VMS Centerline ASTRO 07 - Varian · V ar inM edc lSy stm. ... Dallas,Texas.Varianshowcasedthe...
24
Paperless Medical Records: Two New Cancer Centers Rely on ARIA Treating Challenging Cases at Stanford University Cancer Center RapidArc * The Next Dimension in Speed and Precision
Transcript of VMS Centerline ASTRO 07 - Varian · V ar inM edc lSy stm. ... Dallas,Texas.Varianshowcasedthe...

Paperless MedicalRecords: Two New CancerCenters Rely on ARIA
Treating ChallengingCases at Stanford UniversityCancer Center
RapidArc*TheNextDimension inSpeed and Precision

CENTERLINE
Centerline magazine ispublished twice a year byVarian Medical Systems,http://www.varian.com.
Centerline welcomes letters tothe editor, contributions forpoint-of-view commentaries,and suggestions for articles.Reprinting of Centerline articlesmay take place with permissionfrom the editor. Address com-ments, contributions, inquiriesabout reprints and permissions,subscription requests, andaddress changes to:
Varian Medical Systems3100 Hansen Way, M/S MGMPalo Alto, CA 94304-1038Attn: Meryl Ginsberg
+1 650.424.6444
ON THE COVER
Varian’s new RapidArc™delivery* will improve doseconformity while significantlyshortening treatment times.Cover photo by Weinberg-Clark Photography.
* Pending FDA 510(k) approval;not available for sale in theUnited States at this time.
© 2007 Varian MedicalSystems, Inc. All rightsreserved.
Clinac, On-Board Imager,Trilogy, Varian, and the VarianMedical Systems logo are regis-tered trademarks and Acuity,ARIA, BrachyVision, DART,Eclipse, GammaMedplus,Implant View, PortalVision,RapidArc, RPM, SmartSegmentation, Tx, VariSeed,and VariSource are trademarksof Varian Medical Systems, Inc.ExacTrac, iPLAN, and Novalisare registered trademarks ofBrainLAB AG. The names ofother companies and productsmentioned herein are used foridentification purposes onlyand may be trademarks orregistered trademarks of theirrespective owners.
C O N T E N T S O C T O B E R 2 0 0 7
FEATURES
Eclipse in Practice 6
At Australia’s University of Newcastle, RTstudents use Eclipse™ software to help developthe knowledge and skills they need to work inclinical environments.
Treating Challenging Cases 9
Clinicians at the Stanford University CancerCenter use Varian IGRT technologies to treatlung and pancreatic cancer.
Research Collaborations 12More than a quarter ofthe presentations at arecent AAPM meetingfeatured research supportedby Varian or performed usingVarian technologies.
Paperless Medical Records 16Two new comprehensive cancer centers areoperating without film or paper. Both designedtheir processes and workflow around the ARIA™oncology information system.
Focus on Service 19In the second of a series on Varian services,Centerline looks at how installation times for
IGRT upgrades andnew machines arebeing cut in half.
DEPARTMENTS
Point of View 1What multislicedid for CT scanning,RapidArc™ deliverywill do for radiationtherapy. Varian’sCorey Zankowski,PhD, explains.
News
ASTRO Round-Up 2A look at the new capabilities Varianshowcased at the 2007 ASTRO meeting:RapidArc, the iX line of HDR afterloaders,updated VariSeed™ LDR brachytherapyplanning software, and the high-definitionmultileaf collimator.
ARIA Demonstrated at ASCO 4At a recent ASCO electronic health recordssymposium, Varian was invited to demonstratethe ARIA oncology information system.
Varian and BrainLAB BundleRadiosurgery Products 4The new Novalis® Tx combines the mostsuccessful Varian and BrainLAB radiosurgerytechnologies for imaging, treatment planning,and treatment delivery.
First IGRT School Held in UK 5Varian and the Clatterbridge Centre forOncology kicked off a new set of IGRTprograms for European clinicians, physicists,and radiographers.
Training Updates 21

C ENTER L I N E | O C TO B E R 2 0 0 7 1
R apidArc*, a major advancethis year from Varian MedicalSystems, will improve dose con-
formity while significantly shorteningtreatment times. RapidArc will achievea physician’s treatment objectives betterthan today’s best IMRT techniques—two to eight times faster than our fastestdynamic treatments can be deliveredtoday. What multislice did for CT scan-ning, RapidArc will do for radiationtherapy.
Volumetric modulated arc therapy
RapidArc is a volumetric arc therapy that delivers a preciselysculpted 3D dose distribution with a single 360-degree rotationof the linear accelerator gantry. It is made possible by a treat-ment planning algorithm that simultaneously changes threeparameters during treatment: the rotation speed of the gantry,the shape of the treatment aperture using the movement ofmultileaf collimator leaves, and the delivery dose rate.
Volumetric modulated arc therapy differs from existingtechniques like helical IMRT or intensity-modulated arc thera-py (IMAT). Helical IMRT treatments apply dose in thick over-lapping slices that take more time to deliver. IMAT, which usesfive to seven concentric arcs to deliver a conformal dose distri-bution, takes up to five times longer to deliver than a treatmentusing RapidArc, which delivers dose to the whole volume ratherthan slice by slice.
Although it represents a major advance in radiotherapytreatment technology, RapidArc is easy to implement. Itrequires no major process changes from the physician, physi-cist, dosimetrist, or therapist, as the steps for planning anddelivering treatments are virtually unchanged.
From funded research to product roadmap
Varian began looking for different ways to deliver a single-arcIMRT treatment more than five years ago. Our objective was totreat the tumor as conformally as possible in the least amountof time, while being extremely efficient in the amount of radia-tion dose used. Our requirements were stringent:
• Use nearly every degree in a 360-degree arc to providethe best chance of finding the optimal dose distributionfor the patient.
• Simultaneously modulate the shape of thetreatment aperture, the dose rate at eachgantry angle, and when necessary, thegantry speed.
• Minimize the total monitor units requiredto generate the optimal dose distribution.
• Minimize the treatment delivery time.
• Calculate the optimal plan in a clinicallyuseful time frame (less than 60 minutes).
Some early solutions gave us the dose distri-butions we needed, but they took too long toplan. Other solutions required multiple arcs and
isocenters, which took too long to deliver and were too compli-cated to be practical. Work by Cedric Yu, DSc, at the Universityof Maryland demonstrated that single-arc IMRT could equal orexceed the target volume coverage achievable with conventionalmultiple-field IMRT. Finally, thanks to some important innova-tions by physicist Karl Otto, PhD, as well as productive, spon-sored research projects at the British Columbia Cancer Agencyand the University of Maryland, we now have an efficient, accu-rate, elegant treatment planning algorithm that meets all of ourrequirements.†
The new RapidArc planning algorithm carefully exploitsmany of the characteristics of Varian’s modern linear accelera-tors and multileaf collimators, including:
• Leaf interdigitation, which is uniquely possible with aVarian multileaf collimator
• Varian’s dynamic “sliding window” approach to beamshaping
• Varian’s patented “gridded gun,” which makes it possibleto vary the dose rate as a function of the gantry angle
Varian sponsored the RapidArc research and developmenteffort with a primary goal of improving clinical outcomes.In the process, we discovered that we could improve doseconformity and simultaneously improve treatment efficiencysignificantly, as RapidArc delivery is anywhere from two toeight times faster than was possible before. We are pleased tohave introduced this exciting new development at this year’sASTRO meeting in Los Angeles. �
Corey Zankowski, PhD, is senior director of software systems marketing atVarian Medical Systems.
* Pending FDA 510(k) approval; not available for sale in the United States at this time.† Researchers Karl Otto, PhD, James Morris, MD, and Tom Keane, MD, of the BritishColumbia Cancer Agency, and William Regine, MD, and Cedric Yu, PhD, of theUniversity of Maryland Cancer Center, contributed to this project through researchfunded in part by Varian Medical Systems.
PO
IN
TO
FV
IEWVarian’s New RapidArc™ Delivery:
The Next Dimension in Speed and PrecisionBy Corey Zankowski, PhD
2 C ENTER L I N E | O C TO B E R 2 0 0 7
ASTR
OR
OU
ND-U
P
RapidArc* is a major advancethat will enable clinicians toimprove dose conformity andsignificantly shorten treatmenttimes. RapidArc delivers a com-plete intensity-modulated radi-ation treatment during a single360-degree rotation of the lin-ear accelerator gantry aroundthe patient.
RapidArc is made possible by apowerful new software algo-rithm that can control changesin three parameters simultaneously: 1) the speed of the gantryrotation, 2) the shape of the aperture created by the movementof multileaf collimator (MLC) leaves, and 3) the dose delivery rate.
“The algorithm is designed to generate highly conformal dosedistributions while taking advantage of the specific capabilitiesof the Varian linear accelerator,” says Karl Otto, PhD, medicalphysicist, British Columbia Cancer Agency (BCCA), a researcherand major contributor to RapidArc R&D efforts. “The speed ofMLC motion, gantry rotation speed, and dose rate are all usedby the algorithm to ensure the treatment is delivered efficientlyand accurately.”
Varian researchers have found that RapidArc dose distributionsare fast to deliver, and they are equivalent to or better than con-ventional IMRT or helical IMRT for a variety of clinical sites. Inone example, a multitarget cancer of the nasopharynx, RapidArcplans were found to be equivalent or better at target coveragefor all targets, and superior in protecting critical structuresincluding the spinal cord, brain stem, eyes, optic nerve and chi-asm, parotid glands, and brain. In this test, the RapidArc deliverytook only 110 seconds and used only 585 monitor units (MUs).Other tests showed that even complex RapidArc treatment planscan be delivered in less than 2.5 minutes, with fewer than 750MUs. In comparison, Varian’s best IMRT treatments, delivered onefield at a time, require approximately one minute per field todeliver, while the average multislice helical IMRT treatmentrequires 10 to 15 minutes.
“Previous approaches to arc IMRT therapy have been restrictive.Some are limited by machine design, and deliver treatmentsin the axial plane only, making it impractical to treat certain
anatomical sites,” saysWilliam F.Regine, MD, professor and chair-man of the Department ofRadiation Oncology at theUniversity of Maryland School ofMedicine and chief of radiationoncology at the University ofMaryland Medical Center, whereresearch into single-arc dosepainting has been taking placefor some time. “Varian’s technol-ogy for image-guided radiationtherapy was technically ahead to
begin with, and now Varian is adding efficient arc therapy thatcan be delivered in multiple planes, i.e., volumetrically.With thesame technology we use to deliver noncoplanar treatments, wecan now also offer very fast arc therapy. It’s a testament to whatcan happen when the thought leaders in industry work togetherwith innovative clinical researchers. The result is something thatmakes a practical difference to patient care and to our ability tooffer whatever is best for each of our patients.”
