionally Pharmacovigilance is based on the gathering,
assessment and analysis of adverse drug reactions spontaneously
reported by Health Care Professionals to the regulatory authorities.

4
Preventing Adverse Drug Reactions Improves Public Health
• 5 % of all hospital admission in EU are related to adverse drug
reactions
• 28% of patients visit emergency department of hospital due to
adverse events
• Averse drug reactions are the 5th most common cause of death of
hospitalized patients.
• Nearly 197,000 death per year due to adverse drug reactions
• Costs 75 Billion US Dollars per year
- Lazarou J et al. Incidence of ADRs in hospitalized patients. JAMA 1998, 279 (15) 1200-1205
- Classen DC et al. ADRs in hospitalized patients: excess length of stay, extra costs, and attributable mortality.
Obstet. Gyncol Surv 1997, 52 (5):291-292
-Ahmad SR: Adverse drug event monitoring at FDA. J Gen Intern Med 2003, 18 (1): 57-60.

5
Literature is the 4th largest source of AE reporting
Adverse events reported in literature can have a high impact — major drug recalls
(e.g., Vioxx, Baycol) were initiated by published adverse reactions.
Often overlaps with reports from health professionals
FDA Adverse Event Reporting System (FAERS) Quarterly Data Files, Q2 and Q3 2013
Reported adverse events by report source,
Q2 & Q3 2013
N = 34,469 unique events
Overlap of adverse events sourced from
literature by reporting sources, Q2 & Q3 2013
N = 4,691 unique events

6
A. Good reporting Practice Spontaneous case reports of adverse events submitted to the sponsor and FDA, and reports from other sources, such as the medical literature or clinical studies, may generate signals of adverse effects of drugs. The quality of the reports is critical for appropriate evaluation of the relationship between the product and adverse events. FDA recommends that sponsors make a reasonable attempt to obtain complete information for case assessment during initial contacts and subsequent follow-up, especially for serious events, and encourages sponsors to used train…
VI.B.1.1.2. Literature reports The scientific and medical literature is a significant source of information for the monitoring of the safety profile and of the risk benefit balance of medicinal products, particularly in relation to the detection of new safety signals or emerging safety issues. Marketing authorization holders are therefore expected to maintain awareness of possible publications through a systematic literature review of widely used reference databases (e.g. Medline, Excerpta Medica or Embase) no less frequently than once a week. The marketing authorization holder should ensure that the literature review includes the use of reference databases that contain the largest reference of articles in relation to the medicinal product properties
Growing regulatory pressure and focus on literature
monitoring in EU & US
Marketing authorization holders are therefore
expected to maintain awareness of possible
publications through a systematic literature
review of widely used reference databases
(e.g. Medline, Excerpta Medica or Embase)
no less frequently than once a week.
The quality of the reports is critical for
appropriate evaluation of the relationship
between the product and adverse events.

7
Quality in literature review
• All MAHs need to implement a systematic approach to collect
information about suspected ADRs from literature sources
• This systematic approach should be:
– Documented in a Standard Operating Procedure
– Undergo Periodic Quality Control Checks >> to determine efficiency
• MAH should track/document:
– Search strategy
– Source Databases used
– Date of search
– Results of search >> specifically in case of ‘No results’
– Date of review & QC
– Names, details reviewer & QC

8
• Systematic review of widely used reference databases (eg. Medline,
Embase) and local journals in countries were medicinal product has
a marketing authorizaton
• Literature search should cover scientific & medical literature
including
– Full text or abstract publications
– Information presented at scientific meetings & conferences
– Systematic reviews & meta-analysis
– Data from competitor products
– Legal documents like Patents etc
– Dissertations & Thesis
– Lay press
• At least once weekly
Systematic review of literature for Safety Signals

9
Types of articles on ADRs between 1999-2003

10
Example 1: Thalidomide-induced Phocomelia (1961)
McBride WG. Thalidomide and congenital abnormalities. Lancet. 1961;278:1358

