VII. PAIN AND TINNITUS
25
VII. PAIN AND TINNITUS 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 3B2v8:06a=w ðDec 5 2003Þ:51c XML:ver:5:0:1 PBR V157 : 57020 Prod:Type: pp:3312353ðcol:fig::NILÞ ED: PAGN: SCAN:
Transcript of VII. PAIN AND TINNITUS

VII. PAIN AND TINNITUS1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
3B2v8:06a=w ðDec 5 2003Þ:51cXML:ver:5:0:1 PBR� V157 : 57020 Prod:Type:
pp:3312353ðcol:fig::NILÞED:
PAGN: SCAN:

1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
Moller (Ed.)
Progress in Brain Research, Vol. 157
ISSN 0079-6123
Copyright r 2006 Elsevier B.V. All rights reserved
CHAPTER 20
Plasticity in brain processing and modulation of pain
Donald D. Price1,�, G. Nicholas Verne2 and Jeffrey M. Schwartz3
1Oral and Maxillofacial SurgeryQA :1 , University of Florida, Gainesville, FL, USA2College of Dentistry, University of Florida, Gastroenterology, University of Florida, Gainesville, FL, USA3College of Medicine, and U.C.L.A. Neuropsychiatric Institute, University of Florida, Gainesville, FL, USA
Abstract: Brain processing of pain in humans is based on multiple ascending pathways and brain regionsthat are involved in several pain components, such as sensory, immediate affective, and secondary affectivedimensions. These dimensions are processed both serially and in parallel. They include spinal ascendingpathways that directly target limbic and brainstem structures involved in pain-related emotions as well as apathway proceeding from the somatosensory cortices to limbic cortical areas. Superimposed on this neuralorganization is the capacity to process the dimensions of pain in multiple ways, as in patients who lack onecerebral hemisphere but can nevertheless locate and rate pain intensity and pain unpleasantness on bothsides of the body. The dimensions of pain also can be psychologically modulated in multiple ways and thesechanges are accompanied by corresponding changes in relevant brain structures. Finally, understandingpsychological modulation of pain and pain-related brain activity is optimized by a scientific framework thatintegrates principles of contemporary physics, neuroscience, and human experiential science.
Keywords: parallel processing; serial processing; multiple representations; pain; quantum zeno effect; self-directed neuroplasticity
Introduction
Beyond the levels of primary afferents and spinalcord neurons, information concerning the process-ing of nociceptive information and representationof different dimensions of pain within the brain,until recently, has been scant and controversial.Prior to the advent of modern neural imaging ofpain, most of the information about brain mech-anisms of pain in humans was derived from studiesthat evaluated effects of destructive lesions orelectrical stimulation. Within the last 15 years,however, considerable neurophysiological and ne-uroanatomical information about brain mecha-nisms of pain has accumulated from animalexperiments, human experiments involving micro-stimulation and microelectrode recordings within
the brain, and animal and human neural-imagingstudies. This chapter reviews brain mechanisms ofpain, with emphasis on neuroplastic mechanisms.It focuses on divergent sources of knowledgeabout brain mechanisms of pain and synthesizesthis information in a manner that helps explainhow pain is highly modified by psychological fac-tors and how different dimensions of pain can berepresented in multiple ways. First, the dimensionsof pain will be described and briefly explained.Second, the ascending pathways for pain andfunctional types of nociceptive neurons of theircentral-target brain structures will be discussed inrelation to the dimensions of pain. Third, brainregions and networks that underlie the represen-tation and processing of different dimensions andstages of pain will be discussed. Neuroplasticity ofthese networks will be emphasized in two ways.First, evidence will be presented that similar types
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
�Corresponding author.; E-mail: [email protected]
DOI: 10.1016/S0079-6123(06)57020-7 333

of pain can be represented in multiple ways and inmultiple circuits, for example, in different path-ways of split-brain patients and persons with earlycerebral damage. Second, evidence will be pre-sented that neural activity in pain-related areas ofthe brain can be powerfully altered by psycholog-ical methods, including placebo, hypnosis, andchanges in attention. Thus, evidence for consider-able plasticity of brain mechanisms underlyingpain will be reviewed. The schematics in Figs. 1and 2 serve as guides to discussions of the dimen-sions of pain and their associated anatomicalpathways and brain structures.
What are the dimensions of pain and how do they
interact?
Pain is an experience that is comprised of uniquesomatic or visceral sensory qualities, such as‘‘burning,’’ ‘‘stinging,’’ or ‘‘aching’’, combinedwith a sense of intrusion or threat, or both, andan associated feeling of unpleasantness or othernegative emotional feelings (Price, 1999). Someemotional feelings pertain to the immediate pre-sent and others may pertain to the long-term fu-ture implications and past. Thus, pain includes asensory dimension, an immediate affective dimen-sion (e.g., unpleasantness), and sometimes a sec-
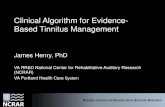
ondary affective dimension, termed pain-relatedsuffering. The latter is based on rumination or re-flection and pertains to the long-term implicationsof having pain, such as interruption of life activ-ities and other concerns with future consequences.Psychophysical studies demonstrate that the firsttwo pain dimensions have reliably different rela-tionships to nociceptive stimulus intensity and canbe differentially influenced by various psycholog-ical factors (Fig. 1; Price, 1999, 2000).
Numerous studies support the view that thesensory and immediate affective dimensions ofpain are separate and unique, even though they areoften closely associated (See Price and Harkins,1992; Price, 1999, 2000; for reviews). Two relatedexperiments clearly illustrate this view and helpestablish the direction of causation between thetwo dimensions (Rainville et al., 1992). Both ex-periments were part of a hypnosis study in whichpain was induced in study participants by immers-ing their left hands in a moderately painful water-bath heated to 47 1C. In the first experiment, hyp-notic suggestions were alternately given to enhanceor decrease pain unpleasantness without changingpain-sensation intensity. In the second, the hyp-notic suggestions were targeted specifically towardenhancing or decreasing pain-sensation intensityand nothing was stated about pain unpleasantness.Pain unpleasantness but not pain-sensation inten-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
Fig. 1. Schematic representation of major dimensions of pain and their interactions.
334

sity ratings were changed in the directions sug-gested in the first experiment, a result that was notsurprising. However, both pain-sensation intensityand pain unpleasantness ratings changed in paral-lel in the second experiment despite the fact thatthe suggestions did not mention pain unpleasant-ness. This study helps to establish that the direc-tion of causation-pain sensation is more of animmediate cause of pain unpleasantness than is thelatter a cause of pain sensation. Thus, there is aserial relationship between the sensation of painand its associated unpleasantness. Other psycho-physical experiments and studies of pain patientsalso support a serial relationship between pain-sensation intensity and pain unpleasantness (Priceet al., 1987; Price, 1999, 2000). At the same time,the first experiment showing selective effects onunpleasantness suggests parallel influences on painunpleasantness (Fig. 1). If pain unpleasantness canbe selectively altered, pain sensation cannot be theonly cause of unpleasantness. Parallel influences
result from physical and psychosocial context andmemory.
Likewise, studies of pain patients show the dis-tinction between immediate pain unpleasantnessand pain-related suffering and their sequential in-teractions. Similar to the selective effects of sometypes of hypnotic suggestion on pain unpleasant-ness, personality traits and some demographiccharacteristics such as age can selectively influencepain-related suffering. For example, neuroticismenhances (Harkins et al., 1989) and age reduces(Riley et al., 2000) pain-related suffering withoutchanging the sensory intensity or immediate un-pleasantness of pain. Pain unpleasantness main-tains and is more of a cause of pain-relatedsuffering than vice versa. However, Rainville etal. (2005) have shown some recursive effects be-tween pain-related suffering and immediate painunpleasantness, because increases in pain-relatedsecondary emotions such as depression, anxiety,anger, and sadness were shown to enhance imme-diate pain unpleasantness. The effects on pain-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
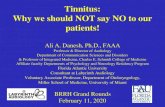
Fig. 2. Schematic of ascending pathways, subcortical structures, and cerebral cortical structures involved in processing pain. Symbols
are those defined and referred to within text.
335

sensation intensity were not significant. Thus, re-cursive effects of the model (Fig. 1) do not extendacross all stages, whereas changes in magnitudes ofnociceptive sensations would normally affect allsubsequent stages.
The sequential model of sensory intensity–un-pleasantness–pain related suffering also is sup-ported by multivariate (linear structural relations)analyses of ratings of these dimensions in largesamples of pain patients (Wade et al., 1996; Rileyet al., 2000, 2002; Lackner et al., 2005). The se-quential model (Fig. 1) has been repeatedly con-firmed and scores high on several indices ofgoodness-of-fit (Wade et al., 1996; Riley et al.,2000, 2002; Lackner et al., 2005). This model pro-vides a psychological framework that will be dis-cussed in relation to ascending pathways and braincircuits, as well as to mechanisms by which paincan be modified. Ideally, physiological activity inascending pathways and brain circuits should helpexplain psychological models of pain, such as theserial/parallel processing model of Fig. 1.
Ascending nociceptive pathways to the brain
The lateral spinothalamic tract and its thalamicprojection to somatosensory cortices
For the most part, the central nervous system or-igin of pain-related pathways is the dorsal horn ofthe spinal gray matter. A major pathway projectsin the lateral spinothalamic tract to the ventralposterior lateral (VPL) nucleus of the thalamus.Dorsal-horn neurons of origin of this pathway arecomprised of wide dynamic range (WDR) neuronsthat respond differentially to gentle and no-ciceptive levels of stimulation as well as no-ciceptive-specific (NS) neurons that respondpredominantly to nociceptive stimuli (Price andVerne, 2002; Price et al., 2003). WDR neurons re-ceive synaptic input from both primary-afferentnociceptive neurons and low-threshold mechano-receptive neurons. As a consequence of this con-vergence, they respond with increasing impulsefrequency over a very wide range of stimulationintensity, such as very gentle touch or hair move-ment to tissue-damaging stimuli (Price et al., 1976,
1978, 1979; Willis, 1985). Hence, the term ‘‘widedynamic range’’ aptly applies to this class of neu-rons. Based on a review by Willis et al. (2003),their anatomical work (Willis et al., 2001), andnumerous studies of nociceptive neurons in thedorsal horn (See references in Price and Verne,2002; Price et al., 2003), VPL (Casey and Morrow,1983; Chung et al., 1986; Lenz et al., 2004), andprimary somatosensory cortex (S1) (Kenshalo andIsensee, 1983; Kenshalo et al., 1988, 2000), there isconsiderable evidence that the large majority(470%) of neurons in the lateral spinothalamictract and its thalamic extension to S1 are WDRneurons and most of the remaining neurons areNS. Spinal-cord WDR and NS neurons at the or-igin of this pathway are located in superficial anddeep layers of the dorsal horn (Price et al., 1976,1978, 1979; Willis, 1985). WDR and NS neuronswithin the lateral spinothalamic tract and its cen-tral targets are intermingled at all levels of thispathway (Kenshalo et al., 2000; Willis et al., 2003;Price et al., 2003).
Similar to psychophysical responses of bothmonkeys and humans, monkey WDR neurons atdorsal horn and cortical levels can detect verysmall changes in nociceptive stimulus intensity.For example, they reliably increase their impulsefrequencies in response to very small 0.2–0.4 1Ctemperature shifts during nociceptive skin temper-atures such as 46 and 47 1C (Bushnell et al., 1984;Dubner et al., 1986; Kenshalo et al., 1988; Ma-ixner et al., 1989). In contrast, NS neurons did notmake such fine discriminations. Based on the ca-pacity of WDR to precisely encode stimulus fea-tures of nociceptive stimuli, the parallels betweenWDR neuron and psychophysical responses tonociceptive stimuli, and the strong predominanceof WDR neurons in the lateral spinothalamictract, it has become abundantly clear that WDRneurons have important roles in the sensoryprocessing of pain.
The predominance of WDR neurons in thispathway has large implications for neuroplasticityin the processing of pain. The reason is that WDRneurons have a distinct receptive-field organizationthat can change over time as a result of severalphysiological and psychological factors. The re-ceptive fields of WDR neurons consist of a rela-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
336

