· Web viewThe association of cardiovascular disease with respiratory disease and impact on...
48
The association of cardiovascular disease with respiratory disease and impact on outcome. Paul Carter, MBChB; 1,2 Jakub Lagan, LEKARZ; 3,4 Christien Fortune, MBChB; 3 Deepak L Bhatt, MD; 5 Jørgen Vestbo, DrMedSci; 4,6 Robert Niven, MBChB; 4,6 Nazia Chaudhuri, PhD; 4,6 Erik B Schelbert, MD; 7-9 Rahul Potluri, MBChB; 1 Christopher A Miller, PhD. 3,4,10 Word count: 4996 Affiliations 1. ACALM Study Unit in collaboration with Aston Medical School, Aston University, Birmingham. 2. Cambridge Epidemiology Unit. Worts' Causeway, University of Cambridge, Cambridge CB1 8RN. 3. Division of Cardiovascular Sciences, School of Medical Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PL. 4. Manchester University NHS Foundation Trust, Wythenshawe Hospital, Southmoor Road, Wythenshawe, Manchester, M23 9LT. 5. Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, MA 6. Division of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PL 7. Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA 8. UPMC Cardiovascular Magnetic Resonance Center, Heart and Vascular Institute, Pittsburgh, PA, USA 9. Clinical and Translational Science Institute, University of Pittsburgh, Pittsburgh, PA, USA 10. Wellcome Centre for Cell-Matrix Research, Division of Cell- Matrix Biology & Regenerative Medicine, School of Biology, Faculty of Biology, Medicine & Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PT Funding: Dr Lagan is funded by a Clinical Research Training Fellowship from the British Heart Foundation (FS/17/47/32805). Dr Miller is funded 1
Transcript of · Web viewThe association of cardiovascular disease with respiratory disease and impact on...

The association of cardiovascular disease with respiratory disease and impact on outcome.
Paul Carter, MBChB;1,2 Jakub Lagan, LEKARZ;3,4 Christien Fortune, MBChB;3 Deepak L Bhatt, MD;5 Jørgen Vestbo, DrMedSci;4,6 Robert Niven, MBChB;4,6 Nazia Chaudhuri, PhD;4,6 Erik B Schelbert, MD;7-9 Rahul Potluri, MBChB;1 Christopher A Miller, PhD.3,4,10
Word count: 4996
Affiliations1. ACALM Study Unit in collaboration with Aston Medical School, Aston University,
Birmingham.2. Cambridge Epidemiology Unit. Worts' Causeway, University of Cambridge, Cambridge CB1
8RN.3. Division of Cardiovascular Sciences, School of Medical Sciences, Faculty of Biology, Medicine
and Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PL.
4. Manchester University NHS Foundation Trust, Wythenshawe Hospital, Southmoor Road, Wythenshawe, Manchester, M23 9LT.
5. Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, MA
6. Division of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PL
7. Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA8. UPMC Cardiovascular Magnetic Resonance Center, Heart and Vascular Institute, Pittsburgh,
PA, USA9. Clinical and Translational Science Institute, University of Pittsburgh, Pittsburgh, PA, USA10. Wellcome Centre for Cell-Matrix Research, Division of Cell-Matrix Biology & Regenerative
Medicine, School of Biology, Faculty of Biology, Medicine & Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PT
Funding: Dr Lagan is funded by a Clinical Research Training Fellowship from the British Heart Foundation (FS/17/47/32805). Dr Miller is funded by a Clinician Scientist Award (CS-2015-15-003) from the National Institute for Health Research. Dr Vestbo is supported by the National Institute for Health Research Manchester Biomedical Research Centre.
DisclosuresThe views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. Dr. Deepak L. Bhatt discloses the following relationships - Advisory Board: Cardax, Elsevier Practice Update Cardiology, Medscape Cardiology, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSoft; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic, Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee
1

funded by Boehringer Ingelheim), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), WebMD (CME steering committees); Other: Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), VA CART Research and Publications Committee (Chair); Research Funding: Abbott, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Eisai, Ethicon, Forest Laboratories, Idorsia, Ironwood, Ischemix, Lilly, Medtronic, PhaseBio, Pfizer, Regeneron, Roche, Sanofi Aventis, Synaptic, The Medicines Company; Royalties: Elsevier (Editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart Disease); Site Co-Investigator: Biotronik, Boston Scientific, St. Jude Medical (now Abbott), Svelte; Trustee: American College of Cardiology; Unfunded Research: FlowCo, Merck, Novo Nordisk, PLx Pharma, Takeda. Dr Nazia Chaudhuri discloses the following relationships - Advisory Board: Roche. Research grants: Roche and Boehringer Ingelheim. Professor Jørgen Vestbo discloses the following relationships - Consultancy for COPD Phase 2 and 3 program and payment for lectures including service in speaker bureau for GlaxoSmithKline, Chiesi Pharmaceuticals, Boehringer-Ingelheim, Novartis and AstraZeneca.
Address for correspondenceDr. Christopher A. Miller, Division of Cardiovascular Sciences, School of Medical Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, University of Manchester, Oxford Road, Manchester, M13 9PLTelephone: 0044 161 291 2034. Fax: 0044 161 291 2389Email: [email protected]: Lung disease is associated with cardiovascular diseases, which contribute significantly to all-cause mortality, independent of shared risk factorsTwitter handle: @DLBHATTMD
2

