€¦ · Web viewIndividuals are considered Ultra-High-Risk (UHR) for psychosis if they meet a set...
40
The Ultra-high Risk for Psychosis groups: Evidence to maintain the status quo. McHugh, M.J 1 ., McGorry, P.D 1 ., Yuen, H.P 1 ., Hickie, I 2 ., Thompson, A 3 ., de Haan, L 4 .,Mossaheb, N. 5 , Smesny, S 6 ., Lin, A 7 ., Markulev, C 1 .,Schloegelhofer, M 5,8 ., Wood, S.J 9,10 ., Nieman, D 11 , Hartmann, J.A 1 ., Nordentoft, N 12 ., Schaefer, M 1 ., Amminger, G.P 1 , Yung, A 13 *, Nelson, B 1 * 1. Orygen, The National Centre for Excellence in Youth Mental Health, 35 Poplar Rd, Parkville, VIC, Australia; 2. Brain and Mind Research Institute , University of Sydney , Sydney , Australia; 3. Division of Mental Health and Wellbeing, The University of Warwick, Coventry, UK. 4. Department of Psychiatry, Early Psychosis Section, Academic Medical Centre, University of Amsterdam, The Netherlands; 5. Department of Psychiatry and Psychotherapy, Medical University of Vienna, Vienna, Austria; 6. Department of Psychiatry and Psychotherapy, Jena University Hospital, Jena, Germany; 7. Telethon Kids Institute, The University of Western Australia, Australia; 8. Department of Child and Adolescent Psychiatry, Medical University Vienna, Vienna, Austria. 9. School of Psychology, University of Birmingham, Birmingham, UK; 10. Melbourne Neuropsychiatry Centre, Department of Psychiatry, University of Melbourne & Melbourne Health, Melbourne, Australia; 11. Department of Psychiatry, Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands ; 12. Mental Health Centre Copenhagen, Mental health Services Capital Region of Denmark, Denmark; 13. Psychiatric Centre Copenhagen, University of Copenhagen, Denmark. 14. Institute of Brain, Behaviour and Mental Health, University of Manchester, Manchester, UK. 1
Transcript of €¦ · Web viewIndividuals are considered Ultra-High-Risk (UHR) for psychosis if they meet a set...

The Ultra-high Risk for Psychosis groups: Evidence to maintain the status quo.
McHugh, M.J1., McGorry, P.D1., Yuen, H.P1., Hickie, I2., Thompson, A3., de Haan, L4.,Mossaheb, N.5, Smesny, S6., Lin, A7., Markulev, C1.,Schloegelhofer, M5,8., Wood, S.J9,10., Nieman, D11,Hartmann, J.A1., Nordentoft, N12., Schaefer, M1., Amminger, G.P 1, Yung, A13*, Nelson, B1*
1. Orygen, The National Centre for Excellence in Youth Mental Health, 35 Poplar Rd, Parkville, VIC, Australia;
2. Brain and Mind Research Institute, University of Sydney, Sydney, Australia;3. Division of Mental Health and Wellbeing, The University of Warwick, Coventry, UK.4. Department of Psychiatry, Early Psychosis Section, Academic Medical Centre,
University of Amsterdam, The Netherlands;5. Department of Psychiatry and Psychotherapy, Medical University of Vienna, Vienna,
Austria;6. Department of Psychiatry and Psychotherapy, Jena University Hospital, Jena, Germany;7. Telethon Kids Institute, The University of Western Australia, Australia;8. Department of Child and Adolescent Psychiatry, Medical University Vienna, Vienna,
Austria.9. School of Psychology, University of Birmingham, Birmingham, UK;10. Melbourne Neuropsychiatry Centre, Department of Psychiatry, University of Melbourne
& Melbourne Health, Melbourne, Australia;11. Department of Psychiatry, Academic Medical Center, University of Amsterdam,
Amsterdam, the Netherlands;12. Mental Health Centre Copenhagen, Mental health Services Capital Region of Denmark,
Denmark;13. Psychiatric Centre Copenhagen, University of Copenhagen, Denmark.14. Institute of Brain, Behaviour and Mental Health, University of Manchester, Manchester,
UK.
Corresponding Author:
Meredith J. McHughOrygen, The National Centre of Excellence in Youth Mental Health35 Poplar RdParkville, VIC, 3052, AustraliaEmail: [email protected]: +61793422800
Word count:Abstract: 229Text body: 2798
Abstract
1

Individuals are considered Ultra-High-Risk (UHR) for psychosis if they meet a set of
standardised criteria including presumed genetic vulnerability (Trait), or a recent history of
Attenuated Psychotic Symptoms (APS) or Brief Limited Intermittent Psychotic Symptoms
(BLIPS). Recent calls to revise these criteria have arisen from evidence that Trait, APS and
BLIPS groups may transition to psychosis at different rates. Concurrently, it has become clear
that the UHR status confers clinical risk beyond transition to psychosis. Specifically, most UHR
individuals will not develop psychosis, but will experience high rates of non-psychotic disorders,
persistent APS and poor long-term functional outcomes. Rather than focus on transition, the
present study investigated whether UHR groups differ in their broader clinical risk profile by
examining baseline clinical characteristics and long-term outcomes other than transition to
psychosis. Four UHR groups were defined: Trait-only, APS-only, Trait+APS, and any BLIPS.
Participants ( N = 702) were recruited upon entry to early intervention services and followed-up
over a period of up to 13 years (Mean=4.53, SD=3.84). The groups evidenced similar symptom
severity (SANS for negative symptoms, BPRS for positive and depression/anxiety symptoms)
and psychosocial functioning (SOFAS, GAF, QLS) at baseline and follow-up as well as similar
prevalence of non-psychotic disorders at follow-up. Our findings demonstrate that UHR groups
evidence a similar clinical risk profile when we expand this beyond transition to psychosis, and
consequently support maintaining the existing UHR criteria.
2

