USE OF IGRAs IN THE FACE OF OTHER CO MORBIDITIES · PDF fileUSE OF IGRAs IN THE FACE OF OTHER...
17
USE OF IGRAs IN THE FACE OF OTHER CO‐MORBIDITIES CO MORBIDITIES Luca Richeldi MD PhD Section of Respiratory Disease, Center for Rare Lung Diseases University Hospital of Modena CO‐MORBIDITIES CO MORBIDITIES
Transcript of USE OF IGRAs IN THE FACE OF OTHER CO MORBIDITIES · PDF fileUSE OF IGRAs IN THE FACE OF OTHER...

USE OF IGRAs IN THE FACE OF OTHER CO‐MORBIDITIESCO MORBIDITIES
Luca Richeldi MD PhDSection of Respiratory Disease, Center for Rare Lung Diseases
University Hospital of Modena
CO‐MORBIDITIESCO MORBIDITIES

CO‐MORBIDITIES:WHY AND WHICH
1. May increase the risk of progression from latent infection to active disease
2. May interfere with IGRA performance
CR Horsburgh and EJ Rubin, N Engl J Med 2011; 364: 1441‐8

10
12
RISK FACTORS FOR INCREASED LIKELIHOOD OF PROGRESSIONFROM LATENT TUBERCULOSIS INFECTION TO ACTIVE DISEASE
2
4
6
8
RR (9
5% CI)
Based on CR Horsburgh and EJ Rubin, N Engl J Med 2011; 364: 1441‐8
0
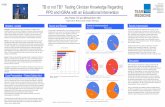
Negative and positive predictive value of a whole‐bloodinterferon‐γ release assay for developing active tuberculosisAn Update
3.1%
TST >5 mm: 604 (63.3%)
TB: 89.5% household contacts
TST+/QFT+: 191 (31.6% of TST+)
QFT /TST 7 (3 5% f QFT )
Diel R et al, Am J Respir Crit Care Med 2011; 83; 88‐95N=954
QFT‐IT >0.35: 198 (20.8%)
12.9%
QFT+/TST‐: 7 (3.5% of QFT+)

Prednisolone treatment affects the performance of the QuantiFERON Gold In‐Tube test and the tuberculin skin test in patients with autoimmune disorders screened for latent tuberculosis infection.
• Prednisolone treatment is significantly associatedwith both reduced response to mitogen in QFT‐IT (p<0.001) and a negative TST result (p=0.01)
Bélard E et al, Inflamm Bowel Dis 2011; 17: 2340‐9
• No effect of other immunosuppressive drugs
N=248
KIDNEY DISEASE DEATHSKIDNEY DISEASE DEATHS
www.worldmapper.org