According to Cedric Yu, DSc, the Carl M. Mansfield, MD, professorof radiation oncology at the University of Maryland MedicalCenter and another important contributor to RapidArc research,his studies of single-arc IMRT have shown it to be equal to or bet-ter than multiple-field IMRT in terms of target volume coverageand normal tissue sparing. He found that a single arc can deliveressentially similar dose distributions compared with IMRT plansthat incorporate as many as 36 fields.
“Clinicians everywhere are rapidly adopting online IGRT tech-nologies like Varian’s On-Board Imager® system,” BCCA’s Ottopoints out. “Patients benefit from a focus on accurate patientpositioning through daily imaging. RapidArc is extremely timeefficient, which contributes to patient comfort. It is likely thatwe will see image-guided arc therapy sessions take less than 10minutes, including imaging and treatment.”
Varian customers who adopt RapidArc will gain this new clinicalcapability without sacrificing the ability to deliver other forms oftreatment if needed. A Trilogy® or Clinac® iX accelerator outfittedto deliver RapidArc can still deliver static fields, noncoplanartreatments, electron therapy, and conventional forms of IMRT,IGRT, SBRT, and SRS. �
* Pending FDA 510(k) approval; not available for sale in the United States at this time.
ASTRO Round-UpVarian exhibited a range of new technologies at this year’s meeting of the American Society for TherapeuticRadiology and Oncology (ASTRO), held October 28 through November 1, 2007, at the Los Angeles ConventionCenter.OndisplaywereVarian’snewRapidArc™delivery technology*,ahigh-definitionmultileaf collimator forradiosurgery, and updated tools for planning and delivering LDR andHDR brachytherapy treatments.
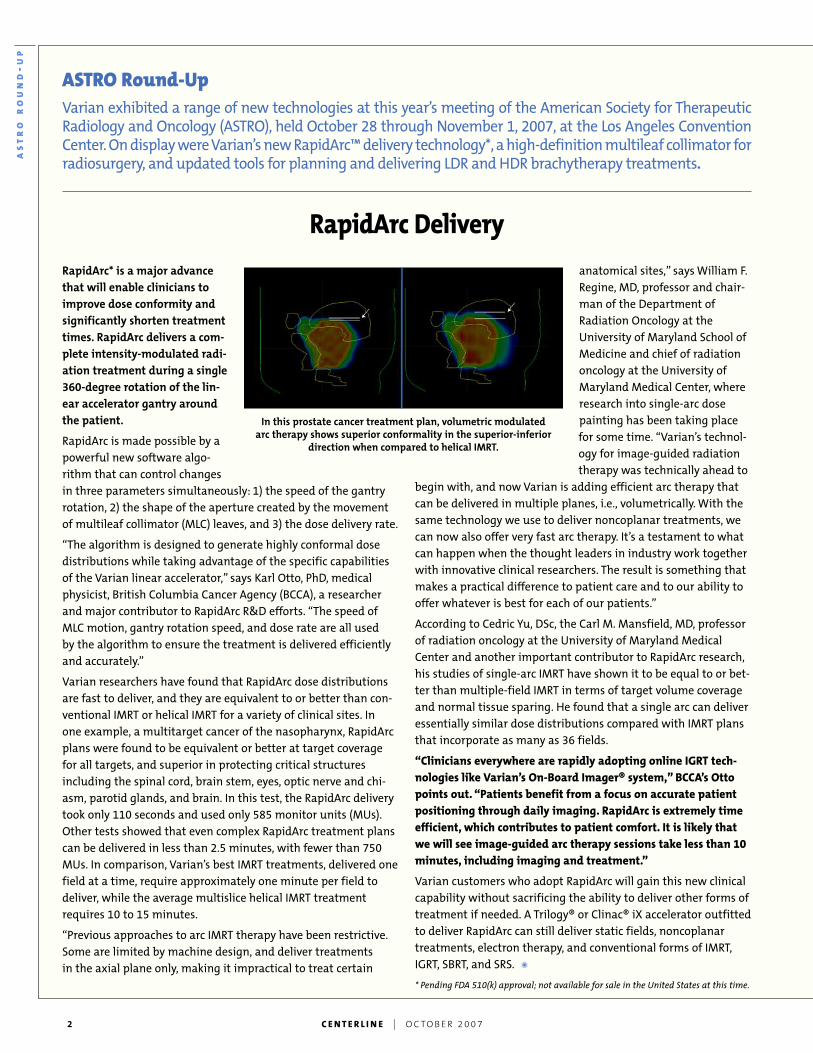
RapidArc Delivery
In this prostate cancer treatment plan, volumetric modulatedarc therapy shows superior conformality in the superior-inferior
direction when compared to helical IMRT.

C ENTER L I N E | O C TO B E R 2 0 0 7 3
iX Line of HDR Afterloaders
Also at ASTRO, Varian introduced the iX
line of afterloaders, advanced devices that
simplify high-dose-rate (HDR) brachyther-
apy delivery and optimize treatment. The
new iX systems are currently being
shipped to customers and are already in
operation at a number of sites.
At the heart of the iX afterloaders is new
Windows-based control software, com-
mon to both the VariSource™ iX and
GammaMedplus™ iX afterloaders, the
computer-controlled devices used for
delivering the radiation sources. The new
software integrates seamlessly with
Varian’s BrachyVision™ treatment plan-
ning system.
“We have introduced a world-class prod-
uct with a console that integrates with all
our brachytherapy delivery products and
software, making it easier to use and
more straightforward to plan treatments,”
saysWilliam Hyatt, head of Varian
BrachyTherapy. “It’s a major leap forward
in brachytherapy treatment delivery.
“We recognize the unique challenges of
delivering high-dose-rate treatments.
Time pressure is high and patients are
anxious, while the importance of getting
it right is paramount. That is why we’ve
worked with customers, engineers, and
software developers to produce an after-
loader control interface that is both intu-
itive and simple to use.”The product’s
interface was developed in conjunction
with IDEO, a leading international indus-
trial design company.
“The iX has really improved the situation
for us and our patients, as it is much more
logical and gives you a better overview of
the treatment’s status,” says Peter Niehoff,
MD, brachytherapy consultant at
University Hospital Kiel, in Germany—the
first hospital in the world to treat patients
using the new system.
According to Niehoff, the iX system makes
it easier for his team to alter the treat-
ment plan once treatment is under way
and to program the afterloaders to make
changes. “If you deliver the first fraction
and then need to change the plan, it’s
vital that you can easily access this infor-
mation,” he says. “Some of these treat-
ments are extremely complex—just
recently we did an interstitial chest well
treatment involving 16 channels and 300
dwell positions—so anything that makes
alterations more straightforward is
extremely valuable.”
His colleague, chief brachytherapy physi-
cist Frank-Andre Siebert, PhD, says the iX
system is so straightforward that even
inexperienced operators can handle it
with ease. “As a test,” he says, “I asked a
young physicist colleague who is not
experienced in brachytherapy to set up
and plan a typical prostate patient using
a dummy. It took him 15 minutes to cre-
ate a perfectly workable treatment.” �
VariSeed LDR BrachytherapyPlanning Software
VariSeed™ 8.0, an updated version ofVarian’s market-leading brachytherapyseed planning software, incorporates newfeatures that give clinicians more ways todefine and visualize seed placementswhen planning and delivering low-dose-rate (LDR) brachytherapy treatments forprostate cancer.
“The new features provide even bettervisibility of the positions of individualseeds in permanent seed implants,” saysRebecca Claydon, software product man-ager with Varian BrachyTherapy. “Basedon feedback from urologists, VariSeed 8.0facilitates the planning of prostate seedbrachytherapy treatments by biopsy sec-tion, so that a localized boost can be deliv-ered to a targeted region of the prostate.”
VariSeed 8.0 offers brachytherapy physi-cists new and improved contouring tools,including the ability to contour in the
LEFT | The VariSource iX HDR afterloader.
BELOW | A screen capture from the VariSeed 8.0treatment planning system.

4 C ENTER L I N E | O C TO B E R 2 0 0 7
ARIA Demonstrated at ASCOEHR Symposium
Earlier this year, Varian was one of
seven vendors selected to participate
in the American Society of Clinical
Oncology (ASCO) Electronic Health
Records (EHR): 2007 Oncology
Symposium held September 19–20 in
Dallas, Texas. Varian showcased the
company’s ARIA™ oncology information
system, a comprehensive EHR for man-
aging patient information in cancer
treatment centers as well as radiation
and medical oncology departments.
“We were honored and pleased to be
among the vendors invited to partici-
pate in the symposium,” says Maureen
Thompson, senior director for Varian’s
oncology information systems. “Varian’s
ARIA system is one of the most compre-
hensive, robust EHR solutions available.
It is unique in its depth of clinical sup-
port for both radiation and medical
oncology treatment processes. In addi-
tion, we continue to enhance our oncol-
ogy information system capabilities,
focusing on quality measures and out-
comes relevant to specific disease sites,
and to track compliance with specific
treatment protocols.We believe that an
oncology-specific EHR can improve the
quality of cancer care.”
At the symposium, Varian and the other
vendors conducted oncology-specific
product demonstrations based on sce-
narios provided by ASCO. “Buying an
EHR is a major decision for an oncology
practice,” says Ken Hotz, EHR product
manager for Varian. “These software
tools become a part of the clinic’s cul-
ture and way of life. Those who attend-
ed the symposium came away with a
very good understanding of the prod-
ucts and how they compare with one
another.” �
Varian and BrainLAB BundleRadiosurgery Products
In a move to offer superior noninvasive
treatment options, Varian and BrainLAB
have teamed up to create Novalis® Tx,
bringing together the most successful
radiosurgery technologies from both
companies for imaging, treatment
planning, and treatment delivery.
Novalis Tx includes Varian’s Trilogy® Tx
linear accelerator and the new HD120
multileaf collimator, which offers 2.5-
mm leaves for finer beam shaping. The
ultraprecise Novalis Tx radiosurgical
instrument will use a variety of stan-
dard and configurable options, includ-
ing Varian’s On-Board Imager® device,
the BrainLAB ExacTrac® X-Ray 6D room-
mounted X-ray imaging system, the
BrainLAB iPLAN® treatment planning
software, and Varian’s Eclipse™ treat-
ment planning and ARIA™ information
management software.
“This powerful platform enables both
companies to offer radiation oncolo-
gists, neurosurgeons, and other medical
specialists the sharpest knife available
for radiosurgery,” says Tim Guertin,
president and CEO of Varian Medical
Systems. “This product introduction is
a natural extension of a relationship
that has been in place since 1996, when
BrainLAB and Varian incorporated linear
accelerator and multileaf collimator
technologies to create the Novalis line
of radiosurgery products.”
“Building upon our long-time relation-
ship with Varian and the strengths of
both organizations, Novalis Tx combines
the most powerful and advanced capa-
bilities available on the market today,”
says Stefan Vilsmeier, president and
CEO of BrainLAB. “More versatility and
efficiency will mean new hope for more
patients.”
