VectivBio R&D Day
73
September 21, 2021 VectivBio R&D Day CONFIDENTIAL
Transcript of VectivBio R&D Day

September 21, 2021
VectivBio R&D Day
CONFIDENTIAL

R&D Day
This presentation contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995 that reflect the current beliefs, expectations and assumptions of VectivBio Holding
AG (the “Company,” “we” or “our”) regarding the future of its business, its future plans and strategies, clinical results, future financial condition and other future conditions. All statements other than statements of
historical facts contained in this presentation, including statements regarding future results of operations and financial position, business strategy, product candidates, planned preclinical studies and clinical trials,
results of clinical trials, research and development costs, regulatory approvals, timing and likelihood of success, as well as plans and objectives of management for future operations, are forward-looking statements.
The words “may,” “will,” “expect,” “anticipate,” “aim,” “estimate,” “intend,” “plan,” “believe,” “is/are likely to,” “potential,” or “continue” or the negative of these terms or other similar expressions are intended to identify
forward-looking statements, although not all forward-looking statements contain these identifying words. These forward-looking statements are subject to a number of risks, uncertainties and assumptions, including,
among other things: the ability of our clinical trials to demonstrate acceptable safety and efficacy of our product candidate; the timing, progress and results of clinical trials for our product candidate, including
statements regarding the timing of initiation and completion of studies or trials and related preparatory work, the period during which the results of the trials will become available, and our research and development
programs; the timing, scope and likelihood of regulatory filings and approvals; our ability to obtain marketing approvals of our product candidate and to meet existing or future regulatory standards or comply with
post-approval requirements; our expectations regarding our ability to fund our operating expenses and capital expenditure requirements with our cash and cash equivalents and net proceeds of this offering; future
milestone or royalty payments to our licensing partners or other third-parties, and the expected timing of such payments; our expectations regarding the potential market size and the size of the patient populations for
our product candidate, if approved for commercial use; our expectations regarding the potential advantages of our product candidate over existing therapies for SBS-IF and our expectations regarding potential uses
of our product candidate to treat other indications; the success of development and commercialization of the CoMET platform; our ability to develop new product candidates using the CoMET platform; developments
and projections relating to our competitors and our industry, including competing therapies; the impact of COVID-19 on our business, operations and prospects and on our clinical trials; our potential to enter into new
collaborations; our expectations with regard to our ability to develop additional product candidates or leverage our current product candidate for other indications, and our ability to identify additional products, product
candidates or technologies with significant commercial potential that are consistent with our commercial objectives; our ability to develop, acquire and advance additional product candidates into, and successfully
complete, clinical trials; the commercialization and market acceptance of our product candidate; our marketing and manufacturing capabilities or those of third parties with which we contract; our ability to operate our
businesses without infringing the intellectual property rights and proprietary technology of third parties; the scope of protection we are able to establish and maintain for intellectual property rights covering our product
candidates; estimates of our expenses, future revenue, capital requirements, our needs for additional financing and our ability to obtain additional capital; regulatory development in the United States, Europe and
other jurisdictions; and other risks described in the “Risk Factors” section of our Registration Statement on Form F-1 declared effective by the Securities and Exchange Commission (SEC) on April 8, 2021 and our
other subsequent filings with the SEC.
The forward-looking statements in this presentation represent our views as of the date of this presentation. Although we believe the expectations reflected in such forward-looking statements are reasonable, we can
give no assurance that such expectations will prove to be correct. Accordingly, readers are cautioned not to place undue reliance on these forward-looking statements. Except as required by applicable law, we do
not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. No representations or
warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. New risk factors and uncertainties may emerge from time to time, and it is not possible to predict all risk
factors and uncertainties.
We file Current Reports on Form 6-K, Annual Reports on Form 20-F, and other documents with the SEC. You should read these documents for more complete information about us. You may obtain these documents
for free by visiting EDGAR on the SEC website at www.sec.gov.
This presentation concerns products that are under clinical investigation and which have not yet been approved for marketing by the relevant regulatory authorities. They are currently limited by federal law to
investigational use, and no representation is made as to their safety or effectiveness for the purposes for which they are being investigated.
Disclaimer and Forward-Looking Statements
2

Luca Santarelli, M.D.CEO & Founder
Introduction

R&D Day
Building a Fully Integrated Global Rare Disease CompanyApraglutide in SBS-IF: an underserved market demanding better products with >$2B potential
*Gattex® (teduglutide), known as Revestive® outside the U.S.
SBS-IF: Short Bowel Syndrome Intestinal Failure; SOC: Standard of Care; MOA: Mechanism of Action
• Designed to address previously
intractable Inherited Metabolic
Diseases and prevent clinical
progression of IMDs
• Modular chemistry designed to
restore fundamental cellular
metabolism
• 4 programs in research, plans to enter the clinic in 18 months
• Apraglutide, a differentiated drug candidate for Short Bowel Syndrome
• >$2B market potential, severely underserved
• Gattex®*, only approved product with several shortcomings and limited penetration
• Apraglutide offers a next generation profile and the potential to establish a new SOC
• MOA and approval path are validated
• Multiple life-cycle opportunities
• Successful rare disease track record in R&D, Commercial and Business Development
• Expertise across multiple disease areas and modalities
• Strong focus on execution and discipline in asset selection
Transformative CoMET platform
SuccessfulTeam
Compelling Ph3 Asset
4

R&D Day
Raised $154M* in Nasdaq IPO (VECT) on April 9, 2021
Cash and Cash Equivalents as of June 30, 2021: $144.6M**
Accomplishments in 2021
Apraglutide: • Ph3 programs started in SBS –
• STARS trial initiated in January
• STARS Extend trial initiated in July
• STARS Nutrition trial initiated in June
• ODD status obtained in GVHD - Ph2 trial in preparation
Pipeline expansion:• CoMET platform acquired – 4 programs added to the pipeline
5
VectivBio: 2021 accomplishments to date
* Includes $146.6M in gross proceeds from Initial Public Offering and $7.5M pursuant to a simple agreement for future equity (SAFE) with an existing shareholder; net proceeds after underwriting discount, commissions and fees of $140.5M
** Unaudited; Cash balance on December 31st, 2020: $40.2M
R&D Day
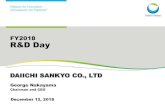
Our Pipeline
1. Our planned pediatric SBS-IF and acute graft versus host disease clinical trials rely on clinical trial data from our completed healthy volunteer Phase 1 and adult SBS-IF patient Phase 2 clinical trials.
To date, we have not completed any dedicated clinical trials in pediatric SBS-IF and acute graft versus host disease.
Indication(s) Stage of Development Upcoming Milestone(s)
Adult SBS-IF
Pediatric SBS-IF1 • Intend to initiate Ph 3 in 2023
Acute Graft Versus Host Disease1 • Intend to initiate Ph 2 in Q1 2022
Preclinical Phase 1 Phase 2 Phase 3
Apraglutide
Discovery
• First readout: H1 2022
• Top-line results: H2 2023
• OLE
VB-1197
VB-1200
VB-1300
VB-1400
CoMET
Malonic and Propionic Acidemia
Other Organic Acidemias
VB-1197 • Intend to initiate Ph 1 by Q1 2023
Urea Cycle Disorders
Fatty Acid Oxidation Disorders
Amino Acidopathies
6

7 R&D Day
Program & Speakers
Luca Santarelli, M.D.Founder and CEO
Omar Khwaja, M.D., Ph.D.Chief Medical Officer
Nader Youssef, M.D., MBA, FACGSVP, Global Medical Affairs & GI Therapeutic
Area Head
Kishore Iyer, MBBS, FRCS, FACSDirector of Adult and Pediatric Intestinal Rehabilitation
& Transplantation at Mount Sinai Medical Center
Robert Zeiser, M.D.Head of Tumor Immunology and Immune Modulation
at the University Medical Center Freiburg
Introduction to VectivBio
ApraglutideShort Bowel Syndrome with Intestinal Failure
ApraglutideAcute Graft-versus-Host-Disease
CoMET – Coenzyme Metabolism PlatformInherited Metabolic Diseases
Conclusion
Question & Answer
7

SBS-IF

R&D Day
SBS-IF Represents a Significant Opportunity
* We estimate that the addressable global market opportunity for apraglutide, if approved, in SBS-IF, could exceed $2 billion per year through significant growth in the number of eligible patients receiving a GLP-2 analog, potentially improved compliance and persistency, and geographic expansion beyond where teduglutide is approved today.
Source: Custom market research commissioned by VectivBio, Nov 2019; internal estimates.
Rest of World Opportunity
~ 1,000 SBS-IF patients in Japan
China
Other Markets
5,000
7,500
2,500
7,500
U.S. Market Opportunity
EU Market Opportunity
We Believe There is a >$2 Billion Peak Market Potential Opportunity*
Est. Peak SBS-IF Patients Treated
with GLP-2
U.S. and EU Market Opportunity
Est. SBS-IF Patients
9