ABSTRACTBackground: The relationship between respiratory diseases and individual cardiovascular diseases, and the impact of cardiovascular diseases on mortality in patients with respiratory disease, are unclear.
Objectives: To determine the relationship between chronic obstructive pulmonary disease (COPD), asthma and interstitial lung disease (ILD), and individual cardiovascular diseases, and evaluate the impact of individual cardiovascular diseases on all-cause mortality in respiratory conditions.
Methods: Cohort study of all patients admitted to seven National Health Service hospitals across the North West of England, between January 1st 2000 and March 31st 2013 with relevant respiratory diagnoses, with age and gender matched control groups. Results: 31,646 COPD, 60,424 asthma and 1,662 ILD patients were included. Control groups comprised 158,230, 302,120 and 8,310 patients respectively (total follow up 2,968,182 patient-years). COPD was independently associated with ischemic heart disease (IHD), heart failure (HF), atrial fibrillation and peripheral vascular disease, all of which were associated with all-cause mortality (e.g. odds ratio for the association of COPD with HF 2.18 [95% confidence interval 2.08-2.26]; hazard ratio (HR) for the contribution of HF to mortality in COPD 1.65 [1.61-1.68]). Asthma was independently associated with IHD, and multiple cardiovascular diseases contributed to mortality (e.g. HF HR 1.81 [1.75-1.87]). ILD was independently associated with IHD and HF, both of which were associated with mortality. Patients with lung disease were less likely to receive coronary revascularization.
Conclusions: Lung disease is independently associated with cardiovascular diseases, particularly IHD and HF, which contribute significantly to all-cause mortality. However, patients with lung disease are less likely to receive coronary revascularization.
CONDENSED / UNSTRUCTURED ABSTRACT:The relationship between respiratory diseases and individual cardiovascular diseases, and their impact on patient outcome, is unclear. We conducted a cohort study of patients with chronic obstructive pulmonary disease, asthma and interstitial lung disease (2,968,182 patient-years follow-up). Lung disease was independently associated with cardiovascular diseases, particularly ischemic heart disease and heart failure, which contributed significantly to all-cause mortality, independent of shared risk factors. However, patients with lung disease were less likely to receive coronary revascularization.
KEY WORDSIschemic heart disease, heart failure, chronic obstructive pulmonary disease, asthma, interstitial lung fibrosis
3

ABBREVIATIONSACALM - Algorithm for Comorbidities, Associations, Length of stay, and MortalityAF – Atrial fibrillationCABG - Coronary artery bypass graftingCI – Confidence intervalCKD - Chronic kidney diseaseCOPD – Chronic obstructive pulmonary diseaseIHD - Ischemic heart diseaseILD - Interstitial lung diseaseNHS - National Health ServicePCI - Percutaneous coronary interventionPVD - Peripheral vascular diseaseT1DM - Type 1 diabetes mellitus
4

INTRODUCTION
Respiratory and cardiovascular disease frequently co-exist. Whilst shared risk factors are common,
it has become clear that the association between chronic obstructive pulmonary disease (COPD) and
cardiovascular disease is independent of these risk factors; indeed, the relationship between severity
of airflow obstruction and cardiovascular disease prevalence and mortality is now well established
(1,2).
The relationships between asthma, characterised by variable airway obstruction, or interstitial lung
disease (ILD), characterised by restrictive lung function, with cardiovascular disease, are less well
defined. Furthermore, the association between respiratory diseases and individual cardiovascular
diseases, which comprise a range of conditions with differing mechanisms and manifestations, is
not well characterised. Moreover, while there are extensive data to show that lung diseases,
particularly COPD (3,4), adversely affect the prognosis of patients with cardiovascular diseases,
few studies have investigated the impact of individual cardiovascular diseases on mortality in
patients with lung diseases.
In this study we aimed to investigate the association between COPD, asthma and ILD, with
individual cardiovascular diseases, and evaluate the impact of individual cardiovascular diseases on
all-cause mortality in these lung conditions, using a large cohort of patients admitted to National
Health Service (NHS) hospitals across the North West of England, UK over a 13-year period.
5

METHODS
Data sources and study population
The study population comprised all patients admitted to seven National Health Service (NHS)
hospitals across the North West of England, UK at least once between January 1st 2000 and March
31st 2013. Anonymised discharge data including diagnoses, comorbidities and procedures were
obtained from the NHS Local Health Authority computerized hospital activity analysis register. The
Algorithm for Comorbidities, Associations, Length of stay, and Mortality (ACALM) study protocol
was subsequently applied to transfer this raw data into an analyzable research database. The
ACALM protocol utilizes the concept of amalgamation of routinely collected data and advances the
concept of the use of big data in medical research, and has been as previously described in
numerous publications (5-7). The ACALM protocol eliminates the possibility of patients being
counted twice. First admission data are used for patients with multiple admissions.
The three study groups comprised all adult patients (≥ 18 years old) with a diagnosis of COPD,
asthma and ILD respectively. Patients were identified using International Classification of Disease
10th edition (ICD-10) and Office of Population Censuses and Surveys Classification of
Interventions and Procedures (OPCS-4) coding systems. Data regarding an additional study group
with asthma-COPD overlap (ACO) are presented in the supplemental file.
Age and sex matched control groups for each of the three study groups were formed independently
from the main study population. SPSS was used to randomly select patients without diagnoses of
COPD, asthma or ILD. Control groups were matched for sex in age deciles for each study group.
Control groups were made five times larger than their corresponding study groups.
Outcomes
6

Cardiovascular diseases (hypertension, hyperlipidaemia, type 1 or type 2 diabetes mellitus, ischemic
heart disease (IHD), heart failure, atrial fibrillation, peripheral vascular disease or cerebrovascular
disease) and cardiac procedures (percutaneous coronary intervention (PCI) or coronary artery
bypass grafting (CABG)) were identified using ICD-10 and OPCS-4 coding as part of the ACALM
study protocol. In addition, diagnoses of the other conditions in the top 10 most common causes of
death in the UK aside from cardiovascular diseases and COPD (i.e. lung cancer, breast cancer,
colon cancer, pneumonia, chronic kidney disease (CKD) and dementia) were identified using ICD-
10 and OPCS-4 coding. Data regarding diagnoses of respiratory disease, cardiovascular disease and
the other common causes of death, as well as age, sex and ethnicity, were available for all patients.
The ACALM algorithm captures tobacco use from ICD-10 coding; however, the NHS hospital
activity analysis register usually records tobacco use using a separate demographic field. Therefore,
tobacco use is substantially under-recorded by the ACALM algorithm. We report tobacco use,
however it was excluded from regression analyses in the main manuscript. Multivariable regression
analysis that includes tobacco use is presented in the supplemental file.
Mortality status at the end of the study period (March 31st 2013) was determined by record linkage
to the National Health Tracing Services (NHS Strategic Tracing Service) which utilizes data from
the UK Office for National Statistics. Mortality status was available for all patients.
Statistical Analysis
Nominal baseline characteristics including the unadjusted prevalence of cardiovascular diseases
were compared between each respiratory group and their respective control group using Chi square
(χ2) tests. Continuous variables were compared using independent t tests. To determine the
relationship between each respiratory condition and cardiovascular disease, logistic regression was
7

used to calculate odds ratios and 95% confidence intervals. Multivariable models included
adjustments for age, sex, ethnic group and the cardiovascular diseases, cardiac procedures and
common causes of death stated above. To determine the relationship between cardiovascular
disease and death in each respiratory condition, multivariable Cox regression models were used to
calculate hazard ratios (HR) and 95% confidence intervals adjusted for age, sex, ethnic group and
the other cardiovascular diseases, cardiac procedures and common causes of death stated above.
Kaplan-Meier curves were used to illustrate the impact of cardiovascular diseases on survival. All p
values were 2-sided and a level of less than 0.05 was considered significant. Analyses were
performed using SPSS version 21.0 (IBM).
8

