
Warm up angina / Pre-conditioning symposium_Chest Pain...Acute Chest Rest Pain Syndrome High Risk...
29
Warren NEJM 1812 Jan Warm up angina / Pre-conditioning
Transcript of Warm up angina / Pre-conditioning symposium_Chest Pain...Acute Chest Rest Pain Syndrome High Risk...
Warren NEJM 1812 Jan
Warm up angina / Pre-conditioning
Warren NEJM 1812 Jan
Warm up angina / Pre-conditioning

Rezkalla S H (2004) Ischemic preconditioning and preinfarction angina in the clinical arena. Nat Clin Pract
Cardiovasc Med 1: 96–102 doi:10.1038/ncpcardio0047
Figure 2 Factors affecting preconditioning and its impact on cardiac events

Chest Pain
Rest Pain
High Risk Features
Duration 20-30 mins
Diaphoresis / SOB
After Food / Shower
Pre-conditioning
Diffuse pain
Radiation to arms / jaws
Severe
Urgent referral
Low risk features
Short Duration < 5 mins
Focal Pain
With Oily Food
Likely non-cardiac
Symptomatic Treatment
Consider referral if persistant
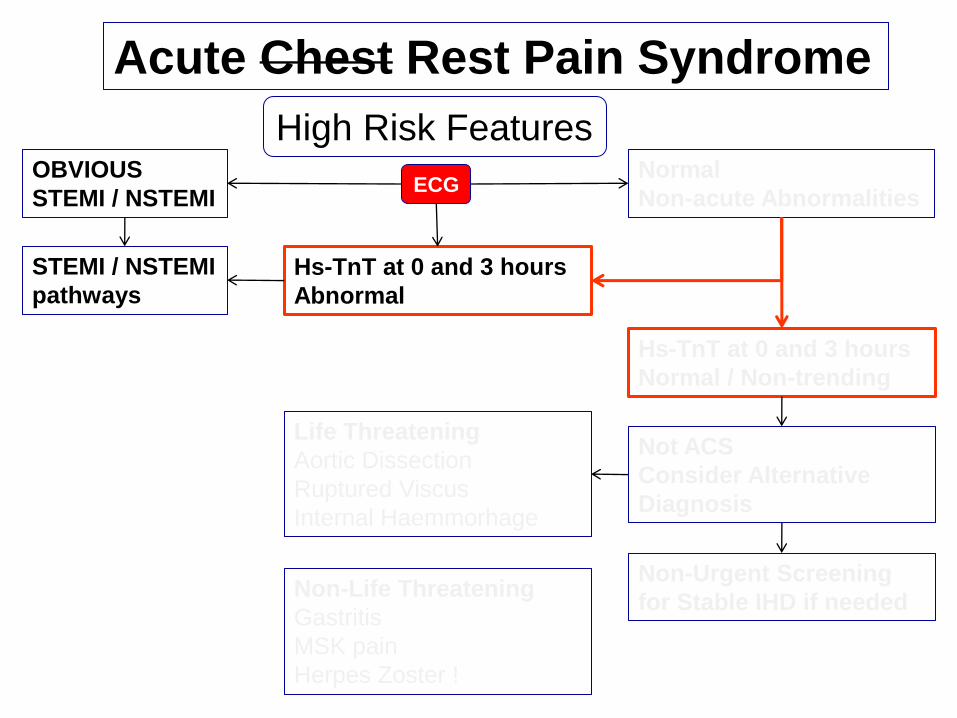
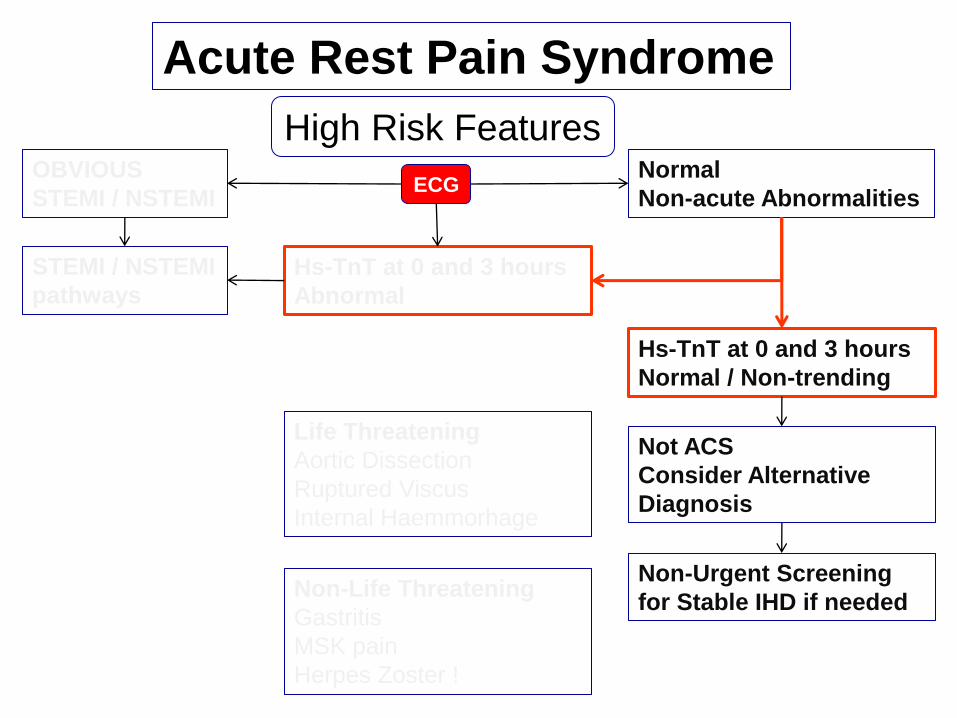
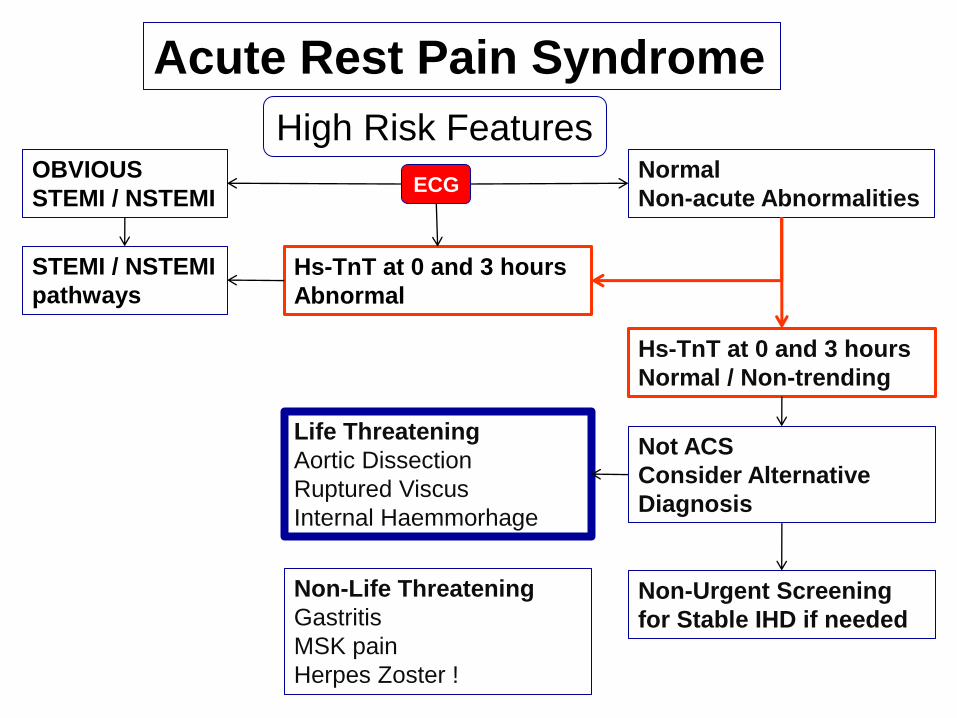
Acute Chest Rest Pain Syndrome