The Novalis Tx offers the widest range of
treatment options for the largest num-
ber of indications, including malignant
and benign lesions, brain metastases,
ASTRO
ROUND-U
P
sagittal and coronal planes. Contouringthe urethra has been simplified by theintroduction of the Structure Sweep,which is also available in the VariSeedImplant View™ module for interactiveseed placement and dosimetry.
Among the new features is a tool thatcreates a digital reconstruction of the CTimage and makes it much simpler todefine the seed placement. A typicalpermanent seed implant involves up to120 radioactive seeds, each the size of agrain of rice.
There are more than 1,200 hospital sitesworldwide using more than 1,600Varian VariSeed software systems forguiding the placement of permanentprostate seed implants. Use of this tech-nique alone or with external beamradiotherapy is increasing for patients,including about 60,000, or one third, ofthe U.S. men who are diagnosed annual-ly with prostate cancer. �
High-Definition MLC
Varian has received FDA 510(k) clear-
ance for a new high-definition MLC. The
new HD120 MLC doubles the resolution
of Varian’s most precise MLC by reduc-
ing the width of the central leaves to
just 2.5 millimeters.
According to Calvin Huntzinger, MS,
marketing and engineering manager for
Varian Surgical Sciences, the HD120 MLC
collimator will be included with the new
Novalis® Tx suite of radiosurgery prod-
ucts that Varian is teaming up with
BrainLAB to offer. Designed for extreme
durability, the new MLC offers improved
dose delivery characteristics, including a
steeper dose fall-off gradient.
“This new high-definition multileaf col-
limator builds on Varian’s widely recog-
nized accomplishments in advancing
MLC technology,” says Huntzinger. “It
underscores our commitment to meet-
ing the unique needs of clinicians offer-
ing stereotactic radiosurgery and
stereotactic body radiotherapy.” �
NEW
S

C ENTER L I N E | O C TO B E R 2 0 0 7 5
arteriovascular malformations, and func-
tional lesions. It features the highest dose
delivery rates in the industry, dynamic
beam shaping, and frameless patient
positioning for more rapid, effective, and
comfortable treatments. Unlike other
radiosurgical devices, which are limited
to a 6 million electron volt (MEV) energy
level, the Novalis Tx allows multiple beam
energies from 6 to 20 MEV for treating
deep-seated tumors and sparing sur-
rounding healthy tissue more effectively.
Clinics should be able to treat twice the
number of patients per day than with any
other radiosurgery system on the market.
The Novalis Tx offers the most comprehen-
sive image-guidance system available,
including Varian’s machine-mounted 3D
CT scanner with 2D radiographic and fluo-
roscopic imaging capability as well as
BrainLAB’s room-mounted X-ray imaging
system for real-time imaging and motion
management. Coupled with BrainLAB’s
6D robotic couch, the system offers an
extremely fast and accurate solution for
setting up and verifying proper patient
position during treatment.
The treatment planning and information
management software presents clinicians
with the fastest, most user-friendly and
versatile platform for managing, plan-
ning, and delivering radiosurgery. �
First European IGRT SchoolHeld in UK
Varian sponsored its first European IGRT
School at the end of September at the
Clatterbridge Centre for Oncology (CCO)
inWirral, UK.
Clinicians, physicists, and radiographers
from hospitals in Italy, Russia, Norway,
Spain, and Scotland attended the three-
day event, taught by clinical experts at
CCO, one of the earliest adopters of
Varian’s On-Board Imager® device for IGRT.
The first two days consisted of presenta-
tion sessions, while the third day focused
on clinical sessions at the hospital. This
format will be followed for subsequent
schools.
“Varian approached me following my
presentation at last year’s ESTRO meeting
to ask if we could offer an IGRT School for
departments across Europe,” says Angela
Heaton, clinical specialist radiographer at
CCO. “We have made the On-Board Imager
a routine part of our treatments on our
linac and I believe we are using it more
than anyone else in Europe.”
According to Julie Massey, head of radio-
therapy, “This recognizes our achieve-
ments in establishing IGRT techniques
within a routine clinical setting at
Clatterbridge Centre for Oncology.We’re
delighted to work closely with Varian and
to be able to offer this school to such a
wide geographical area.”
The schools will be run four times a year,
and will be offered to all treatment cen-
ters purchasing the On-Board Imager kV
imaging system. The next school takes
place December 6–8, 2007, and 2008 ses-
sions have been scheduled for dates in
February, June, October, and December. �
Clinicians who attended the first Varian-sponsored IGRT School in Europe.
The Novalis Tx suiteof radiosurgeryproducts.
6 C ENTER L I N E | O C TO B E R 2 0 0 7
By Shane Dempsey,University of Newcastle
At the Universityof Newcastle inNew South
Wales, Australia, abachelor’s degree pro-gram teaches studentsto work in radiationtherapy departmentsacross all elements ofpractice. By trainingstudents on Version 8 of Varian’s Eclipse™treatment planning software, the universityhelps ensure that graduates have the knowl-edge and skills to work effectively in clinicalenvironments.Among University of Newcastle’s more than 20,000 stu-
dents is a cluster of future radiation therapists. The universi-ty’s School of Health Sciences runs a three-year, six-semesterbachelor of medical radiation science (radiation therapy) pro-gram on its largest campus in the city of Newcastle.
With an intake of around 50 students, the program educatesgraduates to work within RT departments across all elementsof practice: simulation, planning (dosimetry), and treatment.While the program teaches professional skills at the university,students also gain around 1,000 hours of workplace experienceby attending a variety of clinical sites over the three years of theprogram. Clinical affiliates include all 19 RT departments inNew South Wales and several departments in Tasmania and
Western Australia where RTtraining does not exist.
The program has a strongcommitment to ensuring thatstudents have the knowledgeand skills to work effectivelyand ethically while on clinicalplacement. Until recently, theprogram had an aging 2Dplanning lab, and there wasa need to commission a newlab capable of training stu-dents in 3D-CRT and IMRT
treatment approaches. The university looked at how this couldbest be done. The solution was a partnership with Varian andthe establishment of a 3D planning lab with a network of 10Eclipse workstations.
Better tools for teaching
There were many reasons for selecting the Varian Eclipsesystem for treatment planning. Eclipse would allow for con-ventional, 3D conformal, and IMRT plans to be developed.We wanted to ensure that the planning system could teachstudents basic conventional concepts such as physical wedgesand manual shielding by slice-by-slice beam configuration anddose analysis. This would allow students to understand theunderpinning clinical concepts of RT. With the software’s 3D-CRT functions, we would be able to teach developments suchas MLC beam shaping rather than shielding, dose volume his-togram (DVH) analysis as an aid to dose and volume analysis,and asymmetric and noncoplanar techniques. With IMRT, wewould be able to teach both forward-planned step-and-shoot
Eclipse in Practiceat the University ofNewcastle, Australia
With an intake of around50 students, the programeducates graduates to work
in RT departmentsacross all elements ofpractice: simulation,
planning, and treatment.

C ENTER L I N E | O C TO B E R 2 0 0 7 7
planning using the field-in-field functionality of Eclipse, aswell as inverse-planned IMRT using dose volume and cost-function optimization.
Eclipse allows for manual and automated methods of dosevolume determination. With Eclipse, we would be able toteach slice-by-slice volume outlining using manual methods;this would allow students to understand the relationships ofvolumes between slices and between structures. We would beable to use automated tools such as Flood Fill, coupled withthe density settings and the Volume Wizard, to autocontourstructures. With the postprocessing tools and Boolean func-tions, we could teach students to construct full and partial vol-umes more quickly. Eclipse allows for overlapping structuresand creating new structures by shrinking or expanding in alldirections from the margins of existing structures.
Eclipse has a great range of plan assessment tools, such asa means of allowing DVH to remain active in the model viewwhile you plan and optimize. The plan comparison DVHfunctions allow for multiple plans to be compared on a singleDVH. The Dose Color Wash display gives students a view ofthe beams and structures through a transparent dose cloud.Recently, final-year students developed a range of prostate
plans on the same data set using early-1980s-standard fourfields (10x10x10 cm fields with small postcorner shielding forthe rectum), a five-to-seven-field 3D-CRT approach, and amultifield inverse-planned IMRT plan. The dose color washacross the adjoining pelvic structures starkly demonstrated theadvantages of each plan over the preceding plan.
In our selection of Eclipse, an added advantage was that thenetworked, Windows-based environment is well supported bythe university’s information technology division, and the uni-versity has a partnership with Dell for hardware support. Theuniversity also has great support from the Varian office inSydney (about two hours away). This allowed the networkedEclipse environment to be set up to suit both Varian’s require-ments and the university’s needs.
Immediate clinical relevance
Eclipse is used widely across Australia and therefore the train-ing of students has immediate clinical relevance in those cen-ters. The system allows students to set up treatments online inRT Chart, so students are being trained to work within thepaperless environment that is becoming increasingly commonin treatment centers.
RT students at Australia’s University of Newcastle. Photo courtesy of the University of Newcastle.
8 C ENTER L I N E | O C TO B E R 2 0 0 7
In February 2007, the staff started using the system anddeveloping the structure that students would work with duringthe upcoming university year. In March, around 60 second-and third-year students were let loose on the system.
In the eight months since they were introduced to Eclipse,students have developed 3D-CRT plans using manual outlin-ing and manual beam-shaping methods, 3D-CRT plans usingautomated methods for contouring all outlines and structures,and automated beam shaping and isocenter placement usingbeam fitting, shaping, and aligning functions. The postpro-cessing and Boolean tools have been extremely popular andeasy-to-use tools to support contouring and volume creation.
The students have developed a range of IMRT plans usingstep-and-shoot, field-in-field methods, and then comparedthese outcomes to inverse-planned, DVH-optimized plans.Students have approved plans in RT Chart and scheduledtreatments. All these activities mean that the University ofNewcastle’s graduates will be prepared for emerging clinicalpractice.
All in all, our experience with Eclipse has been fantastic.Our system of choice has worked well for us and has beenextremely stable under the conditions of use of 60 students.Even with as much fun as we are having with the current sys-tem, which will remain clinically relevant for years to come, Ilook forward to future releases and to exploring what else canbe achieved with things such as gantry-optimized IMRT. �
Shane Dempsey is program director for the University of Newcastle’sbachelor of medical radiation science (radiation therapy) program.