RESULTS
Study Population
Between January 1st 2000 and March 31st 2013, 1,220,024 patients were admitted to the seven
hospitals included in the study. Of these patients, 31,646 patients (2.59%) had COPD, 60,424
(4.95%) had asthma and 1,662 (0.14%) had ILD at baseline. Control groups comprised 158,230
patients, 302,120 patients and 8,310 patients for the COPD, asthma and ILD groups respectively.
Baseline characteristics of patients with each respiratory condition and their matched controls are
presented in Table 1. Mean follow up was 5.2 ± 3.6 years (2,968,182 patient-years).
COPD
The unadjusted prevalence of cardiovascular diseases was higher among patients with COPD than
among controls at baseline (Table 1). Rates of pneumonia and lung cancer were also higher.
In multivariable analysis (Table 2), COPD was independently associated with IHD (odds ratio [OR]
1.74; 95% confidence interval [CI] 1.69-1.80), heart failure (OR 2.17; 95% CI 2.08-2.26), AF (OR
1.39; 95% CI 1.34-1.44) and peripheral vascular disease (OR 1.85; 95% CI 1.74-2.00). COPD was
not independently associated with cerebrovascular disease (OR 0.97; 95% CI 0.92-1.03).
During study follow-up 16,812 patients (53.1%) with COPD died, compared with 46,873 (29.6%)
matched controls (p < 0.001). In multivariable Cox regression, IHD (HR 1.03; 95% CI 1.01-1.05),
heart failure (HR 1.65; 95% CI 1.61-1.68), AF (HR 1.08; 95% CI 1.06-1.10), cerebrovascular
disease (HR 1.84; 95% CI 1.80-1.89) and peripheral vascular disease (HR 1.32; 95% CI 1.27-1.37)
were independently associated with death in patients with COPD (Table 3 and Figure 1).
Despite the higher prevalence of IHD, patients with COPD were less likely to receive coronary
9

revascularization, either via percutaneous coronary intervention (PCI) (OR 0.48; 95% CI 0.44-0.54)
or coronary artery bypass grafting (CABG) (OR 0.42; 95% CI 0.36-0.49), but coronary
revascularization was associated with a lower rate of death (PCI HR 0.35; 95% CI 0.32-0.39;
CABG HR 0.52; 95% CI 0.46-0.58)
Asthma
The unadjusted prevalence of hypertension, hyperlipidaemia, type II diabetes, IHD, heart failure,
and AF was higher among patients with asthma than among controls at baseline (Table 1). Rate of
pneumonia was also higher.
In multivariable analysis (Table 2), asthma was independently associated with IHD (OR 1.48; 95%
CI 1.44-1.53). Asthma was not independently associated with heart failure (OR 1.06; 95% CI 1.00-
1.12) or AF (OR 1.02; 95% CI 0.97-1.07) and was associated with lower rates of cerebrovascular
disease (OR 0.77; 95% CI 0.72-0.82) and peripheral vascular disease (OR 0.79; 95% CI 0.72-0.87).
During study follow-up 6,649 patients (11.0%) with asthma died, compared with 36,624 (12.1%)
matched controls (p < 0.001). In multivariable Cox regression, IHD (HR 1.04; 95% CI 1.01-1.07),
heart failure (HR 1.81; 95% CI 1.75-1.87), AF (HR 1.07; 95% CI 1.04-1.10), cerebrovascular
disease (HR 2.10; 95% CI 2.03-2.17) and peripheral vascular disease (HR 1.39; 95% CI 1.32-1.47)
were independently associated with death in patients with asthma (Table 3 and Figure 2).
Despite the higher prevalence of IHD, patients with asthma were less likely to receive coronary
revascularization, either via PCI (OR 0.75; 95% CI 0.70-0.82) or CABG (OR 0.60; 95% CI 0.53-
0.67), but coronary revascularization was associated with a lower rate of death (PCI HR 0.41; 95%
CI 0.37-0.47; CABG HR 0.57; 95% CI 0.50-0.65).
10

ILD
The unadjusted prevalence of type II diabetes, IHD, heart failure and AF were higher among
patients with ILD than among controls at baseline (Table 1). Rates of pneumonia and lung cancer
were also higher.
In multivariable analysis (Table 2), ILD was independently associated with IHD (OR 1.57; CI 1.37-
1.81) and heart failure (OR 2.23; 95% CI 1.88-2.66). ILD was not independently associated with
AF (OR 1.10; 95% CI 0.93-1.30) or peripheral vascular disease (OR 1.09; 95% CI 0.78-1.52). ILD
was associated with lower rates of cerebrovascular disease (OR 0.61; 95% CI 0.47-0.78).
During study follow-up 1,149 patients (69.1%) with ILD died, compared with 2737 (32.9%)
matched controls (p < 0.001). In multivariable Cox regression, IHD (HR 1.10; 95% CI 1.02-1.19),
heart failure (HR 1.59; 95% CI 1.45-1.74), cerebrovascular disease (HR 1.89; 95% CI 1.70-2.09)
and peripheral vascular disease (HR 1.27; 95% CI 1.07-1.50) were independently associated with
death in patients with ILD (Table 3 and Figure 3).
Despite the higher prevalence of IHD, patients with ILD were less likely to receive coronary
revascularization, either via PCI (OR 0.42; 95% CI 0.25-0.71) or CABG (OR 0.47; 95% CI 0.25-
0.87), but coronary revascularization was associated with a lower rate of death (PCI HR 0.43; 95%
CI 0.28-0.66; CABG HR 0.43; 95% CI 0.26-0.70).
Asthma-COPD overlap
Results are presented in the supplemental file.
11

Tobacco Use
Tobacco use was recorded in 9.2% of patients with COPD compared to 1.8% of the COPD control
population (5.11 fold higher). In patients with asthma, tobacco use was 5% compared to 2.7% in the
asthma control group (1.85 fold higher) and in patients with ILD, tobacco use was 2.8% compared
to 1.5% in the ILD control group (1.86 fold higher). Multivariable-adjusted associations of
cardiovascular diseases with each respiratory disease, including adjustment for tobacco use, are
presented in the supplemental file (Table S4).
12

