Volume 5 // Issue 2 // June 2020
72
Contents EDITORIAL 27 Cardiovascular Healthcare in 2020 – Alarming Realities in Romania Roxana Hodas REVIEW 30 Disease Burden, Mechanism and Management of Obesity – Where Do We Stand? Irfan Sharif Shakoori, Gohar Ashraf, Fauzia Aslam, Hammad Akram ORIGINAL RESEARCH 35 Effects of Pirfenidone on Echocardiographic Parameters of Left Ventricular Structure and Function in Patients with Idiopathic Pulmonary Fibrosis Shehab Al-Ansari, Allen Borowski, Ali Fuad, Omar Alawadhi, Haris Riaz, Vikram Sharma, Nauman Khan, Brian D. Southern, W.H. Wilson Tang 43 Malaria and HIV Infection among Febrile Patients in a Large Area of Southwestern Nigeria Oyetunde T. Oyeyemi, Edet J. Etim 48 Ultrasound-Guided Core-Needle Biopsy of Suspicious Breast Lesions Kincső-Zsófia Lőrincz, Zsuzsánna Pap, Simona Lileana Mocan, Csanád-Endre Lőrincz, Beáta-Ágota Baróti 56 Proper Surgical Treatment of Small and Medium Size Umbilical Hernias. A Single Surgeon Experience Etele Élthes, Daniela Sala, Radu Mircea Neagoe, János Székely, Márton Dénes 64 Epicardial Fat Volume as a New Imaging-Based Feature Associated with Risk of Recurrence after Pulmonary Veins Ablation in Atrial Fibrillation Emanuel Blîndu, Szilamér Korodi, Lehel Bordi, István Kovács, Imre Benedek ORIGINAL RESEARCH / / BRIEF REPORT 71 Incidence of Periodontal Disease among Adolescents Delia-Roxana Dicu, Ana Petra Lazăr, Luminița Lazăr 76 Immunosuppressive Medication and Non- Rejection-Related Complications Following Heart Transplantation Dumitru Costel, Dana Ghiga, Simona Voidazan, Alexandra Grosan, Dan Simpalean, Anca Sin CASE REPORT 81 Acute Drug-Induced Cholestatic Syndrome in Basedow Graves’ Disease Robert Aurelian Tiucă, Alina Mioara Boeriu, Rareș Adrian Georgescu, Ionela Maria Pașcanu Volume 5 / / Issue 2 / / June 2020
Transcript of Volume 5 // Issue 2 // June 2020

Contents
Editorial
27 Cardiovascular Healthcare in 2020 – Alarming Realities in Romania
Roxana Hodas
rEViEW
30 Disease Burden, Mechanism and Management of Obesity – Where Do We Stand?
Irfan Sharif Shakoori, Gohar Ashraf, Fauzia Aslam,
Hammad Akram
oriGiNal rESEarCH
35 Effects of Pirfenidone on Echocardiographic Parameters of Left Ventricular Structure and Function in Patients with Idiopathic Pulmonary Fibrosis
Shehab Al-Ansari, Allen Borowski, Ali Fuad, Omar
Alawadhi, Haris Riaz, Vikram Sharma, Nauman Khan,
Brian D. Southern, W.H. Wilson Tang
43 Malaria and HIV Infection among Febrile Patients in a Large Area of Southwestern Nigeria
Oyetunde T. Oyeyemi, Edet J. Etim
48 Ultrasound-Guided Core-Needle Biopsy of Suspicious Breast Lesions
Kincső-Zsófia Lőrincz, Zsuzsánna Pap, Simona Lileana
Mocan, Csanád-Endre Lőrincz, Beáta-Ágota Baróti
56 Proper Surgical Treatment of Small and Medium Size Umbilical Hernias. A Single Surgeon Experience
Etele Élthes, Daniela Sala, Radu Mircea Neagoe, János
Székely, Márton Dénes
64 Epicardial Fat Volume as a New Imaging-Based Feature Associated with Risk of Recurrence after Pulmonary Veins Ablation in Atrial Fibrillation
Emanuel Blîndu, Szilamér Korodi, Lehel Bordi, István
Kovács, Imre Benedek
oriGiNal rESEarCH // briEf rEport
71 Incidence of Periodontal Disease among Adolescents
Delia-Roxana Dicu, Ana Petra Lazăr, Luminița Lazăr
76 Immunosuppressive Medication and Non-Rejection-Related Complications Following Heart Transplantation
Dumitru Costel, Dana Ghiga, Simona Voidazan,
Alexandra Grosan, Dan Simpalean, Anca Sin
CaSE rEport
81 Acute Drug-Induced Cholestatic Syndrome in Basedow Graves’ Disease
Robert Aurelian Tiucă, Alina Mioara Boeriu, Rareș Adrian
Georgescu, Ionela Maria Pașcanu
Volume 5 // Issue 2 // June 2020


Editorial Board
Editor-iN-CHiEf
Theodora Benedek Clinic of Cardiology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Center for Advanced Research in Multimodality Cardiac Imaging, Cardio Med Medical Center, Târgu Mureș, Romania
dEputy EditorS
Charalambos AntoniadesDivision of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, UK
Imre BenedekClinic of Cardiology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Christos ChantziantoniouUniversité Pierre-et-Marie-Curie, Sorbonne Uni-versités, Paris, France
Dietmar GlogarMedical University of Vienna, Austria
Ota HlinomazClinic of Cardiology, University of Brno, Czech Republic
Monica Marton PopoviciDepartment of Critical Care, Swedish Hospitals, Seattle, USA
maNaGiNG EditorS
Diana OpincariuUniversity of Medicine and Pharmacy, Târgu Mureș, Romania
Nóra RatUniversity of Medicine and Pharmacy, Târgu Mureș, Romania
Editorial board
Charalambos AntoniadesDivision of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, UK
Vladimir BacâreaDepartment of Research Methodology, Univer-sity of Medicine and Pharmacy, Târgu Mureș, Romania
Simona BățagăClinic of Gastroenterology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Imre BenedekClinic of Cardiology, University of Medicine and Pharmacy Târgu Mureș, Romania
Carmen BirișDepartment of Dental Health, University of Medi-cine and Pharmacy Târgu Mureș, Romania
Elena BobescuClinic of Cardiology, "Transilvania" University, Brașov, Romania
Florin BuicuDepartment of Public Health, University of Medi-cine and Pharmacy, Târgu Mureș, Romania
Simona CerneaDepartment of Internal Medicine, University of Medicine and Pharmacy, Târgu Mureș, Romania
Christos ChantziantoniouUniversité Pierre-et-Marie-Curie, Sorbonne Uni-versités, Paris, France
Călin ChibeleanClinic of Urology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Monica ChițuClinic of Cardiology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Radu Ciudin"Carol Davila" University of Medicine and Phar-macy, București, Romania
István ÉdesUniversity of Debrecen, Hungary
Dan GeorgescuClinic of Gastroenterology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Dietmar GlogarMedical University of Vienna, Austria
Mariann GyöngyösiMedical University of Vienna, Austria
Ota HlinomazClinic of Cardiology, University of Brno, Czech Republic
Adrian IancuClinic of Cardiology, "Iuliu Hațieganu" University of Medicine and Pharmacy, Cluj Napoca, Romania
Radu IliescuDepartment of Physiology, University of Medicine and Pharmacy, Iași, Romania
Piroska KelemenClinic of Internal Medicine, University of Medicine and Pharmacy, Târgu Mureș, Romania
István KovácsClinic of Cardiology, University of Medicine and Pharmacy Târgu Mureș, Romania
Erzsébet LázárClinic of Haematology and Stem Cell Transplanta-tion, University of Medicine and Pharmacy, Târgu Mureș, Romania
Marius George LinguraruSheikh Zayed Institute for Pediatric Surgical Innovation, Children’s National Health System, Washington DC, USA
Monica Marton PopoviciDepartment of Critical Care, Swedish Hospitals, Seattle, USA
Pál Maurovich HorváthSemmelweis University, Budapest, Hungary
Călin MolnarClinic of Surgery, University of Medicine and Phar-macy, Târgu Mureș, Romania
Anca NegovanClinic of Internal Medicine, University of Medicine and Pharmacy, Târgu Mureș, Romania
Dan OlinicClinic of Cardiology, "Iuliu Hațieganu" University of Medicine and Pharmacy, Cluj Napoca, Romania

iNdExiNG
The Journal of Interdisciplinary Medicine is indexed via De Gruyter Open in the following international databases:
•Baidu Scholar•Celdes•CNKI Scholar (China National Knowledge
Infrastructure)•CNPIEC•EBSCO Discovery Service•Google Scholar
• J-Gate•Naviga (Softweco)•Primo Central (ExLibris)•ReadCube•Summon (Serials Solutions/ProQuest)•TDOne (TDNet)•WorldCat (OCLC)
Mihaela OprișClinic of Cardiology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Zoltán PávaiDepartment of Pathology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Maria PeleFaculty of Biotechnology, University of Agronomic Sciences and Veterinary Medicine, București, Romania
Alexandru Rafila"Carol Davila" University of Medicine and Phar-macy, București, Romania
Alexandru Rogobete"Victor Babeș" University of Medicine and Phar-macy, Timișoara, Romania
Simona StolnicuDepartment of Pathology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Mónika SzabóClinic of Diabetology, University of Medicine and Pharmacy, Târgu Mureș, Romania
Sándor SzilágyiDepartment of Medical Informatics, "Petru Maior" University, Târgu Mureș, Romania
Tamás Szili-TörökErasmus Medical Center, Rotterdam, The Neth-erlands
Mariana TilincaDepartment of Cell and Molecular Biology, Univer-sity of Medicine and Pharmacy, Târgu Mureș, Romania
Rodica TogănelClinic of Pediatric Cardiology, University of Medi-cine and Pharmacy, Târgu Mureș, Romania
Ioan ȚileaClinic of Cardiovascular Rehabilitation, Univer-sity of Medicine and Pharmacy, Târgu Mureș, Romania
Lia Yero EremieDepartment of Dental Health, University of Medi-cine and Pharmacy, Târgu Mureș, Romania
Endre ZimaSemmelweis University, Budapest, Hungary
tECHNiCal Editor
Zoltán Sárkány

The Journal of Interdisciplinary Medicine aims to publish top quality papers related to any fields of medicine that present an interdisciplinary dimension.
The journal will mainly focus on recent advances in the field of diagnosis and treatment of the most common situations encountered in the clinical or research prac-tice. Interdisciplinary approaches will be extremely wel-comed, presenting new advances in the approach of dif-ferent pathologies from the perspective of various clinical fields.
The Journal of Interdisciplinary Medicine will publish high-quality basic and clinical research related to interdis-
ciplinary medical fields, in a common approach that will integrate the clinical studies with the pre-clinical work dedicated to the discovery of new mechanisms involved in the development and progression of a large spectrum of diseases.
The journal will try to provide the entire medical com-munity with the perspective of the regional specifics of Central and Eastern European countries. The journal will primarily focus on publishing original research papers, but also other types of materials (such as review articles, case reports, state-of-the-art papers, comments to editor, etc) will be extremely welcomed.
Aims and scope


Journal of Interdisciplinary Medicine 2020;5(2):27-29
Cardiovascular Healthcare in 2020 – Alarming Realities in RomaniaRoxana Hodas
"George Emil Palade" University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania
Editorial
DOI: 10.2478/jim-2020-0014
The unprecedented progress recorded over the last decades in the field of pre-vention and management of cardiovascular disease (CVD) has led to a signifi-cant reduction of premature cardiovascular (CV) mortality across Europe.1 De-spite this progress, a new reality is emerging and generates serious concerns for public health policies. The burden of CVD presents alarming inequalities among different European regions, remaining disproportionately larger in low- and middle-income countries (LMICs) compared to high-income countries (HICs). Moreover, economic constraints at local level involve substantial disparities in availability of CV care and services, with dramatic effects on the healthcare ben-efits of CV patients in LMICs.2
The recently published map of “ESC Cardiovascular Realities 2019”, a map of ESC member countries based on monitoring CV health expenditure, infra-structure, and workforce across European countries, raised alarming signs for healthcare systems regarding the social and economic burden of CVD in differ-ent regions of Europe.3
From this point of view, Romania presents a concerning reality in all points of interest highlighted by the ESC’s call to action: insufficient control of risk factors and harmful behaviors, increased burden of CVD, and disparities in availability of CV care.
Extensively investigated, the important influence of potentially reversible well-established risk factors in the determination and progression of CVD pro-vides a strong rationale for giving a higher priority to risk reduction strategies. In HICs, the ongoing modern-day epidemics of obesity and type 2 diabetes, par-ticularly in younger adults, represent the most serious public health challenges which threaten to erode the health gains of recent years.4
In this European context, Romania seems to present inadequate strategies. Besides the negligible decrease in hypertension prevalence, poor strategies for the identification and effective treatment of people with established hyperten-sion contribute to the continuing high rates of myocardial infarction and CV death. Moreover, the daily intake of large quantities of alcohol, insufficient self-reported physical activity, and altered nutritional intake proved to be important
CORRESPONDENCE
Roxana HodasStr. Gheorghe Marinescu nr. 50 540136 Targu Mures, RomaniaTel: +40 372 653 100E-mail: [email protected]

28 Journal of Interdisciplinary Medicine 2020;5(2):27-29
contributors to the national burden of CV disease encoun-tered in this country.
Even if longitudinal data show a steady decline of CVD mortality across European regions, mortality burden con-tinues to show large geographical inequalities. In Romania, CVD accounts for more than 50% of all recorded deaths compared with below 30% in countries from Western Eu-rope. In terms of CVD morbidity statistics, inequalities in CVD burden are even greater among different European countries, in correlation with national economic status. A negative association between total health expenditure per capita and age-standardized CVD burden has been identi-fied, Romania reporting a greater than two-fold difference of disability-adjusted life years (DALYs) lost to CVD, with an average of about 9,000 DALYs per 100,000 people com-pared with 3,500 in HIC.5 This fact emphasizes that limited economic resources and health expenditure derive into in-equitable health outcomes.
The ESC map of CVD care delivery across European countries highlights the gaps and inequalities in the avail-ability of appropriate CV care as a consequence of the large differences in healthcare expenditure. According to recent ESC data, the Romanian healthcare system aligns with the group of countries defined by the World Health Organiza-tion as “lagging behind in infrastructure, human resource, and therapeutic procedures, mainly those with a low gross national product, typically the ESC member countries of Eastern Europe and Northern Africa”.6
In terms of human resources, Romania reported 63.0 cardiologists per million people, an appalling number com-pared with other ESC countries such as Greece or the Re-public of Georgia reporting >250 cardiologists per million people. This worrying situation remains the same for in-terventional cardiology statistics. The number of interven-tional cardiologists reported by Romania is 4.37 per million people, only ahead of countries such as Kyrgyzstan, Azer-baijan, or Kazakhstan, while the average number reported across ESC countries is 11.8 per million people, with an out-standing value of 30.96 per million in HICs such as Austria. The same sad reality was recorded for the density of inter-ventional centers: 0.7 per million people in Romania com-pared with 6.6 per million people in Germany. The situation is even worse in the field of interventional electrophysiol-ogy, since Romania, alongside Azerbaijan and Bosnia and Herzegovina, reported less than 1 electrophysiologist per million people, while other countries, such as Poland and Sweden, have an average number of 17 electrophysiologists per million people.3,7 The situation is identical regarding the number of centers of interventional electrophysiology, ablation procedures, and device implantations.8
As at this moment we face a more than 10-fold varia-tion in healthcare expenditures compared to Western European countries, lagging behind in human and capi-tal healthcare resources is readily apparent in the num-ber of performed procedures.9 With a mean number of 4,122 coronary angiograms performed across ESC mem-ber countries, Romania reported only 1,306 procedures, much behind other countries such as Germany which re-ported 9,392 procedures. In terms of percutaneous coro-nary interventions (PCIs), only 753 procedures per mil-lion people were reported in Romania, while the average number of PCIs in Europe was estimated at 2,211 per mil-lion, and Germany reported 3,975 procedures per million people. The same disparities are recorded for structural heart interventions, Romania alongside Egypt and Turkey being placed at the bottom of the list with 25 procedures per million people, while more than 150 procedures per million are performed annually in Switzerland and Ger-many. Even worse, Romania is on the last place in Europe in terms of both mitral valve percutaneous interventions with 0.2 procedures per million people and transcatheter aortic valve implantations with only 2.3 procedures per million people.2
These numbers provide a stark image of the gap in hu-man resources needed for the effective management of di-agnostic and therapeutic CV procedures in Romania. Un-doubtedly, much needs to be done in order to bridge the gaps in CVD healthcare delivery and to raise the quality of care in all European countries. Besides raising measures to control the well-established risk factors and harmful be-havior, it is of vital importance to raise awareness, high-light inequality, advice decision-makers, and sustain in-vestments for proper implementation of guidelines across all regions of Europe.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES
1. Vardas P, Maniadakis N, Bardinet I, Pinto F. The European Society of
Cardiology Atlas of Cardiology: rationale, objectives, and methods. Eur
Heart J Qual Care Clin Outcomes. 2016;2:6-15.
2. Timmis A, Townsend N, Gale C, et al. European Society of Cardiology:
Cardiovascular Statistics 2017. Eur Heart J. 2018;39:508-579.
3. Timmis, A, Townsend, N, Gale, et al. European Society of Cardiology:
Cardiovascular Disease Statistics 2019. Eur Heart J. 2019;1-74.
4. Capewell S, O’Flaherty M. Rapid mortality falls after risk-factors changes in
population. Lancet. 2011;378:752-3.
5. World Health Organisation. Global Health Observatory (GHO) data.
Available at: https://apps.who.int/gho/data/node.imr
6. Prüss-Üstün A, Mathers C, Corvalán C, Woodward A. Assessing the
environmental burden of disease at national and local levels: Introductions

29Journal of Interdisciplinary Medicine 2020;5(2):27-29
and Methods. WHO Environmental Burden of Disease Series 1. Geneva: World Health Organisation. 2003. Available at: http://www.who.int/quantifying_ehimpacts/publications/9241546204/en/index
7. Cenko E, Ricci B, Kedev S, et al. Reperfusion therapy for ST-elevation acute myocardial infarction in Eastern Europe: the ISACS-TC registry. Eur Heart J Qual Clin Outcomes. 2016;2:45-51.
8. Raatikainen MJ, Arnan DO, MErkely B, et al. Access to and clinical use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology Countries: 2016 Report from the European Heart Rhythm Association. Europace. 2016;18:Suppl 3:iii1-iii79.
9. Walker S, Asaria M, Manca A, et al. Long-term healthcare use and costs in the patients with stable coronary artery disease: a population-based cohort using linked health records (CALIBER). Eur Heart J Qual Care Clin Outcomes. 2016;2:125-140.

Journal of Interdisciplinary Medicine 2020;5(2):30-34
CORRESPONDENCE
Hammad AkramIndependent work, 1201 S. Trl. Waco, TX, USA Tel: +92 335 420 0717E-mail: [email protected]
ARTICLE HISTORY
Received: April 1, 2020Accepted: May 22, 2020
Disease Burden, Mechanism and Management of Obesity – Where Do We Stand?Irfan Sharif Shakoori1, Gohar Ashraf2, Fauzia Aslam3, Hammad Akram4
1 Family Medicine Consultant, Cort Piil Helsesenter, Bergen, Norway2 University of Pittsburgh Medical Center, Pittsburgh, PA, USA3 Baqai Medical University, Karachi, Pakistan4 Independent researcher, Waco, TX, USA
rEViEW ALTERNATIVE MEDICINE // PUBLIC HEALTH
DOI: 10.2478/jim-2020-0008
ABSTRACT
The role of increased body mass index in general morbidity and mortality is well documented. This global public health issue continues to represent a major burden and threat to health sys-tems and the population’s wellbeing. Global statistics show that the prevalence of obesity has increased about three times since the mid-1970s, and an upward trend is still observed, not only in developed but also in developing countries. We used several databases, including PubMed, ProQuest, and Google Scholar, to perform a literature search and review on obesity. Keywords such as “obesity”, “overweight”, and “BMI” were used in combination with multiple keywords such as “mechanism”, “factors”, “socio-economic”, “environmental”, “social determinants”, “man-agement”, “treatment”, “non-traditional treatment”, “alternative therapies”, “non-pharmaceutical treatment” etc. and related phrases. According to the literature, the management of obesity is difficult due to the complex nature of this problem in terms of its course, complications, risks, and etiological factors. The role of alternative therapies in obesity management is still unclear, and further research is needed in this area. Recently introduced weight-loss and -management devices can also help in losing excess bodyweight. The present article summarizes relevant information related to obesity, collected from different regions of the world, and discusses di-verse interventional approaches to treat obesity.
Keywords: obesity, overweight, BMI, behavioral factors
Irfan Sharif Shakoori • Cort Piil-smauet 7, 5005 Bergen, Norway. Tel: +47 55 23 60 10, E-mail: [email protected]
Gohar Ashraf • 200 Meyran Ave # 318, Pittsburgh, PA 15213, USA. Tel: +1 412 647 8586, E-mail: [email protected]
Fauzia Aslam • Baqai Medical University, Karachi, Pakistan. E-mail: [email protected]
iNtroduCtioN
The impact of increased body weight on health outcomes and the associated morbidity and mortality are well documented.1 Obesity (OB) is a complex com-munity health problem connected to several physical and non-physical factors.2 The body mass index (BMI) is a parameter that is widely used to classify over-weight (OW) and OB categories by taking weight and height into account.3 His-torical trends and patterns demonstrate increasing OW and OB rates, especially in developed countries.3 It is also evident that developing countries are also

31Journal of Interdisciplinary Medicine 2020;5(2):30-34
affected by this public health issue and have been experi-encing an upward trend of increased body weight and re-lated health conditions in recent decades.3 Another critical health issue of concern is childhood and adolescent OW and OB, with long-term psychological and physical con-sequences.2,3 Many children with OB grow up to become obese adults and continue to suffer from the detrimental effects of OB.3 In the present paper, we explore geographi-cally unique characteristics of OW and OB while sharing relevant data and challenges of this major public health issue. Furthermore, while presenting medical and surgi-cal remedies of OB, we examine non-pharmaceutical and alternative approaches that can help in the management of this morbid condition. The present article summarizes relevant information from different regions of the world and discusses diverse interventional approaches to treat obesity, useful for both professionals and society.
matErialS aNd mEtHodS
A careful examination of existing data published in se-lected regions of the world was carried out. We used sev-eral databases, including PubMed, ProQuest, and Google Scholar, to perform a literature search and review. Key-words such as “obesity”, “overweight”, and “BMI” were used in combination with multiple keywords such as “mechanism”, “factors”, “socio-economic”, “environmen-tal”, “social determinants”, “management”, “treatment”, “non-traditional treatment”, “alternative therapies”, “non-pharmaceutical treatment” etc. and related phrases. Ab-stracts were reviewed to assess the appropriateness of ar-
ticles for the topic of our literature review. We preferred articles published in the past 15 years; however, older articles were also considered if insufficient research was available on a given subtopic. For certain parts of the pa-per, we discussed characteristics of issues from selected geographical regions considering that the authors had current, recent, or past affiliations and experiences within these areas.
mECHaNiSm, prEdiSpoSiNG faCtorS,
aNd maGNitudE of tHE problEm
According to global statistics, the prevalence of OB has in-creased almost three times since the mid-70s.3 According to the World Health Organization (WHO), in 2016, around 52% of adults and 18% of children aged 5–19 years were overweight and obese.3 The associated mortality was high-er than the one of individuals who died because of prob-lems associated with lower than normal body weight (un-derweight).3 Compared to the global prevalence of 13% in 2016, 39.8% of adults were suffering from OB in the US in 2015–2016.4 In the last decades, the prevalence of OB presented increasing trends in all regions of the world, Eu-rope, America, and Eastern Mediterranean regions show-ing the highest prevalence and exhibiting an upward trend between 2000 and 2016 (Figure 1).5
The mechanisms and underlying phenomena behind OW and OB have been explored before.1–4 There is, how-ever, variation in causes found in different cultures and re-gions of the world. For example, in the US, Hispanic and African-American individuals have the highest prevalence
FIGURE 1. Prevalence of obesity among adults, BMI ≥ 30, age-standardized. Estimates by WHO region
(2000-2016). Source: WHO, Global Health Observatory data repository5

32 Journal of Interdisciplinary Medicine 2020;5(2):30-34
of OB.4 Furthermore, the prevalence of OB is lower among individuals with higher educational and/or socioeconomic status.4 Among men, however, the lowest income groups are also less likely to have OB.4
Studies show that the prevalence of OW and OB has also increased among children and adults living in the Middle East.6,7 In the Persian Gulf region, this increase can be at-tributed to major changes in the population’s lifestyle over the past few decades.6–8 In Qatar for example, the preva-lence of OB has increased due to the recent industrial-ization and socioeconomic progress along with cultural factors, transition to a sedentary lifestyle, popularity or acceptance of fast food as a norm, and environmental fac-tors such as extremely hot weather most of the year.7 In a 2012 survey, over 70% of Qatari nationals were found to be overweight and obese, with 41% having a BMI in the obese category.7 The survey also showed that around 91% of adults were not consuming enough fruits and vegeta-bles, and 71% were not fulfilling recommended vigorous activity requirements as well.7 Furthermore, related health problems such as high blood pressure (~33%), high blood glucose or diabetes (16.7%), and hypercholesterolemia (~22%) were also alarming.7 Further analysis of this data showed that nutritional factors were impacting OB rates among young adults versus physical activity among older adults. Also, generalized and abdominal types of OB were significantly associated with diabetes among Qatari citi-zens.7,9 OW/OB is linked to the consumption of energy-rich food items, and the Qatari population is consuming higher-than-recommended amounts of energy-dense food items.3,10,11 OW/OB prevalence is also documented to be high among children and adolescents in Qatar.12–14
Population dynamics, especially immigration, can im-pact the health of migrant populations by adopting be-haviors and experiencing opportunities that were not common in their country of origin. Recent immigrants to communities with high prevalence of OB can lead to the so-called healthy migrant effect. However, after resid-ing in new countries for a longer duration of time, immi-grants also tend to experience unhealthy weight gain.15 In Norway, OW/OB has been an emerging issue among im-migrant populations. A study carried out in 2010 with a sample comprising of 208 Somali immigrants showed that both generalized and abdominal OB had a direct positive association with the length of residence in Norway. By gender, the prevalence of OB was higher among Somali (immigrant) female respondents vs. males, similarly to the Qatari population.7,16
The challenges in OB prevention and reversal can be related to multiple factors. A 2013 article reveals that the
study participants were not able to follow healthy diet plans due to stress, depression, cravings, and social situa-tions where they could not avoid certain foods.17 Respon-dents felt challenged by the cost, time, and motivation associated with maintaining healthy dietary habits.17 Ad-herence to physical activity was found to be difficult due to various reasons such as lack of time and motivation, or not having a partner to perform exercise with.17 Cultural norms and environmental factors can also impact the ad-herence to health programs; for example, a study from the Arab Gulf region showed that the main issues in sustaining healthy eating were due to unwillingness, family norms, and social gathering, where it was difficult to avoid certain food items.18 Moreover, lack of time, underlying health conditions, and extreme weather were found to repre-sent the main challenges in performing regular exercise.18 Other factors include easy access to low-cost high-calorie food items such as fast food, limited access to healthier food items, increased screen time especially among youth, sedentary work environment, lack of information, skills, and interest in certain exercise/sports, not having support (family- or costs-related) to be physically active etc.19–21
maNaGEmENt
OW and OB can be prevented or reduced by changing lifestyle, e.g. performing physical activities and modify-ing the diet by including more fruits, vegetables, or other aliments with high fiber content, and by avoiding high en-ergy foods such as sugar and fats etc.3 Dietary modification and caloric monitoring may help in maintaining a healthy body weight. Incorporating fruits, vegetables, and whole grains in the diet along with physical activity can help in weight loss if practiced as a routine behavior. The impact of weight-loss diets, especially if followed for a shorter du-ration of time, is variable. Exercise can certainly help in weight loss and maintenance of a healthy weight if prac-ticed continuously, and can play an important role in the improvement of both physical and mental wellbeing.3,7,22 The aim is to reduce energy intake and increase energy ex-penditure. In certain situations, OW and OB can be man-aged by using pharmaceutical agents. These medicines are usually recommended if physical activity and/or dietary measures are not efficient, and the BMI is higher than 30 or 27 with underlying medical conditions.23,24 Table 1 lists the types of approaches used in the management of OB based on our literature review.22–28
The role of alternative and herbal therapies in the re-duction or prevention of OB requires further scientific ex-ploration. Triphala, which is a combination of three plant

33Journal of Interdisciplinary Medicine 2020;5(2):30-34
species (Indian gooseberry, Terminalia bellirica, and Ter-minalia chebula), has shown some evidence in reducing body fat.29,30 In addition to decreasing body fat percent-age, body weight, and energy intake in mice, it also helped lower blood cholesterol and sugar levels.29,30 In a 12-week randomized double-blinded placebo-controlled trial with 62 participants, the treatment group experienced a signifi-cant decline in mean weight and waist circumference.31
Nigella sativa (black cumin) was found to have mixed effects on OB and metabolic syndrome. Findings from 11 studies showed that Nigella sativa had some positive role in reducing body weight, BMI, and waist circumference.32 Furthermore, clinical trials have shown that it also helped in reducing blood sugar, lipids, and body weight among study participants; however, more research is needed to understand this relationship.33 Garcinia cambogia inhibits the citrate lyase enzyme and can help in reducing appe-tite.34 Camellia sinensis may have some role in appetite sup-pression, enhanced energy use, and decrease absorption of nutrients.34 Chromium picolinate is a quite common supplement known to help in glucose metabolism and food behavior, leading to possible weight loss; however, its long-term impacts on OB prevention and remission are unclear.34,35
Allison et al. reviewed the impact of 18 different alterna-tive or non-traditional therapies on body weight and found that there is not enough evidence that these treatments are effective.35 There is some reasonable evidence from well-designed studies suggesting that compounds containing ephedrine and caffeine may have some benefits.35 Caffeine has been found to be beneficial in weight maintenance and appetite suppression in another study.36 The role of alter-native therapies in OB management is still unclear and fur-ther research is needed in this area.
Recently introduced weight-loss and weight-manage-ment devices can be used for patients in whom lifestyle modification approaches are not working.37 Some exam-ples of these devices are: gastric bands, gastric emptying system, and gastric balloons. Preliminary data show that
there is reasonable benefit seen among patients who have used these devices.37 Body countering through noninva-sive methods, such as high intensity focused ultrasound, low-level laser therapy, cryolipolysis, or radiofrequency, and invasive approaches, such as liposuction, could also be beneficial but costly alternatives.34
Summary aNd CoNCluSioNS
Increased body weight and waist circumference are as-sociated with several diseases and health conditions. OB has become a significant public health concern that can lead to diverse types of chronic diseases. High morbidity and mortality associated with body weight-related health issues exert tremendous economic burden on health sys-tems and communities. The complex nature of this is-sue can be managed only by applying multi-dimensional well-researched strategies as provision of complex care needs can be challenging, especially in the presence of ad-ditional co-morbidities.38 Programs targeted at youth can certainly help as the behavioral modification is easier if started earlier; hence, school-based programs can play an essential role in the long-term management of this issue. Incorporating recommended levels of physical activity and opting for healthier food choices in the daily routine can help reduce the incidence of chronic diseases such as heart disease, stroke, diabetes, and some cancers through reducing body weight.7,39–41 Since OB is associated with other chronic health problems, it may also aggravate the prognosis of patients who are suffering from the novel CO-VID-19 infection. The mechanism of this is not yet clear, as the COVID-19 infection is relatively new and has not been sufficiently studied yet; however, OB can exert increased burden on breathing mechanics and could have a negative impact on disease course.42,43
CoNfliCt of iNtErESt
Nothing to declare.
TABLE 1. Different types of management approaches for obesity
Non-pharmaceutical Pharmaceutical (mechanism) Surgical
Physical activity Orlistat (inhibits gastric lipases) Sleeve gastrectomy
Diet Sibutramine (satiety, metabolic) Laparoscopic adjustable gastric banding (LAGB)
Transcranial direct current stimulation Diethylpropion (appetite suppressant) Roux-en-Y gastric bypass (RYGB)
Cognitive behavioral interventions Phentermine (appetite suppressant) Single anastomosis gastric bypass (SAGB)
Liraglutide (satiety, (GLP-1 receptor agonist) Biliopancreatic diversion/duodenal switch (BPD/DS)
Lorcaserin (satiety)