R&D Day
Significant Unmet Medical Needs Remain with Gattex
PS, parenteral support (includes parenteral nutrition and/or intravenous fluid)
1. Gattex® (teduglutide) for injection. Prescribing Information; 2. Revestive® Summary of Product Characteristics; 3. Gattex® (teduglutide) Instructions for Use; 4. Jeppesen PB, et al. Gastroenterology. 2012; 5. Jeppesen PB et al. Clin. Nutr. 2013; 6. Jeppesen PB, et al. Gastroenterology. 2018; 7. CRA Market Research, Nov 2019 (U.S. and EU5); 8. Symphony Health, PatientSource®, Dec 2015–Jan 2019 (analysis period of claims); patient cohort: U.S. patients starting Gattex who have had an SBS diagnosis and at least 180 days of parenteral nutrition prior to receiving Gattex and who could be followed for at least 24 months; patients are considered discontinued if they have a gap in therapy >90 days; patients are considered persistent until first event of discontinuation.
10
Gattex® / Revestive®
(only GLP-2 analog approved for SBS-IF since 2021)1,2
Limitations of Gattex
• 2hr half life, daily subcutaneous injections1
• Lengthy and complex administration procedure3
• Only partially addresses the needs of
SBS-IF patients:
• Adverse events: injection site reactions and abdominal pain1,4
• No demonstrated impact on patients’ quality of life5
• Colon-in-continuity patients treated with Gattex did not exhibit a
significant reduction in PS volume as compared to placebo-treated
patients in Phase 3 trial6
• Gattex is predominantly used in stoma/high PS SBS-IF patients7
Gattex 24-Month Persistency, U.S. (n=194)8
74%
62%
48%
34%
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6 7 8 9 101112131415161718192021222324Months
Despite significant limitations, Gattex revenue was >$600M in FY20
Increases intestinal absorption and reduces the volume of parenteral support*
Limited/niched use, sub-optimal persistency
R&D Day
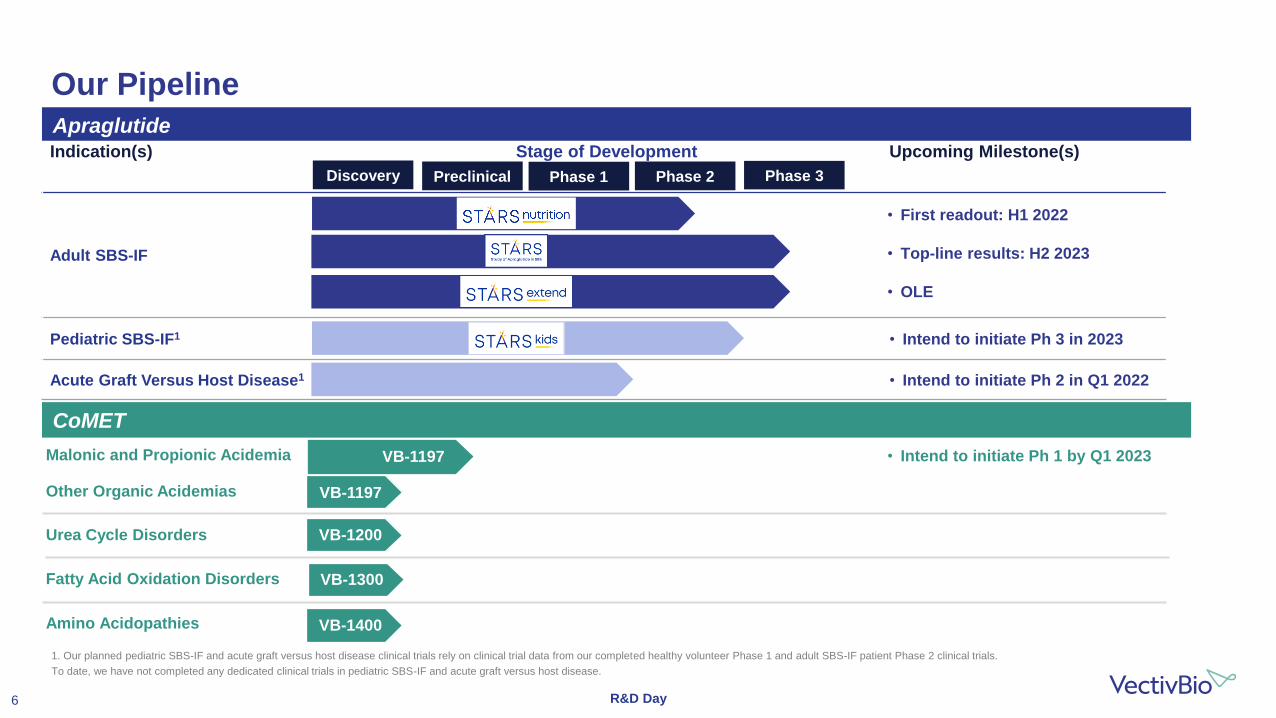
Apraglutide Has the Potential to Establish a New Standard of Care
*Management expectations, based on clinical trials to date.
1. Martchenko SE et al. J Pharmacol Exp Ther. 2020; 2. Hargrove DM et al. J Pharmacol Exp Ther. 2020; 3. Eliasson J et al. Clinical Nutrition ESPEN 40 (2020), 459; 4. Eliasson J et al. Clinical Nutrition ESPEN 40 (2020), 436.
11
Enhanced Value Proposition
Differentiated Apraglutide Target Profile*
• Convenient administration
• Weekly dosing3,4
• Developing pre-filled syringe
• Demonstrated robust pharmacology
• Improved intestinotrophic effects in preclinical models1,2
• Enhanced energy absorption in SBS patients in Phase 23
• Differentiated clinical and regulatory strategy in Phase 3
• Takes into account remnant bowel anatomy when weaning PS and assessing benefits from GLP-2 treatment
• Focuses on clinically meaningful effects, including enteral autonomy and quality of life measurements
R&D Day
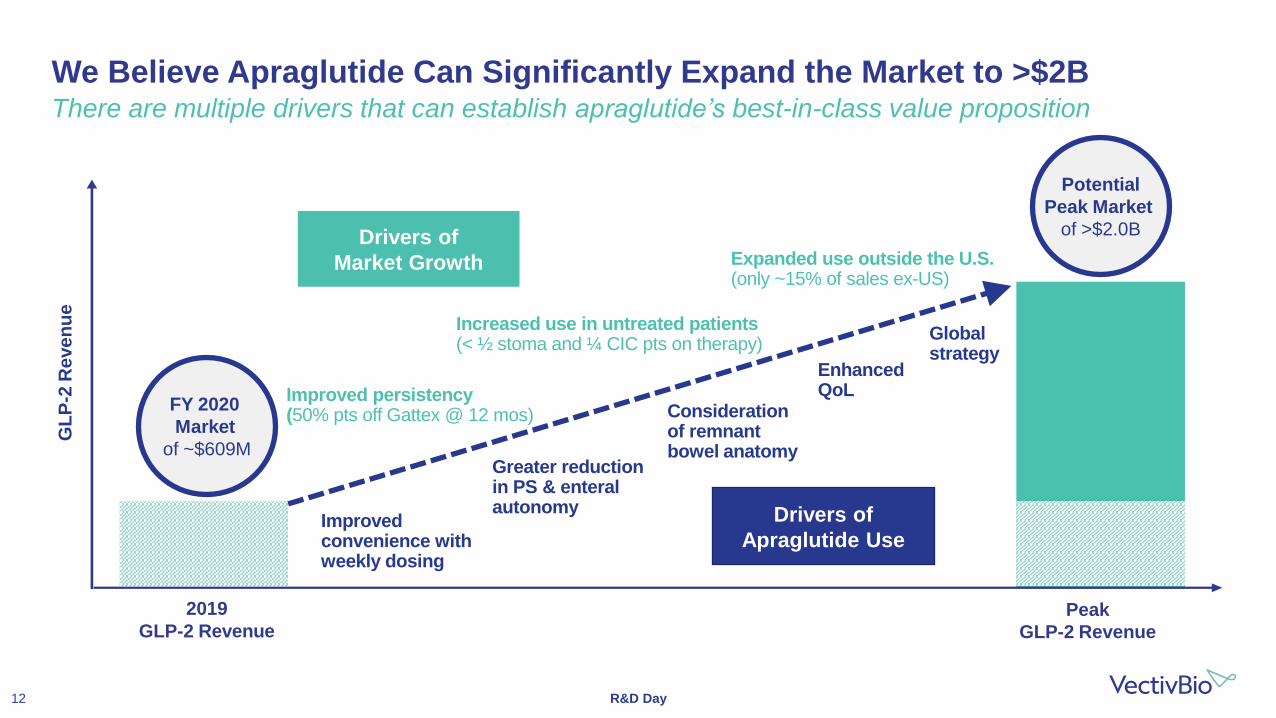
We Believe Apraglutide Can Significantly Expand the Market to >$2BThere are multiple drivers that can establish apraglutide’s best-in-class value proposition
GL
P-2
Re
ve
nu
e
2019
GLP-2 RevenuePeak
GLP-2 Revenue
FY 2020
Market
of ~$609M
Potential
Peak Market
of >$2.0BDrivers of
Market Growth
Drivers of
Apraglutide UseImproved convenience with weekly dosing
Greater reduction in PS & enteral autonomy
Consideration of remnant bowel anatomy
Enhanced QoLImproved persistency
(50% pts off Gattex @ 12 mos)
Increased use in untreated patients(< ½ stoma and ¼ CIC pts on therapy)
Expanded use outside the U.S.(only ~15% of sales ex-US)
Global strategy
12

Short Bowel Syndromewith Intestinal Failure (SBS-IF)
Nader Youssef, M.D., MBA, FACGSVP, Global Medical Affairs & Therapeutic Area Head, GI