tively small skin area (e.g., 15 cm2) within whichnociceptive stimuli (e.g., 45–511C) evoke higherimpulse frequencies than gentle mechanical stimuli(e.g., guard hair deflection or indentation with vonFrey filaments with forces less than 50mg), sur-rounded by a larger area (e.g., 50–70 cm2) whereinintense (e.g., 41 g von Frey filament) or no-ciceptive stimuli are needed to evoke impulse re-sponses. However, the sizes of these receptive-fieldareas are not constant but critically depend on thehistory of stimulation and upon psychological fac-tors such as attention. The factors that inducechanges in WDR-receptive field sizes will be dis-cussed in the section on pain modulation.
The organization and sizes of WDR-receptivefields are integral to their ability to distinguishnociceptive from non-nociceptive stimulation andto encode the intensity of nociceptive stimulation(Price et al., 2003). Populations of WDR neuronsare capable of encoding these distinctions as wellas localizing the peripheral source of nociceptivestimulation (Price et al., 1978; Price 1988, 1999;Coghill et al., 1993).
Unlike WDR neurons, NS neurons receive ex-clusive synaptic input from primary nociceptiveafferent neurons and they comprise 20–30% ofneurons within the spinothalamocortical pathwayto S1 (Kenshalo et al., 2000). They also have animportant role in pain, probably that of identify-ing some of the stimulus features of nociceptivestimuli. Because of their small receptive fields andspecific responsiveness to one or more forms ofnociceptive stimulation (e.g., heat, pinch), theymay fine-tune the ability to recognize the body lo-cation and particular type of nociceptive stimulus(e.g., mechanical). NS neurons are likely to func-tion in concert with WDR neurons. In general, thephysiological characteristics of both types of neu-rons observed at the level of the spinal-cord dorsalhorn appear to be preserved within brain areasthat receive input from these spinal-cord neurons.Thus, both WDR and NS neurons are present atseveral brainstem and cortical levels and theirphysiological characteristics resemble those of dor-sal horn nociceptive neurons in many ways.
Other ascending nociceptive pathways to the brain
Several other ascending spinal pathways are im-portant for pain (Fig. 2). An interesting differencebetween some of these pathways and the lateralspinothalamic tract is that unlike the latter, theformer often reflect a preponderance of NS neu-rons. For example, Bernard and colleagues havecharacterized two novel pathways for pain, termedthe spino-parabrachio-amygdaloid and the spino-parabrachio-hypothalamic pathway (Bernard etal., 1989; Bernard and Besson, 1990). The mostremarkable and consistent feature of nociceptiveneurons within these two pathways is that theymainly comprised of neurons predominantly re-sponsive nociceptive stimulation, that is, NS neu-rons. This pattern is nearly the reverse of thelateral spinothalamic tract. Consistent with thisunique feature is the finding that spinal-cord neu-rons of the origin of these pathways are exclusivelywithin layer I of the dorsal horn, a region con-taining more NS than WDR neurons (Price andDubner, 1977). Neurons within these pathwaysappear to encode nociceptive stimulus intensitywith some degree of precision. These two path-ways offer a striking comparison with the lateralspinothalamic tract because of the very differentproportions of WDR and NS neurons and becausetheir central targets appear functionally verydifferent. Whereas the lateral spinothalamic tractand pathway to S1 is likely to be heavily involvedin sensory-perceptual aspects of pain, the twopathways to the amygdala and hypothalamus aremore likely to be heavily involved in autonomicprocesses and behaviors related to fear and def-ense. The central nucleus of the amygdala has beenstrongly implicated in fear, emotional memory andbehavior, and autonomic and somatomotor re-sponses to threatening stimuli (Bernard and Bes-son, 1990). Various hypothalamic nuclei have alsobeen implicated in these functions. Based largelyon their central targets, these pathways are verylikely to strongly participate in the affective di-mension of pain, particularly the initial affect as-sociated with acute pain. There is also aspinohypothalamic pathway that contains neuronslike those of the spinothalamic tract, and in factmany of the latter send axonal projections to both
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
337

thalamus and hypothalamus (Burstein et al., 1987;Dado et al., 1994; Giesler et al., 1995). Spin-othalamic tract neurons projecting to more ventraland medial thalamic nuclei also appear to havemuch greater proportions of NS neurons (Willis,1985; Giesler et al., 1981; Lenz et al., 1993).
Which central targets of ascending pathways
participate in sensory and emotional aspects of pain?
The foregoing analysis suggests the existence ofseveral functionally different ascending pathwaysfor pain. WDR neurons are critical for appreciat-ing the intensity of painful sensations, which inturn contribute to pain-related emotions. Otherpathways that contain mostly NS neurons are alsoimportant for several aspects of pain, includingaffect, motivation, autonomic and somatomotoractivation, and possibly pain sensation. Althoughthese different pathways are functionally diverse,we do not interpret them as supporting the classicview of two ascending spinothalamic systems forpain, a lateral system for sensory discriminationand a medial one for pain-affect (Melzack andCasey, 1968). We are in strong disagreement withthis classic view because it is overly simplistic anddoes not account for numerous anatomical, phys-iological, and psychological observations. Mostcritically, it does not take into account the possi-bility of multiple central representations of thesame pain dimension (e.g., pain-sensation intensityand pain unpleasantness) and the role of neuro-plasticity. The following discussion provides analternative account of how sensory and emotionaldimensions of pain are represented within thebrain and depend on interactions within a distrib-uted network.
As illustrated in the schematic of Fig. 2, someascending spinal pathways target limbic structuressuch as the amygdala, insular cortex (IC), and an-terior cingulate cortex. Some of these structures,such as the amygdala, are likely to be involved inrudimentary emotions such as fear. Others termi-nate in brainstem areas involved in arousal (re-ticular-formation nuclei), motoric orientation(superior colliculus), autonomic nervous-systemresponses (parabrachial nucleus, hypothalamus),
and neuroendocrine responses (hypothalamus).All of these structures are involved in monitoringthe state and integrity of the body, and are part ofthe regulation of emotions and consciousness itself(Damasio, 1994; Price 1999, 2000). However, thesomatosensory cortices and posterior parietal cor-tices are equally important inputs to limbic corticalstructures, such as the insula and anterior cingu-late cortex (Friedman et al., 1986; Neal et al., 1987,1990). Therefore, there are two general ways thatascending pain-related information can accessbrainstem and limbic cortical structures involvedin pain affect. One type of pathway targets thesestructures without directly activating somatosen-sory cortices, and the other proceeds through thesomatosensory and posterior parietal cortices. Asshown in Fig. 2, the lateral spinothalamocorticalpathway is anatomically interconnected from S1 toa ventrally directed corticolimbic, somatosensorypathway that targets the very same limbic corticalareas that are more directly targeted by ascendingspinal pathways. It has been proposed that thiscorticolimbic pathway integrates somatosensoryinput with other sensory modalities such as visionand audition and with learning and memory(Friedman et al., 1986). This pathway proceedsfrom S-1/S-2 to posterior parietal cortical areasand to IC and from IC to amygdala, perirhinalcortex, and hippocampus (Friedman et al., 1986;Neal et al., 1987, 1990; Price, 2000).
One can conceptualize the schematic model ofFig. 2 as supporting the existence of both serialand parallel pathways for processing the differentdimensions of pain. The serial pathway projectsvia a somatosensory–limbic connection and theparallel pathway through lower brainstem andthalamic nuclei to limbic structures. In our view,the serial pathway contributes to both sensory andaffective dimensions of pain and other parallelpathway also contributes to multiple componentsof pain, including emotional feelings. This expla-nation is also consistent with the way pain dimen-sions are psychologically processed, as shown inFig. 1.
Neurological evidence supports this view aswell. Thus, it shows involvement of the lateralspinothalamic tract to VPL and pathway to S1 inboth sensory and affective dimensions of pain.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
338