34 Journal of Interdisciplinary Medicine 2020;5(2):30-34
rEfErENCES1. CDC. The Health Effects of Overweight and Obesity. Available at: https://
www.cdc.gov/healthyweight/effects/index.html2. Akram H, Ashraf G, Ijaz MA. The Impacts of Complex Social, Environmental,
and Behavioral Factors on Obesity. International Journal of Basic Science in Medicine. 2018;3:94-98.
3. WHO. Obesity and Overweight. Available at: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight
4. CDC. Adult Obesity Facts. Available at: https://www.cdc.gov/obesity/data/adult.html
5. WHO Global Health Observatory data repository. Prevalence of obesity among adults, BMI ≥ 30, age-standardized. Estimates by WHO region. Available at: http://apps.who.int/gho/data/view.main.REGION2480A
6. Badran M, Laher I. Obesity in Arabic-speaking countries. J Obes. 2011;2011:686430.
7. Al-Thani MH, Al-Thani AA, Al-Chetachi WF, et al. Dietary and nutritional factors influencing obesity in Qatari adults and the modifying effect of physical activity. Journal of Obesity and Weight-loss Medication. 2015;1:007.
8. Klautzer L, Becker J, Mattke S. The curse of wealth – Middle Eastern countries need to address the rapidly rising burden of diabetes. Int J Health Policy Manag. 2014;2:109.
9. Al-Thani M, Al-Thani AA, Al-Chetachi W, et al. Situation of diabetes and related factors among Qatari adults: findings from a community-based survey. JMIR Diabetes. 2017;2:e7.
10. Al-Thani M, Al-Thani AA, Al-Mahdi N, et al. An overview of food patterns and diet quality in Qatar: findings from the National Household Income Expenditure Survey. Cureus. 2017;9:e1249.
11. Al-Thani M, Al-Thani A, Al-Chetachi W, Akram H. Obesity and related factors among children and adolescents in Qatar. Int J Basic Sci Med. 2017;2:161-165.
12. Kerkadi A, Sadig AH, Bawadi H, et al. The relationship between lifestyle factors and obesity indices among adolescents in Qatar. Int J Environ Res Public Health. 2019;16:4428.
13. Kerkadi A, Hassan AS, Al Chetachi W, et al. Prevalence of general and abdominal obesity among adolescents attending independent schools in Qatar. Nutrition & Food Science. 2019;49:687-699.
14. Al-Thani M, Al-Thani A, Alyafei S, et al. The prevalence and characteristics of overweight and obesity among students in Qatar. Public Health. 2018;160:143-149.
15. Murphy M, Robertson W, Oyebode O. Obesity in international migrant populations. Curr Obes Rep. 2017;6:314-323.
16. Gele AA, Mbalilaki AJ. Overweight and obesity among African immigrants in Oslo. BMC Research Notes. 2013;6:119.
17. Sharifi N, Mahdavi R, Ebrahimi-Mameghani M. Perceived barriers to weight loss programs for overweight or obese women. Health Promot Perspect. 2013;3:11-22.
18. Serour M, Alqhenaei H, Al-Saqabi S, Mustafa AR, Ben-Nakhi A. Cultural factors and patients’ adherence to lifestyle measures. British Journal of General Practice. 2007;57:291-295.
19. Middleton KR, Anton SD, Perri MG. Long-term adherence to health behavior change. American Journal of Lifestyle Medicine. 2013;7:395-404.
20. Al-Thani M, Al-Thani A, Alyafei S, et al. Prevalence of physical activity and sedentary-related behaviors among adolescents: data from the Qatar National School Survey. Public Health. 2018;160:150-155.
21. Andajani-Sutjahjo S, Ball K, Warren N, Inglis V, Crawford D. Perceived personal, social and environmental barriers to weight maintenance among young women: A community survey. Int J Behav Nutr Phys Act. 2004;1:15.
22. Higuera-Hernández MF, Reyes-Cuapio E, Gutiérrez-Mendoza M, et al. Fighting obesity: Non-pharmacological interventions. Clinical Nutrition ESPEN. 2018;25:50-55.
23. Mayer MA, Hocht C, Puyó A, Taira CA. Recent advances in obesity pharmacotherapy. Current Clinical Pharmacology. 2009;4:53-61.
24. Mayo Clinic. Healthy Lifestyle, Weight loss. Available at: https://www.mayoclinic.org/healthy-lifestyle/weight-loss/in-depth/weight-loss-drugs/art-20044832
25. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA. 2014;311:74-86.
26. Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100:342-362.
27. O’Brien P. Surgical Treatment of Obesity. In: Feingold KR, Anawalt B, Boyce A, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000.
28. Valezi AC, Herbella FA. Historical Notes on the Surgical Treatment of Morbid Obesity. In: Foregut Surgery. Cham: Springer, 2020; p. 219-226.
29. Peterson CT, Denniston K, Chopra D. Therapeutic uses of triphala in ayurvedic medicine. J Altern Complement Med. 2017;23:607-614.
30. Mohammad K, Larijani B. A systematic review of the antioxidant, anti-diabetic, and anti-obesity effects and safety of triphala herbal formulation. J Med Plants Res. 2013;7:831-844.
31. Kamali SH, Khalaj AR, Hasani-Ranjbar S, et al. Efficacy of ‘Itrifal Saghir’, a combination of three medicinal plants in the treatment of obesity; A randomized controlled trial. DARU. 2012;20:33.
32. Namazi N, Larijani B, Ayati MH, Abdollahi M. The effects of Nigella sativa L. on obesity: A systematic review and meta-analysis. J Ethnopharmacol. 2018;219:173-181.
33. Tavakkoli A, Mahdian V, Razavi BM, Hosseinzadeh H. Review on clinical trials of black seed (Nigella sativa) and its active constituent, thymoquinone. J Pharmacopuncture. 2017;20:179.
34. Esteghamati A, Mazaheri T, Rad MV, Noshad S. Complementary and alternative medicine for the treatment of obesity: a critical review. Int J Endocrinol Metab. 2015;13: e19678.
35. Allison DB, Fontaine KR, Heshka S, Mentore JL, Heymsfield SB. Alternative treatments for weight loss: a critical review. Crit Rev Food Sci Nutr. 2001;41:1-28.
36. Icken D, Feller S, Engeli S, et al. Caffeine intake is related to successful weight loss maintenance. Eur J Clin Nutr. 2016;70:532-534.
37. U.S Food & Drug Administration. Medical Devices for Weight Loss and Weight Management: What to Know. Available at: https://www.fda.gov/consumers/consumer-updates/medical-devices-weight-loss-and-weight-management-what-know
38. Gordon K, Steele Gray C, Dainty KN, DeLacy J, Ware P, Seto E. Exploring an Innovative Care Model and Telemonitoring for the Management of Patients With Complex Chronic Needs: Qualitative Description Study. JMIR Nursing. 2020;3:e15691.
39. Akram H, Aslam F. An Overview of Disease Burden, Mechanism, Traditional and Non-traditional Management of Type 2 Diabetes. Journal of Interdisciplinary Medicine. 2019;4:124-131.
40. World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Available at: https://apps.who.int/iris/handle/10665/44203
41. Shakoori IS, Aslam F, Ashraf G, Akram H. Understanding chronic disease risk factors and multimorbidity. Int J Community Med Public Health. 2020;7:1990-1993.
42. CDC. Coronavirus Disease 2019 (COVID-19).Groups at Higher Risk for Severe Illness. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/groups-at-higher-risk.html
43. WebMD. Obesity New Risk Factor for Young COVID Patients. Available at: https://www.webmd.com/lung/news/20200429/obesity-new-risk-factors-for-young-covid-patients

Journal of Interdisciplinary Medicine 2020;5(2):35-42
CORRESPONDENCE
Shehab Al-AnsariDepartment of Hospital MedicineM75. 9500 Euclid Avenue Cleveland, OH 44195, USATel: +1 216 218 5795E-mail: [email protected]
ARTICLE HISTORY
Received: May 15, 2020Accepted: May 24, 2020
Effects of Pirfenidone on Echocardiographic Parameters of Left Ventricular Structure and Function in Patients with Idiopathic Pulmonary FibrosisShehab Al-Ansari1, Allen Borowski2, Ali Fuad3, Omar Alawadhi4, Haris Riaz2, Vikram Sharma1,
Nauman Khan1, Brian D. Southern5, W.H. Wilson Tang2
1 Department of Hospital Medicine, Medicine Institute, Cleveland Clinic, Cleveland, OH, USA 2 Department of Cardiovascular Medicine, Heart, Vascular, and Thoracic Institute, Cleveland Clinic, Cleveland, OH, USA 3 Royal College of Surgeons in Ireland, Dublin, Ireland 4 Department of Surgery, Tawam Hospital, Abu Dhabi, United Arab Emirates 5 Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA
oriGiNal rESEarCH CARDIOLOGY // SURGERY
DOI: 10.2478/jim-2020-0009
ABSTRACT
Aim: Pirfenidone is a novel anti-fibrotic agent utilized in the treatment of idiopathic pulmonary fibrosis (IPF). It has been implicated in mitigating myocardial fibrosis and left ventricular (LV) systolic and diastolic dysfunction in animal models. However, its impact on LV mechanics in humans remains unknown. The aim of this study was to retrospectively evaluate the effects of pirfenidone on echocardiographic parameters of LV function and structure in patients with IPF. Methods: A total of 124 patients with IPF were included in this study: 64 patients treated with pirfenidone (treatment group) and 60 patients not taking pirfenidone (control group), who had serial pretreatment/baseline and posttreatment/follow-up echocardiograms done within a time frame of four years. Changes in the means of parameters of LV function (systolic, diastolic, and global longitudinal strain) and LV structure (mass and indexed volume indices) were compared between the treatment and control groups. This was followed by a subgroup analysis that included only 88 patients (47 treated, 41 controls) with echocardiographic evidence of myo-cardial dysfunction at baseline (defined as an ejection fraction of ≤45, or diastolic dysfunction stage 1 or more) in addition to a known clinical diagnosis of congestive heart failure. To account for potential confounders, a secondary adjusted analysis by way of 1:1 propensity score match-ing (PSM) was carried out. This yielded a sample consisting of 62 patients with 56 patients in the subgroup cohort. Results: Patients in the treatment group were significantly younger (69.4 vs. 77 years, p<0.001) and had relatively lower forced vital capacity (69.9% vs. 80.6%, p = 0.005) in comparison to the control group. However, after PSM, the age demographics were comparable between both groups (72.18 vs. 72.15, p = 0.9). In the primary unadjusted analysis, there was no statistically significant change in any of the mean parameters of LV function and structure after pirfenidone administration when compared to the control group. Further-more, no significant differences were noted in the subgroup cohort. Such findings were re-demonstrated after a secondary analysis with PSM. Conclusion: From an echocardiographic perspective, pirfenidone had no significant effects on LV structure and function in patients with IPF, even in patients with more overt cardiac dysfunction.
Keywords: pirfenidone, idiopathic pulmonary fibrosis, heart failure, myocardial dysfunction
Allen Borowski • Cleveland Clinic, 9500 Euclid Avenue, Cleveland, Ohio 44195, USA. Tel: +1 216 444 2200
Ali Fuad • 123 St Stephens Green, Dublin, Ireland. Tel: +353 1 402 2100
Omar Alawadhi • Tawam Hospital, Abu Dhabi, United Arab Emirates. Tel: +971 3 767 7444
Haris Riaz • Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA. Tel: +1 216 444 2200
Vikram Sharma • Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA. Tel: +1 216 444 2200
Nauman Khan • Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA. Tel: +1 216 444 2200
Brian D. Southern • Cleveland Clinic, 9500 Euclid Avenue OH 44195, USA. Tel: +1 216 444 2200
W.H. Wilson Tang • Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA. Tel: +1 216 444 2200

36 Journal of Interdisciplinary Medicine 2020;5(2):35-42
iNtroduCtioN
Pirfenidone, a novel anti-fibrotic agent, has been shown to reduce the rate of pulmonary function decline and im-prove disease-free progression in patients with idiopathic pulmonary fibrosis (IPF).1 Although its precise mecha-nism of action remains to be deciphered, pirfenidone in-hibits transforming growth factor-beta (TGF-β)-mediated fibroblast activation and collagen synthesis,2 one of the key pathways in the pathogenesis of myocardial fibrosis.3 Myocardial fibrosis is known to occur in both subtypes of heart failure, being more pronounced in heart failure with reduced (HFrEF) rather than preserved ejection fraction (HFpEF).4 However, in patients with HFpEF, the degree of myocardial fibrosis is significantly correlated to the se-verity of diastolic dysfunction.4
In pre-clinical studies, pirfenidone was found to miti-gate myocardial fibrosis and attenuate left ventricular (LV) remodeling and diastolic and systolic dysfunction in ani-mal models,5–9 suggesting the possibility of a mechanistic overlap between cardiac and pulmonary fibrosis. This may prove beneficial in the treatment of congestive heart fail-ure (CHF), and in particular HFpEF, where disease-spe-cific therapy is lacking and thus carries a poor prognosis.10
To date, the effects of pirfenidone on LV mechanics in humans remains unknown. We therefore sought to inves-tigate this further by retrospectively examining the effects of pirfenidone on echocardiographic parameters of LV structure and function in patients with IPF. This was fol-lowed by a subgroup analysis to only include patients with more overt cardiac dysfunction. We hypothesize that pa-tients taking pirfenidone will have more favorable changes in markers of LV function and structure compared to the control group.
Such a hypothesis-generating study from an already ex-isting patient cohort could elucidate the implications of pirfenidone on human myocardial mechanics and poten-tially lead to newer indications.
matErialS aNd mEtHodS
Patient selection
In this single-center retrospective study, 900 consecutive patients with an International Classification of Diseases (ICD)-10 diagnosis code of IPF were initially identified between June 1, 2014 and June 1, 2018. Electronic medi-cal records were then reviewed for clinical and echocar-diographic data. Patients were included if they had a confirmed radiological or histological diagnosis of IPF
in addition to serial baseline and follow-up echocardio-grams, both done after the diagnosis was established. In patients who were on pirfenidone (treatment group) we defined baseline/pretreatment echocardiograms as those done within two years before treatment and follow-up/posttreatment echocardiograms as those done within two years after treatment. Only patients taking pirfenidone continuously throughout the defined time interval were included. The control group consisted of patients with IPF not taking pirfenidone or any other pulmonary disease modifying medications and who had two serial echocar-diograms done within four years of each other. Patients with mitral stenosis or mitral valve surgery, severe mitral regurgitation, severe aortic stenosis or regurgitation, and atrial fibrillation at the time of echocardiographic analysis were excluded. Of note, patients who had a history of atrial fibrillation were only included if they were in normal sinus rhythm during echocardiographic analysis, to allow for de-tailed diastolic assessment.
Sequentially, a total of 124 patients with IPF were in-cluded in the primary analysis, 64 treated with pirfenidone and 60 controls not on pirfenidone. This was followed by a subgroup analysis that included only 88 patients (47 treated, 41 controls) with echocardiographic evidence of myocardial dysfunction at baseline (defined as either EF of ≤45% or grade 1 or more diastolic dysfunction) in ad-dition to a known clinical diagnosis of CHF. In this study, the clinical diagnosis of CHF was established if a patient fulfilled the well-validated Framingham criteria.11 Clinical data pertaining to the diagnosis was obtained from elec-tronic medical records of patient encounters with inter-nists or cardiologists within our institution.
Institutional Review Board approval was granted for retrospective collection of data and informed consent was waived. This study complied with the Declaration of Hel-sinki.
Statistical considerations
Statistical analysis was performed using the Statistical Package for the Social Sciences software (SPSS v26 for Windows, SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation if normally distributed, and as mean (median, interquartile range) if non-normally distributed, as determined by the Shapiro-Wilk W test. Independent t test score and Mann-Whitney U test were utilized to assess for any statistical significance for normal and non-normally distributed vari-ables, respectively. Categorical variables were expressed as a percentage, and the Chi-squared test was used to ascer-

37Journal of Interdisciplinary Medicine 2020;5(2):35-42
tain any statistical significance. A two-tailed p value of less than 0.05 was considered significant. In the primary unad-justed analysis, changes in the means of echocardiographic parameters of LV structure and function were compared between the treatment and control groups. This was fol-lowed by a subgroup analysis to only include patients with more overt echocardiographic evidence of myocardial
dysfunction at baseline in addition to an established clini-cal diagnosis of heart failure.
To account for confounding variables that can poten-tially impact changes in parameters of LV function and structure, an adjusted secondary analysis was carried out by way of 1:1 propensity score matching (PSM). To es-timate the propensity score, a set of variables (including
FIGURE 1. Patient selection process and statistical methodology
900 patients with idiopathic pulmonary fibrosis
presenting between 2014 and 2018
124 patients with baseline and follow-up
echocardiograms
Treatment group: 31 patients in total.
Subgroup cohort: 28 patients
Control group: 60 patients not on
pirfenidone in total, 40 patients
included in the subgroup cohort
Treatment group: 64 patients taking
pirfenidone in total, 47 patients
included in the subgroup cohort**.
Treatment group: 31 patients in total.
Subgroup cohort: 28 patients
Inclusion criteria*:
• Patients with a confirmed diagnosis of IPF
• Serial baseline and follow-up echocardiograms done after the diagnosis of IPF
• Treatment group: pretreatment echocardiogram done within 2 years before pirfenidone administration. Posttreatment echocardiogram done within 2 years after pirfenidone administration (maximum time interval of 4 years).
• Control group (patients not taking pirfenidone or any other pulmonary disease-modifying medications): baseline and follow-up echocardiograms done within 4 years of each other.
Exclusion criteria*:
• Mitral stenosis, mitral valve surgery, severe mitral regurgitation, severe aortic stenosis or regurgitation and atrial fibrillation at the time of assessment.
Subgroup cohort**:
Includes patients with baseline echocardiographic myocardial dysfunction in addition to a clinical diagnosis of congestive heart failure.
Inclusion and exclusion criteria*
Primary unadjusted analysis
Propensity score matching

38 Journal of Interdisciplinary Medicine 2020;5(2):35-42
age, gender, body mass index, history of coronary artery disease, chronic kidney disease, diabetes, hypertension, atrial fibrillation, use of beta blockers, and use of renin-angiotensin-aldosterone inhibitors) that could poten-tially impact the degree of myocardial fibrosis and thus LV function and structure were selected. Such variables were then included in a multi-variable logistic regres-sion model which produced a propensity score for each of the 124 patients included in the primary analysis. Tak-ing the estimated propensity score of each patient, a 1:1 match analysis without replacement was carried out using the nearest-neighbor matching technique, with a match tolerance of 0.2 of the pooled standard deviation of the logit of the propensity score, as previously described in the literature.12 This yielded a sample consisting of 62 patients with IPF in total (31 treated, 31 controls), all of which were included in the secondary adjusted analysis. Finally, the process was repeated once more to only in-clude the matched subgroup cohort, which resulted in 56 patients with relatively more severe cardiac dysfunction (28 treated, 28 controls). The C-statistic of the propensity score models was approximately 0.8, which is considered an adequate model fit.12
Figure 1 summarizes the patient selection process ac-cording to the aforementioned inclusion criteria, exclu-sion criteria, and statistical methodology.
Echocardiographic analysis
Comprehensive echocardiographic data extracted from a total of 248 echocardiograms (two echocardiograms per patient) were reviewed for parameters of LV structure, systolic function and diastolic function. Missing data, in-cluding detailed diastology analysis and global longitudi-nal strain, were obtained by directly performing measure-ments on stored images offline. This was performed by an experienced research sonographer in a blinded man-ner, using commercially available software from Siemens Healthcare (Syngo Dynamics 9.0). LV ejection fraction (EF) and cardiac volumes (indexed LV end-systolic vol-ume, LV end-diastolic volume, and left atrial volume) were calculated using the modified Simpson bi-plane method in the apical 2- and 4-chamber views. In the parasternal short axis view, LV mass was estimated utilizing the Devereux formula after measuring the LV end-diastolic dimension, interventricular septal thickness, and posterior wall thick-
TABLE 1. Baseline demographic and clinical characteristics
Treatment group (n = 64)
Control group (n = 60)
p value
Age (years) 69.4 ± 7 77 ± 8.8 <0.001
Male % (n) 71.9 (46)** 65 (39) 0.4
Body surface area (m2) 2 ± 0.2 1.9 ± 0.3 0.1
Body mass index (kg/m2) 30.1 ± 4.8 28.2 ± 6 0.1
Systolic blood pressure (mmHg) 122.6 ± 14.9 127.9 ± 16.5 0.2
Diastolic blood pressure (mmHg) 73 ± 7.3 76 ± 6.2 0.2
Cardiac risk factors and co-morbidities % (n)
Hypertension 68.7 (44) 56.6 (34) 0.2
Diabetes 21.9 (14) 15 (9) 0.5
Hyperlipidemia 67.2 (43) 51.2 (31) 0.08
Chronic kidney disease 31.3 (20) 45 (27) 0.07
Atrial fibrillation 17.2 (11) 30 (18) 0.09
Coronary artery disease 42.2 (27) 41.7 (25) 0.6
Cardiac medications % (n)
Beta-blockers 43.8 (26) 35 (21) 0.6
Diuretics 34.3 (22) 33.3 (20) 0.9
Renin-angiotensin-aldosterone inhibitors 39.1 (25) 35 (21) 0.5
Pulmonary function testing
Baseline predicted forced vital capacity (%) 69.9 ± 18.2 80.6 ± 42.8 0.005
Laboratory testing
Serum creatinine (mg/dL) 1.1 ± 0.4 1.2 ± 0.7 0.2
Time interval between baseline and follow-up echocardiogram (years)
1.7 ± 1.3 1.5 ± 1.1 0.2
n, number of patients; **numbers within the brackets represent absolute figures

39Journal of Interdisciplinary Medicine 2020;5(2):35-42
ness. In this study, several parameters of diastolic function measured in the apical 4-chamber view were obtained by placing the sample volume at the mitral annulus as well as the tip of the mitral valve leaflets; peak mitral inflow ve-locities during early and late atrial filling (E and A waves), mitral valve deceleration time and peak early velocity (e´) measured at both septal and lateral locations. Subsequent-ly, pulmonary vein systolic wave and diastolic wave were measured by placing the sample volume at the right upper or lower pulmonary vein, and the systolic to diastolic wave ratio was then calculated.
The severity of diastolic dysfunction was graded in ac-cordance to the American Society of Echocardiography/European Association of Cardiovascular Imaging.13 Global longitudinal strain was assessed using velocity vector im-aging; strain contours were drawn from the apical 4-cham-
ber, 2-chamber, and the apical long axis view in those with adequate frame-rate capture, respectively. Endocardial borders were automatically generated by the software and were manually adjusted as needed.
rESultS
As illustrated in Table 1, patients in the treatment group were significantly younger (69.4 vs. 77 years, p <0.001) and had relatively lower forced vital capacity (69.9% vs. 80.6%, p = 0.005) in comparison to the control group. Other baseline clinical and echocardiographic variables were statistically comparable between the two groups (p >0.05). Moreover, after PSM, the age demographics of both groups were comparable as well (72.18 vs. 72.15 years, p = 0.9).
TABLE 2. Baseline echocardiographic characteristics
Baseline echocardiographic parameter Treatment group (n = 64)
Control group (n = 60)
p value
LV structure
Indexed LV mass (gm2) 91.6 ± 31.2 94.1 ± 30.1 0.7
LV diastolic internal dimension (cm) 4.5 ± 0.7 4.4 ± 0.8 0.6
LV systolic internal dimension (cm) 3.3 ± 1.9 3.12 ± 0.7 0.6
Intraventricular septal wall thickness (cm) 1.12 ± 0.1 1.19 ± 0.2 0.2
Posterior wall thickness (cm) 1.03 ± 0.1 1.11 ± 0.2 0.1
Indexed LV end-systolic volume (mL/m2) 17.8 ± 9.5 20.4 ± 9.6 0.2
Indexed LV end-diastolic volume (mL/m2) 44.5 ± 20 45.6 ± 12.9 0.8
LV systolic function
EF (%) 60.1 ± 6.2 60.2 ± 10.4 0.7
Patients with EF ≤45% (n) 9.4% (6) 15% (9) 0.5
LV diastolic function
Indexed left atrial volume (mL/m2) 27.3 ± 10 31.2 ± 13.3 0.1
Mitral valve E wave 67 (73, 37.5) 76 (65, 19) 0.1
Mitral valve A wave 81 ± 9.6 88 ± 21.1 0.1
Mitral valve E/A ratio 0.89/0.4 0.88/0.4 0.1
Mitral valve deceleration time (ms) 43 (226, 72) 38 (203, 74) 0.1
Septal e´ (cm/s) 6.3 ± 1.3 5.8 ± 1.6 0.1
Septal E/e´ 11.8 ± 4.4 13.1 ± 4.7 0.1
Lateral e´ (cm/s) 8.2 ± 2.1 8.1 ± 2.9 0.8
Lateral E/e´ 8.9 ± 3.2 9.94 ± .1 0.1
Pulmonary vein systolic wave (cm/s) 52 ± 15.1 56 ± 15.3 0.3
Pulmonary vein diastolic wave (cm/s) 40.3 (40, 12.5) 42.7 (38, 13.5) 0.8
Pulmonary vein systolic wave to diastolic wave ratio 1.4 (1.5, 0.4) 1.4 (1.5, 0.4) 0.9
Diastolic stage % (n)
0 26.5% (17) 33.3% (20) 0.9
1 67.2% (43) 51.7% (31) 0.1
2 6.3% (4) 15% (9) 0.2
3 0 0 1
LV global longitudinal strain (%) –16.5 (–16.5, 1.09) –15.6 (16, 2.8) 0.1
n, number of patients; LV, left ventricle; EF, ejection fraction
40 Journal of Interdisciplinary Medicine 2020;5(2):35-42
Of note, baseline and follow-up echocardiograms were done at similar time intervals in treatment and control groups, respectively: 1.7 vs. 1.5 years (p >0.05).
Table 2 summarizes the various baseline echocardio-graphic parameters measured in this study, all of which were comparable between the treatment and the control group, respectively (p >0.05): mean baseline LVEF was 61% vs. 62%, 9.4% vs. 15% of patients had an impaired LVEF ≤45%, 51.7% vs. 67.2% of the patients had grade 1 diastolic dysfunction, 6.3% vs. 15% grade 2 and 0% grade 3. Global longitudinal strain was –16.5% vs. –15.6%, mean indexed end-diastolic volume was 44.5 mL/m2 vs. 45.6 mL/m2, and mean indexed end-systolic volume was 17.8 mL/m2 vs. 20.4 mL/m2.
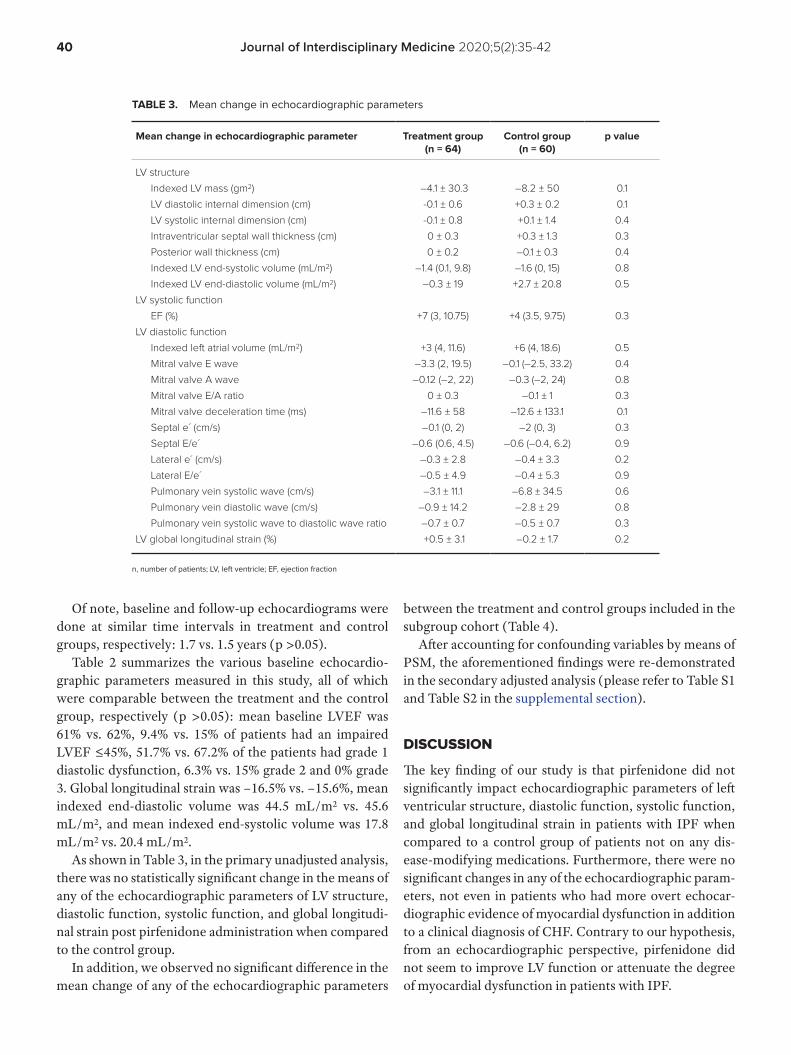
As shown in Table 3, in the primary unadjusted analysis, there was no statistically significant change in the means of any of the echocardiographic parameters of LV structure, diastolic function, systolic function, and global longitudi-nal strain post pirfenidone administration when compared to the control group.
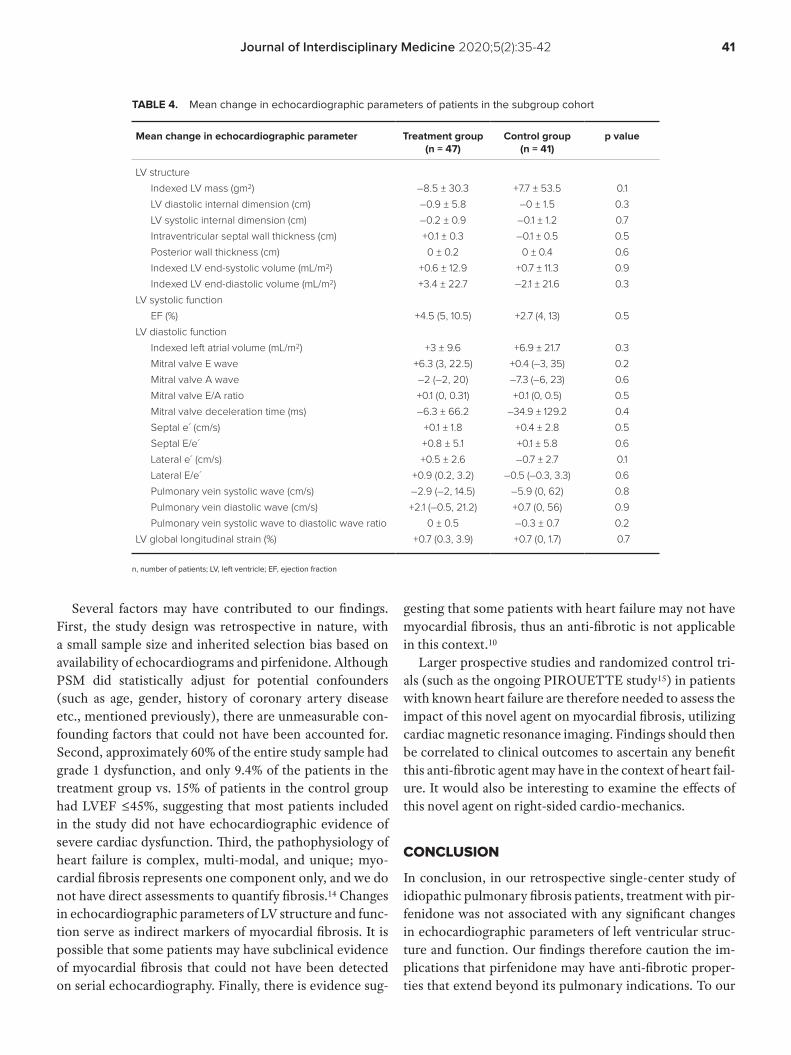
In addition, we observed no significant difference in the mean change of any of the echocardiographic parameters
between the treatment and control groups included in the subgroup cohort (Table 4).
After accounting for confounding variables by means of PSM, the aforementioned findings were re-demonstrated in the secondary adjusted analysis (please refer to Table S1 and Table S2 in the supplemental section).
diSCuSSioN
The key finding of our study is that pirfenidone did not significantly impact echocardiographic parameters of left ventricular structure, diastolic function, systolic function, and global longitudinal strain in patients with IPF when compared to a control group of patients not on any dis-ease-modifying medications. Furthermore, there were no significant changes in any of the echocardiographic param-eters, not even in patients who had more overt echocar-diographic evidence of myocardial dysfunction in addition to a clinical diagnosis of CHF. Contrary to our hypothesis, from an echocardiographic perspective, pirfenidone did not seem to improve LV function or attenuate the degree of myocardial dysfunction in patients with IPF.
TABLE 3. Mean change in echocardiographic parameters
Mean change in echocardiographic parameter Treatment group (n = 64)
Control group (n = 60)
p value
LV structure
Indexed LV mass (gm2) –4.1 ± 30.3 –8.2 ± 50 0.1
LV diastolic internal dimension (cm) -0.1 ± 0.6 +0.3 ± 0.2 0.1
LV systolic internal dimension (cm) -0.1 ± 0.8 +0.1 ± 1.4 0.4
Intraventricular septal wall thickness (cm) 0 ± 0.3 +0.3 ± 1.3 0.3
Posterior wall thickness (cm) 0 ± 0.2 –0.1 ± 0.3 0.4
Indexed LV end-systolic volume (mL/m2) –1.4 (0.1, 9.8) –1.6 (0, 15) 0.8
Indexed LV end-diastolic volume (mL/m2) –0.3 ± 19 +2.7 ± 20.8 0.5
LV systolic function
EF (%) +7 (3, 10.75) +4 (3.5, 9.75) 0.3
LV diastolic function
Indexed left atrial volume (mL/m2) +3 (4, 11.6) +6 (4, 18.6) 0.5
Mitral valve E wave –3.3 (2, 19.5) –0.1 (–2.5, 33.2) 0.4
Mitral valve A wave –0.12 (–2, 22) –0.3 (–2, 24) 0.8
Mitral valve E/A ratio 0 ± 0.3 –0.1 ± 1 0.3
Mitral valve deceleration time (ms) –11.6 ± 58 –12.6 ± 133.1 0.1
Septal e´ (cm/s) –0.1 (0, 2) –2 (0, 3) 0.3
Septal E/e´ –0.6 (0.6, 4.5) –0.6 (–0.4, 6.2) 0.9
Lateral e´ (cm/s) –0.3 ± 2.8 –0.4 ± 3.3 0.2
Lateral E/e´ –0.5 ± 4.9 –0.4 ± 5.3 0.9
Pulmonary vein systolic wave (cm/s) –3.1 ± 11.1 –6.8 ± 34.5 0.6
Pulmonary vein diastolic wave (cm/s) –0.9 ± 14.2 –2.8 ± 29 0.8
Pulmonary vein systolic wave to diastolic wave ratio –0.7 ± 0.7 –0.5 ± 0.7 0.3
LV global longitudinal strain (%) +0.5 ± 3.1 –0.2 ± 1.7 0.2
n, number of patients; LV, left ventricle; EF, ejection fraction
41Journal of Interdisciplinary Medicine 2020;5(2):35-42
Several factors may have contributed to our findings. First, the study design was retrospective in nature, with a small sample size and inherited selection bias based on availability of echocardiograms and pirfenidone. Although PSM did statistically adjust for potential confounders (such as age, gender, history of coronary artery disease etc., mentioned previously), there are unmeasurable con-founding factors that could not have been accounted for. Second, approximately 60% of the entire study sample had grade 1 dysfunction, and only 9.4% of the patients in the treatment group vs. 15% of patients in the control group had LVEF ≤45%, suggesting that most patients included in the study did not have echocardiographic evidence of severe cardiac dysfunction. Third, the pathophysiology of heart failure is complex, multi-modal, and unique; myo-cardial fibrosis represents one component only, and we do not have direct assessments to quantify fibrosis.14 Changes in echocardiographic parameters of LV structure and func-tion serve as indirect markers of myocardial fibrosis. It is possible that some patients may have subclinical evidence of myocardial fibrosis that could not have been detected on serial echocardiography. Finally, there is evidence sug-
gesting that some patients with heart failure may not have myocardial fibrosis, thus an anti-fibrotic is not applicable in this context.10
Larger prospective studies and randomized control tri-als (such as the ongoing PIROUETTE study15) in patients with known heart failure are therefore needed to assess the impact of this novel agent on myocardial fibrosis, utilizing cardiac magnetic resonance imaging. Findings should then be correlated to clinical outcomes to ascertain any benefit this anti-fibrotic agent may have in the context of heart fail-ure. It would also be interesting to examine the effects of this novel agent on right-sided cardio-mechanics.
CoNCluSioN
In conclusion, in our retrospective single-center study of idiopathic pulmonary fibrosis patients, treatment with pir-fenidone was not associated with any significant changes in echocardiographic parameters of left ventricular struc-ture and function. Our findings therefore caution the im-plications that pirfenidone may have anti-fibrotic proper-ties that extend beyond its pulmonary indications. To our
TABLE 4. Mean change in echocardiographic parameters of patients in the subgroup cohort
Mean change in echocardiographic parameter Treatment group (n = 47)
Control group (n = 41)
p value
LV structure
Indexed LV mass (gm2) –8.5 ± 30.3 +7.7 ± 53.5 0.1
LV diastolic internal dimension (cm) –0.9 ± 5.8 –0 ± 1.5 0.3
LV systolic internal dimension (cm) –0.2 ± 0.9 –0.1 ± 1.2 0.7
Intraventricular septal wall thickness (cm) +0.1 ± 0.3 –0.1 ± 0.5 0.5
Posterior wall thickness (cm) 0 ± 0.2 0 ± 0.4 0.6
Indexed LV end-systolic volume (mL/m2) +0.6 ± 12.9 +0.7 ± 11.3 0.9
Indexed LV end-diastolic volume (mL/m2) +3.4 ± 22.7 –2.1 ± 21.6 0.3
LV systolic function
EF (%) +4.5 (5, 10.5) +2.7 (4, 13) 0.5
LV diastolic function
Indexed left atrial volume (mL/m2) +3 ± 9.6 +6.9 ± 21.7 0.3
Mitral valve E wave +6.3 (3, 22.5) +0.4 (–3, 35) 0.2
Mitral valve A wave –2 (–2, 20) –7.3 (–6, 23) 0.6
Mitral valve E/A ratio +0.1 (0, 0.31) +0.1 (0, 0.5) 0.5
Mitral valve deceleration time (ms) –6.3 ± 66.2 –34.9 ± 129.2 0.4
Septal e´ (cm/s) +0.1 ± 1.8 +0.4 ± 2.8 0.5
Septal E/e´ +0.8 ± 5.1 +0.1 ± 5.8 0.6
Lateral e´ (cm/s) +0.5 ± 2.6 –0.7 ± 2.7 0.1
Lateral E/e´ +0.9 (0.2, 3.2) –0.5 (–0.3, 3.3) 0.6
Pulmonary vein systolic wave (cm/s) –2.9 (–2, 14.5) –5.9 (0, 62) 0.8
Pulmonary vein diastolic wave (cm/s) +2.1 (–0.5, 21.2) +0.7 (0, 56) 0.9
Pulmonary vein systolic wave to diastolic wave ratio 0 ± 0.5 –0.3 ± 0.7 0.2
LV global longitudinal strain (%) +0.7 (0.3, 3.9) +0.7 (0, 1.7) 0.7
n, number of patients; LV, left ventricle; EF, ejection fraction