R&D Day
Short Bowel Syndrome with Intestinal Failure
Short Bowel Syndrome (SBS)
SBS-Intestinal Failure
(SBS-IF) • Requires intravenous supplementation
of parenteral nutrition to maintain life
• Standard of care includes PN, symptom management teduglutide
• Significant unmet need
• Improve nutrient and fluid absorption
• Reduce PN dependence and serious complications
• Achieve enteral autonomy from PNIBD, inflammatory bowel disease
Pironi L et al. Clin Nutr. 2015 Apr;34(2):171-8014
• Loss of significant length of bowel
due to disease or surgical resection
• Causes include: IBD, trauma,
mesenteric infarction, bariatric
surgery, etc.
• Patients may require short-term
intravenous parenteral nutrition (PN),
or permanent PN and become SBS-IF

R&D Day
SBS-IF is Associated with Significant Burden
SBS-IF, intestinal failure associated with short bowel syndrome; SBS, short bowel syndrome; PS, parenteral support (includes parenteral nutrition and/or intravenous fluid); GI, gastrointestinal; QoL, quality of life
1. Parrish CR et al. Gastroenterol Hepatol (N Y). 2017 Oct;13(10):600-608; 2. Billiauws L et al. J Visc Surg. 2018 Sep;155(4):283-291; 3. Schalamon J et al. Best Pract Res Clin Gastroenterol. 2003 Dec;17(6):931-42; 4. Howard L. Gastroenterology. 2006 Feb;130(2 Suppl 1):S52-9; 5. Ballinger R et al. ISPOR 2019; 6. Piamjariyakul U et al. Nurs Econ. 2010 Jul-Aug;28(4):255-63.
15
• 30% mortality after 5 years SBS patients on home PS3
• PN Complications impact long-term survival3Increased Mortality1,3
• Central venous access complications1,2
• Organ damage1,2
• GI complications1,2
Significant Morbidity1,2
• Significant reductions in patient QoL:4
• Negative QoL impact on caregivers5
Reduced Quality of Life1,4,5
• Average annual costs of chronic PS is $185-594k6
• Significant indirect costs from disability & lost productivity
Burden to the Healthcare System6
1
2
3
4

R&D Day
• Decreased bacterial infection
• Decreased gut injury in chemically induced enteritis
• Modulation of intestinal microbiome
GLP-2 Pharmacological ActionsAn enteroendocrine tissue hormone produced by intestinal L cells
Actions are mediated by a distinct GLP-2 receptor expressed on subsets of enteric nerves and enteroendocrine cells in the stomach and small and large intestine
Preclinical data
GLP-2, Glucagon-like peptide 2; GI, gastrointestinal
Drucker DJ. Gastroenterology. 2002
• Improved intestinal adaptation after bowel resection
• Promoted nutrient and fluid absorption via expansion of the mucosal epithelium
↑ Enterocyte Proliferation
↑ Intestinal Barrier Function & ↓ Epithelial Damage
• Decreased meal-stimulated gastric acid secretion and GI motility
Enterocytes
GLP-2
Villus
Crypt
L-cells
Intestinal Stem Cells
Paneth Cells
Subepithelial Myofibroblasts
Enteric Nerves
16
↑ Intestinal Blood Perfusion
↓ GI Motility
• Vascular-ischemia reperfusion injury, and dextran sulfate-induced colitis

R&D Day
Apraglutide Rationally Designed to Have Enhanced PK/PDComparative peptide sequence of apraglutide to teduglutide and glepaglutide
PK, pharmacokinetic; PD, pharmacodynamic; GLP-2, Glucagon-like peptide 2; DPP-IV, dipeptidyl peptidase IV; SC, subcutaneous
Adapted from K Wisńiewski et al., J. Med. Chem. 2016, 59, 3129−3139
17
Molecular class: Peptide, chemically synthesized
Chemical name: [Gly2, Nle10, D-Phe11, Leu16]hGLP-2 (1-33)-NH2
Structural formula: H-His-Gly-Asp-Gly-Ser-Phe-Ser-Asp-Glu-Nle-D-Phe-Thr-Ile-Leu-Asp-Leu-Leu-Ala-Ala-Arg-Asp-Phe-Ile-
Asn-Trp-Leu-Ile-Gln-Thr-Lys-Ile-Thr-Asp-NH2 (Sodium salt)
The sequence of apraglutide contains one D stereoisomer-amino acid (D-phenylalanine) and two achiral amino acids (glycine).
All other amino acids are of L-configuration. Apraglutide is synthesized as a single enantiomer with all stereo-centers of defined chirality
Replacement of two asparagines, Asn11 by D-Phe11 and Asn16 by Leu16, causes a significant change in plasma protein binding and corresponding remarkable decrease in totalclearance. (K Wisńiewski et al.)
Replacement of Met10 by Nle10 provides enhanced chemical stability. (K Wisńiewski et al.)
The lower charge due to the amide group is thought to result in a more limited solubility, thereby slowing down the absorption from the SC injection site intothe circulation and increasing the terminal half-life.
Gly2 eliminates enzymaticcleavage by DPP-IV enzyme.(K Wisńiewski et al.)
AA Pos. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33
Native GLP-2 H A D G S F S D E M N T I L D N L A A R D F I N W L I Q T K I T D
Teduglutide H G D G S F S D E M N T I L D N L A A R D F I N W L I Q T K I T D
Glepaglutide H G E G T F S S E L A T I L D A L A A R D F I A W L I A T K I T D K
Apraglutide H G D G S F S D E Nle D-Phe T I L D L L A A R D F I N W L I Q T K I T D
Chemical
Name and
Structure
34+
OH
OH
K K K K K K NH2
NH2

R&D Day
Apraglutide Possesses Differentiated Pharmacology (Half-Life)Pharmacokinetic comparisons vs. teduglutide and glepaglutide1
PK, pharmacokinetic; hGLP-2, human glucagon-like peptide 2
1. Hargrove et al. J Pharmacol Exp Ther. 2020 May;373(2):193-203; 2. Bolognani F et al. ESPEN 2020.
18
Human
Rat
1
10
1,000
10,000
90 120
Pla
sm
aC
on
ce
ntr
ati
on
(ng
/ml)
60Time (min)
hGLP-2
Teduglutide
Glepaglutide
Apraglutide
100
300
Apraglutide
Half Life (T1/2) 70–72 hours2
Manufacturing Synthetic
PK supports weekly dosing

R&D Day
Apraglutide Possesses Differentiated Pharmacology (Intestinotrophic)Greater efficacy on intestinal growth in head-to-head preclinical studies in rats
* = p< 0.05 vs corresponding vehicle control.
^ = p< 0.05 vs. corresponding apraglutide treatment group.
Hargrove et al. J Pharmacol Exp Ther. 2020 May;373(2):193-203
19
Daily Injection (24 hrs. Dosing Interval)Intestine weight 96 hours post 1st injection
Single InjectionIntestine weight 72 hours post injection
60
50
40
30
20
10
0
30 nmol/kg 300 nmol/kg
Sm
all
Inte
stin
e W
etW
eig
ht
(% in
cre
ase o
ve
rve
hic
le)
*
* ^ * ^
* ^
* ^
*
-10
0
10
20
30
30 nmol/kg 300 nmol/kg
Sm
all
Inte
stin
e W
etW
eig
ht
(% incre
ase o
vervehic
le)
*
^ ^ ^
* ^
*
Apraglutide Teduglutide Glepaglutide

R&D Day
GLP-2 Activation by Apraglutide Significantly Increased Intestinal Mucosal Mass and Length
GLP-2, Glucagon-like peptide 2
1. Slim GM et al. JPEN J Parenter Enteral Nutr. 2019 Sep;43(7):891-898; 2. Data on File. VectivBio. Basel, Switzerland.
20
Saline Apraglutide
lnte
stin
ele
ng
th(c
m)
20
15
10
5
0
-5
-10
-15
Representative samples of jejunum from JC piglets (magnification = 20X)
ApraglutideVehicle
Mu
co
sa
l Ma
ss
(mg
/cm
)
210
190
170
150
130
110
90
Change in Intestinal Length
Change in Mucosal Mass
Histological observations of the jejunum in apraglutide-treated jejunostomy
piglets demonstrated elongated villi compared to control

R&D Day
Methodology for Phase 2 Studies in SBSThe effects of GLP-2 on output assessed while input is maintained constant
SBS, short bowel syndrome; GLP-2, Glucagon-like peptide 2
21
Phase 2
Baseline 4 Weeks
Phase 3
Baseline 4 WeeksBaseline 4 Weeks Baseline 6 Months
Stable External Fluids
surface area
fluid absorption
Phase 2
Baseline 4 Weeks
Phase 3
Baseline 4 WeeksBaseline 4 Weeks Baseline 6 Months
Stable External Fluids
surface area
fluid absorption
After 4 Weeks
Phase 2
Baseline 4 Weeks
Phase 3
Baseline 4 Weeks
Urine Output
Stoma Bag Volume & Calories
Baseline
Phase 2
Baseline 4 Weeks
Phase 3
Baseline 4 Weeks
Stoma Bag Volume& Calories
Low Urine Output

R&D Day
Apraglutide Phase 2: Once-Weekly Proof of Concept Achieved in SBSClinically relevant pharmacodynamic effects observed in ALL subjects at 5 mg/week
SBS, short bowel syndrome; SEM, standard error of mean
Eliasson J et al. Oral presentation at the American Society for Parenteral and Enteral Nutrition (ASPEN) Nutrition Science and Practice Conference on March 20-23, 2021. Virtual meeting. Abstract # 944900
22
Urinary Output Wet Weight Absorption Energy Absorption
0
200
400
600
800
1,000
Baseline End of Treatment
Ch
an
ge
fro
m B
as
eli
ne
, g
/da
y
Mean +/- SEM
0
200
400
600
800
1,000
Baseline End of Treatment
Ch
an
ge
fro
m B
as
eli
ne
, g
/da
y
Mean +/- SEM
0
250
500
750
1,000
1,250
1,500
Baseline End of Treatment
Ch
an
ge
fro
m B
as
eli
ne
, k
J/d
ay
Mean +/- SEM