The latest version of Eclipse incorporatesmany features that make treatmentplanning better and faster, including:
• Beam-angle optimization
• Smart Segmentation™ automaticcontouring
• Planning on 4D data sets for motionmanagement
• Library of disease-specific clinicalplanning protocols and treatmentplan templates
• Interactive fluence optimization
• Remote planning capabilities
• Fast 3D image registration formatching cone-beam CT imageswith planning CT images
• Dynamic adaptive radiotherapy(DART™) planning based on up-to-the-minute image information
• The AAA dose-calculation algorithmfor planning treatment in hetero-geneous areas of the body
• The electron Monte Carlo algorithmfor planning electron treatments
Eclipse: A Spectrum of Advanced Features
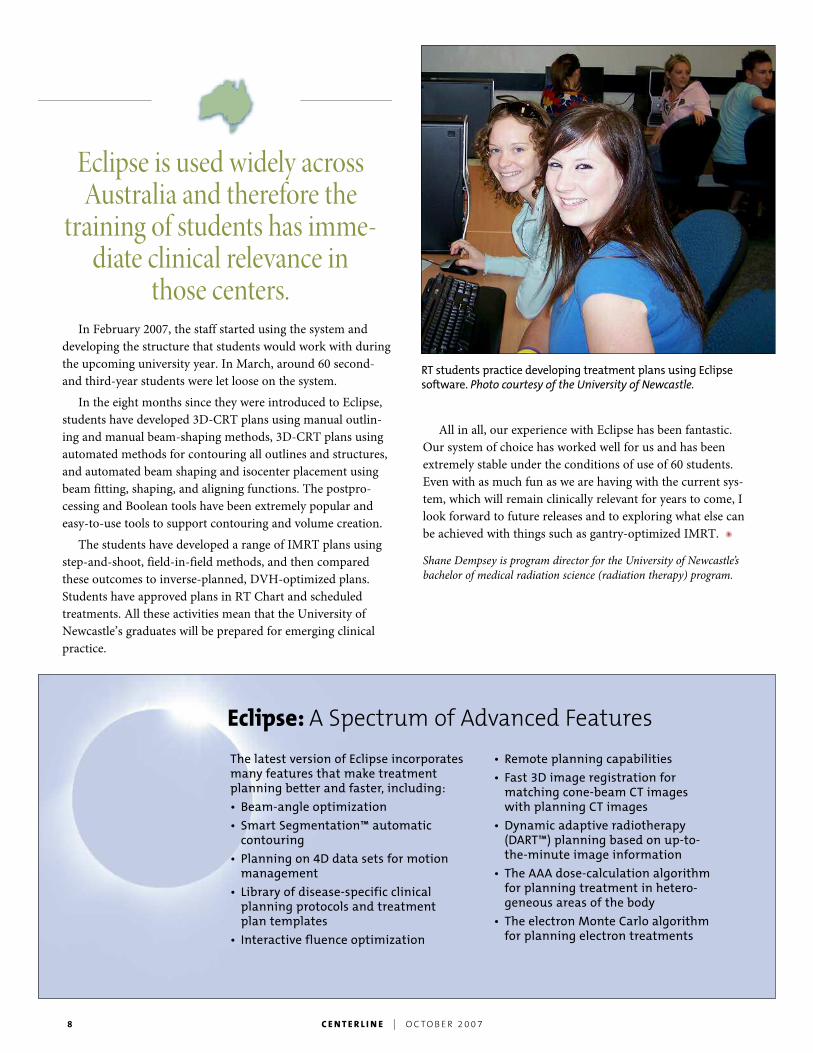
RT students practice developing treatment plans using Eclipsesoftware. Photo courtesy of the University of Newcastle.
Eclipse is used widely acrossAustralia and therefore the
training of students has imme-diate clinical relevance in
those centers.
C ENTER L I N E | O C TO B E R 2 0 0 7 9
By Nancy Heifferon
Clinicians at the Stanford University CancerCenter have been pulling out all the stopsto find optimal ways of using Varian tech-
nology to treat moving tumors close to sensitivestructures. Using a Trilogy® machine outfittedwith an On-Board Imager® device and a Real-TimePosition Management (RPM™) system for gatingand motion management, they are treating diffi-cult cases throughout the body.
More flexibility for treating lung cases
Billy W. Loo, Jr., MD, PhD, is program leader in thoracic radia-tion oncology at the Stanford Cancer Center. Advances in imag-ing and tumor motion management are giving him the flexibili-ty he needs for treating challenging lung tumors.
When treating lesions in the lung, it can be difficult to deliv-er high enough doses to a targeted lesion because of the limitedtolerance of normal tissues in the lungs, esophagus, heart, andspinal cord—especially in frail patients with low lung reserve.“The more precise and conformal we can be, the better the ther-apeutic index is, in terms of delivering more dose to the tumorwhile limiting the dose to surrounding tissues,” explains Loo.
IMRT for a stage III tumor
Take the recent case of a man in his late 50s with a prior leftpneumonectomy for early-stage lung cancer, presenting with anew stage III non–small cell lung cancer in his right lower lobe.Dynamic 4D-CT imaging demonstrated that the new primarytumor, which sat close to the diaphragm, moved nearly 3 cen-timeters as he breathed. With limited healthy lung remaining,he was ineligible for further surgery and also at high risk forlung injury from conventional radiation therapy fields.
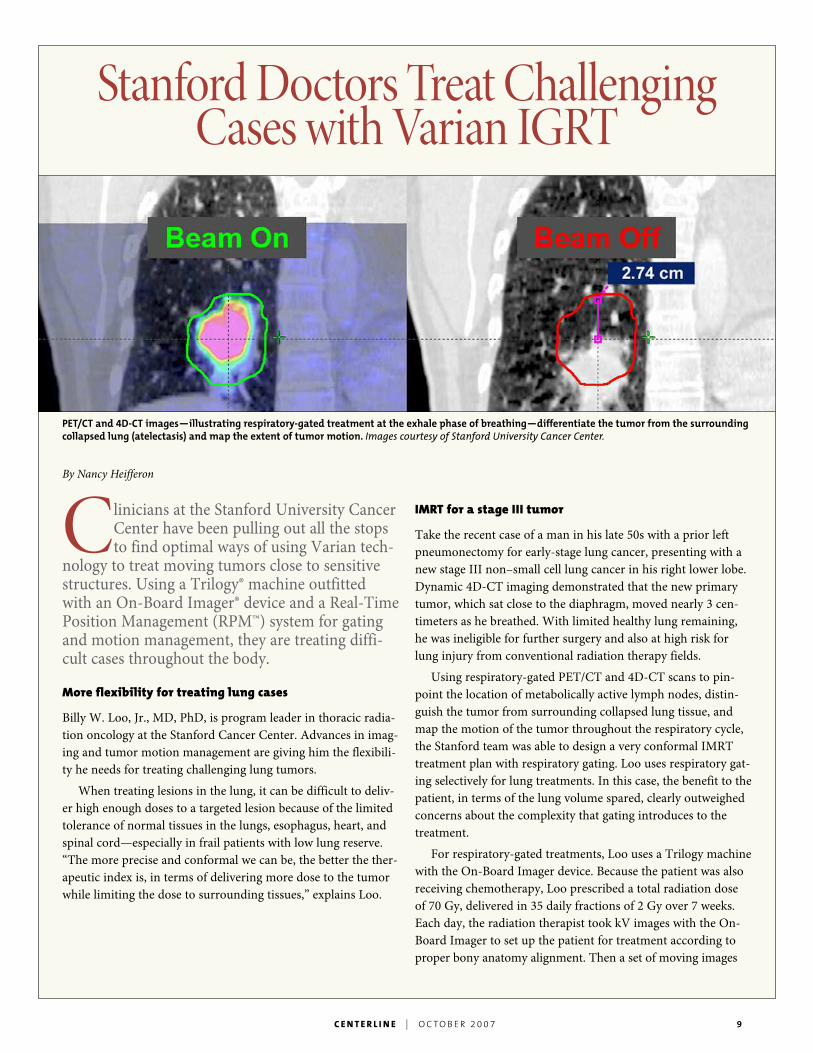
Using respiratory-gated PET/CT and 4D-CT scans to pin-point the location of metabolically active lymph nodes, distin-guish the tumor from surrounding collapsed lung tissue, andmap the motion of the tumor throughout the respiratory cycle,the Stanford team was able to design a very conformal IMRTtreatment plan with respiratory gating. Loo uses respiratory gat-ing selectively for lung treatments. In this case, the benefit to thepatient, in terms of the lung volume spared, clearly outweighedconcerns about the complexity that gating introduces to thetreatment.
For respiratory-gated treatments, Loo uses a Trilogy machinewith the On-Board Imager device. Because the patient was alsoreceiving chemotherapy, Loo prescribed a total radiation doseof 70 Gy, delivered in 35 daily fractions of 2 Gy over 7 weeks.Each day, the radiation therapist took kV images with the On-Board Imager to set up the patient for treatment according toproper bony anatomy alignment. Then a set of moving images
StanfordDoctors Treat ChallengingCases withVarian IGRT
PET/CT and 4D-CT images—illustrating respiratory-gated treatment at the exhale phase of breathing—differentiate the tumor from the surroundingcollapsed lung (atelectasis) and map the extent of tumor motion. Images courtesy of Stanford University Cancer Center.

10 C ENTER L I N E | O C TO B E R 2 0 0 7
was taken with the device in fluoro-scopic mode. “With real-time fluoro-scopic images of tumor motion at thetime of treatment, we have the flexi-bility on the spot to adjust the respi-ratory gating to ensure that thebeam comes on when the internalanatomy is in proper position,”explains Loo. This patient tended tobe fairly consistent in his breathing,but not all patients are, cautionsLoo. “Daily position verification anddaily pretreatment fluoroscopic veri-fication ensure the reproducibility ofthe internal anatomy compared tothe plan.”
On short-term follow up, thispatient is doing well clinically.“Emerging data suggests that earlyresponse to treatment is a prognosticindicator,” says Loo. “I am encour-aged to see a good tumor responseindicated by both PET and CT fol-low-up imaging.”
Pulmonary radiosurgery for a small metastasis
In a second case, a young man in his 30s with chondrosarcoma,a rare, slow-growing cancer of the cartilage, had a single 1-cmlung metastasis in the right lower lobe. He had already beensubjected to repeated thoracotomies for previous metastatictumors in the lungs. Although this tumor was resectable, con-cerns about further loss of lung reserve and the man’s ability totolerate the rigors of another major operation made it reason-able to consider stereotactic radiosurgery. The local control ratefor small peripheral tumors like the one in this case is over 90percent with pulmonary radiosurgery.
Following Stanford’s pulmonary radiosurgery protocol, Lootreated this patient with 25 Gy in a single fraction, using theTrilogy machine. The patient was a good candidate for thistreatment option because his tumor demonstrated relatively lit-tle respiratory motion on 4D CT. This meant Loo could expectreasonable visualization of the small tumor without fiducialmarkers, using the On-Board Imager’s cone-beam CT capabili-ty. “Though we routinely use fiducial markers for pulmonaryradiosurgery, we wanted to avoid the invasive procedure in thiscase,” explains Loo. “The cone-beam CT option gives us thisadditional flexibility.”
Over the course of the hour-long treatment, the patient’sbreathing pattern gradually changed, growing deeper on inhala-tion and shallower on exhalation, probably due to the discom-fort of immobilization. “The only way we could have picked
that up and compensated for it waswith cone-beam CT imaging betweentreatment fields,” says Loo.