DISCUSSION
In this study, we found COPD, asthma and ILD to be strongly and independently associated with
cardiovascular diseases. Furthermore, cardiovascular diseases were independently and often
strongly associated with all-cause mortality in patients with lung diseases. Despite these findings,
patients with COPD, asthma and ILD were less likely to receive coronary revascularization than
patients without these lung conditions. Strengths of this study include its prospective design, large
sample, length of follow-up and completeness of mortality status. We used all-cause mortality
because cause of death reporting is often inaccurate in lung conditions (8).
The association between ILD and IHD seen in our study, by far the largest to investigate this
relationship, is in keeping with the findings of smaller previous studies (9,10). Importantly, our
study is the first to demonstrate that IHD is independently associated with all-cause mortality in
patients with ILD. Higher unadjusted rates of heart failure have been observed in patients with ILD
compared with patients without ILD (11), but our study is the first to demonstrate an independent
association between ILD and heart failure, and in addition, the first to show that heart failure is
independently associated with all-cause mortality in ILD, with an associated 1.6 fold increased risk.
We found ILD was not independently associated with AF, which is in keeping with a previous
smaller study by Hubbard et al (10), and additionally found, for the first time, that AF did not
contribute significantly to death in ILD. In the first study to investigate the relationship between
ILD and peripheral vascular disease, we found ILD was not associated with peripheral vascular
disease.
The association between asthma and IHD found in our study is in keeping with the findings of
recent meta-analyses (12,13). However, our study is the first to demonstrate that IHD is
independently associated with all-cause mortality in patients with asthma, albeit the association was
13

relatively small. Unlike the study by Iribarren et al (14), we did not find an independent association
between asthma and heart failure, although the rate of heart failure in our asthma and asthma
control cohorts was 3.3 times higher than that in the study by Iribarren et al. We did find heart
failure conferred a highly increased risk of death. The relationship between asthma and
cerebrovascular disease has been inconsistent across previous studies and we found patients with
asthma had lower rates of cerebrovascular disease than non-asthmatic patients, after multivariable
adjustment (14,15). Our study is by far the largest to investigate the relationship between asthma
and peripheral vascular disease and asthma and AF, and the first to investigate their contribution to
mortality, showing that asthma is not independently associated with either condition, but both
contribute significantly to all-cause mortality.
The unadjusted prevalence and adjusted risk of IHD and heart failure in patients with COPD in our
study are in keeping with those reported in a recent systematic review (16). There is substantially
less data regarding the relationship between COPD and peripheral vascular disease, and COPD and
AF, but the independent associations with both peripheral vascular disease and AF found in our
study are in keeping with the findings of previous smaller studies (17,18). A variable relationship
has been observed across the published literature between COPD and cerebrovascular disease and
we did not find an independent association (17,19,20).
Our findings regarding the impact of IHD and heart failure on mortality in patients with COPD are
in keeping with those of Sidney et al (21), who found myocardial infarction and heart failure were
independently associated with all-cause mortality in patients with COPD, although Sidney et al did
not adjust for other causes of death and follow-up in our study was considerably longer. Our study
is the first to investigate the impact of AF and peripheral vascular disease on all-cause mortality in
14

COPD, finding that AF and peripheral vascular disease are associated with 1.1- and 1.3-fold higher
risks of death respectively.
Population prevalence of tobacco use in UK adults is reported as 17.2% (22). Therefore, while we
were able to identify variations in tobacco use in patients with COPD, asthma, and ILD compared to
their respective control groups, tobacco use was substantially under-recorded, the reason for which
is described in the Methods section. Recent UK data found 89.4% of COPD patients had a current
or past history of smoking, which is 5.2 fold higher than the population prevalence (23). This is
very similar to the difference in tobacco use (5.1 fold higher) between COPD and COPD control
groups in our study. Similar findings are found in the Asthma and ILD groups. As such, the under-
reporting of tobacco use in our study appears to be consistent across the whole study population
rather than being disease specific. Nevertheless, the observed associations between lung diseases
and cardiovascular diseases persisted after adjusting for tobacco use.
The risk and impact of heart failure in lung disease was found to be particularly strong and is
independent of the increased risk of IHD. Myocardial inflammation occurring as part of systemic
inflammation, with subsequent interstitial myocardial fibrosis, which in turn leads to mechanical,
electrical and vasomotor dysfunction of the myocardium, is a widely held pathophysiological
hypothesis (24). Circulating inflammatory biomarkers are strongly associated with heart failure in
COPD (25). Myocardial injury (elevated troponin level) is observed in chronic stable COPD, the
magnitude of which is determined by immune activation (26), and inflammatory biomarkers are
independently associated with natriuretic peptide levels (27). López-Sánchez et al found patients
with COPD and LV diastolic dysfunction had significantly higher levels of circulating
inflammatory and fibrotic biomarkers compared to COPD patients without diastolic dysfunction
(28), and collagen remodeling biomarkers are associated with increased mortality (29).
15

Interestingly, targeted anti-inflammatory therapy may reduce cardiovascular events and incident
lung cancer (30). However, the relationship between lung disease, inflammation and heart failure is
inconsistent and mechanisms extrinsic to the myocardium, such as reduced left ventricular pre-load
secondary to pulmonary dysfunction, increased after-load due to arterial stiffness and autonomic
dysfunction, have been proposed (31,32). In particular, COPD exacerbations are associated with
increased arterial stiffness and frequent exacerbations are associated with chronically elevated
arterial stiffness, possibly mediated by loss of elastic connective tissue (32).
The role of inflammation in ILD is less clear. Nevertheless, following the initial injury, many of the
molecular (e.g. transforming growth factor β, angiotensin II, endothelin-1, extracellular regulated
kinase 1/2 and matrix metalloproteinases), and cellular (proliferation and transdifferentiation of
fibroblasts, collagen secretion) fibrotic mechanisms are common to pulmonary and myocardial
tissue (33). Diastolic dysfunction is observed in ILD and it may be that myocardial fibrosis
contributes to the association between ILD and heart failure, although this requires investigation
(34). The nature of heart failure associated with lung disease (i.e. reduced versus preserved ejection
fraction) remains poorly characterised.
Multiple mechanisms have been proposed to explain the link between lung disease and IHD.
Subclinical atherosclerosis is observed early in the COPD disease process and is related to
circulating markers of systemic inflammation (35). Impaired endothelial-dependent and
independent vasodilatation is observed in patients with COPD without cardiovascular disease, the
severity of which is related to systemic inflammation (36). Vijayakumar et al demonstrated
increased arterial inflammation in patients with asthma using 18F-fluorodeoxyglucose positron
emission tomography, which remained significant after adjusting for traditional cardiovascular risk
factors, and which was related to severity of airflow obstruction (37). Plasma fibrinogen is
16

