YEAR 5 MBChB Professional Practice Block Prescribing ...
37
YEAR 5 MBChB Professional Practice Block Prescribing Tutorial Tutor Notes 2014/15 1
Transcript of YEAR 5 MBChB Professional Practice Block Prescribing ...
YEAR 5 MBChB Professional Practice Block Prescribing Tutorial Tutor Notes
2014/15
1

Prescribing Tutorial Tutors notes
Year 4 had a series of practical prescribing tutorials in each block, taught by a pharmacist. The students had a lecture on common prescribing issues for new doctors at the start of the year 5. They should have been learning how to prescribe on the wards over the year also. For this session, the students have been given a booklet of questions and a booklet of blank prescription sheets and medicine reconciliation forms to write on. They should work through as many of these as there is time for (it is likely that they will not get through everything but can take the rest away with them). You may wish to get them working in groups or alone. There are some suggested answers with the questions in this booklet, but you are free to use your own judgement. **Please advise students not to use latin abbreviations – bd, tds, qds, prn etc. Prescribing is a potentially dangerous patient safety activity – using latin in the 21st century is not acceptable. They may be marked down during exams if they use latin** If you have any comments about the exercises, we would be happy to receive them on paper or by email ([email protected]). Online BNF resource http://www.evidence.nhs.uk/formulary/bnf/current NHS Grampian Protocols:
• Reversal of anticoagulation with warfarin http://www.nhsgrampian.com/grampianfoi/files/WOA_560_0113.pdf
• Peri-op guide: http://www.nhsgrampian.com/grampianfoi/files/PeriOp_697_0714.pdf
• Tranquillisation Policy NHS Grampian http://www.nhsgrampian.com/grampianfoi/files/NHSGRapTranq.pdf
• Diabetes Guidance www.nhsgrampian.org/guidelines/diabetes •
NICE Guidelines on IV Fluids https://www.nice.org.uk/guidance/cg174 NICE pathway ACS http://pathways.nice.org.uk/pathways/acute-coronary-syndromes Following page numbers relate to student copy: Admission Cases Pages 3 – 5 Discharge Cases Pages 5 – 14 Anticoagulation Cases Pages 15 – 16 DVT case Page 17 Peri-operative cases Page 17 Sedation Cases Page18 Acute Pain cases Page 19 Alcohol Withdrawal Case Page 19 IV Fluids Cases Pages 20 -23 Diabetes Cases Pages 24 – 27 Chestpain Case Page 27
2

ADMISSION CASE 1 It’s Saturday afternoon. Mr Tom Smith is a 76 year old man being admitted to a medical ward with a raised INR. His GP checked it yesterday after Mr Smith noticed some bruising and the laboratory called GMEDs today as the INR was 8.2. The warfarin is prescribed for atrial fibrillation and previous TIAs. He is well with no obvious bleeding. He is currently being treated for a urine infection which is improving. He tells you that these are his current medicines: Warfarin usual dose 3mg once daily Ramipril 10mg once daily Amlodipine 10mg once daily Simvastatin 20mg once daily Ciprofloxacin 500mg twice daily for last 3 days Tasks: 1. Complete the medicines reconciliation form, including action plan for each medicine. 2. Write up the prescription sheets for continuing medicines 3. Make a decision regarding how you will deal with the raised INR, what you will do about his warfarin dose and when you will check his INR again Tutor notes: Ask the students to think about whether there are any medicines which are involved in causing this admission. Check students know how to look up drug interactions in back of BNF (appendix one), or on-line. http://www.evidence.nhs.uk/formulary/bnf/current/a1-interactions/list-of-drug-interactions/anticoagulants/coumarins Ciprofloxacin is the most likely culprit as it is the new drug - possibly enhances anticoagulation effects of warfarin - needs to be stopped and either another antibiotic used (is there an MSSU result?) or new urine sample taken. Note the simvastatin also has potential to alter INR, but this is OK if dose of warfarin adjusted to suit. Students may also notice interaction between simvastatin and amlodipine – this is OK as long as dose of simvastatin not more than 20mg. Warfarin should be withheld but documented on the kardex. They should use the anticoagulation reversal guidance in the BNF (see below excerpt) to determine that oral vitamin K between the doses 1 - 5mg should be given and the INR checked the next day. NHS Grampian guidance is also available – see below (Protocol for the Reversal of Over-Anticoagulation with Warfarin) which advises in this scenario to give 2.5mg orally. This is the injection (10mg/ml Konakion) and 2.5mg diluted in small amount of juice /water after drawing up in an oral syringe. They should also consider whether the patient still requires warfarin, which is the case, so large doses of vitamin K may be detrimental.
3