High Risk Features
ECG OBVIOUS
STEMI / NSTEMI
STEMI / NSTEMI
pathways
Normal
Non-acute Abnormalities
Hs-TnT at 0 and 3 hours
Normal / Non-trending
Hs-TnT at 0 and 3 hours
Abnormal
Not ACS
Consider Alternative
Diagnosis
Non-Urgent Screening
for Stable IHD if needed
Life Threatening
Aortic Dissection
Ruptured Viscus
Internal Haemmorhage
Non-Life Threatening
Gastritis
MSK pain
Herpes Zoster !
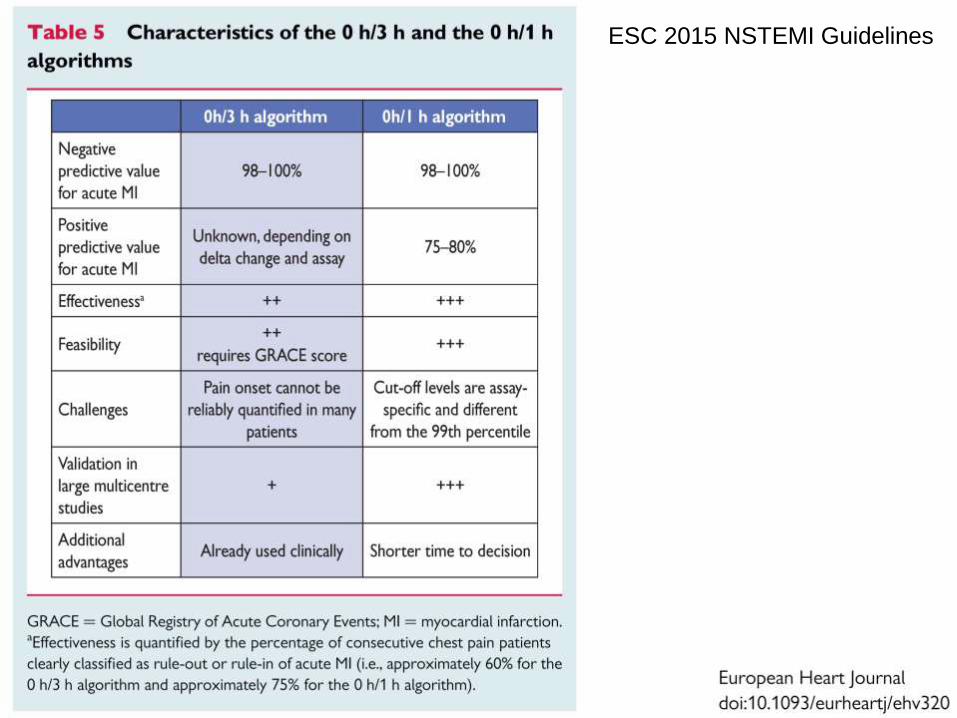
ESC 2015 NSTEMI Guidelines
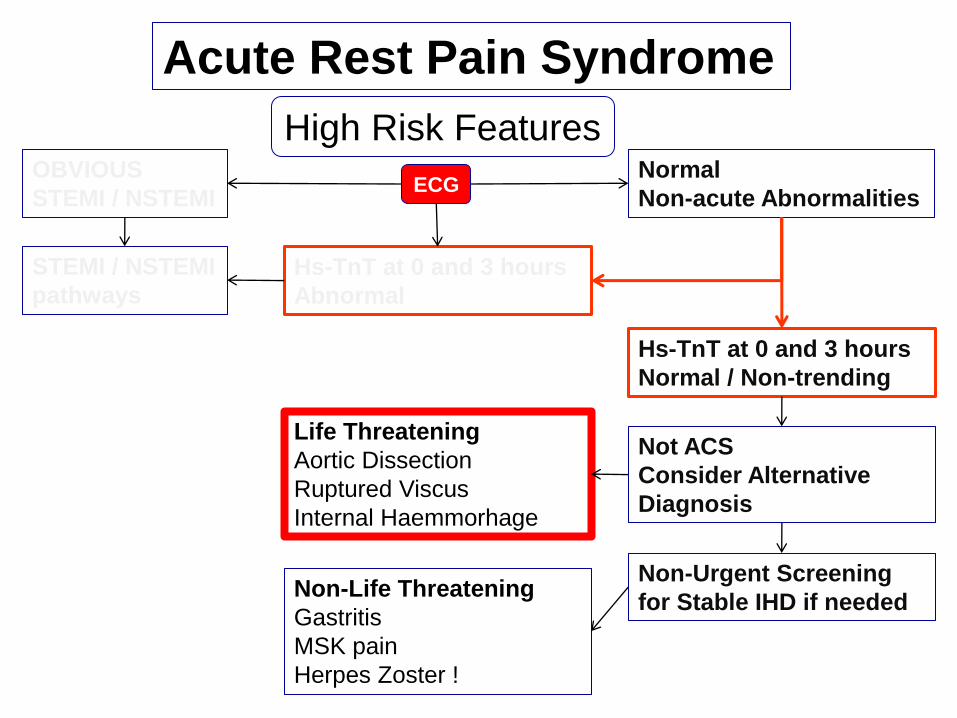
Acute Rest Pain Syndrome
High Risk Features