Damage to S1 or to the lateral thalamus producesreduced capacity to appreciate both the sensoryintensity and unpleasantness of a nociceptive stim-ulus (Head and Homes, 1911; Echols and Clogc-lough, 1947; Kenshalo et al. 1989; Greenspan etal., 1997; Ploner et al., 1999;;). Lesions of thepostcentral gyrus produce a temporary reductionin ongoing clinical pain intensity (Lewin and Phil-lips, 1952; White and Sweet, 1969QA :2 ). Both Ploner etal. (1999) and Head and Holmes (1911) found pa-tients with lesions of either the somatosensorycortices or lateral somatosensory thalamus (one ofthese was histologically verified to be within VPL)to have deficits in pain appreciation, includingboth pain-sensation intensity and pain unpleasant-ness. This deficit was manifested as an inability toexperience either sensations or unpleasantness inresponse to mild or moderate nociceptive stimulusintensities, such as 45–47 1C skin temperatures(Head and Holmes, 1911). These same patients,however, developed vague feelings of unpleasant-ness or ‘‘pain-like’’ feelings when the stimulus in-tensity was raised to still higher levels ofstimulation, such as 50 1C. Thus, interruption ofthe pathway to VPL and S-1/S-2 cortex produces adeficit in pain sensation and pain-related unpleas-antness throughout most of the nociceptive range.When the stimulus intensity reaches a high-enoughlevel, other pathways contribute in a parallel man-ner to unpleasantness. Finally, recent observationsfrom lesion and brain-imaging studies in humanssuggest that S1, S2, and IC may be necessary forthe recognition of negative emotions in others aswell as self-generated negative emotions (Damasio,1994; Adolphs et al., 2000).
Electrical stimulation of some sites withinthalamic VPL elicits pain, often with normal sen-sory qualities (Lenz et al., 2004). These sites werestimulated in patients who were undergoing brainsurgery for movement disorders (n ¼ 50) orchronic pain (n ¼ 16). They were awake and ratedevoked pain on visual analog scales. Two types ofresponses were observed. At some ‘‘pain sites’’ in-creasing frequencies of stimulation evoked gradedsensations that extended from nonpainful to pain-ful, similar to the graded responses of WDR neu-rons recorded in VPL of the same participants.Stimulation of other sites specifically evoked only
pain, consistent with the selective nociceptive re-sponses of NS neurons in VPL of these partici-pants. Using the same technique of combiningsingle-neuron recording and electrical stimulationin awake patients, neurons have been found withinthe region posterior and inferior to VPL that re-spond exclusively to noxious stimuli (Lenz et al.,1988, 1993). Microstimulation of these sites at ornear these NS neurons evoked only pain sensa-tions (e.g., heat but not touch). These sites arelikely to correspond to the posterior nuclear com-plex of other primates.
Although the evidence is more scant and con-troversial, electrical stimulation within the post-central gyrus sometimes evokes pain in humans.Though a systematic search was not undertaken tofind cortical sites involved in pain, Penfield andBoldrey (1937) found 11 out of 426 stimulationsites wherein electrical stimulation of the exposedpostcentral gyrus produced painful sensations inpatients. These reports were such rare occurrencesthat the investigators concluded that appreciationof pain was not represented in the postcentralgyrus (S1). However, the fact that stimulation of atleast some postcentral gyrus sites produced pain isevidence in favor of a role of the postcentral gyrusin sensory discriminative aspects of pain. The pau-city of specific pain-related cortical sites couldpartly reflect the fact that Penfield and Boldreywere not specifically searching for pain sites. An-other attempt to evoke pain by stimulation of thepostcentral gyrus has shown that intense and un-pleasant pains could be consistently elicited bystimulation of some sites within this region (Echolsand Cogclough, 1947). The problem with thisstudy is that it was carried out on patients suffer-ing from phantom limb pain, a condition that mayhave potentiated pain or lowered the corticalthreshold for pain. Thus, both lesion and electri-cal-stimulation studies generally support the in-volvement of thalamic VPL and somatosensorycortices in sensory and affective dimensions ofpain, though the deficits from lesions are usuallypartial and often there is recovery of function.That these deficits are partial and temporary at-tests to the existence of multiple representations ofpain and the potential for neuroplastic reorgani-zation of brain circuitry, as will be discussed later.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
339

More selective deficits in emotional dimensionsof pain are observed in patients with large lesionsof the IC (Weinstein et al., 1955; Berthier et al.,1988), anterior cingulate cortex (Foltz and White,1962; White and Sweet, 1966), or prefrontal cortex(Hardy et al., 1952; White and Sweet, 1962QA :3 ). Dam-age to large parts of IC has been found amongpatients with pain asymbolia (Rubins and Fried-man, 1948; Weinstein et al., 1955; Berthier et al.,1988). Patients with this condition do not displaybehavior indicative of threat or intrusion in re-sponse to painful stimuli. They no longer appre-ciate the destructive significance of pain and donot withdraw from pain stimuli or threateninggestures. This is so despite their capacity to detectthe sensory features of nociceptive stimulation.Likewise, focal damage to the posterior parietalcortical area 7b in the monkey results in an ab-sence of escape responses to normally painful tem-peratures (i.e., 51–521C) despite preservation ofthe ability to detect the offset of noxious thermalstimuli (Dong et al., 1996). Infraparietal area 7breceives input from S1 and S2 somatosensory cor-tex and projects to the IC. Therefore, this region ofthe parietal cortex and the IC may be a criticalinterface between sensory-discriminative and theimmediate affective-motivational dimension ofpain. However, electrical stimulation of severalsites within the posterior insula has been shown toevoke unpleasant pains, often with distinct sensoryqualities (Ostrowsky et al., 2002). These observa-tions suggest that the posterior insula may func-tion in to some extent in both sensory and affectivecomponents of pain.
The involvement of the prefrontal cortical lobesin complex aspects of cognitive-evaluative andhence pain-related suffering is supported by de-tailed observations carried out on patients beforeand after prefrontal lobotomy. Hardy et al. (1952)found that prefrontal lobotomy produced no over-all change in heat-induced experimental painthresholds in eight patients tested. Nevertheless,there was some reduction in perceived intensity ofclinical pain in four of five patients studied. How-ever, the most striking changes were in patients’attitudes, emotional reactions, and cognitiveprocessing of pain. The lobotomized patients wereemotionally indifferent to low-intensity pains,
which, though perceived, evoked few affective re-actions. A statement that epitomized this attitudewas ‘‘Yes, I feel the pain but it doesn’t bother me’’.Moderate to high intensity pains sometimesevoked overreactions manifested by a show ofgrimacing, fears, and agitation when direct ques-tions forced them to focus on the pain. However,when patients were left alone, spontaneous suffer-ing and pain-related behaviors were nearly absent.They showed little spontaneous concern about thenegative implications of pain as regards damage tothe body or threat to life. White and Sweet (1966)have corroborated these observations. Evidently,lobotomy somehow interferes with the spontane-ous ongoing cognitive evaluations that are relatedto the long-term implications of having a persist-ent pain condition. It is possible that lobotomyselectively reduces pain-related suffering, a stagethat is partly based on reflective processes relatedto memory of past consequences of having pain aswell as future implications (Fig. 1). The lack ofspontaneous pain-related suffering of patients withprefrontal lobotomy represents a deficit thatdiffers from that which occurs in pain asymbolia(Rubins and Friedman, 1948; Weinstein et al.,1955). Lobotomized patients appear to perceivethe immediate threat of pain once it is brought totheir attention (Hardy et al., 1952), whereas pa-tients with pain asymbolia appear incapable ofperceiving the threatening nature of nociceptivestimuli under any circumstances.
Immediate threat and sense of intrusion arecognitive mediators of what is unpleasant aboutpain and this component of pain affect is sup-ported by insular and anterior cingulate corticalactivity (Fig. 2). These areas, in turn, interact withposterior parietal, temporal, and prefrontal cortex,to integrate inputs from multiple sensory modali-ties related to present context with inputs relatedto past events. These interactions support the in-terface between immediate unpleasantness andpain-related suffering.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
340

Electrophysiological studies of central neurons that
integrate nociceptive with other inputs
Most of the studies described in the preceding sec-tion are based on mainly on observations of hu-man responses to nociceptive stimuli after centrallesions and after electrical stimulation of centralpathways and brain regions. The emphasis ofelectrophysiological studies of pain-related path-ways has been on sensory processing and earlystages of pain. However, beyond the immediateprocessing associated with pain-sensation inten-sity, it seems reasonable that further processing ofpain requires an evaluation of the pain sensation inrelationship to the overall context in which thenociceptive stimulus occurs. This evaluation mayrepresent part of the interface between sensory andaffective dimensions of pain. Thus, one might ex-pect that neurons involved in such a functionwould integrate sensory inputs from multiplesources, that is, they would be multisensory. Forexample, if the perceived degree of threat of a beesting is enhanced by hearing and seeing the sting-ing bee, then such enhancement could occuramong multisensory neurons and could be veri-fied in neurophysiological experiments that usecombinations of visual, auditory, and nociceptivestimuli.
Infraparietal cortex
In direct support of this possibility, some neuronsof the infraparietal cortex in area 7b in the monkeyrespond optimally to nociceptive stimuli yet alsorespond to visual stimuli (Dong et al., 1989, 1994).Dong et al. (1994) found that the responses of 7bneurons to mildly noxious heat stimuli (44–451C)were enhanced by antecedent or concurrent visualstimuli. However, this enhancement only occurredif the target location or direction of motion withinthe visual receptive field was spatially aligned withthe cutaneous receptive field. The enhancementwas much greater for mild nociceptive stimuli(44–451C) than for stronger stimuli (471C). Thus,it would appear that the neural organization ofthis region of the posterior partietal cortex is thatof integrating nociceptive inputs with other sen-
sory inputs in a manner that conveys informationabout the overall degree of threat presented to anorganism (i.e., seeing a bee while feeling its sting).This integration is especially critical at the low endof the nociceptive stimulus range, wherein an or-ganism must make a behaviorally relevant decisionabout the extent of threat presented by an object.This interpretation is based on principles of mul-tisensory integration that have been elaborated ingreat detail by Stein and colleagues (Stein andMeredith, 1993). Although insular cortical neu-rons are often multimodal (Hicks et al., 1988),possibly because they receive multimodal sensoryinput from parietal 7b cortex, they have yet to betested for multisensory integration. Given thetypes of deficits in patients with pain asymboliaand the multimodal integration in parietal area 7b,it is certainly reasonable to hypothesize that itwould occur in the IC.
Anterior cingulate cortex
The physiology of the ACC and its role in pain iseven more complex than that of the posterior pa-rietal and IC. Electrophysiological studies of neu-rons in ACC suggest that they are involved inadvanced stages of pain-related processing (Is-omura et al., 2004 QA :4). Similar to posterior parietaland insular cortices, ACC neurons appear to in-tegrate multiple sensory inputs. They integratesensory input with attention, memory, and alter-native motor responses. Whereas S1 somatosen-sory neurons are involved in processing thediscriminative features of nociceptive stimuli, suchas intensity encoding and detection of differences,neuronal activity in the ACC is more closely as-sociated with escape responses, attention, and re-sponse selection in monkeys (Iwata et al., 1980;Isomura and Takada, 2004; Nakamura et al.,2005). For example, ACC neuronal activity wasfound to be significantly higher when monkeys es-caped from a nociceptive heat stimulus than whenthey detected a small change in nociceptive tem-perature (Iwata et al., 1980). Neurons of the ros-tral anterior cingulate motor area appear to beinvolved in the selection of appropriate motor re-sponses as well as in the planning of movements
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
341