chronically elevated in COPD and increases further during acute exacerbations, asthma is
associated with platelet activation and inhibition of fibrinolysis and clotting cascade activation is
observed in ILD (38). Nevertheless, the design and size of our study allows the relationship
between lung disease and other vascular disease (peripheral and cerebral) to be investigated
concurrently, and it shows that while there is a consistent association between the lung conditions
studied and IHD, the association with other vascular disease is inconsistent or indeed not present.
This suggests that if there is an underlying systemic process, it may have a differential effect
according to vascular location.
Despite the association with IHD and its impact on outcome, patients with the studied lung diseases
were less likely to undergo coronary revascularization than patients without lung diseases. Patients
with lung disease are generally underrepresented in trials and it may be that guidelines are
perceived to be less valid in this group (39). Elevated troponins may be attributed to decreased
oxygen supply (type 2 myocardial infarction) rather than a pathologic coronary artery process (type
I), albeit with similar associated risk. Patients with COPD have higher in hospital mortality and
higher rates of adverse cardiac events following PCI, and higher rates of postoperative pulmonary
infections and longer length of hospital stay following CABG, compared with patients without
COPD (40). Perhaps reflecting these data, in our study, patients receiving revascularization were
generally younger and had fewer co-morbidities (supplemental Table S5). While the SYNTAX
Score II generally favors PCI over CABG in patients with COPD, we found similarly low rates for
both (41).
There has been a long-standing debate about the safety of particularly long-acting beta-agonists in
asthma (42), with the FDA adding a black box warning in 2006. The FDA required large post-
marketing studies to evaluate this risk and following the findings from 4 studies including 41,297
17

patients, the black box was removed in December 2017 (43). In COPD there has also been a
concern surrounding both the use of inhaled long-acting beta-agonists and long-acting
anticholinergics. The concern regarding beta-agonists were laid to rest by the SUMMIT trial (44,45)
and the TIOSPIR trial could not replicate the risk of cardiovascular death (46) suggested by a
previous meta-analysis (47).
Limitations
The study is limited by its observational cohort design. There may be residual confounding; in
particular, tobacco use was under-recorded as discussed, although a multivariable adjustment
including tobacco use was performed. The cardiovascular and respiratory diagnoses rely on the
disease coding of the individual hospitals involved, although these data are determined by the
diagnoses made by the treating physicians and are what the hospitals and the NHS use for
operational purposes (e.g. reimbursement and performance evaluation). Our data are limited to
hospitalized patients whereas most COPD and asthma exacerbations are treated in an outpatient
setting; thus, our findings are more likely to be driven by patients with more advanced lung disease.
Data regarding antihypertensive, lipid-lowering and smoking cessation therapy, as well as the type
of heart failure (i.e., reduced versus preserved ejection fraction) were not available.
Conclusions
In conclusion, in a large cohort study, we found that COPD, asthma and ILD were independently
associated with cardiovascular diseases, and, cardiovascular diseases were independently associated
with all-cause mortality in these lung conditions. Despite these findings, patients with COPD,
asthma and ILD were less likely to receive coronary revascularization than patients without these
lung conditions.
18

Clinical perspectives
Competency in Medical Knowledge 1: COPD, ILD and asthma are independently associated with a
range of cardiovascular diseases, and, cardiovascular diseases are independently associated with all-
cause mortality in these lung conditions.
Competency in Medical Knowledge 2: Despite these associations, patients with lung conditions are
less likely to receive coronary revascularization.
Translational Outlook: Elucidation of the pathophysiological mechanisms underlying the
relationship between respiratory disease and cardiovascular disease is urgently required.
19

REFERENCES
1. Lange P, Mogelvang R, Marott JL, Vestbo Jr, Jensen JS. Cardiovascular Morbidity in
COPD. Copd 2010;7:5-10.
2. Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular
mortality. Chest 2005;127:1952-9.
3. Ather S, Chan W, Bozkurt B et al. Impact of noncardiac comorbidities on morbidity and
mortality in a predominantly male population with heart failure and preserved versus
reduced ejection fraction. J Am Coll Cardiol 2012;59:998-1005.
4. Rothnie KJ, Smeeth L, Herrett E et al. Closing the mortality gap after a myocardial
infarction in people with and without chronic obstructive pulmonary disease. Heart
2015;101:1103-1110.
5. Potluri R, Baig M, Mavi JS et al. The role of angioplasty in patients with acute coronary
syndrome and previous coronary artery bypass grafting. Int J Cardiol 2014;176:760-3.
6. Uppal H, Chandran S, Potluri R. Risk factors for mortality in Down syndrome. J Intellect
Disabil Res 2015;59:873-81.
7. Carter P, Reynolds J, Carter A et al. The impact of psychiatric comorbidities on the length
of hospital stay in patients with heart failure. Int J Cardiol 2016;207:292-6.
8. Jensen HH, Godtfredsen NS, Lange P, Vestbo J. Potential misclassification of causes of
death from COPD. Eur Respir J 2006;28:781-785.
9. Raghu G, Amatto VC, Behr J, Stowasser S. Comorbidities in idiopathic pulmonary fibrosis
patients: a systematic literature review. Eur Respir J 2015;46:1113-1130.
10. Hubbard RB, Smith C, Le Jeune I, Gribbin J, Fogarty AW. The Association between
Idiopathic Pulmonary Fibrosis and Vascular Disease. Am J Respir Crit Care Med
2008;178:1257-1261.
20