42 Journal of Interdisciplinary Medicine 2020;5(2):35-42
knowledge, this is the first study in humans reviewing the implications of this novel agent outside the field of pulmo-nary medicine.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES
1. King TE, Jr., Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370:2083-2092.
2. Conte E, Gili E, Fagone E, Fruciano M, Iemmolo M, Vancheri C. Effect of pirfenidone on proliferation, TGF-beta-induced myofibroblast differentiation and fibrogenic activity of primary human lung fibroblasts. Eur J Pharm Sci. 2014;58:13-19.
3. Travers JG, Kamal FA, Robbins J, Yutzey KE, Blaxall BC. Cardiac Fibrosis: The Fibroblast Awakens. Circ Res. 2016;118:1021-1040.
4. Su MY, Lin LY, Tseng YH, et al. CMR-verified diffuse myocardial fibrosis is associated with diastolic dysfunction in HFpEF. JACC Cardiovasc Imaging. 2014;7:991-997.
5. Nguyen DT, Ding C, Wilson E, Marcus GM, Olgin JE. Pirfenidone mitigates left ventricular fibrosis and dysfunction after myocardial infarction and reduces arrhythmias. Heart Rhythm. 2010;7:1438-1445.
6. Li C, Han R, Kang L, et al. Pirfenidone controls the feedback loop of the AT1R/p38 MAPK/renin-angiotensin system axis by regulating liver X
receptor-alpha in myocardial infarction-induced cardiac fibrosis. Sci Rep.
2017;7:40523.
7. Mirkovic S, Seymour AM, Fenning A, et al. Attenuation of cardiac fibrosis by
pirfenidone and amiloride in DOCA-salt hypertensive rats. Br J Pharmacol.
2002;135:961-968.
8. Van Erp C, Irwin NG, Hoey AJ. Long-term administration of pirfenidone
improves cardiac function in mdx mice. Muscle Nerve. 2006;34:327-334.
9. Wang Y, Wu Y, Chen J, Zhao S, Li H. Pirfenidone attenuates cardiac
fibrosis in a mouse model of TAC-induced left ventricular remodeling by
suppressing NLRP3 inflammasome formation. Cardiology. 2013;126:1-11.
10. Graziani F, Varone F, Crea F, Richeldi L. Treating heart failure with
preserved ejection fraction: learning from pulmonary fibrosis. Eur J Heart
Fail. 2018;20:1385-1391.
11. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history
of congestive heart failure: the Framingham study. N Engl J Med.
1971;285:1441-1446.
12. Baek S, Park SH, Won E, et al. Propensity Score Matching: A Conceptual
Review for Radiology Researchers. Korean J Radiol. 2015;16:286-296.
13. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the
Evaluation of Left Ventricular Diastolic Function by Echocardiography:
An Update from the American Society of Echocardiography and the
European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc
Imaging. 2016;17:1321-1360.
14. Mohammed SF, Redfield MM. Response to Letters Regarding Article,
"Coronary Microvascular Rarefaction and Myocardial Fibrosis in Heart
Failure With Preserved Ejection Fraction". Circulation. 2015;132:e206.
15. Lewis GA, Schelbert EB, Naish JH, et al. Pirfenidone in Heart Failure with
Preserved Ejection Fraction-Rationale and Design of the PIROUETTE Trial.
Cardiovasc Drugs Ther. 2019.

Journal of Interdisciplinary Medicine 2020;5(2):43-47
CORRESPONDENCE
Oyetunde OyeyemiUniversity of Medical SciencesLaje Road, Ondo, NigeriaTel: +23 481 635 467 87E-mail: [email protected], [email protected]
ARTICLE HISTORY
Received: April 18, 2020Accepted: May 16, 2020
Malaria and HIV Infection among Febrile Patients in a Large Area of Southwestern NigeriaOyetunde T. Oyeyemi1, Edet J. Etim2
1 Department of Biological Sciences, University of Medical Sciences, Ondo, Nigeria2 Department of Biosciences and Biotechnology, Babcock University, Ilishan-Remo, Ogun State, Nigeria
oriGiNal rESEarCH EPIDEMIOLOGY // INFECTIOUS DISEASES
DOI: 10.2478/jim-2020-0011
ABSTRACT
Background: Malaria and HIV/AIDS are two major diseases that represent serious public health threats in Nigeria. They have been ascribed diseases of poverty, and therefore their distribution is expected to be overlapping. Aim: The aim of this study was to determine the prevalence of malaria parasites and HIV among febrile patients in the Ikeja area of Lagos State, Nigeria. Materials and Methods: The study was conducted on 300 patients attend-ing medical consultation and referred to blood screening for malaria parasites at Reddington Hospital, Lagos State. Malaria parasites were identified microscopically, and HIV screening was carried out using rapid diagnostic tests (RDT). Results: The prevalence of malaria and HIV was 98.7% and 3.7%, respectively. All HIV-positive individuals were also infected by ma-laria parasites. Mean parasitemia was significantly higher in HIV-positive individuals (16,507.9 ± 2,280.7 P/μL) than in HIV-negative subjects (3,252.505 ± 236.3 P/μL) (p <0.05). Conclusions: Our results suggest that HIV-infected individuals are more susceptible to infection with malaria parasites. Prompt HIV management is necessary in malaria-endemic areas to reduce disease severity in case of coinfection with HIV.
Keywords: malaria, HIV/AIDS, association, morbidity, Nigeria
Edet J. Etim • Babcock University, Ilishan-Remo, Ogun State, Nigeria. Tel. +23 470 320 494 18, E-mail: [email protected]
baCkGrouNd
Malaria and HIV/AIDS are two major diseases with serious public health impli-cations in Nigeria. Globally, Nigeria is ranked number one and two in the total number of people affected by malaria and HIV/AIDS, respectively.1,2 Both dis-eases are poverty-related, as the poorest segment of the population is the most vulnerable due to the lack of access to information, quality education, and good health facilities.3 Each year, malaria and HIV cause over 2 million deaths glob-ally.4 Children under the age of 5 and pregnant women have the highest morbid-ity associated with malaria parasites infection,5,6 while women and adolescent girls have the highest risk of HIV infection.7 During concurrent malaria parasites and HIV infections, approximately 1 million pregnant women experience vari-

44 Journal of Interdisciplinary Medicine 2020;5(2):43-47
ous degrees of complications in countries of sub-Saharan Africa,8 thus endangering the lives of both the mothers and the fetuses.
The geographical overlap between malaria parasites and HIV infections has generated research interest in terms of co-morbidity impact of concomitant infections. Some studies have suggested that there is no association between malaria parasites and HIV infection,9 especially in popu-lations where the prevalence of HIV is low.10 However, others have reported a bidirectional and synergistic in-teraction.11 Evidence has implicated concomitant malaria parasite and HIV infection in facilitating the progression of malaria. Importantly, malaria and HIV coinfection has been linked to an increased risk of severe malaria in adults, congenital infection, and increased transmission dynam-ics of the two diseases.12–14 On the other hand, malaria has been reported to cause a reduction in CD4 cell count, thus exacerbating the clinical course of those infected with HIV.15 Another study showed a significant rise in HIV-1 plasma load in individuals infected with malaria parasites compared to those without infection, even after up to 10 weeks of treatment.16 Factors influencing the clinical im-pact of these interactions could include extent of malaria transmission in the area, host immunity, and the individual affected (e.g., adult, child, or pregnant woman).17
The aim of this study was to determine the prevalence of malaria and HIV among febrile patients in the Ikeja area of Lagos State, Nigeria. The study also sought to gather more evidence on the susceptibility of individuals to malaria par-asites infection in case of concomitant infection with HIV.
matErialS aNd mEtHodS
The study was carried out in Ikeja, a city with a popula-tion of about 437,400 people, located in Lagos State, Ni-geria. The city is close to the popular Murtala Muhammad International Airport. It is the capital of Lagos State with a very large residential zone, and it is set near the Lagos Lagoon. There were over 60,000 cases of malaria in Ikeja in 2013.18 The closeness of the city to Lagos Lagoon and the poor drainage system found in some of its areas could provide suitable breeding sites for mosquito malaria para-site vectors, enabling stable transmission of malaria. As far as HIV/AIDS is concerned, its transmission is largely as-sociated with large population sizes and fluid movement of people in and out of the state.19
A descriptive cross-sectional study was conducted among febrile patients who presented themselves for medi-cal examination at Reddington Hospital, one of the many hospitals in Ikeja receiving malaria patients. To calculate
our sample size, we used the prevalence of malaria and HIV coinfection (2.9%) previously reported in Ikeja,20 and a pre-cision (d) of 2%. Using the method of Daniel,21 a minimum sample size of approximately 270 participants was calculat-ed. The study included 300 subjects, regular dwellers of the area or Lagos. Only febrile patients with signs and symp-toms of uncomplicated malaria, such as fever ≥40°C, chill, headache, rigor, and joint pain, were included.22
Venous blood samples were obtained from the subjects by a trained laboratory staff on duty. Clean and grease-free labeled glass slides were prepared, and then thick and thin blood films were made by spreading a drop of blood on the slides. The blood was allowed to dry and then stained with 10% Giemsa stain solution. After 10 min, the stain was washed with clean running water and then dried. A drop of immersion oil was applied to each slide and was examined under ×100 objective lens for malaria parasites. Parasitemia was estimated using the methods described by Cheesbrough.23
All subjects were screened using Determine (DT) HIV-1/2 test kits (Alere Medical Company Limited, Chiba, Japan). About 3–5 mL of blood was collected by veni-puncture and transferred to an EDTA bottle. The blood was properly mixed and then centrifuged at 1,500 rpm for 10 min. The plasma was stored in a plain tube and kept at –20°C until used. For testing, 50 μL of the plasma was added to the test spot on the kit, and the result was read after 15 min. The result was interpreted according to the kit instructions.
All kits were purchased centrally and were stored at the temperature specified by the manufacturer. Malaria and HIV tests were performed independently and were confirmed by another trained personnel. Participation in the study was voluntary, and only those who gave their consent were included. Children were included based on their parents’ consent. Institutional ethical approval was obtained from Olabisi Onabanjo University Teaching Hos-pital (OOUTH), Ogun State, Nigeria.
Data were analyzed using SPSS for Windows version 22.0 (IBM Corp, Armonk, NY, USA). Counts and percent-ages were used to summarize categorical variables, and the mean ± SE was used to summarize numerical variables. Differences in prevalence by subject categories were an-alyzed using the chi-square and Fisher’s exact test, while malaria parasitemia was analyzed using one-way ANOVA. Tukey’s post-hoc test was used to compare significant dif-ferences between groups. Significant differences in ma-laria parasitemia in relation to the participant’s HIV status was tested using Student’s t-test. A p value less than 0.05 (p <0.05) was considered statistically significant.
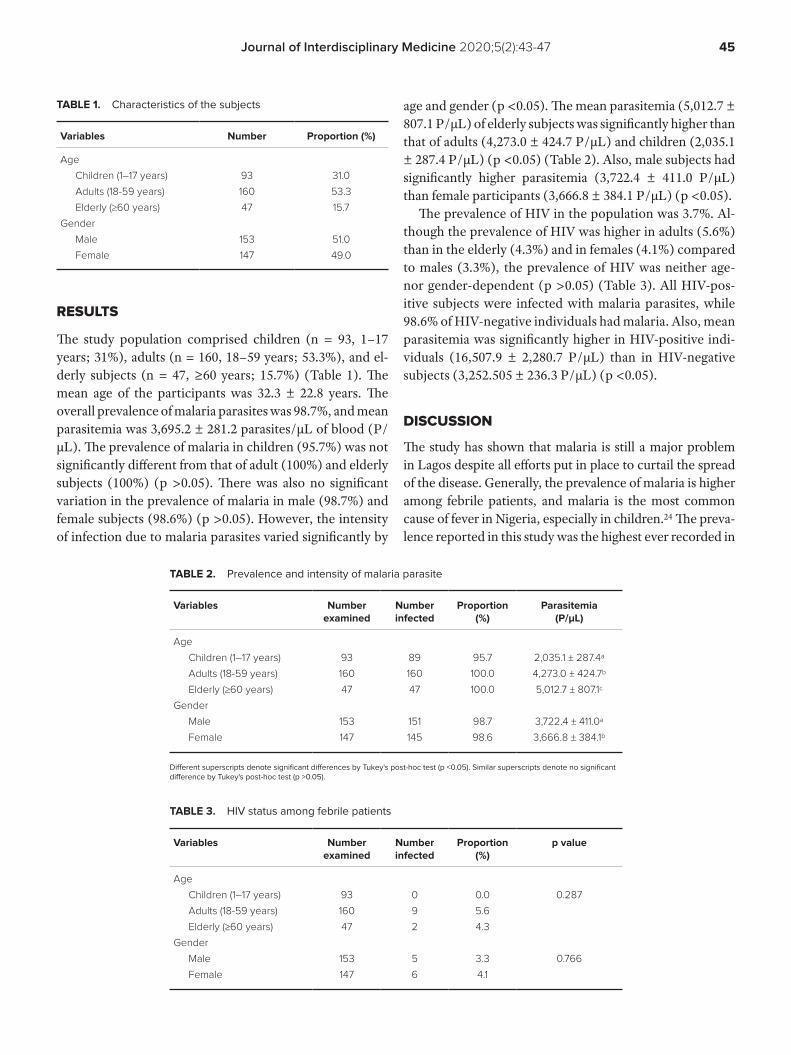
45Journal of Interdisciplinary Medicine 2020;5(2):43-47
rESultS
The study population comprised children (n = 93, 1–17 years; 31%), adults (n = 160, 18–59 years; 53.3%), and el-derly subjects (n = 47, ≥60 years; 15.7%) (Table 1). The mean age of the participants was 32.3 ± 22.8 years. The overall prevalence of malaria parasites was 98.7%, and mean parasitemia was 3,695.2 ± 281.2 parasites/μL of blood (P/μL). The prevalence of malaria in children (95.7%) was not significantly different from that of adult (100%) and elderly subjects (100%) (p >0.05). There was also no significant variation in the prevalence of malaria in male (98.7%) and female subjects (98.6%) (p >0.05). However, the intensity of infection due to malaria parasites varied significantly by
age and gender (p <0.05). The mean parasitemia (5,012.7 ± 807.1 P/μL) of elderly subjects was significantly higher than that of adults (4,273.0 ± 424.7 P/μL) and children (2,035.1 ± 287.4 P/μL) (p <0.05) (Table 2). Also, male subjects had significantly higher parasitemia (3,722.4 ± 411.0 P/μL) than female participants (3,666.8 ± 384.1 P/μL) (p <0.05).
The prevalence of HIV in the population was 3.7%. Al-though the prevalence of HIV was higher in adults (5.6%) than in the elderly (4.3%) and in females (4.1%) compared to males (3.3%), the prevalence of HIV was neither age- nor gender-dependent (p >0.05) (Table 3). All HIV-pos-itive subjects were infected with malaria parasites, while 98.6% of HIV-negative individuals had malaria. Also, mean parasitemia was significantly higher in HIV-positive indi-viduals (16,507.9 ± 2,280.7 P/μL) than in HIV-negative subjects (3,252.505 ± 236.3 P/μL) (p <0.05).
diSCuSSioN
The study has shown that malaria is still a major problem in Lagos despite all efforts put in place to curtail the spread of the disease. Generally, the prevalence of malaria is higher among febrile patients, and malaria is the most common cause of fever in Nigeria, especially in children.24 The preva-lence reported in this study was the highest ever recorded in
TABLE 1. Characteristics of the subjects
Variables Number Proportion (%)
Age
Children (1–17 years) 93 31.0
Adults (18-59 years) 160 53.3
Elderly (≥60 years) 47 15.7
Gender
Male 153 51.0
Female 147 49.0
TABLE 3. HIV status among febrile patients
Variables Number examined
Number infected
Proportion (%)
p value
Age
Children (1–17 years) 93 0 0.0 0.287
Adults (18-59 years) 160 9 5.6
Elderly (≥60 years) 47 2 4.3
Gender
Male 153 5 3.3 0.766
Female 147 6 4.1
TABLE 2. Prevalence and intensity of malaria parasite
Variables Number examined
Number infected
Proportion (%)
Parasitemia (P/μL)
Age
Children (1–17 years) 93 89 95.7 2,035.1 ± 287.4a
Adults (18-59 years) 160 160 100.0 4,273.0 ± 424.7b
Elderly (≥60 years) 47 47 100.0 5,012.7 ± 807.1c
Gender
Male 153 151 98.7 3,722.4 ± 411.0a
Female 147 145 98.6 3,666.8 ± 384.1b
Different superscripts denote significant differences by Tukey's post-hoc test (p <0.05). Similar superscripts denote no significant difference by Tukey's post-hoc test (p >0.05).

46 Journal of Interdisciplinary Medicine 2020;5(2):43-47
any region of Nigeria among febrile patients. Previous stud-ies reported a prevalence of 7.4% in Ilorin,25 29.7% in Oyo town,26 and 37.6% in Ikare-Akoko, Ondo.27 Higher preva-lences of 54%,28 56%,29 63%,30 56.8%,31 and 65.5%32 were re-ported in Jos, Sokoto, Simawa Ogun State, Keffi, and Birnin Kudu in Kano State, respectively. In Lagos, our previous study found a prevalence of 39.5%, 61% and 61.3% among febrile infants, non-pregnant women, and pregnant women, respectively.22 Another study in Lagos reported a very high prevalence (92.1%) among febrile infants (age 0–5 years).24
This study confirmed that Lagos State is a suitable re-gion for stable transmission of malaria. Evidence from the State’s report on malaria cases showed that malaria transmission is far from being under control. Reports have shown an increase in malaria cases from 488,780 in 2012 to 547,150 in 2014.33 The probable reasons for this unabated increase in transmission include the presence of abundant water bodies in close proximity to human dwellings, suit-able for the breeding of mosquitoes and subsequent trans-mission of malaria parasite to humans. Due to poor drain-ing systems in many areas, this expanse of water bodies sometimes finds its way into canals and drainage systems, especially during flooding, to create further temporary breeding sites for these mosquitoes. Another possible rea-son could be the very low utilization of long-lasting insec-ticide-treated nets (LLIN) in Lagos, with a reported utili-zation rate of 18%.34 This value is significantly lower than the 59% and 67.6% LLIN utilization rates recorded in Osun and Ekiti State, respectively.34,35 Lagos is a megacity, and LLIN distribution through the government’s malaria con-trol program may pose some difficulties. In another study, adherence to current malaria treatment guidelines in La-gos was generally poor, as only 7% of people were using an artemisinin-based combined therapy in their last malaria episode; the majority of patients still preferred sulphadox-ine-pyrimethamine and chloroquine.36 This could increase the development of resistant parasite strains, especially in the case of chloroquine.
Although there was no significant difference in the prevalence of malaria among different population groups, parasitemia varied significantly, with the older population carrying the higher burden of the disease. It is usually ex-pected that children, especially infants, would bear the greatest burden of malaria, because acquired immunity may still be not well developed. However, advocacy for ma-laria prevention in children and pregnant women has been strong recently in Nigeria. This may yield a better adher-ence to malaria control in these groups. Even with limited resources, children (0–5 years) and pregnant women are given priority in malaria control programs in every state
of Nigeria. These programs may have an impact by reduc-ing the extent of exposure to mosquitoes and subsequently lowering the intensity of malaria parasites infection in these groups. Nevertheless, the mean parasitemia recorded in children was very high in our study, and efforts towards abating transmission should be further strengthened, not only in children, but also in the adult population (age 18–59 years) that has a significant number of pregnant women.
In our study, the prevalence of HIV was lower than in many studies reported elsewhere in Nigeria. A prevalence of 4.9% was reported in Osogbo,37 6.2% in Abeokuta,38 24.1% in Borno,39 10% in Benin, and 16% in Zaria.40 The low prevalence we found in Lagos could represent the positive impact of the various HIV/AIDS prevention programs in the state. Of importance is the possible contribution of HIV infection to increasing susceptibility to malaria parasites in-fection. This was demonstrated by the increased prevalence and intensity of malaria parasites infection in HIV-positive subjects compared to HIV-negative individuals. While ear-lier studies have shown no relationship between HIV and the severity of malaria in children and adults,41,42 our results seem to confirm the findings of studies that have linked HIV infection to a predisposition to more frequent episodes of symptomatic and severe malaria.43 It is possible that by sup-pressing the immune system, HIV favors the multiplication and proliferation of malaria parasites.
CoNCluSioN
This study has shown that malaria was hyperendemic among febrile patients, while HIV had a low incidence in Ikeja, La-gos. Due to the possible interactions between malaria and HIV/AIDS, the presence of one can influence the morbid-ity associated with the other. HIV increases susceptibility to malaria parasites and could therefore aggravate the burden associated with malaria in infected individuals, with more serious consequences in pregnant women and infants. In order to minimize the impact of HIV on malaria, malaria and HIV control programs should be integrated into one another. The distribution of LLIN and promotion of their usage should be incorporated into voluntary counselling and testing programs in malaria endemic areas. Prompt treatment of malaria confirmed febrile patients is also high-ly recommended, especially in HIV/AIDS endemic areas.
aCkNoWlEdGEmENt
The authors acknowledge the participants and the person-nel on duty in Reddington Hospital, Ikeja, Lagos, Nigeria during data collection for their cooperation.