INR target for AF is 2.5 (2 – 3)
BNF excerpt - warfarin
Haemorrhage
The main adverse effect of all oral anticoagulants is haemorrhage. Checking the
INR and omitting doses when appropriate is essential; if the anticoagulant is
stopped but not reversed, the INR should be measured 2–3 days later to ensure
that it is falling. The cause of an elevated INR should be investigated. The
following recommendations (which take into account the recommendations of the
British Society for Haematology(2)) are based on the result of the INR and
whether there is major or minor bleeding; the recommendations apply to patients
taking warfarin:
• Major bleeding—stop warfarin; give phytomenadione (vitamin K1) 5 mg by
slow intravenous injection; give dried prothrombin complex (factors II,
VII, IX, and X—section 2.11) 25–50 units/kg (if dried prothrombin
complex unavailable, fresh frozen plasma 15 mL/kg can be given but is
less effective); recombinant factor VIIa is not recommended for
emergency anticoagulation reversal
• INR > 8.0, minor bleeding—stop warfarin; give phytomenadione (vitamin
K1) 1–3 mg by slow intravenous injection; repeat dose of phytomenadione
if INR still too high after 24 hours; restart warfarin when INR <5.0
• INR > 8.0, no bleeding—stop warfarin; give phytomenadione (vitamin K1) 1–5 mg by mouth using the intravenous preparation orally [unlicensed use]; repeat dose of phytomenadione if INR still too high after 24 hours; restart warfarin when INR <5.0
• INR 5.0–8.0, minor bleeding—stop warfarin; give phytomenadione
(vitamin K1) 1–3 mg by slow intravenous injection; restart warfarin when
INR <5.0
• INR 5.0–8.0, no bleeding—withhold 1 or 2 doses of warfarin and reduce
subsequent maintenance dose
• Unexpected bleeding at therapeutic levels—always investigate possibility
of underlying cause e.g. unsuspected renal or gastro-intestinal tract
pathology
4
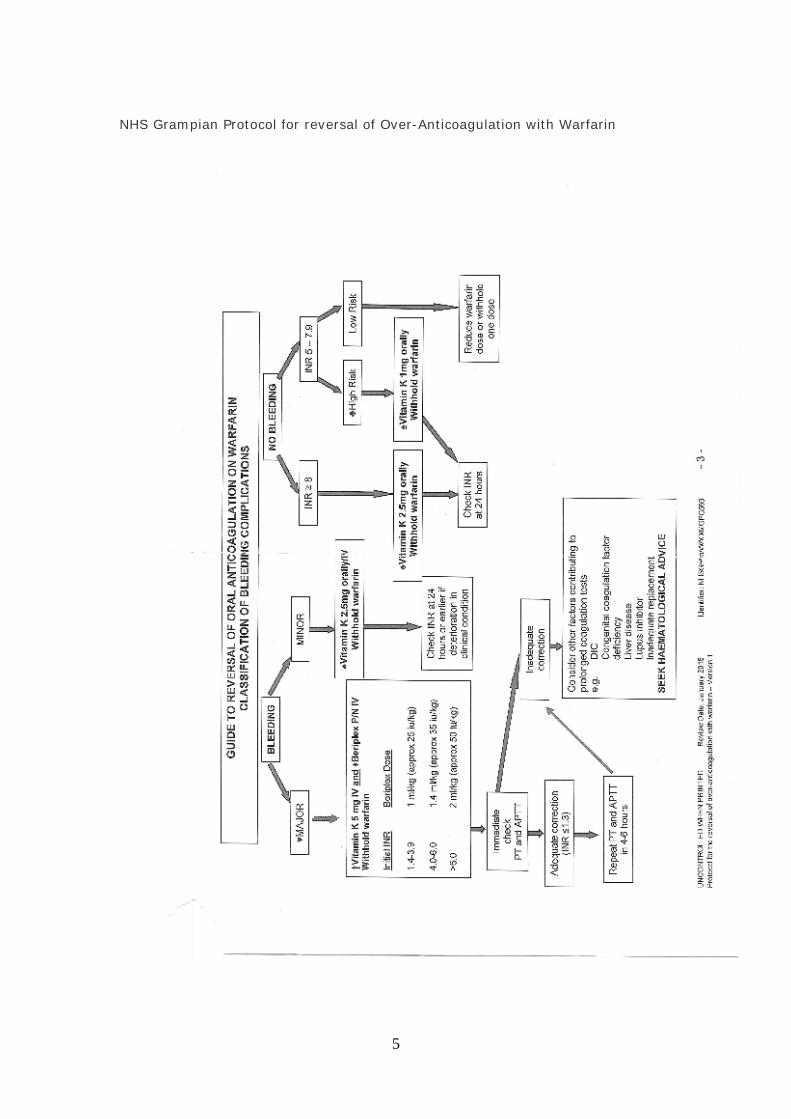
NHS Grampian Protocol for reversal of Over-Anticoagulation with Warfarin
5

ADMISSION CASE 2 It’s 8pm on Wednesday. Jessie Kesson is an 80 year old lady admitted to the orthopaedic ward with a right fractured neck of femur. She has a past history of ischaemic heart disease, osteoarthritis, COPD and recent DVT. Her AMT is 7/10. Your registrar thinks she will need an operation. Medication history: Information from Jessie
Information from Jessie’s daughter
Information from the ambulance crew who found the following medicines in Jessie’s House, so brought them in
“Puffers” “water pills” Salbutamol inhaler 2 puffs if required for wheeze
“Wee white pills”
“blood thinner” Tiotropium inhaler 18mcg daily
Pain “killers” Heart pills Rivaroxaban 20mg once dialy Might be able to bring in
note from house Atenolol 50mg once daily
Questions whether Jessie has been taking her medicines properly
Felodipine 5mg once daily
Furosemide 20mg once daily Co-dydramol 2 tabs as required for
pain Tasks: Write up the medicines reconciliation form, complete the medicine action plan on this form and then write up the prescription sheet. Tutor note: These may not be all her medicines. The students should consider what other sources of information can be accessed to improve accuracy of medicines reconciliation as have only one reliable source at the moment – the patients own medicines. e.g. Emergency Care Summary (or Key Information Summary in future), ask GP surgery for Admission Summary, recent ride-hand side of prescription (ask relative to bring in from home if possible). Antihypertensives /beta-blocker may be implicated in her fall. Check BP, pulse and ECG. Probably best to start from scratch with analgesia but be aware of fact that not opiate naïve. Peri-op management – no information in the BNF. NHS Grampian provide guidance on this, but it will ultimately be the surgeon / anaesthetist who gives direction on this. Link to NHSG Peri-op guide: http://www.nhsgrampian.com/grampianfoi/files/PeriOp_697_0714.pdf Atenolol – beta blocker – don’t stop unless obviously hypotension or bradycardic /heart block on ECG. Patients at risk of coronary artery disease have substantially reduced mortality and cardiovascular events following discharge after non-cardiac surgery if beta blockers are continued. (P.T.O)
6
Felodipine - Continuation is recommended for control of hypertension and angina, haemodynamic stability and reduction of ischaemic burden and to avoid withdrawal syndromes. Furosemide may cause hypokalaemia – correct this pre-op. Rivaroxaban – a DOAC (Direct Oral Anti-Coagulant) or NOAC (New Oral AntiCoagulant). Increased risk of bleed in surgery. aPTT is not reliable in estimating the degree of anticoagulation. Risk of VTE / Stroke if stopped. Whether it is stopped or not depends on risk of whether minor/major surgery involved, renal function and bleeding risk. Discussion with surgeon needed. Bridging with unfractionated heparin might be an option if risk of stroke/VTE very high, but more likely stop rivaroxaban for a couple of days. ADMISSION CASE 3 Mrs Middleton (aged 60) arrives in the AMAU from A&E on a Saturday morning. She has had an episode of chest pain which the registrar thinks may be due to gastro-oesophageal reflux, but is waiting for a 12 hour troponin. She has taken along all her drugs in a carrier bag. This is what it contains: 3 empty packets of aspirin – 75mg tablets, dated 12, 8 and 3 months ago, 56 tablets per pack 1 half full packet of co-codamol (30/500), dated 4 months ago, 112 tablets 2 packets of paracetamol – 1 empty, 1 half full - no date 1 half full packet of co-dydramol, dated 2 months ago (for James Middleton) 1 half full bottle of lactulose, dated 4 months ago 1 empty packet of clopidogrel, dated last year 1 GTN spray, dated 19 months ago 2 strips of sertraline, each containing 14 tablets, unopened 3 salbutamol MDI inhalers, 2 almost empty 2 seretide accuhalers 1 half strip of clarithromycin 250mg tabs dated 7 months ago 1 half packet of benson and hedges 1 packet of atenolol 50mg dated 1 month ago 1 half used grotty tube of betnovate (no instructions or date) Tasks: 1. Please complete the medicines reconciliation form, action plan and prescription chart for continuing medicines. 2. What medicines related problems might this patient have? Tutor notes: Need another information source for accuracy – ECS etc. Likely poor compliance – need to discuss in detail with patient what she has been taking. May be taking too much paracetamol chronically. Aspirin may be implicated in cause of pain but as well to continue until cardiac cause excluded/bloods back for haemoglobin result. Also Clopidogrel – is she taking them both or none at all? P.T.O
7