(Isomura and Takada, 2004). In the context of apain condition, all of these functions may be in-terrelated with the immediate affective dimensionof pain. After all, the unpleasantness of pain isassociated with domination of attention and mo-tivation for escape or termination.
Some ACC neurons respond during cues thatsignal impending pain and therefore during antic-ipation of pain, while others respond to anticipa-tion of a reward (Koyama et al., 2001), consistentwith neuroimaging studies showing that the rostralACC is activated during anticipation of pain.Thus, the anterior cingulate cortex may be a partof an attention-evaluation network. It may coor-dinate input from IC with output to the prefrontalcortex. As discussed earlier, the IC may combinenociceptive inputs with those of other sensory mo-dalities to provide an integrated output related to asense of intrusion or threat to the physical body(Dong et al., 1994). The ACC may coordinate in-put from the insula and medial thalamic nucleiwith prefrontal cortical areas and limbic structuressuch as the amygdala to provide an appropriatemotor response or plan of action (Fig. 2). Theconcomitant activation of the ACC and prefrontalcortex may be related to a part of a feedback net-work related to attention, cognitive evaluation,and self-awareness (Cohen, 1993). This possibilityis consistent with the effects of prefrontal damagethat include impairments in planning, behavioralcontrol, affective attachment, and directed/sus-tained attention (White and Sweet, 1966; Cohen,1993; Damasio, 1994).
Are there multiple ways that pain can be processed
or represented in the brain?
As shown in Fig. 2, the dimensions of pain arerelated to multiple ascending pathways and a dis-tributed network of multiple brain regions. Thisnetwork contains both serial and parallel process-ing of visceral and somatosensory information.This neurophysiological model has at least a gen-eral correspondence with the psychological man-ner in which pain is processed (Fig. 1). Forexample, there is psychophysical, neuroanatomi-cal, neurological, and physiological evidence for
both serial and parallel relationships between sen-sory and immediate unpleasantness of pain, as hasbeen discussed so far. Although all regions of thepain matrix are involved in pain affect, some aremore proximal to the affective feelings and ex-pressions of pain. This issue is complicated stillfurther by the possibility that there exist alterna-tive ways that the sensory and affective dimensionsof pain can be represented in the brain. This pos-sibility also is of interest to philosophers whoquestion whether a given type of subjective expe-rience, such as pain, can be realized in multipleways.
Two studies support this possibility. Psycho-physical analysis of pain ratings of a man withtotal corpus callosum section provided an unusualopportunity to assess the contributions of alterna-tive ascending pathways to pain and alternativeneural representations of the dimensions of pain(Stein et al., 1989). As discussed earlier, a majorascending pathway for pain is that of the crossed-spinothalamic tract to VPL and somatosensorycortices S1/S2 (Fig. 2). Normally, the two cerebralhemispheres can share nociceptive information ar-riving at S1/S2 by means of the corpus callosum.When the collosum is sectioned, the experience ofnociceptive stimuli presented ipsilateral to the re-sponding hemisphere can only result from im-pulses from ascending pathways that are not partof the crossed pathway to VPL and S1/S2 cortex,whereas the experience of contralateral nociceptivestimuli would reflect input from all nociceptivepathways. Two contact thermodes were placed onboth feet in some trials or on both hands in others.Nociceptive temperatures of 43–511C could thenbe delivered to either the right or left foot (or rightor left hand) and both the intensities and the stim-ulus locations were randomized. As might be ex-pected, his ratings of stimuli presentedcontralateral to the responding hemisphere werenormal and like those of most participants, that is,they increased monotonically from 43 to 511C. Incontrast, when these same stimuli were presentedispsilateral to the responding hemisphere, he gavemuch lower unpleasantness and intensity ratingsto low to moderate nociceptive temperatures(45–471C). This deficit reflects an absence of thecontribution of the major contralateral pathways
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
342

and S1/S2 to pain sensation and unpleasantness.Recall that similar deficits occur with lateralthalamic lesions (Head and Holmes, 1911; Green-span et al., 1997). Surprisingly, when high-inten-sity nociceptive stimuli (49 to 511 skintemperatures) were presented ipsilateral to the re-sponding cerebral hemisphere, he gave high painsensation and pain unpleasantness ratings, similarto those obtained from contralateral stimuli. Thispattern of responses suggests that at high enoughnociceptive levels, recruitment of pathways otherthan the classical crossed spinothalamic-corticalpathway may make up for the pain sensory deficitthat occurs when one cerebral hemisphere is nolonger able to share nociceptive information withthe other via the corpus callosum. The other im-plication of this pattern of results is that bothsensory and unpleasantness components of paincan be represented in multiple pathways. If that isthe case, then effects of damage to one or the otherpathway may be temporary if remaining pathwaysincrease their responsiveness as a result of func-tional or anatomical reorganization.
This possibility is supported by a study of painand tactile sensitivity in four patients with com-plete unilateral hemispherectomy (Olausson et al.,2001). All four patients were easily able to perceivetactile and painful stimuli on both legs and therewas a deficit in ability to localize pain in two of thepatients. Ratings of pain intensity and unpleas-antness ratings induced by contact heat and rat-ings of brushing were similar for both legs andsimilar to that of normal individuals. fMRI brainimaging of these patients revealed that brushingand painful heat-activated normal pain-related ar-eas, S1, S2, insula, and anterior cingulate cortex,regardless of which leg was stimulated. These re-sults show that ascending pathways and brain re-gions can develop the capacity for processingtactile and nociceptive information arriving as aresult of stimuli presented ipsilateral to the re-sponding cerebral hemisphere.
Modulating pain and neural representations of pain
The widely distributed activations of multiplepathways and brain areas associated with pain
can also be modulated on a moment-by-momentbasis by numerous psychological factors, includ-ing, attention, expectations, anticipations of pain,and emotional states. Each of the locations ofsynaptic interaction shown in Fig. 2 represents apotential point at which processing of pain-relatedinformation can be modified by psychological fac-tors. Presumably, this modification is accompa-nied by changes in different aspects of painexperience. Demonstrations of parallel changes inpain experience and neural processing reflect bothpsychological and neural plasticity. The followingsection discusses these parallel changes in the con-text of how attention, expectations, placebo, andhypnotic suggestions modulate central neural ac-tivity and pain.
Brain-to-spinal-cord modulation of pain
Descending modulation of spinal-cord processingof nociception has been a major topic in pain re-search over the last 35 to 40 years and has a vo-luminous literature (see Basbaum and Fields,1978; Fields and Price, 1997 QA :5for reviews). Detailedexplanations of descending modulation are be-yond the scope of this chapter. Instead, a few ex-amples will be given of studies that characterizethe dynamic nature of brain-to-spinal-cord mod-ulation of pain. Descending modulation of spinal-cord nociceptive processing begins in the forebrainof mammals and includes such structures as theamygdala and rostral anterior cingulate cortex.These areas are also those which receive inputfrom ascending nociceptive pathways. A majortarget of these structures includes the per-iaqueductal grey (PAG) of the midbrain. ThePAG, in turn, projects to the rostroventral medulla(RVM) onto three types of neurons, on-cells, off-cells, and neutral cells. All three types of RVMneurons project to the dorsal horn of the spinalcord, where on-cells amplify and off-cells inhibitnociceptive transmission. Amplification and inhi-bition presumably occur under different psycho-logical circumstances, such as stress, fear,anticipation, and different types of attentional fo-cus. Thus, this descending control system has bi-directional control of pain at the first synapse on
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
343

neurons of origin of ascending spinal pathways.This system also is integrally related to endog-enous opioid mechanisms, as demonstrated by along history of research.
Descending modulatory influences from atten-tion on dorsal-horn sensory projection neuronshave been shown in experiments in awake-trainedmonkeys (Hayes et al., 1981; Hoffman et al.,1981). These studies showed that responses oftrigeminothalamic WDR and NS neurons of themedullary dorsal horn could be modified by differ-ent attentional sets and conditions of stimulus rel-evance (Bushnell et al., 1984). Nociceptivetemperatures (45–491C) applied to the monkeys’face evoked impulse discharges in these neuronsthat were an increasing function of stimulus tem-perature. For a given temperature, a neuron wouldincrease its firing rate and then reach a steadyplateau frequency. At a randomly determined timeduring the plateau, a small temperature increasewas presented. This small increase was accompa-nied by a corresponding increase in impulse fre-quency. WDR neurons were especially sensitiveand could detect small temperature increases of0.2–0.3 1C (e.g., from 46.0 to 46.3 1C). However,these responses to small temperature shifts in-
creased during a task in which the monkey had todetect them in order to receive a reward (a relevantattentional set). They decreased when they per-formed a similarly demanding visual-discrimina-tion task (an irrelevant attentional set). Theseopposing effects predict that attending to smalldifferences in nociceptive temperatures would en-hance pain and attending to small differences inlight intensity during the same nociceptive stimu-lus would decrease pain. A psychophysical studyby Miron et al. (1989) confirmed this prediction.
The impulse frequencies elicited in WDR andNS trigeminothalamic neurons by nociceptive tem-peratures (45–491C) also can be modified by at-tentional factors related to anticipation. Impulsefrequencies of WDR neurons were higher and theirreceptive fields were larger when a warning lightpreceded nociceptive stimuli as opposed to whenthese stimuli occurred unexpectedly. As discussedearlier, receptive-field sizes of WDR neurons aresomewhat large and complex and this complexityis compounded by the fact that they are under
moment-by-moment modulatory control. Thus,the magnitudes of the stimulus–response relation-ships are under dynamic modulatory control andmay play as direct a role in determining pain per-ception as do the peripheral stimulus events them-selves. The dorsal horn is part of a networkinvolved in shaping pain perception, a networkthat includes the first synapse in ascending path-ways for pain. This type of modulation had beenanticipated by existing theories of pain (e.g., thegate control theory), but these studies were the firstto demonstrate this principle in a behavioral con-text.
It is more difficult to determine modulatoryeffects at a spinal level in humans. However, animportant consequence of inhibition (or facilita-tion) at the level of the dorsal horn is that all of thecentral targets of ascending pathways should beinhibited as a consequence of inhibition at theearliest central level. This potential consequence isalso important for reducing the physiologicallydetrimental consequences of pain, such as reducedimmune responses and deleterious autonomic andneuroendocrine responses. If a given type of an-algesic mechanism involves brain-to-spinal cordinhibition, then one should observe reductions inmany pain-related areas of the brain, includingthalamus, S1/S2, insula, and ACC. Thus, if atten-tion modulates human pain in a manner suggestedby studies of dorsal horn neurons in awake mon-keys, inhibition should occur at all of these centralregions.
Effects of attention and distraction at multiple pain-related brain regions
This prediction is supported by imaging studies ofthe effects of attention and distraction in humanson pain-evoked activity in the thalamus and sev-eral cortical regions, such as the primary somato-sensory cortex (S1), anterior cingulate cortex(ACC), and IC (Bushnell et al., 1999; Bantick etal., 2002; Brooks et al., 2002;Hoffman et al., 2004;Seminowicz et al., 2004; Valet et al., 2004). In onestudy, several pain-related brain regions were moreactivated during a pain-attention condition com-pared to a distraction condition (Peyron et al.,
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
344

