
Vietnam Osteoporosis Workshop, HCMC 2006 Assessment of Skeleton Health Tuan Van Nguyen and Nguyen...
71
Vietnam Osteoporosis Workshop, HCMC 2006 Assessment of Skeleton Health Tuan Van Nguyen and Nguyen Dinh Nguyen Garvan Institute of Medical Research Sydney, Australia
-
date post
19-Dec-2015 -
Category
Documents
-
view
226 -
download
3
Transcript of Vietnam Osteoporosis Workshop, HCMC 2006 Assessment of Skeleton Health Tuan Van Nguyen and Nguyen...

Vietnam Osteoporosis Workshop, HCMC 2006
Assessment of Skeleton Health
Tuan Van Nguyen and Nguyen Dinh Nguyen
Garvan Institute of Medical Research
Sydney, Australia

Vietnam Osteoporosis Workshop, HCMC 2006
Overview
• Background
• Normal bone and bone remodelling
• Bone loss and age
• Definitions
• Measurements of bone strength:
– Bone mass and DXA, QUS
– Bone turnover markers

Vietnam Osteoporosis Workshop, HCMC 2006
Background
• Aging population: fastest growing age group
• Osteoporosis and osteoporotic fracture: age-related disorders
• Osteoporosis and osteoporotic fracture:
– Common
– Cause serious disability and excess mortality
– Major economic burden on healthcare system

Vietnam Osteoporosis Workshop, HCMC 2006
Residual lifetime risk of different diseases
Residual lifetime risk (%)0 10 20 30 40 50 60
Any fracture*
Hip fracture*
Vertebral fracture*
Cancer (all sites)**
Diabetes Mellitus+
Breast cancer**
Coronary heart +
Lung/bronchus**
(*, from age 60y; **, from birth, + from age 50)
3/5
~ 1/4
1/6
2/5
1/3
1/8
1/4
1/16
WomenMen
Residual lifetime risk (%)0 10 20 30 40 50 60
Any fracture*
Hip fracture*
Vertebral fracture*
Cancer (all sites)**
Diabetes Mellitus+
Prostate cancer**
Coronary heart +
Lung/bronchus**
(*, from age 60y; **, from birth, + from age 50)
1/3
1/14
1/8
3/7
1/2
1/8
1/3
1/16
(Source: Nguyen ND et al, 2006, under review process)

Vietnam Osteoporosis Workshop, HCMC 2006
Survival probability and fracture
Age (y)
Women Men
Cum
ulat
ive
surv
ival
rat
e
(Soure: Center J, Nguyen TV et al., Lancet 1999;353:878-82)

Vietnam Osteoporosis Workshop, HCMC 2006
Burden of Osteoporotic fractures
• Annual cost of all osteoporotic fractures: $20 billion in USA and ~$30 billion on EU1.
• Worldwide direct and indirect cost of hip fracture: US$131.5 billion2.
(Sources: 1Cummings et al., Lancet 2002;359:1761-67; 2Johnell O, Am J Med 1997;103:20S-26)

Vietnam Osteoporosis Workshop, HCMC 2006
Cortical and Trabecular Bone
• 80% of all the bone in the body
• 20% of bone turnover
• 20% of all bone in the body
• 80% of bone turnover
Cortical Bone
Trabecular Bone

Vietnam Osteoporosis Workshop, HCMC 2006
Cortical (Compact) Bone
• 80% of the skeletal mass
• Provides a protective outer shell around every bone in the body
• Slower turnover
• Provides strength and resists bending or torsion