It has been two decades since Yung and colleagues (Yung and McGorry, 1996a) introduced a set
of standardised criteria to identify individuals at Ultra-High-Risk (UHR) of developing a
psychotic disorder (also known as the At Risk Mental State or ‘prodromal’ phase of psychosis).
Since this time, the UHR paradigm has provided a window into risk factors and aetiological
mechanisms involved in psychosis onset and an opportunity to trial preventive interventions (van
der Gaag et al., 2013). To be considered UHR, help-seeking individuals must be in the age range
of highest risk for psychosis (late adolescence, early adulthood) and meet one or more of the
following 3 criteria: 1) Attenuated Psychotic Symptoms (APS): sub-threshold positive psychotic
symptoms during the past 12 months; 2) Brief Limited Intermittent Psychotic Symptoms
(BLIPS): frank psychotic symptoms for less than one week which resolve spontaneously; 3)
Genetic vulnerability (Trait) – meet criteria for Schizotypal Personality Disorder or have a first-
degree relative with a psychotic disorder. Each risk criteria must also be associated with a
deterioration in functioning or chronic low functioning1.
Over the years, evidence has pointed to variability between groups defined by these UHR criteria
in relation to risk of transitioning to a psychotic disorder (Fusar-Poli et al., 2015; Nelson et al.,
2013, 2011) . A history of BLIPS (regardless of APS or Trait risk) has consistently been linked to
the highest risk of transitioning to a psychotic disorder (Fusar-Poli et al., 2015; Nelson et al.,
2013, 2011) . Presumed genetic vulnerability (Trait) with no history of APS or BLIPS (Trait-
only) confers the lowest transition risk (Fusar-Poli et al., 2015; Nelson et al., 2011) . An early
study found that the combination of genetic vulnerability and APS (Trait+APS) was strongly
predictive of transition to psychosis by twelve months (Yung et al., 2004) . However, more recent
evidence suggests similar risk trajectories for Trait+APS individuals and individuals who meet
1 The requirement for deterioration in functioning has changed over the years (see Table 1 for a summary of the changes).
3

APS criteria alone (APS-only) (Fusar-Poli et al., 2015; Nelson et al., 2011) .
Evidence of variability in transition risk has prompted some researchers to challenge the current
composition of the UHR criteria. In a guidance paper for the European Psychiatric Association,
Schultz-Lutter and colleagues recommended that having a first-degree relative with a psychotic
illness should not be considered a clinical marker of risk for psychosis even in the presence of
functional decline (Schultze-lutter et al., 2015) . Others have proposed that BLIPS should be
treated as a separate clinical entity based on both higher transition risk and diagnostic overlap
with DSM/ICD brief psychotic disorders (Fusar-Poli et al., 2015) .
Concurrently, it has become increasingly evident that clinical implications of UHR status extend
beyond risk of transition to psychosis. Most individuals who meet UHR criteria will not develop
a psychotic disorder (Nelson et al., 2013; Simon et al., 2011) but will experience persistent
attenuated psychotic symptoms (de Wit et al., 2014a; Simon et al., 2011) , poor psychosocial
functioning (Rutigliano et al., 2016a) and high rates of non-psychotic disorders (de Wit et al.,
2014b; Lin et al., 2015; Rutigliano et al., 2016b) . Such findings have driven a reframing of UHR
as a clinical state signifying pluripotent, transdiagnostic risk and the need for clinical care, rather
than simply a marker of psychosis risk (McGorry et al., 2006; McGorry and Nelson, 2016; Yung
et al., 2012) .
In the current study we investigated possible differences between the UHR groups in clinical risk
other than transition to psychosis. Specifically, we examined baseline clinical characteristics
known to contribute to poor outcomes in UHR populations, including symptom severity (Fusar-
Poli et al., 2013; Nelson et al., 2013; Seidman et al., 2010) , psychosocial functioning (Nelson et
al., 2013; Seidman et al., 2010) , duration of symptoms prior to first contact with clinical services
4

(Nelson et al., 2013) and the year that individuals entered clinical services (Nelson et al., 2013;
Simon et al., 2014; Yung et al., 2007) . We also examined long-term non-transition outcomes
including symptom severity, psychosocial functioning and the prevalence of non-psychotic
disorders . A large cohort ( N = 702) of UHR individuals were recruited at entry to treatment and
re-assessed up to thirteen years later. For consistency with previous studies (Fusar-Poli et al.,
2015; Nelson et al., 2011) , we defined four combinations of UHR risk group: Trait-only, APS-
only, Trait+APS, and any BLIPS (regardless of Trait or APS criteria). If the UHR groups defined
here engender truly distinct psychopathological risk profiles, we would expect group differences
to emerge in baseline characteristics and long-term non-transition outcomes.
2. Methods
2.1 Participants and Setting
The present sample (N = 702) were recruited between 1995 and 2013, across 10 research sites in
Australia (Melbourne, Sydney), the Netherlands (Amsterdam), Germany (Jena), Switzerland
(Basel, Zurich), Austria (Vienna), Denmark (Copenhagen), Singapore, and Hong Kong (Pok Fu
Lam). Each site has an established early psychosis clinical service that conducts research with
UHR clients. From 1995 to 2006 participants were recruited for UHR research studies at the
Melbourne site only (N = 398). These included three intervention (Berger et al., 2012; McGorry
et al., 2002; Yung et al., 2011) and four cohort studies (Phillips et al., 2009; Thompson et al.,
2007; Yung et al., 2003, 1996). This is the same group as previously reported in the PACE 400
long-term follow-up study (Nelson et al., 2013), excluding 18 participants for whom UHR risk
group could not be determined. The sample (recruited to baseline studies between 1995 and
2006) were followed up between 2007-2008 (for full details see Nelson et al, 2013). The
5

