University of Groningen Antenatal diagnosis and management ...
167
University of Groningen Antenatal diagnosis and management of fetal megacystis and lower urinary tract obstruction Fontanella, Federica IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2019 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Fontanella, F. (2019). Antenatal diagnosis and management of fetal megacystis and lower urinary tract obstruction. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 15-12-2021
Transcript of University of Groningen Antenatal diagnosis and management ...

University of Groningen
Antenatal diagnosis and management of fetal megacystis and lower urinary tract obstructionFontanella, Federica
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2019
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Fontanella, F. (2019). Antenatal diagnosis and management of fetal megacystis and lower urinary tractobstruction. University of Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 15-12-2021

Antenatal diagnosis and management of fetal megacystis and lower urinary tract obstruction
F. Fontanella

Antenatal diagnosis and management of fetal megacystis and lower urinary tract obstruction
Federica Fontanella, The Netherlands, 2018
ISBN 978-94-034-1269-6ISBN (PDF) 978-94-034-1268-9
Printed by Ridderprint BV, www.ridderprint.nl Layout by Jos HendrixCoverdesign and illustrations on page 17, 71, 101 by Laura Fontanella
© 2018 F. Fontanella, Groningen, The NetherlandsThe copyright of the articles that have been published has been transferred to the respective journals. No parts of this thesis may be reproduced or transmitted in any form by any means, without prior permission of the copyright owner.

Antenatal diagnosis and managementof fetal megacystis and lower urinary tract obstruction
PhD thesis
to obtain the degree of PhD at theUniversity of Groningen on the authority of the
Rector Magnifi cus prof. E. Sterkenand in accordance with
the decision by the College of Deans.
This thesis will be defended in public on
Wednesday 9 January 2019 at 14.30 hours
by
Federica Fontanella
born on 13 November 1989 in Rome, Italy

SupervisorsProf. C.M. BilardoProf. D. Oepkes
Assessment CommitteeProf. A.F. BosProf. J.M. NijmanProf. M.D. Kilby
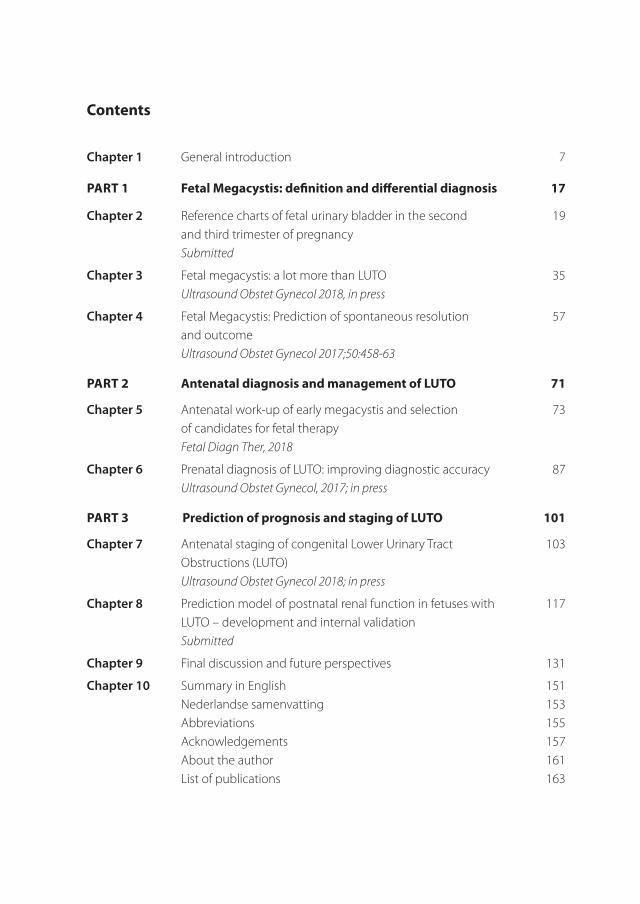
Contents
Chapter 1 General introduction 7
Part 1 Fetal Megacystis: definition and differential diagnosis 17
Chapter 2 Reference charts of fetal urinary bladder in the second 19 and third trimester of pregnancy Submitted
Chapter 3 Fetal megacystis: a lot more than LUTO 35 UltrasoundObstetGynecol2018,inpress
Chapter 4 Fetal Megacystis: Prediction of spontaneous resolution 57 and outcome UltrasoundObstetGynecol2017;50:458-63
Part 2 antenatal diagnosis and management of LUtO 71
Chapter 5 Antenatal work-up of early megacystis and selection 73 of candidates for fetal therapy FetalDiagnTher,2018
Chapter 6 Prenatal diagnosis of LUTO: improving diagnostic accuracy 87 UltrasoundObstetGynecol,2017;inpress
Part 3 Prediction of prognosis and staging of LUtO 101
Chapter 7 Antenatal staging of congenital Lower Urinary Tract 103 Obstructions (LUTO)
UltrasoundObstetGynecol2018;inpress
Chapter 8 Prediction model of postnatal renal function in fetuses with 117 LUTO – development and internal validation
Submitted
Chapter 9 Final discussion and future perspectives 131
Chapter 10 Summary in English 151 Nederlandse samenvatting 153 Abbreviations 155 Acknowledgements 157 About the author 161 List of publications 163

1General introduction
8
Chapter 1

1
9
General introduction
Background
During fetal life, a number of conditions can potentially disrupt the in-utero development and lead to short and long-term damaging effects for the fetus. For a minority of them, an intervention during pregnancy can limit the life-threatening consequences of the disease and potentially ameliorate the prognosis. In these cases, fetal specialists are not only expected to diagnose the condition, but also to inform parents on the available therapies and help them choose the best option for their unborn baby.
To date, the effectiveness of fetal surgery has been ascertained for some congenital conditions such as for sacrococcygeal teratoma (1), cystic pulmonary adenomatoid malformations (2) and myelomeningocele (3). For other disorders, the benefit of fetal therapy is still unclear and the lack of large studies and high-quality evidences limits the ability of counseling parents exhaustively and correctly on therapeutic options. This is the case for Lower Urinary Tract Obstruction (LUTO).
Lower Urinary tract Obstruction: etiology and physiopathology.
The term LUTO refers to a heterogeneous group of anatomical anomalies causing an obstruction in the urethra, such as urethral atresia, urethral stenosis or, most commonly, posterior urethral valves. The incidence of LUTO is reported between 1 in 5.000 to 1 in 25.000 pregnancies, without accounting for cases with elective termination, intrauterine fetal demise (IUFD), or cases with postnatal diagnosis (4).
Congenital obstructive uropathy accounts for the largest identifiable cause of kidney failure in infants and children (7). In fact, during fetal life LUTO can affect the renal (glomerular and tubular) function and lead to cystic renal dysplasia (6). In the second trimester, when fetal urine starts to constitute 90% of the amniotic fluid (8), severe forms of LUTO progressively cause oligohydramnios, with subsequent pulmonary hypoplasia and respiratory insufficiency at birth, being the primary cause of neonatal death in LUTO. For these reasons, congenital LUTO is associated with high perinatal mortality and postnatal morbidity owing to pulmonary hypoplasia and renal dysplasia (5).
From fetal megacystis to the antenatal diagnosis of LUtO
The suspicion of LUTO typically arises from the ultrasound (US) evidence of an enlarged fetal bladder, also called megacystis (10). However, fetal megacystis is not only associated with LUTO, but also with chromosomal abnormalities, anorectal malformations and other
10
Chapter 1
miscellaneous syndromal associations (11). Moreover, the bladder enlargement can also spontaneously resolve during pregnancy (12)(13)(14).
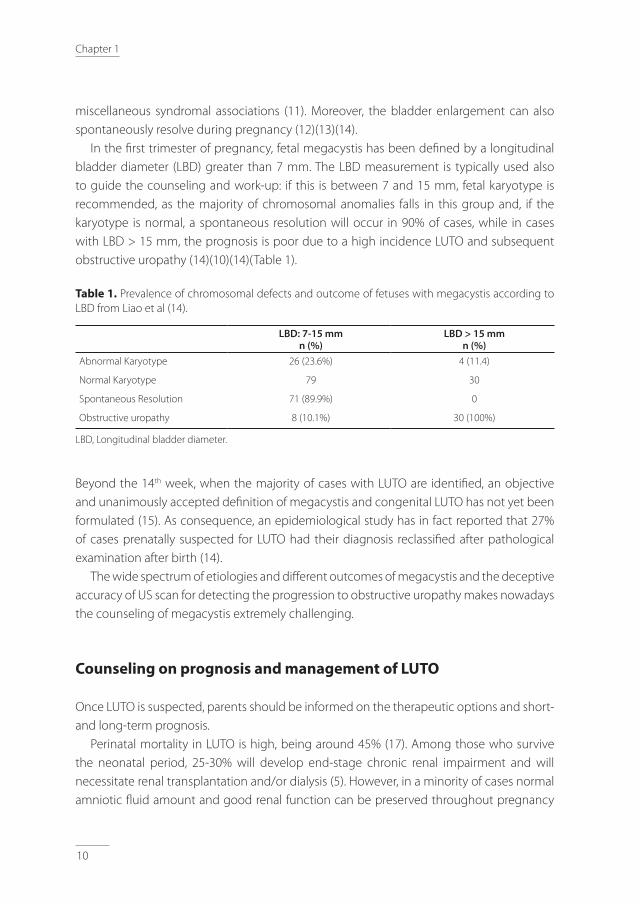
In the first trimester of pregnancy, fetal megacystis has been defined by a longitudinal bladder diameter (LBD) greater than 7 mm. The LBD measurement is typically used also to guide the counseling and work-up: if this is between 7 and 15 mm, fetal karyotype is recommended, as the majority of chromosomal anomalies falls in this group and, if the karyotype is normal, a spontaneous resolution will occur in 90% of cases, while in cases with LBD > 15 mm, the prognosis is poor due to a high incidence LUTO and subsequent obstructive uropathy (14)(10)(14)(Table 1).
table 1. Prevalence of chromosomal defects and outcome of fetuses with megacystis according to LBD from Liao et al (14).
LBD: 7-15 mmn (%)
LBD > 15 mmn (%)
Abnormal Karyotype 26 (23.6%) 4 (11.4)
Normal Karyotype 79 30
Spontaneous Resolution 71 (89.9%) 0
Obstructive uropathy 8 (10.1%) 30 (100%)
LBD, Longitudinal bladder diameter.
Beyond the 14th week, when the majority of cases with LUTO are identified, an objective and unanimously accepted definition of megacystis and congenital LUTO has not yet been formulated (15). As consequence, an epidemiological study has in fact reported that 27% of cases prenatally suspected for LUTO had their diagnosis reclassified after pathological examination after birth (14).
The wide spectrum of etiologies and different outcomes of megacystis and the deceptive accuracy of US scan for detecting the progression to obstructive uropathy makes nowadays the counseling of megacystis extremely challenging.
Counseling on prognosis and management of LUtO
Once LUTO is suspected, parents should be informed on the therapeutic options and short- and long-term prognosis.
Perinatal mortality in LUTO is high, being around 45% (17). Among those who survive the neonatal period, 25-30% will develop end-stage chronic renal impairment and will necessitate renal transplantation and/or dialysis (5). However, in a minority of cases normal amniotic fluid amount and good renal function can be preserved throughout pregnancy
1
11
General introduction
(16). To sum up, natural history of LUTO is highly variable and fetal specialists can only rely on gestational age at onset of obstruction and sex of the baby to have a general idea of the outcome (9).
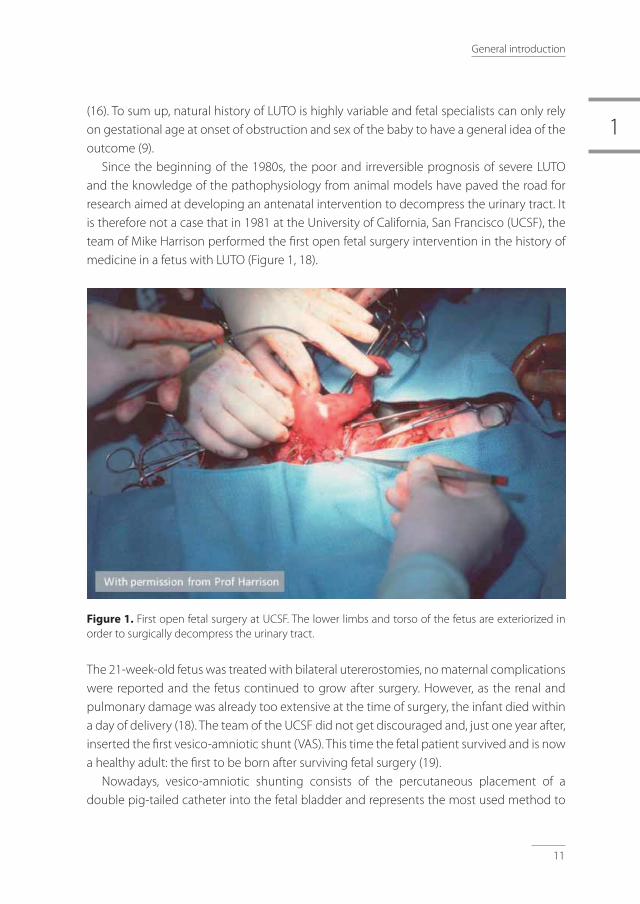
Since the beginning of the 1980s, the poor and irreversible prognosis of severe LUTO and the knowledge of the pathophysiology from animal models have paved the road for research aimed at developing an antenatal intervention to decompress the urinary tract. It is therefore not a case that in 1981 at the University of California, San Francisco (UCSF), the team of Mike Harrison performed the first open fetal surgery intervention in the history of medicine in a fetus with LUTO (Figure 1, 18).
Figure 1. First open fetal surgery at UCSF. The lower limbs and torso of the fetus are exteriorized in order to surgically decompress the urinary tract.
The 21-week-old fetus was treated with bilateral utererostomies, no maternal complications were reported and the fetus continued to grow after surgery. However, as the renal and pulmonary damage was already too extensive at the time of surgery, the infant died within a day of delivery (18). The team of the UCSF did not get discouraged and, just one year after, inserted the first vesico-amniotic shunt (VAS). This time the fetal patient survived and is now a healthy adult: the first to be born after surviving fetal surgery (19).
Nowadays, vesico-amniotic shunting consists of the percutaneous placement of a double pig-tailed catheter into the fetal bladder and represents the most used method to

12
Chapter 1
relieve the urinary obstruction during fetal life (Figure 2)(6).An alternative intervention for LUTO is fetal cystoscopy. This allows the direct
visualization of the obstruction and ablation of the PUV using hydro-ablation, guide-wire or laser fulguration (20)(21)(22)(23)(24). Fetal cystoscopy is technically complicated and not therapeutic in fetuses with urethral atresia, but has the advantage to restore the physiological bladder dynamic and to not require amnioinfusions (25).
Despite these developments, most of the parents currently choose for terminating the pregnancy or opt for a conservative management (4)(26). This last option includes regular US scans for monitoring the bladder distension, amniotic fluid amount and fetal kidneys (6). Main goal is the surveillance of fetal well-being until an estimated weight of 2-2.5 kg is achieved in order to allow peritoneal dialysis catheter placement candidacy (25). Another recently proposed option consists in performing serial amnioinfusions until the 28th-30th week of gestation in order to protect from oligohydramnios. This approach should be still considered experimental as further studies are needed to assess its safety and benefits (27)(28)(25).
PLUtO trial, open questions and rational of this thesis
In the last decade, the above mentioned management options have been further investigated. In 2006, the first randomized, multicenter control trial (PLUTO trial) to assess the effectiveness of vesico-amniotic shunting compared to conservative management has been started and in 2010 prematurely ended because of poor recruitment. The PLUTO trial showed a higher survival to 28 days, 1 year, and 2 years in fetuses treated with VAS. However, due to the small numbers of participants recruited (only 20% of the planned 150 pregnancies were randomized), the benefit of VAS was not conclusively proven. The PLUTO trail also reported that irrespective of whether or not vesico-amniotic shunting was done, the overall postnatal outlook was very poor (26).
With the premature conclusion of the PLUTO trial, the fetal medicine community has missed an important opportunity of high-quality evidence for clarifying the role of VAS and the appropriate antenatal management for LUTO (29). Since then, a second RCT comparing fetal cystoscopy and VAS has been started (Clinicaltrials.gov, identifier NCT01552824) (30) and new observational studies have been conducted (30)(31)(32).
In summary, the literature suggests a beneficial role of both VAS and cystoscopy in terms of perinatal survival in fetuses with severe LUTO. However, concerning the postnatal renal function, the role of VAS is still unclear, while fetal cystoscopy has been suggested as beneficial selectively in fetuses with PUV (30). To date, the role, best candidates and best timing for these antenatal interventions is still unclear and a new RCTs would represent the gold standard for further evaluating treatment effectiveness. However, in order to clarify

1
13
General introduction
these points, a more standardized and accurate diagnostic evaluation, staging approach and prognostic assessment of LUTO is first needed. For this purpose, multicenter co-operations and large-scale registries can firstly help set up the groundwork needed before moving towards the design of a new RCT.
aim and outline of the thesis
In this thesis we gathered information at a national level and collected prenatal and post-natal information on fetuses diagnosed with megacystis. The final aim was to investigate the above-mentioned open questions and be able to guide fetal specialists in the difficult counseling and diagnostic work-up, from fetal megacystis to congenital LUTO.
Part 1 - Fetal Megacystis: definition and counselingIn the first part of the thesis, the definition and differential diagnosis of fetal megacystis is discussed. In chapter 2, reference values for the definition of a normal fetal urinary bladder during second and third-trimester megacystis are provided for the first time in the literature. In chapter 3, we propose a flowchart for guiding the differential diagnosis of megacystis and ruling out genetic syndromes, developmental and chromosomal abnormalities. Chapter 4 focuses on prediction of spontaneous resolution of megacystis and postnatal outcome after resolution.
Part 2 - Prenatal diagnosis and management of LUTOThe second part of the thesis aims at improving the accuracy of US scan examination in the diagnosis of LUTO and its underlying cause (PUV or urethral atresia). Chapter 5 focuses on early megacystis and on the optimal criteria for selecting cases with PUV, thus eligible for fetal therapy early in pregnancy. In chapter 6, we propose a new scoring system for fine-tuning the prenatal diagnosis of LUTO in cases with late megacystis, diagnosed after the 17th week of gestation.
Part 3 - Prediction of prognosis and staging of LUTOIn the last part of the thesis, the focus is on predicting the prognosis of LUTO, in terms of perinatal survival and postnatal renal function. Chapter 7 aims at predicting of the risk of perinatal death and proposing of a new staging system for LUTO, while in chapter 8, a prediction model for postnatal renal function is presented.
The thesis ends with a general discussion of the implications of our findings and future perspective (chapter 9).

14
Chapter 1
references
1. Flake A, Harrison M, Adzick N, Laberge J, Warsof S. Fetal sacrococcygeal teratoma. J Pediatr Surg. 1986;21(7):563–6.
2. Adzick N, Harrison M, Flake A, Howell L, Golbus M, Filly R. Fetal surgery for cystic adenomatoid malformation of the lung. J Pediatr Surg. 1993;28(6):806–12.
3. Adzick S, Thom E, Spong C, Brock J, Burrows P, Johnson M, Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB, D’Alton ME, Farmer DL; MOMS Investigators. A Randomized Trial of Prenatal versus Postnatal Repair of Myelomeningocele. N Engl J Med. 2011;365:883–91.
4. Anumba DO, Scott JE, Plant ND, Robson SC. Diagnosis and outcome of fetal lower urinary tract obstruction in the northern region of England. Prenat Diagn. 2005;25(1):7–13.
5. Parkhouse HF, Barratt TM, Dillon MJ, Duffy PG, Fay J, Ransley PG, Woodhouse CR, Williams DI. Long-term outcome of boys with posterior urethral valves. Br J Urol [Internet]. 1988;62(1):59–62.
6. Morris RK, Kilby MD. Congenital urinary tract obstruction. Best Pract Res Clin Obstet Gynaecol. 2008;22(1):97–122.
7. Chevalier R. Fetal urinary tract obstruction: pathophysiology. Fetal Therapy: Scientific Basis and Critical Appraisal of Clinical Benefits. Kilby, M.D. Oepkes, D. Johnson, A. Cambridge University Press; 2012. 238 p.
8. Vanderheyden T, Kumar S, Fisk NM. Fetal renal impairment. Semin Neonatol. 2003;8(4):279–89.
9. Khalek N JM. Fetal urinary tract obstruction: prenatal assessment and prognosis. In Fetal Therapy: Scientific Basis and Critical Appraisal of Clinical Benefits. Kilby D, O. Cambridge CU press:, editor.
10. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8(6):387–90.
11. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, El-Ghoneimi A, Oury JF, Muller F. Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn. 2013;33(12):1162–6.
12. Fievet L, Faure A, Coze S, Harper L, Panait N, Braunstein D, Carson J, Gorincour G, Chaumoitre K, Guys JM, Alessandrini P, D’Ercole C, Merrot T. Fetal megacystis: Etiologies, management, and outcome according to the trimester. Urology. 2014;84(1):185–90.
13. Matsui F, Shimada K, Matsumoto F, Obara T. Prenatal resolution of megacystis possibly caused by spontaneous rupture of posterior urethral valves. J Pediatr Surg. 2008;43(12):2285–7.
14. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: Chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol. 2003;21(4):338–41.
15. Taghavi K, Sharpe C, Stringer MD. Fetal megacystis: A systematic review. J Pediatr Urol. 2017;13(1):7–15.
16. Johnson MP, Danzer E, Koh J, Polzin W, Harman C, O ’shaughnessy R, Brown R, Zaretsky MV; North American Fetal Therapy Network (NAFTNet). Natural History of Fetal Lower Urinary Tract Obstruction with Normal Amniotic Fluid Volume at Initial Diagnosis.
17. Freedman a L, Johnson MP, Gonzalez R. Fetal therapy for obstructive uropathy: past, present.future? Pediatr Nephrol [Internet]. 2000;14(2):167–76.
18. Harrison MR, Golbus MS, Filly RA, Callen PW, Katz M, de Lorimier AA, Rosen M., Jonsen AR. Fetal surgery for congenital hydronephrosis. N Engl J Med [Internet]. 1982;306(10):591–3.
19. Chur E. Michael Harrison: Inventing Devices & a New Field. 2017. Available from: https://surgicalinnovations.ucsf.edu/spotlight/innovator-profiles/michael-harrison,-md.aspx
20. Ruano R. Fetal surgery for severe lower urinary tract obstruction. Vol. 31, Prenatal Diagnosis. 2011. p. 667–74.
21. Ruano R, Pimenta EJ, Duarte S, Zugaib M. Four-dimensional ultrasonographic imaging of fetal lower urinary tract obstruction and guidance of percutaneous cystoscopy. Ultrasound Obstet Gynecol [Internet]. 2009 Feb 1 [cited 2018 Feb 1];33(2):250–2.
22. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F,Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: A multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015;
23. Ruano R, Yoshisaki CT, Salustiano EMA, Giron AM, Srougi M, Zugaib M. Early fetal cystoscopy for first-trimester severe megacystis. Ultrasound Obstet Gynecol. 2011;

1
15
General introduction
24. Ruano R, Yoshizaki CT, Giron AM, Srougi M, Zugaib M. Cystoscopic placement of transurethral stent in a fetus with urethral stenosis. Ultrasound Obstet Gynecol. 2014 Aug 1;44(2):238–40.
25. Haeri S. Fetal Lower Urinary Tract Obstruction (LUTO): a practical review for providers. Matern Heal Neonatol Perinatol [Internet]. 2015;1:26.
26. Morris RK, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan KS, Deeks J, Kilby MD. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): A randomised trial. Lancet. 2013;
27. Haeri S, Simon DH, Pillutla K. Serial amnioinfusions for fetal pulmonary palliation in fetuses with renal failure. J Matern Neonatal Med [Internet]. 2017;30(2):174–6.
28. Polzin WJ, Lim FY, Habli M, Van Hook J, Minges M, Jaekle R, Crombleholme TM. Use of an Amnioport to Maintain Amniotic Fluid Volume in Fetuses with Oligohydramnios Secondary to Lower Urinary Tract Obstruction or Fetal Renal Anomalies. Fetal Diagn Ther. 2017;41(1):51–7.
29. Van Mieghem T, Ryan G. The PLUTO trial: a missed opportunity. Lancet. 2013 Nov;382(9903):1471–3.
30. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F,Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: a multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015 Apr;45(4):452–8.
31. Ruano R, Yoshisaki CT, Salustiano EMA, Giron AM, Srougi M, Zugaib M. Early fetal cystoscopy for first-trimester severe megacystis. Ultrasound Obstet Gynecol. 2011 Jun;37(6):696–701.
32. Nassr AA, Shazly SAM, Abdelmagied AM, Araujo Júnior E, Tonni G, Kilby MD, Ruano R. Effectiveness of vesico-amniotic shunt in fetuses with congenital lower urinary tract obstruction: An updated systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2016 Jun.


Part 1
Fetal Megacystis: definition
and differential diagnosis


2Reference charts of fetal urinary bladder in the second and third trimester of pregnancy
F. Fontanella, H. Groen, R. Smidt, L. Duin and C.M. Bilardo
Submitted

20
Chapter 2
abstract
Objective: To use 3D ultrasound images to construct reference values for fetal normal urinary bladder size and volume between 15 and 35 weeks of gestation.
Methods: This was a prospective cross-sectional study carried out from 2016 to 2017 at the University Medical Centre Groningen, the Netherlands. Singleton pregnancies in absence of fetal abnormalities were included in the study between 15 and 35 weeks’ gestation. All ultrasound examinations were performed by a trained sonographer. During each scan, lasting approximately 40-60 minutes, at least three 3D volumes of the urinary bladder were obtained for each fetus. Fetal bladder volume was calculated offline by the automatic volume calculation (AVC) tool and the manual virtual organ computer-aided analysis (VOCAL) technique, with 30° rotation angles. Postnatal data were reviewed, and only live-born children without congenital anomalies were kept in the study.
results: A 3D ultrasound sweep of the fetal bladder was obtained every 20 minutes in 225 pregnant women between 15 and 35 weeks of gestation. A total of 1238 measurements of urinary bladder volume (BV) and largest bladder diameter (LBD) were obtained. Urinary BV was successfully measured by the semi-automatic SonoAVC tool in 123 cases (55%) and by VOCAL method in all cases. There was no significant correlation between measurements obtained by SonoAVC and by VOCAL technique (r = 0.37). A linear relationship was observed between LBD and GA (r2: 0.78 for the largest LBD and 0.76 for the mean LBD), while a polynomial regression line was fitted for the BV according to GA. Gestational age based normal ranges for the largest and mean LBD and bladder volume (BV) were constructed.
Conclusions: This normative data will be useful to establish if a bladder is pathologically enlarged in the second half of fetal life.