Vietnam Osteoporosis Workshop, HCMC 2006
Trabecular (Cancellous) Bone•20% of the skeletal mass, but 80% of the bone surface .
• less dense, more elastic, and higher turnover rate than cortical bone.
• appears spongy
• found in the epipheseal and metaphysal regions of long bones and throughout the interior of short bones.
• constitutes most of the bone tissue of the axial skeleton (skull, ribs and spine).
• interior scaffolding maintains bone shape despite compressive forces.
Vietnam Osteoporosis Workshop, HCMC 2006
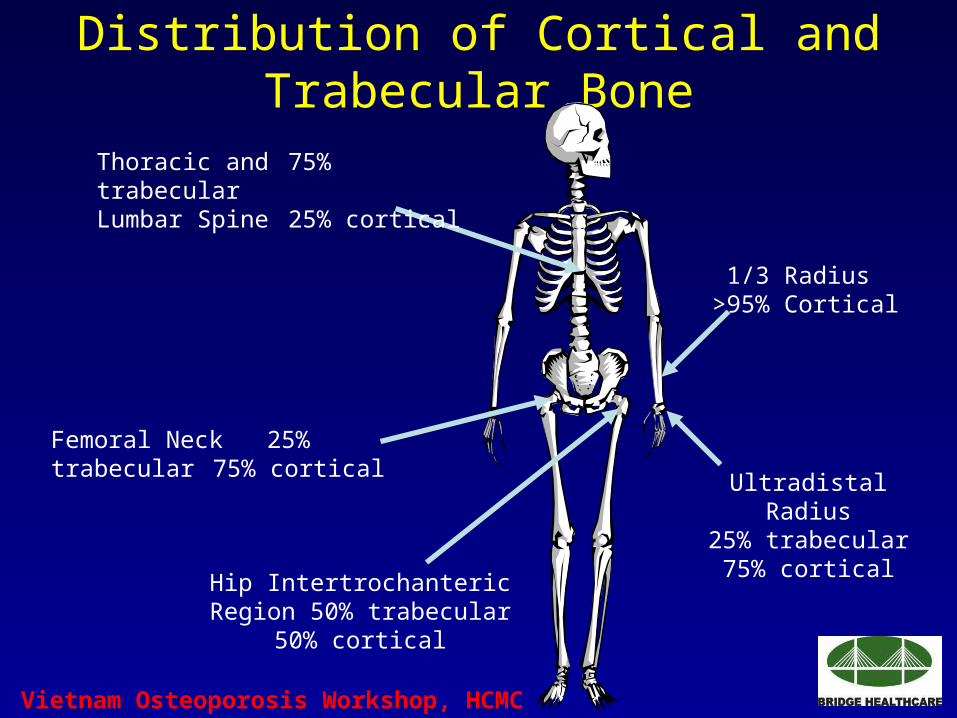
Distribution of Cortical and Trabecular Bone
Thoracic and 75% trabecularLumbar Spine 25% cortical
Femoral Neck 25% trabecular75% cortical
Hip Intertrochanteric Region 50% trabecular
50% cortical
1/3 Radius >95% Cortical
Ultradistal Radius25% trabecular
75% cortical

Vietnam Osteoporosis Workshop, HCMC 2006
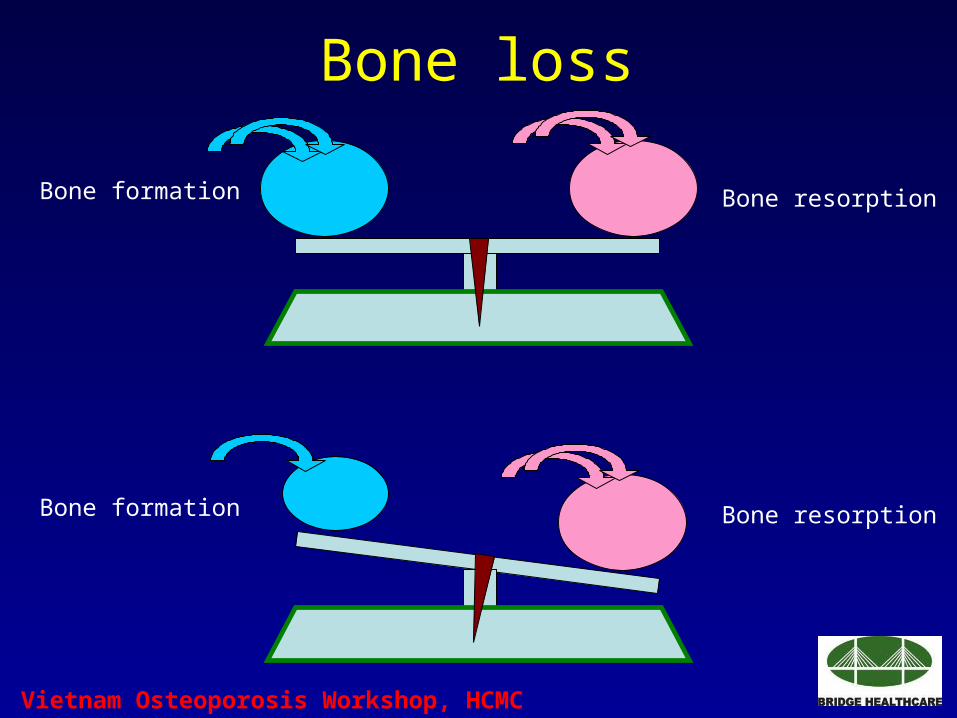
How does bone loss happen?
Bone is a living, growing, tissue
• Healthy bones are not quiescent. They are constantly being remodeled.
• This is not simply a problem of bony destruction, but imbalance between the formation and destruction of bone.