1999). In a similar study, Bushnell et al. (1999)showed the greatest attentional modulation ofpain-evoked activity in S1 cortex, perhaps becauseparticipant’ attention was directed toward a sen-sory feature of the stimulus. Other regions, in-cluding the periaqueductal gray matter (PAG),ACC, and orbitofrontal cortex, may also be in-volved in the modulatory circuitry related to at-tention, as they have been shown to be activatedduring pain-distraction tasks (Petrovic et al., 2000;Tracey et al., 2002).
Expectation effects at multiple pain-related brainregions
A study by Koyama et al. (2005) similarly dem-onstrates that expected pain levels powerfullyshape pain-related neural activity in multiple brainregions. By combining psychophysical and fMRItechniques, brain activation associated with theintensity of expected pain and experienced actualpain was characterized. Expectation was manipu-lated by providing cues that impending skin-tem-perature stimuli would be higher or lower thanthose actually delivered. When cues were providedthat signaled lower stimulation intensities, bothratings of expected pain and ratings of pain in re-sponse to actual stimuli were significantly reduced.The latter were reduced by 28%, approximatelyequivalent to a clearly analgesic dose of morphine(0.08mg/kg of body weight) (Price et al., 1985).Nearly 85% of the variability of changes in expe-rience of pain could be accounted for by changesin expected magnitudes of pain. Correspondinglarge reductions in neural activity occurred inmultiple pain-related brain areas, including thethalamus, S1/S2 somatosensory cortices, insula,and dorsolateral prefrontal cortex. Consistent withfindings of other studies of mental representation,brain regions involved in processing of expecta-tions overlapped with those involved in theprocessing of afferent sensory information (Kos-slyn et al., 2002). Koyama et al. propose that ex-pectation-related information is integrated withafferent sensory information within the pain ma-trix of the brain to provide a complete cognitiveexperience of pain. However, widespread modula-
tion within this matrix also could be a result ofbrain-to-spinal-cord descending modulation, asdescribed above for attention. It is not clear yetwhether these are two mutually exclusive explana-tions and how either possibility can be ruled out.
Placebo effects at multiple pain-related brainregions
Similar to both brain-imaging studies of effects ofattention and expectation on pain, two studiesfound that placebo manipulations produced re-ductions in pain ratings and widespread decreasesin neural activity of pain-related areas of the brain(Wager et al., 2004; Robinson et al., 2006). In thefirst study, decreases in pain-related brain activitywere only statistically significant after terminationof stimuli and at a later time when individualsrated pain (Wager et al., 2004). This type of effectcould reflect modulation of cognitive processes re-lated to the experience of representing pain andcould be at least partly related to report bias. Asecond brain-imaging study examined whetherplacebo analgesia is accompanied by reductionsin neural activity in pain-related areas of the brainduring the time of stimulation (Robinson et al.,2006). Brain activity of irritable-bowel syndromepatients was measured in response to rectal dis-tension by a balloon barostat. A large placeboeffect produced by placebo suggestion was accom-panied by large reductions in regional cerebralblood flow in thalamus, somatosensory cortices,insula, and anterior cingulate cortex, providingevidence for active afferent inhibition in placeboanalgesia. These results constitute evidence againstthe hypothesis that placebo analgesic effects reflectnothing beyond report bias and provide furtherevidence for widespread inhibition of pain process-ing within the brain. The similarity between effectsof expectation described above and results of pla-cebo manipulation provide further support to thehypothesis that expectation is salient factor in pla-cebo analgesia.
Although it is a major factor in placebo anal-gesia, expectation is unlikely to operate alone. De-sire for pain relief and the positive (or lessnegative) feelings associated with perception of
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
345

the therapeutic intervention have also been pro-posed to contribute to placebo analgesia. Else-where, we have argued that a way of accountingfor psychological mechanisms of placebo analgesiais by means of an emotion model (Price and Barr-ell 1984; Price et al., 1985; Vase et al., 2003). Thismodel proposed that positive and negative emo-tional feelings are often co-determined by strengthof desire and degree of expectation about an out-come, such as pain relief (Price and Barrell 1984;Price et al., 1985). The model accounts for the ob-servations made in some studies that expectationratings account for 44–60% of the variability inpain ratings during the placebo condition (Price,1999), for observations in other studies that desireand expectation ratings account for even more ofthis variance (Vase et al., 2003), and observationsin some studies that changes in emotions accountfor placebo responses (Vase et al., 2003, 2005).Finally, it accounts for observations that changingemotional feelings by means other than placebointerventions can modulate pain (Rainville et al.,2005). Expectations, desires, and emotional feelingstates are all examples of ‘qualia’ (Price, 1999). Inphenomenological terms, there is something it islike to have desires, expectations, and emotionalfeeling states and their existence and magnitudecan only be directly reported by those who expe-rience them (Price and Barrell, 1980, 1984; Price etal., 1985). These first-person mentalistic conceptsof course have potential neural correlates. A sat-isfying explanation of placebo mechanisms wouldinvolve integrating both experiential (first person)and neural (third person) cause–effect relation-ships. This type of integration is currently a highlydiscussed topic among psychologists, neuroscien-tists, and philosophers (Velmans, 1996, 2002QA :6 ).
Can the different dimensions of pain be selectively
modulated?
Some psychological factors and interventions canselectively change the unpleasantness of pain with-out altering the strength of the painful sensation,as was explained in the first section of this chapter(Price et al., 1987; Rainville et al., 1992; Price 1999,2000). When this happens, it would be informative
to know which brain structures are altered underthese conditions. This question also relates theproblem of determining which brain structures aremost proximately related to the different dimen-sions of pain. Attempts to analyze the differentialrepresentations of sensory and affective dimen-sions of pain are provided by two positron emis-sion tomography (PET) studies. In both studies,significant activation occurred in the somatosen-sory area I, anterior cingulate cortex (area 24), andanterior IC both before and during hypnosis. Inthe first study, hypnotic suggestions were given toselectively alter the affective dimension of painwithout changing the perceived intensity of thepainful sensation (Rainville et al., 1997). Recallthat this approach was successfully used in a psy-chophysical study by Rainville et al. (1992). Theexperimental conditions included immersion of theleft hand in moderately painful water (47 1C)without hypnosis, with hypnosis but without sug-gestions, with hypnosis with suggestions for in-
creased unpleasantness, and finally with hypnosiswith suggestions for decreased unpleasantness.These manipulations were successful in providingmuch larger unpleasantness ratings during the high
unpleasantness condition as compared to the low
unpleasantness condition, but no differences inpain-sensation ratings. Consistent with thesechanges, no differences occurred across high andlow unpleasantness conditions in somatosensoryarea I, a region considered to process sensorycomponents of pain. In striking contrast and con-sistent with unpleasantness ratings, activity in an-terior cingulate cortical area 24b was much greaterin the high as compared to the low unpleasantnesscondition. A separate regression analysis, control-ling for factors such as individual differences inglobal cerebral blood flow and pain-sensation in-tensity ratings, showed that pain unpleasantnessratings were significantly associated only with an-terior cingulate activity in a specific region of area24 (R ¼ 0.55, Po0.001). These results indicatethat hypnotic modulation of the affective dimen-sion of pain is at least partly reflected by changesin cortical limbic regional activity (i.e., anteriorcingulate cortical area 24b). As discussed earlier,the anterior cingulate cortex may be a part of anattention–evaluation–affect network that at-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
346

tributes emotional valence and attention to pain. Italso may represent a region that coordinates in-puts from parietal areas involved in perception ofbodily threat with frontal cortical areas involved inplans and response priorities for pain-related be-havior. Thus, the role of the ACC in pain-relatedaffect is likely to be both pivotal and complex.This view contrasts with that which simply at-tributes the function of pain affect to the ACC.The strategy of using psychological manipulationsto selectively alter the immediate unpleasantness ofpain without changing the intensity of painful sen-sation is a potentially powerful one because itcould be used to selectively alter other dimensionsof pain affect, for example the secondary stageassociated with suffering. This strategy also dem-onstrates that hypnotic modification of pain isboth a real psychological and biological event.Mental events change the activity of the brain in adynamic manner.
A second similarly designed study used hypnoticsuggestions that were selectively targeted towardthe sensory intensive dimension of pain (Hofbaueret al., 2001). However, the suggestions were effec-tive in modulating both sensory and affective di-mensions of pain experience, as measured by theparticipants’ ratings of these dimensions. Unlikethe first study, both somatosensory S1 neural ac-tivity as well as pain-sensation ratings were higherin the high as compared to the low sensory inten-sity condition. There was a similar but nonsignifi-cant trend in the anterior cingulate cortex. Themost important result of the second study is that itprovides a confirmation of the role of S-I somato-sensory cortex in the sensory-discriminative di-mension of pain.
What are the relationships between activity in the
pain matrix and pain-related experiences?
Anticipation, expectation, and magnitude judgmentsof pain
The classic view of neural representations of painsuggests that the different dimensions of pain arerepresented in distinctly separate parallel pathwaysand brain centers. The alternative view presented
in this chapter is different from this classic view inseveral ways. First, it proposes that there existsboth serial and parallel processing of sensory andaffective dimensions of pain, both at a psycholog-ical and neurobiological level. If that is the case,then somatosensory processing regions of thebrain are also integral components of affectiveprocessing. This view is consistent with neurolog-ical evidence that the somatosensory cortices areinvolved in emotions. For example, the ability torecognize emotional states of others is reduced af-ter damage to the somatosensory cortices (Dam-asio, 1994; Adolphs et al., 2000). Second, thealternative view presented here takes into accountneuroplastic mechanisms and the likelihood thatthere exist multiple ways that the dimensions ofpain can be represented, such as in split-brain in-dividuals and persons with total absence of onecerebral hemisphere. Finally, our account suggeststhat the pain matrix is involved not only appreci-ation the qualities and intensity of actual pain, assuggested by classical theories, but additionally inseveral other pain-related experiences. These in-clude the anticipation of pain and expectation ofspecific pain intensities (Koyama et al., 2005), asdiscussed in this chapter, and the act of represent-ing pain through rating it on a scale. The latterfunction is elegantly illustrated by a study byMoulton et al. (2005). They found that pain-re-lated areas, such as S1 somatosensory cortex, wereactivated not only when a painful stimulus waspresented, but also a second time when partici-pants rated the pain. Apparently, the act of rep-resenting a pain through a rating requires some ofthe same brain structures that are activated duringpain itself. Since the pain is rated after it is expe-rienced, the somatosensory cortex must somehowrerepresent the pain. This would entail integrationwith memory.
Two types of observations in explaining pain and itsneural representations
Explanations of interrelationships between neuralactivity within the pain matrix and different as-pects of pain and pain-related experiences requiretwo types of observations. One type of observation
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
347

