Urinary System-1
86
Urinary System
-
Upload
greatmoosa -
Category
Documents
-
view
4.733 -
download
5
Transcript of Urinary System-1

Urinary System

2
Components of Urinary System

3
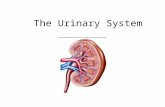
Longitudinal Section of a Kidney

4
Blood Supply of the Kidney
• Although weight of both the kidneys is less than 1% of the total body weight their blood supply is 21% of the Cardiac Output (CO).
• On the average it is 1200 ml / min which is equivalent to 22.8% of CO.
• Plasma flow is 650 ml / min• G.F.R is 125 ml / min.
• Filtration fraction = GFR / Renal plasma flow = 0.2 or 20%.

5
Functions of the kidney
• Homeostatic Function
• Excretory Function
• Endocrine Function
• Synthetic function

6
Homeostatic Function
• This function is essential for survival and normal functioning of the cells of the body.
• It is achieved by:– Regulation of Water Balance– Regulation of Electrolyte Balance– Regulation of Osmolarity– Regulation of Salt and Water Balance which
ultimately regulates ECF volume and BP– Regulation of pH of body fluids.

7
Excretory Function
• Kidneys excrete metabolic end products like urea, uric acid and creatinine, which if accumulate in the body are toxic to the brain.
• They also excrete foreign compounds like drugs, food additives, pesticides and other exogenous non nutritive material that have gained entrance to the body.

8
Endocrine &Synthetic Function
• Kidneys synthesize following hormones– Erythropoietin– Renin ( An enzymatic hormone )– Activation of Vitamin D– Kinins
• Kidneys can also synthesize glucose from amino acids and other precursors during prolong fasting. However it is the hormonal and liver mechanism which regulates the blood glucose level and not the kidneys

9
Functional Units of the Kidney
• Nephrons are the microscopic functional units of the kidney. Each kidney contains more than 1 million nephrons. Once they are destroyed they can not be regenerated so their number decreases with aging process. Each nephron has two major parts which are Vascular part (Glomerulus) and Tubular part
• Tubular part is composed of – Proximal convoluted tubule (PCT)– Loop of Henle (LH)– Distal Convoluted tubule (DCT)– Collecting Tubules (CT)

10
Types of Nephrons
Cortical Juxtamedullary
80% in Number 20% in Number
Located in the outer
part of Cortex
Located in the Inner part of Cortex
Have Shorter Loop of Henle Have Longer Loop of Henle
Have Peritubular Capillary Network around them
Have Vasa recta around them

11
Glomerulus
• Glomerular filtrate is protein free plasma which is filtered across glomerular capillary membrane in a unit time.

12
Structure of Glumerular Capillary Membrane

13
Structure of Glumerular Capillary Membrane…
• Substances having diameter more than 8nm can not pass.
• Permeability of Glomerular membrane is 100 times greater than that of systemic capillaries because their capillary hydrostatic pressure and Kf is more.

14
Histological Structure of the Tubules

15
General Functions of Tubules
• In the PCT there is uncontrolled re-absorption or secretion of substances.
• LH establishes vertical osmotic gradient in the renal medulla to enable the kidneys to produce urine of varying concentration.
• DCT and CT provide controlled (hormonal) re-absorption of Na+ and water and controlled secretion of K+ and H+.

16
Glomerular Filtration Rate (GFR)
• It is the amount of plasma which is filtered in glomeruli of both the kidneys per minute.
• Glomerular filtrate is the result of three passive physical forces of the body.– Glomerular Capillary Hydrostatic Pressure (60 mmHg)– Glomerular Capillary Osmotic Pressure (32 mmHg)– Bowman’s Capsule Hydrostatic Pressure (18 mmHg)
• Net filtration pressure = 60 – (32 + 18) = 10 mmHg• As compared to other capillaries glomerular filtrate is
formed through out the length of a capillary.

17
Determinants of GFR
• GFR = Kf * Net Filtration Pressure
• In the past it was considered that filtration coefficient (Kf ) remains constant and changes only under pathological states like uncontrolled diabetes mellitus and hypertension in which thickness of this membrane is increased.

18
Determinants of GFR…
• Recent view is that mesangial cells in between Glumerular capillaries and podocytes have actin filaments which when contract or relax Kf is changed and hence GFR.
• Kf is the product of Surface Area and Permeability of the membrane

19
Net Filtration Pressure
• It is affected by – Glomerular Capillary Hydrostatic pressure– Glomerular Capillary Osmotic pressure– Bowman’s Capsule Hydrostatic pressure
• The first one is responsible for spontaneous and day to day regulation of GFR where as last two factors are affect the GFR in the pathological states.