Validity of interferon‐γ‐release assays for the diagnosis of latent tuberculosis in haemodialysis patients.
Indeterminate results were higher with
Low LTBI risk High LTBI risk
QFT‐IT 41.2% 62.5%
TS TB 58 9% 65 7%
Indeterminate results were higher with QFT‐IT (12.6%) than with TS.TB (4.8%)
Chung WK et al, Clin Microbiol Infect 2010; 16: 960‐5
TS.TB 58.9% 65.7%
N=167
Serial testing of interferon‐gamma‐release assays for the diagnosis of latent tuberculosis in hemodialysis patients.
High LTBI risk Low LTBI risk
QFT‐IT conversion 2.0
TS.TB conversion 7.8
QFT‐IT reversion 18.9
TS TB reversion 6 2
Chung WK et al, J Infect 2010; 61: 144‐9
TS.TB reversion 6.2
N=98
Odds Ratio values
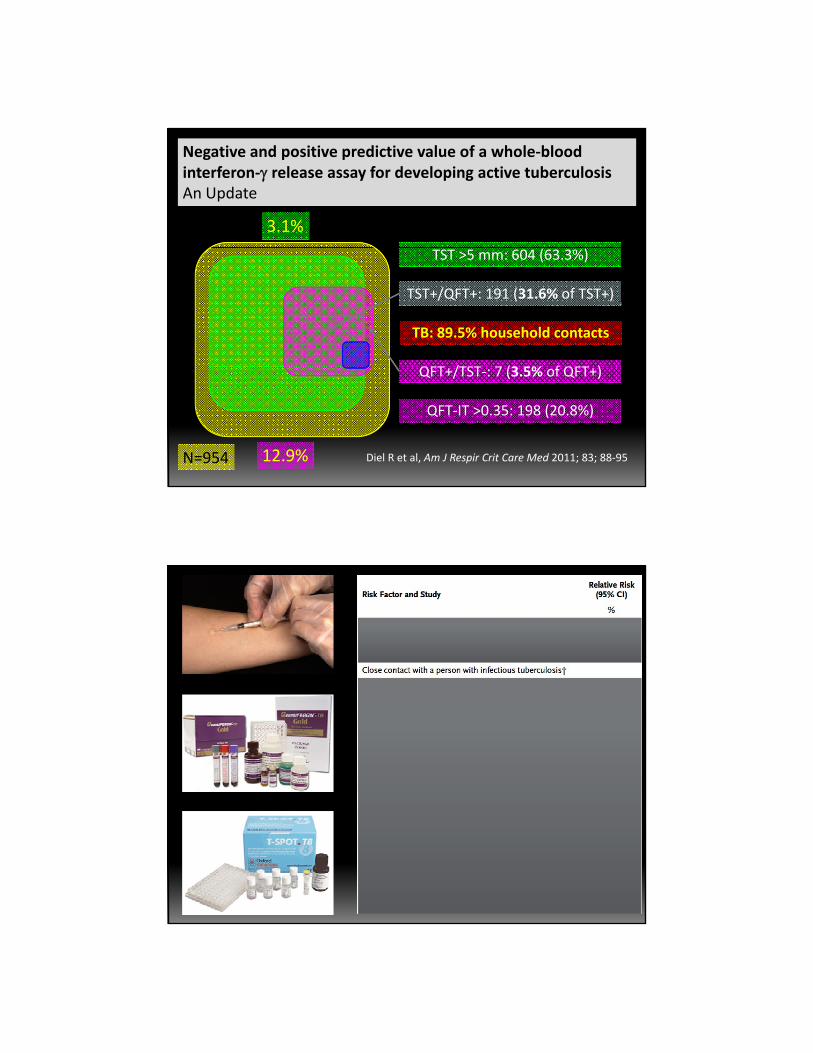
High prevalence of latent tuberculosis infection in dialysis patients using the interferon‐γ release assay and tuberculin skin test.
34.4% positive QFT‐IT, 53.9% positive TST
Lee S S‐Y et al, Clin J Am Soc Nephrol 2010; 5: 1451‐7N=93
No influence of haemodialysis on interferon production in the QuantiFERON‐TB Gold‐In‐Tube test.
No statistically significant differences in interferon‐gamma production in the nil‐ and antigen tubes between pre‐HD, during and after HD.
Hoogewerf M et al, J Nephrol 2011; 24: 625‐30N=20
RHEUMATOID ARTHRITIS DEATHSRHEUMATOID ARTHRITIS DEATHS
www.worldmapper.org
Detection of latent tuberculosis in immunosuppressed patients with autoimmune diseases: performance of a Mycobacterium tuberculosis antigen‐specific interferon gamma assay.
• QFT‐IT more closely associated with LTBI risk factors than TST
• Corticosteroids or DMARDs did not affect IFN‐γlevels
Matulis G et al, Ann Rheum Dis 2008; 67: 84‐90N=142
• Odds of a positive QFT‐IT decreased in patients treated with anti‐TNF‐α drugs

DIABETES DEATHSDIABETES DEATHS
www.worldmapper.org
Sensitivity of Interferon‐γ release assays is not compromised in tuberculosis patients with diabetes.
Active TB patients with concomitant
Positive TB cases
QFT‐IT 70.4%
TS TB 93 0%
diabetes in about half of cases
Walsh MC et al, Int J Tuberc Lung Dis 2011; 15: 179N=169 (QFT), 43 (TS.TB)
TS.TB 93.0%