2
21
Normograms of fetal bladder
Introduction
The function of the bladder is storing urine at low pressure and expelling it periodically via coordinated and sustained contractions (1). Neurogenic bladder dysfunctions, lower urinary tract obstruction (LUTO) or vesico-ureteral reflux can prejudice this function during fetal life and alter the physiological bladder filling and voiding process. When one of these conditions is suspected prenatally, it is crucial for the differential diagnosis and prognosis to objectively assess if the bladder size falls within normal ranges and to reproducibly triage an eventual pathological bladder enlargement (2)(3)(4).
Fetal bladder is standardly assessed at the first trimester scan, when the normal longitudinal bladder diameter measures less than 7 mm (5). However, beyond the 14th week of gestation, although the assessment of bladder filling is part of every standard ultrasound examination (6)(7), a clear cut-off for defining normal or enlarged bladder size is lacking. Since the 1970s, hourly fetal urine production throughout gestation has been studied by using both 2D and 3D US (8)(9)(10)(11)(12)(13)(14)(15), showing that urinary production and bladder capacity progressively increase during gestation (16). However, all these studies have failed to report reference ranges and growth charts for fetal urinary bladder size beyond 14 weeks’ gestation. This means that currently the diagnosis of an enlarged bladder is largely based on a subjective judgment, rather than on objective parameters defining a normal or pathological bladder distension.
Main objective of the study was therefore to fill this gap and to construct charts of fetal bladder volume (BV) and longitudinal bladder diameter (LBD) from 15to 35 weeks of pregnancy.
Methods
A cross-sectional prospective study was carried out from May 2016 to October 2017 at the University Medical Center Groningen. Pregnant women with a viable singleton uncomplicated pregnancy and with an accurate gestational-age assessment were recruited from the 15th week of gestation age until 35 weeks’ gestation. Exclusion criteria were: multiple pregnancies, fetal congenital abnormalities -detected either before or after birth-, and the use of medications or maternal diseases that could potentially affect fetal growth or diuresis (diabetes mellitus, smoking, hypertensive disorders). Postnatal data were collected in order to exclude neonates with abnormalities of pathological conditions at birth.
A trans-abdominal US scan was performed only once for each patient by a trained operator (FF) using either a Voluson E8 or E10 system (GE Voluson TM Healthcare, Zipf, Austria). The scan lasted 40 minutes and serial 2D and 3D ultrasound images of the fetal

22
Chapter 2
urinary bladder were collected. For the measurement of the urinary bladder volume (BV), 3D sweeps of the lower fetal
abdomen were taken, digitally stored and subsequently analyzed with the 4D View software (GE VolusonTM Healthcare, Zipf, Austria). The BV was calculated by using two methods: Sono automatic volume calculation (SonoAVC) and manual Virtual Organ Computer-aided Analysis (VOCAL), drawing the contours of the fluid filled area at every 30º of rotation (Figure 1). Additionally, the longitudinal bladder diameter (LBD) was measured manually on the multiplanar 3D image, corrected to the exact mid-sagittal plane, by placing one caliper on the inner border of the bladder wall at the upper pole (bladder dome) and the other on the inner border of the lower pole (bladder neck). A single trained operator measured manually the LBD and drew the contours of the bladder.For the study design, patient selection and statistical method, the guidelines from Altman and Chitty (1993) and by Ioannou et al (2011) were followed. The measurements were modeled against the gestational age and reference charts were constructed. Polynomial regression models were fitted to the mean and standard deviation (SD) of each measurement as functions of gestational age.
The study was authorized by the Medical Ethics Committee in Groningen (dossier number NL54636.042.15).
Figure 1. 3D sweeps of fetal pelvis with manual Virtual Organ Computer-aided Analysis of bladder contours.

2
23
Normograms of fetal bladder
results
A total of 225 pregnant women at different gestation age participated once into the study (Table 1). BV and LBD were measured at 20 minutes’ interval. In 56 cases, the scan lasted less than 40 minutes and the third US measurement was not performed. In total, 1238 measurements were obtained.
table 1. Gestational age distribution of the study population.
GA N %
15 12 5,3
16 11 4,9
17 13 5,8
18 9 4,0
19 10 4,4
20 15 6,7
21 17 7,6
22 15 6,7
23 19 8,4
24 16 7,1
25 12 5,3
26 13 5,8
27 7 3,1
28 14 6,2
29 9 4,0
30 9 4,0
31 6 2,7
32 5 2,2
33 5 2,2
34 4 1,8
35 4 1,8
Total 225 100
The BV was measured by using both the SonoAVC and the VOCAL method. The SonoAVC tool was successful in identifying and calculating the BV in 123 (55%). In the remaining 102 cases (45%) where the SonoAVC failed to semi-automatically identify and calculate the BV, this was only calculated by the Vocal method. In the 123 cases with volume measured by both SonoAVC or VOCAL, the bladder measurements differed by 3% (mean difference 6 cm3) and a significant correlation was not found (r = 0.37).
24
Chapter 2
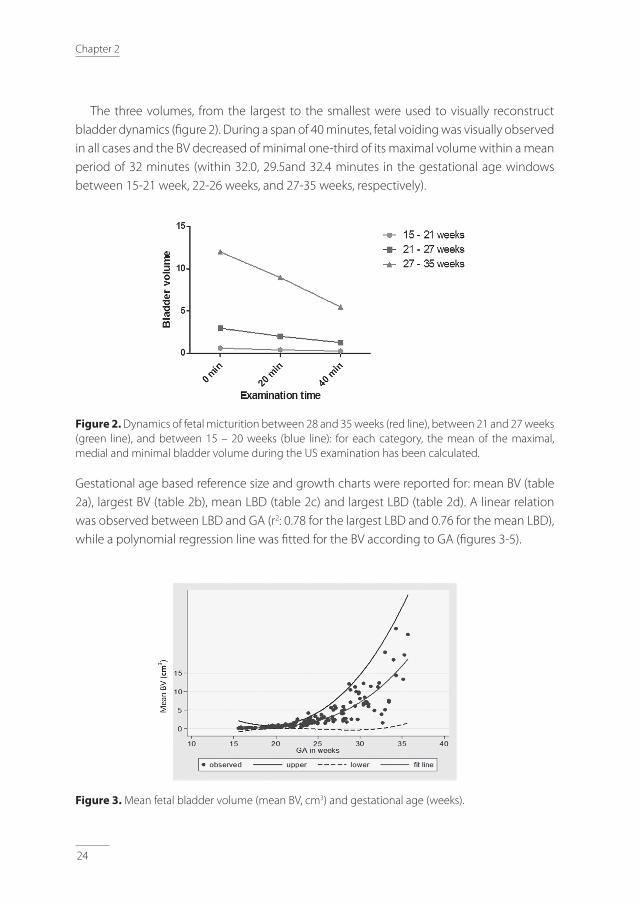
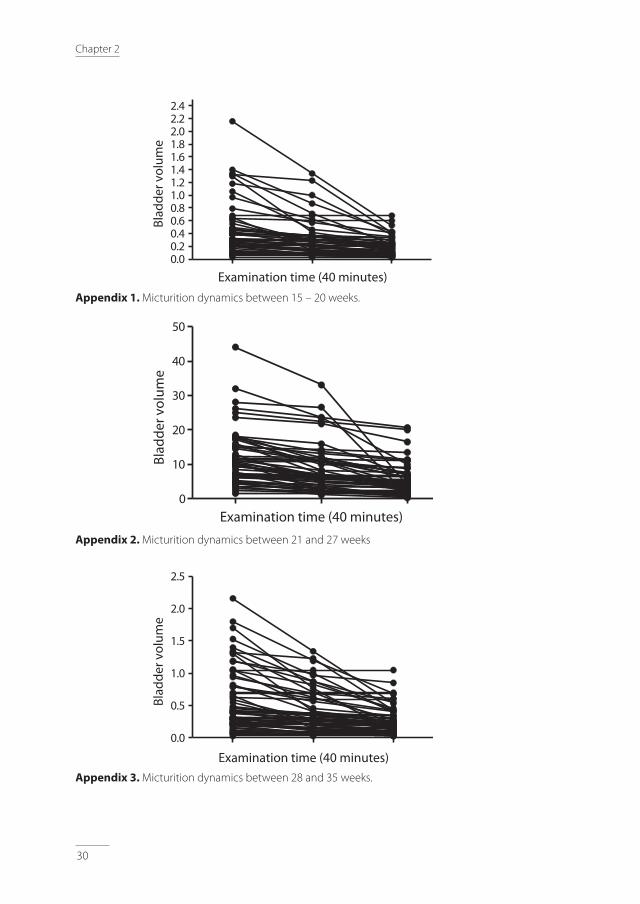
The three volumes, from the largest to the smallest were used to visually reconstruct bladder dynamics (fi gure 2). During a span of 40 minutes, fetal voiding was visually observed in all cases and the BV decreased of minimal one-third of its maximal volume within a mean period of 32 minutes (within 32.0, 29.5and 32.4 minutes in the gestational age windows between 15-21 week, 22-26 weeks, and 27-35 weeks, respectively).
Figure 2. Dynamics of fetal micturition between 28 and 35 weeks (red line), between 21 and 27 weeks (green line), and between 15 – 20 weeks (blue line): for each category, the mean of the maximal, medial and minimal bladder volume during the US examination has been calculated.
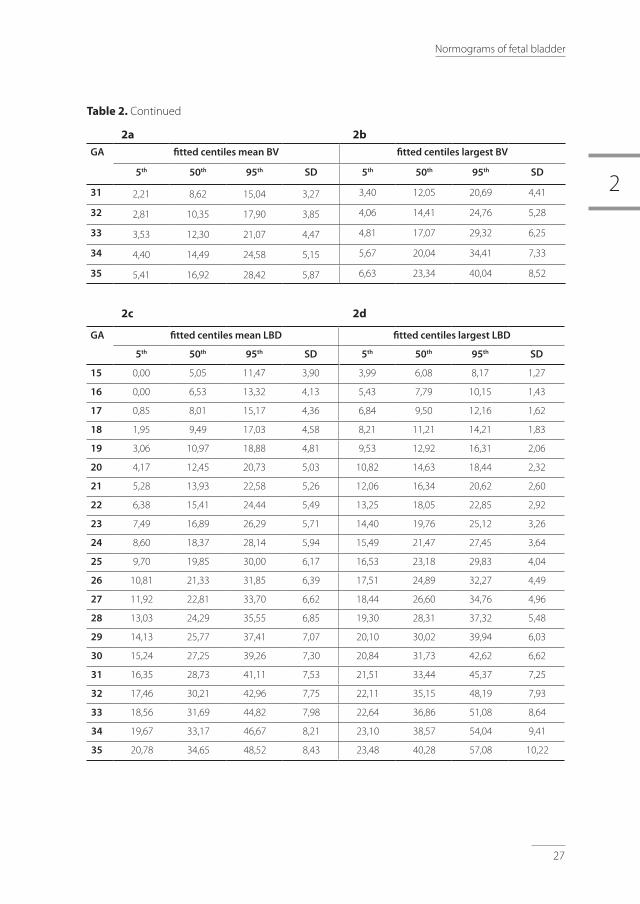
Gestational age based reference size and growth charts were reported for: mean BV (table 2a), largest BV (table 2b), mean LBD (table 2c) and largest LBD (table 2d). A linear relation was observed between LBD and GA (r2: 0.78 for the largest LBD and 0.76 for the mean LBD), while a polynomial regression line was fi tted for the BV according to GA (fi gures 3-5).
Figure 3. Mean fetal bladder volume (mean BV, cm3) and gestational age (weeks).

2
25
Normograms of fetal bladder
Figure 4. Largest fetal bladder volume (max BV, mm) and gestational age (weeks)
Figure 5. Mean longitudinal diameter (cm3)and gestational age (weeks).
Figure 6. Largest longitudinal bladder diameter (mm) and gestational age (weeks).

26
Chapter 2
Discussion
This study reports normograms for the longitudinal bladder diameter and bladder volume from 15throughout 35weeks of gestation. These are, to our knowledge, the first normative data enabling the definition of a normal bladder size during the second and third trimester of pregnancy.
Cut-offs of normal bladder size have long been known in the first trimester of pregnancy (2). However, LUTO, posterior urethral valves, VUR or neurogenic bladder dysfunctions are more frequently suspected later in pregnancy, when bladder size assessment has already proved valuable for predicting prognosis (2)(3)(17). So far, previous studies have reported the hourly urinary fetal production (HUFP) throughout gestation without reporting on the size of the urinary bladder(18)(12)(14).The lack of normative data on urinary bladder size has represented a major issue, in particular for the definition of megacystis in the second and third-trimester of pregnancy (19).
table 2. Fitted centiles of the largest longitudinal diameter (largest LBD, mm; 2d), mean longitudinal bladder diameter (mean LBD, mm; 2c), largest bladder volume (BV, cm3; 2b) and mean bladder volume (BV, cm3; 2a) for exact gestational week between 15 and 35 weeks of gestational age (GA).
2a 2b
GA fitted centiles mean BV fitted centiles largest BV
5th 50th 95th SD 5th 50th 95th SD
15 0,00 0,69 1,99 0,66 0,00 0,85 2,10 0,64
16 0,00 0,55 1,46 0,46 0,00 0,69 1,66 0,50
17 0,00 0,45 1,06 0,31 0,00 0,57 1,33 0,39
18 0,00 0,39 0,79 0,21 0,00 0,53 1,13 0,31
19 0,10 0,39 0,68 0,15 0,03 0,55 1,08 0,27
20 0,18 0,46 0,73 0,14 0,14 0,67 1,20 0,27
21 0,24 0,60 0,96 0,18 0,27 0,89 1,52 0,32
22 0,29 0,82 1,36 0,27 0,41 1,23 2,05 0,42
23 0,34 1,15 1,95 0,41 0,57 1,70 2,83 0,58
24 0,40 1,58 2,75 0,60 0,76 2,32 3,87 0,79
25 0,49 2,13 3,77 0,84 0,98 3,09 5,21 1,08
26 0,62 2,81 5,01 1,12 1,24 4,05 6,85 1,43
27 0,79 3,64 6,49 1,45 1,55 5,20 8,84 1,86
28 1,02 4,62 8,22 1,84 1,91 6,55 11,19 2,37
29 1,33 5,77 10,21 2,27 2,34 8,14 13,93 2,96
30 1,72 7,10 12,48 2,74 2,83 9,96 17,09 3,64
2
27
Normograms of fetal bladder
GA fitted centiles mean BV fitted centiles largest BV
5th 50th 95th SD 5th 50th 95th SD
31 2,21 8,62 15,04 3,27 3,40 12,05 20,69 4,41
32 2,81 10,35 17,90 3,85 4,06 14,41 24,76 5,28
33 3,53 12,30 21,07 4,47 4,81 17,07 29,32 6,25
34 4,40 14,49 24,58 5,15 5,67 20,04 34,41 7,33
35 5,41 16,92 28,42 5,87 6,63 23,34 40,04 8,52
2c 2d
GA fitted centiles mean LBD fitted centiles largest LBD
5th 50th 95th SD 5th 50th 95th SD
15 0,00 5,05 11,47 3,90 3,99 6,08 8,17 1,27
16 0,00 6,53 13,32 4,13 5,43 7,79 10,15 1,43
17 0,85 8,01 15,17 4,36 6,84 9,50 12,16 1,62
18 1,95 9,49 17,03 4,58 8,21 11,21 14,21 1,83
19 3,06 10,97 18,88 4,81 9,53 12,92 16,31 2,06
20 4,17 12,45 20,73 5,03 10,82 14,63 18,44 2,32
21 5,28 13,93 22,58 5,26 12,06 16,34 20,62 2,60
22 6,38 15,41 24,44 5,49 13,25 18,05 22,85 2,92
23 7,49 16,89 26,29 5,71 14,40 19,76 25,12 3,26
24 8,60 18,37 28,14 5,94 15,49 21,47 27,45 3,64
25 9,70 19,85 30,00 6,17 16,53 23,18 29,83 4,04
26 10,81 21,33 31,85 6,39 17,51 24,89 32,27 4,49
27 11,92 22,81 33,70 6,62 18,44 26,60 34,76 4,96
28 13,03 24,29 35,55 6,85 19,30 28,31 37,32 5,48
29 14,13 25,77 37,41 7,07 20,10 30,02 39,94 6,03
30 15,24 27,25 39,26 7,30 20,84 31,73 42,62 6,62
31 16,35 28,73 41,11 7,53 21,51 33,44 45,37 7,25
32 17,46 30,21 42,96 7,75 22,11 35,15 48,19 7,93
33 18,56 31,69 44,82 7,98 22,64 36,86 51,08 8,64
34 19,67 33,17 46,67 8,21 23,10 38,57 54,04 9,41
35 20,78 34,65 48,52 8,43 23,48 40,28 57,08 10,22
table 2. Continued
2a 2b

28
Chapter 2
Thus far, the definition of megacystis beyond the first trimester has been heterogeneous including: a longitudinal bladder measurement above the 99th centile without referring to any normative data (20); a fetal bladder reaching the umbilical cord insertion, or most commonly, a bladder failing to empty within 45 minutes (21). All these definitions lack an objective cut-off to define a physiological and pathological bladder distension and to allow reproducibility and consistency among the studies. Maizels et al. were the first in the literature to propose a mathematical formula to calculate the LBD according to GA, but only based on 39 normal bladders measurements between 15 and 40 weeks’ gestation (22). The study reported a linear relationship between GA and largest LBD and the calculated formula was LBD = GA – 5. We also found a linear relationship between LBD and GA, but with the following formula defining the mean physiological LBD: LBD = 1.48 * GA - 17.15.
The bladder volume can be assessed either by applying a mathematical formula for the three bladder diameters (longitudinal, antero-posterior and transverse) obtained by 2D US, or by directly calculating the volume on 3D pictures taking into account the true shape of the fetal bladder. Two major limitations can be envisaged with the first approach: first, the fact that the volume is calculated on an arbitrarily selected image, assumed to represent the maximal bladder size and (8) second, the difficulty of choosing an appropriate formula to calculate the BV from the bladder diameters. In fact, throughout the filling phase, the bladder shape changes from an ellipsoid to a super-ellipsoid, a virtually more cylindrical shape(8). Therefore, the use of a unique formula for estimating the bladder volume at different filling phases and GA it is not appropriate (23)(8). Both these limitations can be overcome by the use of a 3D US technique enabling accurate volume estimation, even in irregularly shaped or asymmetrical organs (24)(25)(26). Three D technique is at present the most accurate method (27) for calculating the BV and we therefore report charts and centiles for the 3D-measured fetal bladder volume.
After acquisition of a 3D image, different methods can be used to measure the volume of an organ, such as the rotational Virtual Organ Computer-aided AnaLysis ((VOCAL); GE Medical Systems, Zipf, Austria) or the automated segmentation tool for fluid-filled spaces Sono-AVC (GE Medical Systems). The Sono-AVC tool semi-automatically recognizes, traces and measures the fluid-filled structures in the 3D volume. This tool represents the easiest and quickest method in daily practice, however the volumes obtained on the same image with either SonoAVC and VOCAL setting in our cohort were not strictly correlated (r=0.037), and the SonoAVC method failed in recognizing the right structure in 45% of our cases. The VOCAL method has been previously used for measuring the BV by Peixoto-Filho et al. (27). The authors also investigated the inter- and intra-observer reliability by using 15 and 30° rotation steps calculation. Since an excellent correlation between the two measurements was found, the authors suggested to use 30° of rotation as this is significantly faster. This is why we adopted 30° rotational angle.

2
29
Normograms of fetal bladder
As 3D technique is not universally available, we also propose reference ranges for LBD, based on 2D Images and therefore more easily applicable in daily practice.
In the present study, the 40-minutes period for the US examination resulted in the observation of a complete bladder cycle of filling and voiding in all fetuses. This confirms the results of Hata et al., which reported that the time needed for observing the bladder empty was approximately 30 minutes at 28 weeks, and 40 minutes at 35 weeks’ gestation (28). These and our results (figure 1), confirm that the capacity of the fetal bladder to store urine and empty changes and matures with advancing gestation, with a progressively increasing capacity and more complete emptying with advancing gestation (1).As we examined the fetuses for 40 minutes, the HUFP could not be calculated. However, the HUFP has been already reported in details by other studies, and recently by using 3D US scans (11)(29).
A strength of this study is its prospective and cross sectional design, in accordance to the best practice for constructing fetal reference charts (30)(31). Moreover, the US examinations were performed by the same operator (F.F.), and the contours of the urinary bladder and the LBD were all measured by another operator (R.S.) This should have limited any inter-operator bias.
In conclusion, we provide normograms for fetal bladder size during the second and third trimester of pregnancy. Future research is needed to validate these results and define an objective threshold for second and third-trimester megacystis.
30
Chapter 2
appendix 1. Micturition dynamics between 15 – 20 weeks.
appendix 2. Micturition dynamics between 21 and 27 weeks
appendix 3. Micturition dynamics between 28 and 35 weeks.
Examination time (40 minutes)
Blad
der v
olum
e
0.00.20.40.60.81.01.21.41.61.82.02.22.4
Examination time (40 minutes)
Blad
der v
olum
e
0
10
20
30
40
50
Examination time (40 minutes)
Blad
der
vol
ume
0.0
0.5
1.0
1.5
2.0
2.5

2
31
Normograms of fetal bladder
references
1. Nguyen HT, Kogan BA. Fetal Bladder Physiology. Fetal Bl Physiol Baskin LS, Hayward SW Adv Bl Res Biol Boston, MA. 1999;vol 462.
2. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: Chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol. 2003;21(4):338–41.
3. Fontanella, F., L. Duin, P. N. Adama van Scheltema, T. E. Cohen - Overbeek, E. Pajkrt, M. Bekker, C. Willekes, C. J. Bax CMB. Fetal Megacystis: prediction of outcome and spontaneous resolution. Ultrasound Obstet Gynecol. 2017;
4. F. Fontanella, L. K. Duin, P. N. Adama van Scheltema, T. E. Cohen – Overbeek, E. Pajkrt, M. Bekker, C. Willekes, C. J. Bax, V. Gracchi DO and CMB. Prenatal diagnosis of LUTO: how to improve diagnostic accuracy. Ultrasound Obstet Gynecol. 2018;1–20.
5. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8(6):387–90.
6. Yiee J, Wilcox D. Abnormalities of the fetal bladder. Semin Fetal Neonatal Med. 2008;13(3):164–70.
7. Jouannic JM, Hyett JA, Pandya PP, Gulbis B, Rodeck CH, Jauniaux E. Perinatal outcome in fetuses with megacystis in the first half of pregnancy. Prenat Diagn. 2003;23(4):340–4.
8. Fägerquist M, Fägerquist U, Steyskal H, Odén A, Blomberg SG. Accuracy in estimating fetal urinary bladder volume using a modified ultrasound technique. Ultrasound Obstet Gynecol. 2002;19(4):371–9.
9. Bernard JP, Rizk E, Camatte S, Robin F, Taurelle R, Lecuru F. Fetal urine production and accuracy when estimating fetal urinary bladder volume. Ultrasound Obstet Gynecol. 2001;17(2):132–9.
10. Campbell S, Wladimiroff JW, Dewhurst CJ. The antenatal measurement of fetal urine production. J Obstet Gynaecol Br Commonw. 1973 Aug;80(8):680–6.
11. Touboul C, Boulvain M, Picone O, Levaillant J-M, Frydman R, Senat M-V. Normal fetal urine production rate estimated with 3-dimensional ultrasonography using the rotational technique (virtual organ computer-aided analysis). Am J Obstet Gynecol. Elsevier; 2008 Jul 1 [cited 2017 Jul 12];199(1):57.e1-57.e5.
12. Takeuchi H, Koyanagi T, Yoshizato T, Takashima T, Satoh S, Nakano H. Fetal urine production at different gestational ages: correlation to various compromised fetuses in utero. Early Hum Dev. 1994 Dec 16 [cited 2017 May 12];40(1):1–11.
13. Lee SM, Park SK, Shim SS, Jun JK, Park JS, Syn HC. Measurement of fetal urine production by three-dimensional ultrasonography in normal pregnancy. Ultrasound Obstet Gynecol. John Wiley & Sons, Ltd.; 2007 Sep 1 [cited 2017 Nov 28];30(3):281–6.
14. Rabinowitz R, Peters MT, Vyas S, Campbell S, Nicolaides KH. Measurement of fetal urine production in normal pregnancy by real-time ultrasonography. Am J Obstet Gynecol. 1989;161(5):1264–6.
15. Stigter RH, Schelven LJ. van, Bruinse HW, Mulder EJH, Gemert MJC. van. On the measurement of fetal bladder volume and urine production: methodological considerations. Prenat neonatal Med. 2000;5:169–76.
16. Baskin L, Meaney D, Landsman A, Zderic SA, Macarak E. Bovine Bladder Compliance Increases with Normal Fetal Development. J Urol [Internet]. Elsevier; 1994 Aug 1 [cited 2018 Mar 20];152(2):692–5.
17. Fontanella F, Duin LK, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M,Willekes C, Bax CJ, Gracchi V, Oepkes D, Bilardo CM. Prenatal diagnosis of LUTO: how to improve diagnostic accuracy. Ultrasound Obstet Gynecol. 2017.
18. Nicolaides KH, Peters MT, Vyas S, Rabinowitz R, Rosen DJD, Campbell S. Relation of rate of urine production to oxygen tension in small-for-gestational-age fetuses. Am J Obstet Gynecol. 1990;162(2):387–91.
19. Taghavi K, Sharpe C, Stringer MD. Fetal megacystis: A systematic review. J Pediatr Urol. 2017;13(1):7–15.
20. Muller F, Dreux S, Vaast P, Dumez Y, Nisand I, Ville Y,Boulot P, Guibourdenche J, Althusser M, Blin G, Gautier E, Lespinard C, Perrotin F, Poulain P, Sarramon MF; Study Group of the French Fetal Medicine Society. Prenatal diagnosis of megacystis-microcolon-intestinal hypoperistalsis syndrome: Contribution of amniotic fluid digestive enzyme assay and fetal urinalysis. Prenat Diagn. 2005;25(3):203–9.
21. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, El-Ghoneimi A, Oury JF, Muller F. Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn. 2013;33(12):1162–6.

32
Chapter 2
22. Maizels M, Alpert SA, Houston JTB, Sabbagha RE, Parilla B V., MacGregor SN. Fetal bladder sagittal length: A simple monitor to assess normal and enlarged fetal bladder size, and forecast clinical outcome. J Urol. 2004;172(5 I):1995–9.
23. Hedriana HL, Moore TR. Accuracy limits of ultrasonograhic estimation of human fetal urinary flow rate. Am J Obstet Gynecol. Mosby; 1994 Oct 1;171(4):989–92.
24. Ioannou C, Sarris I, Salomon LJ, Papageorghiou AT. A review of fetal volumetry: The need for standardization and definitions in measurement methodology. Vol. 38, Ultrasound in Obstetrics and Gynecology. 2011. p. 613–9.
25. Riccabona M, Nelson TR, Pretorius DH, Davidson TE. In vivo three-dimensional sonographic measurement of organ volume: Validation in the urinary bladder. J Ultrasound Med. 1996;15(9):627–32.
26. Rousian M, Koning AHJ, Van Oppenraaij RHF, Hop WC, Verwoerd-Dikkeboom CM, Van Der Spek PJ, Exalto N, Steegers EA. An innovative virtual reality technique for automated human embryonic volume measurements. Hum Reprod. 2010;25(9):2210–6.
27. Peixoto-Filho FM, Sá RAM, Lopes LM, Velarde LGC, Marchiori E, Ville Y. Three-dimensional ultrasound fetal urinary bladder volume measurement: Reliability of rotational (VOCALTM) technique using different steps of rotation. Arch Gynecol Obstet. 2007;276(4):345–9.
28. Hata T, Dater RL. A review of fetal organ measurements obtained with ultrasound: normal growth. J Clin Ultrasound. 1992;Mar-Apr;20.
29. Lee SM, Park SK, Shim SS, Jun JK, Park JS, Syn HC. Measurement of fetal urine production by three-dimensional ultrasonography in normal pregnancy. Ultrasound Obstet Gynecol. 2007;30(3):281–6.
30. Ioannou C, Talbot K, Ohuma E, Sarris I, Villar J, Conde-Agudelo A, Papageorghiou AT. Systematic review of methodology used in ultrasound studies aimed at creating charts of fetal size. BJOG An Int J Obstet Gynaecol. 2012;119(12):1425–39.
31. Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound in Obstetrics and Gynecology. 1993;3(6):378–84.