May be constipated secondary to weak opiates. Need to check GTN spray in date. (remember if GTN tablets then they need discarded 8 weeks after opening as lose potency) Need to clarify lung disease – if asthma, beta blocker contraindicated. If COPD use beta-blocker with caution. Smoker – likely COPD BP and heart rate may drop if prescribe beta blocker (as may not have been taking it) but could cause problems if not prescribed and pain is cardiac. DISCHARGE CASE 1 Margaret MacPherson is a 77 year old woman who has been in hospital for a vaginal hysterectomy. This has all been straightforward. This is her prescription chart and original medicines reconciliation form. Please write her discharge flimsy. Tutor notes: ACE inhibitor stopped – should be restarted after surgery Unnecessary drugs should not be given on discharge – anti-emetics, painkillers not been needed Can give LMWH in community if this has to be continued, but would be unusual in this case.
8

9

10

11

12
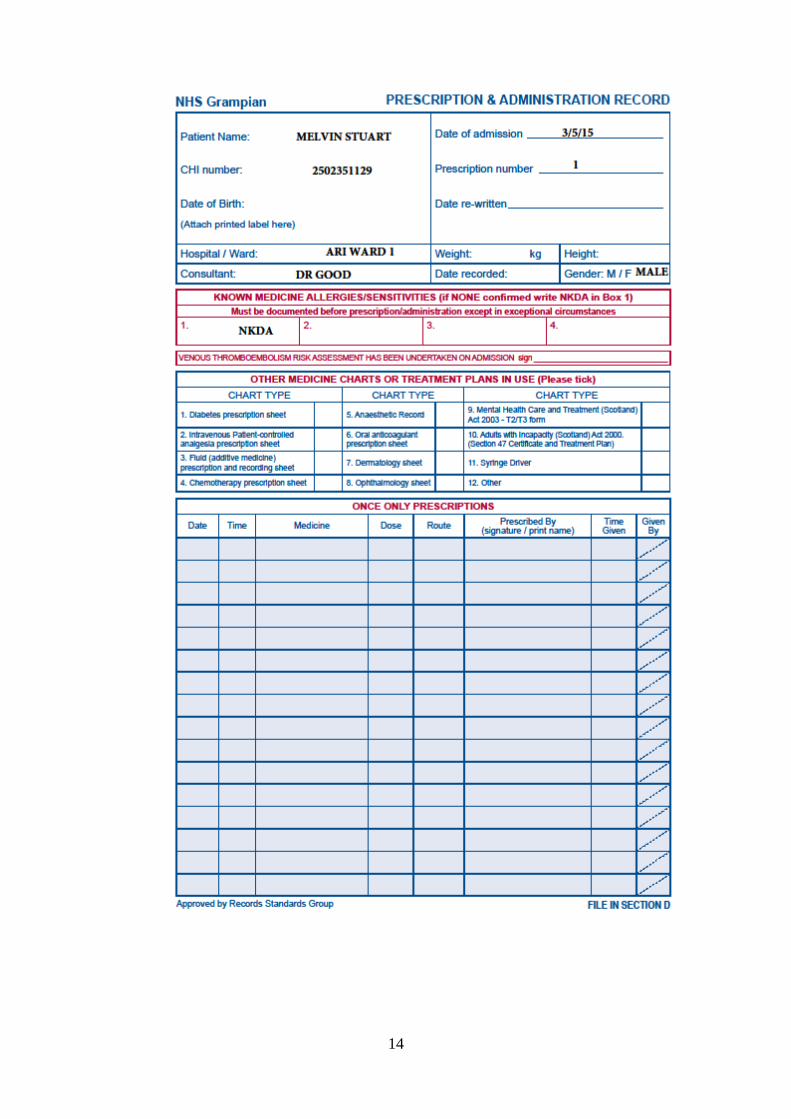
DISCHARGE CASE 2 Melvin Stuart is a 75 year old man with non-small cell lung cancer. He was admitted with chest pain. His primary cancer has infiltrated the surrounding tissues and he has bony metastases. He has been started on opiates for analgesia to good effect. Patient’s prescription chart is as follows (4 pages) Please write his discharge (IDL – Immediate Discharge Letter) prescription, using one sheet for all the controlled drugs and one for the other medicines. Tutor notes
1. Dexamethasone – ask students why he has been prescribed these steroids – could be for a variety of reasons:
• Anti-inflammatory painkiller/reduction of any oedema • Could be used to potentiate effects of chemotherapy (which may have
been prescribed on a different chart) • Might inhibit progression of cancer cell growth
o reducing dose – if given for more than 2 weeks can suppress hypo-pit-adrenocortical axis so taper off. It appears here that it was just started on the 6th May, so there may be other reasons why in this patients case.
o Example of reducing dose – reduce by 2 to 4mg every 1 to 3 days. Note steroids given in the morning
o E.g. 8mg at 8am for 2 days then 6mg at 8am for 2 days then 4mg at 8am for 2 days then 2mg at 8am for 2 days then stop OR 6mg for one week, 4 mg for 1 week, 2mg for 1 week. In reality you would ask your senior how quickly to reduce the steroids. Ask student to choose a reducing regimen and prescribe on discharge – a new line for each dose reduction
2. Analgesia • Diclofenac and Paracetamol straightforward • MST and Sevredol are different forms of morphine sulphate - a
controlled drug, subject to prescribing regulations. See front of BNF section on prescribing controlled drugs. It is important to find out which strength of each preparation exist.With electronic IDL’s the CD page will need to be printed off and signed/dated by the Prescriber using legible ink and taken to the pharmacy before they can release the medicines. e.g MST 10mg tablets dose is 10mg at 8am and 8pm. Supply 14 (fourteen) tablets of 10mg (ten milligrams). Sevredol does not come in 5mg doses, therefore needs to be prescribed as follows: Sevredol tablets dose 5mg 2 hourly as required for pain .Supply 10 (ten) of the 10mg (ten milligram) tablets.
3. Inhalers – important to specify inhaler device, be it an MDI or a Handihaler. Also check that the Tiotropium is prescribed as 18 micrograms not mcg. 3 inhalers – seretide, tiotropium, salbutamol.
4. Docusate important – if any opiates prescribed co-prescribe laxative in majority of cases.
5. Omeprazole – this might just be co-prescribed for the duration of the dexamethasone, to reduce GI irritation - ask for a review when steroids stop.
13
14