remaining 304 participants were recruited from 2010 to 2013 across the 10 research sites listed
as part of a large multi-site intervention study (Neurapro; Markulev et al., 2015; McGorry et al.,
2017).
Participants were required to meet criteria for at least one of the three UHR groups (APS, BLIPS
or Trait risk). Criteria used to assess each are summarized in Table 1. As illustrated, over the
years there have been changes in the requirement for functional deterioration across the three risk
groups as well as in measures used to assess risk. Exclusion criteria were known history of a
psychotic episode (treated or untreated); known organic cause of symptoms (e.g., epilepsy); or a
lifetime antipsychotic dose equivalent to or greater than 15mg of haloperidol.
2.2 Measures
2.2.1 UHR Status. Measures and methods used to assess UHR status from 1995 to 2013 are
outlined in Table 1.
2.2.2 Symptoms and psychosocial functioning. The Brief Psychiatric Rating Scale (BPRS;
Overall and Gorhum, 1962) was administered to assess positive symptoms (BPRS Psychosis
subscale) and depression/anxiety (BPRS Depression and Anxiety subscale). Negative symptoms
were assessed with the Schedule for the Assessment of Negative Symptoms (SANS; Andreasen,
1982). Psychosocial functioning was assessed with the Global Assessment of Functioning (GAF;
American Psychiatric Association, 1994), Social and Occupational Functioning Assessment
Scale (SOFAS; American Psychiatric Association, 1994) and Quality of Life Scale (QLS;
Heinrichs et al., 1984). SOFAS scores are reported for follow-up only as this measure was not
administered at baseline prior to 2010. QLS and GAF were available at baseline and follow-up,
but only for members of the PACE 400 subcohort.
6

2.2.3 Non-psychotic disorders. The presence of Axis I non-psychotic disorders at follow-up was
determined with the Structured Clinical Interview for DSM-IV disorders (SCID-IV; First et al.,
2002).
2.3 Procedures
Participants completed baseline assessments at entry to the clinical service. Follow-up interviews
were conducted in 91.1% (n=277) of the Neurapro cohort and 71.1% (n=283) of the PACE 400
cohort. For PACE 400 participants, where face-to-face interviews were not possible assessments
were conducted over the phone. Full details of follow-up procedures for the PACE 400 cohort
are reported elsewhere (Nelson et al., 2013). Mean time to follow-up interviews was 11.35
months (range 1.05 to 21.48 months) and 78.62 months (range 5.15 – 156.59 months) for the
Neurapro and PACE 400 cohorts respectively.
2.4 Data analysis
Group differences at baseline and follow-up for BPRS, SANS, GAF and QLS were examined
using general linear models with group (4 levels: Trait-only, Trait+APS, APS-only and any
BLIPS) as a fixed factor. Where baseline group differences in sample characteristics were
present (Table 2), models were run with and without including these characteristics as covariates.
Alpha was set at p = .01 at each time point (baseline, follow-up) for primary outcome variables
to adjust for multiple comparisons. Group differences in the prevalence of non-psychotic
disorders were examined using a logistic regression model with the presence or absence of non-
psychotic disorders as a binary outcome variable. We defined three levels of baseline year (1995-
1999, 2000-2006 and 2010-2013) to capture changes in transition rate over the years (Nelson et
7

al., 2013), as well as changes in methods and measures for assessing UHR status over time (see
Table 1).
3. Results
3.1 Sample characteristics
Table 2 presents baseline demographic and clinical characteristics for each of the four risk
groups. As illustrated, the APS-only group were, on average, younger at baseline than Trait-only
(p<.001) and Trait +APS (p = .018) and any BLIPS (p = .026) individuals. Groups also differed
in terms of year recruited into the study (baseline year: 1995-1999, 2000-2006, 2010-2013)
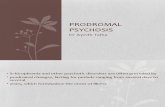
largely driven by a decline in any BLIPS and an increase in APS-only in later years (see Figure 1
and Table 2). Consequently, years to follow-up interview also differed between the groups. APS-
only individuals had the shortest time to follow-up relative to all other groups (all ps<.001). Any
BLIPS had a longer time to follow-up than Trait-only (p = .033) and Trait+APS (p = .003).
Across the sample, baseline year was highly correlated with time to follow-up interview, r(558)
= -.92, p<.001, due to the fact that participants from earlier baseline years necessarily had a
longer time to follow up.
3.2 Do the UHR risk groups vary in symptom severity and psychosocial functioning at baseline?
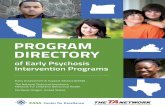
Figure 2, Table 3 and Table S1 summarise mean symptom severity (BPRS and SANS) and
functioning (GAF and QLS) at baseline and follow-up across the four UHR risk groups, and
present significant group differences where these emerged. Group effects emerged for the BPRS
Psychotic subscale at baseline, F(3, 685) = 20.07, p<.001), reflecting significantly lower scores
at baseline in Trait-only individuals relative to all other groups (ps< .001). Groups also varied at
baseline in GAF scores, F(3, 393) = 6.50, p <.001, with any BLIPS individuals showing higher
8