2
33
Normograms of fetal bladder


3Fetal megacystis: a lot more than LUTO
F. Fontanella, L. Maggio, J.B.G.M. Verheij, L.K. Duin, P.N. Adama van Scheltema, T.E. Cohen – Overbeek, E. Pajkrt, M. Bekker, C. Willekes, C.J. Bax, V. Gracchi, D. Oepkes and C.M. Bilardo
UltrasoundinObstetrandGynecol.2018;inpress

36
Chapter 3
abstract
aim: Megacystis represents a challenge in terms of counseling and management due to its various etiology and evolution. The aim of this study is to present a comprehensive overview of the underlying etiologies and structural anomalies associated with fetal megacystis.
Methods: This was a retrospective multicenter study carried out at the Fetal Medicine Units (FMUs) of the eight Academic Hospitals in the Netherlands. For each case referred to one of these centers due to fetal megacystis, data and measurements of fetal urinary tract and associated structural anomalies were collected. All available postmortem examinations and postnatal investigations were reviewed in order to establish the final diagnosis. In the first trimester, fetal megacystis was defined as a bladder with a longitudinal diameter (LBD) ≥ 7 mm, and in the 2nd and 3rd trimester as an enlarged bladder failing to empty during an extended US examination lasting at least 40 minutes.
results: Out of 541 megacystis, megacystis was isolated (or merely accompanied by other signs of LUTO) in 360 cases (66%); and associated with other abnormal ultrasound findings in 181 cases (34%). The most common associated anomaly was an increased nuchal translucency (NT, 22%), followed by SUA and cardiac defects (10%). A final diagnosis was established in 418 cases, including 222 cases with isolated LUTO (53%) and 60 infants (14%) with normal micturition or isolated urological anomalies. In the remaining 136 cases (33%), a genetic syndrome, developmental or chromosomal abnormality was diagnosed.
In total, 40 chromosomal abnormalities were diagnosed, including: Trisomy 18 (n = 24), Trisomy 21 (n = 5), Turner syndrome (n = 5), Trisomy 13 (n = 3) and deletion 22q11 (n = 3). Thirty-two cases presented with Ano-Rectal Malformations involving anus, rectum and urogenital tract. In cases with confirmed urethral and anal atresia, megacystis occurred early in pregnancy and the bladder appeared severely distended (the longitudinal diameter was equal or greater than twice the gestational age). Fetal macrosomia was detected in 6 cases and an overgrowth syndrome was detected in other 4 cases: 2 infants with Beckwith–Wiedemann and 2 infants with Sotos syndrome. Megacystis-microcolon-intestinal hypoperistalsis syndrome was diagnosed in five cases (1%) and prenatally suspected only in one case.
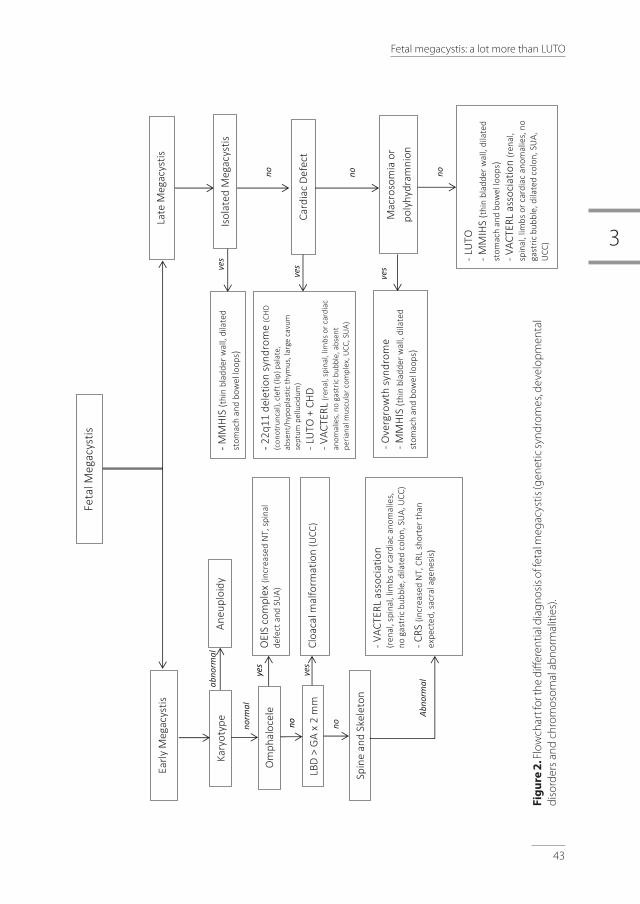
Conclusions: Although the main cause of megacystis is LUTO, an enlarged fetal bladder can also be present as corollary finding of miscellaneous genetic syndromes, developmental disturbances and chromosomal abnormalities. This study provides an overview of the structural anomalies and congenital disorders associated with megacystis and proposes a flowchart for the differential diagnosis of genetic syndromes, chromosomal and developmental abnormalities, focusing on the morphological examination of the fetus.

3
37
Fetal megacystis: a lot more than LUTO
Introduction
Fetal urine production begins at about 10 weeks’ gestation, when the urinary bladder can be identified as an anechoic structure within the fetal pelvis, surrounded by the two umbilical arteries1. The evidence of a distended urinary bladder, also known as megacystis, is an ultrasound finding as easily identifiable as hardly manageable, due to its various etiology and uncertain evolution. In the first-trimester, fetal megacystis is defined by a longitudinal bladder diameter (LBD) greater than 7 mm and is reported in 0.06% of pregnancies (2). Beyond the first trimester, prevalence of megacystis remains unclear and its definition is still ambiguous (3).
The main cause of fetal megacystis, diagnosed at any trimester in pregnancy, is bladder outlet obstruction, also known as Lower Urinary Tract Obstructions (LUTO) (4,5,6). In cases with severe early megacystis, parents often choose for termination of pregnancy. In less severe cases with early megacystis (with LBD ≤12 mm) and negative work-up, a spontaneous resolution often occurs4,6,7. In fetuses surviving the second half of pregnancy LUTO commonly leads to hydronephrosis, renal dysplasia and severe oligohydramnios with a known poor prognosis. However, besides isolated LUTO, the differential diagnosis of fetal megacystis should also include chromosomal abnormalities, genetic syndromes and developmental anomalies. The wide spectrum of etiologies and prognoses makes the counseling and management of this condition particularly challenging (8). Given the low prevalence of megacystis (9,10) and the main focus on LUTO as etiology, the other causes of enlarged bladder have been thus far poorly investigated.
The main aim of this study is to present a comprehensive overview of the underlying etiologies and structural anomalies associated with fetal megacystis and to identify patterns of anomalies and US features related to specific complex anomalies and syndromes, beyond LUTO.
Methods
This study is part of a large retrospective multicenter study carried out at the Fetal Medicine Units (FMUs) of all eight Academic Hospitals in the Netherlands, acting as referral centers for fetal anomalies detected at ultrasound examination. Cases with fetal megacystis were retrieved from local databases according to when registration in the databases had started (from year 2000 to 2014 at Erasmus Medical Center, Academic Medical Center, Amsterdam and at the University Medical Center, Maastricht; between 2004 and 2015 at the University Medical Center Groningen and at the Radboud University Medical Center, Nijmegen; between 2007 and 2014 in the remaining centers). In the first trimester fetal megacystis

38
Chapter 3
was defined as a bladder with longitudinal diameter (LBD) ≥ 7 mm (2), and in the 2nd and 3rd trimester as an enlarged bladder failing to empty during an extended US examination lasting at least 40 minutes (11).
In the Netherlands, all cases suspected for megacystis are referred to one of the eight FMUs for confirmation of diagnosis and further investigations. Cases were referred after either a dating scan, first-trimester scan, 20-week anomaly scan or after a scan performed on other indications later in pregnancy. All cases had undergone a detailed anomaly scan, except for those pregnancies that had not reached the 18th week of gestation (n = 142, including 115 pregnancies terminated and 27 miscarriages). Parents were counseled about the prognosis and informed about the possibility of in-utero treatment. The vesico-amniotic shunt placement was only offered to chromosomally normal male fetuses with isolated signs of LUTO and with concomitant oligohydramnios.
For each case, the following prenatal data were collected: gestational age at diagnosis (GA), longitudinal bladder diameter (LBD) and associated US findings. The LBD was obtained from a mid-sagittal view of the fetus, by measuring the distance from fetal bladder dome to bladder neck. The US findings typically associated with LUTO, such as hydronephrosis, abnormal renal cortical appearance, keyhole sign and oligohydramnios (with eventual compression deformities), were not regarded as associated US anomalies. The nuchal translucency was considered increased if greater than the 95th percentile according to the GA12. We considered the NT measured at referral for cases referred in the first trimester of pregnancy while, in fetuses referred later in pregnancy, we retrospectively collected the NT measurement.
All available postmortem examinations and postnatal investigations were reviewed in order to establish a final diagnosis. LUTO was defined as a bladder outlet obstruction caused by urethral valves, urethral stenosis or urethral atresia. With the term Ano-Rectal Malformation (ARM) reference is made to a group of complex congenital anomalies characterized by an abnormal development of the urorectal septum, therefore resulting in congenital abnormalities of the distal anus, rectum and genitourinary tract13. Among this group, cloacal dysgenesis or cloacal malformations were characterized by the absence of anal, genital and urinary orifices14. VACTERL association was diagnosed if three of the following criteria were met: Vertebral defects, Anal atresia/imperforate anus, Cardiovascular anomalies, Tracheo-esophageal fistula or Esophageal atresia, Renal anomalies and Limb defects (including radial anomalies) in at least two of the three regions involved (thorax, pelvis/lower abdomen and limb)15. Caudal regression spectrum (CRS) was defined by the occurrence of abnormalities at the level of caudal spinal segments, ranging from minor sacrococcygeal malformations to complete absence of sacrum and lumbar spine16. OEIS complex was diagnosed in case of Omphalocele associated with bladder Exstrophy, Imperforate anus and Spinal defect17. Infants without LUTO or other severe congenital

3
39
Fetal megacystis: a lot more than LUTO
abnormalities or congenital syndromes were included in the group with normal urinary tract or isolated urological anomaly, such as vesico-ureteral reflux (VUR) or duplex collecting system. In case of isolated LUTO, the postnatal renal function was evaluated by considering the estimated glomerulaater filtration rate (eGFR): this was calculated using the Schwartz formula and by taking into account the infant’s length and the creatinine nadir in the first year of diagnosis18.
results
During the study period, 541 pregnancies (25 twin and 516 singleton pregnancies) were referred to one of the eight Fetal Medicine Unit in the Netherlands owing to the finding of fetal megacystis. Out of 541 cases, 233 pregnancies (43%) were referred before the 18th week of gestation (early megacystis), and 308 cases (57%) at or after the 18th week of gestation (late megacystis; figure 1). This study has dealt with structural anomalies, genetic syndromes, and developmental or chromosomal abnormalities associated with megacystis. Other outcome measures relative to this cohort have been reported on different studies (4,5,6).
Figure 1. Study population (TOP: 188, IUFD: 50, neonatal death: 68).
TOP, termination of pregnancy; IUFD intrauterine fetal death; NA, not available; MCA, multiple congenital anomalies.
541 Fetal megacystis
233 Early Megacystis (<18th week) 308 Late Megacystis (≥18th week)
188 TOP 50 IUFD
68 Neonatal death 235 Children
418 Final diagnosis
Postmortem examinations (n=139) Prenatal evidence of MCA or abnormal karyotype (n=50) Postnatal examinations (n=229)
Lost to follow-up (n=6) Postmortem examination NA/unclear final diagnosis (n=117)

40
Chapter 3
Fetal megacystis was isolated (or merely associated with other signs of LUTO) in 360 cases (66%), and associated with other abnormal US findings in 181 cases (34%). In 70 cases, more than a single associated anomaly was found and in a total of 293 associated US findings were observed (Table 1). Overall, the most common associated US anomaly was an increased NT (22%), followed by a SUA and cardiac defects (10%).
table 1. Severe anomalies and ultrasound markers associated with fetal megacystis.
Abnormal ultrasound findings(n = 293)
n (%)
NT ≥ 95 centille 64 (22%)
Single umbilical artery 30 (10%)
Cardiac defects 30 (10%)
Ventricular Septal Defect 3 (1%)
Umbilical cord cyst 27 (9%)
Spine or skeletal anomalies 19 (6%)
Sacrococcygealteratoma 1 (0.3%)
Abdominal wall defects 18 (6%)
Urogenital anomalies 15 (5%)
Intrauterine growth restriction 7 (2%)
Macrosomia 6 (2%)
Macroglossia 1 (0.3%)
Central Nervous System 5 (2%)
Cleft lip/palate 3 (1%)
Fetal Hydrops 8 (3%)
Diaphragmatic hernia 3 (1%)
Plexus choroideus cyst 15 (5%)
Echogenic bowel 11 (4%)
Short long bones 6 (2%)
Ventriculomegaly 2 (0.7%)
Echogenic intracardiac focus 2 (0.7%)
Miscellaneous syndromal markers 16 (5%)
*Miscellaneous syndromal marker included: hypertelorism, strawberry skull, micrognathia, club foot.
Overall 88 pregnancies (35%) were terminated, 50 (9%) resulted in intra-uterine deaths (9%), 68 (13%) in neonatal deaths, and 235 (43%) children were live-born. Of the terminated pregnancies, parents did not consent to postmortem examination in 117 (62,2%) cases. Six cases were lost to follow-up (Figure 1). A final causal diagnosis was thus possible in 418 cases (77%), including 222 cases (53%) with isolated LUTO, 60 infants (14%) with another

3
41
Fetal megacystis: a lot more than LUTO
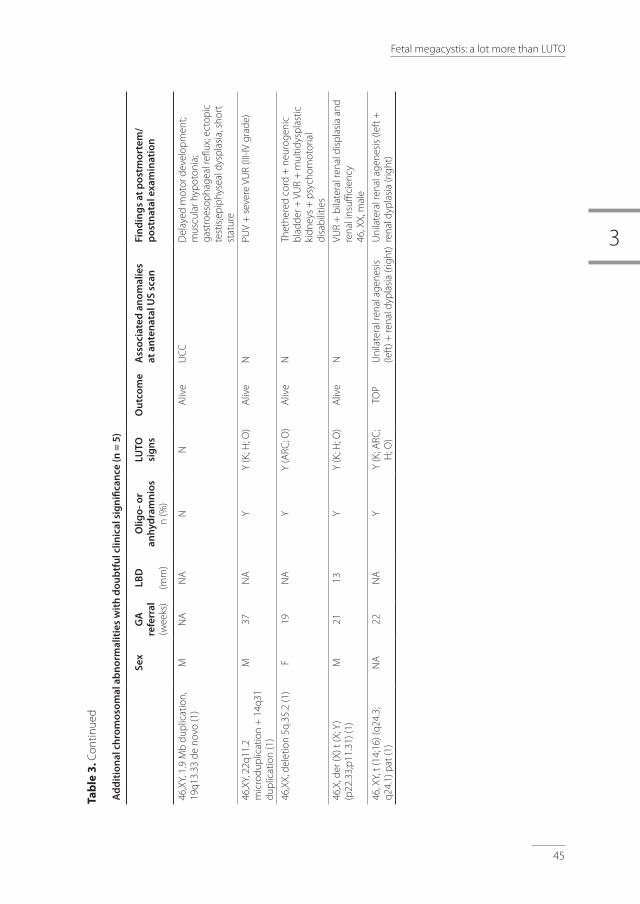
minor isolated urological anomaly or normal urinary tract anomaly at birth and 136 (33%) ‘syndromic’ cases with miscellaneous chromosomal abnormalities, genetic syndromes or developmental anomalies (Table 2). This last group consisted of four categories: 1) major chromosomal abnormalities (n = 40), 2) ARM (n = 32), 3) fetuses with macrosomia or overgrowth genetic syndromes (n = 10) and 4) other cases with multiple congenital abnormalities (MCA) or other miscellaneous genetic syndromes (n = 54). Table 3 summarizes GA at referral, LBD, fetal gender, amniotic fluid (AF) volume, pregnancy outcome and findings at postnatal or postmortem investigations in the syndromic cases. In table 4, we report outcome and postnatal renal function of cases with isolated LUTO.
In total, 40 chromosomal abnormalities were diagnosed (table 2 and 3), with a predominance
of trisomy 18 (24 cases, including 22 with trisomy 18, and 2 with trisomy 18 mosaicisms),
followed by trisomy 21 (5 cases), Turner syndrome (5 cases: 1 with Turner syndrome and 4 with
Turner mosaicisms), trisomy 13 (3 cases) and deletion 22q11 (3 cases). In the chromosomally
abnormal fetuses megacystis was diagnosed at a mean GA of 17 weeks and was associated
with increased NT or other severe structural anomalies. AF volume was normal in 30% of
cases. In addition, 5 fetuses presented with miscellaneous chromosomal abnormalities of
unclear clinical significance and likely unrelated to the observed phenotypes.
table 2. Final diagnosis and GA at diagnosis of 418 fetal megacystis (TOP: 188, IUFD: 50, neonatal death: 68).
Final diagnosis n (%) GA at diagnosis (wks)mean (SD)
LUTO 222 (53%) 22.6 (±7)
Normal micturition at birth or other isolated urological anomaly 60 (14%) 21.7 (±10)
Miscellaneous congenital syndromes 136 (33%) 18.8 (±7)
- Chromosomalabnormalities 40 (10%) 15.3 (±4)
- Anorectal Malformations 32 (8%) 15.9 (±5)
- Fetal Macrosomia or Overgrowth syndrome 10 (2%) 22.7 (±8)
- MCA and other syndromes 54 (13%) 20 (±7)
TOP, termination of pregnancy; IUFD intrauterine fetal death; MCA, multiple congenital anomalies.
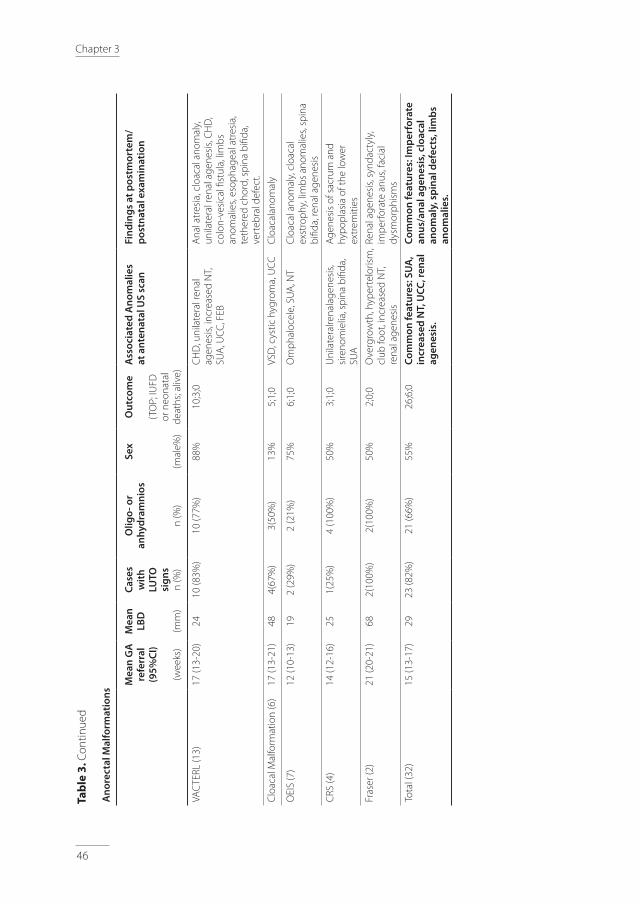
Thirty-two cases presented with a wide spectrum of developmental abnormalities involving anus, rectum and urogenital tract, and classified as ARM. This group included: 13 VACTERL associations, 6 cloacal malformations, 7 OEIS complex, 2 Fraser syndrome and 4 CRS. In fetuses with ARM, megacystis was detected already early in pregnancy (mean GA at referral: 16 weeks). In all cases with urethral and anal atresia, fetal bladder was severely distended with LBD equal or greater than twice the GA, while in case of moderate bladder

42
Chapter 3
distension, with LBD lower than GA x 2 mm, a spinal or vertebral anomaly was found either at the antenatal scan or at the postmortem examination. In this group, the AF volume was reduced in 66% of cases.
Fetal macrosomia was detected in 6 cases and an overgrowth syndrome in other 4 cases: 2 infants with Beckwith–Wiedemann (BWS) and 2 infants with Sotos syndrome.
Megacystis-microcolon-intestinal hypoperistalsis syndrome (MMIHS) was diagnosed in 5 fetuses, 4 of which had normal AF volume during pregnancy. Moreover, a similar phenotype with intestinal hypoperistalsis and detrusor hypotonia was observed in one infant with Ochoa syndrome. Other miscellaneous genetic and structural anomalies observed are reported in Table 3.
Based on the antenatal findings and final diagnosis, a flowchart was designed to guide the differential diagnosis of fetal megacystis and rule out major genetic syndromes and developmental abnormalities (Figure 2).
In our study population, 360 fetuses had isolated megacystis (megacystis without other associated US abnormality or merely with associated signs of LUTO). This subgroup of fetuses showed a better outcome as reported on Figure 3. Their GA at onset of oligo or anhydramnios was related to fetal outcome. This was 17 weeks in the pregnancies that were terminated (n = 116), 20 weeks in pregnancies that ended in a IUFD (n = 19), 24 weeks in those that resulted in a neonatal death (n = 28) and 30 weeks in children that survived (n = 197). Among the 197 alive children, LUTO was confirmed in 129 cases, while in the remaining 70 a normal micturition or an isolated urological anomaly (including vesico-ureteral reflux or duplex collecting system) was diagnosed. A severely impaired renal function within the first year of life (< 30 mL/min/1.73m2) was observed in sixteen children with confirmed LUTO and in only one child without LUTO, but with severe vesico-ureteral reflux.
3
43
Fetal megacystis: a lot more than LUTO
Feta
l Meg
acys
tis
Early
Meg
acys
tis
Kary
otyp
e
- 22q
11 d
elet
ion
synd
rom
e (C
HD
(con
otru
ncal
), cl
eft (
lip) p
alat
e,
abse
nt/h
ypop
last
ic th
ymus
, lar
ge c
avum
se
ptum
pel
luci
dum
) - L
UTO
+ C
HD
- V
ACTE
RL (r
enal
, spi
nal,
limbs
or c
ardi
ac
anom
alie
s, n
o ga
stric
bub
ble,
abs
ent
peria
nal m
uscu
lar c
ompl
ex, U
CC, S
UA)
- O
verg
row
th sy
ndro
me
- MM
HIS
(thi
n bl
adde
r wal
l, di
late
d
stom
ach
and
bow
el lo
ops)
Late
Meg
acys
tis
- VAC
TERL
ass
ocia
tion
(r
enal
, spi
nal,
limbs
or c
ardi
ac a
nom
alie
s,
no g
astr
ic b
ubbl
e, d
ilate
d co
lon,
SU
A, U
CC)
- CRS
(inc
reas
ed N
T, C
RL s
hort
er th
an
expe
cted
, sac
ral a
gene
sis)
- LU
TO
- MM
IHS
(thin
bla
dder
wal
l, di
late
d
stom
ach
and
bow
el lo
ops)
- V
ACTE
RL a
ssoc
iatio
n (r
enal
, sp
inal
, lim
bs o
r car
diac
ano
mal
ies,
no
gast
ric b
ubbl
e, d
ilate
d co
lon,
SU
A,
UCC
)
Om
phal
ocel
e
Aneu
ploi
dy
OEI
S co
mpl
ex (i
ncre
ased
NT,
spin
al
defe
ct a
nd S
UA)
abno
rmal
yes
LBD
> G
A x
2 m
m
Cloa
cal m
alfo
rmat
ion
(UCC
)
Spin
e an
d Sk
elet
on
Abno
rmal
Isol
ated
Meg
acys
tis
- MM
HIS
(thi
n bl
adde
r wal
l, di
late
d
stom
ach
and
bow
el lo
ops )
yes
Card
iac
Defe
ct
Mac
roso
mia
or
poly
hydr
amni
on
norm
al
no
yes
no
yes
yes
no
no
no
Fig
ure
2. F
low
char
t for
the
diffe
rent
ial d
iagn
osis
of f
etal
meg
acys
tis (g
enet
ic sy
ndro
mes
, dev
elop
men
tal
diso
rder
s an
d ch
rom
osom
al a
bnor
mal
ities
).