20
Net Filtration Pressure...
• GCO pressure is decreased in nephrotic syndrome and severe burns.
• BCH pressure is increased by a renal stone and enlarged prostate.

21
Glomerular Capillary Hydrostatic Pressure
• It is the major outward force which is affected by – Blood Flow – Arterial Blood Pressure– Afferent arteriolar resistance – Sympathetic activity– Effect of hormones

22
Afferent arteriolar resistance
• It is affected by auto regulation or intrinsic mechanism aimed at spontaneous regulation of GFR despite rapid changes in blood pressure.
• Sympathetic stimulation or extrinsic mechanism aimed at long term regulation of BP.
• Auto regulation is the function of Juxtaglomerular apparatus.

23
Juxtaglomerular Apparatus

24
Function of JG Apparatus
• Secretes Renin in response to decrease in ECF volume, plasma volume, blood pressure and sodium.
• Regulates Renal blood flow and GFR by secreting vasoactive substances through auto regulation.
• Auto regulation means regulation of GFR despite rapid changes in BP from 80-180 mmHg.
• There are two mechanisms for auto regulation of GFR– Myogenic Mechanism– Tubulo Glomerular feedback mechanism

25
Tubulo Glomerular Feedback Mechanism

26
Hormones Affecting GFR
• Nor epinephrine decreases GFR• Epinephrine decreases GFR• Endothelin decreases GFR• Angiotensin-2 prevents decrease in GFR• Endothelial derived Nitric Oxide increases GFR• Prostaglandins increase GFR

27
Formation of Urine
• Urine is formed by three processes– Filtration – Reabsorption– Secretion

28
Re-absorption
• It is highly selective and variable for example – 100% of filtered glucose– 99.5% of filtered Salt– 99% of filtered water– 50% of filtered urea
• Tubular reabsorption involves trans epithelial transport in which there are 5 steps.

29
Re-absorption…
• Re-absorption may be passive or active.• In Passive Transport no ATP is involved and it occurs
down the electro chemical gradient or Osmotic gradient.
• In Active Transport ATP is involved may be in 1 out of 5 steps. It occurs against the concentration gradient.
• Among the substances which are actively re-absorbed include glucose, amino acids and other organic nutrients. In addition Na+ and other electrolytes like PO4
3-.

30
Re-absorption of Sodium Ions
• It is absorbed by active process occurring at basolateral surfaces of Tubular Epithelial Cells.
• 80% of the energy required for kidney is utilized for Na+
transport.• 67% Na+ is reabsorbed through PCT which is important
for re-absorption of glucose, AA, water, Chloride ions and urea.
• 25% Na+ is re-absorbed through LH which along with chloride ions re-absorption provides vertical osmotic gradient.

31
Re-absorption of Sodium Ions…
• 8% Na+ is reabsorbed through distal tubules which is controlled by Aldosterone hormone and ANP.
• Aldosterone is secreted from Adrenal Cortex through Renin Angiotensin Aldosterone mechanism when there is decrease in sodium level or there is decrease in ECF volume or plasma volume or blood pressure.
• Aldosterone secretion is also released if there is excess of potassium ions in the plasma.
• Aldosterone increases re-absorption of Salt and Water through Distal Tubules hence increases extra cellular fluid volume and pressure.

32
Release of Renin

33
Re-absorption of Sodium Ions…
• In the complete absence of aldosterone 20 grams of the salt may be lost in the urine per day.
• With maximum aldosterone secretion all filtered salt will be re-absorbed.
• In spite of wide variations in the intake of salt or its loss the system maintains normal sodium chloride concentration in the plasma.
• Some cases of hypertension are due to abnormal increase in Renin Angiotensin Aldosterone activity

34
Re-absorption of Sodium Ions…
• This system is also responsible for fluid retention and edema accompanying congestive heart failure in which CO and BP is decreased in spite of normal or increased plasma volume.

35
Treatment of CHF
• Low salt diet• Use of diuretics which are therapeutic agents to
cause diuresis and help to reduce excess ECF volume.
• ACE inhibitors can be useful in CHF and some cases of hypertension.

36
ANP and its Action

37
Re-absorption of Glucose & Amino Acids
• Glucose and AA are reabsorbed by secondary active transport through PCT.
• With the exception of sodium ions active re-absorption of substances exhibits tubular transport maximum (Tm) because carrier protein is specific for each substance and is a rate limiting factor.