47Journal of Interdisciplinary Medicine 2020;5(2):43-47
StatEmENt of EtHiCS
Informed consent was obtained from the participants. Eth-ical approval with approval number OOUTH/DA.326/899 was obtained from Olabisi Onabanjo University Teaching Hospital, Ogun State, Nigeria.
CoNfliCt of iNtErESt
None declared.
rEfErENCES1. National Agency for the Control of AIDS (NACA). National Strategic
Framework on HIV and AIDS: 2017-2021. Available at: https://naca.gov.ng/wp-content/uploads/2017/09/NATIONAL-HIV-AND-AIDS-STRATEGIC-FRAMEWORK.pdf
2. World Health Organisation (WHO). World Malaria Report, 2018. Available at. https://www.who.int/malaria/publications/world-malaria-report-2018/report/en/
3. Kwenti TE. Malaria and HIV coinfection in sub-Saharan Africa: prevalence, impact, and treatment strategies. Res Rep Trop Med. 2018;9:123–36.
4. World Health Organisation (WHO). Malaria in HIV/AIDS Patients. Geneva: WHO; 2017. Available at: https://www.who.int/malaria/areas/high_risk_groups/hiv_aids_patients/en/
5. World Health Organisation (WHO). World Malaria Report 2015. Geneva: WHO; 2015. Available at: https://www.who.int/malaria/publications/world-malaria-report-2015/report/en/
6. Kwenti TE, Kwenti TD, Latz A, Njunda LA, Nkuo-Akenji T. Epidemiological and clinical profile of paediatric malaria: a cross sectional study performed on febrile children in five epidemiological strata of malaria in Cameroon. BMC Infect Dis. 2017;17:499.
7. Joint United Nations Programme on HIV and AIDS. Fact sheet: World AIDS Day 2017. 2017. Available at: http://www.unaids.org/sites/ default/files/media_asset/UNAIDS_FactSheet_en.pdf.
8. González R, Ataíde R, Naniche D, Menéndez C, Mayor A. HIV and malaria interactions: where do we stand? Expert Rev Anti Infect Ther. 2012;10:153-165.
9. Salako LA, Idigbe EO, Erinosho MA, Akinosho RO, Mafe AG. Malaria and Human Immunodeficiency Virus (HIV) infection among adults in Ogun State, South-Western Nigeria. Niger Quarterly J Hospital Med. 1996;6:279-283.
10. Cuadros DF, Branscum AJ, García-Ramos G. No evidence of association between HIV-1 and malaria in populations with low HIV-1 Prevalence. PLoS ONE. 2011;6: e23458.
11. Alemu A, Shiferaw Y, Addis Z, Mathewos B, Birhan W. Effect of malaria on HIV/AIDS transmission and progression. Parasites Vect. 2013;6:18.
12. French N, Nakiyingi J, Lugada E, Watera C, Whitworth JA, Gilks CF. Increasing rates of malarial fever with deteriorating immune status in HIV-1-infected Ugandan adults. AIDS. 2001;15:899-906.
13. Abu-Raddad LJ, Patnaik P, Kublin JG. Dual infection with HIV and malaria fuels the spread of both diseases in sub-Saharan Africa. Science. 2006;314:1603-1606.
14. Perrault SD, Hajek J, Zhong K, et al. Human immunodeficiency virus coinfection increases placental parasite density and transplacental malaria transmission in Western Kenya. Am J Trop Med Hyg. 2009;80:119-125.
15. Kublin JG, Patnaik P, Jere CS, et al. Effect of Plasmodium falciparum malaria on concentration of HIV-1-RNA in the blood of adults in rural Malawi: a prospective cohort study. Lancet. 2005;365:233-240.
16. Mermin J, Lule JR, Ekwaru JP. Association between malaria and CD4 cell count decline among persons with HIV. J Acquir Immune Defic Syndr. 2006;41:129-130.
17. Kamya MR. Effect of HIV-1 infection on antimalarial treatment outcomes in Uganda: a population-based study. J Infect Dis. 2000;193:9-15.
18. Omogunloye OG, Abiodun OE, Olunlade OA, Epuh EE, Asikolo I, Odumosu JO. Modeling malaria prevalence rate in Lagos state using multivariate environmental variations. Geoinformatics FCE CTU. 2018;17:61-86.
19. Ehiri JE, Alaofè HS, Yesufu V, et al. AIDS-related stigmatisation in the healthcare setting: a study of primary healthcare centres that provide
services for prevention of mother-to-child transmission of HIV in Lagos, Nigeria. BMJ Open. 2019;9:e026322.
20. Sanyaolu AO, Fagbenro-Beyioku AF, Oyibo WA, Badaru OS, Onyeabor OS, Nnaemeka CI. Malaria and HIV co-infection and their effect on haemoglobin levels from three health-care institutions in Lagos, southwest Nigeria. Afr Health Sci. 2013;13:295-300.
21. Daniel WW. Biostatistics: a foundation for analysis in the health sciences. 7th ed. New York: John Wiley and Sons, 1999.
22. Oyeyemi OT, Sode OJ, Adebayo OD, Mensah-Agyei GO. Reliability of rapid diagnostic tests in diagnosing pregnancy and infant-associated malaria in Nigeria. J Inf Public Health. 2016;9:471-477.
23. Cheesbrough M. District Laboratory Practice in Tropical Countries, 2nd ed. Norfolk: Tropical Health Technology, 2009; p. 239-259.
24. Enya VNV, Idika N, Mafe AG, et al. Aetiology of fever among under-fives in Lagos, Nigeria. BMC Infect Dis. 2014;14:P42.
25. Kolawole OM, Irekeola AA, Seriki AA, Bello KE. Investigation of risk factors associated with malaria and yellow fever coinfection among febrile patients in Ilorin, Nigeria. J Med Soc. 2018;32:33-39.
26. Adedotun AA, Salawu OT, Morenikeji OA, Odaibo AB. Plasmodial infection and haematological parameters in febrile patients in a hospital in Oyo town, South-western Nigeria. J Public Health Epidemiol. 2013;5:144-148.
27. Igharo EA, Osazuwa F, Ajayi SA, Ebueku A, Igbinigie O. Dual infection with typhoid and malaria in febrile patients in Ikare Akoko, Nigeria. Int J Trop Med. 2012;7:49-52.
28. Ukaegbu CO, Nnachi AU, Mawak JD, Igwe CC. Incidence of concurrent malaria and typhoid fever infections in febrile patients in Jos, Plateau State Nigeria. Int J Sci Tech Res. 2014;3:157-161.
29. Singh S, Madaki AJ, Jiya NM, Singh R, Thacher TD. Predictors of malaria in febrile children in Sokoto, Nigeria. Niger Med J. 2014;55:480-485.
30. Ayorinde AF, Oyeyiga AM, Nosegbe NO, Folarin OA. A survey of malaria and some arboviral infections among suspected febrile patients visiting a health centre in Simawa, Ogun State, Nigeria. J Inf Public Health. 2016;9:52-59.
31. Jemimah Y, Victor O, Elizabeth A, Akpu P, Lynda A. Plasmodium falciparum infection among febrile patients attending a tertiary healthcare facility in Central Nigeria: prevalence, hematologic and sociodemographic factors. Int J Trop Dis. 2019;2:1-6.
32. Michael GC, Aliyu I, Idris U, et al. Investigation of malaria by microscopy among febrile outpatients of a semi-rural Nigerian medical center: what happened to malaria control programs? Niger J Gen Pract. 2019;17:23-30.
33. Osunkiyesi, M. The road to 2020: mobilising the private sector in Nigeria’s fight against malaria – the Lagos State approach. Presented at the 2015 CAMA Annual Technical Forum.
34. Israel OK, Fawole OI, Adebowale AS, et al. Caregivers’ knowledge and utilization of long-lasting insecticidal nets among under-five children in Osun State, Southwest, Nigeria. Malar J. 2018;17:231.
35. Omonijo A, Omonijo AO. Assessment of the status of awareness, ownership, and usage of long-lasting insecticide treated nets after mass distribution in Ekiti State, Nigeria. J Parasitol Res. 2019:1273714.
36. Wright KO, Tayo F, Odusanya OO, et al. Perception and practices of Lagos state residents on the prevention and control of malaria in Lagos, Nigeria. Ann Trop Med Public Health. 2013;6:503-507.
37. Umolu PI, Okoror LE, Orhue P. Human immunodeficiency virus (HIV) seropositivity and hepatitis B surface antigenemia (HBSAG) among blood donors in Benin City, Edo state, Nigeria. Afr Health Sci. 2005;5:55-58.
38. Motayo BO, Faneye AO, Udo UA, Olusola BA, Ezeani I, Ogiogwa JI. Seroprevalence of transfusion transmissible infections (TTI), in first time blood donors in Abeokuta, Nigeria. Afr Health Sci. 2015;15:19-25.
39. Onoja A, Mohammed SB, Ya’aba Y, Liman M, Njab J. Seroprevalence of HIV among the people of Lake Chad Basin of Borno State, Nigeria. JOPAT. 2016;15:31-39.
40. Simon M, Anyebe EE, Ojo CO, Ankuma, SJ. Prevalence of HIV among pregnant women attending antenatal clinic in a teaching hospital in Northwest Nigeria. West Afr J Nursing. 2016;27:56-74.
41. Kalyesubula I, Musoke-Mudido P, Marum L, et al. Effects of malaria infection in human immunodeficiency virus type 1-infected Ugandan children. Pediatr Infect Dis J. 1997;16:876-881.
42. Chandramohan D, Greenwood BM. Is there an interaction between human immunodeficiency virus and Plasmodium falciparum? Int J Epidemiol. 1998;27:296-301.
43. Kamya MR, Gasasira AF, Yeka A, et al. Effect of HIV1 infection on antimalarial treatment outcomes in Uganda: a population-based study. J Infect Dis. 2006;193:9-15.

Journal of Interdisciplinary Medicine 2020;5(2):48-55
CORRESPONDENCE
Zsuzsánna PapStr. Gheorghe Marinescu nr. 38540139 Targu Mureş, RomaniaTel: +40 265 215 551E-mail: [email protected]
ARTICLE HISTORY
Received: May 19, 2020Accepted: May 25, 2020
Ultrasound-Guided Core-Needle Biopsy of Suspicious Breast LesionsKincső-Zsófia Lőrincz1, Zsuzsánna Pap2, Simona Lileana Mocan3,4, Csanád-Endre Lőrincz5,
Beáta-Ágota Baróti6
1 Radiology and Medical Imaging Laboratory, Mures County Emergency Clinical Hospital, Targu Mures, Romania2 Department of Anatomy and Embryology, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology,
Targu Mures, Romania3 SC Morphomed SRL, Targu Mures, Romania4 Department of Pathology, Mures County Emergency Clinical Hospital, Targu Mures, Romania5 Hungarian Department of Biology and Ecology - Medical Biology, Babes-Bolyai University, Cluj Napoca, Romania6 Department of Radiology and Medical Imaging, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology,
Targu Mures, Romania
oriGiNal rESEarCH RADIOLOGY // ANATOMICAL PATHOLOGY
DOI: 10.2478/jim-2020-0010
ABSTRACT
Background: Breast cancer is the female cancer with the highest mortality. While early de-tection is a public health priority in Western European countries, a screening program in our country has yet to be implemented. The best diagnostic accuracy is achieved through the use of triple assessment: clinical examination, imaging, and core-needle biopsy where indicated. Prognosis is influenced by clinical, histological, and biological factors, and therapy is most ef-fective when individually tailored. Aim of the study: To analyze the clinical, histological, and immunohistochemical characteristics of the biopsied nodules and summarize our experience from the last three years. Material and Methods: We retrospectively analyzed data from 137 patients who underwent core-needle biopsy between 2017 and 2019. Imaging score was as-signed based on ultrasound examination or mammography. Clinical and pathological param-eters were recorded, followed by statistical processing of the data. Results: The mean age of the patients was 58 ± 14 years, lesions had a mean size of 22.83 ± 14.10 mm. Most nodules (n = 63, 47.01%) were located in the upper-outer quadrant, and bilateral presence was found in 4 (3.08%) cases. We found a significant positive correlation between lesion size and the patients’ age (Spearman r = 0.356; 95% CI 0.186, 0.506; p = 0.000). The malignancy rates within the Breast Imaging Reporting and Data System (BI-RADS) categories were as follows: 0% for „4a”, 31.58% for „4b”, 71.42% for „4c”, and 97.72% for „5”. Most malignancies (n = 73, 78.35%) were represented by invasive ductal carcinoma of no special type, 58.43% (n = 52) were grade 2, 89.13% (n = 82) were estrogen receptor positive, and Luminal B-like type was the most common (n = 63, 78.75%). Conclusions: The mean size of tumors was larger than the average size at discovery described in the literature. In our region, age and tumor size are positively correlat-ed. Preoperative histological results may indicate the reliability of the imaging risk stratification system. Most cases can benefit from adjuvant endocrine therapy.
Keywords: breast cancer, screening, imaging, biopsy, immunohistochemistry
Kincső-Zsófia Lőrincz • Str. Gheorghe Marinescu nr. 50, 540136 Targu Mureş, Romania. Tel: +4,0 372 653 100. E-mail: [email protected]
Simona Lileana Mocan • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mureş, Romania. Tel: +40 265 215 551, E-mail: [email protected]
Csanád-Endre Lőrincz • Str. Mihail Kogălniceanu nr. 1, 400000 Cluj-Napoca, Romania. Tel: +40 264 405 300, E-mail: [email protected]
Beáta-Ágota Baróti • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mureş, Romania. Tel: +40 265 215 551, E-mail: [email protected]

49Journal of Interdisciplinary Medicine 2020;5(2):48-55
iNtroduCtioN
Breast cancer accounts for a quarter of all female cancers and is among the leading causes of cancer deaths. In Ro-mania, its general mortality is lower than in Western Euro-pean countries, with an age-standardized incidence of 54.5 cases per 100,000 and a 15.5 mortality rate in 2018.1
While national mortality has decreased in the younger population over the last two decades, it is still rising in the 65+ age group, suggesting that information about the necessity of screening has not reached the target popu-lation.2 On the other hand, screening carries the risk of overdiagnosis, followed by overtreatment, and can lead to a 20% increase in mastectomies and more use of ra-diotherapy, according to a Danish study.3 Cancer experts from several countries advise making early detection a public health priority and taking action to decrease the number of false positive diagnoses, which could be facili-tated by the use of core-needle biopsy in the evaluation process.4,5
In multidisciplinary breast clinics, lumps undergo a triple assessment consisting of clinical examination, im-aging, and preoperative biopsy, where needed.6 While the Breast Imaging Reporting and Data System (BI-RADS) developed by the American College of Radiology approximates the risk of malignancy in breast lumps, ul-trasound-guided core-needle biopsy provides gold-stan-dard histological results, with a sensitivity of 97–99%.7 Therapy is most effective when individually tailored; as a result, in addition to histological classification, it is of great importance to establish hormone-receptor status and the molecular subtype of each tumor. The urge to request the estrogen receptor (ER), progesterone recep-tor (PR), and human epidermal growth factor receptor 2 (HER2) status of all invasive breast cancers is included in the United Kingdom National Health Service guidelines for the diagnosis and management of early and locally ad-vanced breast cancer.8 The traits that characterize the dif-ferent subtypes are pathological grade and proliferation, response to chemotherapy, and response to endocrine therapy.9 In addition, Ki-67 protein status is possibly a prognostic and predictive factor for adjuvant chemo-therapy.10–12
In the effort to diagnose breast cancer in its early stages, we have been performing core-needle biopsies as part of the triple assessment used in multidisciplinary breast clin-ics. The aim of this study is to analyze the clinical, imaging, histological, and immunohistochemical characteristics of the biopsied nodules and summarize our experience from the last three years.
matErial aNd mEtHodS
We retrospectively analyzed the case records of 137 pa-tients with breast lesions who underwent triple assess-ment consisting of clinical examination, imaging, and core-needle biopsy between January 2017 and December 2019. During the selection of the cases, we divided the pa-tients into two groups. The first one was formed of 130 fe-male patients, of all ages, with no personal medical history of breast malignancies. The second group of 7 patients was formed of special cases which corresponded to one of the following criteria: male; previous treatment for breast can-cer; metastasis found in the breast, with the primary tumor located in other organs. Bilateral breast nodules were cata-logued as two separate cases. Clinical information includ-ed the patients’ sex, age, and relevant personal and family medical history. During ultrasound examination, the loca-tion and size of the lump, morphologic features, imaging characteristics, and presence of suspicious lymph nodes were noted. The risk of breast cancer was determined by mammography and ultrasound in the majority of cases; for patients younger than 35 only ultrasonography was used. Cancer risk was estimated using the BI-RADS risk strati-fication tool: 0 – incomplete; 1 –negative; 2 – benign; 3 – probably benign; 4 – suspicious for malignancy, where 4a represents a probability of 2–9%, 4b 10–49%, 4c 50–94%; 5 – highly suspicious of malignancy, with a probability of over 95%. The core-needle biopsy was performed with ultrasound guidance, under local anesthesia with 1% lido-caine using a Bard Magnum biopsy gun with a 14-gauge needle. Histopathological examination of the bioptic ma-terial delivered information about the histological type and grade of malignancy of the tumor. We used the pro-tocol of the College of American Pathologists (CAP) for the examination of biopsy specimens from patients with invasive carcinoma of the breast to report every malignant specimen; we also included current WHO classification of breast tumors and the Nottingham combined histologic grade (Elston-Ellis modification of Scarff-Bloom-Richard-son grading system).13–16 A surrogate molecular breast can-cer classification was used based on immunohistochemi-cal assessment of biomarkers (ER, PR, HER2, and Ki-67) and in situ hybridization confirmation, adopted by the 13th St. Gallen International Breast Cancer Conference (2013).17–19 The five categories were: Luminal A-like (ER positive, PR positive, HER2 negative, Ki-67 low), Luminal B-like (HER2-negative) (ER positive, HER2 negative, and at least one of the following: Ki-67 high, or PR negative or low), Luminal B-like (HER2-positive) (ER positive, HER2 overexpressed or amplified, PR any), HER2-positive (non-

50 Journal of Interdisciplinary Medicine 2020;5(2):48-55
luminal) (HER2 overexpressed or amplified, ER negative, PR negative), and Triple-negative (ER negative, PR nega-tive, HER2 negative). Cut-off values were set according to the guideline of the American Society of Clinical Oncol-ogy/College of American Pathologists for immunohisto-chemical testing.20
Statistical analysis was performed using Microsoft Ex-cel Professional Plus 2010 (version 14.0.7116.5000) and Graph Pad Prism (version 8.4.0.671). Numerical data were expressed as mean ± standard deviation. Categorical data were expressed as frequency and percentage. Associations between age and other prognostic factors were evaluated by Chi square tests. P values smaller than 0.05 were consid-ered statistically significant.
The study was conducted in accordance with the prin-ciples stipulated in the Declaration of Helsinki. Informed consent was waived by the ethics committee of the institu-tion, as the study was retrospective.
rESultS
The study population consisted of 137 patients with breast lumps who underwent core-needle biopsy, 136 (99.27%) of which were females. The mean age of the patients was 58 ± 14 years. Malignant tumors were found in 97 (80.17%) cases, and 24 (19.83%) cases were benign. In 17.05% (n = 15) of breast cancer cases, family history was positive for breast cancer, and two of these patients were younger than the rec-ommended screening age for normal risk of breast cancer.
Upon presentation, the lesions had an overall mean size of 22.83 ± 14.10 mm, malignant lesions being slightly larger (23.46 ± 10.75 mm) (Table 1). Nodules were most frequently located in the upper-outer quadrant (UOQ) (n = 63, 47.01%), and bilateral presence was found in 4 cas-es (Table 1). Tumor frequency for each site and BI-RADS scores are listed in Table 1, along with size and age distribu-tions. We found a significant positive correlation between lesion size and the patient’s age (Spearman r = 0.356; 95% CI 0.186, 0.506; p = 0.00), suggesting an increase in tumor size with the advancement of age (Figure 1).
The malignancy rates within the BI-RADS categories were as follows: 0% for „4a”, 31.58% for „4b”, 71.42% for „4c” and 97.72% for „5”.
Tumor histological types for each category are listed in Table 2.
The occurrence of benign/malignant tumor types was significantly different (p <0.0001) in patients aged 40 or younger, mostly diagnosed with benign nodules (n = 8, 88.89%), compared to older patients whose nodules were mostly malignant (n = 92, 85.19%). Malignancy rates based
on age categories are presented in Figure 2. The cancer-free biopsies were mostly fibroadenomas (n = 15, 62.5%), normal breast tissue being found in 4 cases (16.67%). Most malignancies (n = 73, 78.35%) were represented by inva-sive ductal carcinoma (IDC) of no special type, followed by lobular (n = 9, 9.28%), mucinous (n = 5, 5.15%), papil-lary (n = 4, 4.12%), tubular (n = 1, 1.03%), cribriform (n = 1, 1.03%), and neuroendocrine (n = 1, 1.03%) types. No cases of carcinoma with medullary pattern were found. The histological type of the tumors showed a correlation of statistical significance with the patient’s age, as IDC was the most frequently diagnosed type in all age categories, except the last one (81 and older), where the mucinous type was the most common (p = 0.044). The rates of tumor types found in each age category are presented in Figure 3. The distribution of malignancy grades across age groups is
TABLE 1. Clinical and imaging data
n %
Laterality Left 61 44.53
Right 72 52.55
Bilateral 4 2.92
Location UOQ 63 47.01
LOQ 6 4.48
UIQ 18 13.43
LIQ 7 5.22
CC 18 13.43
U 10 7.46
L 7 5.22
I 0 0
O 5 3.73
Size <10 mm 18 14.52
10.1–20 mm 50 40.32
20.1–30 mm 32 25.81
31–40 mm 12 9.68
41–50 mm 10 8.06
>50 mm 2 1.61
Age (years) <20 2 1.50
20-30 2 1.50
31-40 6 4.51
41-50 32 24.06
51-60 22 16.54
61-70 37 27.82
71-80 24 18.05
>80 4 3.01
BI-RADS 4a 7 5.79
4b 19 15.70
4c 7 5.79
5 88 72.73
UOQ, upper-outer quadrant; LOQ, lower-outer quadrant; UIQ, upper-inner quadrant; LIQ, lower-inner quadrant; CC, central; U, limit of upper quadrants; L, limit of lower quadrants; I, limit of inner quadrants; O, limit of outer quadrants

51Journal of Interdisciplinary Medicine 2020;5(2):48-55
presented in Figure 4. Grade 2 tumors were the most com-mon (n = 52, 58.43%), especially in the 61–70 and 41–50 age groups. Grade 1 tumors were observed in patients aged 41 and older, becoming more and more frequent until the age of 70. Grade 3 tumors were present in patients aged between 41 and 80, most of them occurring in the 61–70 age group. There was no statistically significant correlation between age and grade of malignancy (p >0.05).
The immunohistochemistry assays concluded that 89.13% (n = 82) of lesions were ER-positive with all specimens above 10% staining, 67.03% (n = 61) were PR positive, and 80.43% (n = 74) expressed high Ki-67 lev-els. HER-2 positivity was 26.09% (n = 24). Luminal B-like (HER2-negative) type was the most common (n = 45, 56.25%), followed by Luminal B-like (HER2-positive) (n = 18, 22.5%), Luminal A-like (n = 8, 10%), and HER2-positive (n = 6, 7.5%). Triple-negative tumors (TNBC) were the least common, accounting for 3.75% (n = 3) of
all cases. Luminal B-like (HER2-positive) tumors were more frequent in patients under 50 years, Luminal B-like (HER2-negative) tumors being dominant above this age. The largest triple-negative tumor rate was observed in the 80+ age category. There was no statistically significant cor-relation between age and tumor molecular type (p >0.05).
A number of 7 cases were not included in the calcula-tions above. One male patient underwent biopsy for a BI-RADS 4c lesion, which proved to be gynecomastia with normal breast tissue. Two female patients, already surgi-cally treated for breast cancer, were found with suspicious lesions. Histopathological examination found no sign of recurrence, the ultrasonographic appearance being due to scar tissue. There were two cases of recurrence, one intra-mammary lymph node metastasis involving IDC of no spe-cial type, and one case of metastatic melanoma.
diSCuSSioNS
In the European Union (EU), the breast is the most com-mon site of cancer among women, whereas male breast cancer represents approximately 1% of all breast cancer cases.21,22 Recommendations of the European Commission (EC), last updated in 2020, include biannual mammogra-phy screening for women aged between 45 and 69 years.23
Over the last two decades, the median tumor size has been decreasing, reaching 11–15 mm with the use of ra-diological screening methods, but remains between 19–21 mm when discovered by self-detection or clinical exami-nation.24,25 The mean age of patients in our study (58 ± 14 years) fits the target age group for screening; however, the mean size at discovery was above average (23.46 vs. 11–15 mm/19–21 mm). The 2017 EC Eurostat report regarding
FIGURE 1. Patient age and tumor size correlation
TABLE 2. Tumor histological type by BI-RADS categories
BIRADS 4a(n)
BIRADS 4b(n)
BIRADS 4c(n)
BIRADS 5(n)
Benign
FA 4 10 1 0
Other 3 3 1 2
Malignant
IDC 0 5 3 68
Lobular 0 0 0 9
Papillary 0 0 2 2
Mucinous 0 0 0 5
Other 0 1 0 2
FA, fibroadenoma; IDC, invasive ductal carcinoma

52 Journal of Interdisciplinary Medicine 2020;5(2):48-55
breast cancer screening places Romania last among EU member states with 0.2% participation in 2015.26 Accord-ing to data collected in 2016, participation reached 6%.21 By contrast, in Western member states, participation is above 75%.26 This discrepancy in screening participation rates and median tumor size suggest that either self-de-tection or clinical examination applied to the majority of our cases. Multiple studies have concluded that tumor size at discovery is correlated with lymph node status and the presence of metastases, and it is an independent predic-tor for mortality.27–31 In a cohort study of 819,647 women, published in 2018, for tumors from 9 to 20 mm, mortal-
ity increased from 7.0 to 22.3%.32 We found a statistically significant positive correlation between lesion size and the patients’ age. Although slower growing tumors are diag-nosed in elderly women, this category of patients is often less informed than the younger population and is reluctant to seek medical help. Studies from other geographical re-gions have reached opposite conclusions, suggesting that size decreases with advancement of age or have not found any significant correlation.33–35
General screening recommendations apply to women aged 45 to 69 with normal risk for breast cancer, but in many cases individual risk factor identification is neces-
1
15
1426
13
1
23
31
2 1
2
2 1 1
0%
20%
40%
60%
80%
100%
31-40 41-50 51-60 61-70 71-80 >80Age groups (years)
IDC Lobular c. Tubular c. Mucinous c. Papillary c.
FIGURE 3. Tumor histological types within age groups
2 2
4
12
31
1
20
1534 20 3
0%
20%
40%
60%
80%
100%
11-20 21-30 31-40 41-50 51-60 61-70 71-80 >80Age groups (years)
Benign Malignant
FIGURE 2. Rate of benign and malignant lesions within age groups

53Journal of Interdisciplinary Medicine 2020;5(2):48-55
sary to provide personalized suggestions such as screening from a younger age. Patients whose first- or second-degree relatives have been diagnosed with breast cancer have a twofold risk or higher, according to a systematic review.36 Similarly to other results,37 among our patients with malig-nant tumors, 15 (17.05%) had a positive family history, two of whom were under the age of 45.
Tumors are located most frequently in the UOQ across multiple populations, which is also our case (47.01%). Al-though tumor location is not an independent prognostic factor, central tumors are more difficult to evaluate mammo-graphically, and as a result, they may be discovered in more advanced stages.38 Other studies have discovered an increas-ing trend in mortality with increasing distance from the ax-illa, regardless of axillary lymph node invasion, concluding that survival is significantly better for UOQ tumours.39,40
Screening mammography can be very useful for de-tecting cancer in early stages; however, it has a major downside: overdiagnosis. Supplemental ultrasound breast screening can be used when breast density is high, but its specificity is low compared to mammography.41 Overdi-agnosis is defined as the discovery of breast lesions that would never cause symptoms or harms in the absence of screening.42 These represent 0–54% of all cases, according to a systematic review.43 Consequential overtreatment can be limited by adding the third step to the diagnostic pro-cess, represented by histopathological evaluation and pro-posing all suspicious lesions (BI-RADS 4 and 5 categories) for core-needle biopsy. In our study, malignancy rates, confirmed by histopathological examinations, were in the estimated range for each category, except BI-RADS 4a (0% vs. estimated 2–10%).
Most tumors (n = 73, 78.35%) were represented by IDC of no special type, with the highest frequency in all age cat-egories, with the exception of patients over 80 years, who were mostly diagnosed with the mucinous type. This sup-ports data from international literature, where the rate of IDC is estimated to 40–75%, and mucinous carcinoma is associated to elderly patients.44 Preoperative histopatho-logical examination is not only useful for avoiding unnec-essary treatment of benign tumors, but also for improving surgical results, including margin negativity, in malignant tumors.45
Once the need for treatment is confirmed, evaluation of prognostic factors is a key part of defining a personalized therapeutic strategy. Practitioners rely on the Nottingham combined histologic grade (Elston-Ellis modification of Scarff-Bloom-Richardson grading system) for malignancy stratification and decision making regarding treatment.46 The Nottingham combined histologic grade evaluates the amount of tubule formation, the extent of nuclear pleomor-phism, and the mitotic count. Tumor grade proportion is variable in the literature, but grade 2 tumors are the most frequent in the majority of studies.447–51 In our study, grade 2 tumors were observed in more than half of the cases.
Besides tumor grade, the molecular subtype of the tu-mor strongly influences survival.52–54 Breast cancer is het-erogeneous at the molecular level, with different patterns of gene expression leading to differences in behavior and prognosis. Due to time and cost constrains, a surrogate molecular breast cancer classification is used, based on im-munohistochemical assessment of biomarkers (ER, PR, HER2, and ki-67).18 Approximately 75% of breast cancers express estrogen and progesterone receptors, which indi-
3
56 5
1
1 125
2013
1
4 4 72
0%
20%
40%
60%
80%
100%
31-40 41-50 51-60 61-70 71-80 >80Age groups (years)
Grade 1 Grade 2 Grade 3
FIGURE 4. Tumor malignancy grades within age groups

54 Journal of Interdisciplinary Medicine 2020;5(2):48-55
cates responsiveness to hormonal therapy. In our study, 89.13% of lesions were ER-positive and 67.03% PR-posi-tive.46 Estrogen expression rate is based on the percentage of cells staining by immunohistochemistry, but in the clini-cal practice the response of low positive (1–10% staining) ER cancers is uncertain. The 2020 guideline of the Ameri-can Society of Clinical Oncology (ASCO)/CAP recom-mends reporting these cases in a new category, ER low positive.55 In order to predict the benefit of hormonal ther-apy, the Allred score combines both the percentage and intensity of staining.20 Luminal B-like subtype was domi-nant in this study, which means that most of our patients will need additional chemotherapy, compared to luminal A, where hormonal therapy is sufficient in most cases.46 The least favorable cases, HER2-positive and TNBC, were found predominantly in the older age groups; however, we have found no significant association between age and molecular subtype. Some studies have reached the same conclusion; at the same time, it is widely recognized in the literature that younger women present with more aggres-sive tumors.51,56
CoNCluSioNS
Most of the newly diagnosed breast cancers in our region are localized in the upper-outer quadrant, the 61–70 age group being most affected. At the time of discovery, these tumors are larger than the average size at discovery de-scribed in the literature, and they also show a positive cor-relation with age. The introduction of triple assessment to our routine was successful; however, it cannot compensate the lack of screening participation. Preoperative histologi-cal results suggest the BI-RADS risk stratification system’s reliability and appropriate use. Most tumors express both ER and PR, and these patients can benefit from adjuvant endocrine therapy.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES
1. Romania in Global Cancer Statistics 2018. Oncology Today. Available
at: https://www.medichub.ro/reviste/oncolog-hematolog-ro/romania-in-
global-cancer-statistics-2018-id-2019-cmsid-68.
2. Tereanu C, Baili P, Berrino F, et al. Recent trends of cancer mortality in
Romanian adults: Mortality is still increasing, although young adults do
better than the middle-aged and elderly population. Eur J Cancer Prev.
2013;22:199-209.
3. Gøtzsche PC, Hartling OJ, Nielsen M, Brodersen J, Jørgensen KJ. Breast
screening: The facts - Or maybe not. BMJ. 2009;338:446-448.
4. Cardoso F, Cataliotti L, Costa A, et al. European Breast Cancer Conference
manifesto on breast centres/units. Eur J Cancer. 2017;72:244-250.
5. Travasso C. Panel issues advice on early detection of oral, breast, and
cervical cancers in India. BMJ. 2015;351:h3807.
6. Britton P, Sinnatamby R. Investigation of suspected breast cancer. Br Med
J. 2007;335:347-348. 7. John M. Eisenberg Center for Clinical Decisions and Communications
Science. Core-Needle Biopsy for Breast Abnormalities. In: Comparative Effectiveness Review Summary Guides for Clinicians. 2007. Available at: http://www.ncbi.nlm.nih.gov/pubmed/27336126.
8. National Guideline Alliance (UK). Early and Locally Advanced Breast Cancer: Diagnosis and Management.2018. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519155/.
9. Jeibouei S, Akbari ME, Kalbasi A, et al. Personalized medicine in breast cancer : pharmacogenomics approaches. Pharmgenomics Pers Med. 2019;12:59-73.
10. Chan CWH, Law BMH, So WKW, Chow KM, Waye MMY. Novel Strategies on Personalized Medicine for Breast Cancer Treatment: An Update. Int J Mol Sci. 2017;18:2324.
11. Balic M, Thomssen C, Würstlein R, Gnant M, Harbeck N. St. Gallen/Vienna 2019: A brief summary of the consensus discussion on the optimal primary breast cancer treatment. Breast Care. 2019;14:103-110.
12. Morigi C. Tailored Treatments for Patients With Early Breast Cancer. ecancer. 2017;11:1-12.
13. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver M. WHO Classification of Tumours of the Breast. Fourth Edition, Geneva, Switzerland: WHO Press.; 2012.
14. Who Classification of Tumours Editorial Board. Breast Tumours. Lyon (France) Internation Agency for Research on Cancer; 2019. (WHO Classification of Tumours Series, 5th Ed.; Vol. 2).
15. Hoon Tan P, Ellis I, Allison K, et al. The 2019 WHO classification of tumours of the breast. Histopathology. 2020. [Ahead of print]
16. Fitzgibbons PL, Connolly JL, Edgerton M, MD, Simpson MR. Protocol for the examination of specimens From patients with invasive carcinoma of the breast. Arch Pathol Lab Med. 2020. [Ahead of print]
17. Untch M, Gerber B, Harbeck N, et al. 13th St. Gallen international breast cancer conference 2013: Primary therapy of early breast cancer evidence, controversies, consensus - Opinion of a German team of experts (Zurich 2013). Breast Care. 2013;8:221-229.
18. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30:1194-1220.
19. Jorns JM. Challenges in routine estrogen receptor, progesterone receptor, and HER2/neu evaluation. Arch Pathol Lab Med. 2019;143:1444-1449.
20. Fitzgibbons PL, Bartley AN, Connolly JL. Template for reporting results of biomarker testing of specimens from patients with carcinoma of the breast. Arch Pathol Lab Med. 2020. [Ahead of print]
21. Bucure C. Luna Internațională de C onstientizare d espre Cancerul de San ( LICCS) 1-31 Octombrie 2019 Analiza de Situație. 2019:1-16. Available at: http://insp.gov.ro/sites/cnepss/wp-content/uploads/2019/10/Analiza-de-situatie.pdf.
22. Pant K, Dutta U. Understanding and management of male breast cancer: A critical review. Med Oncol. 2008;25:294-298.
23. Schünemann HJ, Lerda D, Quinn C, et al. Breast cancer screening and diagnosis: A synopsis of the european breast guidelines. Ann Intern Med. 2020;172:46-56.
24. Güth U, Huang DJ, Huber M, et al. Tumor size and detection in breast cancer: Self-examination and clinical breast examination are at their limit. Cancer Detect Prev. 2008;32:224-228.
25. Shaevitch D, Taghipour S, Miller A, Montgomery N, Harvey B. Tumor size distribution of invasive breast cancers and the sensitivity of screening methods in the Canadian National Breast Screening Study. J Cancer Res Ther. 2017;13:562-569.
26. European Comission E. Breast Cancer and Cervical Cancer Screenings.; 2017. Available at: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20200109-1.
27. Carter CL, Allen C, Henson DE. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer. 1989;63:181-187.
28. Orang E, Marzony ET, Afsharfard A. Predictive role of tumor size in breast cancer with axillary lymph node involvement - can size of primary tumor be used to omit an unnecessary axillary lymph node dissection? Asian Pacific J Cancer Prev. 2013;14:717-722.
29. Michaelson JS, Silverstein M, Sgroi D, et al. The Effect of Tumor Size and Lymph Node Status on Breast Carcinoma Lethality. Cancer. 2003;98:2133-2143.