MALIGNANCIES MAY CAUSE FALSE NEGATIVE TST RESULTS
• Positive RD1‐ELISpot in a TST‐negative patient with hairy cell leukemia and disseminated active tuberculosisleukemia and disseminated active tuberculosis.
Leukemia 2006
Interferon‐gamma release assays for the detection of Mycobacterium tuberculosis infection in children with cancer.
17 6% iti ith ith t t17.6% positive with either test
Positive Indeterminate
TST 8.8% ‐
QFT‐IT 8 8% 14 7%
Stefan DC et al, Int J Tuberc Lung Dis 2010; 14: 689‐94 N=34
QFT‐IT 8.8% 14.7%
TS.TB 17.6% 11.8% (+ 17.6%)
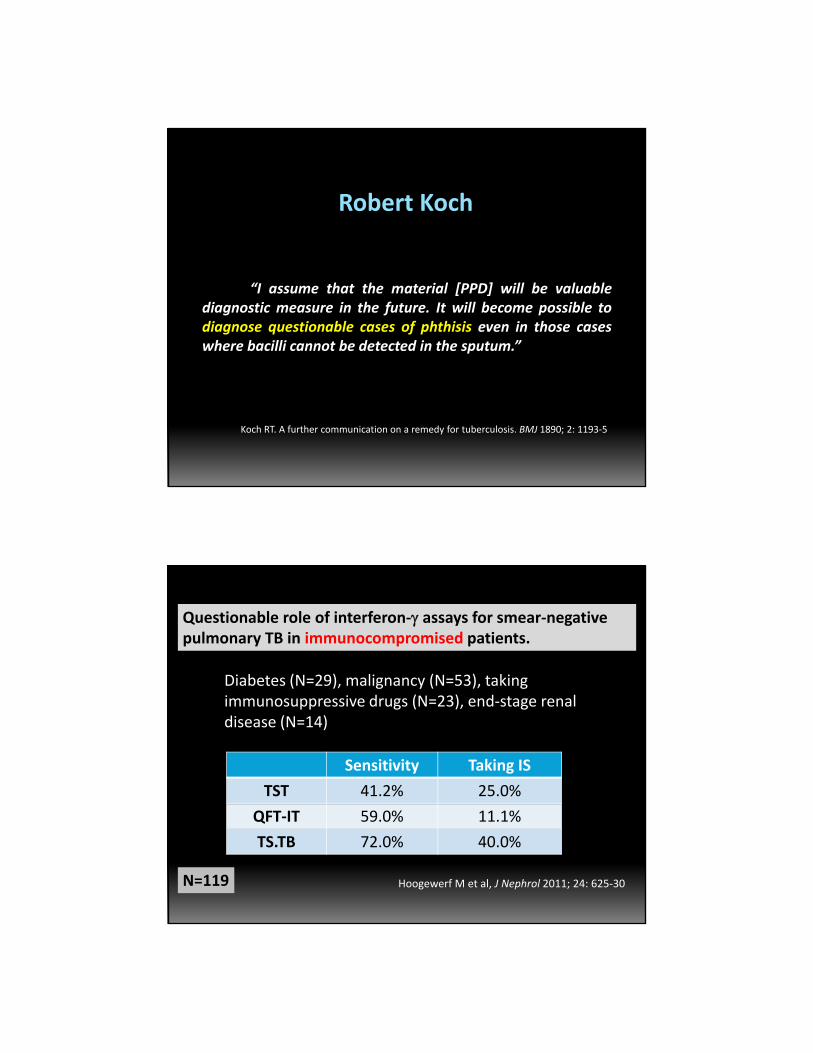
Robert Koch
“I assume that the material [PPD] will be valuablediagnostic measure in the future. It will become possible todiagnose questionable cases of phthisis even in those caseswhere bacilli cannot be detected in the sputum.”
Koch RT. A further communication on a remedy for tuberculosis. BMJ 1890; 2: 1193‐5
Questionable role of interferon‐γ assays for smear‐negative pulmonary TB in immunocompromised patients.
Diabetes (N=29), malignancy (N=53), takingDiabetes (N 29), malignancy (N 53), taking immunosuppressive drugs (N=23), end‐stage renal disease (N=14)
Sensitivity Taking IS
TST 41.2% 25.0%
Hoogewerf M et al, J Nephrol 2011; 24: 625‐30N=119
QFT‐IT 59.0% 11.1%
TS.TB 72.0% 40.0%