R&D Day
Apraglutide Studied in a Metabolic Balance TrialApraglutide demonstrated statistically significant increases in energy absorption with weekly dosing
*p=0.0374, **p=0.0150, ***p=0.0236
CFB, change from baseline; GLP-2, Glucagon-like peptide 2
1. Eliasson J et al. Clinical Nutrition ESPEN 40 (2020), 459; 2. Jeppesen PB et al. Gut. 2005 Sep;54(9):1224-31; 3. Naimi RM et al. EBioMedicine. 2019 Aug;46:444-451
23
Apraglutide1
5 mg ONCE-WEEKLY
Urinary Output (% CFB) 39.1%*
Wet Weight Absorption (CFB) 740.7 g/day**
Energy Absorption (CFB) 1,094.8 kj/day***
• Only GLP-2 to demonstrate robust absorption
enhancements after weekly dosing
• Only GLP-2 to demonstrate statistically
significant enhancement in energy absorption
in Phase 22,3
• Enhanced energy absorption could result in
better outcomes in patients

R&D Day
SBS is Heterogeneous Based on Remnant Bowel AnatomyStoma and CIC patients have different responses to Gattex1
*As compared to placebo at six months in the phase 3 study
SBS, short bowel syndrome; PS, parenteral support
1. Jeppesen PB et al. Gastroenterology. 2018 Mar;154(4):874-885; 2. Company Phase 3 feasibility and CRA Market Research, Nov 2019 (U.S. and EU5).
24
Stoma Colon-in-Continuity (CIC)
Prevalence2 ~45% of Patients ~55% of Patients
Anatomy No functional colon ≥50% of colon remaining
Absorption deficits Limited oral absorption of fluids Sufficient oral absorption of fluids
PS requirements Require large volume of PS consisting of fluids &
nutrientsRequire lower PS volume to deliver nutrients
• Stoma patients require more fluids in their PS because they cannot absorb water
• CIC patients require mainly ‘additional calories’ with an overall lower PS volume
Duodenum
Jejunocolonic
Anastomosis
Jejunum
Colon
Duodenum
Jejunum
Stoma(on abdominal surface)
Stoma Bag Adapted from: Jeppesen P et. al., Gastroenterology, 2018

Kishore Iyer, MBBS, FRCS, FACSDirector of Adult and Pediatric Intestinal Rehabilitation
& Transplantation at Mount Sinai Medical Center
SBS-IFLessons Learned in the GLP-2 Era:
Can We Improve Outcomes Further?

R&D Day
• Scientific advisor (Pharma):
‒ VectivBio
‒ Zealand
‒ Takeda
‒ Hanmi
• Investigator (Pharma):
‒ VectivBio
‒ Takeda
‒ Zealand
• Grant support (Pharma):
‒ Takeda
‒ Zealand
Disclosure
26

R&D Day
*Based on N=85 (Gattex® (teduglutide) for injection. Prescribing Information)
PS, parenteral support
Jeppesen PB, et al. Gastroenterology. 2012;143:1473-1481
Teduglutide Phase 3 STEPS Study Design & Patient Characteristics
N=86
Remnant Bowel Anatomy n (%)*
Stoma
Colon-in-continuity
38 (45)
47 (55)
PS Dependence, mean (SD)
PS dependence, years
PS volume, L/week
PS infusion, days/week
6.3 (6.0)
12.9 (7.6)
5.8 (1.6)
PS stabilization
Teduglutide 0.05 mg/kg/day
Placebo
PS optimization
4–8 weeks0–8 weeks
Urine volume 1–2 L/day
24 weeks
27

R&D Day
PS, parenteral support
Jeppesen PB, et al. Gastroenterology. 2012;143:1473-1481
Teduglutide Phase 3 STEPS Study Significant effect in Responder Rate analysis (primary endpoint)
Responders defined as patients with ≥20%reduction from baseline in weekly PS volume at Weeks 20 and 24
63%*
30%
0
10
20
30
40
50
60
70
Placebo (n=43)
Teduglutide 0.05 mg/kg/day(n=43)
Resp
on
ders
, % *P=0.002 vs placebo
Cochran-Mantel-Haenszel Test
• Primary endpoint defined as ≥20% reduction in weekly PS volume from baseline at both Weeks 20 and 24:
‒ Clinically meaningful to patients and physicians
‒ Reflects increased intestinal absorption
• Potential for 1 additional day off PS
28

R&D Day
Teduglutide STEPS Phase 3 Retrospective Analysis (i)Response was driven by effects on PS volume reduction in stoma patients only
a. n=14 with data available; b. n=6 with data available; c. n=13 with data available.
TED, teduglutide; PBO, placebo; PS, parenteral support; SD, standard deviation; CIC, colon in continuity
Jeppesen PB et al, Gastroenterology. 2018 Mar;154(4):874-885
29
Group 1
• Stoma anatomy • 0% colon remaining
Group 2
• Colon in continuity • ≥50% colon remaining• No stoma
Parameter TED (n=17)a PBO (n=16) TED (n=18) PBO (n=20)
PS volume % change from baselinemean (SD)
–40.3 (18.26) –18.8 (29.10)c –23.3 (15.84) –23.8 (22.23)
• While the study met its primary endpoint, the results were mostly driven by patients with stoma and high PS volume requirements at baseline
• 55.6% of patients treated with teduglutide had CIC, however, benefits in these patients were minimal

R&D Day
Teduglutide STEPS Phase 3 Retrospective Analysis (ii)An increase in PS days off was observed in CIC patients
a. n=14 with data available; b. n=6 with data available; c. n=13 with data available.
CIC, colon in continuity; TED, teduglutide; PBO, placebo; PS, parenteral support
Jeppesen PB et al, Gastroenterology. 2018 Mar;154(4):874-885
30
Additional days off PS per weekn (%)
Group 1
• Stoma anatomy • 0% colon remaining
Group 2
• Colon in continuity • ≥50% colon remaining• No stoma
TED (n=17)a PBO (n=16) TED (n=18) PBO (n=20)
≥1-day reduction at Week 24 6 (42.9) 2 (15.4)c 10 (55.6) 6 (30.0)
• CIC patients have higher likelihood of achieving clinically meaningful days off compared to stoma patients
‒ Days off PS and enteral autonomy are important to patients
• Enteral absorption must be considered along with urine volume in CIC patients

R&D Day
• 11/18 patients achieved enteral autonomy
‒ 1/3 (33%) stoma patients
‒ 10/15 (67%) CIC patients
Single Center Experience1
(N=18)
• 13/54 achieved enteral autonomy
‒ 2/19 (11%) stoma patients
‒ 11/35 (31%) CIC patients
French National Cohort Study2
(N=54)
Real-world data of GLP-2 in SBS-IF patientsEvidence that CIC patients could achieve higher rates of enteral autonomy with GLP-2 treatment
GLP-2, Glucagon-like peptide 2; CIC, colon in continuity
1. Lam K et al. JPEN J Parenter Enteral Nutr. 2018 Jan;42(1):225-230; 2. Joly F et al. Clin Nutr. 2020 Sep;39(9):2856-2862
31

R&D Day
Single-Center US Experience in Adult PatientsReal-world data supports benefit of GLP-2 in CIC patients achieving enteral autonomy
GLP-2, Glucagon-like peptide 2; CIC, colon in continuity; PS, parenteral support
Lam K et al. JPEN J Parenter Enteral Nutr. 2018 Jan;42(1):225-230
32
Baseline Characteristics of Patients on teduglutide
N = 18
Stoma 3
CIC 15
Median (range)
Age, years 47 (20–81)
Time between last bowel resection and
initiation of teduglutide, years4 (1–13)
Time on PS prior to teduglutide, months 36 (4–96 )
Weekly PS volume prior to teduglutide, L 9.9 (2.7–30)
PS calories prior to teduglutide, kcal/day 682 (0–1823)
Small bowel length, cm 55 (6–180)
• 16/18 decreased PS
‒ 11/18 (61%) patients achieved enteral
autonomy
▪ Total median duration of teduglutide
therapy prior to achieving enteral
autonomy was 10 months (range: 3–36)
▪ 10/11 patients with CIC
‒ 2/18 decreased PS volume by 50%
‒ 2/18 decreased PS volume by 20%
Results

R&D Day
French Real-world Experience
* Includes patients with ≥50% and <50% of colon in continuity
SBS, short bowel syndrome; PS, parenteral support; CIC, colon in continuity
Joly F et al. Clin Nutr. 2020 Sep;39(9):2856-2862
33
• Open-label, observational study (N=74)
‒ 15 sites in France allowed to prescribe teduglutide
‒ Retrospective analysis at 6 months
• Objective: To evaluate in a “real world setting” SBS cohort, predictive factors for response & weaning off PS
• Of 74 patients who initiated teduglutide treatment, 54 received ≥6 months of teduglutide treatment
Baseline Characteristics N = 54
Age, year (range) 52.3 (22–84)
Gender 22 F 32 M
Remnant Bowel Anatomy, n (%)
Stoma
CIC*
19 (35)
35 (65)
PS Duration, year (range) 9.8 (0.5–31)
Infusion per Week, days (range) 4.3 (2–7)
Volume of PS, L/week (range) 11.1 (2–38.5)
Energy from PS, Kcal/ week (range) 6747 (0–16800)
Remnant Bowel Length, cm (range) 61 (0–200)