15

16

17

ANTICOAGULATION CASE 1 Jennifer McRobert is a 62 year old woman who was admitted to the medical ward 2 weeks after getting an elective left hip replacement. She has no past medical history other than osteoarthritis of her hips. She was prescribed aspirin as DVT prophylaxis but has complained of 3 days of a more swollen left leg and today experienced sudden onset right sided pleuritic chest pain and shortness of breath. She mentions that her brother had a post operative PE. She weighs 68 kg. Following a high probability V/Q scan, a pulmonary embolism is diagnosed. Please prescribe low molecular weight heparin (dalteparin is local choice) and start warfarin. Please write down your plan for warfarinisation. Tutor notes: Low dose Aspirin is sometimes prescribed post-hip replacement as DVT prophylaxis for 4 to 6 weeks only. It may not be as effective as low dose heparin or NOAC. In Grampian Rivaroxaban is often used instead. Dalteparin dose is calculated by weight (in BNF). This patient should get 12,500 units subcutaneously once a day (time of day doesn’t matter but must get initial dose asap). Write up in once-off section of prescription sheet then continue second dose on regular section, usually given at 18:00 hours. This should be stopped when INR>2. Patient does not need to stay in hospital just for target INR to be reached – they can be discharged on dalteparin as long as appropriate primary care management set up (e.g. can they self-administer the dalteparin or do they need a community/practice nurse to do) Note new warfarin prescription sheet introduced NHSG beginning of 2014. Warfarin is obviously a high risk medicine. Requires fast initiation of warfarin – see back of warfarin prescription sheet. This is based on modified Fennerty regime. This suggests for ages 51 – 65 years of age a starting dose of 9mg on day 1. This would be prescribed at 18:00 hours in Grampian – just a locally agreed time, nothing special about this – the important point being that it is always taken at the same time of day. Day 2 dose depends on INR, but will probably be 9mg again. Day 3 dose choice may vary more. For ages under 50 it will probably be a 10/ 10/5mg regimen. Should check baseline INR then daily and adjust doses accordingly. Should not just write up all 3 days doses at start. Should document indication (PE), duration of treatment (3 - 6 months) and target INR is 2.5 (2-3) on warfarin prescription chart. Then ensure patient has had appropriate counselling on the warfarin – yellow anticoagulant booklet given with alert card, and that you or another member of the team (nurse/pharmacist) has gone over this with patient. ADVISE STUDENTS LOOK FOR ONE THESE YELLOW BOOKLETS ON THE WARD. If time, discuss the main points of counselling regarding warfarin:
• This will thin your blood and protect from harmful clots • However more at risk of bleeding if dose is too high so report any bleeding
(gums, prolonged nosebleeds, blood in sit/urine/stools/severe bruising, unusual headaches, heavy periods)
• blood clotting will need to be monitored by GP surgery • take at same time each day • if forget dose don’t double up. If take too much then contact pharmacy/Dr • if buying over-the-counter medicines ask pharmacist if safe to take with
warfarin – definitely no aspirin or NSAIDs
18

• avoid major dietary changes – vitamin K rich foods can affect blood clotting. NO cranberry juice
• no binge drinking alcohol. Only alcohol in small measures, If being discharged the patient will need to know about follow-up – i.e. when their next appointment is with GP surgery to have INR checked – you may have to organise this with GP surgery prior to patients discharge. The GP should also be informed of any new starts on warfarin. You must provide enough information for them to continue to prescribe – most recent doses and INRs NB NOAC would now be a reasonable treatment instead of the heparin/warfarin – they may have seen this practice. Check most up to date SPC for the product to ensure using for licenced indication. BNF number 68 (Sept 2014 – March 2015) is too old as it hasn’t got up to date licencing.
19
ANTICOAGULATION CASE 2 Martin McKendrick is a 36 year old man who has recently had an aortic valve replacement (metallic valve) for endocarditis. He was initially treated with intravenous heparin and has now been started on warfarin. Today his INR is 3.2. Please write his discharge prescription, including all the information that the GP needs. (You will need to make decisions about the target INR and length of treatment.) Tutor notes Treatment should be life-long; INR target for new AV valves (mechanical) is 2.5 (2-3) unless there are other related risk factors. Depends on type and location of valve, and patient related factors – e.g. cardiac rhythm, dilatation. Note the prescriber has not ticked this target on warfarin sheet but should have done (but then this would have given the answer away to students!). “Todays” INR just above target – note falling INR’s over last few days – could try 3mg on discharge, ask GP to check INR in 2 days Discharge should include at minimum: indication, target INR, length of treatment, most recent dose, most recent INR and recommended time of next INR check. Ideally, student should discuss sending GP warfarin chart or other method of providing more than one INR and that they would make an arrangement with the practice for the next check. For instance they could write the last few days doses and INR’s into yellow booklet. Patient must also be counselled. NB NOACs should not be used in valvular heart disease – must stick with warfarin
20