55Journal of Interdisciplinary Medicine 2020;5(2):48-55
30. Narod SA. Tumour size predicts long-term survival among women with lymph node-positive breast cancer. Curr Oncol Vol. 2012;19:249‐253.
31. Laura S, Coombs NJ, Ung O, Boyages J. Tumour size as a predictor of axillary node metastases in patients with breast cancer. ANZ J Surg. 2006;76:1002-1006.
32. Sopik V, Narod SA. The relationship between tumour size, nodal status and distant metastases: on the origins of breast cancer. Breast Cancer Res Treat. 2018;170:647-656.
33. Rambau P, Chalya P, Manyama M, Jackson K. Pathological features of Breast Cancer seen in Northwestern Tanzania: A nine years retrospective study. BMC Res Notes. 2011;4:214.
34. Bonnier P, Romain S, Charpin C, et al. Age as a prognostic factor in breast cancer: Relationship to pathologic and biologic features. Int J Cancer. 1995;62:138-144.
35. Alieldin NH, Abo-Elazm OM, Bilal D, et al. Age at diagnosis in women with non-metastatic breast cancer: Is it related to prognosis? J Egypt Natl Canc Inst. 2014;26:23-30.
36. Nelson H, Zakher B, Cantor A, et al. Risk Factors for Breast Cancer for Women Aged 40 to 49 Years A Systematic Review and Meta-analysis. Ann Intern Med. 2012;156:635-648.
37. Brewer HR, Jones ME, Schoemaker MJ, Ashworth A, Swerdlow AJ. Family history and risk of breast cancer: an analysis accounting for family structure. Breast Cancer Res Treat. 2017;165:193-200.
38. Rummel S, Hueman MT, Costantino N, Shriver CD, Ellsworth RE. Tumour location within the breast: Does tumour site have prognostic ability? Ecancermedicalscience. 2015;9:1-10.
39. Kroman N, Wohlfahrt J, Mouridsen HT, Melbye M. Influence of tumor location on breast cancer prognosis. Int J Cancer. 2003;105:542-545.
40. Sohn VY, Arthurs ZM, Sebesta JA, Brown TA. Primary tumor location impacts breast cancer survival. Am J Surg. 2008;195:641-644.
41. Geisel J, Raghu M, Hooley R. The Role of Ultrasound in Breast Cancer Screening: The Case for and Against Ultrasound. Semin Ultrasound, CT MRI. 2018;39:25-34.
42. Jacklyn G, McGeechan K, Houssami N, Bell K, Glasziou PP, Barratt A. Overdiagnosis due to screening mammography for women aged 40 years and over. Cochrane Database Syst Rev. 2018;2018:CD013076.
43. HD N, A C, L H, et al. Screening for Breast Cancer: A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation. In: Evidence Syntheses. Vol 124. ; 2016. Available at: http://europepmc.org/abstract/med/26889531.
44. Makki J. Diversity of breast carcinoma: Histological subtypes and clinical
relevance. Clin Med Insights Pathol. 2015;8:23-31.
45. Klimberg VS., Rivere A. Ultrasound image-guided core biopsy of the
breast. Chinese Clin Oncol. 2016;5:1-9.
46. Julia Y.S. Tsang P and GMT. Molecular Classification of Breast Cancer. Adv
Anat Pathol. 2020;27(1):27-35.
47. Hamza AA, Idris SA, Al-haj MB, Mohammed AA. Prognostication of breast
cancer using Nottingham Prognostic Index in Sudanese patients. 2014;2:1-5.
48. Thomas JSJ, Kerr GR, Jack WJL, et al. Histological grading of invasive breast
carcinoma - A simplification of existing methods in a large conservation
series with long-term follow-up. Histopathology. 2009;55:724-731.
49. Megha T, Neri A, Malagnino V, et al. Traditional and new prognosticators
in breast cancer: Nottingham index, Mib-1 and estrogen receptor signaling
remain the best predictors of relapse and survival in a series of 289 cases.
Cancer Biol Ther. 2010;9:266-273.
50. Oluogun WA, Adedokun KA, Oyenike MA, Adeyeba OA. Histological
classification, grading, staging, and prognostic indexing of female breast
cancer in an African population: A 10-year retrospective study. Int J Health
Sci (Qassim). 2019;13:3-9.
51. Salhia B, Tapia C, Ishak EA, et al. Molecular subtype analysis determines
the association of advanced breast cancer in Egypt with favorable biology.
BMC Womens Health. 2011;11:44.
52. Kermani T, Kermani I, Faham Z, Dolatkhah R. Ki-67 status in patients with
primary breast cancer and its relationship with other prognostic factors.
Biomed Res Ther. 2019;6(2 SE-Research articles).
53. Kasangian AA, Gherardi G, Biagioli E, et al. The prognostic role of tumor
size in early breast cancer in the era of molecular biology. PLoS One.
2017;12:e0189127.
54. Giuliano AE, Connolly JL, Edge SB, et al. Breast Cancer-Major changes in
the American Joint Committee on Cancer eighth edition cancer staging
manual. CA Cancer J Clin. 2017;67:290-303.
55. Allison KH, Hammond MEH, Dowsett M, et al. Estrogen and Progesterone
Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J Clin
Oncol. 2020;38:1346-1366.
56. Kuijer A, King TA. Age, molecular subtypes and local therapy decision-
making. Breast. 2017;34:S70-S77.

Journal of Interdisciplinary Medicine 2020;5(2):56-63
CORRESPONDENCE
Daniela Sala Str. Nicolae Grigorescu nr. 15, ap. 11540095 Targu Mures, RomaniaPhone number: +40 726 167 557E-mail: [email protected]
ARTICLE HISTORY
Received: April 19, 2020Accepted: May 20, 2020
Proper Surgical Treatment of Small and Medium Size Umbilical Hernias. A Single Surgeon ExperienceEtele Élthes1,2, Daniela Sala1,2, Radu Mircea Neagoe1,2, János Székely1, Márton Dénes1,2
1 “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania2 2nd Department of Surgery, Emergency County Clinical Hospital, Targu Mureş, Romania
oriGiNal rESEarCH PLASTIC SURGERY // GENERAL SURGERY
DOI: 10.2478/jim-2020-0007
ABSTRACT
Introduction: Minimally invasive surgical procedures have become routine interventions nowa-days and represent an effective therapeutic option even for small umbilical hernias, providing favorable postoperative and aesthetic results. Aim of study: To determine the most appropriate minimally invasive treatment option for small and medium size umbilical hernias. Materials and methods: We conducted a prospective study on 50 patients with small or medium umbilical hernia (<4 cm). All patients benefited of minimal invasive surgery with mesh implantation. De-pending on the surgical procedure, two major groups were defined: group A – patients with open surgical approach (n = 24) and group B – patients undergoing laparoscopic surgery (n = 26). Clinical, surgical, postoperative, and follow-up data were analyzed. Results: Mesh re-placement via open approach through the umbilicus was associated with significantly reduced surgical time (p = 0.0359), administration of painkillers (p = 0.0461), and use of anticoagulants (p = 0.0404). Hospital stays (p = 0.0001) and costs (p = 0.0005) were also significantly lower in this group. After 6 months of follow-up, no recurrence was observed, and no significant differ-ences were detected regarding postoperative pain and the patients’ professional reintegration. Patient satisfaction regarding postoperative scar was superior in the open group. Conclusion: The present study indicates that the ventral patch technique is a safe and effective method for the treatment of small and medium size umbilical hernias.
Keywords: small umbilical hernia, ventral patch, minimally invasive, esthetics
Etele Élthes • Str. Păcii nr. 68B, ap.14, 540118 Targu Mures, Romania. Tel: +40 746 556 355, E-mail: [email protected]
Radu Mircea Neagoe • Str. Gheorghe Marinescu nr. 38, 540136 Targu Mures, Romania. Tel: +40 265 215 551, E-mail: [email protected]
János Székely • Str. Gheorghe Marinescu nr. 50, 540136 Targu Mures, Romania. Tel: +40 372 653 100, E-mail: [email protected]
Márton Dénes • Aleea Carpați nr. 29, Ap. 65, 540336 Targu Mures, Romania. Tel: +40 744 509 214, E-mail: [email protected]
iNtroduCtioN
Abdominal wall hernias are quite common surgical conditions affecting all ages and both genders. A hernia represents an abnormal protrusion of a peritoneum-lined sac through the muscular covering of the abdomen. The umbilicus is one of the weak points of the abdominal wall and a relatively common site for her-niations. Nowadays, umbilical hernias still represent an important medical issue, affecting a significant part of the population. Because of the increased recurrence rates following suture repair, closure of the abdominal wall defect using a synthetic prosthesis has been shown to be superior to other surgical techniques, even for

57Journal of Interdisciplinary Medicine 2020;5(2):56-63
small size hernias. The outcome of hernia repair may also be affected by the surgical approach. Minimally invasive tech-niques for mesh placement have been shown to reduce post-operative complications and may offer a satisfying esthetic result as well. Synthetic patches are particularly suitable for small hernias because they require a smaller dissection; how-ever, it is still unclear whether the results of this procedure are at least equal to other minimally invasive techniques.1–3
The aim of the study was to assess the efficacy of two minimally invasive (open versus laparoscopic) surgical op-tions in treating small and medium size umbilical hernias.
matErialS aNd mEtHodS
Patient selection
Between January 1, 2018 and June 30, 2019 we conducted a prospective study at the 2nd Department of General Sur-gery of Mureș County Emergency Clinical Hospital on 50 patients diagnosed with small or midsized umbilical herni-as. All patients underwent surgical treatment and benefit-ed of minimally invasive care of the abdominal wall defect.
The laparoscopic approach was performed using the standard three-trocar method, and reinforcement of the abdominal wall was carried out with composite surgical mesh fastened with surgical tacks. For the open surgical procedure, a single microincision was performed at the level of the umbilicus. After careful dissection, the parietal defect was identified, and the hernia content was reintro-duced in the peritoneal cavity. Succeeding cautious exami-nation of possible adhesions around the abdominal wall defect, a ventral patch-type synthetic mesh (Figure 1) was introduced through the umbilicus and fastened with two separate sutures. The abdominal wall defect and the skin incision were closed with separate sutures.
The surgical procedures were performed by a single surgeon, with competency and experience in minimally invasive hernioplasty. Follow-up for these patients was per-formed at 6 months after surgical treatment. Patients requir-ing hernia repair in emergency conditions, those with in-creased size umbilical defects, advanced stages of obesity, or undergoing other surgical treatment options than minimally invasive techniques were excluded from the study.
Subdivision of patients and collected data
Based on the surgical intervention performed, the patients were divided into two groups: 1) a study group (SG), with open approach, including 24 patients who underwent open surgical treatment of the umbilical hernia; 2) a con-trol group (CG), with laparoscopic approach, including 26 patients who benefited of reinforcement of the abdominal wall with composite surgical mesh via laparoscopic repair. All patients were carefully questioned and examined. At the same time, data was gathered from medical charts and operatory protocols.
The first subanalysis of the study compared the two surgical procedures analyzing clinical, surgical, and post-operative data. Clinical characteristics included the pa-tients’ gender, age, weight, and size of umbilical defect. For interpretation of age, three subgroups were defined: young adults (<44 years), middle-aged adults (45–69 years), and elderly adults (>70 years). For obesity assess-ment, the internationally applied body mass index (BMI) was calculated. For categorization of the abdominal wall defect, we used the classification proposed by the Euro-pean Hernia Society: hernias with diameters <2 cm were defined as small sized, and hernias with diameters between 2–4 cm were defined as medium sized. Regarding surgi-cal and postoperative data, the following variables were examined: number of abdominal incisions, mesh fixation method, duration of surgical intervention, mobilization after surgery, postoperative medication (painkillers, an-ticoagulants, and antibiotics), length of hospital stay, and hospitalization costs. For easier assessment of surgical time, short surgical interventions (<60 minutes) and pro-longed operations (>60 minutes) were defined. The early mobilization subgroup contained patients who sustained physical effort (walking) on the day of surgical interven-tion, while those with delayed mobilization performed physical activity later during the postoperative recovery. Regarding the postoperative medication, three subgroups were distinguished, based on the length of medicine intake (without treatment, treatment only on the day of surgical intervention, and more than one-day treatment).
FIGURE 1. Ventral patch for hernia repair

58 Journal of Interdisciplinary Medicine 2020;5(2):56-63
During the second subanalysis we mainly focused on statistical analysis of data gathered throughout patient follow-up. These aspects included evaluation of postop-erative pain, the patients’ professional reintegration, and assessment of recurrence rate. For the evaluation of post-operative pain, the following numerical rating scale was applied: 0 = no pain, 1–3 = reduced pain, 4–6 = moderate pain, 7–9 = significant pain, 10 = worst pain ever. Profes-sional reintegration was measured in time (weeks) spent from surgical intervention until return to work.
Esthetic results were assessed in the third subanalysis, through which the following aspects were analyzed: num-ber of abdominal incisions, wound closing methods, and the patients’ satisfaction on wound healing. Postoperative scar healing results were analyzed with the Vancouver Scar Scale (VSS), which is widely used in clinical practice and research.
Statistical analysis
The collected information was processed using Microsoft Excel. The statistical analysis of the database was per-formed using GraphPad InStat software (GraphPad Soft-ware, Inc., San Diego, USA). Quantitative variables were presented by mean and median, while qualitative and cat-egorical variables were expressed both as integer and per-centage values. A normality test was applied for all variable groups in order to determine the distribution of values. Furthermore, for the quantitative statistical analysis, Stu-
dent’s t-test was applied for groups with Gaussian distri-bution of values, while the Mann-Whitney nonparametric test was used for groups with non-Gaussian distribution. The level of statistical significance for the present research was set at a p value of 0.05, while the confidence interval was 95% for all calculated parameters.
rESultS
Basic comparison of the surgical procedures
The results of the first subanalysis comparing patients un-dergoing the two studied procedures is presented in Table 1, which indicates that male patients were present in a high-er proportion in both of the studied groups (SG – 79.17%, CG – 65.38%), but without statistically significant differ-ence. Analysis of age indicated a majority of middle-aged adults (n = 26), followed by young adults (n = 20) and elder-ly patients (n = 4). However, age-related data did not show any significant differences between the groups. Regarding obesity, the majority of patients (SG – 70.83%, CG – 50%) had a BMI in the normal range; overweight patients were present in a higher proportion in the laparoscopic group, while obese patients were present in just a small percent-age. Neither of these data showed significant differences during statistical analysis. The last investigated clinical as-pect was the size of the parietal defect. Abdominal wall de-fects smaller than 2 cm benefited mainly of classic approach (SG – 54.17%, p = 0.0938), while umbilical hernias with
TABLE 1. Clinical characteristics of the study population
Study groupOpen approach
n = 24 (%)
Control groupLaparoscopic approach
n = 26 (%)
p value
Gender
Male 19 (79.17) 17 (65.38) 0.3
Female 5 (20.83) 9 (34.62) 0.3
Age (years)
25–44 11 (45.83) 9 (34.61) 0.4
45–69 10 (41.67) 16 (61.54) 0.2
>70 3 (12.5) 1 (3.85) 0.5
BMI
Normal (18.5–24.9) 17 (70.83) 13 (50) 0.2
Overweight (25–29.9) 7 (29.17) 11 (42.31) 0.4
Obese (30–34.9) 0 (0) 2 (7.69) –
Severely obese (35–39.9) 0 (0) 0 (0) –
Morbidly obese (40+) 0 (0) 0 (0) –
Size of hernia defect (cm)
<2 cm 13 (54.17) 7 (26.92) 0.09
2–4 cm 11 (45.83) 19 (73.08)

59Journal of Interdisciplinary Medicine 2020;5(2):56-63
diameters between 2–4 cm were predominantly treated via laparoscopic approach (CG – 73.08%, p = 0.0938).
Surgical and postoperative details are presented in Table 2. Patients who benefited of abdominal reinforce-ment with ventral patch composite synthetic mesh need-ed a single abdominal microincision, while patients from the CG had at least three abdominal microincisions. For wound closure during classic surgical intervention, exclu-sively simple interrupted sutures were utilized, while in case of laparoscopic surgery, significantly more patients benefited of intradermal suture (p = 0.0001). In case of the ventral patch method, mesh fixation happened via separate sutures, while in case laparoscopic hernioplasty, metallic or absorbable tacks were used in order to fix the
composite surgical mesh. No significant differences were observed during the analysis of these data. Regarding the duration of surgical intervention, patients from the SG had a significantly shorter operation compared to patients who benefited of laparoscopic intervention (p = 0.0359). Early postoperative mobilization was encouraged for all patients, and statistical analysis of these characteristics did not indicate any significant difference for neither of the studied groups.
Postoperative medication represented an important part of our investigation, and we noticed that patients with clas-sic hernioplasty benefited of significantly less painkillers and anticoagulant therapy. There were no statistically significant differences between the study groups in terms of antibiotic
TABLE 2. Surgical and postoperative data in the study population
Study groupOpen approach
n = 24 (%)
Control groupLaparoscopic approach
n = 26 (%)
p value
No. of abdominal incisions
One 24 (100) 0 (0) –
Three 0 (0) 26 (100) –
Wound closing technique
Simple interrupted suture 24 (100) 8 (30.77) 0.0001
Intradermal suture 0 (0) 18 (69.23)
Mesh fixation method
Separate sutures 24 (100) 0 (0) –
Tacks 0 (0) 26 (100) –
Duration of surgery (min)
Average 45 minutes 70 minutes –
Short (<60 min) 22 (91.67) 15 (57.69) 0.03
Prolonged (>60 min) 2 (8.33) 11 (42.31)
Mobilization
Early (Day 0) 23 (95.83) 22 (84.62) 0.4
Delayed (Day 1) 1 (4.17) 4 (15.38)
Use of painkillers (days)
Average 1.33 days 2.80 days
Without treatment 4 (16.67) 0 (0) 0.04
Only one day of treatment 9 (37.5) 1 (3.85) 0.004
More than one day of treatment 11 (45.83) 25 (96.15) 0.0001
Use of anticoagulant (days)
Average 0.95 2.34 –
Without treatment 13 (54.17) 6 (23.08) 0.04
One day of treatment 0 (0) 0 (0) –
More than one day of treatment 11 (45.83) 20 (76.92) 0.04
Use of antibiotic (days)
Average 0.72 0.92 –
Without treatment 0 (0) 5 (19.23) 0.05
One day of treatment 21 (87.5) 18 (69.23) 0.1
More than one day of treatment 3 (12.5) 3 (11.54) 1.0
Average length of hospital stay (days) 2.65 4.19 0.0001
Average hospitalization costs (EUR) 718.23 1185.08 0.0005

60 Journal of Interdisciplinary Medicine 2020;5(2):56-63
use. On the other hand, the length of hospital stay seemed to be significantly longer for patients with laparoscopic her-nioplasty (p = 0.0001), while hospitalization costs were sig-nificantly higher in patients from the CG (p = 0.0005).
Follow-up
The second subanalysis in our study focused on patient follow-up. Figure 2 presents the distribution of postop-erative pain among patients, which showed no significant differences between the two studied groups. The profes-sional reintegration of the patients is illustrated in Figure 3, where a slightly difference can be observed between the two studied groups. Ventral patch-type hernioplasty
seemed to assure faster return to work, but with no statisti-cal significance (p = 0.0944). As for hernia recurrence, no reappearance of umbilical defects was registered in neither group during the six months of follow-up.
Esthetic issues after minimally invasive hernioplasty
The open surgical approach required a single incision, while in order to perform laparoscopic hernioplasty, the patients suffered at least three incisions in the abdominal wall. Regarding wound closing technique, the majority of patients from the CG benefited of intradermal suture. Fur-thermore, VSS assessment indicated a significantly higher
17
43
0 0
13
6 6
10
0
2
4
6
8
10
12
14
16
18
Without Reduced Moderate Significant Worst everSG - open approach CG - laparoscopic approach
FIGURE 2. Distribution of postoperative pain
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Day
s
Patients
SG - open approach CG - laparoscopic approach
FIGURE 3. The professional reintegration of patients

61Journal of Interdisciplinary Medicine 2020;5(2):56-63
index for patients from the CG (mean = 4 points), while ventral patch-type hernioplasty seemed to yield higher sat-isfaction among patients (mean = 2.5 points, p = 0.0109).
diSCuSSioN
Primary considerations
There is no consensus on the ideal technique for repair-ing small and medium size umbilical hernias in adults, both presented surgical procedures representing current op-tions for minimally invasive hernioplasty. The laparoscopic repair of parietal defects has been widely applied, and sev-eral studies have confirmed the procedure’s benefits; the patch-type surgical mesh represents a new open-technique solution for small and medium size umbilical hernias, with at least similar efficacy as other treatment options.4,5
Choosing the right surgical intervention is not always easy, and the surgical decision should be guided by the general condition of the patients, as well as the clinical considerations. Regarding age and gender, the current lit-erature is vague.6 However, in our experience, advanced age associated with comorbidities requires cautious deci-sion and a careful analysis of the risk-benefit ratio.
Obesity is a well-known risk factor for abdominal wall defects, but an excessive amount of adipose tissue can also cause difficulties during surgical interventions.7 Therefore, patient selection had an important role in our study. Bono-mo et al. also highlighted the importance of patient selec-tion during minimally invasive surgery.8 In many cases, the current literature recommends laparoscopic treatment of umbilical hernia in obese patients; contrariwise, Was-senber et al., in a single center experience, highlighted the benefits of the ventral patch technique.9,10
The size of the parietal defect should also be considered when opting for the right surgical technique. Due to the technical difficulty of retro-rectus and preperitoneal dis-section for these small abdominal wall defects, effective al-ternative approaches seem to be the use of a self-expanding mesh device introduced into the peritoneal cavity through a single microincision (open ventral patch method), or laparoscopic abdominal wall reinforcement. Results simi-lar to ours can be found in the literature.11,12
Regarding mesh fixation, the two surgical procedures are completely different. During open surgical interven-tion, the composite patch is fastened with separate sutures in a few key points, while laparoscopic surgery requires surgical tacks in order to secure the composite mesh. Fixa-tion of the synthetic patch seemed more easy to perform, a fact underlined by other researchers as well.13
There is a strong relationship between mesh fixation methods and surgical time, since laying and fastening the composite surgical mesh during laparoscopic hernioplasty requires additional minutes. In a multicenter prospective study, Berrevoet et al. assessed surgeon satisfaction related to ease of mesh use in 95% of surgeries and reported an average surgical time of 36.2 minutes, favoring the open ventral patch technique.14
Both surgical procedures represent minimally invasive techniques, therefore early mobilization of the patients is characteristic for these type of interventions. Vychnevs-kaia et al. and Vorst et al. highlighted the benefits of mini-mally invasive procedures.15,16 The shorter operation time and the integrity of the abdominal wall allow patients to perform physical effort on the day of surgical intervention.
Medication after surgery is essential in avoiding serious complications and granting comfort in the postoperative period. In the present study, similar medication has been utilized for both of the studied groups, with slightly better results for patients from the open group regarding painkill-ers and anticoagulant therapy. As for antibiotic use, no dif-ferences worth mentioning were registered. The majority of patients benefited of prophylactic, single-dose antibiot-ic treatment prior to surgical intervention. Prolonged an-tibiotic intake was registered only in case of patients with high BMI who are more prone to wound complications. In a randomized controlled, multicenter trial, Ponten et al. mentioned similar considerations regarding postoperative medication.17
Both surgical interventions were generally associated with a short hospital stay. The minimally invasive approach assured patients early hospital discharge after a short post-operative recovery, and the ventral patch technique seems to ensure an even more reduced hospitalization. For in-stance, Zarmpis et al. reported an average hospital stay of 4 days.18
In the modern era of medical care, the financial aspects of therapeutic methods cannot be ignored. According to Roumm et al., the costs of laparoscopic surgery are fre-quently high.19 The present article identified an average hospitalization cost of 718.23 euro per patient with the composite ventral patch technique, while the mean cost of laparoscopic surgery was 1.65 time higher.
Follow-up
Postoperative pain represented the first aspect followed during the 6-month follow-up. Most of the time, minimally invasive surgical procedures are associated with reduced perioperative pain, a fact also confirmed during the pres-

62 Journal of Interdisciplinary Medicine 2020;5(2):56-63
ent study, both surgical methods being linked with a low pain index during postoperative recovery.
In general, less invasive surgical treatments ensure an early possibility for work resumption. Based on our expe-rience, patients who benefited of the open approach and reinforcement of the abdominal wall defect with the ven-tral patch technique presented a slightly faster professional reintegration. However, Agca et al. found that this type of surgical intervention does not influence postoperative pain and early return to work significantly.20
During the follow-up period, no recurrence was regis-tered for either of the studied groups. However, we must underline that the follow-up period was relatively short. Further studies with longer follow-up periods are needed to draw conclusions. Venclauskas et al. reported that lapa-roscopic surgery for umbilical hernia repair can be safely applied with favorable long-term outcomes regarding re-currence.21 As for open repair with synthetic patch implan-tation, Ambe et al. reported a low recurrence rate for this type of intervention.22
Esthetics after umbilical hernioplasty
Nowadays, esthetic results are an important issue in gener-al surgery. During our research, the following aspects were followed for defining an esthetic result: the number of ab-dominal incisions, wound closure techniques, and patient satisfaction regarding scar healing.
Regarding the number of incisions, the open technique with ventral patch implantation offers a more satisfying re-sult, with a single microincision at the level of umbilicus (Figure 4), compared to laparoscopic hernioplasty, which requires at least three abdominal incisions.
As far as wound closing methods are concerned, the ma-jority of patients from the laparoscopic group benefited of intradermal closure of the incisions. Being a more delicate
area, we exclusively used separate surgical sutures for clos-ing umbilical wounds.
Patient satisfaction regarding scar healing was estimat-ed using the Vancouver Scar Scale, our results showing a lower VSS index during follow-up for the open hernioplas-ty group. In 2019, Berrevoet et al. published a large mul-ticenter prospective study about the ventral patch tech-nique, with results similar to our study. They concluded that open hernioplasty with ventral patch implantation offers satisfying results.23
limitatioNS of tHE Study
Our study has several limitations. Firstly, the fact that no recurrence was observed may be related to the relatively short follow-up period of 6 months; a longer follow-up period may identify several long-term complications. Secondly, the sample size was relatively small, and sta-tistical significance had not been reached in several parts of the study. With a larger sample size, probably some of the statistical analysis would have reached significant thresholds.
CoNCluSioN
Placement of a synthetic patch through a minimally in-vasive open approach as treatment for umbilical defects is associated with low recurrence rate, low postoperative pain, lower hospitalization costs, and high esthetic satis-faction. These confirm that hernioplasty with the ventral patch technique via open procedure is an effective option for small and medium size hernia repair.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES
1. Kulacogiu H. Current options in umbilical hernia repair in adult patients. Ulus Cerrahi Derg. 2015;31:157-161.
2. Kaufmann R, Halm JA, Eker HH, et al. Mesh Versus Suture Repair of Umbilical Hernia in Adults: A Randomised, Double-Blind, Controlled, Multicentre Trial. Lancet. 2018;391:860-869.
3. Ahmed Alenazi A, Alsharif MM, Hussain MA, et al. Prevalence, risk factors and character of abdominal hernia in Arar City, Northern Saudi Arabia in 2017. Electron Physician. 2017;9:4806-4811.
4. Gonzalez R, Mason E, Duncan T, Wilson R, Ramshaw BJ. Laparoscopic versus open umbilical hernia repair. JSLS. 2003;7:323-328.
5. Wang D, Chen J, Chen Y, Han Y, Zhang H. Prospective analysis of epigastric, umbilical and small incisional hernia repair using the modified kugel oval patch. Am Surg. 2018;84:305-308.
6. Saber AA, Elgamal MH, Manci TB, Norman E, Boros MJ. Advanced age: is it an indication or contraindication for laparoscopic ventral hernia repair? JSLS. 2008;12:46-50.
FIGURE 4. Postoperative esthetic results with the ventral patch
technique

63Journal of Interdisciplinary Medicine 2020;5(2):56-63
7. Giordano SA, Garvey PB, Baumann DP, Liu J, Butler CE. The impact of body mass index on abdominal wall reconstruction outcomes: a comparative study. Plast Reconstr Surg. 2017;139:1234-1244.
8. Bonomo LD, Giaccone M, Caltagirone A, et al. Patient selection criteria for an effective laparoscopic intraperitoneal ventral hernia repair in day surgery. Updates Surg. 2019;71:549-553.
9. Colon MJ, Kitamura R, Telem DA, Nguyen S, Divino CM. Laparoscopic umbilical hernia repair is the preferred approach in obese patients. Am J Surg. 2013;205: 231-236.
10. Wassenberg D, Zarmpis N, Seip N, Ambe PC. Closure of small and medium size umbilical hernias with the proceed ventral patch in obese patients: a single center experience. Springerplus. 2014;3:686.
11. Kulacoglu H. Current options in umbilical hernia repair in adult patients. Ulus Cerrahi Derg. 2015;31:157-161.
12. Salati SA, Al Kadi A. Umbilical hernia repair with proceed ventral patch. Pol Przegl Chir. 2014;86:350-352.
13. Tollens T, Struyve D, Aelvoet C, Vanrijkel JP. Introducing the proceed ventral patch as a new device in surgical management of umbilical and small ventral hernias: preliminary results. Surg Technol Int. 2010;19: 99-103.
14. Berrevoet F, Doerhoff C, Muysoms F, et al. A multicenter prospective study of patient undergoing open ventral hernia repair with intraperitoneal positioning using the monofilament polyester composite ventral patch: interim results of the PANACEA study. Med Devices (Auckl). 2017;10:81-88.
15. Vychnevskaia K, Mucci-Hennekinne S, Casa C, et al. Intraperitoneal mesh repair of small ventral abdominal wall hernias with a Ventralex hernia patch. Dig Surg. 2010;27:433-435.
16. Vorst AL, Kaoutzanis C, Carbonell AM, Franz MG. Evolution and advances in laparoscopic ventral and incisional hernia repair. World J Gastrointest Surg. 2015;7:293-305.
17. Ponten JEH, Leenders BJM, Leclercq WKG, et al. Mesh versus patch repair for epigastric and umbilical hernia (MORPHEUS Trial); one-year results of a randomized controlled trial. World J Surg. 2018;42:1312-1320.
18. Zarmpis N, Wassenberg D, Ambe PC. Repair of small and medium size umbilical hernias with the proceed ventral patch in the preperitoneal position. Am Surg. 2015;81:1144-1148.
19. Roumm AR, Pizzi L, Goldfarb NI, Cohn H. Minimally invasive: minimally reimbursed? An examination of six laparoscopic surgical procedures. Surg Innov. 2005;12:261-287.
20. Agca B, Iscan Y. Comparison of intraperitoneal ventralex st patch versus onlay mesh repair in small and medium primer umbilical hernia. International Journal of Abdominal Wall and Hernia Surgery. 2019;2:1-6.
21. Venclauskas L, Jokubauskas M, Zilinskas J, Zviniene K, Kiudelis M. Long-term follow-up results of umbilical hernia repair. Wideochir Inne Tech Maloinwazyjne. 2017;12:350-356.
22. Ambe P, Meyer A, Kohler L. Repair of small and medium size ventral hernias with a proceed ventral patch: a single center retrospective analysis. Surg Today. 2013;43:381-385.
23. Berrevoet F, Doerhoff C, Muysoms F, et al. Open ventral hernia repair with a composite ventral patch – final results of a multicenter prospective study. BMC Surg. 2019;19:93.