Vietnam Osteoporosis Workshop, HCMC 2006
Bone remodeling cycleBone remodeling cycle
Endosteal sinus
Monocyte
Pre-osteoclast
Osteocyte
Osteoclast
Macrophage
Pre-osteoblast
Osteoblast Bone-lining cell
Osteoid
New bone
Old bone

Vietnam Osteoporosis Workshop, HCMC 2006
OsteoclastsMonocytes
Pre-osteoblasts
Osteoblasts
Osteocytes
Bone remodeling cycleBone remodeling cycle
Vietnam Osteoporosis Workshop, HCMC 2006
Bone loss
Bone formation Bone resorption
Bone formation Bone resorption

Vietnam Osteoporosis Workshop, HCMC 2006
Bone Remodelling:Normal and Osteoporosis

Vietnam Osteoporosis Workshop, HCMC 2006

Vietnam Osteoporosis Workshop, HCMC 2006
Vietnam Osteoporosis Workshop, HCMC 2006

Vietnam Osteoporosis Workshop, HCMC 2006

Vietnam Osteoporosis Workshop, HCMC 2006
Vietnam Osteoporosis Workshop, HCMC 2006
Vietnam Osteoporosis Workshop, HCMC 2006
Vietnam Osteoporosis Workshop, HCMC 2006
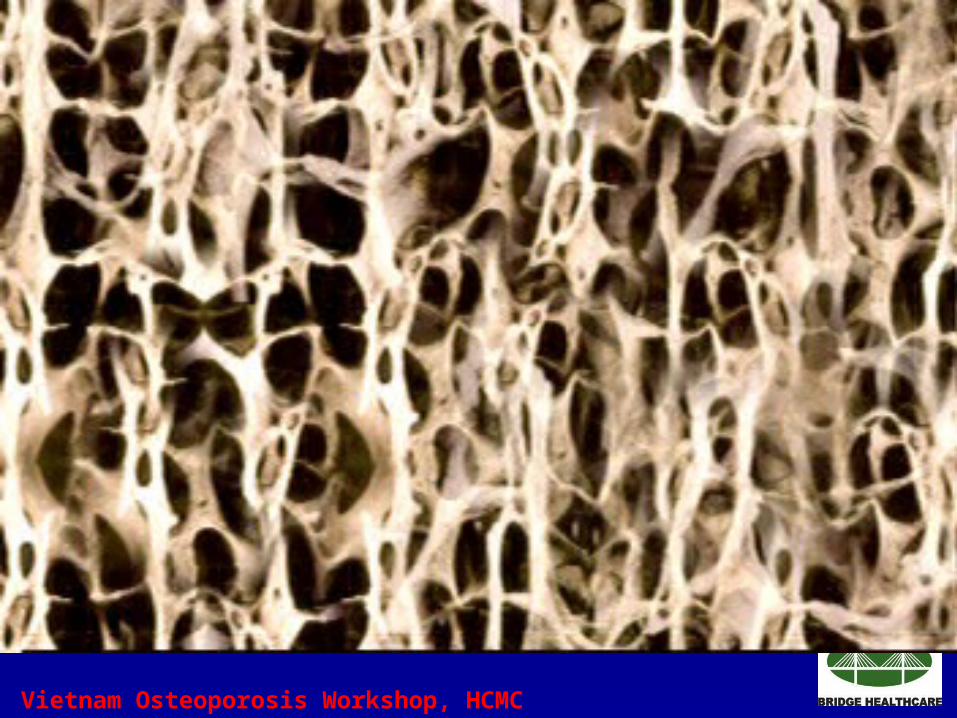
Bone mass declines with age
• Remodeling occurs at discrete foci called bone remodeling units (BRUs).
• Number of active BRUs with age bone turnover.
• Osteoblasts not able to completely fill cavities created by osteoclasts and less mineralized bone is formed.
• Endosteal bone loss partially compensated by periosteal bone formation trabecular thinning.