11. Collard HR, Ward AJ, Lanes S et al. Burden of illness in idiopathic pulmonary fibrosis.
Journal Medical Economics 2012;15:829-835.
12. Liu H, Fu Y, Wang K. Asthma and risk of coronary heart disease: A meta-analysis of cohort
studies. Ann Allergy Asthma Immunol 2017;118:689-695.
13. Wang L, Gao S, Yu M, Sheng Z, Tan W. Association of asthma with coronary heart disease:
A meta analysis of 11 trials. PLoS ONE 2017;12:e0179335-9.
14. Iribarren C, Tolstykh IV, Miller MK, Sobel E, Eisner MD. Adult asthma and risk of
coronary heart disease, cerebrovascular disease, and heart failure. Am J Epidemiol
2012;176:1014-24.
15. Tattersall MC, Guo M, Korcarz CE et al. Asthma predicts cardiovascular disease events.
Arterioscler Thromb Vac Biol 2015;35:1520-1525.
16. Müllerova H, Agusti A, Erqou S, Mapel DW. Cardiovascular Comorbidity in COPD. Chest
2013;144:1163-1178.
17. Finkelstein J, Cha E, Scharf SM. Chronic obstructive pulmonary disease as an independent
risk factor for cardiovascular morbidity. Copd 2009;4:337-349.
18. Baty F, Putora PM, Isenring B, Blum T, Brutsche M. Comorbidities and Burden of COPD.
PLoS ONE 2013;8:e63285-9.
19. Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major
comorbidities in subjects with COPD and incidence of myocardial infarction and stroke.
Thorax 2010;65:956-962.
20. Allen NB, Holford TR, Bracken MB et al. Geographic variation in one-year recurrent
ischemic stroke rates for elderly Medicare beneficiaries in the USA. Neuroepidemiology
2010;34:123-9.
21. Sidney S, Sorel M, Quesenberry CP et al. COPD and incident cardiovascular disease
hospitalizations and mortality. Chest 2005;128:2068-2075.
21

22. http://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/
healthandlifeexpectancies/bulletins/adultsmokinghabitsingreatbritain/2015.
23. Josephs L, Culliford D, Johnson M, Thomas M. Improved outcomes in ex-smokers with
COPD. Eur Respir J 2017;49.
24. Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction. J
Am Coll Cardiol 2013;62:263-71.
25. Thomsen M, Dahl M, Lange P, Vestbo J, Nordestgaard BG. Inflammatory biomarkers and
comorbidities in chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2012;186:982-8.
26. Neukamm AM, Hoiseth AD, Hagve TA, Soyseth V, Omland T. High-sensitivity cardiac
troponin T levels are increased in stable COPD. Heart 2013;99:382-7.
27. Patel AR, Kowlessar BS, Donaldson GC et al. Cardiovascular risk, myocardial injury, and
exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2013;188:1091-9.
28. Lopez-Sanchez M, Munoz-Esquerre M, Huertas D et al. Inflammatory markers and
circulating extracellular matrix proteins in patients with chronic obstructive pulmonary
disease and left ventricular diastolic dysfunction. Clin Resp J 2015.
29. Sand JM, Leeming DJ, Byrjalsen I et al. High levels of biomarkers of collagen remodeling
are associated with increased mortality in COPD. Resp Research 2016;17:125.
30. Ridker PM, MacFadyen JG, Thuren T et al. Effect of interleukin-1beta inhibition with
canakinumab on incident lung cancer in patients with atherosclerosis. Lancet
2017;390:1833-1842.
31. Smith BM, Martin R Prince MD P, PhD EAH et al. Impaired Left Ventricular Filling in
COPD and Emphysema: Is It the Heart or the Lungs? Chest 2013;144:1143-1151.
22

32. Patel ARC, Kowlessar BS, Donaldson GC et al. Cardiovascular Risk, Myocardial Injury,
and Exacerbations of Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med
2013;188:1091-1099.
33. Murtha LA, Schuliga MJ, Mabotuwana NS et al. The Processes and Mechanisms of Cardiac
and Pulmonary Fibrosis. Front Physiol 2017;8:777.
34. Papadopoulos CE, Pitsiou G, Karamitsos TD et al. Left ventricular diastolic dysfunction in
idiopathic pulmonary fibrosis. Eur Respir J 2008;31:701-6.
35. Iwamoto H, Yokoyama A, Kitahara Y et al. Airflow limitation in smokers is associated with
subclinical atherosclerosis. Am J Respir Crit Care Med 2009;179:35-40.
36. Eickhoff P, Valipour A, Kiss D et al. Determinants of systemic vascular function in patients
with stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2008;178:1211-8.
37. Vijayakumar J, Subramanian S, Singh P et al. Arterial inflammation in bronchial asthma. J
Nucl Cardiol 2013;20:385-95.
38. Wedzicha JA, Seemungal TA, MacCallum PK et al. Acute exacerbations of chronic
obstructive pulmonary disease are accompanied by elevations of plasma fibrinogen and
serum IL-6 levels. Thromb Haemost 2000;84:210-5.
39. Bhatt DL, Roe MT, Peterson ED et al. Utilization of early invasive management strategies
for high-risk patients with non-ST-segment elevation acute coronary syndromes. JAMA
2004;292:2096-104.
40. Bundhun PK, Gupta C, Xu GM. Major adverse cardiac events and mortality in chronic
obstructive pulmonary disease following percutaneous coronary intervention. BMC
cardiovascular disorders 2017;17:191.
23

41. Farooq V, van Klaveren D, Steyerberg EW et al. Anatomical and clinical characteristics to
guide decision making between coronary artery bypass surgery and percutaneous coronary
intervention for individual patients. Lancet 2013;381:639-50.
42. Salpeter SR, Buckley NS, Ormiston TM, Salpeter EE. Meta-analysis: effect of long-acting
beta-agonists on severe asthma exacerbations and asthma-related deaths. Ann Intern Med
2006;144:904-12.
43. https://http://www.fda.gov/Drugs/DrugSafety/ucm589587.htm.
44. Brook RD, Anderson JA, Calverley PM et al. Cardiovascular outcomes with an inhaled
beta2-agonist/corticosteroid in patients with COPD at high cardiovascular risk. Heart
2017;103:1536-1542.
45. Vestbo J, Anderson JA, Brook RD et al. Fluticasone furoate and vilanterol and survival in
chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT).
Lancet 2016;387:1817-26.
46. Wise RA, Anzueto A, Cotton D et al. Tiotropium Respimat inhaler and the risk of death in
COPD. N Engl J Med 2013;369:1491-501.
47. Singh S, Loke YK, Enright PL, Furberg CD. Mortality associated with tiotropium mist
inhaler in patients with chronic obstructive pulmonary disease. BMJ 2011;342:d3215.
24