GAF scores at baseline compared to all other groups (all ps < .002). No baseline group
differences were observed for BPRS Anxiety and Depression (p=.523), SANS (p=.087) or QLS
(p = .320). This pattern of results remained the same after controlling for age at baseline.
3.3 Do the UHR risk groups vary on long-term non-transition outcomes?
The UHR risk groups did not differ at follow-up on either symptom severity (SANS, BPRS
Psychotic, BPRS Anxiety and Depression: all ps > .190; see Table S1 and Figure 2) or
psychosocial functioning (GAF, QLS, SOFS: all ps >. 293; see Table S1, Table 3 and Figure 2).
Additionally, the proportion of individuals meeting criteria for at least one Axis 1 non-psychotic
disorder at follow-up did not differ between the groups (p = .477, see Table 3). Results of long-
term outcomes analyses remained the same after controlling for age at baseline and time to
follow-up interview.
4. Discussion
In recent years the criteria that define UHR groups have been called into question due to
differences observed between these groups in transition risk (Fusar-Poli et al., 2015; Schultze-
lutter et al., 2015). At the same time, it has become evident that as a clinical entity UHR status
reflects more than simply a marker of psychosis risk, and may be more aptly considered a
transdiagnostic risk state signifying the need for clinical care (van Os and Guloksuz, 2017). The
present study thus aimed to compare UHR groups (APS-only, Trait-only, Trait+APS, any
BLIPS) in their broader psychopathological profile by exploring clinical characteristics at entry
into treatment as well as long-term outcomes other than onset of psychosis.
As expected (based on the definition of UHR criteria) Trait-only individuals reported less severe
positive psychotic symptoms at baseline. No other group differences in symptom severity at
9

baseline were observed. Notably, while Trait-only individuals presented with less severe baseline
positive symptoms at baseline they did not differ from the other groups in their negative
symptom severity. Zubin’s (Zubin, 1985) Vulnerability model considers negative symptoms,
such as social withdrawal and blunted affect, to be enduring characteristics that precede
psychosis onset and reflect underlying vulnerability to developing a psychotic disorder, which is
consistent with this finding. Alternatively, heightened negative symptoms could be secondary to
elevated depression and anxiety in this group (Lincoln et al., 2016). We found no evidence of
group differences in long-term non-transition outcomes, including symptom severity (BPRS,
SANS), psychosocial functioning (GAF, QLS, SOFAS) and prevalence of non-psychotic
disorders at follow-up. Our findings conflict with a recent study reporting that BLIPS individuals
were at lower risk of developing non-psychotic disorders than individuals with APS (Fusar-Poli
et al., 2017).
Interestingly, in the present sample we observed a significant shift in the proportion of UHR
groups over the years sampled (1995-2013). Most notably, we see an increasing proportion of
APS individuals in later years and a declining proportion of any BLIPS individuals. Earlier
detection of at-risk individuals may, at least in part, explain this effect. If we assume that a
history of APS can precede the occurrence of BLIPS (Shah et al., 2017; Yung and McGorry,
1996b), then it is possible that earlier detection (prior to BLIP onset) is resulting in a greater
proportion of individuals presenting with APS and a drop in individuals presenting with BLIPS
at treatment entry (Nelson et al., 2016). That our APS-only group were younger at treatment
entry is consistent with this conjecture. In conjunction, increased public awareness of early
intervention services and UHR criteria, as well as clinic screening processes (Wiltink et al.,
10

2015), could be resulting in a disproportionate increase in APS-only individuals being referred to
clinical services.
It is also important to highlight that the ‘any BLIPS’ group contained proportionally more
individuals recruited during earlier years when transition rates were higher (Nelson et al., 2013),
and had, on average, a longer time to follow-up, hence more opportunity to transition. It will be
important for future studies to consider whether these factors are contributing to the appearance
of group differences in transition risk. Unfortunately, sample size limitations prevented us from
fully exploring this in the present study.
Overall, our findings show a strong degree of homogeneity in both baseline characteristics and
long-term non-transition outcomes between the four UHR risk groups. This is critical given that
most UHR individuals will not develop a psychotic disorder (Nelson et al., 2013; Simon et al.,
2011), but do evidence poor long-term outcomes including high rates of non-psychotic disorders,
poor psychosocial functioning and persistent APS (de Wit et al., 2014a; Lin et al., 2015;
Rutigliano et al., 2016a). Thus if we consider the UHR construct as not simply a marker of
psychosis, but rather a transdiagnostic risk state signifying the need for clinical care (van
Prooijen et al., 2006), our findings do not support the segregation of UHR groups into separate
clinical entities as others have called for (Fusar-Poli et al., 2015; Schultze-lutter et al., 2015).
Some limitations of the present study should be noted. Firstly, it is possible that group
differences in non-transition outcomes were diluted by variance in treatment received and other
unmeasured participant and therapeutic factors that may contribute to variability in outcome
measures. It is also possible that the different study sites contributed variability to outcomes that
we could not measure in the present study due to the relatively small number of participants
11

recruited from sites other than Melbourne. Additionally, although we found no difference in the
prevalence of non-psychotic disorders across the risk groups, sample size limitations precluded
our capacity to explore types of non-psychotic disorders across groups.
Notwithstanding the aforementioned limitations, the present findings contrast with earlier results
by indicating a similarity in the clinical risk profile of the four UHR risk groups at entry to
clinical services and in long-term functional outcomes. Based on our findings we believe there is
currently insufficient evidence to support further partitioning the UHR population according to
the risk groups studied here. Pathways to psychosis are varied and likely involve a multitude of
interacting, time-varying factors. Rather than adopting further diagnostic ‘silos’, we believe that
efforts to assay true risk for psychosis that consider the complex array of social, psychological,
genetic and neurobiological mechanisms will be most fruitful. Moreover, the high rate of non-
psychotic disorders at follow-up across all groups reinforces the clinical utility of the UHR
construct and our view that it identifies a pluripotent, transdiagnostic risk state (McGorry and
Nelson, 2016), the identification of which can be further refined in an expanded set of ‘at risk’
criteria (Hartmann et al., In Press).
Funding
This work was funded by the Colonial Foundation Philanthropic Trust; Stanley Medical
Research Institute, and National Health and Medical Research Council Program Grant (#566529
and #350241). The Authors have declared that there are no conflicts of interest in relation to the
subject of this study.
Acknowledgments
The authors would especially like to thank the participants of all the studies and the researchers
involved in the original research studies.
12