Vietnam Osteoporosis Workshop, HCMC 2006
Relative Influence of Inner and Outer Diameters on Bone Strength
(Adapted from Lee CA, and Einhorn TA. Osteoporosis 2nd Ed. 2001)

Vietnam Osteoporosis Workshop, HCMC 2006
5 15 25 35 45 55 65 75 85
Gain and loss of Bone throughout the lifespan
Age (Years)
Pubertal Growth Spurt Menopause
BMD
Resorption
Formation

Vietnam Osteoporosis Workshop, HCMC 2006 (VN 2006, unpublished data)
Relationship between BMD and Age

Vietnam Osteoporosis Workshop, HCMC 2006
A systematic skeleton disease characterized by:
- low bone mass
- microarchitectural deterioration of bone tissue
- consequent increase in bone fragility and susceptibility to fracture
Definition of OsteoporosisDefinition of Osteoporosis(WHO)(WHO)
Consensus Development Conference: Diagnosis, Prophylaxis, and Treatment of Osteoporosis, Am J Med 1993;94:646-650. WHO Study Group 1994.

Vietnam Osteoporosis Workshop, HCMC 2006
OsteoporosisOsteoporosis
Normal Osteopenia Osteoporosis

Vietnam Osteoporosis Workshop, HCMC 2006
OsteoporosisNormal bone

Vietnam Osteoporosis Workshop, HCMC 2006
Osteoporosis is defined as a skeletal disorder characterized by:
-compromised bone strength predisposing a person to an increased risk of fracture.
-bone strength primarily reflects the integration of bone density and bone quality.
(Source: NIH Consensus Development Panel on Osteoporosis JAMA 285:785-95; 2001)
Definition of OsteoporosisDefinition of Osteoporosis(NIH)(NIH)

Vietnam Osteoporosis Workshop, HCMC 2006
Gram of mineral per area
Bone architecture
Bone size &
geometry
Bone turnover
BONE QUALITYBONE MINERALDENSITY
BONE STRENGTH
Vietnam Osteoporosis Workshop, HCMC 2006
Bone Quality
( NIH Consensus Development Panel on Osteoporosis. JAMA 285:785-95; 2001)
• Architecture• Turnover Rate• Damage Accumulation• Degree of Mineralization• Properties of the collagen/mineral matrix

Vietnam Osteoporosis Workshop, HCMC 2006
Bone mass, Bone mineral density (BMD)
• Bone mass = the amount of bone tissue as the total of protein and mineral or the amount of mineral in the whole skeleton or in a particular segment of bone. (unmeasurable)
• BMD = the average concentration of mineral per unit area assessed in 2 dimensions (measurable)

Vietnam Osteoporosis Workshop, HCMC 2006
Effect of Size on Areal BMD
1
11
2
22
3
3
3
BMC
1 1 1
AREA BMD
8 4 2
27 9 3
“TRUE” VALUE = 1 g/cm3
(Adapted from Carter DR, et al. J Bone Miner Res 1992)

Vietnam Osteoporosis Workshop, HCMC 2006
Bone Densitometry
• Non-invasive test for measurement of BMD
• Major technologies
– Dual-energy X-ray Absorptiometry (DXA)
– Quantitative Ultrasound (QUS)
– Quantitative Computerized Tomography (QCT)
• Many manufacturers
• Numerous devices
• Different skeletal sites

Vietnam Osteoporosis Workshop, HCMC 2006
DXA (or DEXA)

Vietnam Osteoporosis Workshop, HCMC 2006
DXA (or DEXA)
• Gold-standard” for BMD measurement
• Measures “central” or “axial” skeletal sites: spine and hip
• May measure other sites: total body and forearm
• Extensive epidemiologic data
• Correlation with bone strength in-vitro
• Validated in many clinical trials