21

DVT PROPHYLAXIS CASE 1 A 64 year old woman is admitted for an abdominal hysterectomy. She is obese. Otherwise she is well with no past medical history. Her current medicines are: tranexamic acid when required and dihydrocodeine. Her HRT was stopped 4 weeks ago. She weighs 90kg. Tasks: 1. Name her risk factors for VTE 2. Name her risk factors for bleeding 3. What prophylaxis would you consider? Please prescribe this on the prescription sheet provided. Tutor notes Risk factors – major surgery plus obesity (HRT also but stopped in line with current guidelines); none for bleeding. Should consider pharmacological prophylaxis. Best option (locally): Dalteparin 2500 to 5000 units subcutaneously once a day. Depends on VTE risk but usually 2500 units daily in ARI surgical wards (5000 units medical wards). PRE-OPERATIVE MANAGEMENT CASE 1 A 72 year old man is admitted with a fractured neck of femur. He has a past medical history of hypertension and atrial fibrillation. These are his usual medicines: Amlodipine 10mg daily Atenolol 50mg daily Warfarin – usual dose 4mg daily at 18:00 hours; INR today is 2.2. He is put on the theatre list tomorrow morning. Consider which of his medicines you should write up on his prescription chart and any other necessary action. Tutor notes – Note BNF advice on peri-op anticoag may differ from local protocol. Link to NHSG Peri-op guide: http://www.nhsgrampian.com/grampianfoi/files/PeriOp_697_0714.pdf
• write up both the Atenolol and Amlodipine • Regarding warfarin – students should say they must DISCUSS WITH
SURGEON/ANAESTHETIST first. They will certainly have to repeat INR in the morning - look for them to repeat INR, consider vitamin K in discussion with Anaesthetist. Assess bleeding risk prior to surgery, in certain types of surgery warfarin can be continued. Consider risk of VTE if patient undercoagulated. In surgery involving increased bleeding risk oral anticoagulants will need to stop a minimum of five days prior to surgery. Patients at higher risk of VTE may require bridging therapy either with unfractionated heparin or low weight molecular heparin. Factors affecting choice of VTE therapy include indication for anticoagulant therapy and renal function. Patients at low risk, cessation of the anticoagulant combined with VTE prophylaxis is sufficient.
22

PRE-OPERATIVE MANAGEMENT CASE 2 A 45 year old woman with type II diabetes mellitus is admitted for an elective cholecystectomy. These are her usual medicines: Metformin 2g daily in divided doses Glipizide 5mg once daily Apixaban 5mg twice daily Felodipine 5mg once daily Atorvastatin 40mg daily Ramipril 10mg daily Consider which of his medicines you should write up on prescription chart and any other necessary action. Tutor notes: Link to NHSG Peri-op guide: http://www.nhsgrampian.com/grampianfoi/files/PeriOp_697_0714.pdf Put first on theatre list if possible. Oral hypoglycaemics - discontinue before surgery. Sulphonylureas may interfere with ischaemic conditioning and increase risk of myocardial injury perioperatively. SU’s can precipitate perioperative hypoglycaemia. How many doses should be with-held depends on number of missed meals, and time of operation. Gliclazide is short-acting SU. Consider a temporary switch to insulin/dextrose/potassium with close monitoring of electrolytes and blood glucose. Metformin - Increased risk of lactic acidosis if renal function decreases. Consider with holding from 48 hours prior to surgery, certainly on morning of operation. Restart when eGFR>50mls/min. Apixaban – NOAC– new(er) oral anti-coagulant or DOAC – Direct oral anticoagulant. Increased surgical bleed risk. DOAC cessation dependent on major/minor surgery, renal function and bleeding risk. Consider prophylactic LWMH or therapeutic LWMH dosing dependent on thrombosis and bleeding risk. Felodipine - Continuation is recommended for control of hypertension and angina, haemodynamic stability and reduction of ischaemic burden and to avoid withdrawal syndromes. Atorvastatin - continue Ramipril – ACEI - May intensify hypotensive effect of anaesthetics which may be less responsive to vasopressors. Consider continuation if prescribed for cardiac failure. Consider omitting morning dose and or prior evening dose if prescribed for hypertension. Consider reducing the dose if patient is persistently hypotensive. Requirement for ephedrine to maintain BP more frequent when ACEI continued. Increased risk of renal impairment, especially if patient is dehydrated, hypotensive or being given other nephrotoxic drugs. Consider withholding post operatively if patient is dehydrated, hypotensive or has been given nephrotoxic drugs (e.g. gentamicin)
23
SEDATION CASE 1 Alexander Ewing is an 89 year old man who normally lives in a nursing home due to dementia. He is admitted to an orthopaedic ward following a fall in which he sustained a fractured neck of femur. He has very poor vision and is almost deaf. Nursing staff report that Mr Ewing is agitated and distressed at times, and they are struggling to stop him trying to climb out of bed. He has not had any treatment for agitation. When you arrive he is staggering around his room and in danger of falling. His current drugs are: Paracetamol 1g four times daily Senna 2 tabs at night Tolterodine MR 4mg once daily Chlorphenamine 4mg three times daily Prochlorperazine 5mg 6 – 8 hourly if needed nausea Tasks: 1. List the possible causes of Mr Ewing’s agitation and consider non-pharmacological measures that could be used. 2. Prescribe once off sedation to deal with the current issue on the prescription chart. Tutor notes:
• Consider causes: moved from familiar surroundings, pain, urine retention, constipation… Use non-pharmacological interventions as much as possible.
• Consider stronger analgesia as agitation may be due to pain – add low dose opiate like dihydrocodeine (30mg not 60mg) but will need to adjust laxatives.
• Also bear in mind that this elderly patient at risk of anticholinergic burden due to current medicines– the tolterodine, prochlorperazine and chlorphenamine all have anticholinergic side-effects – increased risk of falls and adverse effects. Advise stop the chlorphenamine and prochlorperazine.
• Link to Tranquillisation Policy NHS Grampian http://www.nhsgrampian.com/grampianfoi/files/NHSGRapTranq.pdf Assess the risk to patient and others, consider whether patient lacks capacity (he does). Adults with Incapacity Scotland Act 2000 or Mental Health (Care and Treatment)(Scotland) Act 2003.
• Offer oral meds before injectable – Lorazepam 1 – 2mg (or 500mcg – 2mg in frail/elderly) +/or Haloperidol 5mg (500mcg – 2mg in frail/elderly). Royal Cornhill Hospital may use Olanzapine in certain cases.
• This patient probably requires I.M haloperidol/lorazepam to settle safely in the acute situation – use minimum dose possible……same doses as for oral above, and give time for the medicine to work (30 minutes).
If using Lorazepam make sure antidote is available – Flumazenil. Flumazenil must be prescribed and administered by a doctor who has knowledge of the prescribing and administration of flumazenil.
24