Journal of Interdisciplinary Medicine 2020;5(2):64-70
CORRESPONDENCE
Szilamér KorodiStr. Doctor Dénes László nr. 2530173 Miercurea Ciuc, RomaniaTel: +40 266 324 193E-mail: [email protected]
ARTICLE HISTORY
Received: April 4, 2020Accepted: May 18, 2020
Epicardial Fat Volume as a New Imaging-Based Feature Associated with Risk of Recurrence after Pulmonary Veins Ablation in Atrial FibrillationEmanuel Blîndu1,2, Szilamér Korodi3,4, Lehel Bordi1,2,3, István Kovács1,2,3, Imre Benedek1,2,3
¹ Center of Advanced Research in Multimodality Cardiac Imaging, Cardio Med Medical Center, Targu Mures, Romania2 Clinic of Cardiology, Emergency Clinical County Hospital, Targu Mures, Romania3 “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania4 Clinic of Cardiology, Emergency County Hospital, Miercurea Ciuc, Romania
oriGiNal rESEarCH CARDIOLOGY // IMAGING
DOI: 10.2478/jim-2020-0012
ABSTRACT
Background: Atrial fibrillation (AF), a common arrhythmia in clinical practice, is associated with
a high rate of complications and an increased risk for thromboembolic events. Pulmonary vein
ablation is a new therapeutic option to cure AF; however, it remains associated with a high rate
of recurrence. In this study we aimed to identify the clinical characteristics and imaging-based
features that may predict the risk of recurrence after pulmonary veins ablation in atrial fibril-
lation. Materials and method: Twenty-four patients with paroxysmal and persistent AF, who
underwent radiofrequency catheter ablation and a 12-month follow-up were included in the
study. Group 1 included 8 patients with AF recurrence, and group 2 included 16 patients with
no AF recurrence. In all cases, cardiovascular risk factors, ejection fraction, left atrial diameter,
atrial volumes, and epicardial fat volume were analyzed. Results: CT analysis revealed that
patients with AF recurrence presented a significantly larger mean index of left atrial volume
(59.57 ± 8.52 mL/m2 vs. 49.99 ± 10.88 mL/m2, p = 0.04), right atrial volume (58.94 ± 8.37 mL/m2
vs. 43.21 ± 6.4 mL/m2, p<0.0001), and indexed bi-atrial volume (118.5 ± 15.82 mL/m2 vs. 93.19 ±
16.42 mL/m2, p = 0.005). At the same time, CT analysis of the epicardial adipose tissue volume
indicated that patients with AF recurrence have a larger amount of epicardial fat than those
without AF recurrence (176.4 ± 100.8 mL vs. 109.8 ± 40.73 mL, p = 0.02). Conclusion: Left atrial
diameter, indexed atrial volumes, and epicardial fat volume may be used as factors to identify
patients at risk for developing recurrence after pulmonary vein ablation.
Keywords: AF recurrence, pulmonary vein ablation, indexed atrial volumes, epicardial adipose tissue
Emanuel Blîndu • Str. 22 Decembrie 1989 nr. 76, 540124 Targu Mures, Romania. Tel: +40 265 217 333, E-mail: [email protected]
Lehel Bordi • Str. Gheorghe Marinescu nr. 38, 540138 Targu Mures, Romania. Tel: +40 265 215 551, E-mail: [email protected]
István Kovács • Str. Gheorghe Marinescu nr. 38, 540138 Targu Mures, Romania. Tel: +40 265 215 551, E-mail: [email protected]
Imre Benedek • Str Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551, E-mail: [email protected]

65Journal of Interdisciplinary Medicine 2020;5(2):64-70
iNtroduCtioN
Atrial fibrillation (AF) is the most common type of atrial rhythm disturbances, being associated with an increased risk for thromboembolic complications and heart failure. The increased incidence of this rhythm disorder can be at-tributed to an increased life expectancy and to a higher rate of predisposing factors. Although AF is not life-threaten-ing, it significantly influences the quality of life through a series of anatomical and hemodynamic changes. A study published in 2014 has shown that AF affects 8 million pa-tients in Europe, and these numbers are expected to in-crease to about 18 million by 2060, with higher incidence and prevalence rates in developed countries.1 Estimates suggest a prevalence of AF of approximately 3% among adults aged 20 years or older, with a higher prevalence in the elderly and in patients with obesity, high blood pres-sure, heart failure, ischemic heart disease, valvulopathy, diabetes, or chronic kidney disease.2–4 As the incidence of AF continues to increase, it is very important to identify therapies that are safe and effective, improving patients’ symptoms and daily life.
Radiofrequency pulmonary vein (PV) ablation is a nov-el and complex procedure that has encountered increasing interest in the last decade. The exponential development of new techniques and the innovation of existing ones are reflected in clinical practice in a continuously increasing number of PV ablation procedures performed. This also leads to an increasing need to establish predictive factors for the success of PV ablation in AF.5 To date, the success rates of ablation are not very satisfactory, reaching only 70% in patients with paroxysmal AF and 60% in patients with persistent AF.6 Recurrences still remain a common problem after the ablation, affecting quality of life through symptomatic episodes and high readmission rates. The recurrence rate after AF ablation has been reported up to 45% in a study published in 2017.7 Therefore, there is con-siderable clinical interest to identify factors that can pre-dict the success of PV ablation, in order to develop person-alized therapeutic strategies for each patient.
Several clinical characteristics have been described as being associated with an increased recurrence rate after ablation procedures such as age, gender, comorbidities (hypertension, obesity, diabetes mellitus, heart failure), or imaging-derived features of cardiac volumes, mainly the diameter or volume of the left atrium.7–15 More re-cently, the amount of epicardial adipose tissue, assessed either by its thickness via echocardiography, or by its vol-ume via cardiac computed tomography (CT), has been described as a reliable predictor for the risk of AF de-
velopment or recurrence.16,17 Given the heterogeneous clinical profile of patients with AF or with AF recurrence after PV isolation, identification of those factors that can predict maintenance of sinus rhythm after ablation could help the clinicians to better select the patients for this complex and expensive procedure. Furthermore, an optimal patient selection for interventional AF therapies could reduce the costs of care and avoid to expose them to unnecessary interventions.
In the present study, we sought to identify clinical and imaging-based predictors for the risk of recurrence at one year following radiofrequency catheter ablation in patients with paroxysmal and persistent atrial fibrillation.
matErialS aNd mEtHod
We analyzed 24 patients with paroxysmal and persistent AF, who underwent radiofrequency catheter ablation in the 2015–2018 period. All patients underwent radiofre-quency ablation for AF using the PV isolation method and presented to follow-up at 1, 3, 6, and 12 months after the intervention. Prior to the procedure, all patients under-went contrast-enhanced cardiac CT for assessment of left and right atrial volumes, as well as for quantification of the epicardial adipose tissue using manual tracing.
Patients were divided into two groups, according to the presence or absence of AF recurrence during follow-up. Group 1 included 8 patients who presented AF recurrence in the first year after ablation, and group 2 included 16 pa-tients without any sign of recurrence during the 12-month follow-up.
The study was approved by the Ethics Committee of the institution where the procedures were performed and was conducted in compliance with the ethical principles stated in the Declaration of Helsinki. All patients gave informed consent for their participation in the study.
Ablation Protocol
After venous access using the Seldinger technique, one sheath was placed in the left femoral vein and two sheaths in the right femoral veins. A 6F decapolar diagnostic catheter was placed in the coronary sinus, one non-steerable sheath was used for positioning the mapping catheter (Lasso) and the other steerable sheath for plac-ing an externally irrigated contact force-sensing ablation catheter. Interatrial septal puncture was performed using transesophageal echocardiography guidance. 3D electro-anatomically mapping of the left atrium and PVs was per-formed using the EnSiteTM NavXTM system, EE3000

66 Journal of Interdisciplinary Medicine 2020;5(2):64-70
version (St. Jude Medical, St. Paul, MN, USA), associ-ated with advanced techniques of fusion imaging, fusing 3D mapping images with those acquired by CT. Aft er inserting the mapping catheter in the ostium of the PV, radiofrequency catheter ablation was initiated in order to isolate the PVs. Ablation was performed by applying a 30 W energy and a 10 to 30 g pressure with temperature adjusted at 50 °C, using an irrigated contact force-sensing catheter positioned on the left atrial wall. A PV was con-sidered electrically isolated when no electrical potentials were identifi ed or when a successful PV potential disso-ciation was demonstrated.
CT Analysis
Th e cardiac CT acquisition was performed using 64- and 128-slice CT (Somatom Sensation 64-slice CT, Somatom Defi nition 128-slice CT, Siemens Healthcare, Germany), and the Syngo.via Frontier soft ware (Siemens Health-ineers, Erlangen, Germany) was used for image post-processing. Quantifi cation of epicardial fat volume was performed by tracing and manually adjusting epicardial contours, as part of postprocessing protocols. Adipose tissue was identified using the attenuation references be-
tween –190 and –30 Hounsfield units. Atrial endocardial profi les were traced semi-automatically on the axial slices.
FIGURE 1. 3D maps of the left atrium and PVs. The red tags represent ablation points around the right and
left pulmonary veins’ ostia. The yellow catheter is the Lasso catheter, positioned in pulmonary vein. The green
catheter is placed in the coronary sinus
FIGURE 2. Exemplifi cation of epicardial adipose tissue quantifi ca-
tion using native CT

67Journal of Interdisciplinary Medicine 2020;5(2):64-70
Atrial volumes were calculated by the software, interpolat-ing the endocardial tracings. Indexed atrial volumes were calculated by indexing atrial volume to body surface area. Body surface area was calculated using the DuBois formula after recording height and weight.
Statistical analysis
Statistical analysis was performed using GraphPad Prism 7 (GraphPad Software, San Diego, CA, USA). Quantitative data were expressed as mean ± standard deviation, and data were compared using Student’s t test or the Mann-Whitney test when appropriate. Qualitative values were expressed as integer values and percentages, and the dif-ference between groups was analyzed using the Chi2 test or its appropriate variants. The threshold for statistical sig-
nificance was set at an alpha of <0.05.
rESultS
Baseline characteristics of the study lot, including demo-graphic data, medical history, comorbidities, and clinical and imaging features of the 24 patients included in the study are listed in Table 1.
There were no statistically significant differences be-tween the two groups in respect to age, gender, or cardio-vascular risk factors (Table 2). There was no significant difference between the study groups regarding the left ventricular ejection fraction evaluated by 2D echocardiog-raphy (51.88 ± 6.55% vs. 53.88 ± 4.28%, p = 0.3); however, clinical symptoms of heart failure were significantly more frequent in patients with AF recurrence following ablation (p = 0.03). Also, left atrium diameter was significantly larg-er in patients with AF recurrence after catheter ablation (p = 0.04) (Table 2).
CT analysis revealed that patients with AF recurrence presented a significantly larger mean index of left atrial vol-ume (LAVI) (59.57 ± 8.52 mL/m2 vs. 49.99 ± 10.88 mL/m2, p = 0.04). Also, the indexed right atrial volume (RAVI) and the indexed bi-atrial volume (BAVI) were higher in the group with AF recurrence (58.94 ± 8.37 mL/m2 vs. 43.21 ± 6.4 mL/m2, p <0.0001 for RAVI and 118.5 ± 15.82 mL/m2 vs. 93.19 ± 16.42 mL/m2, p = 0.005 for BAVI). Figure 3 indicates the difference between the groups in respect to anatomic features as assessed by cardiac CT, namely calculated indexes of atrial volumes.
At the same time, CT analysis of the epicardial adipose tissue volume indicated that patients with AF recurrence have a larger amount of epicardial fat compared with pa-tients without recurrence (176.4 ± 100.8 mL vs. 109.8 ± 40.73 mL, p = 0.02). Figure 4 represents the difference be-tween the groups in respect to the volume of epicardial fat as computed by CT.
TABLE 1. Baseline characteristics of the study population
Age (years) 57.25 ± 11.72
Gender, male, n (%) 14 (58.33%)
History
Hypertension, n (%) 17 (70.83%)
Diabetes, n (%) 7 (29.16%)
Dyslipidemia, n (%) 5 (20.86%)
Obesity, n (%) 12 (50%)
Clinical characteristics
eGRF (mL/m2/min) 79.85 ± 17.51
Ejection fraction (%) 53.21 ± 5.09
Left atrium (mm) 41.54 ± 6.43
Heart failure, n (%) 10 (41.66%)
CAD, n (%) 10 (41.66%)
AF type
Persistent AF 10 (41.66%)
Indexed atrial volume
LAVI (mL/m2) 58.18 ± 10.98
RAVI (mL/m2) 48.45 ± 10.41
BAVI (mL/m2) 101.6 ± 20.02
Epicardial fat volume (mL) 132 ± 72.14
TABLE 2. Clinical and echocardiographic features associated to AF recurrence after ablation
AF recurrencen = 8
No AF recurrencen = 16
p value
Heart failure, n (%) 6 (75%) 4 (25%) 0.03
Left atrium (mm) 45.25 ± 5.14 39.69 ± 6.33 0.04
LAVI (mL/m2) 59.57 ± 8.52 49.99 ± 10.88 0.04
RAVI (mL/m2) 58.94 ± 8.37 43.21 ± 6.74 <0.0001
BAVI (mL/m2) 118.5 ± 15.82 93.19 ± 16.42 0.005
Epicardial fat volume (mL) 176.4 ± 100.8 109.8 ± 40.73 0.02

68 Journal of Interdisciplinary Medicine 2020;5(2):64-70
diSCuSSioNS
AF is a disease with a high prevalence and is associated with increased mortality and morbidity. PV catheter ab-lation has emerged as a first-line treatment option, espe-cially in cases resistant to antiarrhythmic medication.18 Immediate success rates have been achieved using PV catheter ablation, but maintaining long-term sinus rhythm in these cases still remains a challenge. Given the average success rates, it is necessary to investigate factors associ-ated to a lower risk of recurrence, which may facilitate a proper selection of patients for ablation. In the last years, several studies have tried to identify predictive factors for a favorable long-term outcome, but reliable markers pre-dicting the maintenance of sinus rhythm have not been identified.9,19,20 The contribution of this study relies on the description of the role of new imaging-based features asso-ciated with the risk of AF recurrence, such as LAVI, RAVI, BAVI, and the volume of epicardial adipose tissue, along with other factors investigated also in other studies, such as AF type, cardiovascular risk factors, left atrium diam-eter, ejection fraction, and renal function.
Our study aimed to identify new predictive factors for the risk of recurrence based on the differences between
patients who presented AF recurrence and those who maintained sinus rhythm. The results of this study indicate that the diameter of the left atrium, the presence of heart failure, atrial volumes, and the amount of epicardial adi-pose tissue are predictive factors for the risk of arrhythmia recurrence at one year after radiofrequency ablation of AF.
The link between the enlargement of the left atrium and the recurrence of AF is still controversial. In the long term, an enlarged left atrium leads to cardiac remodeling,
118.5 ± 15.82 p = 0.005
BAVI and AF recurrence (mL/m2)
93.19 ± 16.42
0
50
100
150
AF recurrence No AF recurrence
59.57 ± 8.52p = 0.04
LAVI and AF recurrence (mL/m2)
49.99 ± 10.88
0
20
40
60
80
AF recurrence No AF recurrence
59.57 ± 8.52p <0.0001
RAVI and AF recurrence (mL/m2)
43.21 ± 6.74
0
20
40
60
80
AF recurrence No AF recurrence
FIGURE 3. Atrial volumes and risk of recurrence after AF ablation. A – Bi-atrial indexed volume in the study
groups; B – Right indexed atrial volume in study groups; C – Left indexed atrial volume in the study groups
176.4 ± 100.8 p = 0.02
EFV and AF recurrence (mL/m2)
109.8 ± 40.73
0
100
200
300
AF recurrence No AF recurrence
FIGURE 4. Epicardial fat volume in the study groups
A
B C

69Journal of Interdisciplinary Medicine 2020;5(2):64-70
manifested by reduced myocardial tissue and increased fi-brosis. The increased diameter of the left atrium, reflect-ing diastolic dysfunction and increased filling pressure due to atrial remodeling, contributes to the vulnerability of atrial myocytes to arrhythmia.9 As it has been shown that the size of the left atrium is an important factor in the oc-currence and maintenance of AF, this could be used in the same way to predict the recurrence after intervention. In a meta-analysis on risk factors for recurrence of post-abla-tion arrhythmias, an increased diameter of the left atrium was found to have predictive value for AF recurrence.13 In our study, patients who had maintained sinus rhythm had a significantly smaller left atrium diameter compared to pa-tients with recurrence.
AF and heart failure are two linked conditions, each one predisposing to the other one, and are associated with con-siderable mortality and morbidity. Important changes in the prevalence of AF in patients with heart failure have been ob-served, AF occurrence being directly linked to the severity of heart failure, from less than 10% in patients with NYHA class I to almost 50% in patients in NYHA class IV.21 In a recent study, patients with heart failure had an increased susceptibility to develop recurrences, compared to patients with normal left ventricular function. The main limitation for using left atrial diameter as a measure of the risk of recur-rence relies on its representation as a one-dimensional val-ue, which can underestimate or overestimate the true size of the atrium. Therefore, assessment of the atrial volume, especially body surface-related volume, is indicated for a more precise assessment of the left atrium, having a superior predictive value.15 Comparing atrial volumes between the two groups, we observed that patients with AF recurrence had significantly larger left, right, and bi-atrial indexed vol-umes than patients who maintained sinus rhythm during follow-up. A number of studies found LAVI to be predic-tive of AF recurrence, but no consensus was reached on the predictive cut-off value.15,22 At the same time, there are few data regarding the effect of an increased right atrial volume on the risk of AF recurrence after PV isolation. Given that ablation targets the myocardial tissue surrounding the PV, the right atrium remains “untreated”, thus maintaining an increased risk of recurrence in patients with a higher right atrial volume. In one study it was found that RAVI has pre-dictive value only for early recurrences of AF, while LAVI has predictive value in recurrences at one year.23
Epicardial adipose tissue is a special type of fat located in the space between the myocardium and the visceral pericardium. This tissue is not just an anatomical depot of fat, but also an active tissue that secretes cytokines and pro-inflammatory hormones, being involved in the patho-
genesis of both structural heart disease and the coronary heart disease independent of body mass index.24 Several studies have evaluated the association between pericardial fat and AF and have shown that an increased volume of pericardial adipose tissue, independent of intrathoracic or intraabdominal adipose tissue, results in a higher risk of AF.16,17 Another important observation is that in patients with persistent AF, the volume of pericardial adipose tis-sue is higher than in patients with paroxysmal AF or in pa-tients with sinus rhythm.25 Several studies have shown that following PV ablation, patients with increased epicardial fat volume had more frequent recurrences, regardless of body mass index and body surface area.26–28 In this paper, the volume of epicardial adipose tissue was determined us-ing computed tomography, and a lower epicardial fat vol-ume was associated with maintenance of the sinus rhythm one year after the intervention.
CoNCluSioNS
AF is a common disorder in clinical practice and is often characterized by recurrences. Therefore, the identification of particular features that can predict the maintenance of sinus rhythm after PV ablation represents an important goal in clinical practice, allowing a more appropriate pa-tient selection. This study shows that left atrial diameter, indexed atrial volumes, and epicardial fat volume may be used as reliable indicators of the risk to develop AF recur-rence after pulmonary vein ablation.
CoNfliCt of iNtErESt
Nothing to declare.
aCkNoWlEdGEmENt
This research was supported via the research grant no. 103544/2016 – PLaqueIMAGE, contract number 26/01.09.2016, financed by the Romanian Ministry of Eu-ropean Funds, the Romanian Government, and the Euro-pean Union.
rEfErENCES
1. Krijthe BP, Kunst A, Benjamin EJ, et al. Projection on the number of
individuals with atrial fibrillation in the European Union, from 2000 to
2060. Eur Heart J. 2013;34:2746-2751.
2. Zoni-Berisso M, Lercari F, Carazza T, Domenicucci S. Epidemiology of
atrial fibrillation. European perspective. Clin Epidemiol. 2014;6:213-220.
3. Ball J, Carrington MJ, McMurray JJ, Stewart S. Atrial fibrillation: Profile
and burden of an evolving epidemic in the 21st century. Int J Cardiol.
2013;167:1807-1824.

70 Journal of Interdisciplinary Medicine 2020;5(2):64-70
4. Nguyen TN, Hilmer SN, Cummings RG. Review on epidemiology and management of atrial fibrillation in developing countries. Int J Cardiol. 2013;167:2412-2420.
5. Kircher S, Hindricks G, Sommer P. Long term success and follow-up after atrial fibrillation ablation. Curr Cardiol Rev. 2012;8:354-361.
6. Spitzer SG, Leitz P, Langbein A, et al. Circumferential pulmonary vein ablation with second generation multipolar catheter in patients with paroxysmal or persistent atrial fibrillation: Procedural and one-year follow-up results. Int J Cardiol. 2017;241:212-217.
7. Sultan A, Luker J, Andrresen D, et al. Predictors of atrial fibrillation recurrence after catheter ablation: Data from the German Ablation Registry. Sci Rep. 2017;7:16678.
8. Rostock T, Salukhe TV, Steven D, et al. Long-term single- and multiple-procedure outcome and predictors, of success after catheter ablation for persistent atrial fibrillation. Heart Rhythm. 2011;8:1391-1397.
9. Vizzardi E, Curnis A, Latini M, et al. Risk factors for atrial fibrillation recurrence. J Cardiovasc Med. 2014;15:235-253.
10. Lau YF, Yiu KH, Siu CW, Tse HF. Hypertension and atrial fibrillation: epidemiology, pathophysiology and therapeutic implications. Journal of Human Hypertension. 2012;26:563-569.
11. Cai L, Yin Y, Ling J, et al. Predictors of late recurrence of atrial fibrillation after catheter ablation. Int J Cardiol. 2013;164:82-87.
12. Chang SL, Tuan TC, Tai CT, et al. Comparison of outcome in catheter ablation of atrial fibrillation in patients with versus without the metabolic syndrome. Am J Cardiol. 2009;103:67-72.
13. Zhuang J, Wang Y, Tang K, et al. Association between left atrial size and atrial fibrillation recurrence after single circumferential pulmonary vein isolation: a systematic review and meta-analysis of observational studies. Europace. 2012;14:638-645.
14. Cheema A, Dong J, Dalal D, et al. Circumferential ablation with pulmonary vein isolation in permanent atrial fibrillation. Am J Cardiol. 2007;99:1425-1428.
15. Njoku A, Kannabhiran M, Arora R, et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: a meta-analysis. Europace. 2018;20:33-42.
16. Wong CX, Sun MT, Odutyo A, et al. Association of epicardiac, abdominal and overall adiposity with atrial fibrillation. Circ Arrhythm Electrophysiol. 2016;pii:e00437.
17. Gaeta M, Bandera F, Tassinari F, et al. Is epicardial fat depot associated with atrial fibrillation? A systematic review and metaanalysis. Europace. 2017;19:747-752.
18. Guo XY, Ma CS. Atrial fibrillation ablation: indications, outcomes, complications, and future directions. Chin Med J. 2017;130:1891-1893.
19. Deneke T, Schade A, Krug J, et al. Predictors of recurrence after catheter ablation of persistent atrial fibrillation. J Atr Fibrillation. 2012;4:498.
20. Balk EM, Garlitski AC, Alsheikh-Ali AA, Terasawa T, Chung M, Ip S. Predictors of atrial fibrillation recurrence after radiofrequency catheter ablation: a systematic review. J Cardiovasc Electrophysol. 2010;21:1208-1216.
21. Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91:2D-8D.
22. Kranert M, Shchetynska-Marinova T, Liebe V, et al. Recurrence of atrial fibrillation in dependence of left atrial volume index. In Vivo. 2020;34:889-896.
23. Moon J, Lee HJ, Kim JY, et al. Prognostic Implications of Right and Left Atrial Enlargement after Radiofrequency Catheter Ablation in Patients with Nonvalvular Atrial Fibrillation. Korean Circ J. 2015;45:301-309.
24. Al Chekakie MO, Akar JG. Epicardial fat and atrial fibrillation: A Review. J Atr Fibrillation. 2012;4:483.
25. Batal O, Schoenhagen P, Shao M, et al. Left atrial epicardial adiposity and atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3:230-236.
26. Thanassoulis G, Massaro JM, O’Donnell CJ, et al. Pericardial fat is associated with prevalent atrial fibrillation: the Framingham Heart Study. Circ Arrhythm Electrophysiol. 2010;3:345-350.
27. Tsao HM, Hu WC, Wu MH, et al. Quantitative Analysis of Quantity and Distribution of Epicardial Adipose Tissue Surrounding the Left Atrium in Patients With Atrial Fibrillation and Effect of Recurrence After Ablation. Am J Cardiol. 2011;107:1498-1503.
28. Wong CX, Abed HS, Molaee P, et al. Pericardial fat is associated with atrial fibrillation severity and ablation outcome. J Am Coll Cardiol. 2011;57:1745-1751.
Journal of Interdisciplinary Medicine 2020;5(2):71-75
CORRESPONDENCE
Ana Petra LazărStr. Gheorghe Marinescu nr. 38540139 Targu Mures, RomaniaTel: +40 265 215 551E-mail: [email protected]
ARTICLE HISTORY
Received: May 28, 2020Accepted: June 15, 2020
Incidence of Periodontal Disease among AdolescentsDelia-Roxana Dicu1, Ana Petra Lazăr2, Luminița Lazăr3
1 Faculty of Dental Medicine, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania2 Department of Oral Rehabilitation and Occlusology, Faculty of Dental Medicine, “George Emil Palade” University of Medicine,
Pharmacy, Science and Technology, Targu Mures, Romania3 Department of Periodontology and Oral Diagnosis, Faculty of Dental Medicine, “George Emil Palade” University of Medicine,
Pharmacy, Science and Technology, Targu Mures, Romania
oriGiNal rESEarCH // briEf rEport EPIDEMIOLOGY // PERIODONTOLOGY
DOI: 10.2478/jim-2020-0013
ABSTRACT
Background: Despite the scarcity of studies regarding periodontal disease in young patients
(teenagers and young adults), it seems that this disorder is also affecting the young population.
Risk factors for periodontal disease include older age, chronic tobacco use, male gender, hab-
its regarding oral hygiene, educational status, ethnicity, and financial status. Aim: This study
aimed to evaluate the periodontal health among adolescents in two high schools in Targu
Mures that had dental practices. Material and Methods: An online questionnaire consisting of
16 questions was distributed among high schoolers of Targu Mures. Data about personal char-
acteristics, oral hygiene habits, family history of periodontal disease, risk factors for periodontal
disease, and symptoms of periodontal disease observed by the respondents were collected
and analyzed. Results: Out of the 501 teenagers who responded to the online questionnaire,
114 (22.8%) were 18 years old and were mostly females (88.2%). Regarding oral hygiene habits,
75.8% prefer a manual toothbrush over an electric toothbrush, 66.7% brush their teeth twice
a day, and 54.1% practice a horizontal method of toothbrushing. Mouthwash was the most
used oral hygiene aid (58.3%). Family history of periodontal disease was observed in 21.9% of
respondents. As favoring factors, nicotine addiction (23.8%), bruxism (24.4%), interposition of
various objects between teeth (48.3%), past or present orthodontic treatments (38.7%) were
recorded. Symptoms of gingivitis and periodontitis, such as gingival bleeding (81.4%), redness
of gingiva (39.3%), increased gingival volume (44.5%), gingival retraction (22.8%), and halitosis
(81%), were present in the responding teenagers. Conclusions: In this study, periodontal dis-
ease was affecting mostly adolescent females who are practicing inappropriate methods of
toothbrushing with inadequate frequency.
Keywords: periodontal health, adolescents, gingivitis, periodontitis
Delia-Roxana Dicu • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 748 864 900, E-mail: [email protected]
Luminița Lazăr • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551, E-mail: [email protected]

72 Journal of Interdisciplinary Medicine 2020;5(2):71-75
iNtroduCtioN
Nowadays, the major focus of dental medicine is maintain-ing a lifelong healthy state of the hard and soft tissues. In order to achieve this goal, periodontal diseases should be diagnosed early in life, starting from childhood and ado-lescence, as they affect more than half of the teenage popu-lation, which are mainly asymptomatic. Bimstein (1991) stressed the importance of prevention, early diagnosis, and early treatment of periodontal diseases in children and adolescents, because the prevalence and severity of peri-odontal diseases is high. Also, the incipient periodontal diseases found in childhood may develop into advanced periodontal diseases during adulthood, and there is a di-rect association between periodontal disease and systemic conditions. Patients, families, or populations at risk could be identified and included in special prevention or treat-ment programs, as prevention and treatment of most peri-odontal diseases is relatively simple and very effective, providing lifetime benefits.1,2
This study aimed to evaluate periodontal health among adolescents in two high schools in Târgu Mureș that had a dental practice.
matErial aNd mEtHodS
The study was initially created as a clinical trial involving the clinical examination of teenagers from “Alexandru Papiu Il-arian” National College and “Traian Săvulescu” Agricultural College that had a dental practice. We determined that 10th and 11th graders were appropriate to be examined. The first step included a presentation concerning periodontal health and a questionnaire about personal characteristics, oral hygiene habits, family history of periodontal disease, favoring factors for periodontal disease, and symptoms of periodontal disease. Then, the next stage included an ob-jective clinical examination in school dental practices using dental examination instruments (probe, mirror, tweezers) and a periodontal probe. We examined plaque index, tar-tar index, gingival index, clinical attachment loss, papillary bleeding index, mobility, furcation involvement, and peri-odontal probing depth on Ramfjord teeth. The study was approved by the Ethics Committee of “George Emil Palade” University of Medicine and Pharmacy, Science and Tech-nology of Târgu Mureș was obtained. All participants gave informed consent for participation in this study and all the study procedures were conducted in accordance with the principles stated in the Declaration of Helsinki.
Due to the worldwide epidemiologic context of the time when we were about to start the study (March 2020),
a safe clinical examination was not possible; therefore, we adjusted accordingly and narrowed the study down to an online questionnaire. Thus, the present study was based on a questionnaire consisting of 16 questions that was dis-tributed among the high schoolers of Târgu Mureș. When formulating the questions, we used colloquial language in order to have a greater addressability. Data about personal characteristics, oral hygiene habits, family history of peri-odontal disease, risk factors for periodontal disease, and symptoms of periodontal disease observed by the respon-dents were collected and analyzed.
The resulting data were collected and interpreted using Google Forms and Microsoft Excel.
rESultS
Data from 501 responding adolescents were collected and analyzed. The respondents were aged between 14 and 19 years, most of them being 18 years old. The majority of the respondents (88.2%) were female. Regarding oral hygiene habits, 75.8% stated that they prefer a manual toothbrush over an electric toothbrush, 66.7% brush their teeth twice a day, and 54.1% practice a horizontal method of tooth-brushing. Mouthwash was the most used oral hygiene aid (58.3%). Data about oral hygiene habits is presented in Table 1.
Family history of periodontal disease was observed in 21.9% of the study population.
Favoring factors that play an important role in the de-velopment of periodontal diseases were also addressed in the questionnaire. The answers revealed that 23.8% of the participants were smokers, 24.4% practiced the habit of bruxism, 48.3% had viciously interposing objects between their teeth, and 38.7% were undergoing an orthodontic treatment.
Given the lack of an objective clinical examination, we focused some of the questions on the symptoms of gin-givitis and periodontitis in order to have a general view regarding these pathologies. When asked about gingival bleeding, 81.4% of the respondents answered positively. A similar percentage of participants (81%) admitted to have halitosis, and 39.3% have observed redness of the gingiva. Increased gingival volume and gingival retractions were observed by 44.5% and 22.8% of respondents, respectively.
diSCuSSioNS
Despite the scarcity of studies regarding periodontal dis-ease in young patients (teenagers and young adults), it seems that this disorder is also affecting the young popula-

73Journal of Interdisciplinary Medicine 2020;5(2):71-75
tion. Risk factors for periodontal disease include older age, chronic tobacco use, male gender, habits regarding oral hygiene, educational status, ethnicity, and financial sta-tus.3,4 In the present study, we aimed to assess the preva-lence of periodontal disease in the high school population of a medium-sized city in Central Romania. Although ini-tially designed as a cross-sectional clinical study, the global COVID-19 pandemic situation has led to a drastic change in the research methodology and study design. Therefore, we conducted a questionnaire-based study on the clinical signs and symptoms of periodontal disease, and also its associated risk factors, on a population of young students aged between 14 and 19 years, from two high schools in Târgu Mureș.
Given the lack of an objective clinical examination, we considered the triad of gingival bleeding – increased gingi-val volume – redness of gingiva as an indicator of gingivitis, regardless of the causal factor (dental plaque, hormones, manifestation of general disease etc.). Gingivitis was pres-ent in a relatively large proportion of respondents (26.5%). Moreover, we considered the simultaneous presence of halitosis and gingival retraction as indicator of periodonti-tis, which was present in a lower rate (19.3%). The gender distribution of subjects with periodontitis and gingivitis in our study population was skewed towards female respon-dents, which was similar to a study conducted in Bucha-rest. On the other hand, two international studies found that males presented higher odds for periodontal disease compared to females.5,6
Regarding the age of the participants, there was a ten-dency for the prevalence of gingivitis and periodontitis to increase with age. The increasing trend of gingivitis and periodontitis during puberty and adolescence could be re-lated to hormonal influences over dental plaque and gingi-
val tissue.7,8 Daily toothbrushing frequency was similar for both individuals who use a manual toothbrush or an elec-tric toothbrush. However, regardless of the type of tooth-brush used, the percentage of teenagers who brush their teeth twice a day was almost double compared to those who brush their teeth once a day. The efficiency of tooth-brushing was also assessed. Gingivitis was more frequent (36.1%) among respondents who brush their teeth once a day and among those who use an electric toothbrush (28.9%). The latter result is inconsistent with other stud-ies that report an increased dental plaque removal using an electric toothbrush by 4% to 29.6%.9–11
By adolescence, people should grasp the correct tech-nique of toothbrushing, which is the vertical one. Most of the respondents were using a horizontal technique, which demonstrates the lack of oral hygiene education. The main consequence of horizontal toothbrushing is gingival re-traction, which is also directly related to bristle hardness, the duration of each toothbrushing session, as well as the frequency of changing a used toothbrush.12,13 Adolescents seem to show a great interest in auxiliary methods of re-moving dental plaque, using mostly mouthwash, interden-tal floss, and wooden toothpicks, although they are not proven to decrease dental plaque; only interdental brushes showed a decrease in dental plaque (32%) and gingivitis (34%).14–16
Gingivitis was predominant among respondents who reported a family history of periodontal disease, although other studies did not confirm whether the disease has a genetic transmission or it is a result of environmental fac-tors.17,18
According to the World Health Organization, nicotine addiction exerts a great influence on oral health, being fre-quently associated with a poor oral hygiene and the pres-
TABLE 1. Distribution of oral hygiene habits among the responding adolescents
Question Possible answers Answered yes (%)
Type of toothbrush Manual 75.8
Electric 24.2
Daily toothbrushing frequency Does not brush on a daily basis 0
Once a day 33.1
Twice a day 66.7
Toothbrushing method Horizontal 54.1
Vertical 45.9
Auxiliary method of removing dental plaque
Mouthwash 58.3
Interdental floss 34.1
Wooden toothpick 29.1
Oral irrigator 13
Interdental toothbrush 12