Vietnam Osteoporosis Workshop, HCMC 2006
DXA Technology
X-ray Source (produces 2 photon energies with different attenuation profiles)
Photons Collimator (pinhole for pencil beam, slit for fan beam)
Patient
Detector (detects 2 tissue types - bone and soft tissue)
Very low radiation to patient.
Very little scatter radiation to technologist
Vietnam Osteoporosis Workshop, HCMC 2006
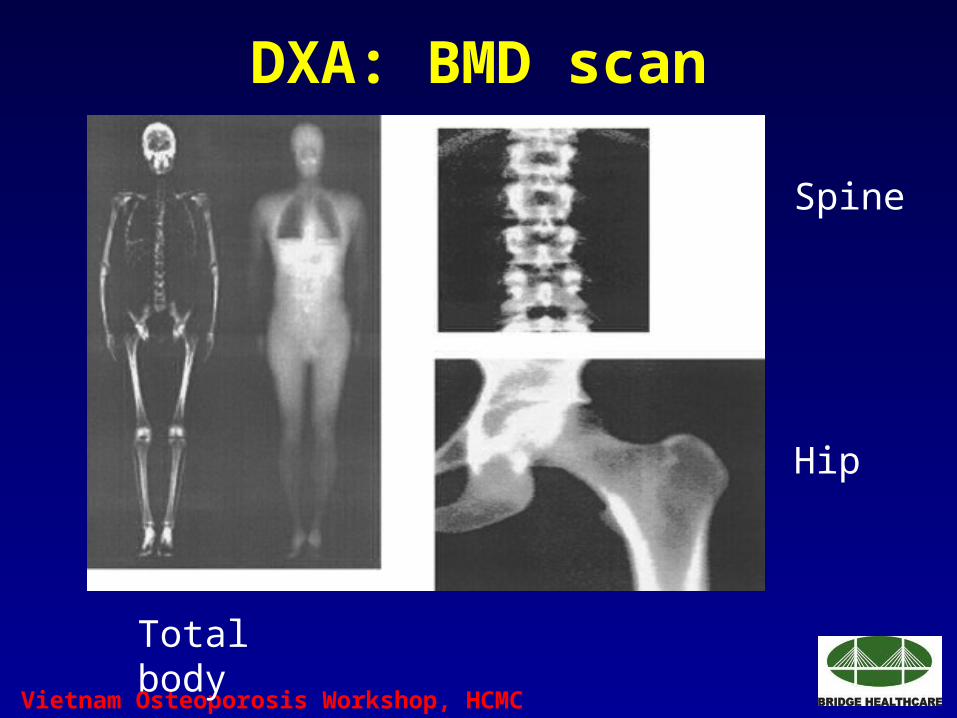
DXA: BMD scan
Total body
Spine
Hip

Vietnam Osteoporosis Workshop, HCMC 2006
DXA: Femoral neck BMD

Vietnam Osteoporosis Workshop, HCMC 2006
DXA: Lumbar spine BMD

Vietnam Osteoporosis Workshop, HCMC 2006
DXA: Hip BMD: Results

Vietnam Osteoporosis Workshop, HCMC 2006
Which Skeletal Sites Should Be Measured?
Every Patient
• Spine
– L1-L4 (L2-L4)
• Hip
– Total Proximal Femur
– Femoral Neck
– Trochanter
Some Patients
• Forearm (33% Radius)
– If hip or spine cannot be measured
– Hyperparathyroidism
– Very obese

Vietnam Osteoporosis Workshop, HCMC 2006
BMD measurement: subject to variability
• In vivo/in situ BMD inaccuracy: effect of bone structure, bone size and shape, and extra-osseous soft tissue
• Measurement error: within subject and between-subject variations.
• Between machine variation.

Vietnam Osteoporosis Workshop, HCMC 2006
In vivo/In situ BMD inaccuracy
X-RAY PATHS
Extra-Osseous Fat+Lean tissue Cortical region
Trabeculaae + Marrow
Bone regionLateral region Lateral region
REGION OF INTEREST
(Adapted from Bolotin HH, Med Phys 2004;31:774-88)

Vietnam Osteoporosis Workshop, HCMC 2006
In vivo/In situ BMD inaccuracy
Under-/or over-estimate BMD (%)
Normal Osteopenia Osteoporosis
Typical lumbar vertebral bone site
~25 ~35 Up to 50
Distal radius, femur ~20 ~25 ~35
Trabecular-free sites (mid-shaft femur, mid-shaft radius…)
<2
(Source: Bolotin HH, Med Phys 2004;31:774-88)
IndividualType of bone