SEDATION CASE 2 Jessie McDougall is a 55 year old woman who has been admitted with a pneumonia (CURB 2). She is concerned that she will not sleep in hospital and you have been asked to write up a sleeping tablet for her. She is haemodynamically stable and her oxygen saturations on 2 litres oxygen by nasal cannula is 96%. Prescribe (or not) an appropriate medicine. Tutor notes: Does she need this? Assess risk/benefit Could prescribe low dose Z-drug – e.g. Zopiclone 3.75mg at night or Zolpidem 5mg at night. Avoid benzodiazepine as may affect respiratory rate. Sedating anti-histamine (e.g. chlorphenamine) might be another option.
25
ACUTE PAIN CASE 1 A 20 year old man presents to A &E after falling off his bike. He is alert and conscious but in obvious distress and states that he is in “absolute agony”. You suspect that he has a simple fracture of the tibia but are awaiting an Xray to confirm. Your registrar asks you to prescribe some parenteral analgesia. Tasks: 1. Consider the issues around administering parenteral analgesia. 2. Prescribe a one off dose of your drug of choice on the prescription chart. Part 2 The fracture is confirmed and the registrar decides it does not need fixation. A plaster cast is applied. The nursing staff approach you and ask you to prescribe him some oral analgesia for when the IV analgesia wears off. 3. Consider the options and prescribe suitable analgesia. Tutor notes: IV morphine would be appropriate initially. They should note that they need to titrate the dose to response then prescribe it – make up 10mg and give slowly iv until desired response. As this is a controlled drug check students understand the ward procedure (locked cupboard, log book, 2 staff to sign out morphine). For the purposes of the prescription chart, they should write up no more than 10mg morphine. The dangers in a 20 year old fit man are less than other patients, but they should still be aware of respiratory depression. Discourage the use of IM NSAIDs, IV may be an option (parecoxib, ketorolac). Oral analgesia – they should probably not start at the bottom of the analgesic ladder given the severity of pain. A weak opiate and paracetamol would be one option; a NSAID and paracetamol might be another. They need to make an assessment. They should have previously been taught about the comparative efficacy of analgesics as well as synergistic use and you could emphasise these concepts.
26
ACUTE PAIN CASE 2 A 63 year old man is admitted to a medical ward with crushing retrosternal chest pain. His ECG shows ST depression and a NSTEMI is suspected. The nurses ask you to prescribe something for his pain. Prescribe your choice of analgesia on the prescription chart. Tutor notes: Should use IV morphine here as well as thinking of GTN as a specific treatment. IV Morphine should be given slowly 1 – 2 mg/minute, titrate to response. No more than 10mg. ALCOHOL WITHDRAWAL CASE 1 A 58 year old man is admitted to the medical ward with diarrhoea and vomiting. He is admits to drinking a couple of vodkas a day. He last had a drink 2 days ago and is quite shaky although he denies any issue. Both you and the nursing staff suspect he drinks more than he admits to (his GGT and MCV are noticeably raised). The nurses are keen that you write up something to prevent the DTs. Prescribe an appropriate regime for this man (he is managing oral intake). Tutor notes: In ARI, the medical wards tend to use 20mg diazepam four times daily and “as required” initially and then reduce quickly. No more than 120mg daily. In A&E a scoring system is used. IV Pabrinex (thiamine) should also be given for 48hours and then oral thiamine (100mg three times daily). Check students know that Pabrinex comes in pairs of ampoules (I + II) and given three times daily. There are 2 formulations (IM and IV) of Pabrinex – make sure right one used. If at risk of Wernickes can give 2 pairs. Given in 100mls of sodium chloride or glucose over 30 minutes – sometimes called affectionately as the “banana bag” as it is yellow. …Very small risk of anaphylaxis with IV form – make sure you know where the adrenaline is kept! Repeated injections may give rise to anaphylactic shock – watch for sneezing or shortness of breath developing. Any individual who has had negligible nutrient intake for more than 5 consecutive days is at risk of refeeding syndrome - Check risk of re-feeding syndrome – U&E, Phosphate, Mg, Calcium – will need supplements. Link to refeeding syndrome guidelines if required: http://www.nhsgrampian.com/grampianfoi/files/VitSupAC_503_1111.pdf
27

IV FLUIDS CASE 1 Mark Smith is a 45 yr old man is admitted at 0800 to a general surgical ward for a hernia repair and he is first on the list. He has been admitted electively and has been fasting since midnight. You receive a phone call from the anaesthetist to say that the operating list has been changed and this patients operation has been delayed to 4pm. The nursing staff bleep you to ask you to prescribe some fluids for this patient. Prescribe appropriate fluids on the IV infusion prescription chart. Tutor notes: No weight, look at patient, assess if dry. Ask them if they feel dry. Maintenance fluids are sufficient and it is reasonable to assume electrolytes etc are normal – approx 2.5 litres a day, with a mix of saline and dextrose and some potassium (say every second bag). NICE Guidelines at this link if required https://www.nice.org.uk/guidance/cg174 IV FLUIDS CASE 2 Mary McPherson is an 80 year old lady with history of 3 previous MI’s. She is admitted to medicine for the elderly with a urinary tract infection (confused and off legs). Her drugs include furosemide and antihypertensives. On examination she looks dry, HR 70 BP 90/40. Her bloods are: Na 154 K 3.7 Urea 21.2 Creat 173 Tasks: 1. Please prescribe initial IV fluids on the prescription chart. 2. Make a plan for further monitoring and fluids. Tutor notes: Needs fluids as dehydrated – dextrose would be a reasonable initial choice although 0.45% saline could be used. Will need maintenance potassium. Rate should be moderate – at risk of pulmonary oedema. Repeat U&Es next day; watch BP and for signs of fluid overload.
28
IV FLUIDS CASE 3 A 34 year old man (Andrew Wright) has had a short section of his distal ileum excised for Crohn’s disease. He is 2 days post-op and will probably not be able to eat and drink for another 2 days. He is stable. There are no blood results for today yet. This is his fluid chart. The nurses ask you to prescribe today’s fluids. Prescribe the fluids on the chart. He had 2 bags of normal saline on this chart (6 hourly). See IV fluids 3 overleaf Tutor notes: Young and fit so no real worries. Maintenance fluids essentially. Reasonable answer – dextrose; standard potassium 8 hourly; check bloods – could have second without potassium Best not to write up more than a bag or two at a time.
29