R&D Day
French Real-world Experience with TeduglutideThe majority of patients weaned off PS had CIC anatomy
* Includes patients with ≥50% and <50% of colon in continuity
PS, parenteral support; SD, standard deviation; CIC, colon-in-continuity
Joly F et al. Clin Nutr. 2020 Sep;39(9):2856-2862
34
• 11/13 patients who weaned from PS had CIC
• Patients who weaned off PS had:
‒ Less PS volume requirement at baseline
‒ More oral intake at baseline
Analysis of predictive factors associated with weaning off PS at 24 weeks
among SBS-IF patients who received ≥6 months of teduglutide (N=54)
Weaned
n=13
Non-weaned
n=41
Bowel anatomy
Stoma, n (%)
CIC, n* (%)
2/13 (15)
11/13 (85)
17/41 (42)
23/41 (56)
Intestinal failure features
Basal PS volume, mean mL/day (SD)
Basal oral intake, mean kcal/day (SD)
738 (272)
2845 (787)
1867 (1253)
2294 (657)

R&D Day
Key Learnings from Past SBS ExperienceOpportunity to improve outcomes by considering an individual’s remnant bowel anatomy
SBS, short bowel syndrome; CIC, colon in continuity
1. Jeppesen PB et al, Gastroenterology. 2018 Mar;154(4):874-885; 2. Joly F et al. Clin Nutr. 2020 Sep;39(9):2856-2862
35
• Diuresis is a good marker of response in stoma patients
• Diuresis alone proved insensitive1 in CIC patients; enteral absorption must be considered2
Establishing Clinical Relevance
DiuresisEnteral
absorption
Consider individual remnant bowel anatomy
Diuresis
Stoma Colon-in-Continuity
Evaluating Efficacy
• PS volume reduction has greatest
therapeutic relevance in stoma patients
• Days off and enteral autonomy are the
therapeutic goals in CIC

R&D Day
Key Learnings for Future Apraglutide Study Design
GLP-2, Glucagon-like peptide 2; PS, parenteral support; SBS-IF, intestinal failure associated with short bowel syndrome
36
SBS is heterogeneous and encompasses a spectrum of anatomical diversity: stoma and CIC
Current experience with GLP-2 analogues focuses mostly on patients with stoma and high PS volume requirements
Post-hoc analysis and real-world data from teduglutide suggests remnant anatomy should be considered when assessing response to GLP-2 analogues
There is opportunity to individualize GLP-2 treatment and improve outcomes by considering an individual’s remnant bowel anatomy
Patients with CIC need to be better characterized
Goal of the apraglutide studies are designs that allow for more clinically meaningful results and captures responses in CIC patients

Nader Youssef, M.D., MBA, FACGSVP, Global Medical Affairs & Therapeutic Area Head, GI
SBS-IFSTARS Clinical Trials

R&D Day
STARS Study Design
Enrollment of 144 SBS-IF patients
Week 24
Primary endpoint: PS volume reduction
Secondary endpoints collected across all patients and by anatomy
Week 48
Secondary endpoints
collected by anatomy
Apraglutide (96 patients)
Placebo (48 patients) 2:1 randomization
Anatomy-specific randomization
Two dose arms: weekly placebo and apraglutide(2.5 or 5 mg depending on body weight)
Primary endpoint (week 24):PS volume reduction in overall population
Secondary endpoints (week 24 and 48):Common and anatomy-specific
Anatomy-specific PS reduction algorithm to best adapt PS requirements
1
2
3
4
5
6
First patient dosed January 2021; Topline results anticipated in 2H2023
Pivotal Phase 3 study in SBS-IF patients
Regulatory alignment obtained from FDA, EMA and PMDA on critical design elements
38

R&D Day
STARS Nutrition Study Design Metabolic Balance Study in SBS-IF patients with CIC anatomy
39
Up to 10 SBS-IF patients with CIC
Open label, baseline controlled
Weekly apraglutide (2.5 or 5 mg depending on body weight)
Primary objective: Calorie absorption increases at week 4 and 48
Secondary endpoint: PS volume reduction/enteral autonomy at week 48
1
2
3
4
5
0-1 4 28 52
MB MB MB
Week
Metabolic Balance
ObjectiveIntestinal
Absorption PS reduction and wean off
Apraglutide Treatment
OLE48
First patient dosed June 2021; Data from first 4 weeks of treatment anticipated in 1H2022

R&D Day
Apraglutide Potential Advantages
40
Improved:
• Efficacy
• Tolerability
• Convenience
Longer half-life
Potent intestinotrophic effects
Weekly dosing
Increased energy absorption
Pre-filled syringe

Omar Khwaja, M.D., Ph.D.Chief Medical Officer
Graft Versus Host Disease (GvHD)

R&D Day
• Emerges within the first 100 days post-transplant1,2
• Predominantly affects the skin, GI tract, and liver3,4
• Secretory and bile salt diarrhea, severe abdominal pain, increasing severe nausea1,3,4
• Malabsorption, weight loss, and need for parenteral support6
• Maculopapular skin rash1
• 30% mortality at 12-months in steroid refractory patients is driven by the severity of GI symptoms5
• Grades II, III, and IV have ~80%, ~25%, and ~5% survival rates, respectively7
Gastrointestinal GvHD is one of the leading causes of morbidity and mortality
Diagnosis
Symptoms
Outcomes
GI, gastrointestinal; GvHD, graft versus host disease
1. Goker H et al. Exp Hematol. 2001 Mar;29(3):259-77; 2. Filipovich AH et al. Biol Blood Marrow Transplant. 2005 Dec;11(12):945-56; 3. MacMillan ML et al. Biol Blood Marrow Transplant. 2002;8(7):387-94; 4. RowlingsPA et al. Br J Haematol. 1997 Jun;97(4):855-64; 5. Dignan Fl et al. Br J Haematol. 2012;158(1):30-45; 6. Naymagon S et al. Nat Rev Gastroenterol Hepatol. 2017 Dec;14(12):711-726; 7. Cahn JY et al. Blood. 2005 Aug 15;106(4):1495-500
Acute GvHD is a Life-Threatening Condition Resulting From Allogeneic Hematopoietic Stem Cell Transplant (HSCT)
Erosion/ulceration in patients with acute GI-GvHD7
© 2018 Ohwada et al.
42

R&D Day
More than 27,000 Allogeneic HSCT take place in US and Europe yearlyAcute GVHD occurs in 50% of patients of whom half will become steroid-refractory
* Calculated based on 50% of allogeneic transplants developing aGvHD
HSCT, hematopoietic cell transplants; 1. Gratwohl A et al. Lancet Haematol. 2015 Mar;2(3):e91-100; 2. World Health Organization. https://www.who.int/transplantation/hsctx/en/. Accessed on Dec 18, 2020; 3. D'Souza A et al. Transplant. 2020 Aug;26(8):e177-e182; 4. Baldomero H et al. EBMT activity survey 2018; 5. Jacobsohn DA, Vogelsang GB. Orphanet J Rare Dis. 2007 Sep 4;2:35; 6. Martin PJ et al, Biol Blood Marrow Transplant 2004; 10:320–327; 7. Martin PJ et al. Biol Blood Marrow Transplant. 2012;18(8):1150-1163; 8. Dignan FL et al . J Haematol. 2012;158(1):30-45; 9. MacMillan ML et al. Biol Blood Marrow Transplant. 2002;8(7):387-394; 10. Schoemans HM et al Bone Marrow Transplant. 2018;53(11):1401-1415.
43

R&D Day
SR aGvHD is Associated with High Mortality Durable overall responses and failure-free survival remain areas of unmet medical need
Figures adapted from R Zeiser et al. N Engl J Med 2020;382:1800-1810.
SR aGVHD steroid refractory acute graft versus host disease
Ruxolitinib for Glucocorticoid-Refractory
Acute Graft-versus-Host Disease
N Engl J Med 2020; 382:1800-1810
Robert Zeiser, M.D., et al., for the REACH2 Trial Group*
44
Prof. Dr. Robert ZeiserHead of Tumor Immunology and Immune Modulation
at the University Medical Center Freiburg
GvHDA Potential New Approach for GvHD:
Modulation of GI GvHD with GLP-2

R&D Day
• Tissue damage mediated by donor T cell responses and inflammatory cytokine
• Recipient intolerance of donor cell due to downregulation or inhibition of recipient Treg cell and upregulation of the recipient TEFF cell
• Immune activation due to dysfunction in recipient antigen-presenting cells
Compromised intestinal epithelium
Immune dysregulation leads to compromised:
• intestinal stem cells• Paneth cells• goblet cells
Gut Microbiota Imbalances
Altered microbiota composition due to:
• conditioning regimens• broad-spectrum antibiotics• immunosuppressants• foreign grafted lymphocytes
Mucosal Barrier Disturbance
Leads to failure of fluid resorption, particularly in the ileum and bacterial
translocation into the systemic circulation
• Osmotic diarrhea due to mucosal cell destruction, compromised brush border tight junctions, and substantial mucosal protein loss
• Bile salt diarrhea due to inflammatory-cell-mediated destruction of apical bile salt transporters in the ileal brush border and bile acid malabsorption
GI Tract is One of the Primary Tissue Systems Damaged in Acute GvHDPlays a major role in the initiation and amplification of systemic immunological reaction driving GvHD
GvHD, graft versus host disease; Treg , regulatory T cell; TEFF, effector T cell
Ghimire et al. Front Immunol. 2017 Mar 20;8:79
• Loss of microbiome diversity early after HSCT has been recognized as a new risk factor for GvHD and HSCT-related complications
46