11
To consider when reviewing literature articles for ICSRs
• Quality and completeness of report
• Report is not always proven, more opinions
• Under-reporting
• Exposure data are often missing >> frequency of ADR difficult to
determine
• Patient identifiers are missing or are presented as aggregated data
• Confounding by indication might play a role
ADRs may be the result of external/human factors (eg. Medication
errors)
• Biased reporting triggered by media attention

12
Literature and impact on benefit-risk balance of medicinal
products
• Literature monitoring for adverse drug reactions might reveal safety
signals that impact the benefit-risk balance of a medicinal product
• Several safety signals detected in literature reports had impact on
the life cycle of the drug
• Reporting rates can differ between reports from literature and other
spontaneous reported ADRs depending on the type of adverse
reaction reported

13
Central system (Eudravigilance) supports detection of
signals of new or changing safety issues
• In 2014, 2,030 potential signals were reviewed:
– 86.7% of potential signals originating from EudraVigilance.
– 8.6% from scientific literature (vs 5% in 2013)
– 3.2% from other regulatory authorities
– 1.5% from other sources.
• 90 signals confirmed
– 40% of the assessed
signals resulted in a
recommendation for an
update of the product
information
2014 annual report on EudraVigilance

14
Safety information from spontaneous and literature adverse
reactions reports differ
Klose J, Fröhling S, Kroth E, Dobmeyer T, Nolting A. Safety information from spontaneous and literature adverse reactions
reports: a comparison. Ther Innov Regul Sci. 2013;47:248–55.
Extracted from Table 4
Reporting rates can differ depending on the type of adverse reaction reported
Drug Substance System Organ Class Literature Cases (%) Spontaneous Cases (%) % Difference
Acetylsalicylic Acid
Nervous System
Disorders 25.6 8 17.6
Gastrointestinal
Disorders 8.4 25.4 17.0
Fentanyl Injury, poisoning,
complications 35.9 7.5 28.3
Alendronic acid
Gastrointestinal disorders 4.6 21.0 16.5
Injury, poisoning,
complications 28.3 5.4 22.9
Tamsulosin Injury, poisoning,
complications 50 4.1 45.9
Etoposide Congenital, familial,
genetic 0 24.3 24.3

15
Example 2: Tamsulosin and ‘Floppy Iris Syndrome’ (2005)
Chang DF, Campbell JR,. Intraoperative floppy iris syndrome associated with tamsulosin.
J Cataract Refract Surg. 2005;3: 664-73
• Intraoperative floppy iris syndrome
occurred in approximately 2% of a
cataract surgery population
• Appeared to be caused by
tamsulosin, a systemic sympathetic
alpha-1A antagonist
• Chang et al. mention 15 patients with
IFIS
• At the time of publication, none had
been reported to the Regulatory
Authorities!

16
Example 3: Off-label use of GM-CSF in HIV-patients
• A systematic qualitative review of the literature was performed to
assess the safety of granulocyte macrophage colony-stimulating
factor (GM-CSF)
• Off-label use in US for treatment of neutropenia in AIDS-patients
• Concerns about the safety as in vitro data showed HIV up-regulation
by GM-CSF
• Meta-analysis showed an increased risk for viral-replication caused
by GM-CSF in AIDS-patients who where not treated with anti-
retroviral products
• Signal was detected based on information from in vitro studies
published in scientific literature
Challenges in Literature Management
for Pharmacovigilance
18
Challenges in literature screening
• Lack of harmonization across Regulatory Authorities and Industry
thought leaders
• Building the perfect search strategy. Does it even exist?
• Meeting the authority requirements and increased attention for
literature management during inspections

19
Challenges in literature screening: Lack of Harmonization
across Regulatory Authorities & thought leaders

20
ICH E2D
Regularly screen worldwide scientific literature by assessing widely
used systematic literature reviews or reference databases
Frequency: according to local/national requirements or at least every
two weeks
Scientific and medical literature
including relevant published meeting & conference abstracts
Including draft manuscripts (Article in press & Article in Process)
Reporting Rules
One form per identifiable patient
Report Source: publication reference
Copy of article might be required (differs between local authorities)