ECG OBVIOUS
STEMI / NSTEMI
STEMI / NSTEMI
pathways
Normal
Non-acute Abnormalities
Hs-TnT at 0 and 3 hours
Normal / Non-trending
Hs-TnT at 0 and 3 hours
Abnormal
Not ACS
Consider Alternative
Diagnosis
Non-Urgent Screening
for Stable IHD if needed
Life Threatening
Aortic Dissection
Ruptured Viscus
Internal Haemmorhage
Non-Life Threatening
Gastritis
MSK pain
Herpes Zoster !
Acute Rest Pain Syndrome
High Risk Features
ECG OBVIOUS
STEMI / NSTEMI
STEMI / NSTEMI
pathways
Normal
Non-acute Abnormalities
Hs-TnT at 0 and 3 hours
Normal / Non-trending
Hs-TnT at 0 and 3 hours
Abnormal
Not ACS
Consider Alternative
Diagnosis
Non-Urgent Screening
for Stable IHD if needed
Life Threatening
Aortic Dissection
Ruptured Viscus
Internal Haemmorhage
Non-Life Threatening
Gastritis
MSK pain
Herpes Zoster !
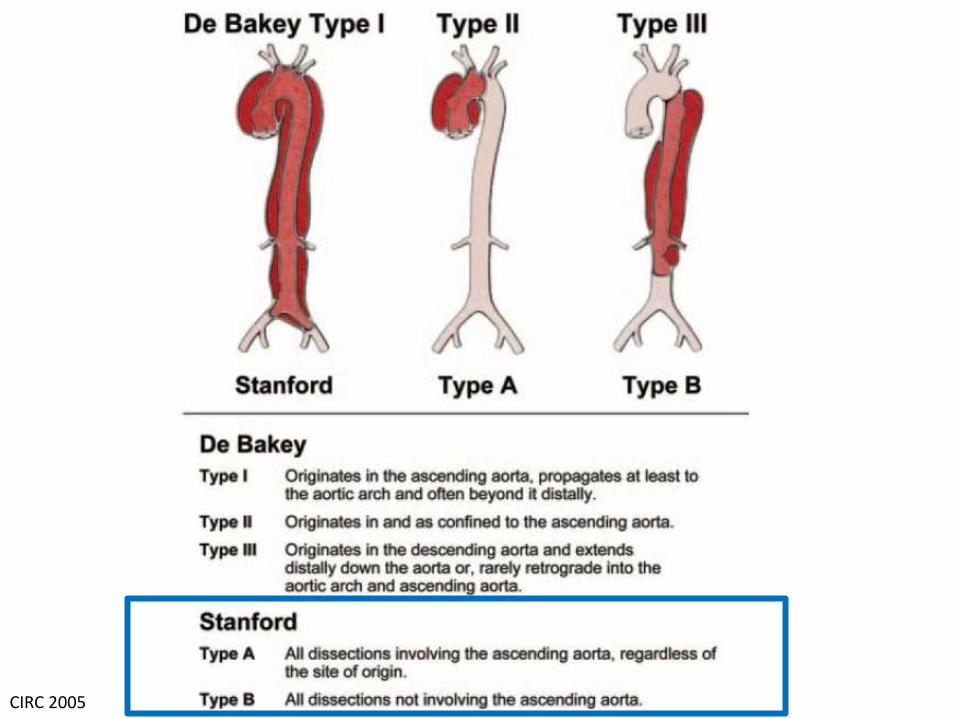
CIRC 2005
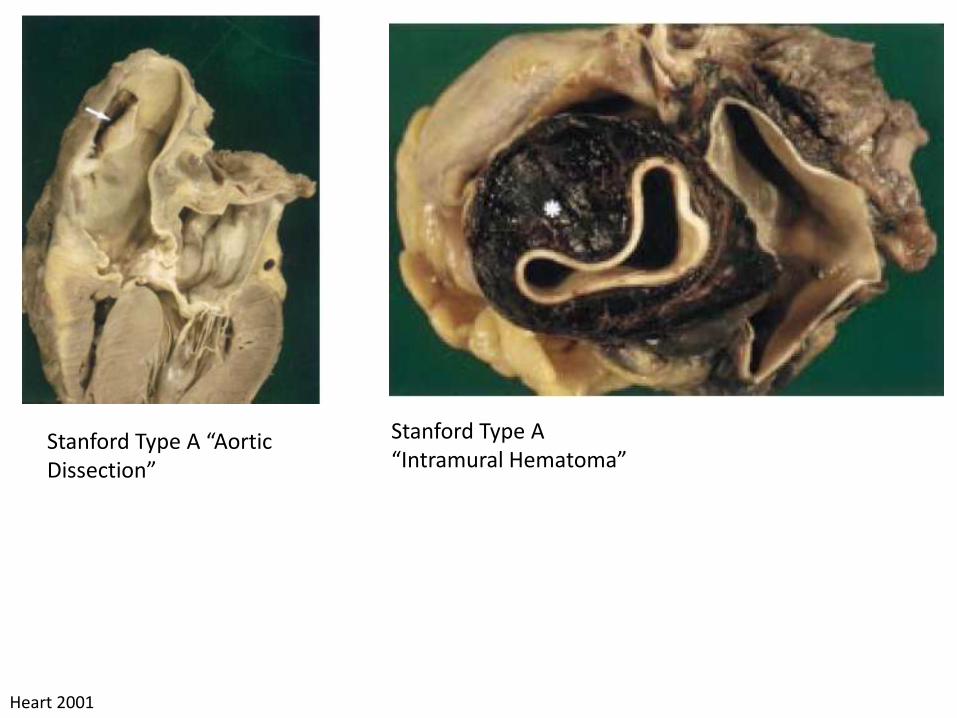
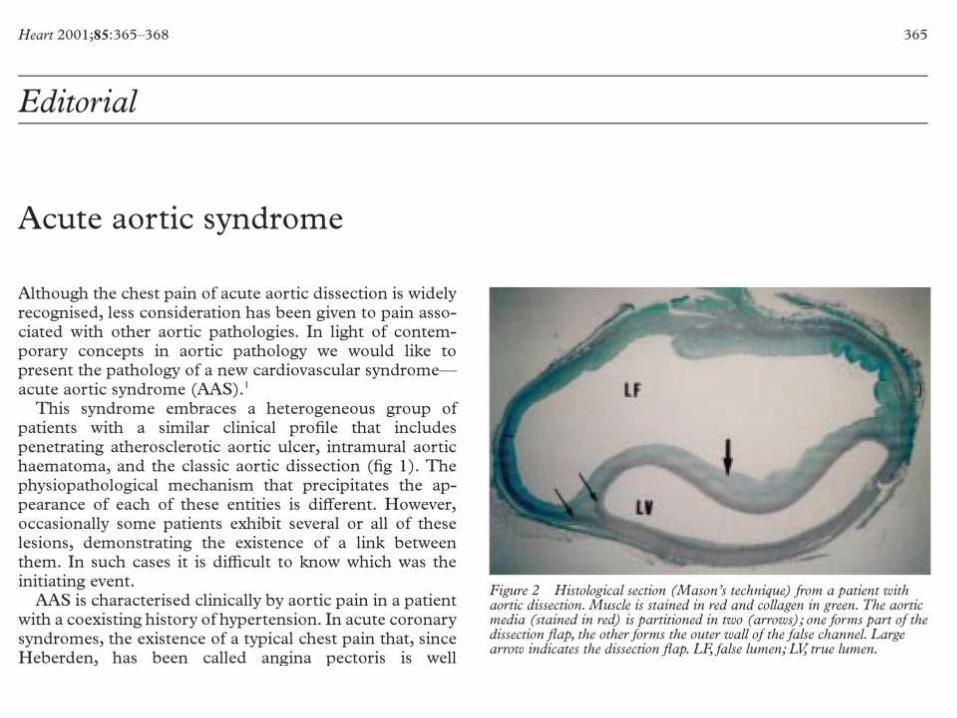
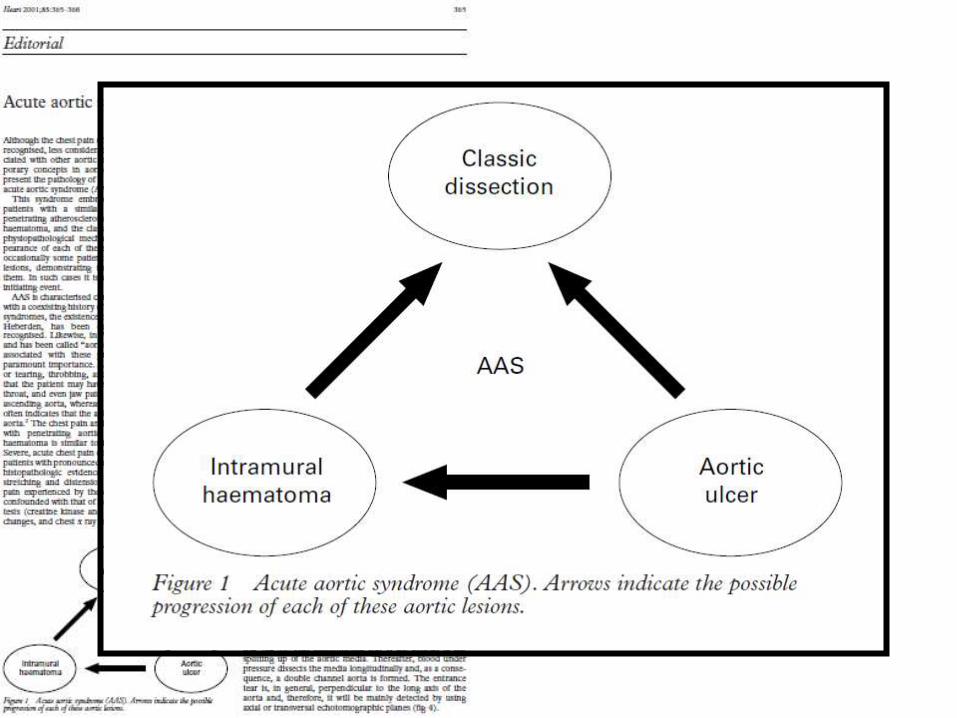
Heart 2001
Stanford Type A “Aortic Dissection”
Stanford Type A “Intramural Hematoma”
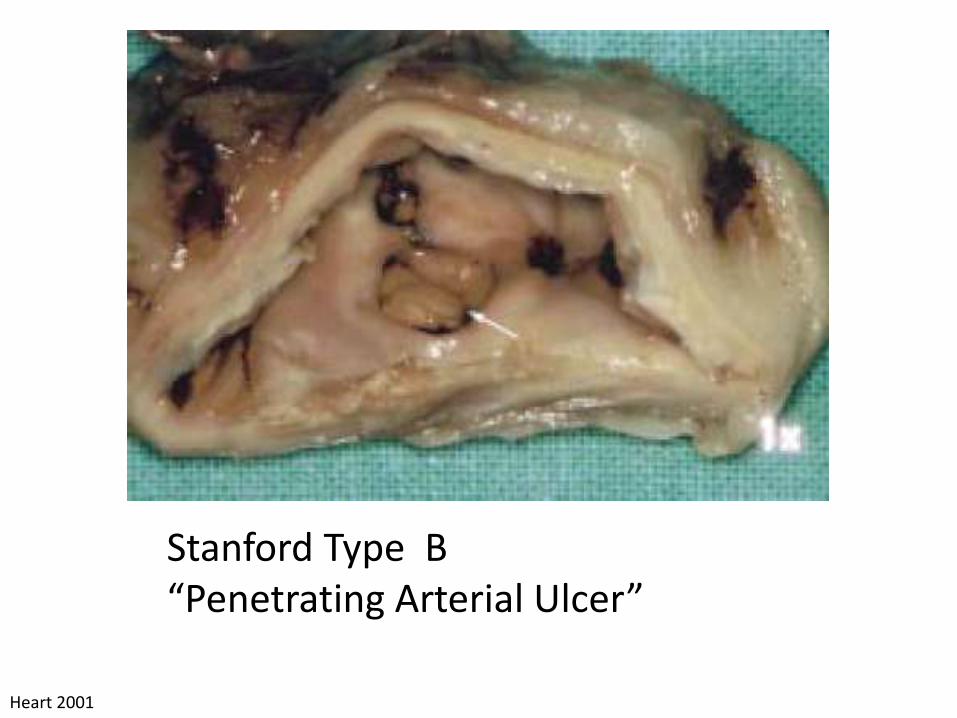