74 Journal of Interdisciplinary Medicine 2020;5(2):71-75
ence of red complex periodontal pathogens.19,20 Although most of the international studies agree that most smok-ers are males, our study shows an increased percentage of female smokers (25.4% vs. 23.5%) and consequently, an increased percentage of gingivitis and halitosis. Other major contributing factors to gingivitis and gingival retrac-tion are bruxism and the vicious habit of interposing vari-ous objects between teeth, which were relatively frequent in the questioned population. It is proven that nocturnal bruxism is present in children and adolescents more often than in adults, but it does not cause gingivitis or gingival retraction without the presence of dental plaque.2,21–24
Orthodontic materials increase the retentivity of the dental arch and, consequently, dental plaque build-up and the development of periodontal disease. Gingivitis was more frequent in teenagers with orthodontic treatment (34.5%) in our study. This result is supported by other studies which state that dental plaque build-up and hyper-plastic gingivitis occur in the first two months after start-ing the orthodontic treatment.25,26 Patients treated with removable materials showed a decreased plaque index and gingivitis due to superior cleaning possibilities com-pared to fixed appliances.27 Gingival retractions are also in-creased in teenagers with orthodontic treatment (24.2%), even though they are not specific to this age group.28
Study limitations
The major limitation of this study was the difficulty to con-duct a more objective clinical examination, in the absence of which the results have only an indicative value. Other sources of error could be misinterpretation of symptoms by the respondents or truncated information, and misin-terpretation of results. The study supports further addi-tions and improvements by adding a clinical examination as it was initially intended.
Such studies are of great value in the current clinical ac-tivity because they evaluate the state of the general popula-tion, and through these studies, health education programs focused on oral health can be implemented. Furthermore, epidemiologic studies justify and support therapeutic pro-tocols by highlighting the risk factors for the evaluated dis-order.
CoNCluSioNS
In this study, periodontal disease was affecting mostly ado-lescent females who are practicing inappropriate methods of toothbrushing with inappropriate frequency. Although the respondents were keen on using auxiliary methods
of removing dental plaque, their effectiveness has not been demonstrated. Bruxism is a major favoring factor for periodontal disease due to an increased prevalence of gingivitis and gingival retraction among adolescents that practice this habit. Another favoring factor, nicotine ad-diction, can cause gingivitis and halitosis among female adolescents. Orthodontic appliances cause increased den-tal plaque retention leading to gingivitis and gingival re-traction.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES1. Oh TJ, Eber R, Wang HL. Periodontal diseases in the child and adolescent.
J Clin Periodontol. 2002;29:400-410. 2. Dumitriu HT, Dumitriu S, Dumitriu AS. Tratat de parodontologie. Bucharest:
Ed. Viața Medicală Romanească, 2015; p. 112-148.3. Peeran SW, Singh AJ, Alagamuthu G, Naveen Kumar PG. Periodontal
status and its risk factors among young adults of the Sebha city (Libya). Dent Res J (Isfahan). 2013;10:533-538.
4. Periodontal Disease in Adults (Age 20 to 64). Available at: https://www.nidcr.nih.gov/research/data-statistics/periodontal-disease/adults
5. Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ. CDC Periodontal Disease Surveillance workgroup: James Beck (University of North Carolina, Chapel Hill, USA), Gordon Douglass (Past President, American Academy of Periodontology), Roy Page (University of Washin. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res. 2012;91:914-920.
6. Grossi SG, Genco RJ, Machtei EE, et al. Assessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J Periodontol. 1995;66:23-29.
7. Dietrich T, Kaye EK, Nunn ME, Van Dyke T, Garcia RI. Gingivitis susceptibility and its relation to periodontitis in men. J Dent Res. 2006;85:1134-1137.
8. Bimstein E, Matsson L. Growth and development considerations in the diagnosis of gingivitis and periodontitis in children. Pediatr Dent. 1999;21:186-191.
9. Elkerbout TA, Slot DE, Rosema NAM, Van der Weijden GA. How effective is a powered toothbrush as compared to a manual toothbrush? A systematic review and meta-analysis of single brushing exercises. Int J Dent Hyg. 2020;18:17-26.
10. Sicilia A, Arregui I, Gallego M, Cabezas B, Cuesta S. A systematic review of powered vs manual toothbrushes in periodontal cause-related therapy. J Clin Periodontol. 2002;29 Suppl3:39-91.
11. Bartizek RD, Biesbrock AR. Dental plaque removal efficacy of a battery-powered toothbrush vs. a control Japanese manual toothbrush. Am J Dent. 2002;15:33A-36A.
12. Heasman PA, Holliday R, Bryant A, Preshaw PM. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. J Clin Periodontol. 2015;42Suppl16:S237-S255.
13. Bergström J, Lavstedt S. An epidemiologic approach to toothbrushing and dental abrasion. Community Dent Oral Epidemiol. 1979;7:57-64.
14. Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev. 2019;4:CD012018.
15. Sälzer S, Slot DE, Van der Weijden FA, Dörfer CE. Efficacy of inter-dental mechanical plaque control in managing gingivitis – a meta-review. J Clin Periodontol. 2015;42Suppl 16:S92-S105.
16. Richards D. The effectiveness of interproximal oral hygiene aids. Evid Based Dent. 2018;19:107-108.
17. Tatakis DN, Trombelli L. Modulation of clinical expression of plaque-induced gingivitis. I. Background review and rationale. J Clin Periodontol. 2004;31:229-238.

75Journal of Interdisciplinary Medicine 2020;5(2):71-75
18. Michalowicz BS, Diehl SR, Gunsolley JC, et al. Evidence of a substantial genetic basis for risk of adult periodontitis. J Periodontol. 2000;71:1699-1707.
19. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013;62:59-94.
20. Honkala S, Honkala E, Newton T, Rimpelä A. Toothbrushing and smoking among adolescents – aggregation of health damaging behaviours. J Clin Periodontol. 2011;38:442-448.
21. Melo G, Duarte J, Pauletto P, et al. Bruxism: An umbrella review of systematic reviews. J Oral Rehabil. 2019;46:666-690.
22. Bosnjak A, Vućićević-Boras V, Miletić I, Bozić D, Vukelja M. Incidence of oral habits in children with mixed dentition. J Oral Rehabil. 2002;29:902-905.
23. Restrepo CC, Tirado M, Jimenez KJ. Association of sleep bruxism and dental plaque factors on signs of periodontal disease in children in the mixed dentition. Int J Paediatr Dent. 2016;26:477-485.
24. Manfredini D, Ahlberg J, Mura R, Lobbezoo F. Bruxism is unlikely to cause damage to the periodontium: findings from a systematic literature assessment. J Periodontol. 2015;86:546-555.
25. Cardoso-Silva C, Barbería E, Ramos Atance JA, Maroto M, Hernández A, García-Godoy F. Microbiological analysis of gingivitis in pediatric patients under orthodontic treatment. Eur J Paediatr Dent. 2011;12:210-214.
26. Alhaija ESA, Al-Saif EM, Taani DQ. Periodontal health knowledge and awareness among subjects with fixed orthodontic appliance. Dental Press J Orthod. 2018;23:40.e1-40.e9.
27. Abbate GM, Caria MP, Montanari P, et al. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J Orofac Orthop. 2015;76:240-250.
28. Alhaija ESA, Al-Saif EM, Taani DQ. Periodontal health knowledge and awareness among subjects with fixed orthodontic appliance. Dental Press J Orthod. 2018;23:40.e1-40.e9.

Journal of Interdisciplinary Medicine 2020;5(2):76-80
CORRESPONDENCE
Dumitru CostelStr. Gheorghe Marinescu nr. 38540139 Targu Mures, RomaniaTel: +40 265 215 551E-mail: [email protected]
ARTICLE HISTORY
Received: April 30, 2020Accepted: June 16, 2020
Immunosuppressive Medication and Non-Rejection-Related Complications Following Heart TransplantationDumitru Costel1, Dana Ghiga2, Simona Voidazan3, Alexandra Grosan4, Dan Simpalean5, Anca Sin6
1 “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania2 Discipline of Methodology of Medical Scientific Research, “George Emil Palade” University of Medicine, Pharmacy, Science and
Technology, Targu Mures, Romania 3 Discipline of Epidemiology, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania4 Discipline of Pharmacology and Clinical Pharmacy, “George Emil Palade” University of Medicine, Pharmacy, Science and
Technology, Targu Mures, Romania5 “Filantropia” Clinical Hospital, Bucharest, Romania6 Discipline of Cell Biology, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania
oriGiNal rESEarCH // briEf rEport PUBLIC HEALTH // EPIDEMIOLOGY
DOI: 10.2478/jim-2020-0015
ABSTRACT
Background: Although the clinical evolution of a patient with heart failure is initially improved
by transplantation, a number of potential complications may occur in the post-transplant pe-
riod, which may be directly related to the effects of chronic immunosuppression. The purpose
of this study was to analyze the occurrence and frequency of post-transplant complications
related to immunosuppressive treatment in the Institute of Cardiovascular Diseases and Trans-
plantation of Targu Mures, Romania. Material and methods: This is a descriptive study includ-
ing 53 patients out of a total of 71 patients who underwent cardiac transplantation between
2000 and 2017 in the Institute of Cardiovascular Disease and Cardiac Transplantation in Targu
Mures, Romania. Data were collected from the patient files and included demographic, clini-
cal and laboratory data, as well as information about post-transplant complications related to
immunosuppressive treatment. Results: The mean age of patients undergoing heart trans-
plantation was 40.72 ± 14.07 years, the majority of patients being male (84.91%) and living in
an urban environment (56.60%). The average length of hospital stay was 33.6 days. From the
total number of patients, 7 (13.2%) presented post-transplantation bacterial infections, while
antibodies indicating the presence or history of B hepatitis, toxoplasma, and cytomegalovirus
infection were identified with a relatively high incidence in the study population. Conclusions:
Infections following surgery are probably the most common post-transplant pathology, the
primary reason being the administration of immunosuppressive medication.
Keywords: cardiac transplant, postoperative complications, immunosuppression
Dana Ghiga • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551
Simona Voidazan • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551
Alexandra Grosan • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551
Dan Simpalean • Blv. Ion Mihalache nr. 11, 011171 Bucuresti, Romania. Tel: +40 21 318 89 37
Anca Sin • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 215 551

77Journal of Interdisciplinary Medicine 2020;5(2):76-80
iNtroduCtioN
Heart transplantation is the treatment of choice in severe cases of end-stage heart failure.1,2 In the absence of heart transplantation, the management of these critical cases is associated with a poor prognosis.3–5 Cardiac transplanta-tion has shown a very good long-term survival rate in pa-tients with dilative cardiomyopathy and end-stage coro-nary heart disease, with up to 85% survival in the first year after transplant, 75% at 5 years, and 56% at 10 years.6,7 Al-though the clinical evolution of a patient with heart fail-ure is initially improved by transplantation, a number of potential complications may occur following the interven-tion, which may be directly related to the effects of chronic immunosuppression, mandatory to prevent the rejection of transplanted hearts.
aim of tHE Study
The purpose of this study was to analyze the occurrence and frequency of post-transplant complications related to immunosuppressive treatment in the Institute of Cardio-vascular Diseases and Transplantation of Târgu Mureș, Romania.
matErial aNd mEtHodS
This is a descriptive study including 53 patients out of a to-tal of 71 patients who underwent cardiac transplantation between 2000 and 2017 in the Institute of Cardiovascular Diseases and Cardiac Transplantation in Târgu Mureș,
Romania. Data were collected from the patient files and included demographic, clinical and laboratory data, as well as information about post-transplant complications related to immunosuppressive treatment. The collected data were analyzed using descriptive statistical methods. Continuous variables were expressed as mean ± standard deviation, and quantitative data as proportions. The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki, and in agreement with the good clinical practice measures. The study was approved by the local ethics committee, and all patients gave informed consent for participation in the study.
rESultS
The mean age of patients undergoing heart transplantation was 40.72 ± 14.07 years, the majority of patients being male (84.91%) and living in an urban environment (56.60%). The average length of hospital stay was 33.6 days.
Infectious complications
From the total number of patients, 7 (13.2%) presented post-transplantation bacterial infections: Klebsiella pneu-moniae was found in 2 cases, while Clostridium difficile, Staphylococcus aureus, methicillin-sensitive Staphylococcus aureus (MSSA), Staphylococcus epidermidis, and Pseudo-monas aeruginosa were identified in the rest of 5 cases.
Viral infections were also diagnosed with a high frequen-cy following heart transplantation. Antibodies indicating the presence or history of B hepatitis, Toxoplasma, and Cy-
36
4543
26
42
25
43 43
9
18
1
20
2 2
0
5
10
15
20
25
30
35
40
45
50
Anti HBc Anti HCV AntiSyphilis TP
Anti ToxopIgG
Anti ToxopIgM
Anti CMVIgG
Anti CMVIgM
Anti HIV
NegativePositive
FIGURE 1. The distribution of positive-tested antibodies in the studied population

78 Journal of Interdisciplinary Medicine 2020;5(2):76-80
tomegalovirus (CMV) infection were identified with a rela-tively high incidence in the study population (Figure 1).
Renal dysfunction
Cyclosporine-induced nephrotoxicity remains a medical challenge in cardiac post-transplant management. In our study, only 1 (2%) patient out of 53 was diagnosed with re-nal failure post-cardiac transplant. Following heart trans-plantation, the mean serum levels of urea and creatinine were 61.13 ± 30.87 mg/dL and 1.002 ± 0.932 mg/dL, re-spectively.
Hyperlipidemia
We assessed the incidence of hyperlipidemia with multi-factorial origin and found mean cholesterol values of 381.0 ± 175.0 mg/dL and mean LDL-cholesterol values post-transplant of 220.1 ± 63.38 mg/dL.
diSCuSSioNS
Post-transplant pathology – development of new clinical conditions favoring infections
According to published literature, post-transplant evolu-tion is frequently marked by the development of new clini-cal conditions which, associated with immunosuppressive treatment, may favor the development of severe infections, reducing the defensive capacity of the body. These condi-tions include new-onset diabetes, hypertension, hyperlip-idemia, renal dysfunction, tumors, or thyroid diseases.
Almost 20% of patients surviving transplant devel-op diabetes in the first year after the intervention, but 5 years later only 15% can be classified as diabetic. This is most likely caused by the use of decreasing doses of corti-costeroids. It has not yet been proven whether transplant patients need to be managed differently in terms of blood glucose, glycated hemoglobin, or medicinal agents used in therapy.8,9 Data from the international literature also show that hypertension after transplantation is common, with an incidence of 70–90% in patients treated with cyclospo-rine and 30–50% in those treated with tacrolimus.10,11 Both tacrolimus and cyclosporine may influence blood pressure levels and favor hyperlipidemia, as shown by Han et al.12
Regarding renal dysfunction, it has been demonstrated that immunosuppressive therapy with cyclosporine has improved graft function and survival time in transplant patients. However, cyclosporine-induced nephrotoxic-ity remains a medical challenge for post-heart transplant
management. Cyclosporine, a highly nephrotoxic immu-nosuppressive agent, causes an initially reversible decrease in glomerular filtration rate (GFR), possibly through ar-teriolar vasoconstriction. The mechanisms by which renal vasoconstriction and decreased filtration rates occur are not known, but it has been suggested that abnormalities of endogenous vasoconstrictor and vasodilator mechanisms may be responsible. In this context, an oral dose of cyclo-sporine (5 mg/kg) was found to strongly affect renal he-modynamics, both in patients with cardiac transplantation and chronic treatment and in healthy volunteers, in whom 10 mg/kg cyclosporine caused an 18% decrease in GFR. Increased serum creatinine levels due to cyclosporine may be associated with hypertension, a disproportion-ate increase in serum urea, hyperkaliemia, increased uric acid levels, mild proteinuria (usually less than 1 g/24 h), and decreased fractional sodium excretion. Increased blood pressure may be associated with decreased sodium excretion, stimulation of the renin-angiotensin system, in-creased local endothelin synthesis and/or decreased local nitric oxide synthesis. Treatment interruption or lowering the dose of cyclosporine may sometimes stabilize kidney function, but even when renal function remains stable, the morphological lesions and proteinuria may progress fur-ther.13–15 Tacrolimus, another immunosuppressive agent, is also associated with a higher risk of nephrotoxicity. This reaction may be explained by the increase in the produc-tion of oxygen free radicals that induce kidney damage.13–15
Hyperlipidemia is one of the most common metabolic dysfunctions encountered in transplanted patients, with an incidence of 60–80%. Studies show that tacrolimus and cyclosporine can influence blood pressure (hypertension) and hyperlipidemia.16–18 It has a multifactorial origin, with mechanisms dependent on abnormalities of the pre-exist-ing lipid status, cyclosporine therapy, and corticosteroids. Discontinuation of corticosteroid treatment has been shown to be associated with low cholesterol. Cyclosporine A (CsA)-induced hyperlipidemia is already known and is a clinically significant problem. CsA affects the metabolism of lipids and lipoproteins; however, the basic mechanisms that cause dyslipidemia are not well known. Additional studies are needed to help identify immunosuppressive agents that do not cause hyperlipidemia, or to support the development of strategies to effectively monitor CsA-induced hyperlipidemia.19
Youn et al. performed a retrospective analysis on 17,587 patients from the International Society of Heart and Lung Transplant (ISHLT) registry over a 10-year period (2001–2011) in order to identify the occurrence of malignant tu-mors after heart transplantation.20 Over 10% of the moni-

79Journal of Interdisciplinary Medicine 2020;5(2):76-80
tored patients have developed de novo malignancy in 1 to 5 years after transplantation. The authors reported a 12.4% increase in de novo malignancies in patients transplanted between 2006 and 2011, compared with 10% in patients treated between 2000 and 2006, resulting in an absolute increase of 2.4%. Skin cancer accounted for most of this in-crease, solid organ malignancy was responsible for a small increase, and the incidence of post-transplant lymphop-roliferative disease (PTLD) was low (approximately 1%) in both cohorts compared to the previously reported 3% to 9%.21 These results are diametrically opposed to those in pediatric heart transplant patients, in whom PTLD is the major post-transplant malignancy. This low incidence may also show that PTLD related to Epstein-Barr virus infection occurs relatively early, usually in the first year after transplantation, and in this analysis, these patients were not included. Although it has been observed that the change in immunosuppression has led to a decrease in the incidence of PTLD, the prevention and more effective treatment of infectious diseases and/or under-reporting to the ISHLT registry remains unclear.22
Thyroid diseases can also deteriorate in most heart transplant patients. After cardiac transplant, the serum levels of TSH hormone should be monitored and con-trolled in all patients, especially in those with a history of thyroid disease.23
Post-transplant pathology – infections related to immunosuppressive treatment
In transplant patients, selective inhibitors of cytokine pro-duction and function (tacrolimus, cyclosporine), immu-nosuppressive antimetabolites (mycophenolate mofetil), and antivirals (valganciclovir) are frequently used to pre-vent graft rejection.
Infections following surgery are probably the most common post-transplant pathology, the primary reason for this being the use of immunosuppressive medication. The latter depends on each patient’s predilection for rejec-tion, which has been shown to decrease exponentially over time.24 Bacteria and viruses are responsible for more than 80% of post-transplant infections.25,26 The most common bacterial infections after cardiac transplantation are noso-comial ones, caused by intravascular catheters, infected gas lines, or occult pneumonias caused by Gram-negative germs.27
In our study, microbiological tests were performed in all 53 patients, starting with the 3rd postoperative day. Twelve per cent of patients developed bacterial infections from the 7th to the 9th postoperative day, manifested by
fever and elevated acute phase inflammatory reactants and confirmed by microbiology.
The most common viral infections following cardiac surgery are generally caused by herpes viruses (CMV, her-pes zoster, and herpes simplex).28 Infections with CMV represent major causes of morbidity, being associated with a high rate of readmission after heart transplantation. In a recent study, data on cytomegalovirus infection were ana-lyzed in 1,553 patients undergoing heart transplantation from 26 centers in the Cardiac Transplant Research Data-base Group, the results indicating 230 confirmed cytomeg-alovirus infections, of which 16 were proven fatal (6%).28 In the same study, 12% of the 200 patients with CMV infec-tion had a recurrent infection during a mean follow-up of 13.9 months.28 In our study, 44.44% of patients have devel-oped a CMV infection, while 40.91% of them tested posi-tive for Toxoplasma IgG antibodies.
CoNCluSioNS
Infections following surgery are probably the most com-mon post-transplant pathology, the primary reason for this phenomenon being immunosuppressive medication. The administration of immunosuppressive agents is dependent on the patient’s predilection for the rejection reaction, which decreases exponentially over time. Our experience has shown that bacteria and viruses are responsible for over 80% of post-transplant infections. The evaluation of post-transplant cardiac complications should be a priority, as they hold a negative impact on the post-operative evolu-tion of heart transplant patients.
CoNfliCt of iNtErESt
Nothing to declare.
rEfErENCES1. Hosenpud JD, Bennett LE, Keck BM, Boucek MM, Novick RJ. The Registry
of the International Society for Heart and Lung Transplantation: eighteenth Official Report-2001. J Heart Lung Transplant. 2001;20:805-815.
2. Mangini S, Alves BR, Silvestre OM, et al. Heart transplantation: review. Einstein (Sao Paulo). 2015;13:310-318.
3. Custódio IL, Lima FE, Lopes MV, et al. Results of medium-term survival in patients undergoing cardiac transplantation: institutional experience. Rev Bras Cir Cardiovasc. 2013;28:470-476.
4. Fiorelli AI, Coelho GHB, Oliveira Junior JL, Oliveira AS. Heart failure and heart transplantation. Rev Med. 2008; 87:105-120.
5. Aranda JM Jr, Hill J. Cardiac transplant vasculopathy. Chest. 2000;118:1792-1800.
6. Wilhelm MJ. Long-term outcome following heart transplantation: current perspective. J Thorac Dis. 2015;7:549-551.
7. Lund LH, Edwards LB, Kucheryavaya AY, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-first official adult heart transplant report – 2014; focus theme: retransplantation. J Heart Lung Transplant. 2014;33:996-1008.

80 Journal of Interdisciplinary Medicine 2020;5(2):76-80
8. Marchetti P. New-onset diabetes after transplantation. J Heart Lung Transplant. 2004;23(5 Suppl):S194-S201.
9. Moro JA, Martínez-Dolz L, Almenar L, et al. Impacto de la diabetes mellitus en el paciente con trasplante cardiaco [Impact of diabetes mellitus on heart transplant recipients]. Rev Esp Cardiol. 2006;59:1033-1037.
10. Patel J, Kittleson M, Czer L, et al. Severity of Hypertension After Heart Transplant: Does It Impact Outcome? J Heart Lung Transplant. 2016;35:S295.
11. Aparicio LS, Alfie J, Barochiner J, et al. Hypertension: the neglected complication of transplantation. International Scholarly Research Notices. 2013:165937.
12. Han SY, Mun KC, Choi HJ, et al. Effects of cyclosporine and tacrolimus on the oxidative stress in cultured mesangial cells. Transplant Proc. 2006;38:2240-2241.
13. Herlitz H, Lindelöw B. Renal failure following cardiac transplantation. Nephrol Dial Transplant. 2000;15:311-314.
14. Straathof K, Anoop P, Allwood Z, et al. Long-term outcome following cyclosporine-related neurotoxicity in paediatric allogeneic haematopoietic stem cell transplantation. Bone Marrow Transplant. 2017;52:159-162.
15. van Hooff JP, Christiaans MH, van Duijnhoven EM. Evaluating mechanisms of post-transplant diabetes mellitus. Nephrol Dial Transplant. 2004;19:vi8-vi12.
16. Øzbay A. Diabetogenicity of Cyclosporine and Tacrolimus (Doctoral dissertation). Faculty of Health Sciences, Aarhus University; 2011.
17. Kockx M, Kritharides L. Cyclosporin A-induced hyperlipidemia. In: Lipoproteins-Role in Health and Diseases. Rijeka: InTech Publishers, 2012; p. 337-354.
18. Youn JC, Stehlik J, Wilk AR, et al. Temporal Trends of De Novo Malignancy Development After Heart Transplantation. J Am Coll Cardiol. 2018;71:40-49.
19. Kumarasinghe G, Lavee O, Parker A, et al. Post transplant lymphoproliferative disease in heart and lung transplantation: defining risk and prognostic factors. J Heart Lung Transplant. 2015;34:1406-1414.
20. Mancini D, Rakita V. Malignancy Post Heart Transplantation. J Am Coll Cardiol. 2018;71:50-52.
21. Simonenko M, Fedotov P, Sazonova Y, et al. Thyroid Disorders in Recipients After Heart Transplantation. Transplantation. 2018;102:826.
22. Jha V. Post-transplant infections: An ounce of prevention. Indian J Nephrol. 2010;20:171-178.
23. Montoya JG, Giraldo LF, Efron B, et al. Infectious complications among 620 consecutive heart transplant patients at Stanford University Medical Center. Clin Infect Dis. 2001;33:629-640.
24. Rostad CA, Wehrheim K, Kirklin JK, et al. Bacterial infections after pediatric heart transplantation: Epidemiology, risk factors and outcomes. J Heart Lung Transplant. 2017;36:996-1003.
25. Guggenbichler JP, Assadian O, Boeswald M, Kramer A. Incidence and clinical implication of nosocomial infections associated with implantable biomaterials – catheters, ventilator-associated pneumonia, urinary tract infections. GMS Krankenhhyg Interdiszip. 2011;6:Doc18.
26. Echenique IA, Angarone MP, Rich JD, Anderson AS, Stosor V. Cytomegalovirus infection in heart transplantation: A single center experience. Transpl Infect Dis. 2018;20:e12896.
27. Carratalà J, Montejo M, Pérez-Romero P. Infections caused by herpes viruses other than cytomegalovirus in solid organ transplant recipients. Enferm Infecc Microbiol Clin. 2012;30:63-69.
28. Kirklin JK, Naftel DC, Levine TB, et al. Cytomegalovirus After Heart Transplantation. Risk Factors for Infection and Death: A Multiinstitutional Study. The Cardiac Transplant Research Database Group. J Heart Lung Transplant. 1994;13:394-404.