FIGURE LEGENDS
Central illustration. Cardiovascular diseases associated with chronic obstructive pulmonary
disease (COPD), asthma and interstitial lung disease (ILD).
On multivariable analysis, COPD was independently associated with ischemic heart disease (IHD),
heart failure (HF), atrial fibrillation (AF) and peripheral vascular disease (PVD); asthma was
independently associated with IHD, and ILD was independently associated with IHD and HF.
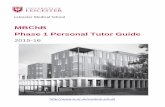
Figure 1. The impact of cardiovascular diseases on all-cause mortality in chronic obstructive
pulmonary disease (COPD).
Between January 1st 2000 and March 31st 2013, 31,646 patients with COPD were admitted to seven
NHS hospitals across the North West of England, UK. During follow up of 5.2 ± 3.6 years, 16,812
patients (53.1%) died. Kaplan-Meier cumulative survival curves are used to illustrate the impact of
(A) ischemic heart disease, (B) heart failure, (C) atrial fibrillation, (D) cerebrovascular disease and
(E) peripheral vascular disease on survival. In multivariable analysis, ischemic heart disease, heart
failure, atrial fibrillation and peripheral vascular disease were independently associated with death.
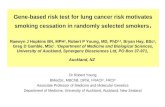
Figure 2. The impact of cardiovascular diseases on all-cause mortality in asthma
Between January 1st 2000 and March 31st 2013, 60,424 patients with asthma were admitted to seven
NHS hospitals across the North West of England, UK. During follow up of 5.2 ± 3.6 years, 6,649
patients (11.0%) died. Kaplan-Meier cumulative survival curves are used to illustrate the impact of
(A) ischemic heart disease, (B) heart failure, (C) atrial fibrillation, (D) cerebrovascular disease and
(E) peripheral vascular disease on survival. In multivariable analysis, ischemic heart disease and
heart failure were independently associated with death.
25

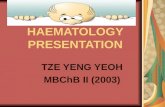
Figure 3. The impact of cardiovascular diseases on all-cause mortality in interstitial lung
disease (ILD)
Between January 1st 2000 and March 31st 2013, 1,662 patients with ILD were admitted to seven
NHS hospitals across the North West of England, UK. During follow up of 5.2 ± 3.6 years, 1,149
patients (69.1%) died. Kaplan-Meier cumulative survival curves are used to illustrate the impact of
(A) ischemic heart disease, (B) heart failure, (C) atrial fibrillation, (D) cerebrovascular disease and
(E) peripheral vascular disease on survival. In multivariable analysis, ischemic heart disease and
heart failure were independently associated with death.
26

TABLES
Table 1. Baseline characteristics according to respiratory disease and matched controls.
COPD Asthma ILD
Characteristic Control
N = 158,230
COPD
N = 31,646
p value Control
N = 302,120
Asthma
N = 60,424
p value Control
N = 8,310
Fibrosis
N = 1,662
p value
Demographics
Age 70.0±12 70.3±12 48.6±20 48.5±20 71.3±12 71.5±12
Male 80,710 (51.0%) 16,142 (51.0%) 110,860 (36.7%) 22,172 (36.7%) 4,715 (56.7%) 943 (56.7%)
Ethnic Group
Caucasian
South Asian
Afro-Caribbean
Other
Unknown
133,209 (84.2%)
6,082 (3.8%)
2,383 (1.5%)
2828 (1.8%)
13,728 (8.7%)
28,527 (90.1%)
555 (1.8%)
175 (0.6%)
292 (0.9%)
2,097 (6.6%)
231,451 (76.6%)
24,604 (8.1%)
9,208 (3.0%)
11273 (3.7%)
25,584 (8.5%)
47,828 (79.2%)
5,343 (8.8%)
1,520 (2.5%)
1870 (3.1%)
3,863 (6.4%)
7,057 (84.9%)
304 (3.7%)
116 (1.4%)
135 (1.7%)
698 (8.4%)
1,427 (85.9%)
113 (6.8%)
17 (1.0%)
15 (0.9%)
90 (5.4%)
Cardiovascular disease
Hypertension
Hyperlipidaemia
T1DM
T2DM
IHD
53,396 (33.7%)
15,855 (10.0%)
2,253 (1.4%)
20,655 (13.1%)
28,380 (17.9%)
11,992 (37.9%)
3,051 (9.6%)
340 (1.1%)
4,879 (15.4%)
9,188 (29.0%)
<0.001
0.040
<0.001
<0.001
<0.001
50,243 (16.6%)
16,181 (5.4%)
3,287 (1.1%)
20,105 (6.7%)
24,149 (8.0%)
14,752 (24.4%)
4,478 (7.4%)
875 (1.4%)
5,945 (9.8%)
7,291 (12.1%)
<0.001
<0.001
<0.001
<0.001
<0.001
2,840 (34.2%)
799 (9.6%)
108 (1.3%)
1,133 (13.6%)
1,526 (18.4%)
575 (34.6%)
150 (9.0%)
17 (1.0%)
281 (16.9%)
452 (27.2%)
0.741
0.455
0.355
<0.001
<0.001
27

Heart Failure
AF
CKD
Cerebrovascular disease
PVD
PCI
CABG
10,076 (6.4%)
15,123 (9.6%)
6,275 (4.0%)
8,304 (5.2%)
3,750 (2.4%)
3,619 (2.3%)
2,153 (1.4%)
5,449 (17.2%)
5,444 (17.2%)
2,290 (7.2%)
1,932 (6.1%)
1,714 (5.4%)
418 (1.3%)
236 (0.7%)
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
7,617 (2.5%)
11,106 (3.7%)
4,653 (1.5%)
6,563 (2.2%)
3,010 (1.0%)
3,843 (1.3%)
1,859 (0.6%)
1,879 (3.1%)
2,504 (4.1%)
925 (1.5%)
1,119 (1.9%)
617 (1.0%)
829 (1.4%)
360 (0.6%)
<0.001
<0.001
0.866
<0.001
0.576
0.047
0.574
560 (6.7%)
896 (10.8%)
357 (4.3%)
512 (6.2%)
204 (2.5%)
180 (2.2%)
113 (1.4%)
295 (17.7%)
263 (15.8%)
149 (9.0%)
79 (4.8%)
52 (3.1%)
16 (1.0%)
12 (0.7%)
<0.001
<0.001
<0.001
0.026
0.113
0.001
0.033
Other disease
Pneumonia
Dementia
Breast Cancer
Lung Cancer
Colon Cancer
6,957 (4.4%)
7,157 (4.5%)
2,509 (1.6%)
2,676 (1.7%)
1,059 (0.7%)
4,870 (15.4%)
1,615 (5.1%)
543 (1.7%)
1,844 (5.8%)
195 (0.6%)
<0.001
<0.001
0.093
<0.001
0.287
5,818 (1.9%)
4,671 (1.5%)
3,532 (1.2%)
2,210 (0.7%)
871 (0.3%)
1,619 (2.7%)
615 (1.0%)
677 (1.1%)
399 (0.7%)
129 (0.2%)
<0.001
<0.001
0.308
0.059
0.001
422 (5.1%)
430 (5.2%)
122 (1.5%)
133 (1.6%)
57 (0.7%)
316 (19.0%)
83 (5.0%)
34 (2.0%)
83 (5.0%)
7 (0.4%)
<0.001
0.761
0.083
<0.001
0.217
Values presented are number and percentage, unless stated. Age is presented as mean years ± standard deviation.
28