References
American Psychiatric Association, 1994. Diagnostic Stastistical Manual of Mental Disorders (4th
ed). Author, Washington DC.
Andreasen, N.C., 1982. Negative symptoms in schizophrenia. Definition and reliability. Arch.
Gen. Psychiatry 39, 784–8.
Andreasen, N.C., Flaum, M., Arndt, S., 1992. The Comprehensive Assessment of Symptoms and
History (CASH). An instrument for assessing diagnosis and psychopathology. Arch. Gen.
Psychiatry 49, 615–23.
Berger, G.E., Wood, S.J., Ross, M., Hamer, C.A., Wellard, R.M., Pell, G., Phillips, L., Nelson,
B., Amminger, G.P., Yung, A.R., Jackson, G., Velakoulis, D., Pantelis, C., Manji, H.,
McGorry, P.D., 2012. Neuroprotective effects of low-dose lithium in individuals at ultra-
high risk for psychosis. A longitudinal MRI/MRS study. Curr. Pharm. Des. 18, 570–5.
de Wit, S., Schothorst, P.F., Oranje, B., Ziermans, T.B., Durston, S., Kahn, R.S., 2014a.
Adolescents at ultra-high risk for psychosis: Long-term outcome of individuals who recover
from their at-risk state. Eur. Neuropsychopharmacol. 24, 865–873.
doi:10.1016/j.euroneuro.2014.02.008
de Wit, S., Schothorst, P.F., Oranje, B., Ziermans, T.B., Durston, S., Kahn, R.S., 2014b.
Adolescents at ultra-high risk for psychosis: Long-term outcome of individuals who recover
from their at-risk state. Eur. Neuropsychopharmacol. 24, 865–873.
doi:10.1016/j.euroneuro.2014.02.008
First, M.., Spitzer, R.., Gibbon, M., Williams, J.B.W., 1997. Structured Clinical Interview for
13

DSM-IV Personality Disorders, (SCID-II). American Psychiatric Press, Inc., Washington,
DC.
First, M., Spitzer, R., Gibbon, M., Williams, J., 2002. Structured Clinical Interview for DSM-IV-
TR Axis I Disorders. Research Version, Patient Edition. Biometrics Research, New York
State Psychiatric Institute, New York, NY.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1995. The structured clinical interview
for DSM–III–R personality disorders (SCI- D–II). J. Pers. Disord. 9, 83–91.
Fusar-Poli, P., Borgwardt, S., Bechdolf, A., Addington, J., Riecher-Rössler, A., Schultze-Lutter,
F., Keshavan, M., Wood, S., Ruhrmann, S., Seidman, L.J., Valmaggia, L., Cannon, T.,
Velthorst, E., De Haan, L., Cornblatt, B., Bonoldi, I., Birchwood, M., McGlashan, T.,
Carpenter, W., McGorry, P., Klosterkötter, J., McGuire, P., Yung, A., 2013. The psychosis
high-risk state: a comprehensive state-of-the-art review. JAMA psychiatry 70, 107–20.
doi:10.1001/jamapsychiatry.2013.269
Fusar-Poli, P., Cappucciati, M., Borgwardt, S., Woods, S.W., Addington, J., Nelson, B., Nieman,
D.H., Stahl, D.R., Rutigliano, G., Riecher-Rössler, A., Simon, A.E., Mizuno, M., Lee, T.Y.,
Kwon, J.S., Lam, M.M.L., Perez, J., Keri, S., Amminger, P., Metzler, S., Kawohl, W.,
Rössler, W., Lee, J., Labad, J., Ziermans, T., An, S.K., Liu, C.-C., Woodberry, K.A.,
Braham, A., Corcoran, C., McGorry, P., Yung, A.R., McGuire, P.K., 2015. Heterogeneity
of Psychosis Risk Within Individuals at Clinical High Risk: A Meta-analytical
Stratification. JAMA psychiatry 73, 1–8. doi:10.1001/jamapsychiatry.2015.2324
Fusar-Poli, P., Rutigliano, G., Stahl, D., Davies, C., De Micheli, A., Ramella-Cravaro, V.,
Bonoldi, I., McGuire, P., 2017. Long-term validity of the At Risk Mental State (ARMS) for
14

predicting psychotic and non-psychotic mental disorders. Eur. Psychiatry 42, 49–54.
doi:10.1016/j.eurpsy.2016.11.010
Hartmann, J.A., Nelson, B., Spooner, R., Amminger, G.P., Chanen, A.M., Davey, C., McHugh,
M., Ratheesh, A., Treen, D., Yuen, H.P., McGorry, P.D. In Press. Beyond Psychosis Risk:
Methodlogy of a cohort study validating criteria for a pluripotent at-risk mental state.
Heinrichs, D.W., Hanlon, T.E., Carpenter, W.T., 1984. The Quality of Life Scale: an instrument
for rating the schizophrenic deficit syndrome. Schizophr. Bull. 10, 388–98.
Initiative, N.G., 1992. Family Interview for Genetic Studies. NIMH, Rockville, MD.
Lin, A., Wood, S.J., Nelson, B., Beavan, A., McGorry, P., Yung, A.R., 2015. Outcomes of
nontransitioned cases in a sample at ultra-high risk for psychosis. Am. J. Psychiatry 172,
249–258. doi:10.1176/appi.ajp.2014.13030418
Lincoln, T.M., Dollfus, S., Lyne, J., 2016. Current developments and challenges in the
assessment of negative symptoms. Schizophr. Res. doi:10.1016/j.schres.2016.02.035
Markulev, C., McGorry, P.D., Nelson, B., Yuen, H.P., Schaefer, M., Yung, A.R., Thompson,
A.D., Berger, G.E., Mossaheb, N., Schlögelhofer, M., Smesny, S., de Haan, L., Riecher-
Rössler, A Nordentoft, M., Chen, E., Verma, S., Hickie, I., Amminger, P., 2015. The
NEURAPRO-E Study Protocol: A Multicenter RCT of Omega-3 Fatty Acids and
Cognitive-Behavioural Case Management for Patients at Ultra High Risk of Schizophrenia
and Other Psychotic Disorders. Early Interv. Psychiatry In Press,.
McGorry, P.D., Hickie, I.B., Yung, A.R., Pantelis, C., Jackson, H.J., 2006. Clinical staging of
psychiatric disorders: a heuristic framework for choosing earlier, safer and more effective
15