44
Chapter 3
tab
le 3
. A
nten
atal
det
ails
and
pos
tnat
al o
r po
stm
orte
m fi
ndin
gs in
meg
acys
tys
case
s w
ith g
enet
ic s
yndr
omes
, dev
elop
men
tal o
r ch
rom
osom
al
abno
rmal
ities
.
Ch
rom
osom
al A
bn
orm
alit
ies
Mea
n G
A
refe
rral
(9
5%C
I)
(wee
ks)
Mea
n
LBD
(mm
)
Cas
es
wit
h
LUTO
si
gns
n (%
)
Olig
o- o
r an
hyd
ram
nio
s
n (%
)
Sex
(mal
e%)
Out
com
e
(TO
P; IU
FD
or n
eona
tal
deat
hs; a
live)
Ass
ocia
ted
An
omal
ies
at a
nten
atal
US
scan
Fin
din
gs
at p
ostm
orte
m/
pos
tnat
al e
xam
inat
ion
Tris
omy
18 o
r mos
aici
sm
(24)
17 (1
5-20
)25
21
(88%
)7
(29%
)88
%15
;9;0
Incr
ease
d N
T; C
HD
; UCC
; om
phal
ocel
e; s
kele
tal/
spin
e de
fect
s
CH
D, a
gene
sis
of th
e ce
rebe
llar
verm
is, o
mph
aloc
ele,
clu
bfoo
t
Tris
omy
21 (5
)16
(12-
21)
263
(60%
)3
(60%
)10
0%4;
1;0
Incr
ease
d N
T;
skel
etal
anom
alie
sN
A
Turn
er s
yndr
ome
or
mos
aici
sm (5
)15
(10-
21)
152
(40%
)1
(20%
)40
%3;
1;1
UCC
, inc
reas
ed N
T Im
perf
orat
e an
us, f
acia
l dy
smor
phis
ms,
CH
D
Tris
omy
13 (3
)12
(10-
15)
93
(100
%)
010
0%3;
0;0
CH
D, l
abio
pala
tosc
hisi
s, SU
A, p
olyd
acty
lyN
A
Del
etio
n 22
q11
synd
rom
e (3
)25
313
(100
%)
1 (3
3%)
100%
1;0;
2C
HD
U
nila
tera
l ren
al a
gene
sis,
CH
D,
VUR
Tota
l (40
)17
(15-
18)
2332
(80%
)12
(30%
)82
%26
;11;
3Co
mm
on fe
atur
es:
incr
ease
dNT
Com
mon
feat
ures
: CH
D
3
45
Fetal megacystis: a lot more than LUTO
Ad
dit
ion
al c
hro
mos
omal
ab
nor
mal
itie
s w
ith
dou
btf
ul c
linic
al s
ign
ifica
nce
(n =
5)
Sex
GA
re
ferr
al
(wee
ks)
LBD
(mm
)
Olig
o- o
r an
hyd
ram
nio
sn
(%)
LUTO
si
gns
Out
com
eA
ssoc
iate
d a
nom
alie
s at
ant
enat
al U
S sc
anFi
nd
ing
s at
pos
tmor
tem
/p
ostn
atal
exa
min
atio
n
46,X
Y, 1
.9 M
b du
plic
atio
n,
19q1
3.33
de
novo
(1)
MN
AN
AN
NA
live
UCC
Del
ayed
mot
or d
evel
opm
ent;
mus
cula
r hyp
oton
ia;
gast
roes
opha
geal
reflu
x; e
ctop
ic
test
is;e
piph
ysea
l dys
plas
ia, s
hort
st
atur
e
46,X
Y, 2
2q11
.2
mic
rodu
plic
atio
n +
14q
31
dupl
icat
ion
(1)
M37
NA
YY
(K; H
; O)
Aliv
eN
PUV
+ s
ever
e VU
R (II
I-IV
grad
e)
46,X
X, d
elet
ion
5q.3
5.2
(1)
F19
NA
YY
(ARC
; O)
Aliv
eN
Thet
here
d co
rd +
neu
roge
nic
blad
der +
VU
R +
mul
tidys
plas
tic
kidn
eys
+ p
sych
omot
oria
l di
sabi
litie
s
46,X
, der
(X) t
(X; Y
) (p
22.3
3;p1
1.31
) (1)
M21
13Y
Y (K
; H; O
)A
live
NVU
R +
bila
tera
l ren
al d
ispl
asia
and
re
nal i
nsuffi
cien
cy46
, XX,
mal
e
46, X
Y, t
(14;
16) (
q24.
3;
q24.
1) p
at (1
)N
A22
NA
YY
(K; A
RC;
H; O
)TO
PU
nila
tera
l ren
al a
gene
sis
(left
) + re
nal d
ypla
sia
(rig
ht)
Uni
late
ral r
enal
age
nesi
s (le
ft +
re
nal d
ypla
sia
(rig
ht)
tab
le 3
. Con
tinue
d
46
Chapter 3
tab
le 3
. Con
tinue
d
An
orec
tal M
alfo
rmat
ion
s
Mea
n G
A
refe
rral
(9
5%C
I)
(wee
ks)
Mea
n
LBD
(mm
)
Cas
es
wit
h
LUTO
si
gns
n (%
)
Olig
o- o
r an
hyd
ram
nio
s
n (%
)
Sex
(mal
e%)
Out
com
e
(TO
P; IU
FD
or n
eona
tal
deat
hs; a
live)
Ass
ocia
ted
An
omal
ies
at a
nten
atal
US
scan
Fin
din
gs
at p
ostm
orte
m/
pos
tnat
al e
xam
inat
ion
VAC
TERL
(13)
17 (1
3-20
)24
10 (8
3%)
10 (7
7%)
88%
10;3
;0C
HD
, uni
late
ral r
enal
ag
enes
is, i
ncre
ased
NT,
SU
A, U
CC, F
EB
Ana
l atr
esia
, clo
acal
ano
mal
y,
unila
tera
l ren
al a
gene
sis,
CH
D,
colo
n-ve
sica
l fist
ula,
lim
bs
anom
alie
s, es
opha
geal
atr
esia
, te
ther
ed c
hord
, spi
na b
ifida
, ve
rteb
ral d
efec
t.
Clo
acal
Mal
form
atio
n (6
)17
(13-
21)
484(
67%
)3(
50%
)13
%5;
1;0
VSD
, cys
tic h
ygro
ma,
UCC
Clo
acal
anom
aly
OEI
S (7
)12
(10-
13)
192
(29%
)2
(21%
)75
%6;
1;0
Om
phal
ocel
e, S
UA
, NT
Clo
acal
ano
mal
y, c
loac
al
exst
roph
y, li
mbs
ano
mal
ies,
spin
a bi
fida,
rena
l age
nesi
s
CRS
(4)
14 (1
2-16
)25
1(25
%)
4 (1
00%
)50
%3;
1;0
Uni
late
ralre
nala
gene
sis,
sire
nom
ielia
, spi
na b
ifida
, SU
A
Age
nesi
s of
sac
rum
and
hy
popl
asia
of t
he lo
wer
ex
trem
ities
Fras
er (2
)21
(20-
21)
682(
100%
)2(
100%
)50
%2;
0;0
Ove
rgro
wth
, hyp
erte
loris
m,
club
foot
, inc
reas
ed N
T,
rena
l age
nesi
s
Rena
l age
nesi
s, sy
ndac
tyly
, im
perf
orat
e an
us, f
acia
l dy
smor
phis
ms
Tota
l (32
)15
(13-
17)
2923
(82%
)21
(66%
)55
%26
;6;0
Com
mon
feat
ures
: SU
A,
incr
ease
d N
T, U
CC, r
enal
ag
enes
is.
Com
mon
feat
ures
: Im
per
fora
te
anus
/an
al a
gen
esis
, clo
acal
an
omal
y, s
pin
al d
efec
ts, l
imb
s an
omal
ies.
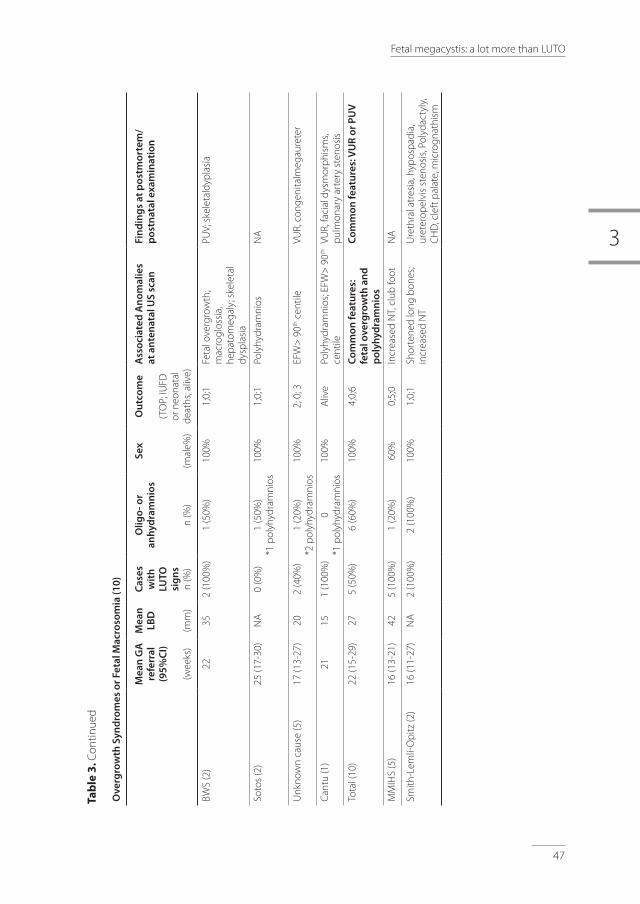
3
47
Fetal megacystis: a lot more than LUTO
Ove
rgro
wth
Syn
dro
mes
or F
etal
Mac
roso
mia
(10)
Mea
n G
A
refe
rral
(9
5%C
I)
(wee
ks)
Mea
n
LBD
(mm
)
Cas
es
wit
h
LUTO
si
gns
n (%
)
Olig
o- o
r an
hyd
ram
nio
s
n (%
)
Sex
(mal
e%)
Out
com
e
(TO
P; IU
FD
or n
eona
tal
deat
hs; a
live)
Ass
ocia
ted
An
omal
ies
at a
nten
atal
US
scan
Fin
din
gs
at p
ostm
orte
m/
pos
tnat
al e
xam
inat
ion
BWS
(2)
2235
2 (1
00%
)1
(50%
)10
0%1;
0;1
Feta
l ove
rgro
wth
; m
acro
glos
sia,
he
pato
meg
aly;
ske
leta
l dy
spla
sia
PUV;
ske
leta
ldyp
lasi
a
Soto
s (2
)25
(17-
30)
NA
0 (0
%)
1 (5
0%)
*1 p
olyh
ydra
mni
os10
0%1;
0;1
Poly
hydr
amni
osN
A
Unk
now
n ca
use
(5)
17 (1
3-27
)20
2 (4
0%)
1 (2
0%)
*2 p
olyh
ydra
mni
os10
0%2;
0; 3
EFW
> 9
0th c
entil
eVU
R, c
onge
nita
lmeg
aure
ter
Cant
u (1
)21
151
(100
%)
0*1
pol
yhyd
ram
nios
100%
Aliv
ePo
lyhy
dram
nios
; EFW
> 9
0th
cent
ileVU
R, fa
cial
dys
mor
phis
ms,
pulm
onar
y ar
tery
ste
nosi
s
Tota
l (10
)22
(15-
29)
275
(50%
)6
(60%
)10
0%4;
0;6
Com
mon
feat
ures
: fe
tal o
verg
row
th a
nd
p
olyh
ydra
mn
ios
Com
mon
feat
ures
: VU
R or
PU
V
MM
IHS
(5)
16 (1
3-21
)42
5 (1
00%
)1
(20%
)60
%0;
5;0
Incr
ease
d N
T, c
lub
foot
NA
Smith
-Lem
li-O
pitz
(2)
16 (1
1-27
)N
A2
(100
%)
2 (1
00%
)10
0%1;
0;1
Shor
tene
d lo
ng b
ones
; in
crea
sed
NT
Ure
thra
l atr
esia
, hyp
ospa
dia,
ur
eter
opel
vis
sten
osis
, Pol
ydac
tyly
, C
HD
, cle
ft p
alat
e, m
icro
gnat
hism
tab
le 3
. Con
tinue
d

48
Chapter 3
Oth
er m
isce
llan
eous
syn
dro
mes
(n =
4)
Sex
GA
at
refe
rral
(w
eeks
)
LBD
(mm
)
Olig
o- o
r an
hyd
ram
nio
sn
(%)
LUTO
si
gns
Out
com
eA
ssoc
iate
d a
nom
alie
s at
ant
enat
al U
S sc
anFi
nd
ing
s at
pos
tmor
tem
/p
ostn
atal
exa
min
atio
n
Mor
ris s
yndr
ome
(1)
M35
570
NA
live
N
Och
oa s
yndr
ome
(1)
M33
540
NA
live
N
Spin
al M
uscu
lar A
trop
hy
(1)
M16
350
Y (K
; ARC
)A
live
NT;
UCC
; Abs
ent D
V;
Hyd
rops
Art
hrog
rypo
sis
+
neur
ogen
icbl
adde
r
Mar
cus
Gun
n Ja
w W
inki
ng
synd
rom
e (1
) M
21N
A0
NA
live
NPU
V +
VU
R +
Dup
lex
Colle
ctin
g sy
stem
GA
, ge
stat
iona
l ag
e; B
LD,
blad
der
long
itudi
nal
diam
eter
; A
F am
ount
, am
niot
ic fl
uid
thro
ugho
ut p
regn
ancy
; O
ligo,
olig
ohyd
ram
nios
; A
ni,
anhy
dram
nios
; Po
li,
polih
ydra
mni
os; C
RS, c
auda
l reg
ress
ion
synd
rom
e; B
WS,
Bec
kwith
-Wie
dem
ann
synd
rom
e; M
MIH
S, m
egac
ystis
-mic
roco
lon-
inte
stin
al h
ypop
eris
tals
is; U
CC, u
mbi
lical
cor
d cy
st; N
T, n
ucha
l tra
nslu
cenc
y ; C
HD
, con
geni
tal h
eart
def
ect;
SUA
, sin
gle
umbi
lical
art
ery;
FEB
, fet
al e
chog
enic
bow
el; V
SD, v
entr
icul
ar s
epta
l def
ect;
N, n
o; N
A, n
ot
avai
labl
e; M
, mal
e; F
, fem
ale;
VU
R, v
esic
o-ur
eter
al re
flux;
EFW
, est
imat
ed fe
tal w
eigh
t; A
RC, A
bnor
mal
rena
l cor
tical
app
eara
nce;
O, o
ligoh
ydra
mio
s ; K
, key
hole
sig
n ; H
, hy
dron
ephr
osis
; A, a
nhyd
ram
nios
; PU
V, p
oste
rior u
reth
ral v
alve
s; VU
R, v
esic
o-ur
eter
al re
flux;
EFW
, est
imat
ed fe
tal w
eigh
t.
tab
le 3
. Con
tinue
d

3
49
Fetal megacystis: a lot more than LUTO
Figure 3. Outcome of fetuses with isolated megacystis.
*The group with normal bladder or isolated urological anomaly includes fetuses without postnatal evidence of LUTO, but normal micturition, vesico-ureteral reflux (VUR) or duplex collecting system.TOP, termination of pregnancy; IUFD, intrauterine fetal death; LUTO, lower urinary tract obstruction
Isolated megacystis
n =360
TOP (n = 116; 32%)
Mean GA at oligo/anhydramnios = 17 (±1) wks
IUFD (n = 19; 5%)
Mean GA at oligo/anhydramnios = 20(±8) wks
Neonatal death (n = 28; 8%)
Mean GA at oligo/anhydramnios = 24 (±4) wks
Alive children (n = 197; 55%)
Mean GA at oligo/anhydramnios = 30 (±5) wks Unclear final diagnosis (n = 8)
Normal bladder or isolated urological anomaly* (n = 60)
- eGFR < 30 (n = 0) - 30 < eGFR < 60 (n = 1) - 60 < eGFR < 90 (n = 3) - eGFR > 90 (n = 6) - Unknown eGFR (n = 58)
Confirmed LUTO (n = 129)
- eGFR < 30 (n = 16) - 30 < eGFR < 60 (n = 20) - 60 < eGFR < 90 (n = 12) - eGFR > 90 (n = 22) - Unknown eGFR (n = 59)

50
Chapter 3
table 4. Outcome and postnatal renal function of cases with isolated LUTO.
Outcome (n = 222)
Termination of pregnancy 54 (24.3%)
Perinatal death 39 (17.6%)
Alive 129 (58.1%)
Cause of obstruction (n = 181)
Posterior urethral valves (PUV) 83 (46%)
Urethral atresia 5 (3%)
Urethral stenosis and others 93 (51%)
Categorical variable are expressed as number and percentage (n, %) Numerical variable are expressed as mean (95%CI) or median. (range)
Discussion
This study shows that, although the main cause of megacystis is LUTO, an enlarged fetal bladder can also be present as corollary finding of miscellaneous genetic syndromes, developmental anomalies and chromosomal abnormalities. The main problem in the work-up of megacystis remains its definition and definition of a standardized antenatal approach (3). With this study we provide an overview of the underlying etiologies and propose a flowchart to guide the differential diagnosis of cases with isolated or associated bladder enlargement.
Megacystis was associated in 1:3 cases. After exclusion of chromosomal anomalies, the most frequently complex anomaly was an ano-rectal-malformation (ARM), diagnosed in 8% of cases. Among this group, fetuses with a cloacal malformation typically presented with a severe and early megacystis with a LBD larger than twice the GA. This anomaly is typically suspected in female fetuses with distended bladder and, behind it, a single or septate anechoic area corresponding to the vagina (19-22). In spite of a predominance in female, we confirm, similarly to other studies (19,14), that a cloacal malformation can also occur in male fetuses.
In 81% of cases (16:32), ARM was part of multisystem anomalies, such as VACTERL association, CRS, OEIS complex and Fraser syndrome. Similarly to Bornes et al., we diagnosed VACTERL association and OIES complex in 20/418 (5%) of fetuses with megacystis. VACTERL association is rarely diagnosed prenatally as the key features, such as anorectal and esophageal atresia (absence of gastric bubble) are not easily detected prenatally (20,21). In fact, absent or small stomach bubble is only present in less than 10% of esophageal atresia, due to the presence of a trachea-esophageal fistula in the majority of cases (22). Similarly, absence of the perianal muscular complex in anorectal atresia is more commonly observed

3
51
Fetal megacystis: a lot more than LUTO
from 23 weeks gestation onwards23,24 and is not part of the routine 20-week scan. In light of this study, we advise to consider this condition in the differential diagnosis of megacystis, in particular if this occurs early in pregnancy with associated spinal, renal, limbs or cardiac defects, single umbilical artery (SUA) and umbilical cord cysts (UCC).
A second striking result of this study was the association of megacystis with overgrowth syndromes (4 cases) and fetal macrosomia. Megacystis was in fact reported in 2 cases of BWS and Sotos syndrome, respectively. In this group, megacystis may be due to a multiplicity of causes: such as obstructive polyps or posterior urethral valves in BWS (25,26,27) and urethral stenosis in Sotos syndrome28, or simply be due to polyuria. Typical antenatal US features of overgrowth syndromes have been described in detail (29), and Vora et al. proposed an algorithm to assist in the differential diagnosis of these syndromes (30). However, it must be remembered that overgrowth/macrosomia is rarely detected at the 20-week scan and in the majority of cases the diagnosis only occurs after birth (30).
MMIHS was only observed in 1% of cases in our cohort. This is a rare syndrome with poor prognosis characterized by a distended non-obstructed bladder and intestinal hypoperistalsis31. MMIHS is considered the most severe form of a spectrum of chronic intestinal pseudo-obstructive disorders, such as to the more common Hirschsprung’s disease (32).The genetic basis of MMIHS has been ascribed to a number of different autosomal dominant and recessive mutations (ACTG2, MYH11 and LMOD1 gene) (33,34,35).
In our study, this syndrome was suspected only in one affected fetus, while in the remaining cases a LUTO was suspected. Prenatal diagnosis of MMIHS is indeed challenging and successful in less than one third of the cases (36). However, discriminating MMIHS from LUTO remains crucial because MMIHS, although usually lethal, is rarely associated with significant renal impairment and thus any form of prenatal bladder drainage would be inappropriate36.
The majority of MMIHS cases in our cohort presented with typical LUTO signs, such as megacystis and bilateral hydronephrosis. This further highlights the importance of considering MMIHS in the differential diagnosis of megacystis with LUTO. To date, this syndrome is typically suspected in female fetuses with coexisting megacystis and normal to increased amniotic fluid. However, in our cohort, fetal gender was not so relevant in predicting MMIHS as three out of five cases were male fetuses. This is in keeping with a systematic review showing that 32% of MMHIS cases occur in boys and polyhydramnios is reported in only 27% of cases (36). For this purpose, we suggest a new clinical score to discriminate LUTO from cases with non-obstructive megacystis (such as MMIHS), and Tuzovic et al. suggested a set of typical US signs of MMIHS, such as dilated fetal stomach, large atonic bladder with a thin wall and dilated bowel loops in the third trimester36. As the gastrointestinal anomalies of MMIHS are scarcely amenable to US diagnosis, fetal MRI can be of help in showing microcolon and dilated esophagus37. Although the genetic base of

52
Chapter 3
MMHIS is heterogeneous and most cases are sporadic, we would recommend that in the presence of the above-mentioned criteria genetic testing for MMHIS should be carried out, especially before prenatal bladder drainage is considered.
In the subgroup of fetuses with isolated megacystis, our outcome data confirm the report by Bornes et al.: with about half (55%) live born and about 1:6 (15%) diagnosed with vesico-ureteral reflux after birth9. However, the most important message of this study is that megacystis can be the common denominator of many more conditions than LUTO only, including complex conditions with poor prognosis such as chromosomal abnormalities or anorectal malformations, as well as merely a sign of isolated urological anomalies with an overall good prognosis.
A limitation of this study is its retrospective nature. In fact, we describe a set of fetal abnormalities and syndromes diagnosed without following a systematic protocol for invasive testing or genetic analyses, but based on local protocols. This implies that other syndromic cases may have been overlooked resulting in an underestimation of the real prevalence of syndromal associations.
To conclude, this study provides an overview of the disorders associated with megacystis and proposes a flowchart (Fig. 2) for the prenatal differential diagnosis of genetic syndromes, chromosomal and developmental abnormalities, focusing on the morphological examination of the fetus. This may be of help in the antenatal work-up and counseling of fetal megacystis.

3
53
Fetal megacystis: a lot more than LUTO
references
1. McHugo J, Whittle M. Enlarged fetal bladders: Aetiology, management and outcome. Prenat Diagn. 2001 Nov;21(11):958-63
2. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8(6):387–90.
3. Taghavi K, Sharpe C, Stringer MD. Fetal megacystis: A systematic review. J Pediatr Urol. 2017;13(1):7–15.
4. Fontanella F, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Oepkes D, Bilardo CM.Antenatal Workup of Early Megacystis and Selection of Candidates for Fetal Therapy. Fetal Diagn Ther. 2018.
5. Fontanella F, Duin LK, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Gracchi V, Oepkes D, Bilardo CM. Prenatal diagnosis of LUTO: how to improve diagnostic accuracy. Ultrasound Obstet Gynecol. 2017.
6. Fontanella F, Duin L, Adama van Scheltema PN, Cohen - Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ CMB. Fetal Megacystis: prediction of spontaneous resolution and outcome. (Ultrasound Obstet Gynecol. 2017 Oct;50(4):458-463
7. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: Chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol. 2003;21(4):338–41.
8. Montemarano H, Bulas DI, Rushton HG, Selby D. Bladder distention and pyelectasis in the male fetus: causes, comparisons, and contrasts. J Ultrasound Med. 1998;17(12):743–9.
9. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: A population-based epidemiological study. BJOG An Int J Obstet Gynaecol. 2012;119(12):1455–64.
10. Al-Hazmi H, Dreux S, Delezoide AL, Dommergues M, Lortat-Jacob S, Oury JF,El-Ghoneimi A, Muller F.Outcome of prenatally detected bilateral higher urinary tract obstruction or megacystis: Sex-related study on a series of 709 cases. Prenat Diagn. 2012;32(7):649–54.
11. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL,El-Ghoneimi A, Oury JF, Muller F. Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn. 2013;33(12):1162–6.
12. Sharifzadeh M, Adibi A, Kazemi K, Hovsepian S. Normal reference range of fetal nuchal translucency thickness in pregnant women in the first trimester, one center study. J Res Med Sci. 2015 Oct;20(10):969–73.
13. Alamo L, Meyrat BJ, Meuwly JY, Meuli RA, Gudinchet F. Anorectal Malformations : Finding the Pathway out of the Lbyrinth. Radiographics. 2013;491–513.
14. Qureshi F, Jacques SM, Yaron Y, Kramer RL, Evans MI, Johnson MP. Prenatal Diagnosis of Cloacal Dysgenesis Sequence: Differential Diagnosis from Other Forms of Fetal Obstructive Uropathy. 1998 Mar-Apr;13(2):69-74.
15. Carli D, Garagnani L, Lando M, Fairplay T, Bernasconi S, Landi A, Presecepe A. VACTERL (vertebral defects, anal atresia, tracheoesophageal fistula with esophageal atresia, cardiac defects, renal and limb anomalies) association: Disease spectrum in 25 patients ascertained for their upper limb involvement. J Pediatr. 2014;164(3):458–462.e2.
16. Boulas MM. Recognition of Caudal Regression Syndrome. Adv Neonatal Care [Internet]. 2009 Apr;9(2):61–9.
17. Carey JC, Greenbaum B, Hall BD. The OEIS complex (omphalocele, exstrophy, imperforate anus, spinal defects). Birth Defects Orig Artic Ser. 1978;14(6B):253–63.
18. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA FS. New Equations to Estimate GFR in Children with CKD. J Am Soc Nephrol. 2009;20:629–37.
19. Banu T, Chowdhury TK, Hoque M, Rahman MAM. Cloacal malformation variants in male. Pediatr Surg Int. 2013 Jul 12;29(7):677–82.
20. Solomon BD. VACTERL/VATER Association. Orphanet J Rare Dis. 2011 Aug 16;6(1):56.
21. Solomon BD, Raam MS, Pineda-Alvarez DE. Analysis of genitourinary anomalies in patients with VACTERL (Vertebral anomalies, Anal atresia, Cardiac malformations, Tracheo-Esophageal fistula, Renal anomalies, Limb abnormalities) association. Congenit Anom (Kyoto). 2011 Jun;51(2):87–91.
54
Chapter 3
22. De Jong EM, De Haan MAM, Gischler SJ, Hop W, Cohen-Overbeek TE, Bax NM, de Klein A, Tibboel D, Grijseels EW. Pre- and postnatal diagnosis and outcome of fetuses and neonates with esophageal atresia and tracheoesophageal fistula. Prenat Diagn. 2010;30(3):274–9.
23. Ochoa JH, Chiesa M, Vildoza RP, Wong AE, Sepulveda W. Evaluation of the perianal muscular complex in the prenatal diagnosis of anorectal atresia in a high-risk population. Ultrasound Obstet Gynecol. 2012;39(5):521–7.
24. Moon MH, Cho JY, Kim JH, Min JY, Yang JH, Kim MY. In-utero development of the fetal anal sphincter. Ultrasound Obstet Gynecol. 2010;35(5):556–9.
25. Buyukcelik M, Satar N, Dursun H, Bayazit Y, Bayazit AK, Soran M, Noyan A, Anarat A. A child with Beckwith-Wiedemann syndrome and posterior urethral valves. Genet Couns. 2005 [cited 2017 Jun 16];16(1):41–4.
26. Anzai Y, Koshida S, Yanagi T, Johnin K, Takeuchi Y. Neonatal urethral polyps associated with Beckwith-Wiedemann syndrome. Pediatr Int. 2013 Oct;55(5):658–61.
27. Bockrath JM, Maizels M, Firlit CF. Benign bladder neck polyp causing tandem obstruction of the urinary tract in a patient with Beckwith-Wiedemann syndrome. J Urol. 1982 Dec;128(6):1309–12.
28. Tatton-Brown K, Rahman N. Sotos syndrome. Eur J Hum Genet. 2007;15(3):264–71.
29. Chen CP. Prenatal findings and the genetic diagnosis of fetal overgrowth disorders: Simpson-Golabi-Behmel syndrome, Sotos syndrome, and Beckwith-Wiedemann syndrome. Taiwan J Obstet Gynecol. 2012;51(2):186–91.
30. Vora N, Bianchi DW. Genetic considerations in the prenatal diagnosis of overgrowth syndromes. Prenat Diagn. 2009;29(10):923–9.
31. Wymer KM, Anderson BB, Wilkens AA, Gundeti MS. Megacystis microcolon intestinal hypoperistalsis syndrome: Case series and updated review of the literature with an emphasis on urologic management. J Pediatr Surg. 2016;51(9):1565–73.
32. Wymer KM, Anderson BB, Wilkens AA, Gundeti MS. Megacystis microcolon intestinal hypoperistalsis syndrome: Case series and updated review of the literature with an emphasis on urologic management. J Pediatr Surg. 2016;51(9):1565–73.
33. Tuzovic L, Tang S, Miller RS, Rohena L, Shahmirzadi L, Gonzalez K, Li X, LeDuc CA, Guo J, Wilson A, Mills A, Glassberg K, Rotterdam H, Sepulveda AR, Zeng W, Chung WK, Anyane-Yeboa K.New Insights into the Genetics of Fetal Megacystis: ACTG2 Mutations, Encoding γ-2 Smooth Muscle Actin in Megacystis Microcolon Intestinal Hypoperistalsis Syndrome (Berdon Syndrome). Fetal Diagn Ther. 2015;38:296–306.
34. Gauthier J, Ouled Amar Bencheikh B, Hamdan FF, Harrison SM, Baker LA, Couture F, Thiffault I, Ouazzani R, Samuels ME, Mitchell GA, Rouleau GA, Michaud JL, Soucy JF. A homozygous loss-of-function variant in MYH11 in a case with megacystis-microcolon-intestinal hypoperistalsis syndrome. Eur J Hum Genet. 2015 Sep 19
35. Halim D, Wilson MP, Oliver D, Brosens E, Verheij JBGM, Han Y,Nanda V, Lyu Q, Doukas M, Stoop H, Brouwer RW, van IJcken WF, Slivano OJ, Burns AJ, Christie CK, de Mesy Bentley KL, Brooks AS, Tibboel D, Xu S, Jin ZG, Djuwantono T, Yan W, Alves MM, Hofstra RM, Miano JM. Loss of LMOD1 impairs smooth muscle cytocontractility and causes megacystis microcolon intestinal hypoperistalsis syndrome in humans and mice.Proc Natl Acad Sci U S A. 2017 Mar 28;114(13):E2739-E2747
36. Tuzovic L, Anyane-Yeboa K, Mills A, Glassberg K, Miller R. Megacystis-Microcolon-Intestinal Hypoperistalsis Syndrome: Case Report and Review of Prenatal Ultrasonographic Findings. Fetal Diagn Ther. 2014;36:74–80.
37. Munch EMS, Cisek LJ, Roth DR. Magnetic Resonance Imaging for Prenatal Diagnosis of Multisystem Disease: Megacystis Microcolon Intestinal Hypoperistalsis Syndrome. Urology. 2009 Sep;74(3):592–4.