R&D Day
Pathophysiology of Acute GvHDDamage to the host tissues leading to release of inflammatory cytokines
GvHD, graft versus host disease
Ghimire et al. Front Immunol. 2017 Mar 20;8:79
• Conditioning regimen cause profound
damage to the host tissues leading to
release of inflammatory cytokines,
activating host antigen-presenting cells
(APCs)
• Loss of microbial diversity and
metabolites leads to loss of epithelial
and immune homeostasis.
• Host APCs activate mature donor T
cells present in stem cell inoculum
• T cells proliferate and differentiate
• Activation of CD4 cytotoxic T
lymphocyte (CTL), CD8 CTL, and
natural killer cells that mediate tissue
damage
• Effector T cells & pro-
inflammatory cytokines attack
the epithelial cells of skin, liver,
lung, and GI
• Damage is further supported by
the lipopolysaccharide (LPS)
that has leaked through
damaged intestinal mucosa
• Myeloid cells recruited to
further produce pro-
inflammatory cytokines and
thus enhance the cytokine
storm
47

R&D Day
Proinflammatory events and intestinal repair mechanisms in GvHD
GvHD, graft versus host disease
Zeiser R, Blazar BR. N Engl J Med. 2017;377(22):2167-2179
48
R&D Day
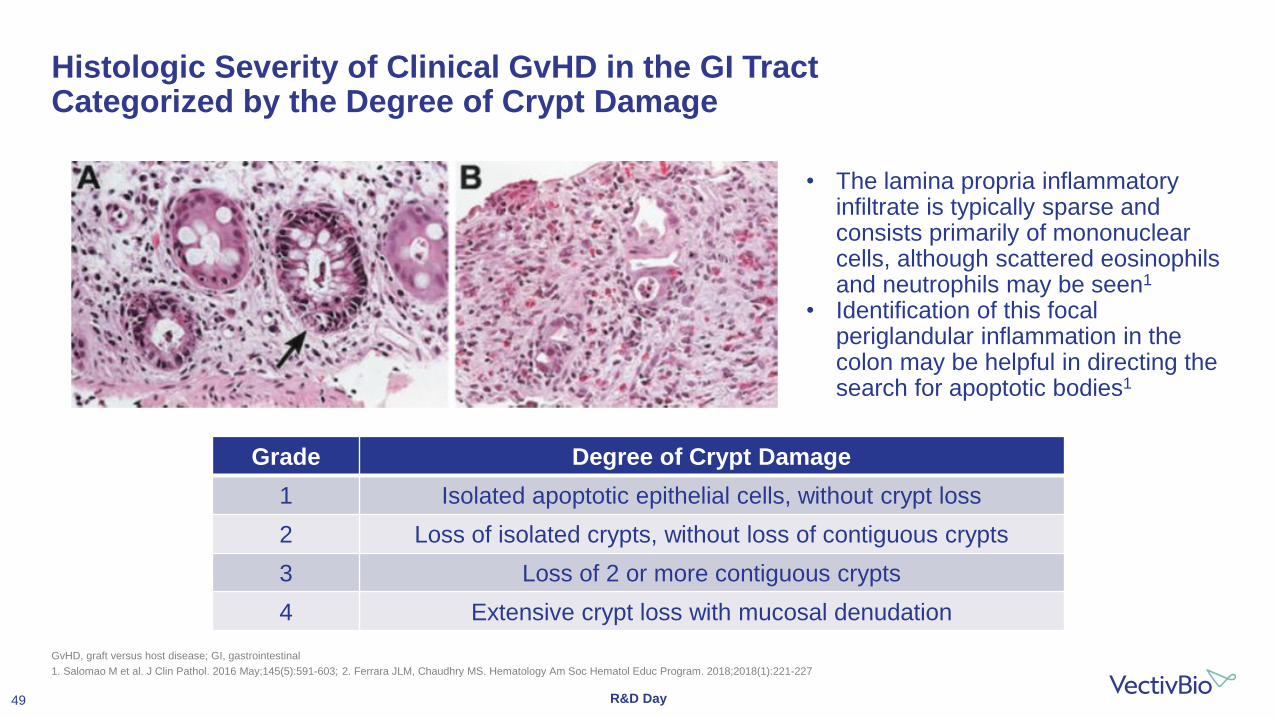
Histologic Severity of Clinical GvHD in the GI Tract Categorized by the Degree of Crypt Damage
GvHD, graft versus host disease; GI, gastrointestinal
1. Salomao M et al. J Clin Pathol. 2016 May;145(5):591-603; 2. Ferrara JLM, Chaudhry MS. Hematology Am Soc Hematol Educ Program. 2018;2018(1):221-227
• The lamina propria inflammatory infiltrate is typically sparse and consists primarily of mononuclear cells, although scattered eosinophils and neutrophils may be seen1
• Identification of this focal periglandular inflammation in the colon may be helpful in directing the search for apoptotic bodies1
Grade Degree of Crypt Damage
1 Isolated apoptotic epithelial cells, without crypt loss
2 Loss of isolated crypts, without loss of contiguous crypts
3 Loss of 2 or more contiguous crypts
4 Extensive crypt loss with mucosal denudation
49

R&D Day
L-Cells are a Target of GvHDChemotherapy, total body irradiation, and GvHD affect L-cells
GvHD, graft versus host disease; GLP-2, glucagon-like peptide 2
1. Sale et al. Am J Surg Pathol. 1979; 2. Epstein et al. Gastroenterology. 1980; 3. Eriguchi et al. Biol Blood Marrow Transplant. 2013; 4. Hanash et al. Immunity. 2012.
Mucosal growth
Reduction of Intestinal inflammation
Reduce apoptosis of enterocytes
L-Cells produces GLP-2 which
Promotes:Chemotherapy or total body irradiation
GvHD
Enterocytes
Villus
Crypt
L-cells
Intestinal Stem Cells
Paneth Cells
Enteric Nerves
50

R&D Day
Role of Paneth Cells in Maintaining Barrier and Antimicrobial FunctionPaneth cells compromised with GvHD
GvHD, graft versus host disease; GLP-2, glucagon-like peptide 2
Serody J. Blood. 2012 Jul 5;120(1):6-7
1. Paneth cells generate antimicrobial peptides in response to bacterial products
2. T-cell immune response leads to loss of Paneth cells, inhibiting antimicrobial peptide
generation leading to bacterial translocation across the mucosa into the systemic
circulation
3. Paneth cell destruction leads to the release of RegIII, which serves as a marker for the
presence of GvHD
Paneth Cell
Antimicrobial Peptides
Systemic Circulation
Crypt Lumen
Bacteria
BacterialProducts
Enterocytes
Villus
Crypt
L-cells
Intestinal Stem Cells
Paneth Cells
Enteric Nerves
51

R&D Day
Results suggested potential use of GLP-2s in the treatment of steroid-resistant aGvHD
Teduglutide, reduced de novo acute GvHD and steroid-refractory GvHD, with no compromising effects on graft-versus-leukemia, an important finding to support clinical studies
Prophylaxis and Treatment Evidence
GLP-2: a potential new approach that aims at protecting and regenerating Paneth cells and intestinal stem cells GLP-2 have promising preclinical rationale to suggest a role in the prevention or treatment of aGvHD
GLP-2, glucagon-like peptide 2; aGvHD, acute graft versus host disease; allo-HSCT, allogeneic hematopoietic stem cell transplant
Norona et al. Blood 2020
Mice treated with teduglutide on day -3 to +3 relative to allo-HSCT demonstrated a lower
GvHD-related mortality vs controls
GLP-2 protected and promoted regeneration of Paneth Cells and intestinal stem cells, which enhanced production of antimicrobial peptides and caused microbiome changes
Mice treated with teduglutide + prednisolone showed lower severity of aGvHD
GLP-2 expanded intestinal organoids and reduced expression of apoptosis-related genes
52

R&D Day
GvHD Results in Decreased Endogenous GLP-2 LevelGLP-2 is an enteroendocrine tissue hormone produced by intestinal L cells
GLP-2, glucagon-like peptide 2; GLP-2+ L-cell, L-cells containing endogenous GLP-2; syn-HCT, syngeneic hematopoietic cell transplantation
Norona et al. Blood 2020
• The number of GLP-2+ L-cell was significantly lower:
‒ When mice developed acute GvHD
‒ In mice that received allo-HCT vs. syn-HCT indicating that the
decrease in L-cell numbers was due to GvHD
‒ In mice developing acute GvHD after chemotherapy conditioning
Mice Colon Sections on Day 10
53

R&D Day
GLP-2 Treatment Reduces GvHD-induced Loss of Paneth Cells
GLP-2, glucagon-like peptide 2; GvHD, graft versus host disease; allo-HSCT, allogeneic hematopoietic stem cell transplant
Norona et al. Blood 2020
• Paneth cells are a target of GvHD
‒ Lysozyme1 Paneth cells
decrease upon GvHD induction
• Paneth cell preserved when mice
were treated with teduglutide
Representative immunohistochemistry staining for the Paneth cell marker, lysozyme (red), in small intestine from allo-HCT BALB/c mice on day 10. Mice treated with vehicle or teduglutide were compared with untreated controls. Mice were treated with teduglutide or vehicle.
54