interventions. Aust. N. Z. J. Psychiatry 40, 616–22. doi:10.1111/j.1440-1614.2006.01860.x
McGorry, P.D., Nelson, B., 2016. Why we need a transdiagnostic staging approach to emerging
psychopathology, early diagnosis, and treatment. JAMA Psychiatry 73, 191–192.
doi:10.1001/jamapsychiatry.2015.2868
McGorry, P.D., Nelson, B., Markulev, C., Yuen, H.P., Schäfer, M.R., Mossaheb, N.,
Schlögelhofer, M., Smesny, S., Hickie, I.B., Berger, G.E., Chen, E.Y.H., de Haan, L.,
Nieman, D.H., Nordentoft, M., Riecher-Rössler, A., Verma, S., Thompson, A., Yung, A.R.,
Amminger, G.P., 2017. Effect of ω-3 Polyunsaturated Fatty Acids in Young People at
Ultrahigh Risk for Psychotic Disorders. JAMA Psychiatry 74, 19.
doi:10.1001/jamapsychiatry.2016.2902
McGorry, P.D., Yung, A.R., Phillips, L.J., Yuen, H.P., Francey, S., Cosgrave, E.M., Germano,
D., Bravin, J., McDonald, T., Blair, A., Adlard, S., Jackson, H., 2002. Randomized
controlled trial of interventions designed to reduce the risk of progression to first-episode
psychosis in a clinical sample with subthreshold symptoms. Arch. Gen. Psychiatry 59, 921–
8.
Nelson, B., Yuen, H.P., Lin, A., Wood, S.J., McGorry, P.D., Hartmann, J.A., Yung, A.R., 2016.
Further examination of the reducing transition rate in ultra high risk for psychosis samples:
The possible role of earlier intervention. Schizophr. Res. 174, 43–9.
doi:10.1016/j.schres.2016.04.040
Nelson, B., Yuen, H.P., Wood, S.J., Lin, A., Spiliotacopoulos, D., Bruxner, A., Broussard, C.,
Simmons, M., Foley, D.L., Brewer, W.J., Francey, S.M., Amminger, G.P., Thompson, A.,
McGorry, P.D., Yung, A.R., 2013. Long-term follow-up of a group at ultra high risk
16

(“prodromal”) for psychosis: the PACE 400 study. JAMA psychiatry 70, 793–802.
doi:10.1001/jamapsychiatry.2013.1270
Nelson, B., Yuen, K., Yung, a. R., 2011. Ultra high risk (UHR) for psychosis criteria: Are there
different levels of risk for transition to psychosis? Schizophr. Res. 125, 62–68.
doi:10.1016/j.schres.2010.10.017
Overall, J.E., Gorhum, D.R., 1962. The Brief Psychiatric Rating Scale. Psychol. Rep. 10, 799–
812. doi:10.2466/pr0.1962.10.3.799
Phillips, L.J., Nelson, B., Yuen, H.P., Francey, S.M., Simmons, M., Stanford, C., Ross, M.,
Kelly, D., Baker, K., Conus, P., Amminger, P., Trumpler, F., Yun, Y., Lim, M., McNab, C.,
Yung, A.R., McGorry, P.D., 2009. Randomized controlled trial of interventions for young
people at ultra-high risk of psychosis: study design and baseline characteristics. Aust. N. Z.
J. Psychiatry 43, 818–29. doi:10.1080/00048670903107625
Rutigliano, G., Valmaggia, L., Landi, P., Frascarelli, M., Cappucciati, M., Sear, V., Rocchetti,
M., De Micheli, A., Jones, C., Palombini, E., McGuire, P., Fusar-Poli, P., 2016a.
Persistence or recurrence of non-psychotic comorbid mental disorders associated with 6-
year poor functional outcomes in patients at ultra high risk for psychosis. J. Affect. Disord.
203, 101–110. doi:10.1016/j.jad.2016.05.053
Rutigliano, G., Valmaggia, L., Landi, P., Frascarelli, M., Cappucciati, M., Sear, V., Rocchetti,
M., De Micheli, A., Jones, C., Palombini, E., McGuire, P., Fusar-Poli, P., 2016b.
Persistence or recurrence of non-psychotic comorbid mental disorders associated with 6-
year poor functional outcomes in patients at ultra high risk for psychosis. J. Affect. Disord.
203, 101–110. doi:10.1016/j.jad.2016.05.053
17