Vietnam Osteoporosis Workshop, HCMC 2006
Source of variability in BMD measurements
(Source: Nguyen TV et al., JBMR 1997;12:124-34)
Number of measurements per subject required to increase the reliability of measurement for a given coefficient of reliability
Vietnam Osteoporosis Workshop, HCMC 2006
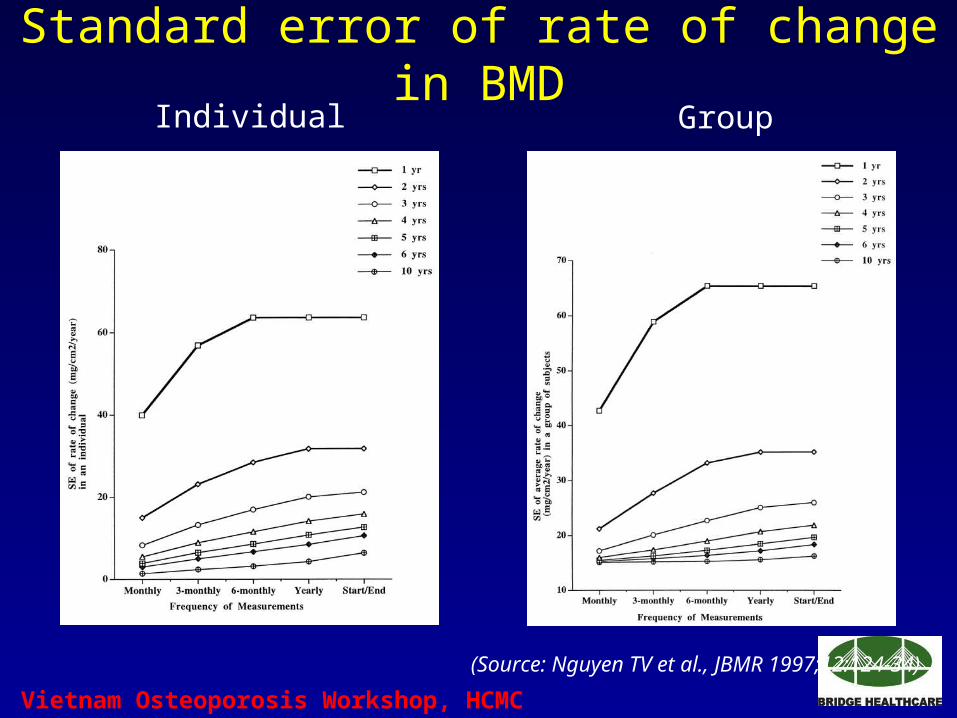
Standard error of rate of change in BMDIndividual Group
(Source: Nguyen TV et al., JBMR 1997;12:124-34)

Vietnam Osteoporosis Workshop, HCMC 2006
• Group level: Intra-subject estimation error could contribute about 90% of the variability component power of study, and underestimate the RR (BMD-fracture).
• Individual level: false +ve & false –ve error rates of diagnostic BMD.
measurement error by multiple measurement.
long-term intra-subject variation by: the length of follow-up and/or the frequency of measurements.
• Studies with 3-5 yrs of follow-up: optimal “cost benefits”.
• More than 2 measurements/year: not improve the precision appreciably.
Source of variability in BMD measurements
(Source: Nguyen TV et al., JBMR 1997;12:124-34)

Vietnam Osteoporosis Workshop, HCMC 2006
“True” level and “True” biological change of BMD
• Factors affect to BMD level and BMD change:
– Invivo/in situ BMD inaccuracy
– Random error
– Measurement errors: intra- and between-subject variability
– Systematic errors
– Effect of regression-toward-the mean(Sources: Bolotin HH, Med Phys 2004;31:774-88; Nguyen TV et al., JBMR 1997;12:124-34; Nguyen TV et al, JCD 2000;3:107-19)