Two years ago, it would have beendifficult or even impossible to treateither of these patients adequately andsafely with radiation therapy becauseof the lack of needed precision. “Wecan do a lot more with radiotherapytoday because new technologies enableus to be more precise in defining thetumor extent and location, character-izing its motion, and designing planswith appropriate margins that allow usto give an adequate dose of radiationto the tumor while sparing surround-ing structures,” says Loo. “4D IGRTfills in a key piece of the puzzle byenabling us to verify that these verycomplex treatments are actually beingdelivered according to plan.”
Targeting locally advancedpancreatic cancer
Other clinicians at Stanford are com-bining a single fraction of radiotherapy (stereotactic body radio-therapy, or SBRT) with gemcitabine chemotherapy to investigatetheir combined effects on locally advanced pancreatic cancer.Early results with the first 20 patients treated on Trilogy areencouraging. The exquisitely precise targeting needed to deliverhigh-dose radiation while sparing the surrounding liver, stom-ach, and bowel is made possible by the latest advances in image-guided radiation therapy.
Pancreatic cancer is a deadly disease with few effective treat-ment modalities. Every year in the United States, more than30,000 patients are newly diagnosed and a similar number ofannual deaths are attributed to this disease. Historically, surgeryis the only option associated with long-term survival. However,only 15 percent of newly diagnosed patients have surgicallyresectable tumors. The majority of pancreatic cancer patientshave metastatic or locally advanced disease—unresectabletumors that have spread beyond the pancreas. With currenttreatment methods, the median life expectancy for thesepatients is six to nine months. Clinical trials to date have shownthat gemcitabine is the single most effective chemotherapy in aspectrum of systemic agents with limited activity in pancreaticcancer. Conventionally fractionated radiotherapy, in combina-tion with chemotherapy, has been shown to improve survivaland is useful in palliation of pain and preventing gastricobstruction.
“With real-time fluoroscopicimages of tumormotion at the timeof treatment, we have the flexibilityon the spot to adjust the respiratorygating to ensure that the beamcomes on when the internal
anatomy is in proper position.”Billy W. Loo, Jr., MD, PhD, Stanford Cancer Center
C ENTER L I N E | O C TO B E R 2 0 0 7 11
Double-teaming achallenging disease
But could an optimal combination ofSBRT and chemotherapy make a dif-ference? That is the question that theStanford team is attempting toanswer in a phase II clinical trial.
“Studies from the 1980s suggestedsome benefit from this dualapproach,” says Albert Koong, MD,PhD, of the Stanford Cancer Center’sDepartment of Radiation Oncology.“However, local control of the tumorwas highly variable in these studies.While it was difficult to determinelocal control before CT scanning waswidely available, most studies suggestthat 25 to 50 percent would faillocally after the radiation therapy.”
In these earlier studies, the totalradiation dose was delivered in acourse of 1.8-to-2-Gy fractions ineither a split course or continuous manner for 4 to 6 weeks.Today, the standard radiotherapy is given in a similar mannerwith concurrent 5-fluorouracil chemotherapy. “Some institu-tions such as the University of Michigan have pioneered anapproach where they have been able to give systemic gemcita-bine with an abbreviated course of radiotherapy over threeweeks instead of six weeks,” says Koong. “They have been rela-tively successful with that approach.”
Under the Stanford protocol, patients newly diagnosed withlocally advanced pancreatic cancer receive a total radiation doseof 25 Gy all in one fraction. The radiotherapy is deliveredsequentially between the first and second cycle of gemcitabinechemotherapy. Integrating SBRT with chemotherapy in thismanner allows full dose systemic therapy without compromis-ing the local radiation dose intensity.
Image guidance for precision
Stanford is able to safely escalate the radiation dose by usingadvanced IGRT technologies such as Varian’s On-Board Imagerand RPM system, which are designed to work in an integratedmanner with the Trilogy machine. “In our approach,” saysKoong, “we have the ability to target these tumors more precise-ly than we ever have in the past.”
The process is a complex one. Preparing the patient andplanning the treatment takes one to two weeks. Gold seed fidu-cial markers, three to five of them, are placed by CT or endo-scopic guidance into the tumor and surrounding pancreas. Abody mold is made to immobilize the patient during the treat-ment. The pancreas is imaged in arterial and venous phases
with spiral CT scanning; 1.25-mmcuts provide maximum resolution ofthe tumor. An FDG-PET scan showsthe metabolic hot spots in the tumor.Additionally, 4D-CT scanning is doneto account for respiratory-associatedtumor motion. According to Koong,pancreatic tumors can move as muchas two to three centimeters during therespiratory cycle.
“We fuse all these images together,reconstruct the anatomic location ofthe tumor during the respiratorycycle, and correlate the location ofthe tumor with the metabolic activityseen on the FDG-PET scan,” explainsKoong. “This gives us the gross tumorvolume, to which we add 2 to 3 mmfor the planned treatment volume.”
To deliver the planned single-fraction treatment, Stanford uses anIMRT approach with respiratory gat-
ing to conform the radiation delivered to the exact location andshape of the tumor. This approach enables clinicians to reducethe treatment margin and maximally spare the surrounding tis-sue from radiation toxicity.
At the time of treatment, the radiation therapist takes both2D and fluoroscopic images with the On-Board Imager to estab-lish correct alignment and confirm that the marker seeds comeinto the right range when the radiation beam is turned on, typi-cally during exhalation phase. The imaging process is repeatedfor each beam angle, and patient position is adjusted as neces-sary. “For each beam angle, using the kV imaging mode, we cansee where the fiducials are in relation to bony anatomy,” saysKoong. “Then we take fluoroscopic images to give us a dynamicpicture of what’s really happening during respiration. Whensuch a high radiation dose is involved, we need this additionallevel of precision so that we can be sure that we are deliveringthe treatment as planned.”
The ultimate in targeted treatment
Eighteen months into the clinical trial, the early findings aretrending positive: no significant acute GI toxicities and only onelocal failure to date.
“As systemic therapies improve, it becomes more importantto integrate these newer therapies with targeted radiotherapyapproaches,” says Koong. “Our medical oncology colleagues arestarting to use targeted therapeutics routinely, but radiation isthe original and ultimate targeted therapy. Advances in imagingtechniques will parallel the advances in radiotherapy by improv-ing our ability to target tumors.” �
Nancy Heifferon is a freelance healthcare writer.
“Our medical oncology colleaguesare starting to use targetedtherapeutics routinely, butradiation is the original andultimate targeted therapy.”
Albert Koong, MD, PhD, Stanford Cancer Center
12 C ENTER L I N E | O C TO B E R 2 0 0 7
Varian Research Collaborationson Display at AAPM

C ENTER L I N E | O C TO B E R 2 0 0 7 13
By Lynn Yarris
Thehistory of Varian Medical Systems issteeped in scientific and engineeringresearch: the company can trace its roots
back to the invention of the klystron, the first com-pact source of high-powered microwaves, by thebrothers Russell and Sigurd Varian. This traditionof research continues today, as was evident at theforty-ninth annual meeting of the AmericanAssociation of Physicists in Medicine (AAPM),which was held July 22–26, 2007, at theMinneapolis (Minnesota) Convention Center.More than 250 papers and posters, or better thana quarter of all the presentations, were aboutresearch that was either directly supported byVarian or performed using Varian technology.“Varian continues to focus on increasing our level of
collaborative activity that can help deliver real solutionsto the problems impacting clinical cancer care,” saysMichael Sweitzer, the manager of Varian’s researchcollaborations. “While we are seeingother companies cut back on theirdevelopment efforts, Varian isexpanding both the breadth anddepth of our research collaborations.”
Current areas of research that areof prime concern to Varian focus onstrategies and techniques for improv-ing dose conformity, advances inimage-guided and adaptive radiother-apy technologies, and more effectivemeans of motion management. TheAAPM meeting saw many excitingnew findings and results reported in each of these areas—allwith connections to Varian. While space constraints preventcoverage of all of the research presented at the meeting, thisarticle seeks to highlight just a few interesting, representativeexamples.
Improving dose conformity
Improved dose conformity means being able to precisely directincreasingly higher doses of radiation to increasingly better-defined targets. Stereotactic radiosurgery (single fraction treat-ment) and stereotactic radiotherapy (multiple fractions oftreatment) can provide exceptionally good conformity andhave proven particularly valuable for attacking tumors in thebrain and spine. As presentations at the AAPM suggest, thefuture for stereotactic treatments looks even better.
Radiation physicists from the Medical Center at theUniversity of California, San Diego, delivered a paper describ-ing their initial experience using a single-isocenter, single-fraction IMRS technique to treat patients with multiple brainmetastases. Ten patients were treated using an IMRT-basedtreatment in which patient setup and target localization duringtreatment were carried out with Varian’s frameless localizationsystem. The results showed that 8 to 12 fixed beams properlyselected with a single isocenter were sufficient to achieve gooddose coverage and organ sparing. The treatment time was lessthan 60 minutes to deliver dose of 16 to18 Gy. The authorsconcluded that IMRT-based SRS treatment of multiple brainmetastases or large irregular lesions saves treatment time andgives the benefits of dose conformity and organ sparing, easyplan QA, and patient setup verification.
Researchers from the M.D. Anderson Cancer Centerreported the use of image-guided stereotactic body radiother-
apy (IG-SBRT) for treatment of spinal tumors usingcone-beam CT for daily pretreatment imaging. A spinephantom was used to study the feasibility and accura-cy of this approach before a patient was successfully
treated for spinal lesions with a pre-scription of 2,700 cGy to the lesion atthe level of L5 in three fractions.
One of the key issues in improvingdose conformity is positioning accura-cy. A pelvis phantom study carried outby researchers at the Duke UniversityMedical Center assessed the 3D targetlocalization accuracy of the cone-beamCT mode of Varian’s On-BoardImager® device. Their results showedthat On-Board Imager’s cone-beam CTimaging is capable of detecting target
shifts and patient rotation to within 1 millimeter (mm) and 0.5degrees respectively. The shifted target could be realigned tothe planned isocenter to within 1-mm accuracy when correct-ing for translational shifts, and within 1.8 mm when correctingfor rotations.
One of the biggest stirs at this year’s AAPM meeting wasgenerated by a paper presented by Karl Otto of the BritishColumbia Cancer Agency. Otto described a technique calledtrajectory-based radiation therapy (TBRT) for planning anddelivering optimized dose distributions with a radiation sourcethat moves along a continuous three-dimensional trajectorydefined by gantry angle, couch angle, and couch position. Ottoreceived a prestigious “reviewer’s choice” time slot for a similarpresentation on volumetric arc treatments—a subset of TBRT—at the ICCR conference in Toronto earlier this year. AtAAPM, he demonstrated that the TBRT technique is well suit-ed for online verification and adaptation, with delivery times
“While we are seeing othercompanies cut back on theirdevelopment efforts, Varianis expanding both the breadthand depth of our research
collaborations.”Michael Sweitzer, Varian Medical Systems

14 C ENTER L I N E | O C TO B E R 2 0 0 7
that are substantially shorter than static-gantry IMRT,intensity-modulated arc therapy (IMAT), andtomotherapy. Says Varian’s Sweitzer, “It appears thatTBRT—and volumetric arc—mayprovide better dose conformity thanthe treatment modalities in commonuse today.”