Schultze-lutter, F., Michel, C., Schmidt, S.J., Schimmelmann, B.G., Maric, N.P., Gaag, M. Van
Der, Nordentoft, M., Raballo, A., Meneghelli, A., Marshall, M., Morrison, A., Ruhrmann,
S., Klosterko, J., 2015. Original article EPA guidance on the early detection of clinical high
risk states of psychoses 30, 405–416. doi:10.1016/j.eurpsy.2015.01.010
Seidman, L.J., Giuliano, A.J., Meyer, E.C., Addington, J., Cadenhead, K.S., Cannon, T.D.,
McGlashan, T.H., Perkins, D.O., Tsuang, M.T., Walker, E.F., Woods, S.W., Bearden, C.E.,
Christensen, B.K., Hawkins, K., Heaton, R., Keefe, R.S.E., Heinssen, R., Cornblatt, B.A.,
2010. Neuropsychology of the prodrome to psychosis in the NAPLS consortium:
relationship to family history and conversion to psychosis. Arch. Gen. Psychiatry 67, 578–
88. doi:10.1001/archgenpsychiatry.2010.66
Shah, J.L., Crawford, A., Mustafa, S.S., Iyer, S.N., Joober, R., Malla, A.K., 2017. Is the Clinical
High-Risk State a Valid Concept? Retrospective Examination in a First-Episode Psychosis
Sample. Psychiatr. Serv. appi.ps.2016003. doi:10.1176/appi.ps.201600304
Simon, A.E., Umbricht, D., Lang, U.E., Borgwardt, S., 2014. Declining transition rates to
psychosis: the role of diagnostic spectra and symptom overlaps in individuals with
attenuated psychosis syndrome. Schizophr. Res. 159, 292–8.
doi:10.1016/j.schres.2014.09.016
Simon, A.E., Velthorst, E., Nieman, D.H., Linszen, D., Umbricht, D., de Haan, L., 2011. Ultra
high-risk state for psychosis and non-transition: a systematic review. Schizophr. Res. 132,
8–17. doi:10.1016/j.schres.2011.07.002
Thompson, K.N., Phillips, L.J., Komesaroff, P., Yuen, H.P., Wood, S.J., Pantelis, C., Velakoulis,
D., Yung, A.R., McGorry, P.D., 2007. Stress and HPA-axis functioning in young people at
18

ultra high risk for psychosis. J. Psychiatr. Res. 41, 561–9.
doi:10.1016/j.jpsychires.2006.05.010
van der Gaag, M., Smit, F., Bechdolf, A., French, P., Linszen, D.H., Yung, A.R., McGorry, P.,
Cuijpers, P., 2013. Preventing a first episode of psychosis: meta-analysis of randomized
controlled prevention trials of 12 month and longer-term follow-ups. Schizophr. Res. 149,
56–62. doi:10.1016/j.schres.2013.07.004
van Os, J., Guloksuz, S., 2017. A critique of the “ultra-high risk” and “transition” paradigm.
World Psychiatry 16, 200–206.
van Prooijen, J.-W., Karremans, J.C., van Beest, I., 2006. Procedural justice and the hedonic
principle: how approach versus avoidance motivation influences the psychology of voice. J.
Pers. Soc. Psychol. 91, 686–697. doi:10.1037/0022-3514.91.4.686
Wiltink, S., Velthorst, E., Nelson, B., McGorry, P.M., Yung, A.R., 2015. Declining transition
rates to psychosis: the contribution of potential changes in referral pathways to an ultra-
high-risk service. Early Interv. Psychiatry 9, 200–6. doi:10.1111/eip.12105
Yung, A.R., McGorry, P.D., 1996a. The prodromal phase of first-episode psychosis: past and
current conceptualizations. Schizophr. Bull. 22, 353–70.
Yung, A.R., McGorry, P.D., 1996b. The Initial Prodrome in Psychosis: Descriptive and
Qualitative Aspects. Aust. New Zeal. J. Psychiatry 30, 587–599.
doi:10.3109/00048679609062654
Yung, A.R., McGorry, P.D., McFarlane, C.A., Jackson, H.J., Patton, G.C., Rakkar, A., 1996.
Monitoring and Care of Young People at Incipient Risk of Psychosis. Schizophr. Bull. 22,
19

283–303. doi:10.1093/schbul/22.2.283
Yung, A.R., Phillips, L.J., Nelson, B., Francey, S.M., PanYuen, H., Simmons, M.B., Ross, M.L.,
Kelly, D., Baker, K., Amminger, G.P., Berger, G., Thompson, A.D., Thampi, A., McGorry,
P.D., 2011. Randomized controlled trial of interventions for young people at ultra high risk
for psychosis: 6-month analysis. J. Clin. Psychiatry 72, 430–40.
doi:10.4088/JCP.08m04979ora
Yung, A.R., Phillips, L.J., Yuen, H.P., Francey, S.M., McFarlane, C.A., Hallgren, M., McGorry,
P.D., 2003. Psychosis prediction: 12-month follow up of a high-risk (“prodromal”) group.
Schizophr. Res. 60, 21–32.
Yung, A.R., Phillips, L.J., Yuen, H.P., McGorry, P.D., 2004. Risk factors for psychosis in an
ultra high-risk group: Psychopathology and clinical features. Schizophr. Res. 67, 131–142.
doi:10.1016/S0920-9964(03)00192-0
Yung, A.R., Woods, S.W., Ruhrmann, S., Addington, J., Schultze-lutter, F., Cornblatt, A.,
Amminger, G.P., Bechdolf, A., Birchwood, M., Borgwardt, S., Cannon, T.D., 2012.
Whither the Attenuated Psychosis Syndrome ? 38, 1130–1134. doi:10.1093/schbul/sbs108
Yung, A.R., Yuen, H.P., Berger, G., Francey, S., Hung, T.-C., Nelson, B., Phillips, L., McGorry,
P., 2007. Declining transition rate in ultra high risk (prodromal) services: dilution or
reduction of risk? Schizophr. Bull. 33, 673–81. doi:10.1093/schbul/sbm015
Yung, A.R., Yuen, H.P., McGorry, P.D., Phillips, L.J., Kelly, D., Dell’Olio, M., Francey, S.,
Cosgrove, E., Killackey, E., Stanford, C., Godfrey, K., Buckby, J., 2005. Mapping the onset
of psychosis: The comprehensive assessment of at risk mental states (CAARMS).
20