Table 2: Multivariable-adjusted association of cardiovascular diseases with each respiratory disease.
COPD Asthma ILD
Odds ratio (95% CI) p value Odds ratio (95% CI) p value Odds ratio (95% CI) p value
Hypertension
Hyperlipidaemia
T1DM
T2DM
IHD
Heart Failure
AF
CKD
Cerebrovascular
PVD
PCI
CABG
1.089 (1.059-1.120)
0.876 (0.837-0.917)
0.662 (0.587-0.746)
1.034 (0.997-1.073)
1.742 (1.688-1.797)
2.167 (2.081-2.255)
1.391 (1.339-1.444)
1.229 (1.164-1.298)
0.973 (0.921-1.027)
1.849 (1.737-1.969)
0.484 (0.435-0.538)
0.422 (0.366-0.485)
<0.001
<0.001
<0.001
0.074
<0.001
<0.001
<0.001
<0.001
0.316
<0.001
<0.001
<0.001
1.656 (1.614-1.698)
1.053 (1.013-1.094)
1.055 (0.976-1.139)
1.295 (1.253-1.339)
1.483 (1.435-1.533)
1.057 (0.999-1.117)
1.016 (0.969-1.066)
0.828 (0.769-0.892)
0.767 (0.718-0.819)
0.792 (0.724-0.866)
0.753 (0.696-0.816)
0.597 (0.531-0.672)
<0.001
0.009
0.176
<0.001
<0.001
0.053
0.505
<0.001
<0.001
<0.001
<0.001
<0.001
0.950 (0.840-1.075)
0.929 (0.758-1.138)
0.709 (0.415-1.211)
1.195 (1.024-1.395)
1.571 (1.367-1.805)
2.234 (1.878-2.657)
1.100 (0.930-1.302)
1.586 (1.276-1.971)
0.606 (0.468-0.784)
1.088 (0.781-1.516)
0.418 (0.246-0.708)
0.469 (0.252-0.872)
0.417
0.475
0.209
0.024
<0.001
<0.001
0.267
<0.001
<0.001
0.617
0.001
0.017
29

Table 3: Multivariable Cox regression models of the contribution of cardiovascular diseases to mortality in patients with each
respiratory disease.
COPD Asthma ILD
No. of
patients
No. of deaths (%) HR p value No. of
patients
No. of deaths
(%)
HR p value No. of
patients
No. of deaths
(%)
HR p value
Total 31,646 16,812 (53.1%) 60,424 6 649 (11.0%) 1,662 1 149 (69.1%)
Hypertension
Hyperlipidaemia
T1DM
T2DM
IHD
Heart Failure
AF
CKD
Cerebrovascular
PVD
11,992
3,051
340
4,879
9,188
5,449
5,444
2,290
1,932
1,714
5,698 (47.5%)
972 (31.9%)
192 (56.5%)
2,546 (52.2%)
5,226 (56.9%)
4,219 (77.4%)
3,785 (69.5%)
1,632 (71.3%)
1,445 (74.8%)
1,079 (63.0%)
0.763 (0.750-0.776)
0.613 (0.592-0.635)
1.346 (1.265-1.433)
1.132 (1.107-1.157)
1.029 (1.009-1.050)
1.645 (1.608-1.684)
1.080 (1.057-1.103)
1.314 (1.277-1.352)
1.843 (1.796-1.891)
1.320 (1.271-1.371)
<0.001
<0.001
<0.001
<0.001
0.004
<0.001
<0.001
<0.001
<0.001
<0.001
14,752
4,478
875
5,945
7,291
1,879
2,504
925
1,119
617
2 671 (18.1%)
487 (10.9%)
197 (22.5%)
1 290 (21.7%)
1 802 (24.7%)
1 005 (53.5%)
940 (37.5%)
445 (48.1%)
550 (49.2%)
213 (34.5%)
0.790 (0.773-0.807)
0.614 (0.589-0.641)
1.612 (1.510-1.720)
1.252 (1.218-1.286)
1.039 (1.013-1.067)
1.808 (1.752-1.866)
1.070 (1.039-1.103)
1.553 (1.494-1.613)
2.098 (2.031-2.168)
1.394 (1.322-1.470)
<0.001
<0.001
<0.001
<0.001
0.003
<0.001
<0.001
<0.001
<0.001
<0.001
575
150
17
281
452
295
263
149
79
52
407 (70.8%)
83 (55.3%)
10 (58.8%)
192 (68.3%)
335 (74.1%)
241 (81.7%)
207 (78.7%)
114 (76.5%)
63 (79.7%)
32 (61.5%)
0.775 (0.723-0.830)
0.619 (0.538-0.712)
1.282 (0.969-1.695)
1.145 (1.049-1.250)
1.098 (1.016-1.187)
1.588 (1.448-1.742)
1.053 (0.966-1.148)
1.183 (1.053-1.328)
1.886 (1.702-2.090)
1.269 (1.072-1.503)
<0.001
<0.001
0.082
0.003
0.018
<0.001
0.239
0.005
<0.001
0.006
PCI 418 52 (12.4%) 0.353 (0.317-0.394) <0.001 829 54 (6.5%) 0.414 (0.367-0.466) <0.001 16 5 (31.3%) 0.427 (0.276-0.659) <0.001
CABG 236 37 (15.7%) 0.516 (0.461-0.579) <0.001 360 28 (7.8%) 0.573 (0.503-0.653) <0.001 12 3 (25%) 0.425 (0.259-0.700) 0.001
30