38
Tm of Glucose• Normal plasma concentration of Glucose is 100 mg per
100ml.• It is freely filtered in the Bowman’s capsule in the same
concentration as in plasma.• As GFR is 125 ml / min so filtered load of glucose will be
125mg / min.• If plasma concentration is 200 mg the filtered load of
glucose will be 250 mg / min.• Tm of glucose is 375 mg / min(males) &
300mg/min(females)• Renal threshold of glucose is 200 mg / 100 ml

39
Tm of Glucose…
• Renal threshold is the plasma concentration of a substance at which Tm of a substance is reached and the substance first starts spilling in the urine.
• Example If plasma concentration of glucose is 400 mg / 100 ml the filtered load will be 500 mg / min. As Tm is 375 mg / min, 125 mg/min glucose will be lost in the urine.

40
Urinary System-II

41
Calcium and Phosphate Re-absorption
• Kidneys directly contribute to the regulation of plasma concentration of Calcium and Phosphate because renal threshold of these inorganic ions is equal to their normal plasma concentration.
• Generally our diet is rich in phosphate ions so excess of these ions are excreted in the urine.
• Re-absorption of calcium and phosphate is also regulated by Parathyroid Hormone which can alter renal threshold of calcium and phosphate depending on the momentary needs of the body.

42
Re-absorption of Chloride Ions
• Chloride ions are re-absorbed passively secondary to active re-absorption of sodium ions.

43
Re-absorption of Water
• Obligatory Water Re-absorption– It is uncontrolled, but constant 65% re-absorption
of water from PCT and 15% from descending limb of Loop of Henle by osmosis after re-absorption of salt.
• Facultative Water Re-absorption– It is Hormone controlled variable re-absorption
(20%) from Distal Tubules and Collecting Tubules.– Vasopressin Hormone is responsible for this re-
absorption which opens water channels at the luminal surface of Renal Tubular cells.

44
Urea Re-absorption
• 50% of filtered load of urea is reabsorbed in the terminal part of PCT by the process of osmosis.
• In the early part of collecting ducts only water is re-absorbed under the effect of vasopressin.
• In the distal half of CD urea is concentrated and in presence of vasopressin is re-absorbed into interstitium by osmosis where it contributes to medullary hyperosmolarity.
• Uremia means increase in blood urea level.• In renal failure BUN is estimated to assess renal
function.

45
Hydrogen Ions Secretion
• Hydrogen ions are secreted by secondary active transport in the PCT.
• They are secreted by primary active transport in the DT and CT according to hydrogen ion status of the body.

46
Potassium Ions Re-absorption & Secretion

47
Potassium Ions Re-absorption & Secretion…
• 67% Potassium ions are re-absorbed actively from PCT in uncontrolled manner.
• In the DCT and CT potassium ions are secreted by primary active transport at basolateral surface under the affect of Aldosterone.
• Normally 10-15% of filtered load of potassium ions are excreted in the urine.
• Normally K+ are secreted more than H+ but in acidosis more H+ are secrete and more K+ are retained.

48
Dual Control of Aldosterone Secretion

49
Effects of Plasma K+ Ions Concentration
• Hyperkalemia causes hypopolarization change in the membranes hence increasing excitability especially in the cardiac muscle leading to increased heart rate and fatal arrhythmias
• Hypokalemia leads to hyperpolarization and decreased excitability in the nerve and muscle cell membranes manifested as muscular weakness, distention of abdomen due to smooth muscle dysfunction, arrhythmias and decreased impulse conduction.

50
Plasma Clearance• Plasma clearance of a substance is the volume of the
plasma that is completely cleared of that substance by the kidneys per minute. It can be calculated by following formula
Clearance Rate of a Substance in ml/min =
(Concentration of the substance in urine mg/ml * Urine flow rate ml/min)
Plasma concentration of that substance g/ml
• It is different for different substances.• If a substance is filtered but not re-absorbed or secreted
then its clearance rate is equal to GFR.

51
Inulin Clearance
• It is harmless foreign carbohydrate which is filtered freely but it is neither re-absorbed nor secreted so its clearance is used to measure GFR.
• Its normal value is 125 ml/min• Although this method is accurate and straight forward
but it is not convenient to infuse it continuously through out the determination to maintain constant plasma concentration.

52
Creatinine Clearance
• Clinically plasma clearance of an endogenous substance like creatinine is used to calculate GFR.
• Creatinine is end product of muscle metabolism produces at relatively constant rate.
• It is freely filtered, not reabsorbed but slightly secreted so its clearance is slightly more than the normal.