Vietnam Osteoporosis Workshop, HCMC 2006
“True” level and “True” biological change of BMD
• BMD level:
– Good agreement between observed and true values
– Individual with low BMD: 20% false +ve and false –ve of diagnosis of osteoporosis.
• BMD change:
– Overall average increase in BMD of 2%: no conclusion of significant change for an individual.
– An observed of at least 5.5% or of at least 7.5%: could be a significantly biological change.
(Source: Nguyen TV et al, JCD 2000;3:107-19)

Vietnam Osteoporosis Workshop, HCMC 2006
“True” level and “True” biological change of BMD
1st measure 2nd measure change
0.70 0.735 ↑ 5.0% Inconclusive
0.70 0.753 ↑ 7.5% Possibly biological change
0.73 0.700 ↓ 4% Inconclusive
0.73 0.690 ↓ 5.5% Possibly biological change

Vietnam Osteoporosis Workshop, HCMC 2006
BMD Values From Different Manufacturers Are Not Comparable
• Different dual energy methods
• Different calibration
• Different detectors
• Different edge detection software
• Different regions of interest

Vietnam Osteoporosis Workshop, HCMC 2006
Peripheral BMD TestingAccurate & Precise
• What it can do
– Predict fracture risk
– Tool for osteoporosis education
• What it cannot do
– Diagnose osteoporosis
– Monitor therapy
1. A “normal” peripheral test does not necessarily mean that the patient does not have osteoporosis.
2. WHO criteria do not apply to peripheral BMD testing.

Vietnam Osteoporosis Workshop, HCMC 2006
• Broad-band ultrasound attenuation or ultrasound velocity
• No radiation exposure
• Cannot be used for diagnosis
• Preferred use in assessment of fracture risk
Quantitative Ultrasound (QUS)
Vietnam Osteoporosis Workshop, HCMC 2006
Bone Quality
( NIH Consensus Development Panel on Osteoporosis. JAMA 285:785-95; 2001)
Architecture
Turnover Rate
Damage Accumulation
Degree of Mineralization
Properties of the collagen/mineral matrix

Vietnam Osteoporosis Workshop, HCMC 2006
Cortical and Trabecular Bone
• 80% of all the bone in the body
• 20% of bone turnover
• 20% of all bone in the body
• 80% of bone turnover
Cortical Bone
Trabecular Bone

Vietnam Osteoporosis Workshop, HCMC 2006
Relevance of Architecture
Normal Loss of Loss of QuantityQuantity and Quantity and Architecture Architecture

Vietnam Osteoporosis Workshop, HCMC 2006
Bone ArchitectureTrabecular Perforation
The effects of bone turnover on the structural role of trabeculae
Risk of Trabecular Perforation increases with:
• Increased bone turnover• Increased erosion depth• Predisposition to trabecular thinning
Vietnam Osteoporosis Workshop, HCMC 2006
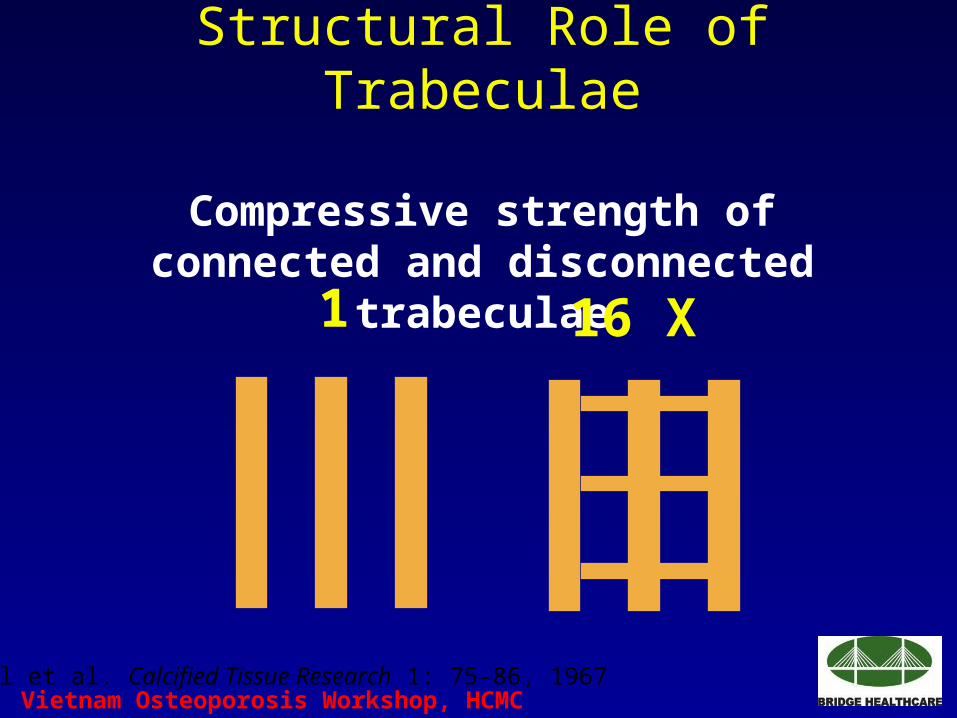
Structural Role of Trabeculae
Compressive strength of connected and disconnected trabeculae
16 X1
Bell et al. Calcified Tissue Research 1: 75-86, 1967