21
ICH E2D
• Local language journals need to be monitored by local affiliates
• Day 0 = The moment the MAHs (or one of his third parties) has
received the minimum criteria for needed to meet the reporting rules.
• When the product source, brand or trade name is not mentioned, the
MAH should assume that it was its product, but the case report
should mention that the brand could not be identified.
• When an article mentions multiple drugs, only a report should be
submitted for the product identified as suspect by the author of the
article

22
FDA
• Serious, unexpected adverse experiences reported in scientific
literature (or in any unpublished scientific paper) that are know to
the applicant must be submitted within 15 days.
• Reports of serious, unexpected adverse experiences described in
scientific literature should be submitted for products with the same
active substance as a product marketing in the US. This is true even
if the excipient, dosage forms, strengths, routes of administration
and indications vary.
• Serious unexpected adverse experiences based on a foreign
language article or manuscript should be translated by the applicant
into English promptly….

23
EMA
• Reports of suspected adverse reactions from scientific and medical
literature, including relevant published abstracts from meetings and
draft manuscripts, should be reviewed and assessed by MAHs to
identify and record ICSRs originating from spontaneous reports, or
non-interventional post-authorisation studies
• If multiple medicinal products are mentioned in the publication, only
those which are identified by the publication’s author as having at
least a possible causal relationship with the suspected adverse
reaction should be considered by the concerned MAHs’

24
EMA -Exclusions
• Exclusion based on primary source country or country of origin of
the ADR, if MAH can demonstrate that the suspect drug never has
been supplied or marketed in that country
• Literature ICSRs from local language journals from countries where
MAH never has supplied or marketed the drug
• Literature ICSRs from analysis from competent authority database
within EU.
• Literature with data analysis from public databases or literature
summarizing aggregated data

25
Challenges in literature screening: When to start?
• When do you start your literature surveillance of a new medicinal
product?
A. After the submission of the application for marketing authorization
B. After the regulatory approval of the marketing authorization
C. After the marketing of an authorized medicinal product

26
Challenges in literature screening: When to start?
• When do you start your literature surveillance of a new medicinal
product?
A. On submission of the application for marketing authorization
B. After the regulatory approval of the marketing authorization
C. After the marketing of an authorized medicinal product
It is expected that literature screening should start on submission of a
marketing authorization application and should continue while
authorization is active.

27
Challenges in literature screening: which sources to monitor?
• Search well recognized scientific and medical journals
• At least two well recognized medical databases Embase
– Medline
– Cochrane Library
– CINAHL
– Other relevant databases
• Conference abstracts, draft manuscripts
• Local Language Journals

28
Challenges in literature screening: handling large amount
of data Number of records added to Embase each year
Embase, July 2015 Millions of Records
The large amount of data increases workload and costs, and may even increase the
risk of losing oversight of the data. Quality of the reports may decrease. Potentially
relevant information might be missed and the risk for missing signals might be
increased. Growing amount of data to be processed requires a structured approach
to handle all data.

29
Searching for safety-relevant information
• Optimizing search strategy by
– Choosing the best source databases and search engines
– Creating the best possible search strategy and search terms
– Using the right search limits
– Using defined review criteria

30
Choice of source databases and Search Engines
• Databases differ in accessibility, coverage & overlap
• No single database has full sensitivity for literature screening
• Periodic literature search and review should be performed in
multiple, carefully selected databases

31
Choice of search strategy
• Balancing between recall and precision = balancing between
‘capturing all relevant information’ and ‘avoiding all noise’
• Ideally the goal would be to build a search strategy with low recall
with high precision
• However, usually when recall , precision ; and visa versa
• So in real-life the goal of building a search strategy is to keep
precision as high as possible while recall is optimized

32
Choice of search strategy
• In case of a very large number of results from the search strategy,
MAHs may prepare two different search strategies and run these
parallel on a weekly basis:
• One for ICSR detection
• One for signal detection
• Search strategy for ICSR detection can exclude records for
pharmaceutical forms or routes of administration that are not
approved for that MAH