3
55
Fetal megacystis: a lot more than LUTO


Fetal Megacystis: prediction of spontaneous resolution and outcome
Fontanella F., Duin L., Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Bilardo CM.
UltrasoundObstetGynecol2017;50:458-63 4

58
Chapter 4
abstract
Objectives: To investigate the natural history of fetal megacystis from diagnosis in utero to postnatal outcome, and to identify prognostic indicators of spontaneous resolution and postnatal outcome after resolution.
Methods: This was a national retrospective cohort study. Fetal megacystis was defined in the first trimester as a longitudinal bladder diameter (LBD) ≥ 7 mm, and in the second and third trimesters as an enlarged bladder failing to empty during the entire extended ultrasound examination. LBD and gestational age (GA) at resolution were investigated with respect to likelihood of resolution and postnatal outcome, respectively. Sensitivity, specificity and area under the receiver–operating characteristics curve (AUC) were calculated.
results: In total, 284 cases of fetal megacystis (93 early megacystis, identified before the 18th week, and 191 late megacystis, identified at or after the 18th week) were available for analysis. Spontaneous resolution occurred before birth in 58 (20%) cases. In cases with early megacystis, LBD was predictive of the likelihood of spontaneous resolution (sensitivity, 80%; specificity, 79%; AUC, 0.84), and, in the whole population, GA at regression was predictive of postnatal outcome, with an optimal cut-off at 23 weeks (sensitivity, 100%; specificity, 82%; AUC, 0.91). In the group with early megacystis, the outcome was invariably good when resolution occurred before the 23rd week of gestation, whereas urological sequelae requiring postnatal surgery were diagnosed in 3/8 (38%) cases with resolution after 23 weeks. In the group with late megacystis, spontaneous resolution was associated with urological complications after birth, ranging from mild postnatal hydronephrosis in infants with resolution before 23 weeks, to more severe urological anomalies requiring postnatal surgery in those with resolution later in pregnancy. This supports the hypothesis that an early resolution of megacystis is often related to a paraphysiological bladder enlargement that resolves early in pregnancy without consequences, while antenatal resolution occurring later in pregnancy (after the 23rd week of gestation) should suggest a pathological condition with urological sequelae.
Conclusions: In fetal megacystis, LBD and GA at regression can be used as predictors of resolution and outcome, respectively. These parameters could help in fine-tuning the prognosis and optimizing the frequency of follow-up scans.
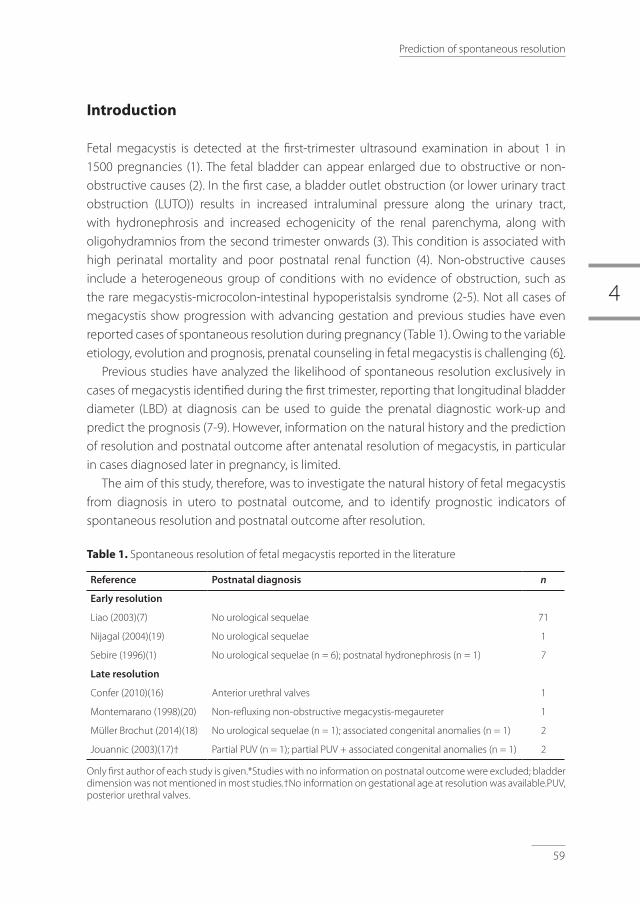
4
59
Prediction of spontaneous resolution
Introduction
Fetal megacystis is detected at the first-trimester ultrasound examination in about 1 in 1500 pregnancies (1). The fetal bladder can appear enlarged due to obstructive or non-obstructive causes (2). In the first case, a bladder outlet obstruction (or lower urinary tract obstruction (LUTO)) results in increased intraluminal pressure along the urinary tract, with hydronephrosis and increased echogenicity of the renal parenchyma, along with oligohydramnios from the second trimester onwards (3). This condition is associated with high perinatal mortality and poor postnatal renal function (4). Non-obstructive causes include a heterogeneous group of conditions with no evidence of obstruction, such as the rare megacystis-microcolon-intestinal hypoperistalsis syndrome (2-5). Not all cases of megacystis show progression with advancing gestation and previous studies have even reported cases of spontaneous resolution during pregnancy (Table 1). Owing to the variable etiology, evolution and prognosis, prenatal counseling in fetal megacystis is challenging (6).
Previous studies have analyzed the likelihood of spontaneous resolution exclusively in cases of megacystis identified during the first trimester, reporting that longitudinal bladder diameter (LBD) at diagnosis can be used to guide the prenatal diagnostic work-up and predict the prognosis (7-9). However, information on the natural history and the prediction of resolution and postnatal outcome after antenatal resolution of megacystis, in particular in cases diagnosed later in pregnancy, is limited.
The aim of this study, therefore, was to investigate the natural history of fetal megacystis from diagnosis in utero to postnatal outcome, and to identify prognostic indicators of spontaneous resolution and postnatal outcome after resolution.
table 1. Spontaneous resolution of fetal megacystis reported in the literature
Reference Postnatal diagnosis n
Early resolution
Liao (2003)(7) No urological sequelae 71
Nijagal (2004)(19) No urological sequelae 1
Sebire (1996)(1) No urological sequelae (n = 6); postnatal hydronephrosis (n = 1) 7
Late resolution
Confer (2010)(16) Anterior urethral valves 1
Montemarano (1998)(20) Non-refluxing non-obstructive megacystis-megaureter 1
Müller Brochut (2014)(18) No urological sequelae (n = 1); associated congenital anomalies (n = 1) 2
Jouannic (2003)(17)† Partial PUV (n = 1); partial PUV + associated congenital anomalies (n = 1) 2
Only first author of each study is given.*Studies with no information on postnatal outcome were excluded; bladder dimension was not mentioned in most studies.†No information on gestational age at resolution was available.PUV, posterior urethral valves.

60
Chapter 4
Methods
This was a national retrospective multicenter study carried out at the Fetal Medicine Units (FMUs) of the eight University Medical Centers in the Netherlands. The time span of data collected from each database was dependent on the period during which data had been stored in the database. This was from January 2000 to the end of 2014 in three centers (Erasmus Medical Center, Rotterdam; Academic Medical Center, Amsterdam; University Medical Center, Maastricht), from January 2004 to the end of 2014 in two centers (University Medical Center, Groningen; Radboud University Medical Center, Nijmegen) and between January 2007 and the end of 2014 in the remaining centers (Leiden University Medical Center, Leiden; Utrecht University Medical Center, Utrecht; Vrije University Medical Center, Amsterdam). These FMUs act as referral centers for all anomalies suspected in peripheral hospitals and external ultrasound clinics in The Netherlands. Fetal megacystis was defined between the 10th and 14th weeks of gestation as LBD ≥ 7 mm, and in the second and third trimesters as an enlarged bladder failing to empty during an extended ultrasound examination lasting at least 40 min. Cases referred either after the routine second-trimester scan or after scans performed later in pregnancy for growth or other obstetric indications were defined as late megacystis, whereas all cases referred before 18 weeks were defined as early megacystis.
Prenatal and postnatal data were collected in all cases. Measurements of LBD at referral, anteroposterior renal pelvic diameter and ureteral enlargement throughout the pregnancy were retrieved from the local databases in 85% of the cases (n = 240), and in the remaining 15% (n = 44) measurements were performed (by F.F.) on suitable images stored in the database with the built-in measurement tool. For subsequent analysis, cases which had been treated with antenatal bladder drainage and terminations of pregnancy were excluded. In continuing pregnancies, the degree of bladder enlargement, together with that of renal pelvis and ureters, was monitored throughout pregnancy by scans performed at regular intervals. Pyelectasis was defined as an anteroposterior renal pelvic diameter ≥ 4 mm or ≥ 7 mm, during the second or third trimester of pregnancy, respectively (10). The megacystis was considered to be resolved if the bladder was observed to be empty following fetal micturition.
For liveborn infants, we collected information on gestational age (GA) at birth, birth weight and final diagnosis, as well as data on postnatal management, surgery and medical examinations. Estimated glomerular filtration rate was calculated using the Schwartz formula (11), using the infant’s length and the creatinine nadir within the first year of diagnosis.
Groups were compared using the chi-square test for categorical variables and independent samples t-test for continuous variables. Receiver–operating characteristics (ROC) curve analysis was used to evaluate the predictive accuracy of LBD and GA at

4
61
Prediction of spontaneous resolution
resolution in predicting the likelihood of resolution and postnatal outcome, respectively. All statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA) and MedCalc (MedCalc, Mariakerke, Belgium) software.
results
We identified from the databases 541 cases of fetal megacystis. Of these, 257 (47.5%) were excluded (Figure 1; Table 2). The natural history, from diagnosis inutero to postnatal outcome, was reviewed in the remaining 284 pregnancies, which included 93 cases of early megacystis (referred before the 18th week) and 191 cases of late megacystis (referred ≥ 18th week). Spontaneous resolution occurred before birth in 58 (20%) cases: in 35 (38%) cases of early and in 23 (12%) cases of late megacystis.
LBD was a good predictor of resolution (area under the ROC curve (AUC), 0.84; Figure 2) for the group with early megacystis, referred before the 18th week, while its reliability was poor when megacystis was diagnosed at or beyond this gestational age (AUC, 0.67; Table 3). Of the 93 cases with early megacystis, 40 had LBD ≤ 12 mm, of which 70% (n = 28) resolved antenatally, and 53 cases had LBD > 12 mm, of which 13% (n = 7) resolved antenatally.
Six infants had no information available for the postnatal period, having been lost to follow-up (Table 4). Overall, after birth, in 33/52 (63%) cases there were no major urological abnormalities found, while 19/52 (37%) infants presented a urological anomaly requiring surgical correction.
GA at spontaneous resolution was a good predictor of the need for urological surgery after birth, with an AUC of 0.91 and an optimal cut-off point at 23 weeks (Figure 3). As shown in Table 5, GA at resolution was accurate in predicting the outcome of the total population, and also separately in the early and the late megacystis groups.
Of the 93 early megacystis cases, antenatal resolution occurred in 35 (38%): in 27 cases before 23 weeks and in eight cases later in pregnancy (Figure 1). Of the 27 cases with resolution before the 23rd week, four were lost to follow-up and the remaining 23 infants did not require any surgical intervention after birth. Conversely, of the eight cases with late resolution, urological surgery was required in 38% (n = 3).

62
Chapter 4
Fig
ure
1: F
low
char
t su
mm
ariz
ing
stud
y po
pula
tion
of c
ases
of f
etal
meg
acys
tis, i
ndic
atin
g nu
mbe
rs w
ith s
pont
aneo
us r
esol
utio
n an
d su
bseq
uent
ou
tcom
e. L
BD, l
ongi
tudi
nal b
ladd
er d
iam
eter
; TO
P, te
rmin
atio
n of
pre
gnan
cy.
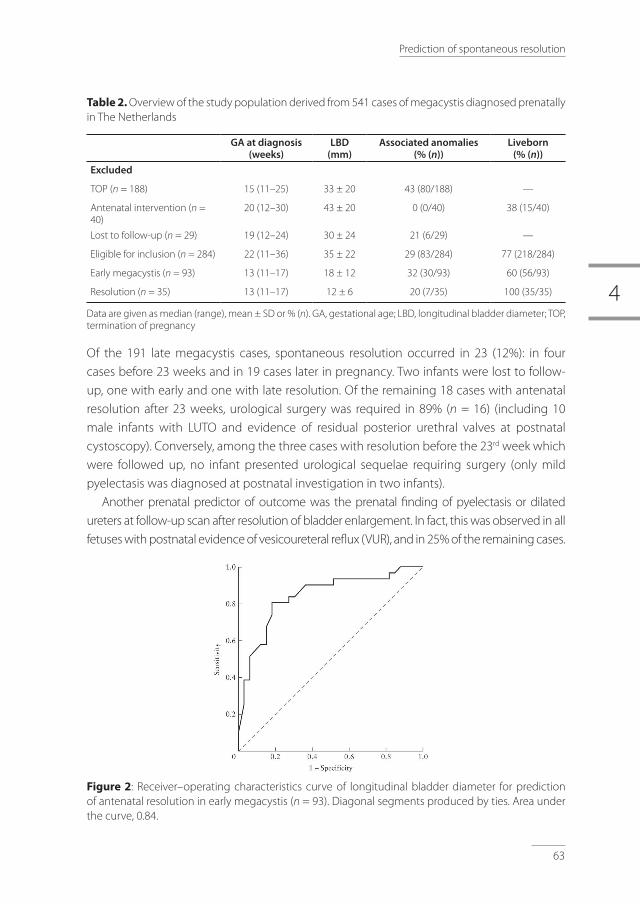
4
63
Prediction of spontaneous resolution
table 2. Overview of the study population derived from 541 cases of megacystis diagnosed prenatally in The Netherlands
GA at diagnosis (weeks)
LBD (mm)
Associated anomalies (% (n))
Liveborn (% (n))
Excluded
TOP (n = 188) 15 (11–25) 33 ± 20 43 (80/188) —
Antenatal intervention (n = 40)
20 (12–30) 43 ± 20 0 (0/40) 38 (15/40)
Lost to follow-up (n = 29) 19 (12–24) 30 ± 24 21 (6/29) —
Eligible for inclusion (n = 284) 22 (11–36) 35 ± 22 29 (83/284) 77 (218/284)
Early megacystis (n = 93) 13 (11–17) 18 ± 12 32 (30/93) 60 (56/93)
Resolution (n = 35) 13 (11–17) 12 ± 6 20 (7/35) 100 (35/35)
Data are given as median (range), mean ± SD or % (n). GA, gestational age; LBD, longitudinal bladder diameter; TOP, termination of pregnancy
Of the 191 late megacystis cases, spontaneous resolution occurred in 23 (12%): in four cases before 23 weeks and in 19 cases later in pregnancy. Two infants were lost to follow-up, one with early and one with late resolution. Of the remaining 18 cases with antenatal resolution after 23 weeks, urological surgery was required in 89% (n = 16) (including 10 male infants with LUTO and evidence of residual posterior urethral valves at postnatal cystoscopy). Conversely, among the three cases with resolution before the 23rd week which were followed up, no infant presented urological sequelae requiring surgery (only mild pyelectasis was diagnosed at postnatal investigation in two infants).
Another prenatal predictor of outcome was the prenatal finding of pyelectasis or dilated ureters at follow-up scan after resolution of bladder enlargement. In fact, this was observed in all fetuses with postnatal evidence of vesicoureteral reflux (VUR), and in 25% of the remaining cases.
Figure 2: Receiver–operating characteristics curve of longitudinal bladder diameter for prediction of antenatal resolution in early megacystis (n = 93). Diagonal segments produced by ties. Area under the curve, 0.84.

64
Chapter 4
Figure 3. Receiver–operating characteristics curve of gestational age at resolution of megacystis for prediction of need for urological surgery after birth in entire cohort (n = 284). Diagonal segments produced by ties. Area under the curve, 0.91.
table 3. Prediction of resolution: performance of longitudinal bladder diameter (LBD) in the prediction of spontaneous resolution in cases of early or late prenatal diagnosis of megacystis and in the entire cohort
LBD cut-off Sensitivity (%) Specificity (%) LR+ LR– AUC (95% CI)
Entire cohort (n = 284) 22 mm 73 83 4.3 0.3 0.83 (0.76–0.90)
Early megacystis (n = 93) 12 mm 80 79 3.9 0.3 0.84 (0.74–0.94)
Late megacystis (n = 191) 22 mm 65 83 3.8 0.4 0.67 (0.52–0.82)
table 4. Infant characteristics and outcome according to gestational age at resolution of fetal megacystis
Resolution
All (n = 58) < 23 weeks (n = 31) ≥ 23 weeks (n = 27) p
Associated ultrasound anomalies 26 (15/58) 23 (7/31) 30 (8/27) NS
No major urological sequelae 63 (33/52) 100 (26/26) 27 (7/26) < 0.01
Urological sequelae requiring surgery
37 (19/52) 0 (0/26) 73 (19/26) < 0.01
Mean eGFR (mL/min/1.73 m2) 98 104 82 < 0.01
Data are given as % (n) unless otherwise stated. Five cases resolving < 23 weeks and one case resolving ≥ 23 weeks were lost to postnatal follow-up.* For difference between resolution < 23 or ≥ 23 weeks of gestation. eGFR, estimated glomerular filtration rate; NS, not significant.

4
65
Prediction of spontaneous resolution
table 5. Prediction of outcome: performance of gestational age (GA) at resolution in the prediction of postnatal urological surgery for bladder enlargement in cases of early or late prenatal diagnosis of megacystis and in the entire cohort
GA cut-off Sensitivity (%) Specificity (%) LR+ LR– AUC (95% CI)
Entire cohort (n = 284) 23 weeks 100 82 5.6 0 0.91 (0.84–0.99)
Early megacystis (n = 93) 23 weeks 100 67 3.0 0 0.88 (0.70–1.00)
Late megacystis (n = 191) 24 weeks 100 84 6.3 0 0.92 (0.81–1.00)
AUC, area under the receiver–operating characteristics curve; LR+/–, positive/negative likelihood ratio.
Discussion
This is the largest study to date on the natural history of fetal megacystis detected at any trimester during pregnancy. We report on the antenatal evolution of 284 cases of early or late diagnosis of megacystis, and on the postnatal outcome of 58 cases which resolved antenatally. Our study shows that LBD is a reliable predictor of spontaneous resolution, particularly of early megacystis, and that GA at resolution is a good predictor of postnatal outcome. From our study it can be inferred that the ideal LBD cut-off associated with antenatal resolution in early megacystis is 12 mm and the critical GA cut-off for an uneventful resolution is 23 weeks.
LBD at the first-trimester scan has been analyzed previously in relation to the risk of chromosomal defects or progression of megacystis. Liao etal.(7) found that about 90% of cases of megacystis with normal karyotype and LBD ≤ 15 mm resolved spontaneously, with all resolving cases presenting LBD ≤ 12 mm. Our study confirms that LBD can indeed be used to inform on the likelihood of spontaneous resolution. Furthermore, the cut-off of 12 mm has been reported in the literature as a method to define cases with moderate first-trimester megacystis (LBD between 12 and 15 mm) (11). Over the last few decades, fetal therapy before 18 or even before 16 weeks, in the form of fetal vesicoamniotic shunt and fetal cystoscopy, has been attempted with the aim of preventing early renal damage. Ruano etal.(11), studying the feasibility of early cystoscopy, considered not eligible for fetal therapy any case with moderate megacystis (LBD, 12–15 mm), performing early fetal cystoscopy only in cases with LBD > 15 mm. Our study confirms that it would be appropriate to exclude from therapy cases with LBD ≤ 12 mm, as in 70% of these cases the bladder enlargement resolved spontaneously.
An interesting finding of this study is the difference in outcome after a diagnosis of megacystis, depending on the timing of resolution, with a worse prognosis in the case of late resolution. In fact, most of the cases resolving at or after the 23rd week required urological surgery after birth, whereas all infants with antenatal resolution before 23 weeks

66
Chapter 4
had a good outcome without major urological sequelae. This finding cannot be compared with those of other published studies as information about resolution is confined to small studies without systematic reporting of postnatal outcome and GA at regression (Table 1).
Thus, in the case of early megacystis the prognosis is good and without urological sequelae if resolution occurs before 23 weeks, whereas major urological sequelae cannot be ruled out in the case of late resolution. The excellent prognosis for infants with early resolution of early megacystis supports the hypothesis of a temporary paraphysiological dilatation of the fetal bladder during the first stages of life, as suggested by Liao etal(7). In fact, autonomic innervation of the bladder and smooth muscle fibers appear only after the 13th week of gestation (12). Therefore, the finding of a dilated bladder before this period can be transient and without any pathological anatomical basis. Conversely, in the case of late megacystis, surgery for LUTO or other urological anomalies was required after birth in 89% of cases with antenatal resolution after the 23rd week of gestation, while no urological sequelae, with the exception of mild pyelectasis postnatally, were recorded in cases with antenatal resolution before 23 weeks.
At follow-up ultrasound examination, even in the presence of apparent fetal micturition, the renal pelvis or ureters remained dilated in all fetuses with postnatal evidence of VUR. Previous studies (13, 14) have shown that a reduction in diameter of a previously enlarged fetal bladder in association with concomitant renal pelvic enlargement does not necessarily indicate ‘micturition’, but rather VUR. In view of these findings, we recommend always including measurements of the renal pelvis both when the bladder appears enlarged and also after resolution. For this purpose, the hydronephrosis index, defined by Leung etal. (15) as the ratio of antero-posterior pelvic diameter/urinary bladder volume, may be helpful in discriminating cases at risk of urological sequelae.
A strength of this study, compared with other large studies in the literature, is that we had data covering at least 6 months of follow-up. Moreover, our follow-up was based mainly on medical reports rather than patient questionnaires, which may reflect only partially the true clinical picture.
An important limitation of our study is that for all cases of late megacystis no information regarding earlier scans was available. This means that we can only assume, and cannot be sure, that the megacystis was late in onset. This also implies that early megacystis cases with spontaneous resolution before the second-trimester scan are not included in the study and the rate of early spontaneous resolution may therefore have been underestimated. Another limitation of this study, and of the other studies investigating second- and third-trimester megacystis, is that there is still no agreement as to which cut-off defines a pathologically enlarged bladder. Previous retrospective studies followed the subjective criteria of a bladder failing to empty over a period of at least 45 min (8, 9). Owing to the retrospective nature of this study, we could not apply this definition, and relied upon the description of fetal

4
67
Prediction of spontaneous resolution
megacystis on the medical reports of extended ultrasound examinations lasting at least 40 min. Further studies are therefore needed in order to establish an objective definition of fetal megacystis during the second and third trimesters.
In conclusion, when faced with a case of early megacystis, the LBD can assist in predicting the chance of resolution, and the outcome will be favorable if resolution occurs before the 23rd week. This applies also to megacystis diagnosed later in pregnancy, as resolution beyond 23 weeks does not exclude urological sequelae. These findings should be of help in informing parents and in deciding upon the optimal medical management of this condition.

68
Chapter 4
references
1. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJ, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol 1996; 8: 387–390.
2. McHugo J, Whittle M. Enlarged fetal bladders: aetiology, management and outcome. Prenat Diagn 2001; 21: 958–963.
3. Clayton DB, Brock JW 3rd. Lower urinary tract obstruction in the fetus and neonate. Clin Perinatol 2014; 41: 643–659.
4. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: a population-based epidemiological study. BJOG 2012; 119: 1455–1464.
5. Tuzovic L, Anyane-Yeboa K, Mills A, Glassberg K, Miller R. Megacystis-microcolon-intestinal hypoperistalsis syndrome: case report and review of prenatal ultrasonographic findings. Fetal Diagn Ther 2014; 36: 74–80.
6. Matias A, Rodrigues M, Mariz C, Monteiro J, Montenegro N. Fetal megacystis as a prenatal challenge: megacystis-microcolon-intestinal hypoperistalsis syndrome in a malefetus. Ultrasound Obstet Gynecol 2013; 41: 345–347.
7. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10–14 weeks of gestation: chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol 2003; 21: 338–341.
8. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, El-Ghoneimi A, Oury JF, Muller F. Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn 2013; 33: 1162–1166.
9. Fievet L, Faure A, Coze S, Harper L, Panait N, Braunstein D, Carson J, Gorincour G, Chaumoitre K, Guys JM, Alessandrini P, D’Ercole C, Merrot T. Fetal megacystis: etiologies, management, and outcome according to the trimester. Urology 2014; 84: 185–190.
10. Corteville JE, Gray DL, Crane JP. Congenital hydronephrosis: correlation of fetal ultrasonographic findings with infant outcome. Am J Obstet Gynecol 1991; 165: 384–388.
11. Ruano R, Yoshisaki CT, Salustiano EM, Giron AM, Srougi M, Zugaib M. Early fetal cystoscopy for first-trimester severe megacystis. Ultrasound Obstet Gynecol 2011; 37: 696–701.
12. Newman J, Antonakopoulos GN. The fine structure of the human fetal urinary bladder: development and maturation. J Anat 1989; 166: 135–150.
13. Satoh S, Inatomi S, Kubota M, Suita S, Nakano H. Antenatal sonographic detection of vesicoureteral reflux. A case report. Fetal Diagn Ther 2002; 17: 277–280.
14. Stewart GD, Ahluwalia A, Gowland M. Case report: diagnosis of fetal vesicoureteric reflux as the cause of pelvicalyceal dilatation on antenatal ultrasound. Clin Radiol 1995; 50: 192–194.
15. Leung VY, Chu WC, Metreweli C. Hydronephrosis index: a better physiological reference in antenatal ultrasound for assessment of fetal hydronephrosis. J Pediatr 2009; 154: 116–120.
16. Confer SD, Galati V, Frimberger D, Kropp BP. Megacystis with an anterior urethral valve: case report and review of literature. J Pediatr Urol 2010; 6: 459–462.
17. Jouannic JM, Hyett JA, Pandya PP, Gulbis B, Rodeck CH, Jauniaux E. Perinatal outcome in fetuses with megacystis in the first half of pregnancy. Prenat Diagn 2003; 23: 340–344.
18. Müller Brochut AC, Thomann D, Kluwe W, Di Naro E, Kuhn A, Raio L. Fetal megacystis: experience of a single tertiary center in Switzerland over 20 years. Fetal Diagn Ther 2014; 36: 215–222.
19. Nijagal A, Sydorak RM, Feldstein VA, Hirose S, Albanese CT. Spontaneous resolution of prenatal megalourethra. J Pediatr Surg 2004; 39: 1421–1423.
20. Montemarano H, Bulas DI, Rushton HG, Selby D. Bladder distention and pyelectasis in the male fetus: causes, comparisons, and contrasts. J Ultrasound Med 1998; 17: 743–749.

4
69
Prediction of spontaneous resolution

Part 2
Antenatal diagnosis and
management of LUTO

Antenatal work-up of early megacystis and selection of candidates for fetal therapy
Fontanella F., Duin L., Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Oepkes D., Bilardo CM.
FetalDiagnosisandTherapy,2018 5

74
Chapter 5
abstract
Objective: To investigate the best criteria for discriminating fetuses with isolated posterior urethral valves from those theoretically not eligible for fetal treatment because of complex megacystis, high chance of spontaneous resolution, and urethral atresia.
Methods: A retrospective national study was conducted in fetuses with megacystis detected before 17 weeks’ gestation (early megacystis).
results: In total, 142 cases with fetal megacystis were included in the study: 52 with lower urinary tract obstruction, 29 with normal micturition at birth, and 61 with miscellaneous syndromal associations, chromosomal and multiple structural abnormalities (complex megacystis). Only a nuchal translucency > 95th centile, and not a longitudinal bladder diameter ≤15 mm (p = 0.24), significantly increased the risk of complex megacystis (p < 0.01). Cases with a high chance of spontaneous resolution were identified by using the cut-off of 12 mm, as demonstrated in a previous study, and the finding of an associated umbilical cord cyst carried a high-risk of urethral atresia (odds ratio: 15; p = 0.026), an unfavorable condition for antenatal treatment. An algorithm encompassing these three criteria demonstrated good accuracy in selecting fetuses theoretically eligible for fetal treatment (specificity 73%; sensitivity 92%).
Conclusions: Cases theoretically eligible for early fetal therapy are those with normal nuchal translucency, a longitudinal bladder diameter > 12 mm, and without ultrasound evidence of umbilical cord cysts.
5
75
Antenatal management of early megacystis
Introduction
An enlarged urinary bladder, also known as megacystis, is a rare ultrasound finding observed in 0.06% [1] of first-trimester pregnancies. This ultrasound anomaly is rather obvious and therefore, it is considered one of the anomalies “expected to be detected” at the currently widely performed first-trimester scans. In 1996, Sebire et al. [1] defined as megacystis a longitudinal bladder diameter (LBD) greater than 7 mm between 11 and 14 weeks’ gestation. The authors described three possible evolutions with different outcomes: chromosomal abnormalities, antenatal spontaneous resolution, or progression to obstructive uropathy [1]. In this historical study, the authors suggested to base the antenatal counseling and workup on the LBD. If this is between 7 and 15 mm, fetal karyotype is recommended, as the majority of chromosomal anomalies falls in this group, and if the karyotype is normal, a spontaneous resolution will occur in 90% of cases; while in cases with LBD > 15 mm, the prognosis is poor, due to a high incidence of lower urinary tract obstruction (LUTO) and subsequent obstructive uropathy.
After the exclusion of cases where spontaneous resolution is likely, first-trimester counseling of fetal megacystis has traditionally been negative, due to the lack of available early therapeutic options [2]. Nowadays, thanks to technical improvements, early fetal therapy has however become plausible [3-5], as it appears that an early intervention is the only strategy potentially capable of preventing the occurrence of renal damage in the very few cases with truly isolated posterior urethral valves (PUV) [3, 6, 7]. In the attempt to identify these rare cases – should parents not consider termination of pregnancy as an option – the challenge remains which criteria should be used to effectively detect first-trimester fetuses with complex megacystis and very poor prognosis, on the one hand, and those with a high chance of spontaneous resolution and favorable prognosis, on the other.
As criterion for triaging fetuses with normal chromosomes and eligible for early intervention, the value of an LBD greater than 15 mm has not yet been extensively tested. Moreover, it is known that, besides chromosomal anomalies, there are other severe causes of complex megacystis that ideally should be identified as soon as possible in order to inform parents on the expected poor prognosis. To date, no effective criteria have been formulated for their identification. Conversely, regarding the prediction of spontaneous resolution, we have recently confirmed the accuracy of the LBD measurement and suggested a new cut-off, i.e., 12 mm, rather than the classic 15 mm, as a more accurate predictor [8].
The aim of this study is therefore to construct a management algorithm aimed at excluding fetuses with complex megacystis or likely to undergo a spontaneous resolution, and at effectively identifying the very few cases with isolated PUV, theoretically eligible for early fetal intervention.