Vietnam Osteoporosis Workshop, HCMC 2006
Resorption Cavities as Mechanical Stress Risers
(Adapted from Parfitt A.M. et al. Am J Med 91, Suppl 5B: 5B-34S)
Normal Osteoporotic

Vietnam Osteoporosis Workshop, HCMC 2006
Hip strength indice• CSMI (cm4): Cross-sectional moment of inertia
• CSA (cm2): Cross sectional area
• Z (cm3): Section modulus= CSMI/distance from the centre of the mass to the superior neck margin.
• Cstress (N/mm2): Compressive stress on the superior surface of the FN during a fall on the greater trochanter. Calculated by combining CSMI and CSA.
• FND (cm): Femoral neck Diameter
• Buckling ratio= radius/thickness

Vietnam Osteoporosis Workshop, HCMC 2006
Cross-Sectional Moment of Inertia CSMI = /4 (r4 outer – r4 inner)
Area (cm2) 2.77 2.77 2.77
CSMI (cm4) 0.61 1.06 1.54
Bending Strength 100% 149% 193%

Vietnam Osteoporosis Workshop, HCMC 2006
Bone strengh indice: summary
• Not well-studied
• Derived from BMC, BMD, and several assumptions
• Used in research field.
Vietnam Osteoporosis Workshop, HCMC 2006
Bone Turnover Markers
• Components of bone matrix or enzymes that are released from cells or matrix during the process of bone remodeling (resorption and formation).
• Reflect but do not regulate bone remodeling dynamics.

Vietnam Osteoporosis Workshop, HCMC 2006
Urinary Markers of Bone Resorption
Marker Abbreviation
Hydroxyproline HYP
Pyridinoline PYD
Deoxypyridinoline DPD
N-terminal cross-linking telopeptide of type I collagen NTX
C-terminal cross-linking telopeptide of type I collagen CTX
(Source: Delmas PD. J Bone Miner Res 16:2370; 2001)

Vietnam Osteoporosis Workshop, HCMC 2006
Serum Markers of Bone Turnover
Marker Abbreviation
Formation Bone alkaline phosphatase ALP (BSAP)Osteocalcin OCProcollagen type I C-propeptide PICPProcollagen type I N-propeptide PINP
ResorptionN-terminal cross-linking telopeptide of type I collagen NTXC-terminal cross-linking telopeptide of type I collagen CTXTartrate-resistant acid phosphatase TRAP
(Source: Delmas PD. J Bone Miner Res 16:2370, 2001)

Vietnam Osteoporosis Workshop, HCMC 2006
• Very low turnover excessive mineralization and the accumulation of microdamage
• Very high turnover accumulation of perforations and a negative bone balance
Bone Turnover Effects Bone Quality

Vietnam Osteoporosis Workshop, HCMC 2006
Summary
• Osteoporosis and osteoporotic fractures are common among aging population
• “Gold standard” of assessment skeleton health is BMD via DXA machine.
• BMD measurement is subject to bias and errors.
• Additional measure of bone health: QUS (BMD), bone strength indice and bone turnover markers.

Vietnam Osteoporosis Workshop, HCMC 2006
Lời Cảm tạ• Chúng tôi xin chân thành cám
ơn Công ty Dược phẩm Bridge Healthcare, Australia là nhà tài trợ cho hội thảo.

Vietnam Osteoporosis Workshop, HCMC 2006
Thank you!


