R&D Day
Initial Clinical Proof-of-Concept Achieved With GLP-2Clinical signs of intestinal GvHD improved in all 6 patients with a decline in diarrhea frequency
GLP-2, Glucagon-like peptide 2; aGvHD, acute graft versus host disease
1. Norona et al. European Society for Blood and Marrow Transplantation Conference, March 2021, Abstract OS9-1 and oral presentation.
Clinical Findings of GLP-2 in aGvHD1
Methods:
• N=6
• Steroid-refractory aGvHD
• Failed multiple therapies – 5 of 6 patients on ruxolitinib + steroids
• Once daily dosing of teduglutide for 10 days
Findings:
• Clinical signs of intestinal GvHD improved in all 6
patients with a decline in the frequency of diarrhea
• Serum albumin levels increased in all patients, a
parameter indicating a positive impact on patients’
nutritional status
Change in Stools Per Day Change in Albumin
Normal range:3.5 – 5.5 g/dL
55

GvHDApraglutide Development in aGvHD
Omar Khwaja, M.D., Ph.D.Chief Medical Officer

R&D Day
Apraglutide, a Novel Regenerative Medicine ApproachCompelling preclinical data support the therapeutic potential in aGvHD
Source: Data on file. VectivBio. Basel, Switzerland.TBI: Total Body Irradiation; BMT: Bone Marrow Transplant; Gy: Gray (unit)
0
20
40
60
80
100
5 6 7 8 9 10 11 12 13 14
Su
rviv
al
(%)
Days Post-Transplant
TBI Only
TBI/BMT + Vehicle
TBI/BMT + apraglutide
Apraglutide Reduced Mortality Apraglutide Prevented GI Damage
TBI (8.5 Gy)/BMT + vehicle TBI (8.5 Gy)/BMT + apraglutide
TBI-BMT Model (7.0 Gy)
5/5
4/10
0/10
Preclinical Findings of Apraglutide
57

R&D Day
Apraglutide in Animal Model of Melphalan-Induced Intestinal DamageThe addition of apraglutide preserved plasma level of citrulline at normal level
Data on File. VectivBio
58
• Increased weight of duodenum, ileum, and jejunum were observed
• In surviving animals treated with apraglutide, examination revealed the absence of melphalan-induced morphological changes of the small intestine
• There was a marked difference of the intestinal morphology between early-euthanized and surviving animals, suggesting that the improvement of survival of the mice was tightly linked to the preservation of the physical integrity and overall function of the intestinal mucosa
Species: BALB/c miceMelphalan: 17.5 mg/kgApraglutide: 3.3 mg/kg

R&D Day
Apraglutide in Animal Model of Cytarabine-Induced Intestinal DamageMaintenance of serum citrulline level suggested protective effect of apraglutide on intestinal
structure
Data are shown as treatment group Mean±SEM. N=3 per treatment group
Data on File. VectivBio
59
• In parallel to the decrease of the body weight, animals treated only with cytarabine/vehicle showed a significant decrease in serum citrulline
• When the animals also received apraglutide, a significantly smaller serum citrulline level decrease was observed suggesting a protective effect of apraglutide on intestinal structure
Species: Balb/c miceCytarabine: 30 mg/kg BIDApraglutide: 0.11 to 1.1 mg/kg
* Significant difference relative to vehicle only control animals
# Significant difference relative to the cytarabine/vehicle-treated animals

R&D Day
VectivBio GvHD ProgramPhase II dose-finding study in patients with steroid-refractory acute GvHD on best available therapy
*best available therapy defined as glucocorticoids and ruxolitinib
60
First patient dosed Q1 2022 Interim data Q4 2022
Dose level 1
Dose level 2
Apraglutide
up to 90 days treatment
External control
Study Objectives
Safety and Tolerability; PK; Response at days 28, 56, 90 and 180• Double-blind externally-
controlled dose-dose
finding study
• Patients aged 12 years
and older
• Steroid-refractory acute
GI-GvHD
• on best available therapy*
Follow up to 2 years

CoMETInherited Metabolic Diseases
Omar Khwaja, M.D., Ph.D.Chief Medical Officer

R&D Day
• Genetic loss of key enzymes required for cellular metabolism
• Failure of energy production and accumulation of toxic metabolites
• 1 in 800 births
• Diagnosed in infancy
• Recurrent metabolic crises
• Coma and high risk of death
• Progressive organ damage
• Brain
• Heart
• Kidney
• Liver
• Impaired growth and severe neurodevelopmental delay
Inherited Metabolic Diseases Are Severe, Life-threatening Genetic DisordersEnzymatic defects result in common pathophysiology and clinical presentation
Yang, L., Guo, B., Li, X. et al. Brain MRI features of methylmalonic acidemia in children: the relationship between neuropsychological scores and MRI findings. Sci Rep 10, 13099 (2020).
Inherited Metabolic Diseases (IMDs)
Clinical Presentation
• No approved treatments
• Intensive care, supportive and dietary management, liver or kidney transplant in selected cases
62

R&D Day
IMDs Fall into Groups that Share Common Affected Pathways Enzyme deficits impair substrate metabolism and coenzyme A (CoA) functionality,
with widespread downstream impact
OTC: ornithine transcarbamylase
MCAD: medium chain Acyl-CoA dehydrogenase
PK: pyruvate kinase
63

R&D Day
Intracellular Delivery of Stabilized Pantetheine with CargoCargo addresses deficiency in specific cluster of metabolic disorders such as MMA and PA
Provide key intermediates to Kreb’s cycle and
fuel energy production
Prevent compensatory
catabolism
Provide CoA for multiple essential
metabolic pathways
Restore correct processing and
avoid build up of toxic metabolites
3
4
Cargo
Pantetheine/Free CoA
Cargo-CoA
Pantetheine + Cargo
1
2
64
R&D Day
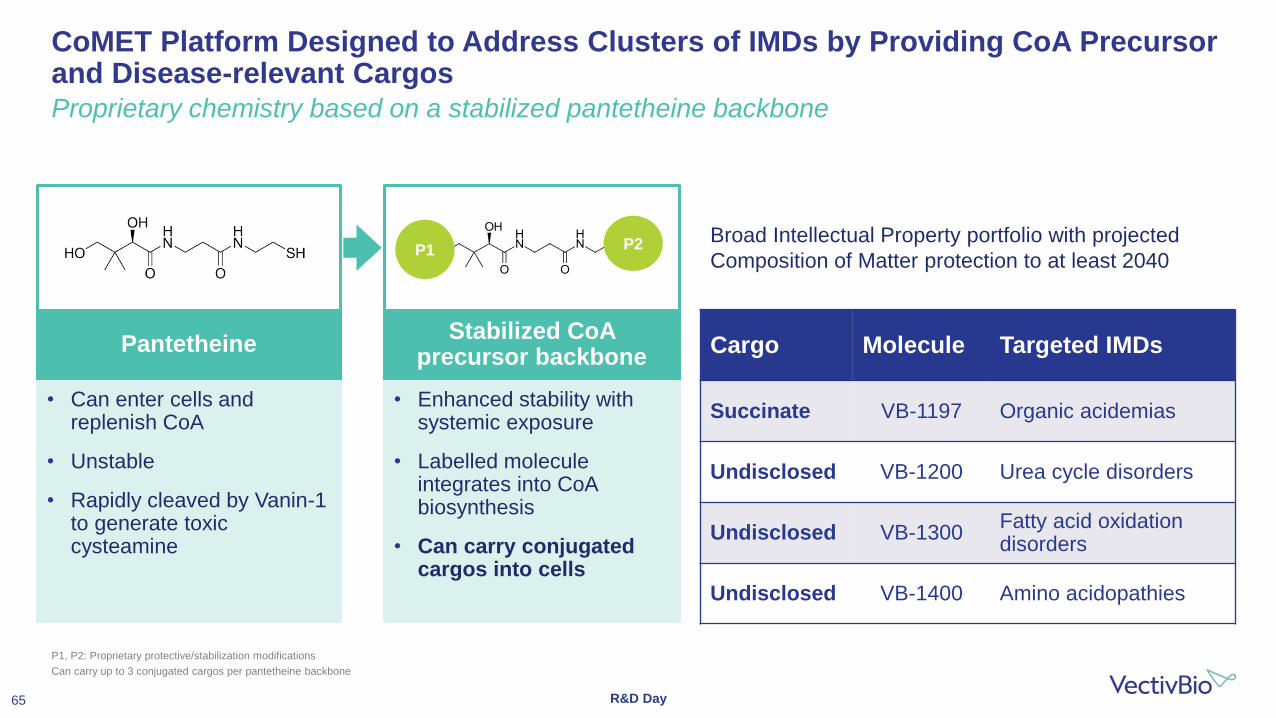
• Can enter cells and replenish CoA
• Unstable
• Rapidly cleaved by Vanin-1 to generate toxic cysteamine
• Enhanced stability with systemic exposure
• Labelled molecule integrates into CoA biosynthesis
• Can carry conjugated cargos into cells
CoMET Platform Designed to Address Clusters of IMDs by Providing CoA Precursor and Disease-relevant CargosProprietary chemistry based on a stabilized pantetheine backbone
P1, P2: Proprietary protective/stabilization modifications
Can carry up to 3 conjugated cargos per pantetheine backbone
PantetheineStabilized CoA
precursor backboneCargo Molecule Targeted IMDs
Succinate VB-1197 Organic acidemias
Undisclosed VB-1200 Urea cycle disorders
Undisclosed VB-1300Fatty acid oxidation disorders
Undisclosed VB-1400 Amino acidopathies
P1 P2 Broad Intellectual Property portfolio with projected
Composition of Matter protection to at least 2040
65