Adds Dow Wilson, president ofVarian’s Oncology Systems business,“RapidArc™, which is Varian’s newtechnology for single-revolution volu-metric arc therapy and a form ofTBRT, will provide better dose con-formity than is possible with currentforms of IMRT or tomotherapy.”*
Advancing image-guided andadaptive radiotherapy
While there were scores of Varian-supported papers on IGRT imaging and beam-deliveryimprovements, there were also significant new developmentsreported that pertain to QA processes for IGRT. Two papers inparticular caught Sweitzer’s attention.
The first paper, presented by a team from the EmoryUniversity School of Medicine, described an automated andcomprehensive QA procedure to monitor the coincidence ofmechanical, radiation, and imaging isocenters using cone-beam CT and planar X-ray imaging. Performing tests on thefour IGRT-enabled machines available in their institution, theauthors found that coincidence between the mechanical, radia-tion, and imaging isocenters was within 1 mm for all fourmachines, as was isocenter stability with gantry angle. Afterimage acquisition, the automated software analysis took lessthan one minute. They concluded that automated image analy-sis may be used as a daily QA procedure.
The second paper came from Varian’s own GinztonTechnology Center. Researchers there have developed an effi-cient analytical scatter-correction algorithm for the On-BoardImager. This algorithm can be applied to both the center-detector and offset-detector geometries used in cone-beam CT.A scatter-kernel model was implemented in which the conebeam was modeled as an array of pencil beams. For each of thepencil beams, a scatter point-spread function was determinedon the basis of measured attenuation values and prior simula-tions of a polychromatic X-ray beam directed through uniformmaterial. Based on test results with a pelvis phantom and acylindrical water phantom, the researchers demonstrated thepotential for successful implementation of a computationallyefficient scatter-kernel model for the On-Board Imager.
Under the category of adaptive radiotherapy, in which radi-ation treatment plans are adjusted while a patient is on the
table, two papers stood out. One came fromSwitzerland’s Radiotherapie Hirslanden. A groupof researchers there evaluated the future potential
of applying the On-Board Imager’scone-beam CT option to therapy plan-ning that allows dynamic adaptationfor target volume changes. Results withreal patient data demonstrated that aproperly calibrated cone-beam CToption allows offline treatment plan-ning. Furthermore, the image qualityof the On-Board Imager is sufficientfor contouring target outlines. Cone-beam CT, the researchers concluded,can serve as the control CT in order toadapt the target volume and resize thetreatment fields and/or optimize thetreatment plan.
The second paper was presentedby a collaboration of researchers from the University ofPittsburgh’s Cancer Institute and the Cancer Institute of NewJersey, in New Brunswick. They reported the development of acone-beam CT–guided online plan modification technique tocompensate for interfractional anatomic changes during IMRTprostate cancer treatments. Three prostate cases were adaptedto evaluate this proposed online method and the results werecompared with those obtained with bony-structure-based,prostate-based, and cone-beam CT–based replanning correc-tion strategies. The researchers found that their cone-beamCT–guided technique is superior to the bony-structure-basedand prostate-based correction techniques, especially whenlarge interfractional target deformation exists. Its dosimetricperformance is similar to that of the replanning strategy, butwith much higher efficiency.
Motion management
With an increase in treatment volume comes an increasedconcern about the issue of motion during treatment delivery.Scores of papers addressed this concern. One was reportedby a team of researchers from Stanford University. Theseresearchers examined the problem of intrafraction tumor-target positioning, which they divided into two separateprocesses: (1) estimating the real-time target position and(2) repositioning the beam to account for intrafraction targetmotion. In their paper, the Stanford team describes and con-trasts various target position estimation and beam reposition-ing processes that are either available for clinical use or indevelopment, and they characterize the advantages and disad-vantages of these systems.
* Pending FDA 510(k) approval; not available for sale in the United States at this time.
“RapidArc, which is Varian’snew technology for single-revolution volumetric arc
therapy and a form of TBRT,will provide better dose
conformity than is possiblewith current forms of IMRT
or tomotherapy.”DowWilson, Varian Medical Systems

C ENTER L I N E | O C TO B E R 2 0 0 7 15
Another paper on the topic of motion management waspresented by a collaboration of researchers from Emory andGeorgia Tech, who reported on the 4D dose verificationaspects of treatment plans that involve intrafraction motion. Stillanother, presented by a collaboration of Stanford and Varianresearchers, reported on an empirical investigation of 3Dintrafraction motion management using a generalized method-ology for tracking, translating, rotating, and deforming targets.
Technology-pushing spirit continues
The papers described here represent only a tiny sample ofthose presented at the AAPM meeting that were either directlysupported by Varian or carried out using Varian equipment.In addition to the research areas already mentioned, there werealso significant developments reported in brachytherapy andradiobiology (referred to as “biosynergy” at Varian) and evenproton therapy, all of which featured integral contributionsfrom Varian. The company’s broad and vital presence at theAAPM meeting was an affirmation that the technology-push-ing spirit of the Varian brothers continues to thrive at VarianMedical Systems. �
Lynn Yarris is a freelance science writer.
References
The papers cited in this article were presented at the American Association of Physicists inMedicine (AAPM) meeting, July 22–26, 2007. Here, in the order of their appearance in the article,are the titles and authors of those papers. The asterisk (*) indicates the presenting author.
“Intracranial Applications of IMRT-Based Stereotactic Radiosurgery to Treat Multiple or LargeIrregular Lesions,” by J. Wang*, R. Rice, T. Pawlicki, A. Mundt, and K. Murphy, UCSD MedicalCenter, La Jolla, California.
“Image-Guided Body Stereotactic Radiotherapy Using Cone-Beam Computer Tomography forTreatment of Spinal Tumors,” by C. Wang*, A. Shiu, H. Wang, and E. Chang, University of TexasM.D. Anderson Cancer Center, Houston, Texas.
“A Phantom Study on the 3-D Target Localization Accuracy Using CBCT of an On-Board Imager,”by L. Zhang*, H. Yan, and F. Yin, Duke University Medical Center, Durham, North Carolina.
“Trajectory-Based Radiation Therapy,” by K. Otto*, British Columbia Cancer Agency,Vancouver, Canada.
“Automated CBCT QA for Image-Guided Radiation Therapy,” by T. Fox, E. Elder, andE. Schreibmann*, Emory University School of Medicine, Atlanta, Georgia.
“Scatter Correction for the On-Board Imager Using a Kernel Model,” by J. Star-Lack*, M. Sun,R. Suri, and G. Virshup, Varian Medical Systems, Mountain View, California, and Baden,Switzerland.
“Linac Cone-Beam-CT Option for Treatment Planning: A Possible Approach for DynamicAdaptive RadioTherapy,” by P. Cossmann*, A. Stuessi, and C. von Briel, RadiotherapieHirslanden, Aarau, Switzerland.
“A Cone Beam CT–guided Online Plan Modification Technique to Correct InterfractionalAnatomic Changes for Prostate Cancer IMRT Treatment,” by W. Fu*, Y. Yang, D. Heron, andM. Huq, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania, and N. Yue, CancerInstitute of New Jersey, New Brunswick, New Jersey.
“Intra-Fraction Target-Beam Positioning,” by P. Keall* and A. Sawant, Stanford University,Stanford, California.
“4D Dose Verification of Treatment Plans Involving Intra-Fraction Motion,” by E. Schreibmann*,I. Crocker, and T. Fox, Emory University, Atlanta, Georgia, and H. Gozbasi, S. Ahmed, andM. Savelsbergh, Georgia Tech, Atlanta, Georgia.
“Empirical Investigation of 3D Intrafraction Motion Management Using a Generalized Methodologyfor Tracking, Translating, Rotating and Deforming Targets,” by A. Sawant*, P. Keall, V. Srivastava,R. Venkat, and D. Carlson, Stanford University, Stanford, California, and H. Cattell andS. Povzner, Varian Medical Systems, Palo Alto, California.
Join the leader incancer-fighting technology.
At Varian Medical Systems, we offer a wide varietyof outstanding career opportunities. And we inviteyou to become part of the team working to help cli-nicians beat cancer by realizing great solutions likethose you read about in Centerline.
You’ll help us create solutions that treat over 100,000patients a day. And you’ll join a company that wasnamed #14 in BusinessWeekmagazine’s list of Top 50Performing Companies.We are also a recent winner ofthe Computerworld 21st Century Achievement Award,which recognizes individuals and organizations that useinformation technology to benefit society.
To learn more, visit us atwww.varian.com/careers.
16 C ENTER L I N E | O C TO B E R 2 0 0 7
On opposite sides of the country, two newAmerican cancer centers offering medicaland radiation oncology are operating with-
out film or paper. Both designed their processes andworkflow around the ARIA™ oncology informationsystem from Varian.
Mid Ohio Oncology/Hematology’sMark H. Zangmeister Center
Mark Thompson, MD, president of Mid Ohio Oncology/Hematology (MOOH), had a vision that, over a decade, trans-formed a small medical oncology practice into a $42 millioncancer treatment center. The Mark H. Zangmeister Center ofColumbus, Ohio, opened in 2007 to provide a full continuum ofoncology care, including medical oncology, radiation oncology,surgical oncology clinic space, outpatient office visits, diagnosticimaging, clinical lab services, cancer research and trials, specialtypharmacy, counseling, and other support and wellness services.
According to Glenn Balasky, executive director of theZangmeister Center, MOOH was a group of eight medicaloncologists working in two locations as recently as 1998. “Theyhad the foresight to adopt the OpTx computerized informationsystem before almost anyone was thinking about going paper-less,” says Balasky. OpTx was later acquired by Varian MedicalSystems and integrated into Varian’s ARIA oncology informa-tion system.
“Those doctors saw the future coming and got on board withautomation early,” Balasky says. “In the late 1990s, they wereseeking to create an environment of consistency and scalabilityin order to deliver care in exactly the same way across a growingnumber of sites. They were also looking at new forms of capitat-ed healthcare, and they knew that they needed better data on
what it was costing to deliver care in order to negotiate reason-able contracts.” That meant implementing a comprehensiveelectronic medical record (EMR).
There are other benefits to an EMR besides the ability toaggregate data. “An EMR gives you immediate access to infor-mation at any time, whether you’re a medical receptionistchecking someone in or a physician who needs to make clinicaldecisions based on lab tests,” Balasky says. “And an EMR canhelp prevent mistakes that happen more easily in a paper-basedenvironment. With consistency comes improved safety.”