53
Urea Clearance
• It a substance is freely filtered and reabsorbed but not secreted then its clearance rate will be less than normal.
• Glucose Clearance is zero which means all filtered load of glucose is re-absorbed.
• Urea clearance is 62.5 ml/min because 50% of filtered laod of urea is re-absorbed

54
PAH Clearance
• PAH is a foreign substance which is filtered and completely secreted by peritubular capillary network into the tubules but it is not re-absorbed.
• PAH clearance is used to measure renal plasma flow.• Its clearance is 625 ml/min which is equal to renal
plasma flow.• If we know inulin clearance and PAH clearance then
we can calculate filtration fraction.• FF = GFR/RPF = 20%

55
Renal handling of Plasma Water
• ECF osmolarity depends upon relative amount of solute to water.
• Isotonic: Normally body fluids are said to be isotonic if they have osmolarity of 300 mOsm/L.
• Hypertonic: If osmolarity > 300 mOsm/L• Hypotonic: If osmolarity < 300 mOsm/L• When the body is in ideal fluid balance then 1 ml/min of
isotonic urine is produced.

56
Renal handling of Plasma Water…
• When the body is over hydrated large volume of dilute urine is excreted (upto 25 ml/min having osmolarity of 100 mOsm / L) is produced.
• When the body is dehydrated less volume of concentrated urine is passed (0.3 ml/min having osmolarity of 1200 mOsm/L)

57
Mechanism of Dilution of Urine
• When the body is over hydrated and osmolarity of the body fluids is less than normal then vasopressin hormone will not be secreted.
• Dilute urine having osmolarity of 100 mOsm/L is passed

58
Mechanism of Dilution of Urine..

59
Mechanism of Concentration of Urine
• When the body is in a dehydrated state that is osmolarity of the body fluids is more than normal then small amount of concentrated urine is passed (1200 mOsm/L)
• For concentration of the urine it is essential that first of all hyperosmolarity of renal medullary interstitial is produced and then maintained.

60
Production of Hyper Osmolarity
• It is produced by following three factors– Counter current multiplier system of Loop of Henle– Secretion of Vasopressin – Urea recycling
• It is maintained by counter current exchange mechanism of vasa recta.

61
Counter Current Multiplier System

62
Vasopressin Mechanism

63
Vasopressin Mechanism…

64
Vasopressin Mechanism…
• Without vasopressin counter current multiplier system is useless and without osmotic gradient vasopressin mechanism is useless so the presence of both is essential to produce concentrated urine.
• When aldosterone is secreted salt is re-absorbed, this increases osmolarity which then causes secretion of vasopressin also to re-absorb water from DT.

65
Urea Recycling

66
Counter Current Exchange Mechanism

67
Water Diuresis
• Increased urinary output of water with little or no salt.– Too much ingestion of water– Alcohol ingestion: because it inhibits vasopressin
secretion. Typically more fluid is lost in urine than consumed in alcoholic beverages so body becomes dehydrated in spite of substantial fluid intake.

68
Osmotic Diuresis
• It is increased urinary output of water and solute caused by excess unabsorbed solute. For example presence of glucose in urine in diabetes mellitus .
• Some diuretics cause diuresis because they block re-absorption of a specific solute from the renal tubules which is then lost in urine along with water.

69
Urinary System-III

70
Buffer Systems of the Body
• Chemical Buffers• Respiratory Buffer • Renal Buffer System

71
H2CO3:HCO-3 Buffer System
• Most important buffer system of ECF for buffering pH changes.
• It is very effective in ECF for two reasons
– H2CO3 and HCO-3
are abundant in ECF and so readily available to resist changes in pH.
– Each component of this pair is closely regulated.
• For example kidneys regulate HCO-3
and respiratory system regulates CO2 which generates- H2CO3 .

72
H2CO3:HCO-3
Buffer System…
• When H+ are added from Lactic Acid during exercise into ECF then H2CO3:HCO-
3 buffer system, buffers it by
forming H2CO3 (weak acid).
• When OH- are added in the system by loosing HCl during vomiting, then water and bicarbonate are formed.
• OH-+ H2CO3 HCO-3 + H2O

73
H2CO3:HCO-3
Buffer System…
• The relationship between hydrogen ion concentration and members of a buffer pair can be expressed according to Henderson Hasselbalch equation which for bicarbonate buffer system is as follows: pH = pK + log [HCO-
3] / [H2CO3]
• The pK H2CO3 is always 6.1.
• Normally [ HCO-3
] : [CO2] =20 : 1
• pH = 6.1 + log [20/1] = 6.1 + 1.3 = 7.4

74
H2CO3:HCO-3
Buffer System…
• When this ratio is increased pH is increased.• The ratio can be increased either by increasing
bicarbonate ions conc. or by decreasing CO2.
• As bicarbonate ions conc. is regulated by kidneys and CO2 conc by lungs. Both these organs can correct changes in pH but can also induce changes in pH.