is neurophysiological and consists of such meas-urements as the recording of impulse activities inneurons, global neural activity, and measurementsof lesion size and location. The other type of ob-servation is the reports of participants, who pro-vide accounts and ratings of their experiences ofpain intensity, pain unpleasantness, and otherqualitative aspects of pain. This second type ofobservation also applies to some of the independ-ent variables of studies, such as expected levels ofpain, magnitude of desire for relief, and degree ofattention to one type of stimulus or another (e.g.,light versus sound). The reports of participants areabout their phenomenal experience and are de-scribed in mentalistic terms. The relationships be-tween the two types of observation are oftencorrelational, as in fMRI experiments, but can alsobe causal, as when unpleasant pains are evoked byelectrical stimulation of VPL of the thalamus. Thecombinations of experiential and neurophysiolog-ical observations in experiments where causal andcorrelational relationships are determined offer astrategy whereby we can explain how pain is rep-resented and dynamically modified.
How do we optimally conceptualize mind–brain
relationships in efforts to understand psychological
modulation of pain?
This review of brain mechanisms of pain has em-phasized neuroplasticity in the neural processingassociated with different pain dimensions. As wehave discussed, this plasticity is manifested bymultiple ways that the brain can process pain andby multiple ways that pain can be modulated byattention, emotions, and expectations. As outlinedby Velmans for consciousness itself (Velmans,2000), causal relationships occur between experi-ential dimensions of pain (mind–mind relation-ships), between different areas within the brain(brain–brain relationships), between brain activityand experiential dimensions (brain–mind relation-ships), and finally between experiential dimensionsand brain activity (mind–brain relationships). Ofthese four types of causal relationships, mind–-brain relationships take on particular interestgiven recent theoretical advances in our under-
standing of possible effects of focused attention onnervous system function (Schwartz and Begley,2002; Schwartz et al., 2005). Specifically, the ap-plication of well-established principles of contem-porary physics to neuroscience allows us to betterunderstand how phenomenal experience (e.g., an‘‘image’’ of pain relief) could modify brain re-sponses, and over time systematically changethem.
The reason why principles of contemporaryquantum physics are fully applicable to brainphysiology stems from the fact that ion channels inthe brain are, at their narrowest point, less than1 nm in diameter, or not much more than a singleion wide. Due to this profound limitation in theuncertainty in the position of all the trillions ofions in the brain as they pass through their rele-vant ion channels, the brain itself must be treatedas a quantum physical environment.
One important and well-verified law in quantumphysics called the quantum Zeno effect is a key tounderstanding how focused attention can system-atically alter the brain’s response to environmentalinputs (see Schwartz and Begley, 2002; Schwartz etal., 2005 for discussion). Quantum Zeno effect wasfirst described nearly 30 years ago and has beenextensively studied many times since then. Oneclassic example of it is the fact that rapid repeatedobservation of a molecule will hold the molecule ina stable state. It does this by markedly slowing therate of fluctuation demonstrated in moleculeswhen they are not measured (i.e., observed) in arepetitive fashion. This is a basic principle ofquantum physics — the rate of observation hasmarked measurable effects on the phenomenonbeing observed.
The quantum Zeno effect for neuroscience ap-plication states that the mental act of focusing at-tention can hold in place brain circuits associatedwith what is focused on (e.g., pain versus pain re-lief). Focusing attention on mental experiencemaintains the brain state arising in associationwith that experience. What this means is that if onefocuses attention on an experience, the set of rel-evant brain circuitry with which that experience isassociated will be held in a dynamically stablestate. For example, an expectation of pain reliefcan elicit a focusing of attention on actual expe-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
348

riences of pain relief that are associated with pat-terns of activity in a given brain circuitry (Koyamaet al., 2005). When sufficient attention is focusedon the experience of pain relief, the associatedbrain circuitry becomes dynamically stable. Thisacute effect of focused attention can then enablethe well-validated principle of Hebb (1955),namely that repeated patterns of neural activitycan cause neuroplastic changes and new connect-ivities to form in well-established neural circuits(‘‘cells that fire together wire together’’). This typeof attention-based mechanism of neuroplasticchange has been termed self-directed neuroplastic-ity to emphasize that alterations in CNS functioncan be readily driven by and dynamically modifiedby willfully directed mental events (Schwartz andBegley, 2002; Schwartz et al., 2005). As was statedabove, mental events change the activity of thebrain in a dynamic manner. Basic principles ofcontemporary physics now enable us to place thisempirically well-validated fact within theoreticallycoherent, scientifically grounded, and technicallydescribed context.
The term attention density has recently beencoined to help clarify this mechanism. Attention
density is defined as the number of observationsper unit time, and thus the higher the intensity offocus of attention the higher the attention density.The term is important because it is this increasednumber of observations per unit time, or increasedfocus that brings the quantum Zeno effect intoplay. This increased focus causes the relevant neu-ral circuitry to become stabilized. It is this fact thatallows us to explain how the brain’s response topain can be systematically modified by the qualityof attention that is focused (or not focused) on it.
These principles of self-directed neuroplasticityare fully testable in experimental contexts. Manyof the experimental findings described in thischapter can be more clearly understood in lightof these theoretical advances, and many new em-pirically based investigations of pain-related eventsin the CNS can be organized within this new the-oretical frame. For example, the rapidly growingdata base on the effects of expectation on S1,ACC, and insular cortices can be better under-stood within this physics-based reasoning. Specifi-cally, if participants’ expectation of pain relief
during placebo analgesia causes them to focus at-tention on experiential aspects of pain relief, thenattention density associated with pain relief will beincreased. This can activate the quantum Zenoeffect that will dynamically stabilize the patterns ofneural activity arising in circuitry associated withpain relief. This can then call Hebbian mechanismsinto play, which can lead to neuroplastic changesin the brain’s response to nociceptive stimuli, oreven the mental events associated with those stim-uli. Findings such as those of Price (2000) Rainv-ille et al. (1992, 2005) and Moulton et al. (2005)could be understood and explained to a significantextent by this mechanism. It is our hope that in-vestigators in a variety of related fields will findthis kind of reasoning conducive to the creationand pursuit of a variety of new and clinically usefulexperimental paradigms.
Uncited References
Anderson, (1987); Coghill et al., 1991; Coghill etal., 1994; Chudler et al., 1990; Dubner et al., 1989;Giesler, 1995; Hassler, 1970; Hofbauer et al., 1998;Hylden et al., 1989; Koshikawa and Kitagawa,2005; Lee et al., 1999; Mark et al., 1960; Mayerand Price, 1976; Petrovic et al., 2001; Pons et al.,1987; Robinson and Burton, 1980; Thompson andRobertson, 1987; Williams et al., 2004.
References
Adolphs, R., Damasio, H., Tranel, D., Cooper, G. and Dam-
asio, A.R. (2000) A role for somatosensory cortices in the
visual recognition of emotion as revealed by three-dimen-
sional lesion mapping. J. Neurosci., 20: 2683–2690.
Anderson, R.A. (1987) Inferior parietal lobule function in spa-
tial perception and visuomotor integration. In: Mountcastle,
V.B., Plum, F., Geiger, S.R. (Eds.), Handbook of Physiol-
ogy, Sect. 1, The Nervous System, Vol. 5, Higher Functions
of the Brain, Part 2. Am. Physiol. Society, Bethesda, MD, pp.
483–518.
Bantick, S.J., Wise, R.G., Ploghaus, A., Clare, S., Smith, S.M.
and Tracey, I. (2002) Imaging how attention modulates pain
in humans using functional MRI. Brain, 125: 310–319.
Basbaum, A.I. and Fields, H.L. (1978) Endogenous pain con-
trol mechanisms: review and hypothesis. Ann. Neurol., 4:
451–462.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
349