False‐negative IGRA In Active Tuberculosis:The FIAT 500 Study.
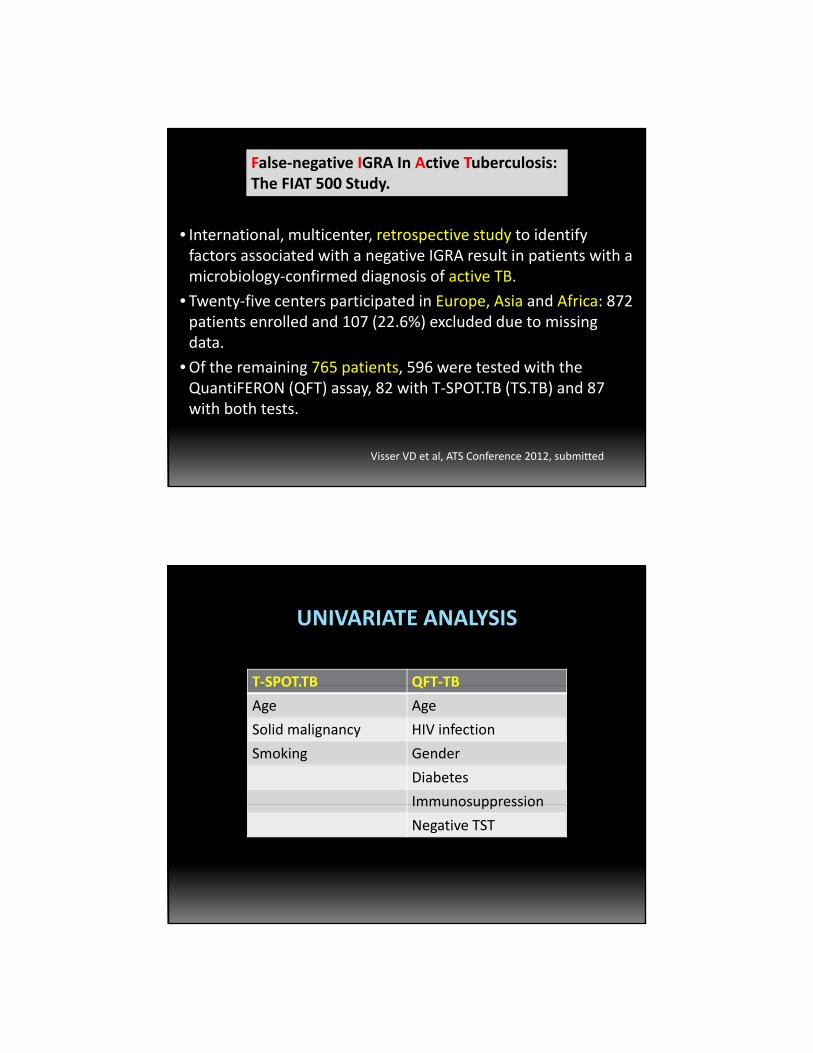
• International, multicenter, retrospective study to identify
False‐negative IGRA In Active Tuberculosis:The FIAT 500 Study.
factors associated with a negative IGRA result in patients with a microbiology‐confirmed diagnosis of active TB.
• Twenty‐five centers participated in Europe, Asia and Africa: 872patients enrolled and 107 (22.6%) excluded due to missing data.
•Of the remaining 765 patients 596 were tested with the•Of the remaining 765 patients, 596 were tested with the QuantiFERON (QFT) assay, 82 with T‐SPOT.TB (TS.TB) and 87 with both tests.
Visser VD et al, ATS Conference 2012, submitted
T‐SPOT.TB QFT‐TB
UNIVARIATE ANALYSIS
T SPOT.TB QFT TB
Age Age
Solid malignancy HIV infection
Smoking Gender
Diabetes
ImmunosuppressionImmunosuppression
Negative TST

T‐SPOT.TB QFT‐TB
UNIVARIATE ANALYSIS
T SPOT.TB QFT TB
Age Age
Solid malignancy HIV infection
Smoking Gender
Diabetes
ImmunosuppressionImmunosuppression
Negative TST

NUTRITIONAL DEFICIENCES DEATHSNUTRITIONAL DEFICIENCES DEATHS
www.worldmapper.org
CO‐MORBIDITIES:WHY AND WHICH
1. May increase the risk of progression from latent infection to active disease
Solid organ transplantation
Chronic disorders in elderly patients (e.g. role of inhaled steroids in COPD)
“Targeted” therapies in cancer and non‐cancer disorders
2. May interfere with IGRA performance

IDIOPATHIC PULMONARY FIBROSIS
Novel agents in IPF clinical trials
Product Company MOA StatusProduct Company MOA StatusBIBF 1120 Boehringer Ingelheim Tyrosine kinase inhibitor Phase III
QAX 576 Novartis Anti‐IL13 monoclonal antibody Phase II
Macitentan Actelion Endothelin receptor antagonist Phase II
CNTO 888 Centocor Anti‐CCL‐2 monoclonal antibody Phase II
FG‐3019 Fibrogen Anti‐CTGF monoclonal antibody Phase II
STX‐100 Stromedix Anti‐avb6 integrin antibody Phase II
CC‐930 Celgene Jun‐kinase inhibitor Phase II
www.clinicaltrials.gov

USE OF IGRAs IN THE FACE OF OTHER CO‐MORBIDITIESCO MORBIDITIES
Luca Richeldi MD PhDSection of Respiratory Disease, Center for Rare Lung Diseases
University Hospital of Modena