33
Challenges in literature screening: ongoing regulatory focus
during inspections
https://www.gov.uk/government/statistics/pharmacovigilance-inspection-metrics-2009-to-present
Finding 2011-2012 2012-2013 2013-2014 2014-2015
Critical
Findings NA NA NA NA
Major Findings 2.3% 15% 11% 11%
Minor Findings 11.2% 8% 11% 5%

34
Challenges in literature screening: Integration EMA MLM
Services
• Since September 2015, EMA started insource literature monitoring
for 300 active chemical substance groups (generics) and 100
herbal substance groups in order to alleviate workload for MAHs
• MAHs need to integrate the dataflow resulting from the EMA MLM
Service into their existing workflow for literature management and
ICSR-management
35
Challenges in literature screening: Integration EMA MLM
Services
• Pharmaceutical manufacturers are responsible for monitoring
scientific and medical publications in local journals
• EMA does not aggregate data for PSURs. Literature searches for
PSURs should be wider than those for individual adverse reaction
cases as they should also include studies reporting safety outcomes
in groups of subjects and other products, including:
– pregnancy outcomes (including termination) with no adverse outcomes
– use in pediatric populations
– compassionate supply, named patient use
– lack of efficacy
– asymptomatic overdose, abuse or misuse
– medication error where no adverse events occurred
– important non-clinical safety results
36
Summary: Challenges in literature screening
• Lack of harmonization across Regulatory Authorities and Industry
thought leaders
• Building the perfect search strategy
• Increasing amount of scientific information needs to be processed
- Increase of costs, more resources needed
- Risk for missing safety information/safety signals
- Difficulties with management of work process/workflow
• Ongoing attention for literature searching during inspections
• Integration EMA MLM Services into company literature
management system

37
Distribution of keywords between abstract and full-text
37 Information extraction from full text scientific articles: where are the keywords?
PMID[12775220]
Conclusion:
Although the abstract contains the best ratio of keywords per total of words, other sections of the
article may be a better source of biologically relevant data
Keyword measure (K) – depends on number and strength of co-occurrence relations within the text
Corpus: 104 articles published in Nature Genetics from June
1998 (volume 19, issue 2) to June 2001 (volume 28, issue 2),
which comply with the AIMRD structure.
“Major” keywords are distributed evenly between
sections, the difference is more noticeable for
“minor keywords”

38
Full text contains more information
38

39
Take Home Message
• Scientific and medical literature is a relevant source of adverse drug
reactions
• Literature screening for single adverse drug reactions does have
impact on patient safety and the life cycle of a drug
• MAHs are facing a number of challenges with regard to literature
management for pharmacovigilance
• Software solutions for literature management improve patient safety,
increase efficiency in literature management, and improve regulatory
compliance