76
Chapter 5
Methods
This was a retrospective multicenter study carried out at the Fetal Medicine Units of the eight University Hospitals in the Netherlands. Cases were collected at the Erasmus Medical Center, Academic Medical Center, Amsterdam, and at the University Medical Center, Maastricht from 2000 to 2015, between 2004 and 2015 at the University Medical Center Groningen and at the Radboud University Medical Center, Nijmegen, and between 2007 and 2014 in the remaining centers. Fetal megacystis was defined as an LBD ≥7 mm [1].
Collected prenatal data of referred cases included: gestational age at diagnosis, LBD, and eventual additional anomalies. The LBD was obtained from a midsagittal view of the fetus, by measuring the distance from fetal bladder dome to bladder neck. Umbilical cord cysts (UCC) were defined as anechoic structures within the umbilical cord eventually described at the ultrasound medical report. The nuchal translucency (NT) was considered increased if greater than the 95th percentile for the gestational age [9]. Final diagnosis was based on postnatal investigations or postmortem examinations. Three main categories of final diagnosis were identified: cases with LUTO, cases with complex megacystis, and cases with normal voiding at birth or isolated urological anomaly. The group with complex megacystis included cases with miscellaneous syndromal associations, chromosomal and multiple structural abnormalities. In 91 cases, a final diagnosis was not established because the pregnancy was terminated, the parents did not consent for the autopsy, and the prenatal investigations were not diagnostic.
In order to identify the candidates for intrauterine surgery, antenatal variables were investigated for their capability of predicting these 4 scenarios: only chromosomal abnormalities; chromosomal abnormalities or other conditions with poor prognosis (complex megacystis); urethral atresia, considered as a very severe form of LUTO; and spontaneous resolution, whereby megacystis is a temporary presentation and the prognosis is mostly benign. The predictors were investigated by using a bivariate logistic regression analysis and the association was described by odds ratios (OR) and 95% confidence intervals (CI). All statistical analyses were performed using SPSS 22.
results
During the study period, 233 pregnancies were referred to one of the eight academic centers in the Netherlands owing to fetal megacystis, detected between the 10th and 17th week of gestation. A clear final diagnosis was possible in 142 cases and included 61 fetuses with complex megacystis, 52 with isolated LUTO, and 29 with normal voiding at birth or isolated urological anomaly (Fig. 1).

5
77
Antenatal management of early megacystis
Figure 1. Study population
ANM, anorectal malformations; LUTO, Lower Urinary Tract Obstruction; PUV, posterior urethral valves.
The group with complex megacystis (n = 61) presented miscellaneous syndromal associations, chromosomal and multiple structural abnormalities and included 28 cases with chromosomal abnormalities (46%), 18 fetuses with anorectal malformations (30%), and 15 cases with other multiple congenital anomalies (25%). LBD and NT were measured at the first ultrasound examination in 124 and 110 pregnancies, respectively.
The most common chromosomal abnormality was trisomy 18 (n = 13; 46%), followed by trisomy 21 (n = 3; 11%), trisomy 13 (n = 3; 11%), Turner syndrome (n = 3; 11%), and other chromosomal abnormalities (n = 6; 21%). The median LBD in fetuses with trisomy 13, 18, and 21 was 8.1 mm, 13 mm, and 24 mm, respectively (Table 1). In total, the LBD was ≤15 mm in 42 cases and > 15 mm in 82 cases, and the incidence of chromosomal abnormalities was 36% (15/42) in the first group and 13% (11/82) in the second group with LBD > 15 mm. Forty-five percent of fetuses with trisomy 18 and 21 had an LBD > 15 mm. Out of 28 cases with abnormal karyotype, 57% (16/28) had an LBD ≤15 mm and 43% (12/28) had an LBD > 15 mm. The accuracy of the classic 15-mm cut-off for the LBD was tested and compared to the accuracy of the NT measurement for identifying fetuses with complex megacystis. The classic criteria of an LBD ≤15 mm slightly increased the risk of chromosomal abnormalities (OR: 0.3 [95% CI: 0.1–0.7], p = 0.01), whereas only an NT > 95th centile, and not an LBD ≤15 mm, significantly increased the risk of complex megacystis in general, including fetuses with miscellaneous syndromal associations, chromosomal and multiple structural abnormalities (NT > 95th centile: OR: 13.7 [95% CI: 3.8–48.5], p < 0.001; LBD ≤15 mm: OR: 0.6 [95% CI: 0.3–1.4], p = 0.24).
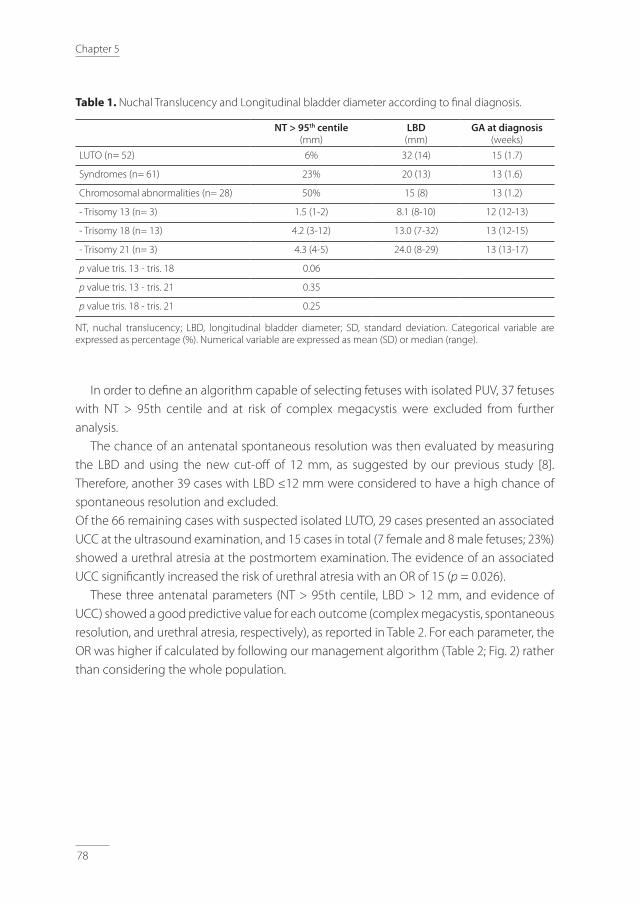
78
Chapter 5
table 1. Nuchal Translucency and Longitudinal bladder diameter according to final diagnosis.
NT > 95th centile(mm)
LBD (mm)
GA at diagnosis(weeks)
LUTO (n= 52) 6% 32 (14) 15 (1.7)
Syndromes (n= 61) 23% 20 (13) 13 (1.6)
Chromosomal abnormalities (n= 28) 50% 15 (8) 13 (1.2)
- Trisomy 13 (n= 3) 1.5 (1-2) 8.1 (8-10) 12 (12-13)
- Trisomy 18 (n= 13) 4.2 (3-12) 13.0 (7-32) 13 (12-15)
- Trisomy 21 (n= 3) 4.3 (4-5) 24.0 (8-29) 13 (13-17)
p value tris. 13 - tris. 18 0.06
p value tris. 13 - tris. 21 0.35
p value tris. 18 - tris. 21 0.25
NT, nuchal translucency; LBD, longitudinal bladder diameter; SD, standard deviation. Categorical variable are expressed as percentage (%). Numerical variable are expressed as mean (SD) or median (range).
In order to define an algorithm capable of selecting fetuses with isolated PUV, 37 fetuses with NT > 95th centile and at risk of complex megacystis were excluded from further analysis.
The chance of an antenatal spontaneous resolution was then evaluated by measuring the LBD and using the new cut-off of 12 mm, as suggested by our previous study [8]. Therefore, another 39 cases with LBD ≤12 mm were considered to have a high chance of spontaneous resolution and excluded.Of the 66 remaining cases with suspected isolated LUTO, 29 cases presented an associated UCC at the ultrasound examination, and 15 cases in total (7 female and 8 male fetuses; 23%) showed a urethral atresia at the postmortem examination. The evidence of an associated UCC significantly increased the risk of urethral atresia with an OR of 15 (p = 0.026).
These three antenatal parameters (NT > 95th centile, LBD > 12 mm, and evidence of UCC) showed a good predictive value for each outcome (complex megacystis, spontaneous resolution, and urethral atresia, respectively), as reported in Table 2. For each parameter, the OR was higher if calculated by following our management algorithm (Table 2; Fig. 2) rather than considering the whole population.
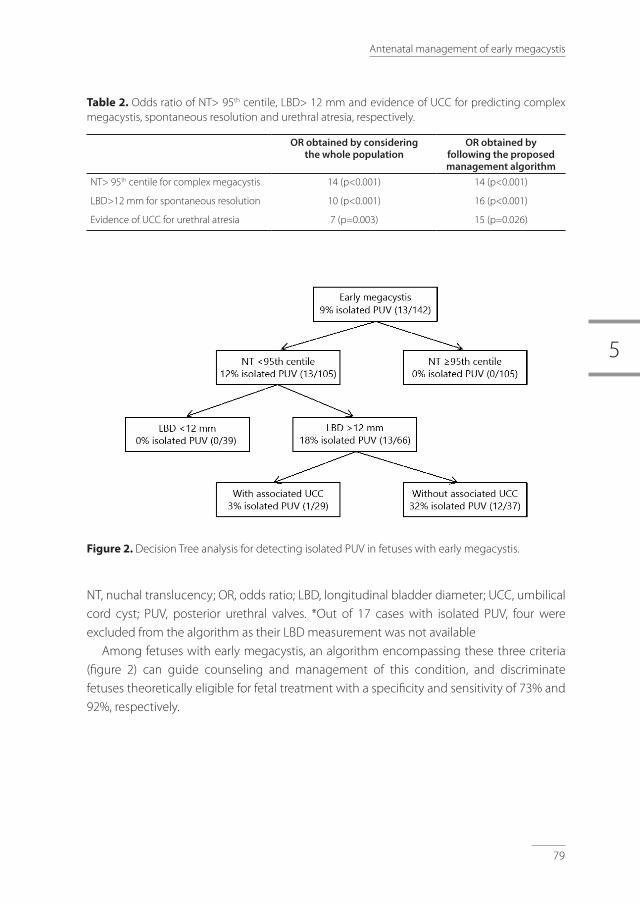
5
79
Antenatal management of early megacystis
table 2. Odds ratio of NT> 95th centile, LBD> 12 mm and evidence of UCC for predicting complex megacystis, spontaneous resolution and urethral atresia, respectively.
OR obtained by consideringthe whole population
OR obtained by following the proposed management algorithm
NT> 95th centile for complex megacystis 14 (p<0.001) 14 (p<0.001)
LBD>12 mm for spontaneous resolution 10 (p<0.001) 16 (p<0.001)
Evidence of UCC for urethral atresia 7 (p=0.003) 15 (p=0.026)
Figure 2. Decision Tree analysis for detecting isolated PUV in fetuses with early megacystis.
NT, nuchal translucency; OR, odds ratio; LBD, longitudinal bladder diameter; UCC, umbilical cord cyst; PUV, posterior urethral valves. *Out of 17 cases with isolated PUV, four were excluded from the algorithm as their LBD measurement was not available
Among fetuses with early megacystis, an algorithm encompassing these three criteria (figure 2) can guide counseling and management of this condition, and discriminate fetuses theoretically eligible for fetal treatment with a specificity and sensitivity of 73% and 92%, respectively.

80
Chapter 5
Discussion
This study shows that in fetuses with early megacystis, the best criteria to guide the parental counseling and select cases with isolated PUV are: a normal NT, an LBD greater than 12 mm, and absence of UCC. These criteria demonstrated good accuracy in evaluating the risk of complex megacystis, spontaneous resolution, and urethral atresia, and in selecting those fetuses theoretically eligible for antenatal treatment.
Historically, an LBD greater or lower than 15 mm was used to evaluate the chance of chromosomal abnormalities or spontaneous resolution [1, 10, 11]. In this study, we showed that an enlarged NT, rather than the LBD measurement, significantly increased the risk of complex megacystis, including fetuses with miscellaneous syndromal associations, chromosomal and multiple structural abnormalities carrying a poor prognosis. We recently demonstrated that the optimal LBD cut-off to predict the chance of spontaneous resolution of megacystis is 12 mm, rather than 15 mm. Therefore, to sum up, the LBD should be considered only as predictor of spontaneous resolution [8], while the NT measurement should be taken into account as predictor of complex megacystis.
Further support to this finding is provided by the prospective study by Syngelaki et al. [12], including 108,982 pregnancies undergoing first-trimester screening. This large study reported a similar distribution of chromosomal abnormalities in cases with megacystis with LBD > 15 or ≤15 mm, and suggested to base the decision for in vasive testing on the results of the combined test or, alternatively, offer cfDNA [12]. This new approach is at variance with the commonly used management protocol for first-trimester megacystis, based on the study by Liao et al. [10]. The discrepancy in results is probably due to the different distribution in chromosomal anomalies between our study, that of Syngelaki et al. [12], and Liao et al.’s study [10]. In fact, similarly to our study, Syngelaki et al. [12] reported trisomy 18 as the most common chromosomal abnormality in fetuses with first-trimester megacystis (5/15; 33%), followed by trisomy 21 (4/15; 27%) and trisomy 13 (3/15; 20%) [12], whereas in the study by Liao et al. [10], the most common chromosomal abnormality in fetuses with megacystis was trisomy 13 (17/29; 59%), followed by trisomy 18 (7/29; 24%) and, as least frequent, by trisomy 21, found in only 7% of cases (2/29; 7%). In this study, we observed that, in fetuses with trisomy 13, megacystis is typically mildly enlarged (mean LBD: 8.7 mm), whereas cases with trisomy 18 and 21 show a more severe degree of bladder distension (mean LBD: 20 and 15 mm, respectively). To date, the pathological background of fetal obstructive uropathy in trisomic fetuses has not yet been fully clarified [13]. We speculate that, among trisomies, there may be a different underlying cause of megacystis, with a varying degree of bladder enlargement, depending on the type of chromosomal abnormality. Hence, an obstructive uropathy is more commonly reported in fetuses with trisomy 18 and 21, but rarely in trisomy 13 [13-15]. Therefore, the different prevalence of trisomies between the studies may explain

5
81
Antenatal management of early megacystis
the divergent results. In light of the prospective nature and the size of Syngelaki et al.’s study [12], this is more likely to reflect the true distribution of chromosomal anomalies in fetuses with first-trimester megacystis.
Since the study by Liao et al. [10], there has been an increased interest in fetal therapy for LUTO. Recent studies have suggested that antenatal treatment improves perinatal survival, but with little effect on postnatal renal function [16-18]. This is probably due to the fact that renal parenchyma is in most cases already damaged at the time of fetal intervention. Animal studies have demonstrated a correlation between early LUTO and severity of renal damage, thus suggesting that an early treatment, although technically more challenging, may potentially improve the outcome [19, 20]. New therapeutic attempts, based on recent technical improvements, aim at sparing renal function starting from 14–16 weeks’ gestation [3-5]. In this context, it has become extremely important to be able to select, as early as possible, fetuses eligible for timely treatment, should the parents choose for this option. Among cases with LUTO, fetuses with urethral atresia often present other associated developmental abnormalities and a poorer prognosis, compared to those with PUV [21]. Furthermore, in cases with urethral atresia, fetal cystoscopy, which specifically attempts to ablate the PUV, is not indicated [17]. Urethral atresia is commonly considered in female fetuses without keyhole sign. However, in our cohort, after excluding fetuses at risk of complex megacystis and spontaneous resolution, half of the fetuses (8/15) with urethral atresia were male, and other studies have already demonstrated that the keyhole sign is not a reliable predictor of PUV [22]. No previous study has so far found other reliable antenatal signs for this subtle differential diagnosis in the first trimester.
In the literature, UCC are reported at the first-trimester scan in 0.4–3.4% of cases [23]. In our cohort, we found a UCC in 12% (29/233) of fetuses with early megacystis. Previous studies have suggested that UCC may be an early sign of severe obstructive uropathy [24, 25]. This study is the first to clearly indicate that evidence of a UCC in conjunction with a megacystis is a strong marker of urethral atresia, already from the first trimester of pregnancy. A plausible explanation for the association between megacystis and urethral atresia is that during the first stages of life, the bladder is connected with the umbilical cord through the allantois, which obliterates at 6–12 weeks’ gestation to form the urachus, a fibromuscular tubular structure located between the apex of the bladder and the umbilical cord insertion. An abnormally distended urinary bladder could prevent the closure of the allantois and eventually lead to a cystic dilatation of the allantois or of the umbilical cord [25, 26]. This is more likely to occur in fetuses with an early and severe bladder enlargement, as it is the case in the setting of urethral atresia. This is another useful element to take into account when counseling parents on both prognosis and therapeutic options of fetal megacystis.
An important limitation of this study in assessing the real prevalence of UCC is that a complete examination of the umbilical cord, from placental to fetal insertion, was not

82
Chapter 5
routinely performed. We speculate that if this would have been done, theoretically even more UCC may have been seen. A second limitation is that, in this national cohort, the parental counseling was guided by Liao et al.’s results [10] and fetal karyotype was mainly recommended to fetuses with LBD ≤15 mm. Although this approach may have affected our results, the impact of this bias has been minimized by establishing the final diagnosis according to both postnatal and postmortem examinations, rather than only considering antenatal scans and fetal karyotype.
To summarize, we propose a new approach in the management and counseling of fetuses with early megacystis. Karyotyping should be offered more liberally and, for the detection of fetuses with complex megacystis, the focus should be on the NT rather than on the LBD. Moreover, cases with a high chance of spontaneous resolution should be identified by using the cut-off of 12 mm, as previously demonstrated. Besides this, the finding of a UCC should be regarded as an unfavorable prognostic factor because of its association with urethral atresia. Therefore, a thorough routine inspection of the umbilical cord should be carried out in all cases of megacystis to identify fetuses at risk of urethral atresia. We have summarized these recommendations in a flowchart to guide the antenatal workup and counseling in early megacystis cases, aiming at identifying fetuses with PUV only, theoretically eligible for early antenatal treatment.

5
83
Antenatal management of early megacystis
references
1. Sebire NJ, Von Kaisenberg C, Rubio C, Snij ders RJM, Nicolaides KH: Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol 1996; 8: 387–390.
2. Jouannic J-M, Hyett JA, Pandya PP, Gulbis B, Rodeck CH, Jauniaux E: Perinatal outcome in fetuses with megacystis in the first half of pregnancy. Prenat Diagn 2003; 23: 340–344.
3. Ruano R, Yoshisaki CT, Salustiano EMA, Giron AM, Srougi M, Zugaib M: Early fetal cystoscopy for first-trimester severe megacystis. Ultrasound Obstet Gynecol 2011; 37: 696–701.
4. Kim SK, Won HS, Shim JY, Kim KS, Lee PR, Kim A: Successful vesicoamniotic shunting of posterior urethral valves in the first trimester of pregnancy. Ultrasound Obstet Gynecol 2005; 26: 666–668.
5. Dębska M, Kretowicz P, Olędzka A, Gastoł P, Dangel J, Świątkowska-freund M, Dębski R: Early vesico-amniotic shunting – does it change the prognosis in fetal lower urinary tract obstruction diagnosed in the first trimester ? Ginekol Pol 2017; 88: 486–491.
6. Carroll SGM, Soothill PW, Tizard J, Kyle PM: Vesicocentesis at 10–14 weeks of gestation for treatment of fetal megacystis. Ultrasound Obstet Gynecol 2001; 18: 366–370.
7. Ruano R, Yoshisaki CT, Salustiano EMA, Giron AM, Srougi M, Zugaib M: Early fetal cystoscopy for first-trimester severe megacystis. Ultrasound Obstet Gynecol 2011; 37: 696–701.
8. Fontanella F, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Bilardo CM: Fetal megacystis: prediction of spontaneous resolution and outcome. Ultrasound Obstet Gynecol 2017; 50: 458–463.
9. Sharifzadeh M, Adibi A, Kazemi K, Hovsepian S: Normal reference range of fetal nuchal translucency thickness in pregnant women in the first trimester, one center study. J Res Med Sci 2015; 20: 969–973.
10. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH: Megacystis at 10–14 weeks of gestation: chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol 2003; 21: 338–341.
11. Kagan KO, Staboulidou I, Syngelaki A, Cruz J, Nicolaides KH: The 11–13-week scan: diagnosis and outcome of holoprosencephaly, exomphalos and megacystis. Ultrasound Obstet Gynecol 2010; 36: 10–14.
12. Syngelaki A, Guerra L, Ceccacci I, Efeturk T, Nicolaides KH: Impact of holoprosencephaly, exomphalos, megacystis and high NT in first trimester screening for chromosomal abnormalities. Ultrasound Obstet Gynecol 2017; 50: 45–48.
13. Hoagland MH, Frank KA, Hutchins GM: Prune-belly syndrome with prostatic hypoplasia, bladder wall rupture, and massive ascites in a fetus with trisomy 18. Arch Pathol Lab Med 1988; 112: 1126–1128.
14. Qureshi F, Jacques SM, Feldman B, Doss BJ, Johnson A, Evans MI, Johnson MP: Fetal obstructive uropathy in trisomy syndromes. Fetal Diagn Ther 2000; 15: 342–347.
15. Frydman M, Magenis RE, Mohandas TK, Kaback MM: Chromosome abnormalities in infants with prune belly anomaly: association with trisomy 18. Am J Med Genet 1983; 15: 145–148.
16. Nassr AA, Shazly SAM, Abdelmagied AM, Araujo Júnior E, Tonni G, Kilby MD, Ruano R: Effectiveness of vesico-amniotic shunt in fetuses with congenital lower urinary tract obstruction: an updated systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017; 49: 696–703.
17. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R: Fetal intervention for severe lower urinary tract obstruction: a multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol 2015; 45: 452–458.
18. Morris RK, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan SK, Deeks J, Kilby MD; Percutaneous vesicoamniotic shunting in Lower Urinary Tract Obstruction (PLUTO) Collaborative Group: Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): a randomised trial. Lancet 2013; 382: 1496–1506.
19. Glick PL, Harrison MR, Noall RA, Villa RL: Correction of congenital hydronephrosis in utero III. Early mid-trimester ureteral obstruction produces renal dysplasia. J Pediatr Surg 1983; 18: 681–687.
20. McVary KT, Maizels M: Urinary obstruction reduces glomerulogenesis in the developing kidney: a model in the rabbit. J Urol 1989; 142: 646–651.
21. Haeri S: Fetal Lower Urinary Tract Obstruction (LUTO): a practical review for providers. Matern Heal Neonatol Perinatol 2015; 1: 26.
84
Chapter 5
22. Bernardes LS, Aksnes G, Saada J, Masse V, Elie C, Dumez Y, Lortat-Jacob SL, Benachi A: Keyhole sign: how specific is it for the diagnosis of posterior urethral valves? Ultrasound Obstet Gynecol 2009; 34: 419–423.
23. Ross JA, Jurkovic D, Zosmer N, Jauniaux E, Hacket E, Nicolaides KH: Umbilical cord cysts in early pregnancy. Obstet Gynecol Surv 1997; 89: 442–445.
24. Sepulveda W, Rompel SM, Cafici D, Carstens E, Dezerega V: Megacystis associated with an umbilical cord cyst: a sonographic feature of a patent urachus in the first trimester. J Ultrasound Med 2010; 29: 295–300.
25. Riddell JVB, Houle AM, Franc-Guimond J, Barrieras D: Prenatal vesico-allantoic cyst outcome – a spectrum from patent urachus to bladder exstrophy. Prenat Diagn 2015; 35: 1342–1346.
26. Sepulveda W, Rompel SM, Cafici D, Carstens E, Dezerega V: Megacystis associated with an umbilical cord cyst. J Ultrasound Med 2010; 29: 295–300.

5
85
Antenatal management of early megacystis


Prenatal diagnosis of LUTO: improving diagnostic accuracy
Fontanella F., Duin L., Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Gracchi V, Oepkes D, Bilardo CM.
UltrasoundinobstetricsandGynecol,inpress 6

88
Chapter 6
abstract
Objective: To propose a clinical score for the optimal antenatal diagnosis of Lower Urinary Tract Obstruction (LUTO) in the second trimester of pregnancy, as alternative to the commonly used ultrasound (US) triad (megacystis, keyhole sign and hydronephrosis).
Methods: This was a national retrospective study carried out at the eight tertiary Fetal Medicine Units (FMUs) in the Netherlands. Only cases referred for megacystis starting from the second trimester and with clear postnatal diagnosis were included in the study. The following antenatal data was collected at referral: amniotic fluid volume, renal cortical appearance, hydronephrosis, bladder volume, fetal ascites, ureteral size, keyhole sign, fetal sex and gestational age at referral. A multivariate analysis was performed starting with the inclusion of all antenatal variables and then excluding the weakest predictors by the backward stepwise strategy.
results: Over a seven-year period, 312 fetuses with a diagnosis of megacystis were referred to one of the eight Dutch tertiary FMUs. A final diagnosis was achieved in 143 cases, including 124 cases of LUTO and 19 cases reclassified after birth as non-obstructive megacystis. The optimal bladder volume cut-off for prediction of LUTO was 35 cm3 (Area Under Curve (AUC)=0.7, p=0.03). On the base of the multivariate analysis, a clinical score was formulated. This included: fetal sex, degree of bladder distension, ureteral size, presence of oligohydramnios and GA at referral. The combination of these five variables demonstrated good accuracy in discriminating LUTO from non-obstructive megacystis (AUC=0.84), compared to the poor performance of the US triad (AUC=0.63, p=0.07).
Conclusions: We propose a clinical score that combines five antenatal variables for the prospective diagnosis of congenital LUTO. This score showed good discriminative capacity in predicting LUTO, and better diagnostic accuracy compared to the classic US triad. Future studies to validate these results are needed in order to refine the antenatal management of LUTO and prevent inappropriate fetal interventions.

6
89
Prenatal diagnosis of LUTO
Introduction
The term Lower Urinary Tract Obstruction (LUTO) refers to an heterogeneous group of anatomical anomalies causing an obstruction in the urethra (1). During fetal life, LUTO entails a sequence of events detectable at the antenatal US scan. This typically starts with the evidence of distended fetal bladder (megacystis) accompanied by hydronephrosis and progressing to renal dysplasia with abnormal renal parenchymal appearance at US scan and, eventually resulting in severe oligohydramnios (2). The condition has high mortality and postnatal morbidity due to lung hypoplasia and impaired renal function (3). When LUTO is suspected in the first trimester and a megacystis greater than 12 mm is seen, the prognosis is extremely poor and parents often opt for termination of pregnancy (4)(5). For cases identified later in pregnancy no hard criteria for defining LUTO and predicting the exact prognosis have yet been proposed (6). Beyond the first trimester, the diagnosis of LUTO is typically based on the evidence of three US findings: megacystis, dilated posterior urethra (known as keyhole sign), and either unilateral or bilateral hydronephrosis.
Over the last 20 years, fetal therapy has been attempted on the assumption that by relieving the intra-cavitary pressure caused by the obstruction, mortality ad renal damage could possibly be prevented. The PLUTO trial investigated this assumption, demonstrated a significant improvement of survival in fetuses treated with vesico-amniotic shunt, and reported an high morbidity among survivors irrespective of the antenatal management (7). To date, whether and when the in-utero treatment should be offered remains a matter of debate, and the eventual selection of candidates is still suboptimal, owing to the high number of false-positive LUTO cases. In fact, a previous study has reported that one third of all prenatally suspected LUTO cases are reclassified postnatally, the majority of them to vesico-ureteral reflux (VUR) (9). For this reason, an improvement in the diagnostic accuracy of US for the diagnosis of LUTO is needed.
The aim of this study was to identify the optimal combination of US parameters for the antenatal diagnosis of LUTO as alternative to the commonly used LUTO triad (megacystis, keyhole sign and hydronephrosis).