MOOH had grown to four offices by 2004, when Balasky wasbrought on board to help develop a more integrated care model.“In this market, people were being sent off for radiation therapyto the hospitals that offered it, and coordinated care was diffi-cult. Our physicians had to do more work to communicate with
Paperless from the Start:TwoNewComprehensive Cancer
Centers Rely on ARIA
“An EMR can help prevent mistakesthat happenmore easily in a paper-based environment.With consistency
comes improved safety.”Glenn Balasky, Mark H. Zangmeister Center

C ENTER L I N E | O C TO B E R 2 0 0 7 17
a radiation oncologist, and we were sending our patients else-where for CT scans, X rays, lab tests, and radiation treatment.The logistics of delivering care were complicated, not to men-tion frustrating for patients.”
These considerations led to the development of theZangmeister Cancer Center, which opened in May 2007. Twelvemedical and two gynecological oncologists work with a separategroup of radiation oncologists to provide clinical care at thecenter. According to Balasky, even though the medical oncologypractice had been utilizing the Varian EMR, it was by no meansa foregone conclusion that they would adopt ARIA for theentire center. “As much as we valued our relationship withVarian, we felt we should look at all the options and see every-thing available from the radiation oncology perspective,” hesays. “After considering our options, however, we decided thatour ultimate goal is what Varian is working toward, namely, a
completely integrated solution. So we adopted ARIA threemonths before the center opened.”
Balasky says the deployment went well, partly because theystarted out committed to the paperless environment, allottedenough time for staff to learn the system, and made sure thatthey were using it from day one when they checked in the firstradiotherapy patient for treatment. “We moved into the centeron May 29, but we didn’t schedule radiotherapy patients untilAugust 15. That gave us plenty of time to learn the system,”Balasky says. “We were able to start with IMRT planned usingPET/CT images right from day one.”
Balasky points out that cancer patients’ treatment times canbe minimized through efficiency. “When an organization canmanage more services in-house, patients can benefit fromimmediate electronic scheduling,” he says. “By consolidating
all sides of the house with the ARIA system, we can save timefor the patient by eliminating the need to fill out paperwork inmultiple care settings.”
Reflecting on the rapid evolution of Mid Ohio Oncology/Hematology and its Zangmeister Center, Balasky says: “Havingan EMR allowed us to build the resources for growing organi-cally and then starting up a brand new center. Right now, forexample, we’re using an outside group to provide our physicsand dosimetry services, and we anticipate outsourcing thoseservices for at least two years. This allows us to match resourcelevels to our current needs. The electronic connectivity possiblewith ARIA makes that feasible.”
The Center for Radiation Therapy of Beverly Hills
The Center for Radiation Therapy of Beverly Hills is a newlyestablished radiation oncology clinic developed by TowerHematology Oncology Medical Group and professionallystaffed by Valley Radiotherapy Associates. Open for about oneyear, this radiation oncology center saw its first patient inSeptember 2006 after installing a Clinac® iX with the On-BoardImager® device. According to Tracey Butler, center manager,their original plan was to treat 25 to 30 patients per day on asingle linear accelerator. “By the end of the first year, we weretreating close to 49 patients a day, so we decided to add aTrilogy® machine, which was installed in early March. We start-ed Trilogy treatments in June. Now we’re averaging a little over60 patients per day.”
Butler was instrumental in helping to establish paperlessprocesses “from the get-go. The doctors designed the depart-ment based on an electronic environment,” she says. “We havecomputers in every consultation and exam room as well as atthe nursing station. We can access the medical and radiationoncology modules on all of our computers, as well as diagnosticimage data from hospitals and freestanding radiology depart-ments in our community. We can also access CT simulationdata stored in the Eclipse™ treatment planning system. Ourphysicians have never picked up a paper chart. From day one,even our billing has been all electronic.”
Leslie E. Botnick, MD, and Christopher M. Rose, MD, theboard-certified radiation oncologists who staff the center, arecommitted to a vision of a patient-centric medical record, andthey feel that Varian’s ARIA oncology information system hastaken them a good distance in this direction. “Eventually, whatthe cancer survivor community will demand from us is aportable record that the patient can take from place to place andthat the patient owns,” Rose says. “ARIA’s flexibility makes itpossible for you to create any kind of EMR, whether it’s patient-,disease-, or treatment-centric.”
All of the center’s clinicians were enthusiastic about workingin a completely paperless environment. “Still, we couldn’t haveaccomplished it without an enthusiastic champion in the
“Our physicians have never picked upa paper chart. From day one, even our
billing has been all electronic.”Tracey Butler, Center for Radiation Therapy of Beverly Hills

Varian Consulting Services:Help with Clinical Implementations
Many Varian customers have a goal ofmigrating their operations to a paperlessenvironment through use of the ARIA™ sys-tem.While some have the luxury of planningfor paperless workflows from the start, mostmust transition from current paper-basedpractices mixed with some electronic recordkeeping. Cathy Tenda, a clinical implementa-tion consultant with Varian’s CustomerSupport Services organization, is expert athelping people analyze their current prac-tices and translate them into electronicprocesses that take advantage of ARIA’s manysophisticated features.
“It takes a lot of collaborative effort, and itdoesn’t happen overnight,”Tenda says.“When customers are converting to ARIAfrom another system, we’re involved up frontfor about two months, on average.We lookfor potential roadblocks in the customer’sworkflow that may have developed becausetheir system forces a certain way of doingthings that are done differently with ARIA.
That might require a process change, or itmight require some customization of thedatabase. Our job is to figure out the short-est distance between the two points and tohelp the customer get there with a minimumof disruption.”
Tenda, herself a radiation therapist andapplications expert, also looks for ways ofreengineering processes for maximum effi-ciency. “For example, if the departmental sec-retary is performing a task that it reallymakes sense for the nurse to do, we can helpstructure a change that takes advantage ofthe ARIA system’s greatest strengths.”
Sue Merritt, Varian’s manager of clinicalimplementation consulting, explains thatconsulting services start with a detailedanalysis of “what is,” to fully understand howthe customer is currently working. The con-sultant then helps to configure ARIA to sup-port their processes.
“We gather every piece of paper a customeruses, whether it’s a form the patient receivesor a document the clinician needs,”Tendasays. “We analyze them to determine if thefunction can be eliminated, if it’s something
that’s already part of ARIA, or if it can beadded to the system using DynamicDocuments.We talk about it with the cus-tomer as we develop the “to be”workflowmap. Because we know the ARIA system, weknow where each element fits in and we cancome close to mimicking what the customeris currently doing.”
Tenda also sometimes weaves in some “bestpractices” suggestions based on her experi-ence with optimal ways of using ARIA. “Butthe main goal is to get the customer up andrunning as quickly as possible without a lotof changes to their processes,” she says.
According to Merritt, Varian is planning tolaunch comprehensive “best practices” con-sulting services in 2008 to augment the serv-ices already offered for those converting toARIA. “This is for customers who have beenworking with ARIA for some time and arelooking to maximize their efficiency throughmore rigorous process reengineering. By theyear 2010, the U.S. government is going torequire all cancer centers to be operatingelectronically. Varian is dedicated to helpingcustomers get there.” �
18 C ENTER L I N E | O C TO B E R 2 0 0 7
department who demanded that we adjust our processes andlearned how to set up dynamic documents within the ARIA sys-tem,” Rose says. “Tracey played that role for us.”
“We established a rule,” Butler adds. “If you want somethingon paper, fine, but it still has to go into the electronic record.”
That meant that Butler had to become intimately acquaintedwith ARIA’s Dynamic Documents feature, which allows her tocreate forms that automatically populate certain fields with datafrom the EMR. “I learned how to create the electronic documentsthat we use throughout our department, following our patient-centric way of working and using information,” she says. “Everytime a therapist comes to me to say, ‘I need a new document forthis or that,’ I’m thrilled. That means they’ve gotten comfortablewith the system. When you keep some piece of information justin your own mind, if something happens to you, it might take thedepartment three days to figure out what you were thinking.Documentation solves those types of problems. Fortunately,everyone here had the mindset for going paperless.”
Compared with their previous experience using paper charts,the doctors appreciate accessing every piece of information theyneed anywhere within the department. “Thank goodness forOffline Review,” Butler says. “Most of our treatments use imageguidance, and we have a comprehensive cone-beam CT pro-gram, so we’re generating a lot of images. The doctors are com-fortable with the system, and they’re reviewing images all dayin real time to satisfy the requirements for IGRT. They alsoapprove documents throughout the day. We don’t have to chase
them around for signatures or search for them because we needa document approved. If the system were less user-friendly, thiswould all be much harder. We just wouldn’t be able to treat thenumber of patients that we do.”
In this paperless environment, the radiation oncology nurse’srole has evolved. According to Rose, the nurse has becomemuch more efficient and is able to spend more time withpatients, assessing their responses to therapy and radiation sideeffects. “The nurse and the physicians interact with each otherin a more collaborative fashion, using the electronic record asthe collaboration environment,” he says. “Doctors and nurses allenter patient data into the record. We’ve also been using ARIAto allow patients to directly enter their own quality-of-life indi-cators. We even show them tumor response by giving themdirect access to their cone-beam CT images.”
These patient-centered processes are enabling a higher levelof personalized, quality care, according to Rose. “Les Botnick,Tracey Butler, and I are excited about future enhancementscoming to the ARIA program, tying together staging and treat-ment information in a tightly linked process of care,” he says.“In the future, we hope to access the ARIA database, which tellsyou everything about every patient and what you’ve done clini-cally in each case, and link that information up with outcomes,to really understand what’s working best and for whom. That’sthe future of informatics, and as a paperless center, we’re welldown that road.” �

C ENTER L I N E | O C TO B E R 2 0 0 7 19
By Steven K. Wagner
Varian’s Customer Support Services organiza-tion is a far-reaching network of profession-als dedicated to meeting customers’ needs for
service and support. Approximately 1,500 people workin positions that directly support customers, whether bystaffing the help desk, managing system installations,providing implementation instruction, or dispatchingfield engineers. “We aim to provide unsurpassed supportso our customers’ clinical teams can focus on patientcare,” says Kolleen Kennedy, Varian’s vice president ofworldwide customer support.With this issue, Centerline publishes its second install-
ment on service and support, focusing on the teams thathandle new installations as well as major upgrades.
As they pondered adding sophisticated new technology fromVarian Medical Systems, the principals at NY RadiationAssociates didn’t want to underestimate the time it would taketo add an On-Board Imager® device to their existing linearaccelerator. Timing, they reasoned, would be crucial to the suc-cess of any effort that enabled implementation of image-guidedradiation therapy (IGRT). It was then mid-2006.
