Use of the automatic stapler in urinary conduit diversions and pelvic exenterations
5
GYNECOLOGIC ONCOLOGY 10, 93-97 (1980) Use of the Automatic Stapler in Urinary Conduit Diversions and Pelvic Exenterations GREGORIO DELGADO, M.D. Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Vincent T. Lombardi Cancer Research Center, Georgetown University Medical Center, 3800 Reservoir Road, N. W., Washington, D.C. 2tWO7 Received October 3 1, 1978 Nine patients previously treated by pelvic irradiation underwent a urinary diversion procedure, four as part of total pelvic exenteration. The automatic surgical staplers used in these procedures, the gastrointestinal anastomosis device, and ligation and division stapler, greatly reduced operating time while preserving a better blood supply to the anastomotic site. The method of use and advantages of the autosuture instruments in urinary diversions are discussed. INTRODUCTION Since Bricker [ 1,2] and Barber and Bruschwig [3] described urinary diversion and pelvic exenteration, numerous modifications have been made to shorten operative time and improve results [4]. All of these operations require gastrointes- tinal anastomosis in areas in which the automatic surgical staple gun could be used safely to reduce operating time. Several reports of anastomosis of the gastrointestinal tract with the surgical stapling gun have indicated very good results [5]. These reports, which have been confined to the nonradiated bowel, emphasize shorter operating time, less trauma to the tissues, and less contamination of the abdominal cavity. Neither the use of the autosuture in the gastrointestinal tract following radiotherapy, nor its use in pelvic exenterations and ileal conduit diversion have been well documented [6]. There is great concern about the high rate of complications after surgery in the postradiated bowel resulting from radiation-induced changes in the bowel wall that make it heal very slowly and vulnerable to infection [7]. Following is a report of the experience of the Division of Gynecologic Oncology at the Georgetown University Medical Center in the use of the automatic staplers in urinary diversion and pelvic exenteration. The use of the Gastro-Intestinal Anastomosis Stapler’ (GIA) facilitates the transection and anastomosis of the bowel; in addition, the division of the bowel mesentery and the detachment of the omentum from the greater curvature of the stomach and transverse colon in pelvic exenterations is simplified by the use of the LDS.2 The use of the autosuture * Gastro-Intestinal Anastomosis Stapler manufactured by U.S. Surgical Corporation. ’ Ligation and division stapler (LDS) manufactured by U.S. Surgical Corporation. 93 0090-8258/80/040093-05$01.00/o Copyright @ 1980 by Academic Press, Inc. All rights of reproduction in any form reserved.
-
Upload
gregorio-delgado -
Category
Documents
-
view
212 -
download
0
Transcript of Use of the automatic stapler in urinary conduit diversions and pelvic exenterations

GYNECOLOGIC ONCOLOGY 10, 93-97 (1980)
Use of the Automatic Stapler in Urinary Conduit Diversions and Pelvic Exenterations
GREGORIO DELGADO, M.D. Department of Obstetrics and Gynecology, Division of Gynecologic Oncology,
Vincent T. Lombardi Cancer Research Center, Georgetown University Medical Center, 3800 Reservoir Road, N. W., Washington, D.C. 2tWO7
Received October 3 1, 1978
Nine patients previously treated by pelvic irradiation underwent a urinary diversion procedure, four as part of total pelvic exenteration. The automatic surgical staplers used in these procedures, the gastrointestinal anastomosis device, and ligation and division stapler, greatly reduced operating time while preserving a better blood supply to the anastomotic site. The method of use and advantages of the autosuture instruments in urinary diversions are discussed.
INTRODUCTION
Since Bricker [ 1,2] and Barber and Bruschwig [3] described urinary diversion and pelvic exenteration, numerous modifications have been made to shorten operative time and improve results [4]. All of these operations require gastrointes- tinal anastomosis in areas in which the automatic surgical staple gun could be used safely to reduce operating time.
Several reports of anastomosis of the gastrointestinal tract with the surgical stapling gun have indicated very good results [5]. These reports, which have been confined to the nonradiated bowel, emphasize shorter operating time, less trauma to the tissues, and less contamination of the abdominal cavity. Neither the use of the autosuture in the gastrointestinal tract following radiotherapy, nor its use in pelvic exenterations and ileal conduit diversion have been well documented [6].
There is great concern about the high rate of complications after surgery in the postradiated bowel resulting from radiation-induced changes in the bowel wall that make it heal very slowly and vulnerable to infection [7].