Bernard, J.F. and Besson, J.M. (1990) The spino(trigemino)po-
ntoamygdaloid pathway: electrophysiological evidence for an
involvement in pain processes. J. Neurophysiol., 63: 473–490.
Bernard, J.F., Peschanski, M. and Besson, J.M. (1989) A pos-
sible spino (trigemino)-ponto–amygdaloid pathway for pain.
Neurosci. Lett., 100: 83–88.
Berthier, M., Starkstein, S. and Leiquarda, R. (1988) As-
ymbolia for pain: a sensory-limbic disconnection syndrome.
Ann. Neurol., 24: 41–49.
Brooks, J.C., Nurmikko, T.J., Bimson, W.E., Singh, K.D. and
Roberts, N. (2002) fMRI of thermal pain: effects of stimulus
laterality and attention. Neuroimage, 15: 293–301.
Burstein, R., Cliffer, K.D. and Giesler, G.J. (1987) Direct so-
matosensory projections from the spinal cord to the hypo-
thalamus and telencephalon. J. Neurosci., 7: 4159–4164.
Bushnell, M.C., Duncan, G.H., Dubner, R. and He, L.F. (1984)
Activity of trigeminothalamic neurons in medullary dorsal
horn of awake monkeys trained in a thermal discrimination
task. J. Neurophysiol., 52: 170–187.
Bushnell, M.C., Duncan, G.H., Hofbauer, R.K., Ha, B., Chen,
J. and Carrier, B. (1999) Pain perception: is there a role for
primary somatosensory cortex? Proc. Natl. Acad. Sci. USA,,
96: 7705–7709.
Casey, K.L. and Morrow, T.J. (1983) Ventral posterior
thalamic neurons differentially responsive to noxious stimu-
lation in the awake monkey. Science, 221: 675–677.
Coghill, R.C., Mayer, D.J. and Price, D.D. (1993) Wide dy-
namic range but not nociceptive-specific neurons encode
multidimensional features of prolonged repetitive heat pain.
J. Neurophysiol., 69: 703–716.
Coghill, R.C., Price, D.D. and Hayes, R. (1991) Spatial distri-
bution of nociceptive processing in the rat spinal cord. J.
Neurophysiol., 65: 133–140.
Coghill, R.C., Talbot, J.D. and Evans, A.C. (1994) Distributed
processing of pain and vibration by the human brain. J. Ne-
urosci., 14: 4095–4108.
Cohen, R.A. (1993) The Neuropsychology of Attention. Ple-
num Press, New York.
Chudler, E.H., Anton, F. and Dubner, R. (1990) Responses of
nociceptive S-1 neurons in monkeys and pain sensation in
humans elicited by noxious thermal stimulation: effect of in-
terstimulus interval. J. Neurophysiol., 63: 559–569.
Chung, J.M., Lee, K.H. and Surmeier, D.J. (1986) Response
characteristics of neurons in the ventral posterior lateral nu-
cleus of the monkey thalamus. J. Neurophysiol., 56: 370–390.
Dado, R.J., Katter, J.T. and Giesler Jr., G.J. (1994) Spin-
othalamic and spinohypothalamic tract neurons in the cer-
vical enlargement in rats. II. Responses to innocuous and
noxious mechanical thermal stimuli. J. Neurophysiol., 71:
981–1002.
Damasio, A. (1994) Descartes Error. Avon Books, New York.
Dong, W.K., Chudler, E.H. and Sugiyama, K. (1994) Somato-
sensory, multisensory, and task-related neurons in cortical
area 7b (PF) of anesthetized monkeys. J. Neurophysiol., 72:
542–564.
Dong, W.K., Roberts, V.J. and Hayashi, T. (1996) Behavioral
outcome of injury in area 7B cortex of monkeys. Pain, 64:
579–587.
Dong, W.K., Salonen, L.D., Kawakami, Y., et al. (1989) No-
ciceptive responses of trigeminal neurons in SII-7b cortex of
awake monkeys. Brain Res., 484: 314–324.
Dubner, R., Bushnell, M.C., Duncan, G.H. (1986) Sensory-
discriminative capacities of nociceptive pathways and their
modulation by behavior, In: Yaksh T.L. (Ed.), Spinal Affer-
ent Processing. Plenum, New York, pp. 331–321.
Dubner, R., Kenshalo Jr., D.R., Maixner, W., Bushnell, M.C.
and Oliveras, J.L. (1989) J. Neurophysiol., 62: 437–449.
Echols, D.H. and Cogclough, J.A. (1947) Abolition of painful
phantom limb by resection of the sensory cortex. JAMA, 134:
1476–1477.
Foltz, E.L. and White, L.E. (1962) Pain ‘‘relief’’ by frontal
cingulumotomy. J. Neurosurg., 19: 89–100.
Friedman, D.P., Murray, E.A. and O’Neill, T. (1986) Cortical
connections of the somatosensory fields of the lateral sulcus
of macaques: evidence for a corticolimbic pathway for touch.
J. Comp. Neurol., 252: 323–347.
Giesler, G.J. (1995) The spino-hypothalamic tract. In: Besson,
J.-M., Guildbaud, G. and Ollat, H. (Eds.), Forebrain Areas
Involved in Pain Processing. Eurotext, Paris, pp. 49–62.
Giesler Jr., G.J., Yezierski, R.P., Gerhart, K.D. and Willis,
W.D. (1981) Spinothalamic tract neurons that project to me-
dial and/or lateral thalamic nuclei: evidence for a physiolog-
ically novel population of spinal cord neurons. J.
Neurophysiol., 46: 1285–1308.
Greenspan, J.D., Joy, S.E. and McGillis, S.L. (1997) A longi-
tudinal study of somesthetic perceptual discorders in an in-
dividual with a unilateral thalamic lesion. Pain, 72: 13–25.
Hardy, J.D., Wolff, H.G. and Goodell, H. (1952) Pain Sensa-
tions and Reactions. Williams and Wilkins, Baltimore, pp.
322–333.
Harkins, S.W., Price, D.D. and Braith, J. (1989) Effects of ex-
traversion and neuroticism on experimental pain, clinical
pain, and illness behavior. Pain, 36: 209–218.
Hassler, R. (1970) Dichotomy of facial pain conduction in the
diencephalon. In: Hassler, R. and Walker, A.E. (Eds.), Trige-
minal Neuralgia. Saunders, Philadelphia, PA, pp. 123–138.
Hayes, R.L., Dubner, R. and Hoffman, D.S. (1981) Neuronal
activity in medullary dorsal horn of awake monkeys trained
in a thermal discrimination task. II. Behavioral modulation
of responses to thermal and mechanical stimuli. J. Ne-
urophysiol., 46: 428–443.
Head, H. and Holmes, G. (1911) Sensory disturbances from
cerebral lesions. Brain, 34: 102–154.
Hebb, D.O. (1955) Drives and the C. N.S. (conceptual nervous
system). Psych. Rev., 62: 243–254.
Hicks, T.P., Benedek, G. and Thurlow, G.A. (1988) Modality
specificity of neuronal responses within the cat’s insula. J.
Neurophysiol., 60: 422–437.
Hofbauer, R.K., Rainville, P., Duncan, G.H. and Bushnell,
M.C. (1998) Cognitive modulation of pain sensation alters
activity in human cerebral cortex. Neurosci. Abstr., 24: 447.5.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
350

Hofbauer, R.K., Rainville, P., Duncan, G.H. and Bushnell,
M.C. (2001) Cognitive modulation of pain sensation alters
activity in human cerebral cortex. J. Neurophysiol., 86:
402–411.
Hoffman, D.S., Dubner, R., Hayes, R.L. and Medlin, T.P.
(1981) Neuronal activity in medullary dorsal horn of awake
monkeys trained in a thermal discrimination task. I. Re-
sponses to innocuous and noxious thermal stimuli. J. Ne-
urophysiol., 46: 409–427.
Hoffman, H.G., Richards, T.L., Coda, B., Bills, A.R., Blough,
D., Richards, A.L. and Sharar, S.R. (2004) Modulation of
thermal pain-related brain activity with virtual reality: evi-
dence from fMRI. Neuroreport, 15: 1245–1248.
Hylden, J.L., Anton, F. and Nahin, R.L. (1989) Spinal lamina I
projection neurons in the rat: collateral innervation of par-
abrachial area and thalamus. Neuroscience, 28: 27–37.
Isomura, Y. and Takada, M. (2004) Neural mechanisms of
versatile functions in primate cingulate cortex. Rev. Neuro-
sci., 15: 279–291.
Iwata, K., Kamo, H., Ogawa, A., Tsuboi, Y., Noma, N.,
Mitsuhashi, Y., Taira, M., Kenshalo Jr., D.R., Giesler, G.J.,
Leonard, R.B. and Willis, W.D. (1980) Responses of neurons
in primate ventroposteriolateral nucleus to noxious stimuli. J.
Neurophysiol., 43: 1594–1614.
Kenshalo Jr., D.R., Chudler, E.H., Anton, F. and Dubner, R.
(1988) SI nociceptive neurons participate in the encoding
process by which monkeys perceive the intensity of noxious
thermal stimulation. Brain Res., 454: 378–382.
Kenshalo Jr., D.R. and Isensee, O. (1983) Responses of SI
cortical neurons to noxious stimuli. J. Neurophysiol., 50:
1479–1496.
Kenshalo, D.R., Thomas, D.A. and Dubner, R. (1989) So-
matosensory cortical lesions change the monkeys’ reaction to
noxious stimulation. J. Dent. Res., 68: 897.
Koshikawa, N. and Kitagawa, J. (2005) Anterior cingulate
cortical neuronal activity during perception of noxious ther-
mal stimuli in monkeys. J. Neurophysiol., 93: 1980–1991.
Kosslyn, S.M., Cacioppo, R.J., Davidson, R.J., Hugdahl, K.,
Lovallo, W.R., Spiegel, D. and Rose, R. (2002) Bridging
psychology and biology. The analysis of individuals in
groups. Am. Psychol., 57: 341–351.
Koyama, T., Kato, K., Tanaka, Y.Z. and Mikami, A. (2001)
Anterior cingulate activity during pain-avoidance and reward
tasks. Neurosci. Res., 39: 421–430.
Koyama, T., McHaffie, J.G., Laurienti, P.J. and Coghill, R.C.
(2005). The subjective experience of pain: where expectations
become reality. Proc. Natl. Acad. Sci.,QA :7
Lackner, J.M., Jaccard, J. and Blanchard, E.B. (2005) Testing
the sequential model of pain processing in irritable bowel
syndrome: a structural equation modeling analysis. Eur. J.
Pain, 9: 207–218.
Lee, J.I., Dougherty, P.M., Antezana, D. and Lenz, F.A. (1999)
Responses of neurons in the region of human thalamic prin-
cipal somatic sensory nucleus to mechanical and thermal
stimuli graded into the painful range. J. Comp. Neurol., 410:
541–555.
Lenz, F.A., Dostrovsky, J.O. and Tasker, R.R. (1988) Single-
unit analysis of the human ventral thalamic nuclear group:
somatosensory responses. J. Neurophysiol., 59: 299–316.
Lenz, F.A., Ohara, S., Gracely, R.H. and Dougherty, P.M.
(2004) Pain encoding in the human forebrain: binary and
analogue exteroceptive channels. J. Neurosci., 24: 6540–6544.
Lenz, F.A., Seike, M., Lin, Y.C., Baker, F.H., Rowland, L.H.
and Gracely, R.H. (1993) Neurons in the area of human
thalamic nucleus ventralis caudalis respond to painful heat
stimuli. J. Neurophysiol., 70: 200–212.
Lewin, W. and Phillips, C.G. (1952) Observations on partial
removal of the postcentral gyrus for pain. J. Neurol. Ne-
urosurg. Psychiatr., 15: 143–147.
Maixner, W., Dubner, R., Kenshalo Jr., D.R. and Oliveras, J.L.
(1989) J. Neurophysiol., 62: 437–449.
Mark, V.H., Ervin, F.R. and Hackett, T.P. (1960) Clinical as-
pects of stereotactic thalamotomy in the human. I. The
treatment of severe pain. Arch. Neurol., 3: 351–367.
Mayer, D.J. and Price, D.D. (1976) Central nervous system
mechanisms of analgesia. Pain, 2: 379–404.
Melzack, R. and Casey, K.L. (1968) Sensory, motivational, and
central control determinants of pain. In: Kenshalo, D.R.
(Ed.), The Skin Senses. C. C. Thomas, Springfield, pp.
423–439.
Miron, D., Duncan, G.H. and Bushnell, M.C. (1989) Effects of
attention on the intensity and unpleasantness of thermal
pain. Pain, 39: 345–352.
Moulton, E.A., Keaser, M.L., Gullapalli, R.P. and Greenspan,
J.D. (2005) Regional intensive and temporal patterns of
functional MRI activation distinguishing noxious and innoc-
uous contact heat. J. Neurophysiol., 93: 2183–2193.
Nakamura, K., Roesch, M.R. and Olson, C.R. (2005) Neuronal
activity in macaque SEF and ACC during performance tasks
involving conflict. J. Neurophysiol., 93: 884–908.
Neal, J.W., Pearson, R.C. and Powell, T.P. (1987) The cor-
tico–cortico connections of area 7b, PF, in the parietal lobe
of the monkey. Brain Res., 419: 341–346.
Neal, J.W., Pearson, R.C. and Powell, T.P. (1990) The ipsilat-
eral cortico–cortico connections of area 7 with the frontal
lobe in the monkey. Brain Res., 509: 31–40.
Olausson, H., Ha, B., Duncan, G.H., Morin, C., Ptito, A.,
Ptito, M., Marchand, S. and Bushnell, M.C. (2001) Cortical
activation by tactile and painful stimuli in hemispherectomi-
zed patients. Brain, 124: 916–927.
Ostrowsky, K., Magnin, M., Ryvlin, Isnard, J., Guenot, M. and
Mauguiere, F. (2002) Representation of pain and somatic
sensation in the human insula: a study of responses to direct
electrical cortical stimulation QA :8. Cerebral Cortex, 12: 376–385.
Penfield, W. and Boldrey, E. (1937) Somatic motor and sensory
representation in the cerebral cortex of man. Brain, 60:
116–126.
Petrovic, P., Kalso, E., Petersson, K.M. and Ingvar, M. (2001)
Placebo and opioid analgesia — imaging a shared neuronal
network. Science, 295(5560): 1737–1740.
Petrovic, P., Petersson, K.M., Ghatan, P.H., Stone-Elander, S.
and Ingvar, M. (2000) Pain-related cerebral activation is al-
tered by a distracting cognitive task. Pain, 85: 19–30.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
351