90
Chapter 6
Methods
This was a retrospective national study carried out at all eight Fetal Medicine Units (FMUs) of University Hospitals in the Netherlands. Cases were collected according to the start of registration in databases: this was from 2000 to 2015 in three centers (Erasmus Medical Center, Rotterdam; Academic Medical Center, Amsterdam; University Medical Center, Maastricht); from 2004 to 2015 in two centers (University Medical Center Groningen and Radboud University Medical Center, Nijmegen); and between 2007 and 2014 in the remaining centers (Leiden University Medical Center, Leiden; Utrecht University Medical Center, Utrecht; VU University Medical Center, Amsterdam). These FMUs act as expert referral center for all anomalies suspected in peripheral hospitals and external ultrasound clinics in the Netherlands. We only included cases referred for fetal megacystis diagnosed from the 18th week’s gestation onwards, thus either directly after the routine second-trimester scan or after US scans performed later in pregnancy for growth or other obstetrical indications. Fetal megacystis was defined as an enlarged bladder failing to empty during an extended US examination lasting at least 40 minutes.
The following antenatal data were collected at referral: gestational age, fetal sex, evidence of keyhole sign, or fetal ascites (caused by leakage or rupture of the distended bladder), hydronephrosis, amount of amniotic fluid, renal cortical appearance, size of right and left ureteral diameter, and antero-posterior, transverse and longitudinal bladder diameter. The bladder volume was calculated using the formula: longitudinal diameter x transverse diameter x antero-posterior diameter x π/6 (10). The sum of right and left ureteral diameter was calculated for each case, and for ureters non-visualized at the US scan the sum was considered as zero millimeters. Amniotic fluid was considered reduced in case of a single deepest pocket (SDP) of less than 2 cm. US reports were reviewed in order to retrieve data on amniotic fluid volume, renal pelvis dilatation and renal parenchymal echogenicity. Only the first detailed US report at referral was used for analysis.
Outcome data included all available postnatal data on surgeries and medical examinations for live-born infants, and postmortem examinations for perinatal deaths, when available. The term LUTO referred to a group of anatomical anomalies causing urethral obstruction (1). This group thus included cases with posterior urethral valves (PUV), urethral stenosis, urethral atresia, and also cases with LUTO reported as final diagnosis, but without further details concerning the type of obstruction (non-specified LUTO).
Antenatal baseline characteristics were compared using the chi-square test or Fisher’s exact test for categorical variables and the Student’s t test for continuous variables. Univariate analysis was performed to examine the association between candidate predictors and final diagnosis. A logistic model was developed considering eight variables first, and then proceeding by the backward stepwise strategy in excluding progressively

6
91
Prenatal diagnosis of LUTO
the weakest predictors. The model performances were assessed by the Hosmer-Lemeshow test for goodness of fit, and the discriminative performance in the model was evaluated by the area under the receiver-operating characteristic (ROC) curve using the predicted and the actual outcome. The model was internally validated with bootstrapping using R-project software 3.4.2 (https://www.r-project.org/; package rms).
A clinical score was developed based on the results of the logistic model. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Data analyses were performed using the statistical software package SPSS Statistics 23 (SPSS Inc., Chicago, IL, USA).
results
During the study period in total 312 pregnancies were referred because of a suspected fetal megacystis from the 18th week onwards. The outcome of the 312 pregnancies was: 71 terminations of pregnancies (TOP), 10 cases of intrauterine fetal death (IUFD), 38 neonatal deaths, and 193 live-born infants. Ninety-eight cases (31%) were excluded from the study because of missing or incomplete data not enabling a final diagnosis (in 55 cases autopsy was declined and 43 cases were lost to follow-up) and 68 cases (22%) were excluded because of incomplete antenatal data or measurements. Moreover, three megacystis cases not suspected for LUTO were excluded from further analysis. They all presented polyhydramnios and macrosomia and an overgrowth syndrome was confirmed after birth (Figure 1).
Based on postnatal investigations or postmortem examinations, a final diagnosis was achieved in 143 cases, including 124 (87%) true LUTO cases (74 PUV, 4 urethral atresia, 6 urethral stenosis and 40 non-specified LUTO) and 19 (13%) cases reclassified postnatally as non-obstructive megacystis (12 infants with VUR (vesico-ureteral reflux), 4 cases of primary mega-ureters, one fetus with megacystis-microcolon-intestinal hypoperistalsis syndrome, and 2 cases without any evidence of urological anomaly and normal voiding at birth).
Descriptive statistics, sensitivity, specificity and details on the univariate analysis according to final diagnosis, are presented in Table 1 and 2. Longitudinal bladder diameter (LBD) showed poorer accuracy at the univariate analysis compared to bladder volume, and was therefore excluded from further analysis. A ROC curve of bladder volume was performed to identify the optimal cut-off for prediction of LUTO (AUC = 0.66 (CI 0.6-0.8), p = 0.03, optimal cut off: 35 cm3). In addition,13 cases showed urinary ascites at referral with a collapsed urinary bladder, suggesting that the a severely enlarged bladder had ruptured and thus making bladder volume measurement no longer reliable. Therefore, severe megacystis was defined by a bladder volume > 35 cm3 or ascites at referral.

92
Chapter 6
Multivariate logistic analysis was performed starting with the inclusion of all the following antenatal variables considered as theoretically relevant in the literature for the prospective diagnosis of LUTO: renal cortical appearance (normal or abnormal), amniotic fluid volume (normal or reduced), gestational age at referral (before or after 28 weeks’ gestation), degree of bladder distension (mild or severe), fetal hydronephrosis, fetal sex (female or male), evidence of keyhole sign (yes or no), and ureteral size, as continuous variable. The stepwise backward method resulted in the progressive collapse of the variables with poorer performance. These were: fetal hydronephrosis, renal cortical appearance and keyhole sign.
table 1. Antenatal ultrasound characteristics according to the final diagnosis.
Non-obstructive megacystis
n = 19
LUTO
n = 124
p value
Sex (male) 14 (74%) 115 (93%) 0.01
Keyhole sign 5 (26%) 59 (47%) 0.08
Echogenic kidneys 4 (21%) 67 (54%) < 0.01
Oligo- or anhydramnios 2 (11%) 55 (44%) < 0.01
Hydronephrosis 15 (79%) 108 (88%) 0.29
Referral before the 28th weeks(median and range, weeks)
8 (42%)25 (19 – 36)
82 (66%) 23 (18 – 36)
0.04
Bladder volume (cm3) 18 (0.7 – 58) 31 (0.3 – 390)
Bladder longitudinal diameter (mm)(median and range)
36 (13) 45 (18) 0.03
Ureteral size (mm)(sum of right and left ureteral diameters)
1.8 (3.5) 5.3 (7.2) < 0.01
*Data are given as n (%), median (range) or media (SD)
Figure 1. Study population
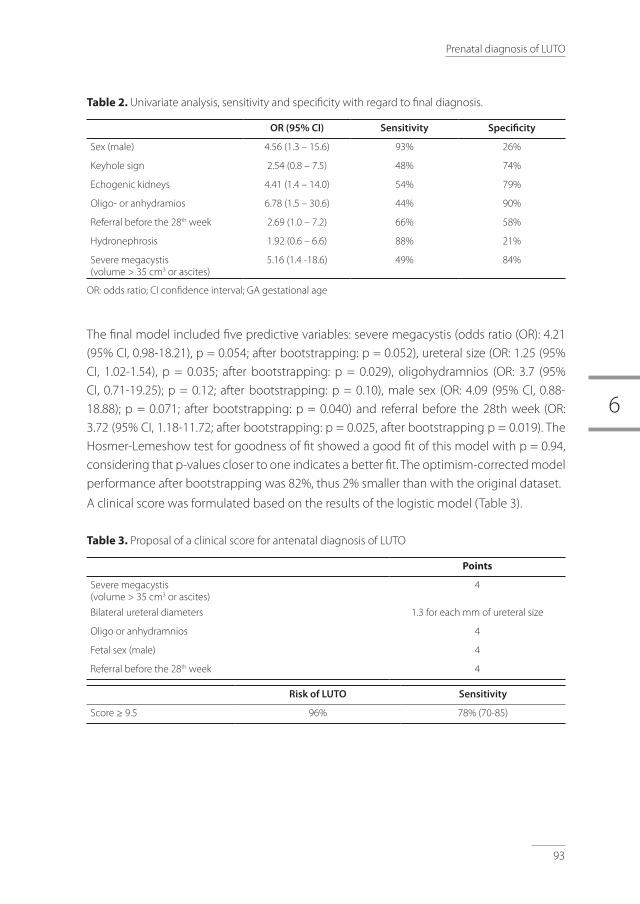
6
93
Prenatal diagnosis of LUTO
table 2. Univariate analysis, sensitivity and specificity with regard to final diagnosis.
OR (95% CI) Sensitivity Specificity
Sex (male) 4.56 (1.3 – 15.6) 93% 26%
Keyhole sign 2.54 (0.8 – 7.5) 48% 74%
Echogenic kidneys 4.41 (1.4 – 14.0) 54% 79%
Oligo- or anhydramios 6.78 (1.5 – 30.6) 44% 90%
Referral before the 28th week 2.69 (1.0 – 7.2) 66% 58%
Hydronephrosis 1.92 (0.6 – 6.6) 88% 21%
Severe megacystis (volume > 35 cm3 or ascites)
5.16 (1.4 -18.6) 49% 84%
OR: odds ratio; CI confidence interval; GA gestational age
The final model included five predictive variables: severe megacystis (odds ratio (OR): 4.21 (95% CI, 0.98-18.21), p = 0.054; after bootstrapping: p = 0.052), ureteral size (OR: 1.25 (95% CI, 1.02-1.54), p = 0.035; after bootstrapping: p = 0.029), oligohydramnios (OR: 3.7 (95% CI, 0.71-19.25); p = 0.12; after bootstrapping: p = 0.10), male sex (OR: 4.09 (95% CI, 0.88-18.88); p = 0.071; after bootstrapping: p = 0.040) and referral before the 28th week (OR: 3.72 (95% CI, 1.18-11.72; after bootstrapping: p = 0.025, after bootstrapping p = 0.019). The Hosmer-Lemeshow test for goodness of fit showed a good fit of this model with p = 0.94, considering that p-values closer to one indicates a better fit. The optimism-corrected model performance after bootstrapping was 82%, thus 2% smaller than with the original dataset.
A clinical score was formulated based on the results of the logistic model (Table 3).
table 3. Proposal of a clinical score for antenatal diagnosis of LUTO
Points
Severe megacystis (volume > 35 cm3 or ascites)
4
Bilateral ureteral diameters 1.3 for each mm of ureteral size
Oligo or anhydramnios 4
Fetal sex (male) 4
Referral before the 28th week 4
Risk of LUTO Sensitivity
Score ≥ 9.5 96% 78% (70-85)

94
Chapter 6
Figure 2 shows the accuracy in discriminating LUTO from non-obstructive megacystis of this proposed clinical score compared to a theoretical model only based on the commonly used LUTO triad (Area Under Curve: 0.84 (95% CI, 0.75-0.93), p < 0.001) vs 0.63 (95% CI, 0.49-0.77), p = 0.07). A ROC curve analysis identified at 9.5 the optimal cut-off point for the clinical LUTO score in predicting the risk of LUTO (Table 3; sensitivity 78%, specificity 79%).
AUC CI (95%) p value
Classic LUTO triad 0.63 0.49 - 0.77 0.07
LUTO clinical score 0.84 0.75 - 0.93 < 0.001
Figure 2 - table 4. Receiver-operating characteristics curves for antenatal prediction of LUTO based on LUTO clinical score (—), or based on the classic LUTO triad (---).
Discussion
In this study, we propose a clinical score for calculating the risk of congenital LUTO during pregnancy, based on five antenatal variables all evaluated at the detailed US scan at referral: bladder distension (severe or moderate), bilateral ureteral dilatation (as continuous variable), amount of amniotic fluid (normal or oligohydramnios), fetal sex and GA at referral (before or after the 28th week). This score demonstrated good discriminative value in distinguishing real LUTO from non-obstructive megacystis, which would not be amenable for antenatal treatment, and a better performance than the classic antenatal triad. The use of this new combination of US parameters enables an optimal identification of LUTO cases at the time of referral, allowing for appropriate counseling and management options.
The role of fetal therapy for LUTO is still debated in the literature and the opportunity to

6
95
Prenatal diagnosis of LUTO
gain high-quality evidence has been missed with the premature conclusion of the PLUTO trial. A retrospective multicenter study was recently published with the aim to explore the effectiveness of fetal therapy in cases with severe LUTO, defined by megacystis, increased bladder-wall thickness, bilateral severe hydronephrosis and oligohydramnios. Despite the strict criteria, still 23% of treated fetuses were wrongly suspected for LUTO (6). We think that both disease severity and selection of candidates for in-utero treatment are influential determinants for fetal therapy’s effectiveness, and that an improvement in the diagnostic accuracy of antenatal US is thus needed.
In this study, fetal hydronephrosis was observed in 88% of LUTO cases, and in 79% of non-obstructive megacystis cases. A recent review reported hydronephrosis even only in 40-50% of LUTO cases and questioned the strength of this association (11). The keyhole sign demonstrated high specificity (74%),but poor sensitivity for LUTO (48%; Table 2). Other studies (12)(13)(14) have previously reported poor accuracy of this US sign for the prospective diagnosis of LUTO and in particular PUV. It has been hypothesized that a possible explanation for its low reliability is that miscellaneous types of bladder dysfunctions such as detrusor instability and bladder-sphincter dyssynergy can cause a dilatation of the bladder neck. The latter has been in fact diagnosed in 30% of male infants with VUR at voiding cystourethrograms (15). The dilatation of the bladder neck at the prenatal ultrasound scan could mimic a dilated posterior urethra, with an ultrasound appearance similar to a keyhole, without being a true dilatation of the posterior urethra (13)(16). Therefore, although keyhole sign and hydronephrosis have been considered thus far as key findings of LUTO, and PUV in particular, they are poorly predictive of the exact postnatal diagnosis.
The amount of amniotic fluid was included in the final model, although it demonstrated poor sensitivity at the univariate analysis. In our cohort in fact 69/124 (56%) of LUTO cases showed normal amniotic fluid at referral. This is consistent with previous studies that reported a rate of 39% (13), albeit they did not set a specific gestational age for evaluating this parameter. Oligohydramnios is typically considered as a characteristic finding of LUTO, as cases with non-obstructive megacystis are unlikely to develop such anomaly. For this reason, a reduced amount of amniotic fluid is often used as an eligibility criterion for the in-utero treatment. However, some fetal medicine expert argue that oligohydramnios occurs when renal parenchyma has already been severely damaged and for this reason in-utero treatment should rather be offered to candidates with normal or just moderately reduced amniotic fluid volume. Our results confirm that the amount of amniotic fluid, evaluated at the first detailed US scan, can be used in evaluating the risk of LUTO. However, its absence should not rule out the antenatal suspicion of LUTO.
Another interesting finding of this study was that the severity of bladder distension is an independent predictor of LUTO. Our results showed that the likelihood of LUTO was four folds higher (OR 4.21,p = 0.05) in case of severe megacystis, defined by bladder volume
96
Chapter 6
greater than > 35 cm3 or fetal ascites at referral. Megacystis has always been considered a key feature of LUTO with a high predictive value (13). However, an objective threshold to define megacystis during the second and third trimester is still lacking. Previous studies (10)(17) have investigated fetal urine production according to GA in healthy fetuses without reporting fetal bladder dimensions. Miscellaneous criteria have been used in the literature for defining megacystis in the second and third trimester, ranging from a bladder length >99th percentile for gestational age in absence of a normogram (18), to the most commonly used definition of a fetal bladder failing to empty during a period of 45 minutes (19)(20)(21)(22). To sum up, at present there have not yet been published prospective studies that have elucidated the normal bladder dimensions during the second and third trimester of pregnancy and defined a threshold for pathological enlargements. This is therefore urgently needed.
A strength of this study is that, at variance with previous studies, the antenatal variables were combined in a multivariate analysis and were only considered at the moment of referral. In spite of the fact that this approach has reduced our cohort to 143 cases, this is thus far the largest study in the literature.
Some critical remarks need to be made. First, not all the antenatal variables were directly measured bythe sonographer, and in a proportion of cases the first author (FF) measured them retrospectively on stored pictures. This also implied that serial bladder measurements were not available in most of the cases. Second, the retrospective design implied that for the renal parenchymal appearance we had to rely upon the subjective judgment reported on the US reports, rather than on an objective measurement. This limitation may have affected the accuracy of this variable.
Statistical bootstrapping showed that the overfitting of the model was small, suggesting that the model could hold for the overall population suspected for LUTO. However, an external validation is essential before endorsing this statement and supporting its clinical applicability.
To conclude, in order to improve the diagnostic accuracy of LUTO in the second and third trimester, the criteria that need to be evaluated are: fetal bladder enlargement, ureteral dilatation, gestational age at referral, fetal sex and evidence of oligohydramnios. Future studies for validating externally these results are needed in order to refine the antenatal identification of LUTO, prevent unnecessary fetal interventions and optimize the prenatal management.
6
97
Prenatal diagnosis of LUTO
references
1. Lissauer D, Morris RK, Kilby MD. Fetal lower urinary tract obstruction. Semin Fetal Neonatal Med. 2007;12(6):464–70.
2. Anumba DO, Scott JE, Plant ND, Robson SC. Diagnosis and outcome of fetal lower urinary tract obstruction in the northern region of England. Prenat Diagn. 2005;25(1):7–13.
3. Morris RK, Kilby MD. Congenital urinary tract obstruction. Best Pract Res Clin Obstet Gynaecol. 2008;22(1):97–122.
4. Fontanella, F., L. Duin, P. N. Adama van Scheltema, T. E. Cohen - Overbeek, E. Pajkrt, M. Bekker, C. Willekes, C. J. Bax CMB. Fetal Megacystis: prediction of outcome and spontaneous resolution. Ultrasound Obstet Gynecol. 2017;2017 Oct;50(4):458-463.
5. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8(6):387–90.
6. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: A multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015 Apr;45(4):452-8.
7. Morris RK1, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan KS, Deeks J, Kilby MD; Percutaneous vesicoamniotic shunting in Lower Urinary Tract Obstruction (PLUTO) Collaborative Group. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): A randomised trial. Lancet. 2013 Nov 2;382(9903):1496-506.
8. Morris RK, Malin GL, Khan KS, Kilby MD. Systematic review of the effectiveness of antenatal intervention for the treatment of congenital lower urinary tract obstruction. Vol. 117, BJOG: An International Journal of Obstetrics and Gynaecology. 2010. p. 382–90.
9. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: A population-based epidemiological study. BJOG An Int J Obstet Gynaecol. 2012;119(12):1455–64.
10. Campbell S, Wladimiroff JW, Dewhurst CJ. The antenatal measurement of fetal urine production. J Obstet Gynaecol Br Commonw 1973 Aug;80(8):680–6.
11. Haeri S. Fetal Lower Urinary Tract Obstruction (LUTO): a practical review for providers. Matern Heal Neonatol Perinatol 2015;1:26.
12. Chitrit Y, Bourdon M, Korb D, Grapin-Dagorno C, Joinau-Zoulovits F, Vuillard E, Paye-Jaouen A, Peycelon M, Belarbi N, Delezoide AL, Schmitz T, El Ghoneimi A, Sibony O, Oury JF. Posterior urethral valves and vesicoureteral reflux: can prenatal ultrasonography distinguish between these two conditions in male fetuses? Prenat Diagn. 2016;36(9):831–7.
13. Bernardes LS, Aksnes G, Saada J, Masse V, Elie C, Dumez Y, Lortat-Jacob SL, Benachi A. Keyhole sign: How specific is it for the diagnosis of posterior urethral valves? Ultrasound Obstet Gynecol. 2009;34(4):419–23.
14. Cohen HL, Zinn HL, Patel A, Zinn DL, Haller JO. Prenatal sonographic diagnosis of posterior urethral valves: identification of valves and thickening of the posterior urethral wall. J Clin Ultrasound. 1998 Sep;26(7):366–70.
15. Boopathy Vijayaraghavan S. Sonography of fetal micturition. Ultrasound Obstet Gynecol. 2004 Nov;24(6):659–63.
16. Yeung CK, Ley MLG, Dh Illon HK, Ord On IG, Uffy PGD, Ansley PGR. The characteristics of primary vesico-ureteric reflux in male and female infants with pre-natal hydronephrosis. Br J Urol. 1997;80:319–27.
17. Touboul C, Boulvain M, Picone O, Levaillant J-M, Frydman R, Senat M-V. Normal fetal urine production rate estimated with 3-dimensional ultrasonography using the rotational technique (virtual organ computer-aided analysis). Am J Obstet Gynecol. 2008 Jul 1 [cited 2017 Jul 12];199(1):57.e1-57.e5.
18. Muller F, Dreux S, Vaast P, Dumez Y, Nisand I, Ville Y, Boulot P, Guibourdenche J, Althusser M, Blin G, Gautier E, Lespinard C, Perrotin F, Poulain P, Sarramon MF; Study Group of the French Fetal Medicine Society. Prenatal diagnosis of megacystis-microcolon-intestinal hypoperistalsis syndrome: contribution of amniotic fluid digestive enzyme assay and fetal urinalysis. Prenat Diagn. 2005 Mar; 25(3):203–9.
19. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, El-Ghoneimi A, Oury JF, Muller F. Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn. 2013;33(12):1162–6.
98
Chapter 6
20. Montemarano H, Bulas DI, Rushton HG, Selby D. Bladder distention and pyelectasis in the male fetus: causes, comparisons, and contrasts. J Ultrasound Med. 1998;17(12):743–9.
21. Müller Brochut A-C, Thomann D, Kluwe W, Di Naro E, Kuhn A, Raio L. Fetal megacystis: experience of a single tertiary center in Switzerland over 20 years. Fetal Diagn Ther. 2014;36(3):215–22.
22. Robyr R, Benachi A, Daikha-Dahmane F, Martinovich J, Dumez Y, Ville Y. Correlation between ultrasound and anatomical findings in fetuses with lower urinary tract obstruction in the first half of pregnancy. Ultrasound Obstet Gynecol. 2005 May;25(5):478–82.

6
99
Prenatal diagnosis of LUTO


Part 3
Prediction of prognosis
and staging of LUTO

Antenatal Staging of congenital Lower Urinary Tract Obstruction (LUTO)
Fontanella F., Adama van Scheltema PN, Duin L., Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Oepkes D, Bilardo CM.
UltrasoundinobstetricsandGynecol2018,inpress 7

104
Chapter 7
abstract
aim: To propose a staging system for congenital Lower Urinary Tract Obstructions (LUTO) capable of predicting the severity of the condition and its prognosis.
Methods: This was a national retrospective study carried out at the eight Academic Hospitals in the Netherlands. We collected prenatal and postnatal data of fetuses at high-risk of isolated LUTO and managed conservatively. Postnatal renal function was assessed by the estimated glomerular filtration rate (eGFR), calculated with the Schwartz formula, considering the length of the infant and the creatinine nadir in the first year of age. Receiver operating characteristic (ROC) curve, univariate analysis and multivariate logistic regression analysis with stepwise backward elimination were performed in order to identify the best antenatal predictors of perinatal mortality and postnatal renal function.
results: In total 261 fetuses suspected for LUTO and managed conservatively were included in the study. The pregnancy was terminated in 110 cases and perinatal death occurred in 35 cases. GA at the appearance of oligohydramnios showed an excellent accuracy in predicting the risk of perinatal mortality with an area under the curve of 0.95 (p < 0.001) and an optimal cut-off at 26 weeks’ gestation. Fetuses with still normal AF at 26 weeks’ gestation presented with low risk of poor outcome and were therefore defined as cases with mild LUTO. In fetuses referred before the 26th week of gestation, the urinary bladder volume (BV) was the best unique predictor of perinatal mortality. ROC analysis identified a BV of 5.4 cm3 at 20 weeks as the best threshold for predicting an adverse outcome. Therefore, LUTO cases with a BV ≥ 5.4 cm3 or abnormal AF before 20 weeks’ gestation were defined as severe and those with BV < 5.4 cm3 and still normal AF at the 20 weeks’ scan were defined as moderate. Risk of perinatal mortality significantly increased according to the stage of severity from mild to moderate and severe stage, from 8%, to 26% and to 55%, respectively. Similarly, risk of severely impaired renal function increased from 11%, to 31% and to 44%, respectively.
Conclusions: Gestational age at first appearance of oligo- or anhydramnios and bladder volume at diagnosis can accurately predict mortality and morbidity in fetuses with LUTO.
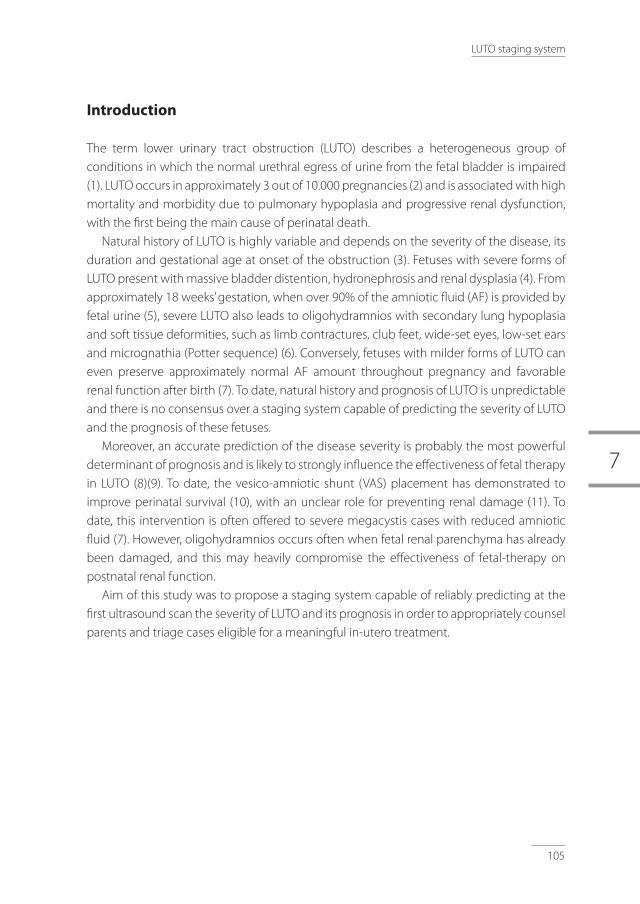
7
105
LUTO staging system
Introduction
The term lower urinary tract obstruction (LUTO) describes a heterogeneous group of conditions in which the normal urethral egress of urine from the fetal bladder is impaired (1). LUTO occurs in approximately 3 out of 10.000 pregnancies (2) and is associated with high mortality and morbidity due to pulmonary hypoplasia and progressive renal dysfunction, with the first being the main cause of perinatal death.
Natural history of LUTO is highly variable and depends on the severity of the disease, its duration and gestational age at onset of the obstruction (3). Fetuses with severe forms of LUTO present with massive bladder distention, hydronephrosis and renal dysplasia (4). From approximately 18 weeks’ gestation, when over 90% of the amniotic fluid (AF) is provided by fetal urine (5), severe LUTO also leads to oligohydramnios with secondary lung hypoplasia and soft tissue deformities, such as limb contractures, club feet, wide-set eyes, low-set ears and micrognathia (Potter sequence) (6). Conversely, fetuses with milder forms of LUTO can even preserve approximately normal AF amount throughout pregnancy and favorable renal function after birth (7). To date, natural history and prognosis of LUTO is unpredictable and there is no consensus over a staging system capable of predicting the severity of LUTO and the prognosis of these fetuses.
Moreover, an accurate prediction of the disease severity is probably the most powerful determinant of prognosis and is likely to strongly influence the effectiveness of fetal therapy in LUTO (8)(9). To date, the vesico-amniotic shunt (VAS) placement has demonstrated to improve perinatal survival (10), with an unclear role for preventing renal damage (11). To date, this intervention is often offered to severe megacystis cases with reduced amniotic fluid (7). However, oligohydramnios occurs often when fetal renal parenchyma has already been damaged, and this may heavily compromise the effectiveness of fetal-therapy on postnatal renal function.
Aim of this study was to propose a staging system capable of reliably predicting at the first ultrasound scan the severity of LUTO and its prognosis in order to appropriately counsel parents and triage cases eligible for a meaningful in-utero treatment.