Following is a report of the experience of the Division of Gynecologic Oncology at the Georgetown University Medical Center in the use of the automatic staplers in urinary diversion and pelvic exenteration. The use of the Gastro-Intestinal Anastomosis Stapler’ (GIA) facilitates the transection and anastomosis of the bowel; in addition, the division of the bowel mesentery and the detachment of the omentum from the greater curvature of the stomach and transverse colon in pelvic exenterations is simplified by the use of the LDS.2 The use of the autosuture
* Gastro-Intestinal Anastomosis Stapler manufactured by U.S. Surgical Corporation. ’ Ligation and division stapler (LDS) manufactured by U.S. Surgical Corporation.
93 0090-8258/80/040093-05$01.00/o
Copyright @ 1980 by Academic Press, Inc. All rights of reproduction in any form reserved.

94 GREGORIO DELGADO
FIG. 1. A section of ileum is being transected by the CIA.
instruments, the TA-30, TA-55,3 and GIA, as well as the LDS, in different phases of the operative procedure as described by Johnson and Fuerst 181, takes consid- erably less time than conventional procedures.
SUBJECTS, METHODS AND RESULTS
The autosuture unit was used in nine patients who underwent urinary diversion in 1977-1978. Four of these patients also had pelvic exenterations as part of invasive cancer treatment. All patients had advanced gynecologic malignancies previously treated by external radiation and, in some cases, intracavitary radia- tion.
Of the nine patients who had urinary diversions, six had ileal conduits and three had sigmoid conduits. One of the patients with ileal diversion had a ureter-ileo- neo-cystotomy for obstruction of the ureter by postradiation fibrosis.
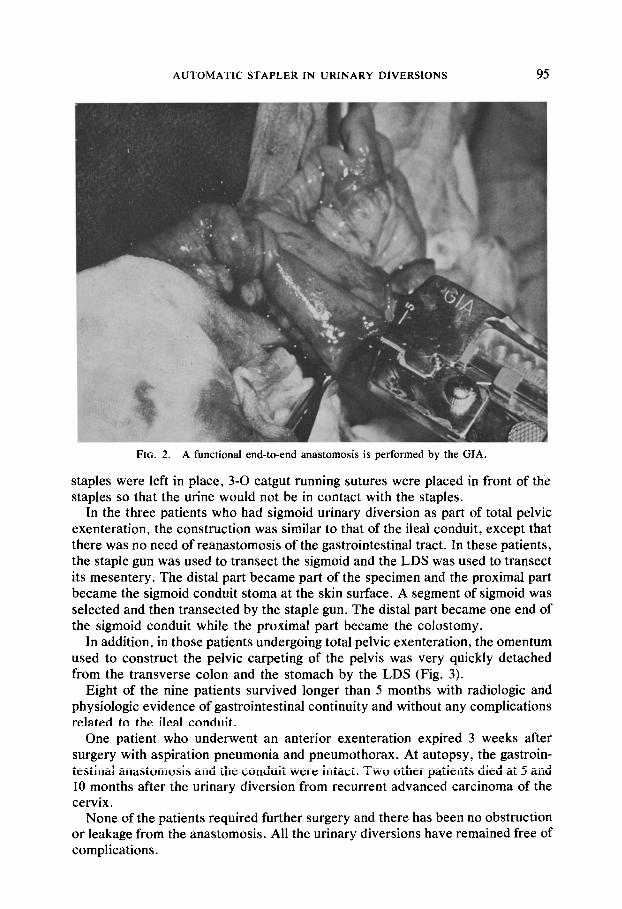
In these cases, the segment of ileum was transected in two separate places by the GIA (Fig. l), and the mesentery of the small bowel was then divided with the LDS, being sure that an adequate blood supply existed in the intestinal segment. A functional end-to-end anastomosis was performed with the GIA (Fig. 2) to estab- lish continuity in the gastrointestinal system using procedures previously de- scribed in other studies [5,8].
One of the ends of the intestinal segment was opened by removing the staples and it became the stoma at the skin surface. At the other end of the segment, where the
3 Thoraco-abdominal (TA) manufactured by U.S. Surgical Corporation.
AUTOMATIC STAPLER IN URINARY DIVERSIONS 95
FIG. 2. A functional end-to-end anastomosis is performed by the GIA.
staples were left in place, 3-O catgut running sutures were placed in front of the staples so that the urine would not be in contact with the staples.