Stanford Type B “Penetrating Arterial Ulcer”
Heart 2001
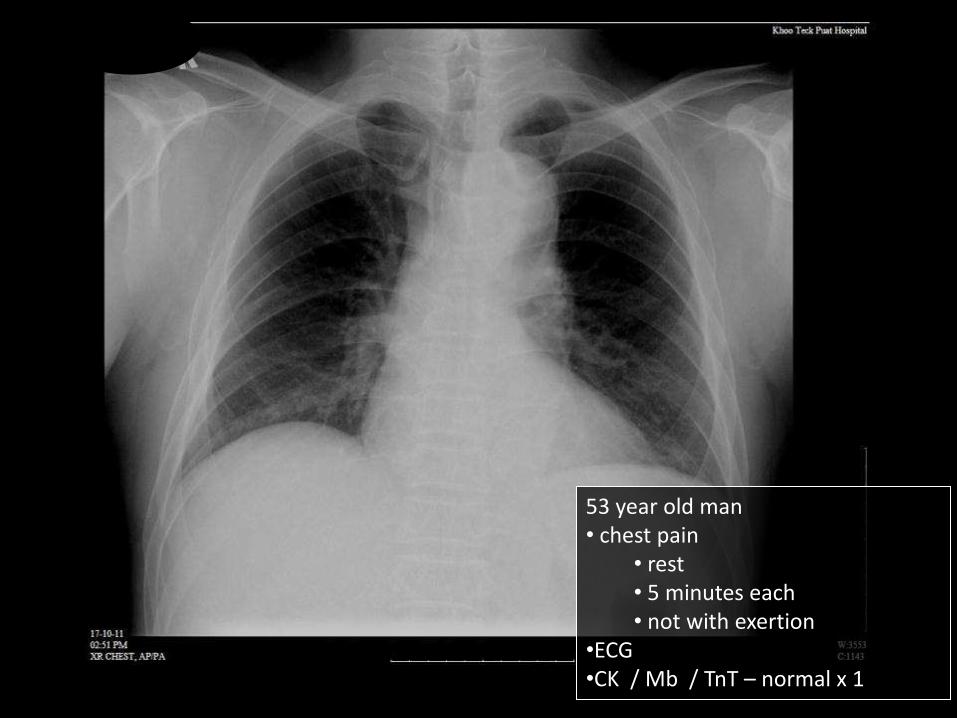
53 year old man • chest pain
• rest • 5 minutes each • not with exertion
•ECG •CK / Mb / TnT – normal x 1
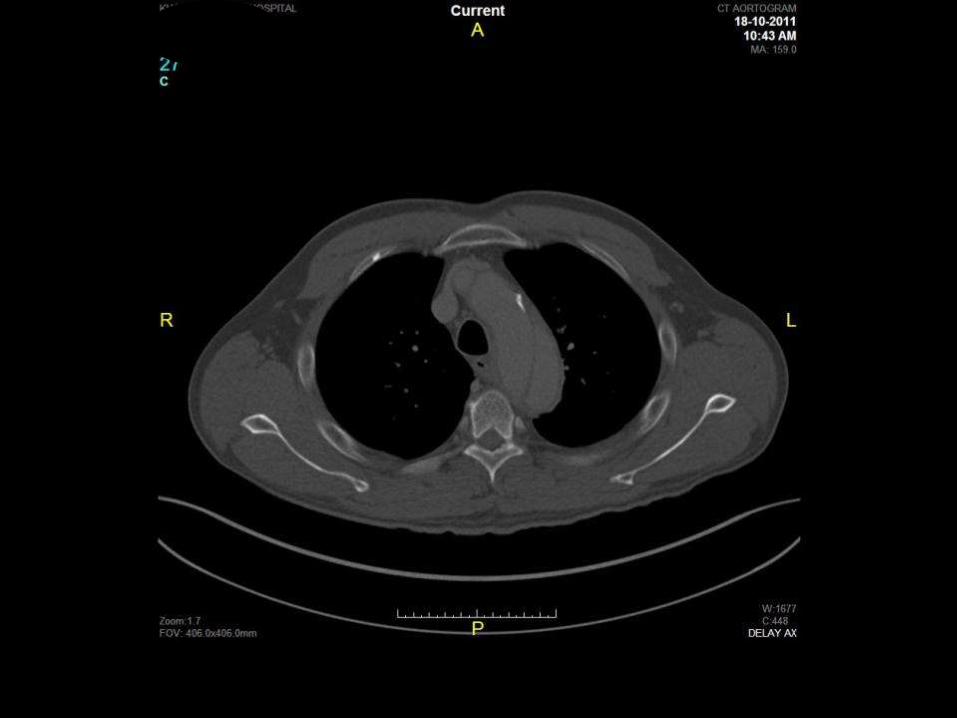
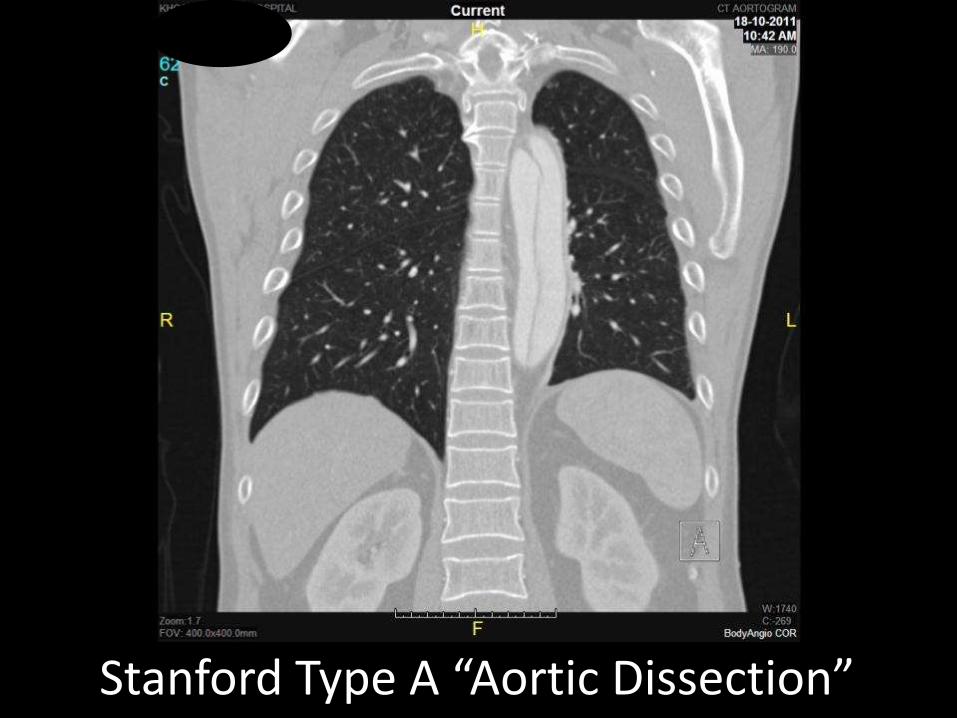
Stanford Type A “Aortic Dissection”
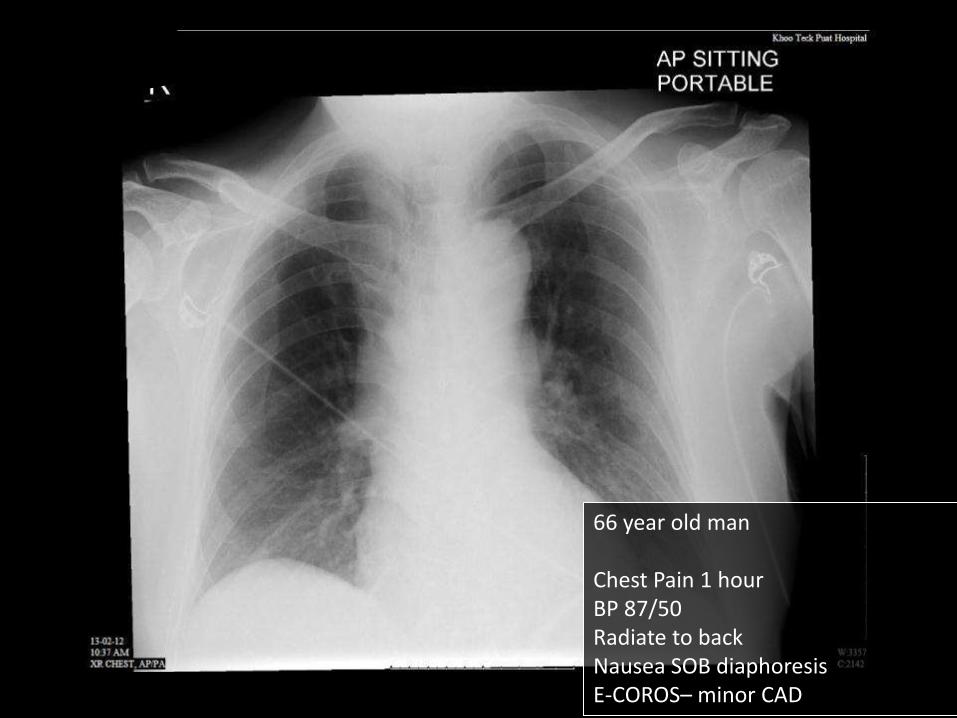
66 year old man Chest Pain 1 hour BP 87/50 Radiate to back Nausea SOB diaphoresis E-COROS– minor CAD

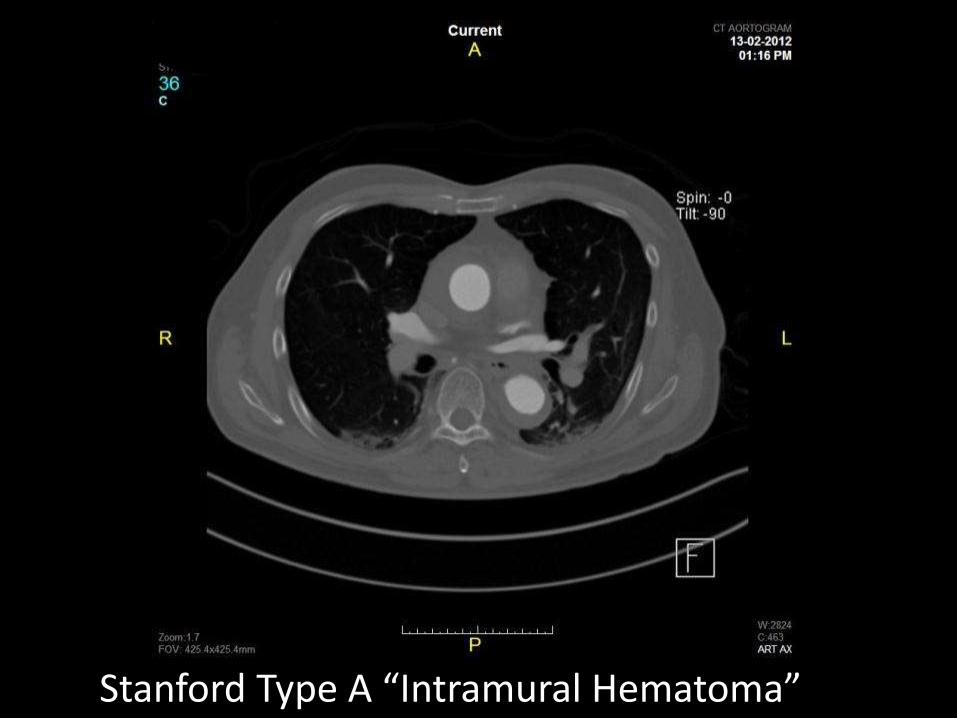
Stanford Type A “Intramural Hematoma”