Schizophr. Res. 60, 30–31. doi:10.1016/S0920-9964(03)80090-7
Zubin, J., 1985. Negative Symptoms: Are they indigenous to Schizophrenia. Schizophr. Bull. 11,
461–470.
Table 1.Criteria for assessing Ultra-High-Risk for psychosis status from 1995 to 2013.
Criteria/Measure Attenuated Psychotic Symptoms (APS)
Brief limited intermittent psychotic symptoms (BLIPS)
Trait and state risk factors (Trait)
Symptom/Trait requirement
Presence of attenuated (subthreshold) positive psychotic symptoms within past 12 months
Presence of frank psychotic symptoms for < 1 week within the past 12 months, which spontaneously resolve (i.e., without treatment)
Presumed genetic vulnerability based on presence of schizotypal personality disorder or a first-degree relative with a psychotic disorder
Measures 1995-1999-BPRS/CASH(Yung et al., 2003, 1996)2000-2006 - CAARMS
1995-1999- BPRS/CASH(Yung et al., 2003, 1996)2000-2006 - CAARMS
1995-2013 - FIGS and SCID-II
Drop in functioning/ sustained low functioning required
1995-2006: N/A2010-2013:30% drop in SOFAS score for a month within the past year OR SOFAS score of 50 or less for the past 12 months or longer.
1995-2006: N/A2010-2013:30% drop in SOFAS score for a month within the past year OR SOFAS score of 50 or less for the past 12 months or longer.
1995-2006: 30% drop in GAF score within the past 12 months OR GAF score of 50 or less for the past 12 months or longer.2010-2013:30% drop in SOFAS score for a month within the past year OR SOFAS score of 50 or less for the past 12 months or longer.
Note: BPRS = Brief Psychiatric Rating Scale(Overall and Gorhum, 1962); CASH = Comprehensive Assessment of
Symptoms and History(Andreasen et al., 1992);CAARMS = Comprehensive Assessment of at-risk Mental
21

States(Yung et al., 2005); FIGS = Family Interview for Genetic Studies(Initiative, 1992); SCID-II = Structured
Clinical Interview for DSM-III-R/DSM-IV Personality Disorders (First et al., 1997, 1995).
22

Table 2.Baseline sample characteristics across the 4 UHR risk groups: Trait-only, APS-only, Trait+APS and Any BLIPS
Participant characteristics
Trait-only
n= 78
APS-only
n = 449
Trait+APS
n = 105
Any BLIPS
n = 70
Statistic P value N
Age at baseline 20.79 (4.71) 19.02 (3.64) 19.98 (3.90) 20.14 (4.32) F(3, 698) = 6.10 <.001 702
Gender (% male) 40 (50.6%) 205 (45.7%) 46 (44.2%) 35 (50.0%) χ2(3) = 1.23 .743 702
Baseline year (N, %)
1995 – 1999 (n = 161)
2000 – 2006 (n = 237)
2010-2013 (n = 304)
25 (15.5%)
30 (12.7%)
23 (7.6%)
69 (42.9%)
149 (62.9%)
231 (76.0%)
27 (16.8%)
42 (17.7%)
36 (11.8%)
40 (24.8%)
16 (6.8%)
14 (4.6%)
χ2(6) = 75.40 < .001 702
Time to follow-up interview
(years)
4.73 (4.10) 3.12 (3.32) 4.47 (4.04) 6.42 (4.50) F(3, 556) =
14.96
<.001 560
Duration of symptoms prior to
first contact with clinical
services (days), Mean (SD)
562.88
(1047.35)
677.46 (874.82) 664.87 (795.47) 487.37
(833.30)
F(3, 657) = 1.16 .325 661
Proportion receiving research
treatment (N, %) (vs treatment
as usual)
29 (36.7) 222 (49.4) 43 (41.3) 31 (44.3) χ2(3) = 5.85 .119 702
a.
23

Table 3. Transition to psychosis and SOFAS and diagnostic outcomes according to UHR risk group
Participant characteristics
Trait-only
n= 76
APS-only
n = 430
Trait+APS
n = 103
Any BLIPS
n = 69
Test Statistic P value N
SOFAS at follow-upa, Mean, SD 68.37 (17.40) 68.40 (15.87) 64.47 (15.32) 67.47 (18.38) F(3, 508) = 1.24 .293 3
Proportion with non-psychotic
Axis I disorders at follow-up
(N, %)b
28 (53.8) 216 (64.3) 47(64.4) 22 (50.0) χ2(3) = 2.49 .477 505
b. Group differences were examined with general linear model with and without including age at baseline and time to follow-up
as covariates. Inclusion of covariates did not affect the results. We therefore report results of models without covariates.
c. Test statistic reflects Wald test on the group coefficient in a logistic regression model including age at baseline and baseline
year as covariates.
24

25
Figure 1. Proportion of UHR sample recruited between 1995 to 1999 (N = 161), 2000 to 2006 (N = 237) and 2010 to 2013 (N = 304) that met criteria for Trait-only, APS-only, Trait+APS and any BLIPS.

26Figure 2. Mean symptom severity and psychosocial functioning at baseline and follow-up for UHR risk groups. Error bars reflect +/- 1 standard error of the mean (SEM). BPRS = Brief Psychiatric Rating Scale, SANS = Schedule for the Assessment of Negative Symptoms; QLS = Quality of Life Scale; GAF = Global Assessment of Functioning.