75
The protein Buffer System
• As proteins are plentiful in the ICF so it acts as a primary buffer system for ICF.
• Proteins are excellent buffers because they contain both acidic and basic groups that can give up or take up H+.

76
The Hemoglobin Buffer System
• This system buffers H+ generated from H2CO3 of CO2 origin as follows:
• From the tissues CO2 enters into the blood from where it enters into RBC’s. Inside RBC’s CO2 combines with water to form corbonic acid in presence of an enzyme carbonic anhydrase.
• Now carbonic acid dissociates to form H+ and HCO-3.
and H+ are buffered by combining with Hb to form HHb.

77
The Hemoglobin Buffer System…
• At the level of lungs HHb combines with oxygen and HbO2 and H+ are formed. Now HCO-
3 enter from plasma into RBC’s. Inside RBC’s, H+ combine with HCO-
3 to form H2CO3 .
• Next H2CO3 dissociates to form CO2 and water.
• CO2 is expelled out of the lungs.

78
Phosphate Buffer System• It is important urinary buffer system composed of
NaH2PO4 : Na2HPO4 .
• If H+ are added then these are buffered by forming NaH2PO4.
• Its concentration is low in ECF but rich in ICF.• Humans normally consume more phosphates than
needed so excess amount of phosphates is excreted in the urine where it buffers H+ secreted by renal tubules.
• Most or all of HCO-3 and CO2 filtered or re-absorbed
where as Hb and proteins are not even filtered.

79
Respiratory Buffer System
• It is called physical buffer system.• It is slow and acts as second line of defense against
pH changes.• Its action starts after few minutes.• When there is metabolic acidosis respiratory rate is
increased to get rid of more acids in the form of CO2.
• When there is metabolic alkalosis respiratory rate is decreased so that CO2 accumulates in the body.
• This system alone can return the pH to only 50-70% of the way towards normal.

80
Renal Buffer System• Kidneys are third line of defense. • It requires hours or days to compensate for the changes
in pH.• They are most potent pH regulators.• Not only H+ are secreted by kidney in variable amounts
but HCO-3 are also conserved or eliminated depending
upon acid-base status of the body.• If there is acidosis more acidic urine is passed.• If there is alkalosis then basic urine is passed.• It means during acidosis, H+ secretion is increased and
HCO-3 re-absorption is increased.

81
Renal Buffer System…
• During renal compensation for acidosis for each H+ excretion in urine, a new HCO-
3 is added to plasma.
• Kidneys remove H+ derived from non carbonic acid source.
• Urine is usually acidic having pH 6.0.• The H+ which are secreted are not passed in the urine as
free H+. First they are buffered with HCO-3,,phosphates
and ammonia.

82
Acid Base Imbalance
• It can arise either by respiratory dysfunction or metabolic dysfunction so there may be respiratory acidosis, respiratory alkalosis, metabolic acidosis or metabolic alkalosis.

83
Causes of Respiratory Acidosis
• It occurs due to hypo ventilation caused by – Destruction of respiratory center– Respiratory Tract Obstruction– Pneumonia– Decreased Respiratory Gasses Exchange

84
Causes of Respiratory Alkalosis
• It occurs due to hyper ventilation caused by – High Altitude – Psychoneurosis
• Treatment Kidney compensates for respiratory acidosis and alkalosis.

85
Causes of Metabolic Acidosis• Ingestion or production of more acids.• Less excretion of acids by kidneys.• Causes include:
– Diarrhea – Vomiting– Renal Failure– Diabetes Mallitus
• It is characterized by:– Hyperventilation as compensatory mechanism– Decreased HCO-
3 in the ECF• Treatment:
– Ingestion of Sodium Bicarbonate , – Sodium Lactate or Gluconate drip

86
Causes of Metabolic Alkalosis
• Increased ingestion of alkalies• Loss of Cl- by vomiting during pyloric stenosis• Alkalosis caused by use of diuretics (except CA inhibiters)• Increased Aldosternoe secretion.• This condition may be characterized by hyper excitibility
leading to tetany.• Treatment:
– Ingestion of Ammonium Chloride