In the three patients who had sigmoid urinary diversion as part of total pelvic exenteration, the construction was similar to that of the ileal conduit, except that there was no need of reanastomosis of the gastrointestinal tract. In these patients. the staple gun was used to transect the sigmoid and the LDS was used to transect its mesentery. The distal part became part of the specimen and the proximal part became the sigmoid conduit stoma at the skin surface. A segment of sigmoid was selected and then transected by the staple gun. The distal part became one end of the sigmoid conduit while the proximal part became the colostomy.
In addition, in those patients undergoing total pelvic exenteration, the omentum used to construct the pelvic carpeting of the pelvis was very quickly detached from the transverse colon and the stomach by the LDS (Fig. 3).
Eight of the nine patients survived longer than 5 months with radiologic and physiologic evidence of gastrointestinal continuity and without any complications related to the ileal conduit.
One patient who underwent an anterior exenteration expired 3 weeks after surgery with aspiration pneumonia and pneumothorax. At autopsy, the gastroin- testinal anastomosis and the conduit were intact. Two other patients died at 5 and 10 months after the urinary diversion from recurrent advanced carcinoma of the cervix.
None of the patients required further surgery and there has been no obstruction or leakage from the anastomosis. All the urinary diversions have remained free of complications.

% GREGORIO DELGADO
FIG. 3. The omentum is being detached from the greater curvature of the stomach by the LDS. Reprinted with the permission of United States Surgical Corporation, copyright United States Surgical Corporation, 1974, all rights reserved.
DISCUSSION
There are two major advantages of using autosuturing for the construction of ileal conduits and pelvic exenterations. First, the transection of the sigmoid colon, the construction of the sigmoid conduit, and the removal of the omentum from the greater curvature of the stomach and the transverse colon are rapidly performed, resulting in a great decrease in total operating time. Second, a better blood supply to the anastomotic site is preserved.
Although there have been reports of urinary tract calculi in urinary conduit diversion after using the staple gun for closure of the isolated loop [9], calculi have also been reported when the autosuture was not used [lo]. To lessen the probabil- ity of this complication, one layer of 3-O GI chromic sutures was placed in front of the closed end of the segment of bowel so that the urine would not be in contact with the steel staples. Thus far, no calculi have developed in the ileal conduit, nor have any problems developed in the gastrointestinal tract in any surviving patient. This suggests that the LDS and GIA are of great value even when patients have had previous radiation therapy, thus allowing an equally good if not better preser- vation of blood supply than the conventional anastomosis.
SUMMARY
Nine patients received urinary conduit diversions using the automatic staple gun for anastomosis. Four of these patients also underwent pelvic exenterations.

AUTOMATIC STAPLER IN URINARY DIVERSIONS 97
The advantages of shortened operative time and preservation of blood supply led to very good results despite previously radiated bowels.
REFERENCES 1. Bricker, E. M. Bladder substitution after pelvic exenteration, Surg. Clin. N. Amer. 30, 1511
(1950). 2. Bricker, E. M. The technique of ileal bladder substitution, inProgress in gynecology (J. V. Meigs,
Ed.), Grime & Stratton, New York, Vol. 3 (1957). 3. Barber, H. R. K., and Brunschwig, A. Results of the surgical treatment of recurrent cancer of the
cervix, in New concepts in gynecological oncology (G. C. Lewis, Jr., W. B. Wentz, and R. M. Jaffe, Eds.), Davis, Philadelphia, p. 145 (1966).
4. Rutledge, F. N. Pelvic exenteration, in Gynecufogic surgery: Errors, safeguards, salvages (J. H. Ridiey, Ed.), Williams & Wilkins, Baltimore, Chap. 9, pp. 278-2% (1974).
5. Ravitch, M. M., Ong, T. H., and Gazzola, L. A new, precise and rapid technique of intestinal resection and anastomosis with staples, Surg. Gynecol. Obstet. 139, 6-10 (1974).
6. United States Surgical Corporation. Stapling techniques in general surgery, United States Surgi- cal Corp. (1974).
7. Smith, J. P., Golden, P. E., and Rutledge, F. N. The surgical management of intestinal injuries following irradiation for carcinoma of the cervix, in Cancer of the uterus and ovary (Anderson Hospital), Year Book Med. Pub., Chicago, pp. 241-256 (1969).
8. Johnson, D. E., and Fuerst, D. E. Use of auto suture for construction of ileal conduits, J. Ural. 109, 821-823 (1973).
9. Assadnia, A., Lee, C. N., Petre, J. H., et al. Two cases of stone formation in ileal conduits after using staple gun for closure of proximal end of isolated loop, J. Ural. 108, 553 (1972).
10. Dretler, S. P. Urinary tract calculi and ileal conduit diversion,Amer. J. Surg. 123,480-483 (1972).