Solutions for literature
management challenges

41
Literature management solutions: decrease risk of missing
information without redundant reviewing
Make sure all relevant
articles are captured
• Capture data from
most comprehensive
source of journals/
conference abstracts
• Develop custom
search strategies to
find all relevant data
Avoid redundant reviews
of the same input
• Save time and avoid
redundant reviewing with
automatic deduplication
of articles
Save time and
stay current
• Stay current and
work more efficiently
with automated
article curation
process
42
Literature management solutions: improve workflow
management and regulatory compliance
Track review process
in case of audit
• Demonstrate procedures
done correctly and
on time with traceable
review process
Improve article pipeline
management
• Identify most relevant
articles with text mining
• Ensure appropriate
personnel receive/
review required data
with alert system
Capture metrics behind
article reviews
• Calculate efficiency
and ensure strict
quality control by
capturing metrics
43
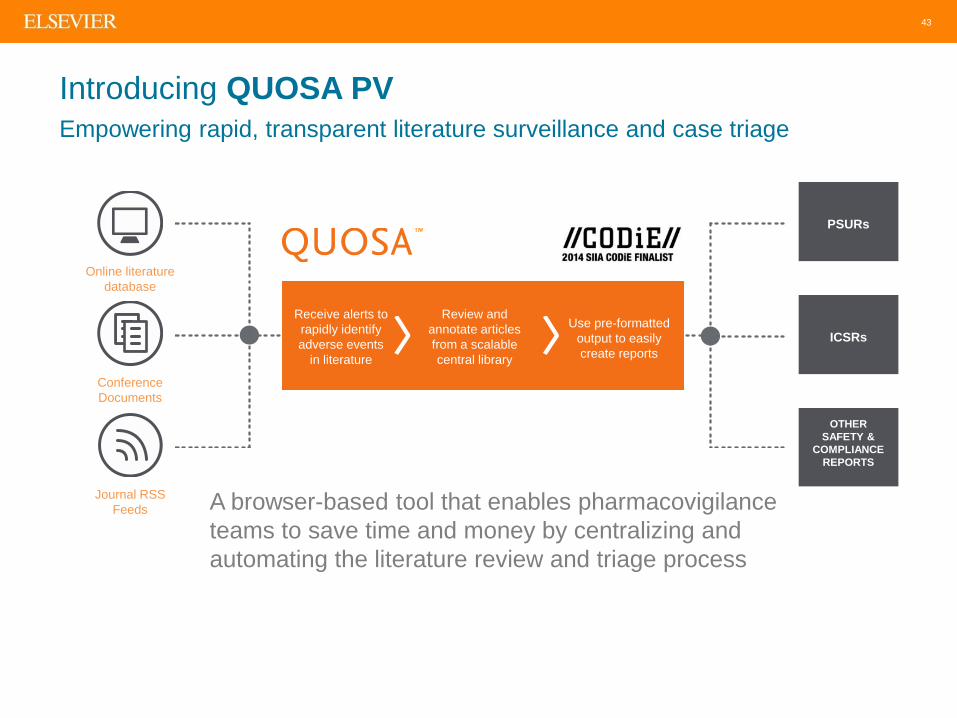
Introducing QUOSA PV
Empowering rapid, transparent literature surveillance and case triage
Conference
Documents
Online literature
database
Journal RSS
Feeds
PSURs
ICSRs
OTHER
SAFETY &
COMPLIANCE
REPORTS
A browser-based tool that enables pharmacovigilance
teams to save time and money by centralizing and
automating the literature review and triage process
Receive alerts to
rapidly identify
adverse events
in literature
Review and
annotate articles
from a scalable
central library
Use pre-formatted
output to easily
create reports

44
Introducing QUOSA PV
Empowering rapid, transparent literature surveillance and case triage
Conference
Documents
Online literature
database
Journal RSS
Feeds
PSURs
ICSRs
OTHER
SAFETY &
COMPLIANCE
REPORTS A combination of software and services that allows customers to
reduce risk, remain compliant and ensure that workgroups have
the latest scientific literature
Supervisors
Track deadlines
And bottlenecks
• Automatic alerts import
• Article deduplication
• E2B case data export
• Document listing
exports in Vancouver
format for PSURs
Administrators
View all aspects of
the review process

45
Reviewer view — Decision tree supports rapid identification
and capturing of cases
View abstracts or full-text and classify relevance with a fully trackable process
• View abstracts
or full text
• Audit trail for
every action
• Supports
multi-drug
annotation

46
Reviewer view — Decision tree supports rapid identification
and capturing of cases
Collaborate with colleagues for additional input/specialist review

47
Take Home Message
• Scientific and medical literature is a relevant source of adverse drug
reactions
• Literature screening for single adverse drug reactions does have
impact on patient safety and the life cycle of a drug
• MAHs are facing a number of challenges with regard to literature
management for pharmacovigilance
• Software solutions for literature management improve patient safety,
increase efficiency in literature management, and improve regulatory
compliance

48
Our mission in pharmacovigilance
Elsevier provides the solutions necessary for
Pharmacovigilance and drug safety groups
to be more efficient, stay compliant and
mitigate risks.
Thank you! Any questions?


