R&D Day
Methylmalonic and Propionic Acidemia are IMDs with Very High Unmet NeedInherited, life-threatening or fatal disorders of branched chain amino acid metabolism
66
Reduced Succinyl-CoA production
impairs Kreb’s cycle function
Reduced Acetyl-CoA impairs metabolic
flux
Toxic organic acid build upCompensatory GABA and glutamine
catabolism impairs CNS function
• Prevalence 15 in 100,000 newborns
• Infantile form:
• fulminant metabolic acidosis
• hyperammonemia,
• liver and bone marrow failure
• encephalopathy and coma
• Chronic intermittent form:
• recurrent life-threatening crises
• developmental delay,
• neurocognitive impairment
• impaired growth
• kidney failure
• Mortality of 40% before age 18 years
• Major disability in adult survivors
• Treatment supportive, strict dietary management, liver and kidney
transplantation
MMA and PA
1
2
2
3
4
4
1
2
3
4

R&D Day
Simple primary screen can identify compounds capable of restoring metabolic processesAssay measures increase in cellular respiration in disease-relevant patient fibroblasts
Source: Data on file. VectivBio. Basil, Switzerland.
Patient derived fibroblast cells (1. Methylmalonic acidemia; 2. Propionic acidemia; 3. Glutaric aciduria type 1) were treated with 10 uM of VB compounds and assayed using the Seahorse XF assay protocol
Respiration in MMA Patient
Fibroblasts1
Strong Potentiation of Cellular Respiration Across Patient Cells from Multiple Organic Acidemias
67
R&D Day
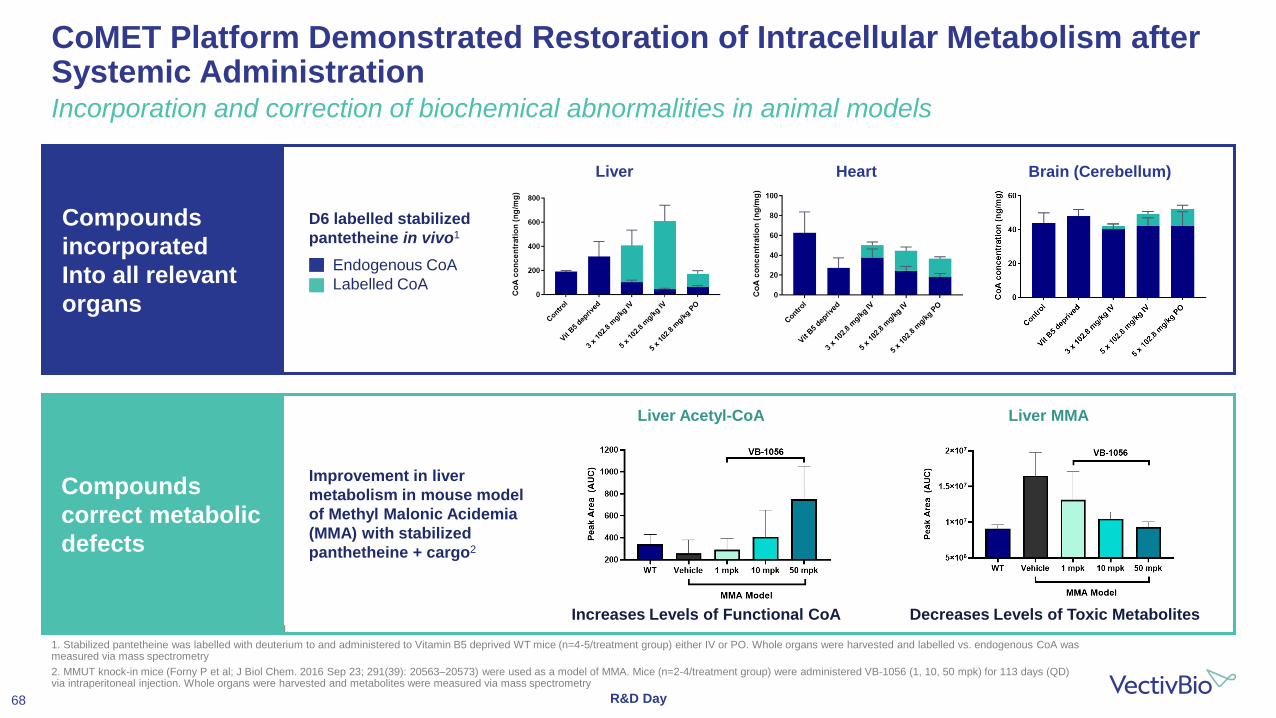
CoMET Platform Demonstrated Restoration of Intracellular Metabolism after Systemic Administration Incorporation and correction of biochemical abnormalities in animal models
Source: Data on file. VectivBio. Basil, Switzerland.
1. Stabilized pantetheine was labelled with deuterium to and administered to Vitamin B5 deprived WT mice (n=4-5/treatment group) either IV or PO. Whole organs were harvested and labelled vs. endogenous CoA was measured via mass spectrometry
2. MMUT knock-in mice (Forny P et al; J Biol Chem. 2016 Sep 23; 291(39): 20563–20573) were used as a model of MMA. Mice (n=2-4/treatment group) were administered VB-1056 (1, 10, 50 mpk) for 113 days (QD) via intraperitoneal injection. Whole organs were harvested and metabolites were measured via mass spectrometry
D6 labelled stabilized
pantetheine in vivo1
Endogenous CoA
Labelled CoA
Improvement in liver
metabolism in mouse model
of Methyl Malonic Acidemia
(MMA) with stabilized
panthetheine + cargo2
Compounds
incorporated
Into all relevant
organs
Compounds
correct metabolic
defects
Increases Levels of Functional CoA Decreases Levels of Toxic Metabolites
Liver Acetyl-CoA Liver MMA
Liver Heart Brain (Cerebellum)
68

R&D Day
Addressing Unmet Needs of Patients Suffering from IMDsCoMET platform has potential to deliver effective systemic therapies for many patients
Desired Goal Organ Transplant Gene Therapy Vision for CoMETPlatform
Broad patient eligibility
Highly selected patients Specific to one genetic defectNo pre-existing immunity to vector
Efficacy across diseases with similar metabolic deficits
Systemic benefit Transplanted organ only Targeted tissues only Systemic efficacy
SafetyImmunosuppression, infection risk
Integration, immunogenicity Large therapeutic index
Sustained efficacy Lasting effect for life of organDuration of effect unknownImmunogenicity prevents re-use
Efficacy maintained by chronic oral or subcutaneous therapy
• Current management aims to manage and prevent metabolic crises through general supportive measures
and strict dietary control
• An ideal therapy would address intracellular metabolic defects in all tissues and for all patients
69

R&D Day
CoMET Platform Aims to Transform the Treatment of IMDsModular approach to address a broad range of severe metabolic disorders
a. Villani GR et al. Clin Exp Med. 2017 Aug;17(3):305-323; b. Brusilow SW, Horwich AL. Urea cycle enzymes. In: Scriver CR, Beaudet AL, Sly WS, Valle D (eds.). The Metabolic and Molecular Bases of Inherited Disease, 8th ed., New York: McGrawHill, 2001:1909–1963; c. Marsden D et al. Genet Med. 2021 May;23(5):816-829; d. Wasim M et al. Biochem Genet. 2018 Apr;56(1-2):7-21
Patients in US & EU
26,000a
26,000b
16,000c
8,000d
FIH Q1 2023
Discovery Preclinical Phase 1
Methyl Malonic and Propionic Acidemia
Other Organic Acidemias
Urea Cycle Disorders
Fatty Acid Oxidation Disorders
Amino Acidopathies
Molecule
VB-1197
VB-1200
VB-1300
VB-1400
Strong development synergies support a potentially transformative, fast-to-patient portfolio
• Modular platform to deliver series of molecules that each address multiple IMDs
• Common pathophysiology and clinical endpoints allow for umbrella and basket trials
• Diagnosis through newborn screening and supported by existing clinical guidelines
• Biochemical endpoints allow rapid biomarker-enabled drug development with small, seamless trials
• Patients treated at specialist metabolic medicine units with center-of-excellence model for delivery and care
70

Conclusion
Luca Santarelli, M.D.CEO & Founder

R&D Day
Building a Fully Integrated Global Rare Disease CompanyMultiple near-term catalysts
Transformative CoMET platform
Designed to address pre-
viously intractable IMDs
4 programs in research, plans to enter the clinic in 18 months
ExperiencedTeam
Apraglutide,a Compelling Phase 3 Asset
SBS-IF, an underserved >$2B market opportunity
Significant life-cycle potential starting with GVHD
Strong track record of success
2021 2022 2023
Key Catalysts
Adult SBS-IF:
-Phase 3 Start: Jan
-Phase 2 Start: Q2
CoMET
-Entry into human trials: Q1
Adult SBS-IF
-Phase 3 Top-Line Results: H2
Pediatric SBS-IF
-Trial Initiation: 2023
Adult SBS-IF CIC
-STARS Nutrition Results: H1
Acute GVHD
-Phase 2 Start: Q1
-Interim POC read out: H2
✓
✓
BD transaction-
achieved
72

VectivBio AGAeschenvorstadt 364051 [email protected]
Thank You
We are on a mission to build a leading, fully integrated global rare disease company using our patient-centric approach to
identify and develop transformative medicines for the treatment of severe rare diseases.