Diagnosis
History
CXR
ECG
D-dimers

D-Dimers
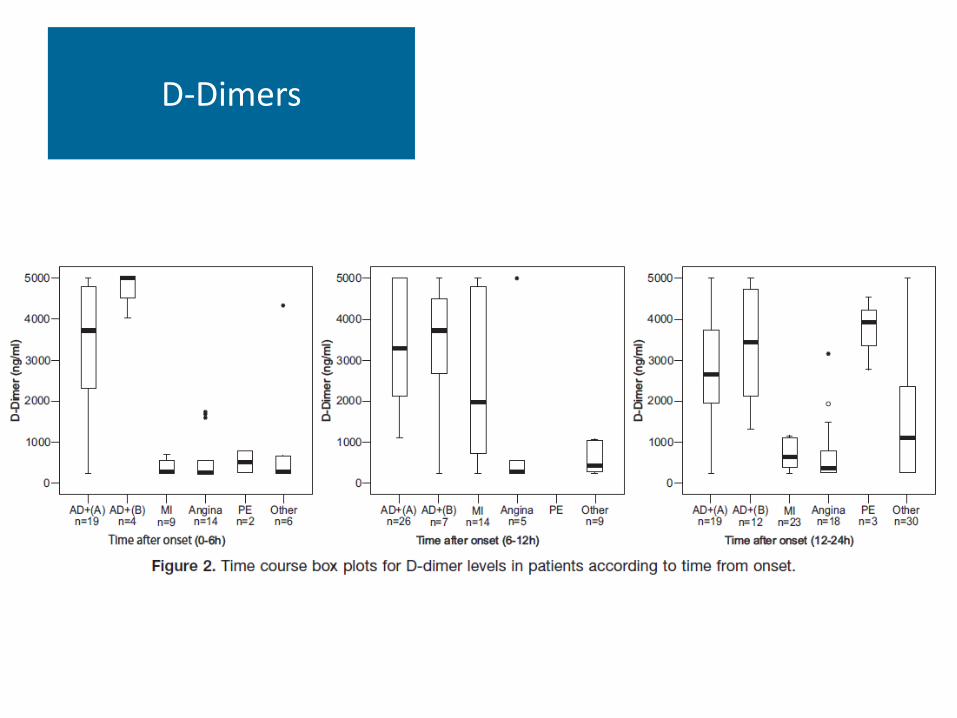
D-Dimers

D-Dimers
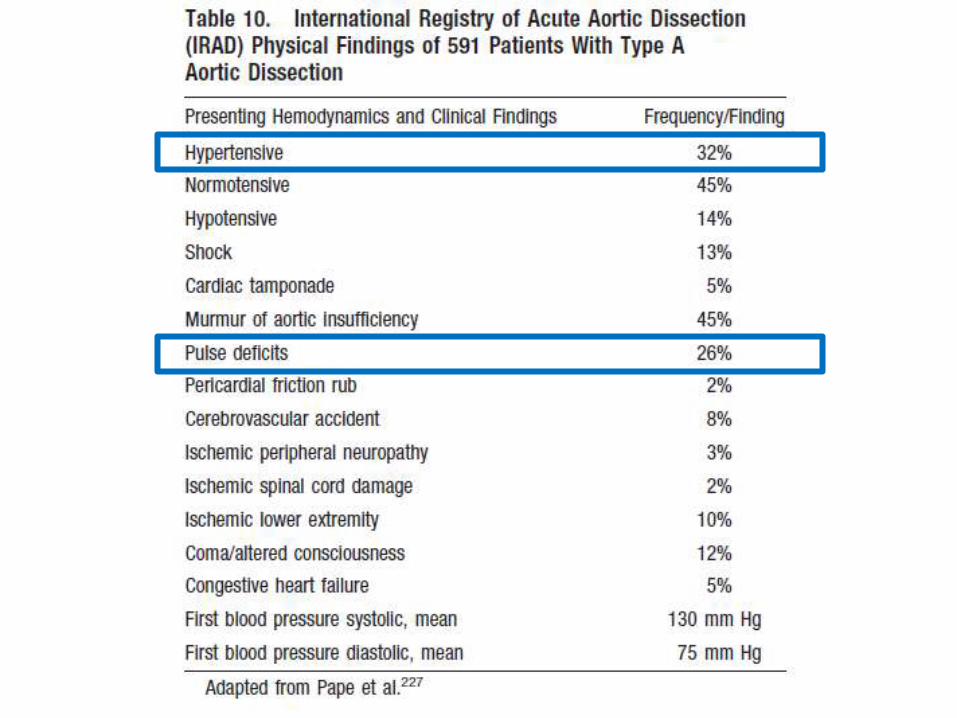
Clinical Pain – severe and acute Pulse deficit > 20 mm Hg Evidence of Aortic regurgitation Family History Associated Connective Tissue (Marfan’s)
High Risk Features
ECG – MI is much more common CXR – normal does not exclude TEE / CT / MRI depending on local resources Repeat if negative and clinically suspicious
Tests
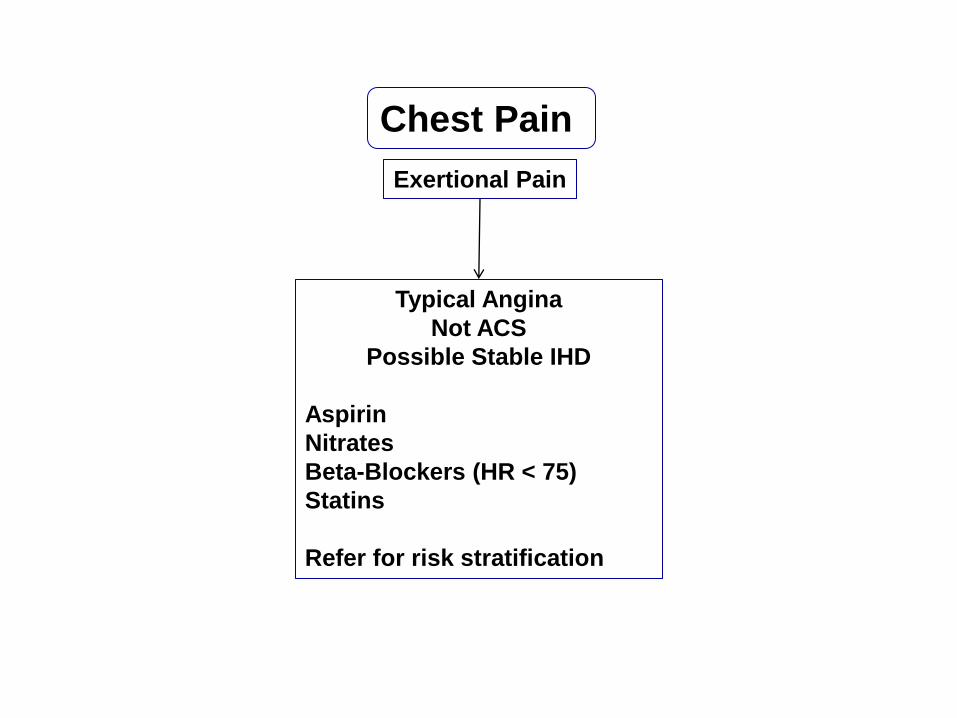
Chest Pain
Exertional Pain
Typical Angina
Not ACS
Possible Stable IHD
Aspirin
Nitrates
Beta-Blockers (HR < 75)
Statins
Refer for risk stratification
Acute Rest Pain Syndrome
High Risk Features
ECG OBVIOUS
STEMI / NSTEMI
STEMI / NSTEMI
pathways
Normal
Non-acute Abnormalities
Hs-TnT at 0 and 3 hours
Normal / Non-trending
Hs-TnT at 0 and 3 hours
Abnormal
Not ACS
Consider Alternative
Diagnosis
Non-Urgent Screening
for Stable IHD if needed
Life Threatening
Aortic Dissection
Ruptured Viscus
Internal Haemmorhage
Non-Life Threatening
Gastritis
MSK pain
Herpes Zoster !



