Journal of Interdisciplinary Medicine 2020;5(2):81-85
CORRESPONDENCE
Alina Mioara BoeriuDepartment of Gastroenterology, County Clinical Hospital MuresStr. Gheorghe Marinescu nr. 1540103 Targu Mures, RomaniaTel +40 265 215 133E-mail: [email protected]
ARTICLE HISTORY
Received: March 14, 2020Accepted: May 15, 2020
Acute Drug-Induced Cholestatic Syndrome in Basedow Graves’ DiseaseRobert Aurelian Tiucă1, Alina Mioara Boeriu2, Rareș Adrian Georgescu3, Ionela Maria Pașcanu4
1 Clinic of Endocrinology, County Clinical Hospital Mures, Targu Mures, Romania2 Department of Gastroenterology, County Clinical Hospital Mures, “George Emil Palade” University of Medicine and Pharmacy,
Science and Technology, Targu Mures, Romania3 Department of Surgery, County Clinical Hospital Mures, “George Emil Palade” University of Medicine and Pharmacy, Science and
Technology, Targu Mures, Romania4 Department of Endocrinology, County Clinical Hospital Mures, “George Emil Palade” University of Medicine and Pharmacy, Science
and Technology, Targu Mures, Romania
CaSE rEport ENDOCRINOLOGY // GASTROENTEROLOGY
DOI: 10.2478/jim-2020-0006
ABSTRACT
Introduction: Graves’ disease (GD), an autoimmune disorder caused by high levels of auto-antibodies against the thyroid-stimulating hormone receptor, is considered the most common cause of thyrotoxicosis, characterized by features such as goiter, ophthalmopathy and der-mopathy. In our country, the administration of antithyroid drugs (ATD) is the first line of treatment in this disease. Side effects are rare but some of them, such as agranulocytosis or liver damage, may become serious. Case presentation: We report the case of a 20-year-old female patient who was diagnosed with GD after being previously diagnosed with viral hepatitis A. Treatment was initiated with methimazole 30 mg/day, and three weeks later she developed intense he-patic cytolysis and cholestatic syndrome, therefore the ATD was stopped. A suspicion of au-toimmune liver disease was raised, and a liver biopsy was performed in order to establish the diagnosis. The next therapeutic option for hyperthyroidism was radioactive iodine (RAI). Three months following RAI, the patient presented severe hypothyroidism, thereupon treatment with levothyroxine was initiated. Conclusions: Although severe acute liver injury is rare, mild liver dysfunction is quite common in patients with GD. The overproduction of thyroid hormones, or the treatment with ATD through immune mediated processes or drug reactions, represent pos-sible mechanisms responsible for liver damage.
Keywords: Graves’ disease, methimazole, hepatitis, cytolysis, cholestatic syndrome
Robert Aurelian Tiucă • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 217 274, E-mail: [email protected]
Rareș Adrian Georgescu • Str. Gheorghe Marinescu nr. 1, 540103 Targu Mures, Romania. Tel: +40 265 215 133, E-mail: [email protected]
Ionela Maria Pașcanu • Str. Gheorghe Marinescu nr. 38, 540139 Targu Mures, Romania. Tel: +40 265 217 274, E-mail: [email protected]
iNtroduCtioN
Graves’ disease (GD) is an organ-specific autoimmune disorder of unknown cause and the most common form of thyrotoxicosis. It affects women more commonly than men (5 : 1), with a peak incidence between the second and forth decade of life.1,2 Thyrotoxicosis, goiter, ophthalmopathy, and dermopa-thy are features that can be typically found in a patient with GD.1 Goiter and hyperthyroidism that appear in GD are due to a high level of circulating autoan-

82 Journal of Interdisciplinary Medicine 2020;5(2):81-85
tibodies that are directed against the thyroid-stimulating hormone (TSH) receptor in the thyroid cell membrane (TRAb).1 These autoantibodies are synthesized by B lym-phocytes in the thyroid gland, which were stimulated by the T lymphocytes.1,2 A thyroid ultrasound usually describes a diffusely enlarged, hypoechoic thyroid with increased vascularity.2 There is evidence that suggests a familial predisposition in developing GD, and environ-mental triggers include stress, tobacco use, pregnancy, viral or bacterial infections, and iodine exposure.1 Treat-ment for GD implies the use of antithyroid drugs (ATDs) such as methimazole, carbimazole, or propylthiouracil in order to reduce the high production of thyroid hor-mones.1,2 Common side effects of ATDs are itching, skin rash, and abnormal hair loss, while less common side ef-fects include muscle and joint pain, headache, swelling, and in severe cases liver injury or agranulocytosis.2 An-other treatment option for GD, which reduces the amount of thyroid tissue, is radioactive iodine treatment (RAI) or total thyroidectomy.1,2 This article aims to present the case of a young female patient with GD who had been previ-ously diagnosed with viral hepatitis A and who developed acute cholestatic syndrome after ATD use.
CaSE prESENtatioN
A 20-year-old female patient was admitted to the Infec-tious Diseases Department of Mureș Clinical County Hospital with symptoms such as nausea, vomiting, jaun-dice, and urinary hyperchromia. The laboratory workup revealed high values of direct bilirubin and total bilirubin, hepatic cytolysis, and positive immunoglobulin M anti-body to hepatitis A virus. Abdominal ultrasound showed hepatosplenomegaly, visible intrahepatic ducts, and gall-bladder wall thickening. A diagnosis of acute viral hepa-titis A was established and treatment with intravenous infusions of glucose 5% and hepatoprotective agents was initiated. The patient’s general status as well as the hepatic panel tests improved. During hospitalization, she present-ed an enlargement of the anterior cervical region, there-fore, two weeks after discharge, she was evaluated by an endocrinologist.
A thyroid ultrasound was performed, which described an increased volume, with inhomogeneous structure and enhanced vascularity, suggesting an autoimmune thy-roid disease. Blood test evaluation showed thyrotoxicosis with a TSH of 0.0090 µUI/mL (normal range: 0.55–4.78),
TABLE 1. The evolution of liver panel, bilirubin tests, and thyroid function
Time frame AST (NR: 5–34 U/L)
ALT(NR: 0–55 U/L)
GGT(NR: 12–64 U/L)
DB(NR: 0.0–0.5 mg/dL)
TB(NR: 0.2–1.2 mg/dL)
Thyroid function
Treatment received
Onset of the viral hepatitis
1516 1727 – 5.22 6.28 – Hepatoprotective drugs+
infusions with glucose 5%
2 weeks after being discharged from the Infectious Diseases Department
80 150 – 0.97 1.44 Thyrotoxicosis Hepatoprotective drugs+
introduction of ATD
3 weeks later 1393 1995 275 8.98 12.39 – Stopping methimazole Hepatoprotective drugs
+prednisone
+gastroprotective agents
+cardioactive agents
After 10 days of treatment
259 628 238 5.24 6.44 –
After 1 month from stopping ATD
46 166 97 1.36 2.22 Euthyroidism
5 months later 25 38 28 – – Relapse of the hyperthyroidism
Hepatoprotective drugs+
cardioactive agents
2 months later 34 60 36 0.44 1.1 Mild thyrotoxicosis
3 weeks after RAIHepatoprotective drugs
+ cardioactive agents
3 months later 23 30 21 – – Severe hypothyroidism
Levothyroxine
AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, gamma-glutamyl transferase; DB, direct bilirubin; TB, total bilirubin

83Journal of Interdisciplinary Medicine 2020;5(2):81-85
free thyroxine (FT4): 4.33 ng/dL (normal range: 0.89–1.76), free triiodothyronine (FT3): 14.68 pg/mL (normal range: 2.3–4.2), with high levels of anti-thyroid peroxi-dase (ATPO) of 1,571.0 UI/mL (normal range: <35) and TRAb: 33.41 UI/L (<1.75). She was eventually diagnosed with GD and treatment with 30 mg of methimazole along with 30 mg of propranolol was started.
After roughly three weeks of treatment with ATDs, the patient was admitted to the Endocrinology Department of Mureș County Clinical Hospital complaining of tired-ness, fatigue, jaundice, and urinary hyperchromia. Physi-cal examination revealed icteric sclera and skin, no signs of ascites or abdominal tenderness, negative Murphy’s sign, and no ophthalmopathy. The liver blood panel described hepatic cytolysis and cholestatic syndrome on several de-terminations (Table 1).
While the patient was admitted to our department, treatment with hepatoprotective drugs was started, whereas the treatment with ATDs was stopped. However, the patient’s general state did not improve. A suspicion of autoimmune cholangiohepatitis was raised, and the pa-tient was transferred to the Gastroenterology Department for further medical investigations.
In the Gastroenterology Department, the physical ex-amination revealed hepatosplenomegaly, normal heart
rate and blood pressure. Liver tests showed severe cy-tolysis and cholestasis. Hepatitis B and C testing, and the markers for autoimmune hepatitis and primary bili-ary cirrhosis (anti-smooth muscle antibodies, anti-liver kidney microsomal type 1 antibodies, antimitochondrial antibodies, antinuclear antibodies, anti-soluble liver anti-gen antibodies) were negative, with normal serum protein electrophoresis, prothrombin time, and albumin levels. Abdominal ultrasound depicted splenomegaly, lymphade-nopathy in the hepatic hilum, hepatomegaly, and gallblad-der wall thickening, with no obstruction of biliary ducts. Infusions with hepatoprotective agents were initiated, as well as treatment with prednisone (1 mg/kg/day) and ur-sodeoxycholic acid (10 mg/kg/day).
Liver biopsy described hepatitis with minimum necrot-ic-inflammatory activity, and minimum inflammatory in-filtrate at the portal space formed by lymphocytes, neutro-phils, and eosinophilic granulocytes (Figure 1).
Under treatment with hepatoprotective, gastroprotec-tive, and cardioactive agents, prednisone tapering regimen and ursodeoxycholic acid, the patient’s liver condition progressively improved. She was retransferred to the En-docrinology Department, where the thyroid function tests were normal, while the hepatic panel described mild cy-tolysis and cholestatic syndrome (Table 1).
FIGURE 1. The microscopic aspect of the liver biopsy

84 Journal of Interdisciplinary Medicine 2020;5(2):81-85
The patient was reevaluated after five months, when the thyroid function tests revealed a relapse of the hyper-thyroidism, whereas the liver function tests were normal. Given the medical history of the patient and the acute liver injury (ALI) secondary to the administration of ATDs, the patient was advised to undergo treatment with RAI. One month later, she received a therapeutic dose of 11.72 mCi of I-131. The patient was reevaluated three weeks later, when she was still in mild thyrotoxicosis, eventually being dis-charged without any additional ATD. Three months later, the patient presented severe hypothyroidism (TSH level of 285.746 µUI/mL and FT3 level of <0.20 pg/mL), with a low thyroid volume and normal liver functions tests, there-upon treatment with levothyroxine was initiated (Table 1).
The patient agreed to the publication of her medical information, the manuscript being written respecting the ethical principles stated in the Declaration of Helsinki.
diSCuSSioNS
We report the case of a 20-year-old female patient who was diagnosed with GD. Prior to the diagnosis, the patient had viral hepatitis A, which required the admission to the In-fectious Diseases Department. ATDs are usually the first-line treatment option with remission rates ranging from 14% to 80%, the recommended duration of therapy being 12–18 months.2,3 In our case, the treatment was started with methimazole 30 mg/day alongside with propranolol 30 mg/day. Our patient had slightly elevated liver func-tion tests before initiating the ATD, most probably due to thyrotoxicosis; nevertheless, three weeks after starting the medication, she developed jaundice, urinary hyperchro-mia, and fatigue, suggesting an ALI.
The incidence of hepatotoxicity associated with the use of any ATD is low (<0.5%), propylthiouracil being the thi-onamide that is reported to have a higher risk of serious, non-dose related liver injury, especially in pediatric pa-tients. The risk of liver failure is 1 in 2,000 children and 1 in 10,000 adults.4,5 On the other hand, methimazole toxicity is found more often in patients over 40 years of age, with no reported deaths from liver failure.4 In the literature, there are several studies that have observed the hepatotox-icity profiles of methimazole vs. propylthiouracil. A study conducted in Japan found a 6.6% incidence of methima-zole-induced hepatotoxicity from 30 mg/day compared to 26.9% in case of propylthiouracil at 300 mg/day.4,6 Wang et al. reported that hepatitis had a higher incidence rate than acute liver failure (ALF) when comparing methimazole vs. propylthiouracil.7 Moreover, methimazole use, especially in high dose, associated an increased risk of hepatitis when
compared with any propylthiouracil use.7 Rivkees & Szarf-man reported that methimazole had a higher rate of mild liver injury (cytolysis, jaundice, or cholestasis) but a lower rate of severe liver injury (hepatitis, ALF, or liver trans-plant) than propylthiouracil.8
A first hypothesis in the mechanism of developing an ALI in patients with GD is that hyperthyroidism can cause liver damage directly by increasing the metabolic rate, resulting in a higher oxidative capacity and oxidative tissue damage.1 Oshima et al. reported in 1990 an autopsy case of death due to hyperthyroidism in which the autopsy revealed he-patic inflammation, fibrosis, and centrilobular necrosis.9–11 Hyperthyroidism increases the production of insulin-like growth factor within the liver, resulting in a hypermetabolic state that can make the liver more prone to injury.12
A second hypothesis in developing an ALI after start-ing treatment with methimazole could be related to the implication of an immune-mediated process and/or drug reactions, though the exact mechanism is not yet fully un-derstood.4 In 2004, Mikhail reported a case of a 43-year-old woman who developed severe, though reversible choles-tatic jaundice after 4 weeks of treatment with methimazole, with an improvement in general state after stopping the medication.13 Drug-induced liver injury due to methima-zole is reported more often in the first weeks after starting the treatment, the injury having usually a cholestatic type pattern with symptoms such as jaundice, fatigue, pruri-tus, and malaise.4,13–15 Chang et al. reported that elevated TRAb levels might predispose the patient to carbimazole/methimazole-induced cutaneous reactions and/or hepato-toxicity.16 Heidari et al. found that mice that were treated with a nonhepatotoxic dose of bacterial lipopolysaccharide (LPS) from E. coli as well as with ATD in nonhepatotoxic doses, presented with hepatic inflammation that eventu-ally led to ALI.17 LPS can stimulate toll-like receptors and activate the Kupffer cells that could damage the hepato-cytes and furthermore, produce inflammatory cytokines and proteolytic enzymes.17 After the inhibition of Kupffer cells by methyl palmitate, methimazole-induced hepato-toxicity as well as propylthiouracil-induced liver injury in LPS-treated mice diminished.17
A third hypothesis for the onset of an ALI is the pres-ence of an underlying autoimmune disease that causes se-rious damage to the liver such as an autoimmune hepatitis. In order to diagnose an autoimmune liver disease, autoim-mune markers and liver biopsy are needed.10 In our case, biopsy found no specific microscopic features for autoim-mune hepatitis, and serum tests were negative.
In our case, the most plausible hypothesis for the oc-currence of ALI is that the recent history of viral hepatitis

85Journal of Interdisciplinary Medicine 2020;5(2):81-85
A, concurrent with the consecutive administration of me-thimazole, led to the development of an acute cholestatic syndrome.
Another treatment option for hyperthyroidism is based on reduction of the amount of thyroid tissue with either RAI or thyroidectomy, especially in patients with relaps-ing hyperthyroidism after stopping the ATD.2 RAI for GD is a safe form of treatment, though with a latency period that can last up to 6 months.3 Sundaresh et al. conducted a retrospective study on 720 patients and reported a failure rate in correcting the hyperthyroidism of 48.3% for ATD treatment compared with 8% for RAI.18 Nearly 3 months after RAI, our patient developed severe hypothyroidism, and treatment with levothyroxine was initiated.
CoNCluSioNS
Although severe ALI is rare, mild liver dysfunction is quite common in patients with GD. Overproduction of thyroid hormones, or treatment with ATD through immune-mediated processes or drug reactions represent possible mechanisms responsible for liver damage. Liver tests mon-itoring during ATD therapy is recommended, especially in patients with prior liver dysfunction. In cases where ATDs are not indicated, definitive treatment with either RAI or total thyroidectomy may represent effective therapeutic options. Although hypothyroidism is a complication of the definitive treatment, management of this condition may be easier than the one of hyperthyreosis.
CoNfliCt of iNtErESt
Nothing to declare.
aCkNoWlEdGEmENt
We acknowledge the cooperation of Prof. Dr. Ovidiu Si-mion Cotoi and Dr. Mihaela Șincu for performing the
pathological evaluation, which played an important role in elucidating the final diagnosis.
rEfErENCES
1. Cooper D, Landenson P. The thyroid gland. In: Gardner D, Shoback D, ed. Greenspan's Basic & Clinical Endocrinology. 10th ed. McGraw-Hill Education, 2017; p. 171-239.
2. Kahaly G, Bartalena L, Hegedüs L, Leenhardt L, Poppe K, Pearce S. 2018 European Thyroid Association Guideline for the Management of Graves’ Hyperthyroidism. Eur Thyroid J. 2018;7:167-186.
3. Cipolla C, Graceffa G, Calamia S, et al. The value of total thyroidectomy as the definitive treatment for Graves’ disease: A single centre experience of 594 cases. J Clin Transl Endocrinol. 2019;16:100-183.
4. Akmal A, Kung J. Propylthiouracil, and methimazole, and carbimazole-related hepatotoxicity. Expert Opin Drug Saf. 2014;13:1397-1406.
5. Karras S, Memi E, Kintiraki E, Krassas G. Pathogenesis of propylthiouracil-related hepatotoxicity in children: present concepts. J Pediatr Endocrinol Metab. 2012;25:623-630.
6. Nakamura H, Noh J, Itoh K, Fukata S, Miyauchi A, Hamada N. Comparison of Methimazole and Propylthiouracil in Patients with Hyperthyroidism Caused by Graves’ Disease. J Clin Endocrinol Metab. 2007;92:2157-2162.
7. Wang M, Lee W, Huang T, Chu C, Hsieh C. Antithyroid drug-related hepatotoxicity in hyperthyroidism patients: a population-based cohort study. Br J Clin Pharmacol. 2014;78:619-629.
8. Rivkees S, Szarfman A. Dissimilar Hepatotoxicity Profiles of Propylthiouracil and Methimazole in Children. J Clin Endocrinol Metab. 2010;95:3260-3267.
9. Oshima T, Maeda H, Takayashu T, et al. An autopsy case of sudden death due to hyperthyroidism. Nihon Hoigaku Zasshi. 1990;44:365-370.
10. Heidari R, Niknahad H, Jamshidzadeh A, Eghbal M, Abdoli N. An Overview on the Proposed Mechanisms of Antithyroid Drugs-Induced Liver Injury. Adv Pharm Bull. 2015;5:1-11.
11. Chen W, Zhu Z, Wang C, Chien M. Cholestasis and Acute Cholecystitis in Hyperthyroidism Treated With Methimazole. Int J Gerontol. 2009;3:248-250.
12. Tseng F, Chen Y, Chi Y, Chen P, Yang W. Serum levels of insulin-like growth factor 1 are negatively associated with log transformation of thyroid-stimulating hormone in Graves’ disease patients with hyperthyroidism or subjects with euthyroidism. Medicine (Baltimore). 2019;98:e14862.
13. Mikhail N. Methimazole-induced Cholestatic Jaundice. South Med J. 2004;97:178-182.
14. Li X, Jin S, Fan Y, et al. Association of HLA-C*03:02 with methimazole-induced liver injury in Graves’ disease patients. Biomed Pharmacother. 2019;117:109095.
15. Cooper D. Antithyroid Drugs. N Engl J Med. 2005;352:905-917.16. Chang L, Chang C, Chen P, et al. Thyrotropin receptor antibodies and a
genetic hint in antithyroid drug-induced adverse drug reactions. Expert Opin Drug Saf. 2018;17:775-784.
17. Heidari R, Ahmadi F, Rahimi H, et al. Exacerbated liver injury of antithyroid drugs in endotoxin-treated mice. Drug Chem Toxicol. 2018;42:615-623.
18. Sundaresh V, Brito J, Thapa P, Bahn R, Stan M. Comparative Effectiveness of Treatment Choices for Graves' Hyperthyroidism: A Historical Cohort Study. Thyroid. 2017;27:497-505.

About JIM
Editorial proCESS
All manuscripts submitted to the Journal of Interdisciplin-ary Medicine ( JIM) will be first subject to a technical re-view, including quality check of all the files submitted, in-cluding tables, figures and references. Plagiarism check will be performed prior to referring the manuscript for review, in order to identify any possible fraud or scientific misconduct.
After technical review and anti-plagiarism assessment, the articles will be referred for review following a double-blinded review procedure. Reviewers can be suggested by the authors, however selection of the reviewers will be made by the editors, according to their expertise in the field of the article. The identity of the reviewers will not be disclosed to the authors, as well as the identity of the authors will not be disclosed to the reviewers.
The possible editorial decisions following the review procedure are: accepted, minor revisions required, major revisions required or rejected.
The editorial decision will be communicated to the au-thors as soon as the review process has been finalized. In case of revisions, the revised article will be sent to the reviewers, who will decide on a new recommendation for revision, ac-ceptance or rejection. The estimated time from the submis-sion to first decision is approximately 4 weeks, and from the final revision to acceptance approximately 2 weeks.
Prior to publication, all corresponding authors will re-ceive a proof of their article in order to confirm the accu-racy of the text or suggest modifications.
publiCatioN EtHiCS aNd publiCatioN
malpraCtiCE StatEmENt
The Journal of Interdisciplinary Medicine adheres to the COPE principles of transparency and best practice in scholarly publishing. The Journal ensures an equal treat-ment for all articles by the Editor, Editorial team and jour-nal reviewers, and has strict rules for confidentiality, dis-closures, conflict of interest and authorship. At the same time, the Journal has strict regulations against publication fraud and plagiarism and well defined procedures to be taken if a publication fraud is suspected.
Conflict of interest
All participants in the peer-review and publication process — not only authors but also peer reviewers, editors, and editorial board members of journals — must consider their conflicts of interest when fulfilling their roles in the pro-cess of article review and publication and must disclose all relationships that could be viewed as potential conflicts of interest.
A conflict of interest exists when professional judgment concerning a primary interest (such as patients’ welfare or the validity of research) may be influenced by a secondary interest (such as financial gain). Perceptions of conflict of interest are as important as actual conflicts of interest.
All manuscripts must acknowledge any possible conflict of interest related to the manuscript. If there is no conflict of interest in relation to the work performed or to the prep-aration of the manuscript, the authors should state that there are no conflict oif interest in relation to the manu-script. All the authors should also acknowledge any kind of material support, financial support or funding grants related to the work described in the manuscript.
Reviewers will be asked at the time they are asked to critique a manuscript if they have conflicts of interest that could complicate their review. Reviewers must disclose to editors any conflicts of interest that could bias their opin-ions of the manuscript, and should recuse themselves from reviewing specific manuscripts if the potential for bias exists. Reviewers must not use knowledge of the work they’re reviewing before its publication to further their own interests.
Editors and Journal Staff Editors who make final de-cisions about manuscripts will recuse themselves from editorial decisions if they have conflicts of interest or re-lationships that pose potential conflicts related to articles under consideration. Editorial staff will not use informa-tion gained through working with manuscripts for pri-vate gain.
In cases where the Managing Editor has any conflict of interest in connection with a manuscript, the entire work related to the review process of that manuscript will be undertaken by the Editor-in-Chief. In cases where the

Editor-in-Chief has any conflict of interest in relation to a manuscript, the entire work related to the review process of that manuscript will be undertaken by the Managing Editor. In cases where both the Managing Editor and the Editor-in-Chief have any conflict of interest in relation to a manuscript, the entire work related to the review process of that manuscript will be undertaken by another member of the editorial board.
Submissions from members of the editorial board, edi-tors and employees of the journal will be handled by the Editor-in-Chief, who will allocate the manuscripts for re-view to independent and blinded reviewers. Submissions from members of the owner institution will be assigned for review to members of the editorial board or external reviewers, taking into consideration the necessity to avoid any potential conflict of interest in the process of reviewer allocation.
Editorial manuscripts sent by members of the editorial board, following an invitation by the Editor-in-Chief, will undergo a review process in the editorial office.
Confidentiality
Editors of JIM will not share information regarding the manuscripts submitted to JIM to any other than the au-thors and the reviewers.At the time of reviewer allocation, reviewers will be instructed to keep the manuscripts and associated material strictly confidential. Reviewers should not publicly discuss author`s work and must not retain any manuscript for their personal use.
In case of manuscript rejection, the full content of the manuscript will be deleted from the editorial content of the Journal. In case of manuscript acceptance and publi-cation, the Journal will keep copied of all the manuscript-related materials for at least three years.
The identity of the reviewers will not be revealed to au-thors, under no circumstances.
Human and animal rights
The authors should make sure that all the experiments on humans or animals are in accordance with the guiding principles described in the Declaration of Helsinki. Ani-mal experiments should comply with the institutional and national guidelines or regulations for laboratory animals. Informed consent should be obtained from all the subjects participating in any experiment or clinical study and all the clinical studies should obtain the approval from the eth-ics committee of the institutions where the study is carried out, prior to initiation of experiments or studies.
When reporting research involving human data, authors should indicate whether the procedures followed have been assessed by the responsible review committee (institutional and national), or if no formal ethics committee is available, were in accordance with the Helsinki Declaration as revised in 2013 (www.wma.net/en/30publica tions/10policies/b3/index.html). If doubt exists whether the research was con-ducted in accordance with the Helsinki Declaration, the authors must explain the rationale for their approach and demonstrate that the institutional review body explicitly approved the doubtful aspects of the study.
When reporting experiments on animals, authors should indicate whether institutional and national standards for the care and use of laboratory animals were followed. Fur-ther guidance on animal research ethics is available from the International Association of Veterinary Editors' Con-sensus Author Guidelines on Animal Ethics and Welfare (http://veteditors.org/ethicsconsensusguidelines.html).
Protection of research participants
In order to respect the patient's right to privacy, no informa-tion related to patients' identification data, such as names, images or hospital identification codes should be included in the manuscript, unless there is a clear written approval ob-tained from the patient for this. This signed approval should be sent to the editorial office along with the manuscript.
Identifying information, including names, initials, or hospital numbers, should not be published in written de-scriptions, photographs, or pedigrees unless the informa-tion is essential for scientific purposes and the patient (or parent or guardian) gives written informed consent for publication. Informed consent for this purpose requires that an identifiable patient be shown the manuscript to be published. When informed consent has been obtained, it should be indicated in the published article.
Scientific misconduct
Scientific misconduct includes but is not necessarily lim-ited to data fabrication; data falsification including decep-tive manipulation of images; and plagiarism. All manu-script submitted to JIM will be first subject to a plagiarism check, that will be performed prior to referring the man-uscript for review, in order to identity any possible fraud or scientific misconduct. The journal will use highly spe-cialized anti-plagiarism softwares and if any suspicion of scientific misconduct is identified, the standard procedure recommended by COPE (Committee on Publication Eth-ics) will be followed.

Clinical trials
Authors of manuscripts related to clinical trials should reg-ister the clinical trial in the official clinical trial related pub-lic registries prior to submission to JIM, following the rules stated by the International Committee of Medical Journal
Editors. Information related to registration of clinical trials can be found at ClinicalTrials.gov. In case of clinical trials, the trial registration number should be mentioned at the end of the abstract. Whenever a trial registration number is available, the authors should list this number the first time they use the trial acronym.

maNuSCript SubmiSSioN
All manuscripts should be submitted via email to [email protected].
The journal does not have article processing charges nor article submission charges.
The submission should include the following attachments:1. Cover letter: all manuscripts submitted to JIM should be accompanied by a cover letter, signed by the corre-sponding author on behalf of all co-authors, stating that the reported study and manuscript are original and have not been published elsewhere, and the manuscript has not been submitted “in extenso” to any other journal. All disclosures relating to the preparation of the manuscript should be mentioned in the cover letter. The correspond-ing author should state clearly whether or not there are any conflicts of interest.2. License to publish: The Journal of Interdisciplin-ary Medicine requires authors of original papers to as-sign copyright of their published contributions to the journal. A model of the License to Publish is available at www.interdisciplinary.ro.
Authorship is based on the following 4 criteria:
1. Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
2. Drafting the work or revising it critically for important intellectual content; AND
3. Final approval of the version to be published; AND4. Agreement to be accountable for all aspects of the work
in ensuring that questions related to the accuracy or in-tegrity of any part of the work are appropriately inves-tigated and resolved. In addition to being accountable for the parts of the work he or she has done, an author should be able to identify which co-authors are respon-sible for specific other parts of the work. In addition, authors should have confidence in the integrity of the contributions of their co-authors. All those designated
as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors. Those who do not meet all four criteria should be acknowledged.
If authors request removal or addition of an author after manuscript submission or publication, journal editors should seek an explanation and signed statement of agree-ment for the requested change from all listed authors and from the author to be removed or added.
The corresponding author is the one individual who takes primary responsibility for communication with the journal during the manuscript submission, peer review, and pub-lication process, and typically ensures that all the journal’s administrative requirements, such as providing details of au-thorship, ethics committee approval, clinical trial registra-tion documentation, and gathering conflict of interest forms and statements, are properly completed, although these du-ties may be delegated to one or more coauthors.
Authors should not submit the same manuscript simul-taneously to more than one journal, in the same or differ-ent language.
maNuSCript typES
The Journal of Interdisciplinary Medicine accepts the fol-lowing categories of articles:
Original research
Manuscripts should be word processed. The manuscript must contain the title of the article, the authors' names, qualifications and address/es.
Peer Review: all articles undergo initial screening for suitability for the Journal of Interdisciplinary Medicine.
The length of contributions: ideally contributions should be no more than 4,000 words, including tables and figures. Suitable papers are then peer reviewed by two or more referees. Additional specialist advice may be sought if necessary, for example, from a statistician, before a final decision is made by the Editor-in-Chief.
Instructions for authors

An original research article should include a short Abstract of no more than 300 words, using the follow-ing headings: Background, Aim of the study, Material and Methods, Results and Conclusions.
The manuscript should be structured as follows:1. Introduction/Background: This introduces the aim
of the study and the corresponding research hypothesis/es.2. Material and methods: This section should describe
all experimental details, research methodology, and study groups. The methodology should be detailed enough to al-low reproducibility of the experiments. Give full descrip-tions of all equipment used (type, manufacturer, town, country). Details of statistical analysis should be reported here together with a level of significance [α value]. Authors should provide details of the statistical software package used (name, version, producer, town, country). Abbrevia-tions of standard SI units of measurement should be em-ployed. Declaration of Helsinki: The authors should state that their study complied with the Declaration of Helsinki, that the locally appointed ethics committee approved the research protocol and that written informed consent was obtained from the subjects (or their guardians) before the commencement of the study. Where animals are involved, the authors should state that their study complies with their institutional guidelines for the care and use of labora-tory animals.
3. Results: This section should present the data arising from the experiments and their statistical significance. Do not discuss these findings in the Result Section.
4. Discussions: This section should contain a detailed analysis and interpretation of the results. Results should not be repeated in the Discussion section.
5. Conclusions: This presents the conclusions deriving from the outcome of the study and their clinical signifi-cance if appropriate.
Case reports
Case reports are intended for the presentation of interesting cases of interdisciplinary medicine encountered in clinical practice and should refer to actual and uncommon cases.
The report should have an abstract limited to 200 words, structured in the following manner: Introduction, Case presentation, and Conclusions.
The manuscript should be no more than a maximum of 2000 words, excluding references, figures, and figure leg-ends. It should be structured as Introduction, Case presen-tation, Discussions, and Conclusions.
A case presentation should have a maximum of four au-thors, twenty references, and five figures.
Case series
Case series should include an abstract limited to 200 words, structured into Introduction, Case series presentation, and Conclusions.
The manuscript should be no more than 2000 words ex-cluding references, tables, figures and figure legends. Case series should have a maximum of four authors, twenty ref-erences, and five figures.
Case report / Image focus
This category is intended to facilitate the publishing of representative images related to any clinical pathology. Ac-cepted images may be published on the cover of the Jour-nal. Images should be submitted as a figure accompanied by a clinical message that contains a description of the case and a detailed explanation of the figure, using a maximum of 300 words. For Case report / Image focus, the number of authors should be limited to four and the number of refer-ences to 10.
Reviews
The Journal of Interdisciplinary Medicine publishes review papers in any medical field of interest at an international level. Review articles should include a non-structured ab-stract of no more than 200 words with a maximum of 6000 words excluding references, tables, and figures.
Clinical update
The Journal of Interdisciplinary Medicine publishes up-date articles that describe current advances in any clinical field related to interdisciplinary medicine. Articles should include a non-structured abstract of no more than 200 words with a maximum of 4500 words excluding referenc-es, tables, and figures.
Letter to the editor
Letters to the editor should address either a recently published article in the Journal of Interdisciplinary Med-icine, or a new topic in the field of cardiovascular emer-gencies.
Concerning a letter, discussing a recently published article, the comments contained in the letter will be for-warded to the authors of the original paper who will be invited to respond. Any response will be published in the same journal issue as the letter to the editor. A letter to the

editor should be no longer than 500 words, 5 references, and three authors. No abstract is required.
Editorial
Editorials should address either a particular topic that is currently of interest in the field of interdisciplinary medi-cine or to an article which is published in the same issue of the journal. The number of references should not exceed twenty-five in total.
maNuSCript CoNtENt
Style and spelling: Authors, whose first language is not English, are requested to have their manuscripts checked carefully, preferably by an English native-speaker, before submission, to expedite the review process.
Manuscript format: The manuscript must be submitted as a Word document and should be presented in the follow-ing order:
•Title page.•Abstract, or a summary of case reports (references
should not be included in abstracts or summaries).•Main text separated under appropriate headings and
subheadings using the following hierarchy: BOLD CAPS, bold lower case, Plain text, italics.
•Tables should be in Word format and placed in the main text where the table is first cited. Tables must be cited in the main text in numerical order.
•Acknowledgements, Competing Interests, Funding, and all other required statements.
•Reference list. • Images must be uploaded as separate files (view
further details under the Figures/illustrations sec-tion). All images must be cited within the main text in numerical order, and legends should be provided at the end of the manuscript. Appendices should be uploaded using the File Designation “Supplementary File” and cited in the main text.
The contents of your manuscript should be arranged in the following order:
1. Title page – should include: (1) the title of the arti-cle; (2) the name(s) of authors; (3) the institutional affiliations of the authors; (4) the position, institu-tion, and location of all authors; (5) the telephone number, fax number and e-mail address of the cor-responding author; (6) disclosure of grants, contracts
and any other form of financial support received for the study.
2. Abstract – an abstract prepared in accordance to the type of the manuscript.
3. Keywords – between 3 and 6 keywords.4. Full text – All manuscripts should be typed double-
spaced, in Times New Roman 12 fonts, using Word format. References, tables and figures should be ci-ted in numerical order, as they appear in the text. The abbreviations should be explained the first time they appear in the text, followed by the abbreviation in brackets.
5. Acknowledgements – should indicate clearly any source of funding received for the study, including grants, research contracts or any form of financial support.
6. References. References should be cited in numerical order, as they appear in the text, and should be indi-cated in superscript following the end of the sentence or the end of the part of the phrase they refer to.
7. Tables should be typed on separate pages at the end of the manuscript and should be numbered in Ara-bic numerals in the order of mention in the text. The abbreviations used in the table should be explained in a footnote below the table. Tables should not repeat the text and should be clear enough to be self-expla-natory.
8. Figures should be prepared in TIF or JPG format, at a resolution of minimum 300 dpi. For figures repro-duced or adapted from another source, this should be labeled as "Reproduced with permission from…" or "Adapted with permission from…" and should be accompanied by written permission from both the author and publisher of the original material. Figures should be combined with a legend which clearly de-scribes the illustration.
rEfErENCE StylE
The journal will publish the reference list according to the style of Index Medicus (or spelled out if not listed in Index Medicus). List all the authors in each reference following the format and punctuation indicated below as examples:
Reference to an article 1. Benedek I, Gyongyosi M, Benedek T. A prospective regional registry of ST-elevation myocardial infarction in Central Romania: impact of the Stent for Life Initia-tive recommendations on patient outcomes. Am Heart J. 2013;166:457-465.
Reference to a book2. Nichols WW, Rourke MF. Aging, High Blood Pressure and Disease in Human. 3rd ed. London/Melbourne: Lea and Febiger; 1990.
Reference to a chapter in a book3. Nichols WW, O'Rourke MF. Aging, high blood pres-sure and disease in humans. In: Arnold E, ed. McDonald's Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles. 3rd ed. London/Melbourne/Auck-land: Lea and Febiger, 1990; p. 398-420.
Reference to a webpage 4. Panteghini M. Recommendations on use of bio-chemical markers in acute coronary syndrome: IFCC proposals. eJIFCC 14. http://www.ifcc.org/ejifcc/vol14no2/1402062003014n.htm (28 May 2004)
ComplaiNtS
In cases where the authors wish to file a complaint, please contact the editorial office:
Journal of Interdisciplinary MedicineStr. 22 Decembrie 1989 nr. 76–78, Târgu Mureș, Romania E-mail: [email protected]
Please describe the reason for complaining and specify the address for correspondence. Where the complaint is related to the editorial process, related to a manuscript, please include the name of the manuscript and the date the manuscript was submitted. The Editor-in-Chief, together with the editorial office will analyze the complaint and will answer in maximum three working days.