Peyron, R., Garcia-Larrea, L., Gregoire, M.C., Costes, N.,
Convers, P., Lavenne, F., Mauguire, F., Michel, D. and
Laurent, B. (1999) Haemodynamic brain responses to acute
pain in humans: sensory and attentional networks. Brain,
122: 1765–1780.
Ploner, M., Freund, H.J. and Schnitzler, A. (1999) Pain affect
without pain sensation in a patient with a postcentral lesion.
Pain, 81: 211–214.
Pons, T.P., Garraghty, P.E. and Friedman, D.P. (1987) Phys-
iological evidence for serial processing in somatosensory cor-
tex. Science, 237: 417–420.
Price, D.D. (1999) Psychological Mechanisms of Pain and An-
algesia. I.A.S.P. Press, Seattle.
Price, D.D. (2000) Psychological and neural mechanisms of the
affective dimension of pain. Science, 288: 1769–1772.
Price, D.D. and Barrell, J.J. (1984) Some general laws of human
emotion: interrelationships between intensities of desire, ex-
pectations, and emotional feeling. J. Person., 52: 389–409.
Price, D.D., Barrell, J.E. and Barrell, J.J. (1985) A quantita-
tive—experiential analysis of human emotions. Motiv. Emo-
tion,, 9: 19–38.
Price, D.D. and Barrell, J.J. (1980) An experiential approach
with quantitative methods: a research paradigm. J. Human-
istic Psych., 20: 75–95.
Price, D.D. and Dubner, R. (1977) Neurons that subserve the
sensory discriminative aspects of pain. Pain, 3: 307–388.
Price, D.D., Dubner, R. and Hu, J. (1976) Trigeminothalamic
neurons in nucleus caudalis responsive to tactile, thermal,
and nociceptive stimulation of the monkey’s face. J. Ne-
urophysiol., 39: 936–953.
Price, D.D., Greenspan, J. and Dubner, R. (2003) Neurons in-
volved in exteroreceptive functions of pain. Pain, 106:
215–219.
Price, D.D. and Harkins, S.W. (1992) The affective-motiva-
tional dimension of pain: a two stage model. APS J., 1:
229–239.
Price, D.D., Harkins, S.W. and Baker, C. (1987) Sensory–affec-
tive relationships among different types of clinical and ex-
perimental pain. Pain, 28(3): 291–299.
Price, D.D., Hayes, R.L., Ruda, M.A. and Dubner, R. (1978)
Spatial and temporal transformations of input to spin-
othalamic tract neurons and their relation to somatic sensa-
tion. J. Neurophysiol., 41: 933–947.
Price, D.D., Hayashi, H., Dubner, R. and Ruda, M.A. (1979)
Functional relationships between neurons of laminae I, II,
and III of the primate dorsal horn. J. Neurophysiol., 42:
1590–1608.
Price, D.D. and Verne, G.N. (2002) Does the spinothalamic
tract to VPL and somatosensory cortex have roles in both
pain sensation and pain-related emotions? J. Pain,, 3:
105–108.
Price, D.D., von der Gruen, A., Miller, J., Rafii, A. and Price,
C. (1985) A psychophysical analysis of morphine analgesia.
Pain, 22: 320–330.
Rainville, P., Bao, Q.V. and Chetrien, P. (2005) Pain-related
emotions modulate experimental pain perception and auto-
nomic responses. Pain, 118: 306–318.
Rainville, P., Duncan, G.H., Price, D.D., Carrier, B. and
Bushnell, M.C. (1997) Pain affect encoded in human anterior
cingulate but not somatosensory cortex. Science, 277:
968–971.
Rainville, P., Feine, J.S., Bushnell, M.C. and Duncan, G.H.
(1992) A psychophysical comparison of sensory and affective
responses to four modalities of experimental pain. Somatos-
ens. Motor Res., 9: 265–277.
Riley, J.L., Wade, J.B., Myers, C.D., Sheffield, D., Papas, R.
and Price, D.D. (2002) Ethnic differences in the experience of
chronic pain. Pain, 100: 291–298.
Riley III., J.R., Wade, J.B., Robinson, M.E. and Price, D.D.
(2000) The stages of pain processing across the adult lifespan.
J. Pain, 1: 162–170.
Robinson, C.J. and Burton, H. (1980) Somatic submodality
distribution within the second somatosensory (SII), 7b, re-
troinsular, postauditory, and granular insular cortical areas
of M. fascicularis. J. Comp. Neurol., 192: 93–108.
Robinson, M.E., Craggs, J., Verne G.N., Perlstein, W.R. and
Price, D.D. (2006) Placebo analgesia is accompanied by ac-
tive afferent inhibition. J. Pain, (Suppl.) (in Press) QA :9.
Rubins, J.L. and Friedman, E.D. (1948) Asymbolia for pain.
Neurol. Psychiatr., 60: 554–560.
Schwartz, J.M. and Begley, S. (2002) The Mind and the Brain:
Neuroplasticity and the Power of Mental Force. Harper
Collins, New York.
Schwartz, J.M., Stapp, H.P. and Beauregard, M. (2005) Quan-
tum physics in neuroscience and psychology: a neurophysical
model of mind-brain interaction. Phil. Trans. R. Soc., 360:
1309–1327.
Seminowicz, D.A., Mikulis, D.J. and Davis, K.D. (2004) Cog-
nitive modulation of pain-related brain responses depends on
behavioral strategy. Pain, 112: 48–58.
Stein, B.E. and Meredith, M.A. (1993) The Merging of the
Senses. MIT Press, Cambridge, MA.
Stein, B.E., Price, D.D. and Gazzaniga, M. (1989) Pain per-
ception in a man with total corpus callosum transection.
Pain, 38: 51–55.
Thompson, S. and Robertson, R.T. (1987) Organization of
subcortical pathways for sensory projections to the limbic
cortex I. Subcortical projections to the medial limbic cortex
in the rat. J. Comp. Neurol., 265: 175–188.
Tracey, I., Ploghaus, A., Gati, J.S., Clare, S., Smith, S., Menon,
R.S. and Matthews, P.M. (2002) Imaging attentional mod-
ulation of pain in the periaqueductal gray in humans. J. Ne-
urosci., 22: 2748–2752.
Valet, M., Sprenger, T., Boecker, H., Wiloch, F., Rummeny, E.,
Conrad, B., Erhard, P. and Tolle, T.R. (2004) Distraction
modulates connectivity of the cingulo-frontal cortex and the
midbrain during pain—an fMRI analysis. Pain, 109:
399–408.
Vase, L., Robinson, M.E., Verne, G.N. and Price, D.D. (2003)
The contribution of suggestion, desire, and expectation to
placebo effects in irritable bowel syndrome patients. Pain,
105: 17–25.
Vase, L., Robinson, M.E., Verne, G.N. and Price, D.D. (2005)
Increased placebo analgesia over time in irritable bowel syn-
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
352

drome (IBS) patients is associated with desire and expecta-
tion but not endogenous opioid mechanisms. Pain, 115:
338–347.
Velmans, M. (2000) Understanding Consciousness. Routledge,
London.
Wade, J.B., Dougherty, L.M., Archer, C.R. and Price, D.D.
(1996) Assessing the stages of pain processing: a multivariate
approach. Pain, 68: 157–168.
Wager, T.D., Rilling, J.K., Smith, E.E., Sokolik, A., Casey,
K.L., Davidson, R.J., Kosslyn, S.M., Rose, R.M. and Co-
hen, J.D. (2004) Placebo-induced changes in fMRI in the
anticipation and experience of pain. Science, 303: 1162–1167.
Weinstein, E.A., Kahn, R.L. and Slate, W.H. (1955) With-
drawal, inattention, and pain asymbolia. Arch. Neurol.
Psychiatr., 74: 235–240.
White, J.C. and Sweet, W.H. (1966) Pain and the Neurosur-
geon. Thomas, Springfield, Illinois.
Williams, Z.M., Bush, G., Rauch, S.L., Cosgrove, G.R. and
Eskandar, E.N. (2004) Human anterior cingulate neurons
and the integration of monetary reward with motor re-
sponses. Nat. Neurosci., 7: 1370–1375.
Willis Jr., W.D. (1985) The Pain System. Karger, New York.
Willis, W.D., Zhang, X., Honda, C.N. and Giesler, G.J. (2001)
Projections from the marginal zone and deep dorsal horn to
the ventrobasal nuclei of the primate thalamus. Pain, 92:
267–276.
Willis, W.D., Zhang, X., Honda, C.N. and Giesler, G.J. (2003)
A critical review of the role of the proposed VMpo nucleus in
pain. J. Pain,, 3: 79–94.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
PBR� V157 : 57020
353

AUTHOR QUERY FORM
ELSEVIER
Progress in Brain Research, Volume 157
Queries and / or remarks
JOURNAL TITLE: PBR-V157ARTICLE NO: 57020
Query No Details required Author's response
AQ1 Please provide the telephone and fax number for the corresponding information.
AQ2 The reference (White and Sweet, 1969) has not been provided in the reference list. Please provide the required details for the reference.
AQ3 The reference (White and Sweet, 1962) has not been included in the reference list. Please provide the required details for the reference.
AQ4 The reference (Isomura et al. 2004) has not been included in the reference list. Please provide the required details for the reference.
AQ5 The reference Fields and Price (1997) has not been included in the reference list. Please provide the required details for the reference.
AQ6 The reference Velmans (1996, 2002) has not been included in the reference list. Please provide the required details for the reference.
AQ7 Please provide the volume number and page range in the reference Koyama et al. (2005).
AQ8 Please provide the forename for author Ryvlin in Ostrowsky et al. (2002).
AQ9 Please provide the volume number and page range for reference Robinson et al. (2006).

AUTHOR QUERY FORM
ELSEVIER
Progress in Brain Research, Volume 157
Queries and / or remarks
JOURNAL TITLE: PBR-V157ARTICLE NO: 57020
Query No Details required Author's response
UC ref.
If references appear under section "Uncited References", then cite at relevant places in the text. In case of nonavailability of citation, the corresponding references will be deleted from the reference list. Please ignore this query if there is no 'Uncited Reference' section.