30

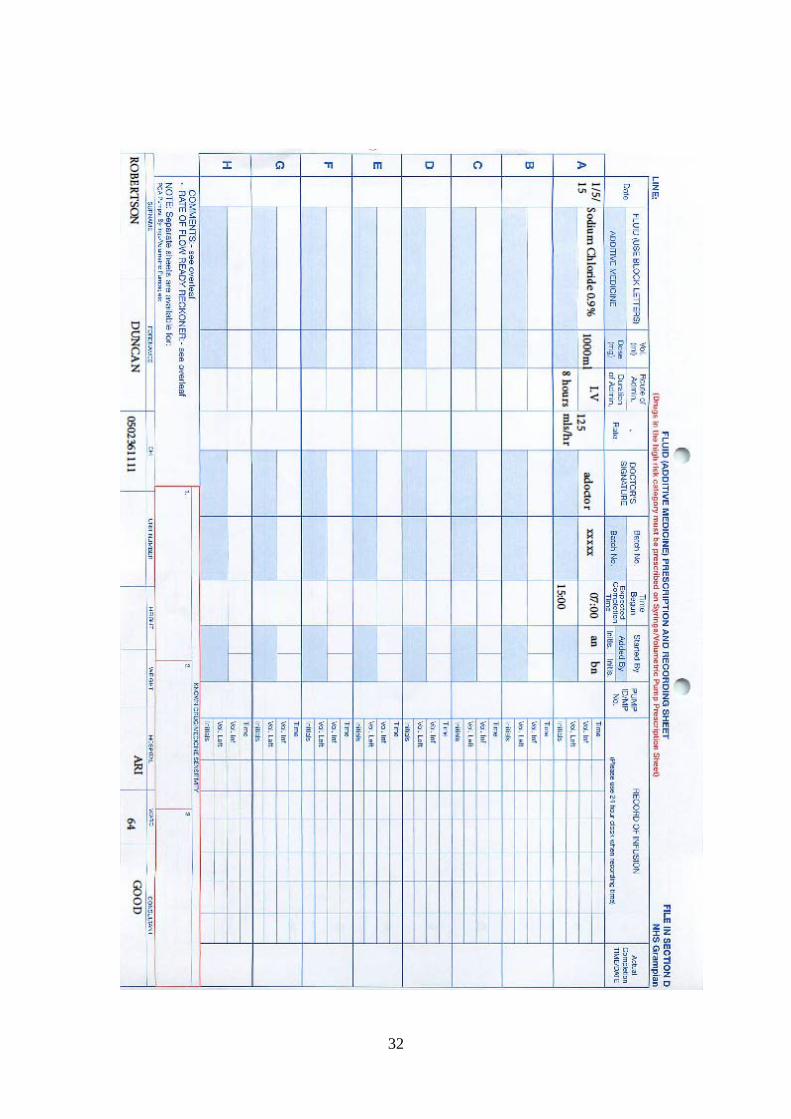
IV FLUIDS CASE 4 A 78 year old man (Duncan Robertson) has been admitted to the surgical ward with a subacute obstruction. He has no cardiac or renal history that you know about. He is initially treated conservatively with a large bore NG tube. He needs I.V fluids as he is nil by mouth. On examination, he looks a little dry, with a HR of 100bpm, BP 120/56. Bloods today are: Na 144 K 5.2 Urea 15.3 Creat 120 These are his charts – urine output 200 mls today; NG output 500mls (until about 15:00, admitted at 06:00) Has had 1 bag of saline over 8 hours so far See IV fluids chart overleaf Please prescribe appropriate fluids. Tutor notes:
• Should consider all losses, maintenance requirements, insensible loss • NG output at this rate might be 1-1.5l over 24 hours • Maintenance approx 2l/24 hrs • Probably a little dry • Caution given age and possible renal/cardiac issues • Reasonable answer – dextrose with no potassium at 6 hourly
31
32

DIABETES PRESCRIBING DIABETES PATIENT ONE Mr David King (CHI 2307752209) has Type 1 Diabetes Mellitus and has presented into the AMAU with shortness of breath and cough. He has been diagnosed with pneumonia and is able to eat and drink. He is on a basal bolus regimen. Novorapid 6 units before breakfast, 8-10 units before lunch and 10-12 units before teatime. He takes his Levemir 12 units at bedtime. Hours 1 - 2 All his medications have been written up apart from his diabetes chart. Prescribe his diabetes medication. His blood sugar is currently 17. What other information do you want to know? Tutor Notes Blood sugar is 17 – need to check for ketones. At risk of developing DKA. Check concordance with therapy – any missed/omitted doses? Could keep on normal insulin but write up safety net doses of Novorapid. Check patients understanding of “sick day rules” – ask students what these are. Note NHS Grampian diabetes prescription sheet will be changing, being piloted 2015. Current one is inadequate. Useful websites www.nhsgrampian.org/guidelines/diabetes http://www.diabetes-healthnet.ac.uk/Default.aspx?pageid=201 Hours 3 - 4 David was commenced on antibiotics but he began to vomit and was unable to keep anything down. It turns out he had also missed his morning insulin. His blood glucose was now 22 and he had 3 plus ketones and 4.2 blood ketones. Task 1: What should be the next step in his management? Signs? Task 2: As suspected he has developed DKA – see the protocol attached. Prescribe fluids and insulin treatment regime on DKA prescription pathway sheet. Tutors notes See attached DKA Pathway 1 prescription sheet – no other prescription sheet is required. Pointers for DKA management on the protocol. This is not a tutorial on DKA management so keep brief. Can also mention the variable rate insulin prescription sheet which is used in non-DKA situations – insulin pumps are always Actrapid (or Novorapid in Sick Kids) 50 units up to 50mls sodium chloride 0.9%.
33