Fortunately for Jack Dalton, MD, and his partner, RobertoLipsztein, MD, just as they were considering how their practicemight fare during the downtime, Varian made an excitingannouncement: every effort would now be made to install On-Board Imager devices within 5 to 10 business days, and IGRT-enabled Clinac® systems within about a month—cutting installa-tion times in half.
Installation Times for IGRTUpgradesand NewMachines Cut in Half
FOCUS ON SERVICE | SECOND IN A SERIES
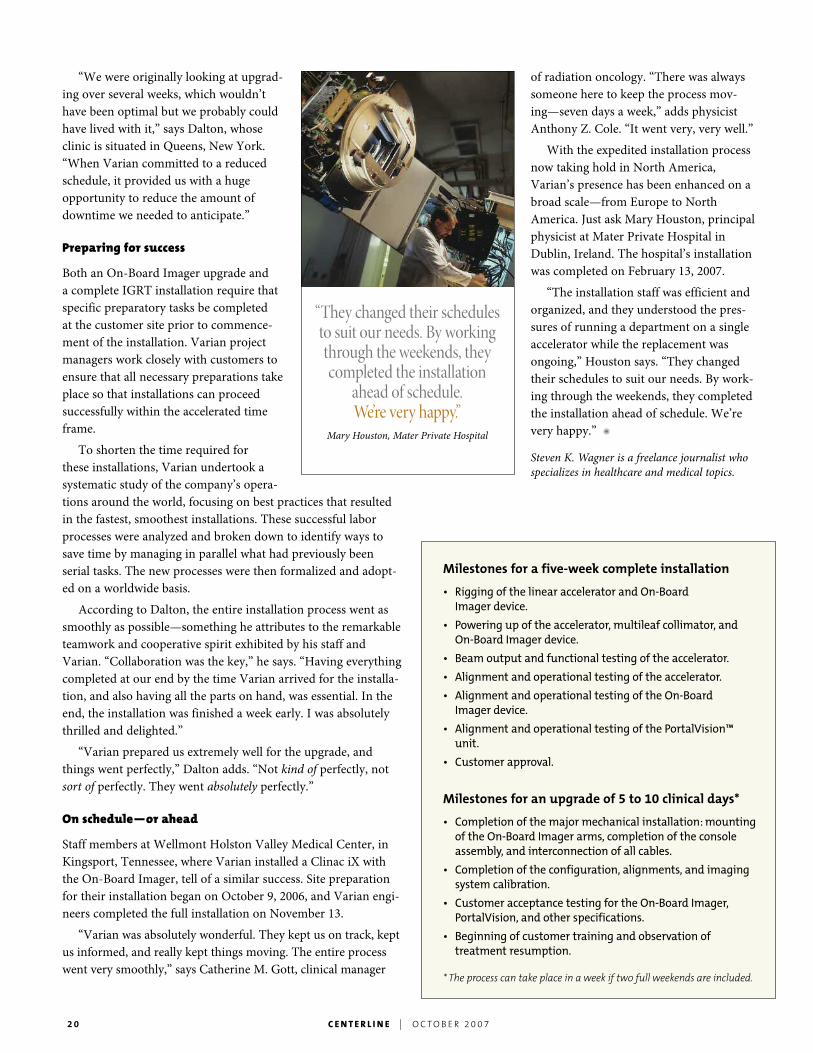
Medical physicist Byong Yi, PhD, conducts quality assurance testson a newly installed Trilogy linear accelerator at the University ofMaryland School of Medicine.
20 C ENTER L I N E | O C TO B E R 2 0 0 7
“We were originally looking at upgrad-ing over several weeks, which wouldn’thave been optimal but we probably couldhave lived with it,” says Dalton, whoseclinic is situated in Queens, New York.“When Varian committed to a reducedschedule, it provided us with a hugeopportunity to reduce the amount ofdowntime we needed to anticipate.”
Preparing for success
Both an On-Board Imager upgrade anda complete IGRT installation require thatspecific preparatory tasks be completedat the customer site prior to commence-ment of the installation. Varian projectmanagers work closely with customers toensure that all necessary preparations takeplace so that installations can proceedsuccessfully within the accelerated timeframe.
To shorten the time required forthese installations, Varian undertook asystematic study of the company’s opera-tions around the world, focusing on best practices that resultedin the fastest, smoothest installations. These successful laborprocesses were analyzed and broken down to identify ways tosave time by managing in parallel what had previously beenserial tasks. The new processes were then formalized and adopt-ed on a worldwide basis.
According to Dalton, the entire installation process went assmoothly as possible—something he attributes to the remarkableteamwork and cooperative spirit exhibited by his staff andVarian. “Collaboration was the key,” he says. “Having everythingcompleted at our end by the time Varian arrived for the installa-tion, and also having all the parts on hand, was essential. In theend, the installation was finished a week early. I was absolutelythrilled and delighted.”
“Varian prepared us extremely well for the upgrade, andthings went perfectly,” Dalton adds. “Not kind of perfectly, notsort of perfectly. They went absolutely perfectly.”
On schedule—or ahead
Staff members at Wellmont Holston Valley Medical Center, inKingsport, Tennessee, where Varian installed a Clinac iX withthe On-Board Imager, tell of a similar success. Site preparationfor their installation began on October 9, 2006, and Varian engi-neers completed the full installation on November 13.
“Varian was absolutely wonderful. They kept us on track, keptus informed, and really kept things moving. The entire processwent very smoothly,” says Catherine M. Gott, clinical manager
of radiation oncology. “There was alwayssomeone here to keep the process mov-ing—seven days a week,” adds physicistAnthony Z. Cole. “It went very, very well.”
With the expedited installation processnow taking hold in North America,Varian’s presence has been enhanced on abroad scale—from Europe to NorthAmerica. Just ask Mary Houston, principalphysicist at Mater Private Hospital inDublin, Ireland. The hospital’s installationwas completed on February 13, 2007.
“The installation staff was efficient andorganized, and they understood the pres-sures of running a department on a singleaccelerator while the replacement wasongoing,” Houston says. “They changedtheir schedules to suit our needs. By work-ing through the weekends, they completedthe installation ahead of schedule. We’revery happy.” �
Steven K. Wagner is a freelance journalist whospecializes in healthcare and medical topics.
Milestones for a five-week complete installation
• Rigging of the linear accelerator and On-BoardImager device.
• Powering up of the accelerator, multileaf collimator, andOn-Board Imager device.
• Beam output and functional testing of the accelerator.
• Alignment and operational testing of the accelerator.
• Alignment and operational testing of the On-BoardImager device.
• Alignment and operational testing of the PortalVision™unit.
• Customer approval.
Milestones for an upgrade of 5 to 10 clinical days*
• Completion of the major mechanical installation:mountingof the On-Board Imager arms, completion of the consoleassembly, and interconnection of all cables.
• Completion of the configuration, alignments, and imagingsystem calibration.
• Customer acceptance testing for the On-Board Imager,PortalVision, and other specifications.
• Beginning of customer training and observation oftreatment resumption.
* The process can take place in a week if two full weekends are included.
“They changed their schedulesto suit our needs. By workingthrough the weekends, theycompleted the installation
ahead of schedule.We’re very happy.”
Mary Houston, Mater Private Hospital
C ENTER L I N E | O C TO B E R 2 0 0 7 21
T R A I N I N G U P DAT E S
High-Dose-Rate Brachytherapyfor Prostate, Gynecological,and Breast Cancer course
Seattle Prostate InstituteSeattle,Washington
November 12–13, 2007February 25–26, 2008June 23–24, 2008
Visit: http://www.seattleprostateinst.com/coursedescriptions.htm
IGRT School for Radiation Therapists
MIMA Cancer CenterMelbourne, Florida
Ongoing; three-day sessionsfrequently scheduled
Call: 321.409.1956
IGRT Short Course
Stanford University Cancer CenterStanford, California
January 18–19, 2008May 2–3, 2008
Visit: http://www.stanford.edu/~lei
IMRT School
UMass Memorial Medical CenterWorcester, Massachusetts
March 29–30, 2008
Visit: http://www.knownexus.com/
Ultrasound-Guided TransperinealBrachytherapy for Early-Stage ProstateCancer course
Seattle Prostate InstituteSeattle,Washington
December 10–11, 2007January 14–15, 2008March 3–4, 2008June 9–10, 2008
Visit: http://www.seattleprostateinst.com/coursedescriptions.htm
Varian product training programs
Varian Training Centers
Milpitas, California, and Las Vegas, Nevada
Visit: http://www.varian.com/courses
Visit http://www.varian.com/oncy/new117.html for a complete calendar of conferences and events.
Acuity™ Support course
Crawley, UK
January 21–25, 2008April 14–18, 2008June 30–July 4, 2008
Acuity TechnicalMaintenance course
Crawley, UK
November 5–9, 2007January 28–February 1, 2008April 21–25, 2008
Eclipse™ Application course
Zug, Switzerland
November 13–15, 2007December 11–13, 2007January 15–17, 2008February 19–21, 2008March 11–13, 2008April 15–17, 2008May 27–29, 2008
Eclipse in Clinical Practicecourse
Zug, Switzerland
January 18, 2008
February 22, 2008March 14, 2008April 18, 2008May 30, 2008
Eclipse Managementcourse
Zug, Switzerland
November 6–9, 2007December 4–7, 2007January 8–11, 2008February 12–15, 2008March 4–7, 2008April 8–11, 2008May 20–23, 2008June 24–27, 2008
Electron Monte CarloAlgorithm course
Zug, Switzerland
November 9, 2007December 7, 2007January 11, 2008February 15, 2008March 7, 2008April 11, 2008May 23, 2008June 27, 2008
Gating School
Copenhagen, Denmark
November 15–17, 2007
IGRT School
Wirral, UK
December 6–8, 2007
IMRT School
Berlin, Germany
November 27–30, 2007January 22–25, 2008March 11–14, 2008May 20–23, 2008
Dijon, France
February 26–29, 2008
Oncology InformationSystem Administrationcourse
Zug, Switzerland
November 12–16, 2007December 10–14, 2007February 4–8, 2008March 3–7, 2008April 7–11, 2008
May 5–9, 2008June 9–13, 2008
Oncology InformationSystem Implementationcourse
Zug, Switzerland
November 6–9, 2007December 4–7, 2007January 15–18, 2008February 12–15, 2008March 11–14, 2008April 15–18, 2008May 27–30, 2008June 24–27, 2008
Oncology InformationSystem Reports course
Zug, Switzerland
November 20–22, 2007February 26–28, 2008April 22–24, 2008
European training opportunitiesCall +41 (0) 41.749.88.44 or e-mail [email protected] to learn more about European training opportunities.
North American training opportunities
Varian Medical Systems3100 Hansen WayPalo Alto, CA 94304-1038
Bulk RateU.S. Postage
PAIDSan Jose, CA
Permit No. 2196
When battling cancer,every second counts.Put time on your side.
RapidArc™.
Pending FDA 510(k) approval; not available for sale in the United States at this time.