David King Model Prescription Sheet (page 2 of DKA sheet):
34
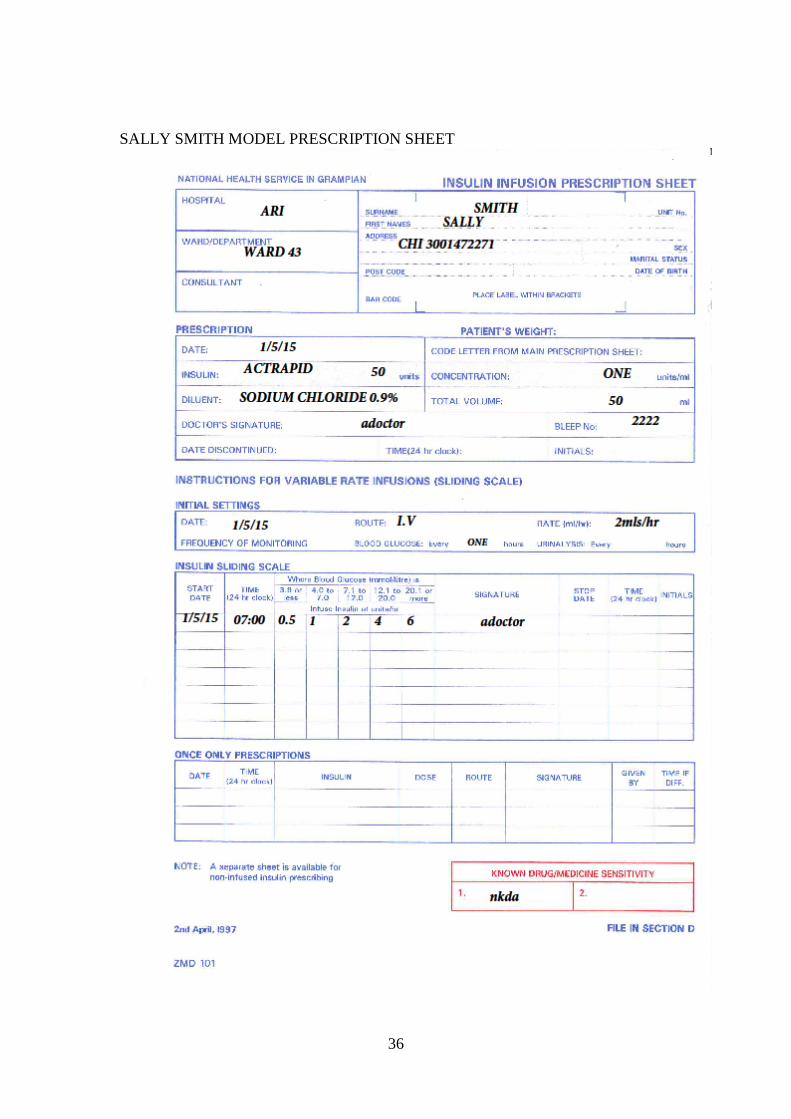
DIABETES PATIENT TWO Sally Smith (CHI 3001472271) has Type 1 Diabetes she is due to have a hysterectomy the following day on ARI Ward 43. Her usual insulin is Novomix 30 at doses of 26 units before breakfast and 14 units before tea. She is listed for surgery in the morning. Please prescribe her insulin and discuss the next step of her management. When do you recommence her insulin and what do you do? Tutor Notes See following prescription sheet for model answer. There are pre-printed variable rate insulin prescription sheets for this available on some wards (in student pack) but ask students to try and fill in the “Insulin Infusion Prescription Sheet” for practice. 50units of Actrapid up to 50mls sodium chloride 0.9%. (Sick Kids use Novorapid). Initial rate will depend on initial blood glucose reading. If blood glucose greater than 14 check every 30 minutes. Ask nurses to inform medical staff if BG greater than 14 mmol/l and rate already 6mls/hr. Check for ketones. The insulin pump can be commenced morning of surgery ie when due next meal but if want good control can commence 12 midnight. Watch for hypoglycaemia if had s/c insulin. When pump starts they are on hourly blood sugars – remember the patients fingers! Concurrent IV fluids will need prescribed also on fluid prescription sheet – glucose must always run concurrently with insulin. e.g. Glucose 4% + 0.18% sodium chloride + 0.15% potassium chloride at 100mls/hr. Recommence normal insulin when eating and drinking. Stop pump 30 - 60 minutes after had Novomix.
35
SALLY SMITH MODEL PRESCRIPTION SHEET
36
Chest pain case Mr Michael Mouse (65) has no significant previous medical history. He is admitted to ARI Ward 101 with chest pain. Serial ECGs show no ST changes but a significant rise on Troponin-1 and he has been diagnosed with an NSTEMI. Following consultation with seniors it was decided not to proceed to PCI. eGFR>60mls/min, BP 165/90 mmHg, Pulse 66/min in SR.
1. Prescribe initial treatment for Mr Mouse 2. Prescribe secondary prevention medications Tutor notes NICE pathway ACS http://pathways.nice.org.uk/pathways/acute-coronary-syndromes 1. Initial treatment – GTN and/or Morphine (with anti-emetic)+/- oxygen if
pain. Fondaparinux 2.5mg SC once daily for up to 8 days (or until hospital discharge if sooner). Stat doses of Aspirin 300mg and Ticagrelor 180mg.
2. Lifestyle advice Plus Low dose Aspirin 75mg daily longterm + Ticagrelor 90mg twice daily for 1 year. Remember to consider increased bleeding risk with this combination. Plus ACE inhibitor – e.g. Ramipril 2.5mg twice daily and ask GP to uptitrate to 5mg twice daily if tolerated Plus a statin – e.g simvastatin 40mg at night or atorvastatin 80mg daily. Betablocker – e.g bisoprolol or carvedilol, start low within 24 hours of ACS and go slow. Plus “as required” GTN spray 1 or 2 sprays s/l
37