106
Chapter 7
Methods
This was a national retrospective study carried out at the eight tertiary care hospitals in the Netherlands from 2007 to 2014. Included were fetuses managed conservatively and at high-risk of isolated LUTO according to the criteria proposed in two previous studies from our cohort (12)(unpublisheddata):• Fetuses referred before the 18th week of gestation (Early Megacystis) were included
in case of: longitudinal bladder diameter greater than 12 mm, normal NT or normal karyotype and absence of umbilical cord cysts (unpublisheddata)
• Fetuses referred at or after the 18th week of gestation (Late Megacystis) were included in case of LUTO score greater than 9.5. The score was calculated by considering fetal sex, ureteral size, presence of oligohydramnios, bladder dimension or ascites (12).
Prenatal data were collected on amniotic fluid index (AFI), single deepest pocket (SDP), bladder volume, ureteral size, antero-posterior renal pelvis diameters, renal cortical appearance and gestational age (GA) at referral; lowest AFI throughout the pregnancy, and GA at first occurrence of oligohydramnios and abnormal renal cortical appearance. Oligohydramnios was defined by an amniotic fluid index (AFI) lower than 5 cm or maximum vertical pocket lower than 2 cm (13). The bladder volume was calculated using the formula: longitudinal diameter x transverse diameter x antero-posterior diameter x π/6 (14).
Postnatal data on outcome, GA and weight at birth were collected. All postnatal investigations and postmortem examinations were reviewed. Neonatal death was defined as deaths among live births during the first 28 completed days of life. Postnatal renal function was evaluated based on estimated glomerular filtration rate (eGFR), calculated with the Schwartz formula by considering the length of the infant and the creatinine nadir
in the first year of diagnosis (15). First, we tested by receiver operating characteristic (ROC) curve analysis the accuracy
of GA at first appearance of oligohydramnios in predicting the risk of perinatal mortality. Second, we investigated by univariate analysis and multivariate logistic regression analysis with stepwise backward elimination the prognostic value of different antenatal US parameters at referral. Statistical analyses were carried out using SPSS 22 (IBM Corp., Armonk, NY, USA).

7
107
LUTO staging system
results
In total 261 fetuses managed conservatively and at high-risk of isolated LUTO were included in the study. In 110 cases, owing to the uncertain prognosis, parents elected to terminate the pregnancy (mean GA: 23 weeks). Among the ongoing 151 pregnancies, perinatal mortality occurred in 35 cases (23%), including 23 neonatal deaths and 12 intrauterine fetal demises.
Table 1 summarizes the pre- and postnatal characteristics of the study population. GA at first appearance of oligo- or anhydramnios showed an excellent accuracy in predicting the risk of perinatal mortality with an area under the curve of 0.95 (p < 0.001, 95% CI: 0.92 – 0.98; Figure 1) and with an optimal cut-off at 26 weeks of gestation. Therefore, fetuses with enlarged bladders, but still normal AF at 26 weeks’ gestation were defined as mild LUTO as their risk of perinatal mortality was 8.6% (Table 2 - 3).
table 1. Antenatal and postnatal characteristics of the study population
Antenatal and postnatal characteristics mean (CI 95%) or median (range)
GA at diagnosis (weeks)
Early Megacystis (referred <18th week)
Late Megacystis (referred ≥18th week)
21 weeks (±8 weeks)97/261 (36%)164/261(63%)
Bladder volume (cm3)
Longitudinal bladder diameter (mm)
37 (±93)41 (±22)
Left antero-posterior pelvic diameter (mm)
Right antero-posterior pelvic diameter (mm)
Hydronephrosis
Ureteral size (mm)
9.8 (7-10)9.9 (8-11)
160/205 (78%)5 (±6)
Oligo- or anhydramnios during pregnancy
GA at first oligohydramnios (weeks)
130/261 (50%)29 (±9)
Intrauterine fetal death
Neonatal death
Alive
Birth weight (gr)
12/151 (8%)23/151 (15%)
116/151 (77%)2680 (±1958)
Data are expressed as mean (CI 95%) or median (range); GA, gestational age.
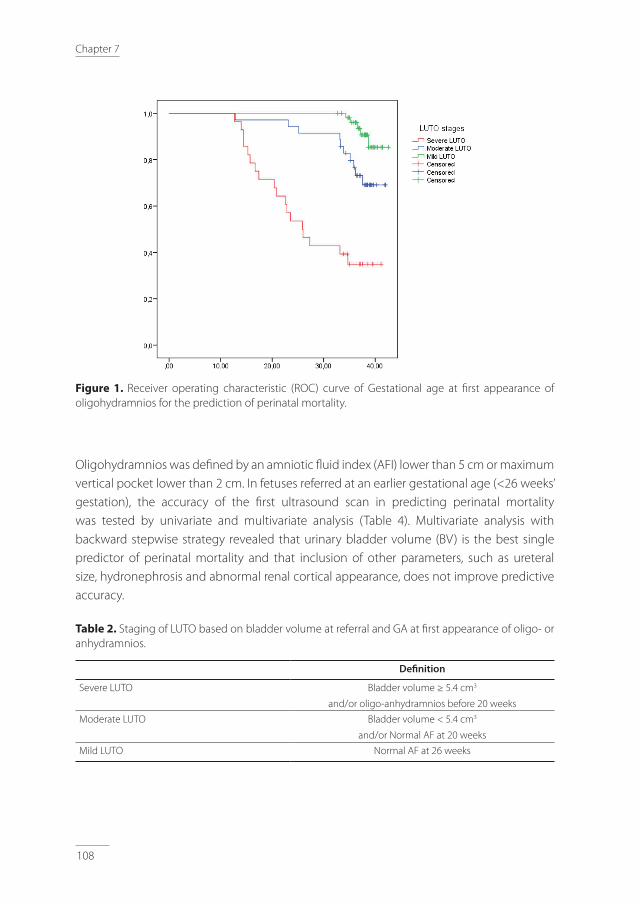
108
Chapter 7
Figure 1. Receiver operating characteristic (ROC) curve of Gestational age at first appearance of oligohydramnios for the prediction of perinatal mortality.
Oligohydramnios was defined by an amniotic fluid index (AFI) lower than 5 cm or maximum vertical pocket lower than 2 cm. In fetuses referred at an earlier gestational age (<26 weeks’ gestation), the accuracy of the first ultrasound scan in predicting perinatal mortality was tested by univariate and multivariate analysis (Table 4). Multivariate analysis with backward stepwise strategy revealed that urinary bladder volume (BV) is the best single predictor of perinatal mortality and that inclusion of other parameters, such as ureteral size, hydronephrosis and abnormal renal cortical appearance, does not improve predictive accuracy.
table 2. Staging of LUTO based on bladder volume at referral and GA at first appearance of oligo- or anhydramnios.
Definition
Severe LUTO Bladder volume ≥ 5.4 cm3
and/or oligo-anhydramnios before 20 weeks
Moderate LUTO Bladder volume < 5.4 cm3
and/or Normal AF at 20 weeks
Mild LUTO Normal AF at 26 weeks

7
109
LUTO staging system
In fetuses referred before the 26th week of gestation, ROC curve analysis indicated as optimal cut-off for the prediction of an adverse outcome a BV of 5.4 cm3 at 20 weeks’ gestation. Therefore, fetuses with a BV ≥ 5.4 cm3 or an abnormal AF before 20 weeks’ gestation were defined as severe LUTO and those with BV< 5.4 cm3 and still normal AF at the 20 weeks’ scan were defined as moderate LUTO (Table 2). Perinatal mortality in fetuses with severe and moderate LUTO was 55% (18/33) and 26% (10/38), respectively (Table 3).
table 3. Survival rate, mean GA at oligo- or anhydramnios and abnormal renal cortical appearance by LUTO stage.
Perinatal mortality
GA at 1stevidence oligohydramnios
(mean ±SD)
ARCA Mean eGFR
ml/min/1.73 m2
eGFR < 30
ml/min/1.73 m2
Severe LUTO 54.5% (18/33) 21 ±8 weeks 79% 65 ±47 44% (4/9)
Moderate LUTO 26.3% (10/38) 29 ±8 weeks 68% 57 ±44 31% (5/16)
Mild LUTO 8.6% (6/70) 35 ±4 weeks 34% 87 ±43 11% (4/36)
ARCA, abnormal renal cortical appearance; eGFR, estimated glomerular filtration rate.
table 4. Univariate analysis for the prediction of perinatal mortality in fetuses referred before the 26th week of gestation.
OR (CI 5-95%) p value
Hydronephrosis 0.9 (0.83-1.52) 1.4
Ureteral size 1.1 (0.98-1.43) 1.3
Bladder volume 0.98 (0.97-0.99) 0.04
Abnormal renal cortical appearance 0.1 (0.04-0.42) 0.01
Based on these results, a staging system capable of stratifying LUTO cases according to their risk of perinatal mortality and postnatal renal function was developed (Figure 2). The prognosis worsens progressively, in terms of perinatal mortality and risk of severely impaired postnatal renal function (eGFR < 30 ml/min/1.73 m2), according to the BV at diagnosis and the GA at first appearance of oligohydramnios, from mild to moderate and to severe LUTO stage (Table 3 - Figure 2). An additional category of cases with ineluctable perinatal mortality was identified: all fetuses with BV > 200 cm3 and oligohydramnios before 18weeks had an adverse prognosis.
110
Chapter 7
Figure 2. Kaplan-Meier curve for the overall survival according to the LUTO stage: cumulative survival on the y axis and gestational age on the x axis.
Discussion
This study shows that in fetuses with LUTO, a staging system taking into account the GA at first evidence of oligo- or anhydramnios and bladder volume can reliably predict survival and postnatal renal function. Fetuses classified as having a mild form of LUTO had approximately a 90% chance of survival with a good renal function in the majority of cases, whereas in moderate and severe LUTO stages, perinatal survival was reduced to 75% and 45%, respectively. In the survivors, severe renal dysfunction (eGFR < 30 ml/min/1.73 m2) requiring renal transplant or dialysis in the first year of life was observed in 31% and 44% of cases, respectively.
The natural history of LUTO is highly variable, and reliable criteria to predict whether renal function and AF volume will be preserved throughout pregnancy or not are still missing (16). This study shows that the GA at the first evidence of oligohydramnios can accurately predict the risk of perinatal mortality and, as expected, the earlier oligohydramnios occurs, the poorer the outcome (17). The optimal threshold for predicting adverse outcome is 26 weeks of gestation at first evidence of oligo- or anhydramnios. This GA corresponds to the end of the canalicular phase (18)(17), a crucial period for the development of the anatomical structures needed for an intact gas-exchange function of the fetal lungs (19)(17). Previous studies have reported similar results showing that the risk of perinatal death is more than 80% in second-trimester oligohydramnios with onset before 25 weeks’ gestation
7
111
LUTO staging system
and persisting for more than 14 days (20)(21)(22)(23). Conversely, if AF is still within normal ranges at 26 weeks, there is a 90% chance of survival with an acceptable postnatal renal function in more than 90% of cases (mean eGFR: 87 ml/min/1.73 m2). These results confirm the findings reported by the North American Fetal Therapy Network (7).
The best single predictor of adverse outcome in LUTO referred before the 26th week of gestation was the bladder size at diagnosis. In fact, we can assume that the larger the bladder, the more severe the obstruction and therefore the higher the chance of developing oligo- or anhydramnios earlier during pregnancy. This finding is in agreement with a few other studies, stressing the importance of bladder measurement for fine-tuning the prenatal diagnosis and the prediction of prognosis in LUTO (24)(25). Unfortunately, the lack of accurate normal ranges for fetal bladder size and urine production in the second and third trimester of pregnancy still lead to inaccuracies with both over- as well as under-diagnoses of enlarged bladders, especially in fetuses with borderline enlargements. However, as suggested by Lee et al., in the future fetal urine production assessment may provide a superior alternative for diagnosing oligohydramnios (26), as the AFI and the SDP measurement are often poor predictors of the actual AF volume (27).
The vesico-amniotic shunt (VAS) placement has demonstrated to improve perinatal survival (10), with an unclear role for preventing renal damage (11), and is therefore typically proposed in fetuses with high risk of perinatal mortality. However, Morris et al showed that in this population the chance of surviving with normal renal function is very low irrespective of whether or not the VAS is placed (10). We believe that the lack of a robust staging system and consistent eligibility criteria has represented major limitations for evaluating the real effectiveness of VAS, that is likely to change according to the LUTO severity (28). This study suggests that offering VAS to cases with early oligohydramnios is at least questionable, as these fetuses have already a high chance of mortality and compromised renal function (10)(29). Future studies are needed to clarify the role of fetal intervention in terms of perinatal survival and postnatal renal function according to each LUTO stage.
Recently, Ruano et al. proposed a management protocol with a classification of LUTO severity based on AF amount and fetal renal function, that was purely inferred from antenatal parameters such as absence of bilateral renal dysplasia, renal cysts and urinary biochemistry, without analyzing postnatal renal function and urological sequelae. Their retrospective study included 25 fetuses with LUTO, 14 of which treated with VAS. In light of the small sample size, the antenatal predictors of survival were analyzed by using a Bayesian methodology.
Similarly, we aimed at stratifying the risk of perinatal mortality by including a much larger population and only managed conservatively during pregnancy. Another strength of our study is that LUTO was defined by a set of antenatal criteria, that we already elaborated in previous studies, rather than on less predictive and non-objective criteria, prone to produce

112
Chapter 7
high rate of false-positive cases (2)(12). This approach is also more suitable than relying upon the evidence of LUTO at pathological examination on terminated or demised fetuses or on the postnatal assessment on surviving infants.
A potential limitation of our study is that we excluded the cases with terminations of pregnancy as no renal function parameters were available. In order to obviate this, we have evaluated retrospectively the severity of LUTO in each single TOP and found that 77% would have been classified as severe or moderate, whereas the remaining 23% would have been milder LUTO cases, where parents opted for termination of pregnancy in view of the uncertain prognosis. This distribution is similar to that of the included cases of this study.
To conclude, this study proposes a staging system based on urinary bladder volume and GA at first evidence of oligohydramnios to reliably triage fetuses with LUTO and predict the risk of perinatal mortality and adverse postnatal outcome. We believe that this classification could help in counseling parents on the prognosis and identifying the few cases eligible for a meaningful antenatal management.
7
113
LUTO staging system
references
1. Farrugia MK. Fetal bladder outlet obstruction: Embryopathology, in utero intervention and outcome. J Pediatr Urol. 2016;12(5):296–303.
2. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: A population-based epidemiological study. BJOG An Int J Obstet Gynaecol. 2012;119(12):1455–64.
3. Khalek N JM. Fetal urinary tract obstruction: prenatal assessment and prognosis. In Fetal Therapy: Scientific Basis and Critical Appraisal of Clinical Benefits. Kilby M, D. Oepkes, A. Johnson. Cambridge CU press.
4. Wu S, Johnson MP. Fetal Lower Urinary Tract Obstruction. Clin Perinatol. 2009;36(2):377–90.
5. Haeri S. Fetal Lower Urinary Tract Obstruction (LUTO): a practical review for providers. Matern Heal Neonatol Perinatol. Maternal Health, Neonatology and Perinatology; 2015;1:26.
6. Christianson C, Huff D, McPherson E. Limb deformations in oligohydramnios sequence: Effects of gestational age and duration of oligohydramnios. Am J Med Genet. 1999;86(5):430–3.
7. Johnson MP, Danzer E, Koh J, Polzin W, Harman C, O’Shaughnessy R, Brown R, Zaretsky MV; North American Fetal Therapy Network (NAFTNet). Natural History of Fetal Lower Urinary Tract Obstruction with Normal Amniotic Fluid Volume at Initial Diagnosis. Fetal Diagn Ther. 2017. DOI: 10.1159/000478011.
8. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: a multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015 Apr;45(4):452–8.
9. Ruano R, Sananes N, Wilson C, Au J, Koh CJ, Gargollo P, Shamshirsaz AA, Espinoza J, Safdar A, Moaddab A, Meyer N, Cass DL, Olutoye OO, Olutoye OA, Welty S, Roth DR, Braun MC, Belfort MA. Fetal lower urinary tract obstruction: proposal for standardized multidisciplinary prenatal management based on disease severity. Ultrasound Obstet Gynecol. 2016;48(4):476–82.
10. Morris RK, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan KS, Deeks J, Kilby MD. Percutaneous vesicoamniotic shunting in Lower Urinary Tract Obstruction (PLUTO) Collaborative Group. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): a randomised trial. Lancet 2013 Nov;382(9903):1496–506.
11. Morris RK, Ruano R, Kilby MD. Effectiveness of fetal cystoscopy as a diagnostic and therapeutic intervention for lower urinary tract obstruction: a systematic review. Ultrasound Obs Gynecol. 2011;37:629–37.
12. Fontanella F, Duin LK, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Gracchi V, Oepkes D, Bilardo CM. Prenatal diagnosis of LUTO: how to improve diagnostic accuracy. Ultrasound Obstet Gynecol. 2017 Dec 20. [Epub ahead of print]
13. Moise KJ. Toward consistent terminology: Assessment and reporting of amniotic fluid volume. Semin Perinatol. 2013 Oct;37(5):370-4.
14. Campbell S, Wladimiroff JW, Dewhurst CJ. The antenatal measurement of fetal urine production. J Obstet Gynaecol Br Commonw. 1973 Aug;80(8):680–6.
15. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA FS. New Equations to Estimate GFR in Children with CKD. J Am Soc Nephrol. 2009;20:629–37.
16. Chitrit Y, Bourdon M, Korb D, Grapin-Dagorno C, Joinau-Zoulovits F, Vuillard E, Paye- Jaouen A, Peycelon M, Belarbi N, Delezoide AL, Schmitz T, El Ghoneimi A, Sibony O, Oury JF. Posterior urethral valves and vesicoureteral reflux: can prenatal ultrasonography distinguish between these two conditions in male fetuses? Prenat Diagn. 2016;36(9):831–7.
17. Laudy JAM, Wladimiroff JW. The fetal lung 2: Pulmonary hypoplasia. Ultrasound Obstet Gynecol. 2000;16(5):482–94.
18. Laudy JAM, Wladimiroff JW. The fetal lung 1: Developmental aspects. Ultrasound Obstet Gynecol. 2000;16(3):284–90.
19. Laudy JAM, Wladimiroff JW. The fetal lung 2: Pulmonary hypoplasia. Ultrasound Obstet Gynecol. 2000;16(5):482–94.
20. Kilbride, Yeast, Thibeault. Defining limits of survival: Lethal pulmonary hypoplasia after midtrimester premature rupture of membranes. Am J Obstet Gynecol. Mosby; 1996 Sep 1;175(3):675–81.

114
Chapter 7
21. Reuss A, Stewart P, Wladimiroff J, Scholtmeijer R. Non-Invasive management of fetal obstructive uropathy. Lancet. 1988;332(8617):949–51.
22. Harrison MR, Golbus MS, Filly RA, Nakayama DK, Callen PW, Lorimier AA, Hricak H. Management of the fetus with congenital hydronephrosis. J Pediatr Surg. 1982;17(6):728–42.
23. Rotschild A, Ling EW, Puterman ML, Farquharson D. Neonatal outcome after prolonged preterm rupture of the membranes. Am J Obstet Gynecol. 1990;162(1):46– 52.
24. Fontanella F, Duin L, Adama van Scheltema PN, Cohen - Overbeek TE, Pajkrt E, Bekker E, Willekes C, Bax CJ, Bilardo CM. Fetal Megacystis: prediction of outcome and spontaneous resolution. Ultrasound Obstet Gynecol. 2017 Oct;50(4):458-463.
25. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: Chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol. 2003;21(4):338–41.
26. Lee SM, Park SK, Shim SS, Jun JK, Park JS, Syn HC. Measurement of fetal urine production by three-dimensional ultrasonography in normal pregnancy. Ultrasound Obstet Gynecol. 2007 Sep 1;30(3):281–6.
27. Magann EF, Chauhan SP, Barrilleaux PS, Whitworth NS, Martin JN. Amniotic fluid index and single deepest pocket: weak indicators of abnormal amniotic volumes. Obstet Gynecol. 2000 Nov;96(5 Pt 1):737-40.
28. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: A multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015 Apr;45(4):452-8.
29. Nassr AA, Shazly SAM, Abdelmagied AM, Araujo Júnior E, Tonni G, Kilby MD, Ruano R. Effectiveness of vesicoamniotic shunt in fetuses with congenital lower urinary tract obstruction: An updated systematic review and meta analysis. Ultrasound Obstet Gynecol. 2017 Jun;49(6):696-703.

7
115
LUTO staging system

Prediction model of postnatal renal function in fetuses with LUTO – development and internal validation
Duin L, Fontanella F., Groen H, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Gracchi V, Oepkes D, Bilardo CM.
Submitted 8

118
Chapter 8
abstract
Objective To develop a prediction model of postnatal renal function in fetuses with lower urinary tract obstruction (LUTO) based on fetal ultrasound parameters and amniotic fluid volume.
Methods Retrospective nationwide cohort study of fetuses with postnatally confirmed LUTO and known estimated glomerular filtration rate (eGFR). Fetuses treated with fetal interventions such as vesico-amniotic shunting or cystoscopy were excluded. Logistic regression analysis was used to identify prognostic ultrasound variables with respect to renal outcome following multiple imputation of missing data. Based on these fetal renal parameters and amniotic fluid volume a model was developed to predict postnatal renal function in fetuses with LUTO. The main study outcome was an eGFR <60 ml/min*1.73 m2 based on the creatinine nadirduring the first year after diagnosis. Model performance was evaluated by receiver operator characteristic (ROC) curve analysis, calibration plots and bootstrapping.
results Ninety-five fetuses with a confirmed diagnosis of LUTO were included, eGFR < 60 was observed in 34 (35.7 %) of them. Variables predicting an eGFR <60 ml/min*1.73m2 included the following sonographic parameters: hyperechogenicity of the renal cortex, keyhole sign visible in the distended fetal bladder and abnormal amniotic fluid volume. The model showed fair discrimination, with an area under the ROC curve of 0.75 (95% confidence interval: 0.65-0.85, 0.69 after bootstrapping) and was well-calibrated.
Conclusion This study shows that a prediction model incorporating ultrasound parameters such as cortical appearance, keyhole sign of the bladder and abnormal amniotic fluid volume, can fairly predict an eGFR below 60 ml/min*1.73m2. This clinical information can be used in to identify fetuses eligible for prenatal interventions and to improve counseling of parents.

8
119
Prediction of postnatal renal function
Introduction
Congenital anomalies of the kidney and urinary tract (CAKUT) refer to a broad spectrum of renal malformations which originate in defects in embryonic kidney development. In the spectrum of major birth defects congenital anomalies of the kidneys and urinary tract account for 20-30% of all congenital malformations with a prevalence of 3-6 per 1000 births. The most common abnormality is ureteropelvic junction obstruction (UPJ), accounting for 20-30 % of the CAKUT spectrum.1,2 But the spectrum ranges from transient hydronephrosis to bilateral renal agenesis and is the leading cause of end stage kidney disease (ESKD), accounting for 41% of children receiving a renal transplant.3,4 In this spectrum lower urinary tract obstruction (LUTO) is a rare condition with an incidence of 2.2 / 10.000 live births, with posterior urethral valves (PUV) as the predominant etiology.5,6 Other underlying pathologies include urethral atresia, urethral stenosis and prune belly syndrome. Although the combination of prenatal signs as oligohydramnios, a distended thick-walled bladder, a keyhole sign, parenchymal abnormalities and hydronephrosis can predict LUTO in 87% of cases, other conditions such as vesicoureteral reflux (VUR) (24.5%), cloacal dystrophy (18.9%), hydronephrosis (11.3%) or no bladder abnormality after birth (18.9%) can erroneously be classified as LUTO and give rise to false positive prenatal diagnosis.6 LUTO itself is a complex condition associated with a high perinatal mortality rate due to the ensuing lung hypoplasia and end stage renal failure. In the setting of LUTO, it is extremely challenging to predict prenatally the exact postnatal renal and pulmonary function, the degree of persistent bladder dysfunction and of hypertensive disease, before undertaking an attempt to alleviate the primary cause of the urethral obstruction. The severity of LUTO, in terms of perinatal mortality and postnatal outcome, is usually estimated on the base of amniotic fluid volume, renal cortical appearance, degree of hydronephrosis, and eventually on the biochemical analysis of fetal serum or fetal urine.7,8 Although the majority of these parameter have demonstrated good accuracy in predicting the outcome of LUTO, they have never been combined in a multivariate analysis to calculate the individual risk of postnatal compromised renal function.
The aim of this study was to develop a model based on fetal renal ultrasound parameters and amniotic fluid volume able to predict postnatal renal function in fetus with LUTO.
Methods
This study is part of a multicenter study performed in the eight University Medical Centers in the Netherlands. We present data from the Erasmus Medical Center, Academic Medical Center (AMC) and the University Medical Center of Maastricht (MUMC+) for cases of LUTO

120
Chapter 8
from a cohort of births between 2000 and 2015. From the University Medical Center Groningen (UMCG) and Radboud University Medical Center (RadboudUMC) between 2004 to 2015 and from 2007 till 2014 in the remaining centers (VU University Medical Center, Amsterdam (VUmc), Leiden University Medical Center (LUMC), University Medical Center Utrecht (UMCU)).
After referral to one of the University Fetal Medicine Units in The Netherlands, all fetus with a prenatally suspected LUTO, and with a postnatally confirmed diagnosis of LUTO and a known eGFR were included in the final cohort. Cases with a false positive diagnosis of LUTO (i.e. vesico-ureteric reflux, neurogenic bladder ) and LUTO cases treated with fetal interventions as vesico-amniotic shunts (VAS) or fetal cystoscopy were excluded. The collected data were used to develop a model to predict the estimated glomerular filtration rate (eGFR) postnatally, after confirmation of the diagnosis of LUTO . The eGFR was calculated using the Schwartz formula, considering the length of the infant and the creatinine nadir in the first year of diagnosis.9
This study was approved by the Medical Ethics committee of the University Medical Center Groningen (METc 2015/445)
Building the prediction modelAccording to the 2012 Chronic Kidney Disease (CKD) guideline “Improving Global Outcomes (KDIGO)” cases with eGFR below <60 ml/min*1.73 m2 were defined as having a compromised renal function and used as the primary end-point of this study. The guideline classifies CKD into category 3a mildly to moderate decreased kidney function (eGFR 59-45 ml/min*1.73 m2), category 3b moderately to severely decreased kidney function (eGFR 44-30 ml/min*1.73 m2), category 4 severely decreased kidney function (eGFR 29-15 ml/min*1.73 m2) and category 5 kidney failure (eGFR <15 ml/min*1.73 m2 and dialysis).10 Based on current literature and ultrasound parameters derived from the database, we identified a number of predictive variables. The candidate parameters were as follows:• Gestational age at diagnosis (weeks) • Bladder longitudinal diameter (mm) • Renal cortical appearance (echogenicity, cystic cortex) • Renal anteroposterior diameter (mm) • Renal pelvis anteroposterior diameter (mm) • Amniotic fluid volume (single deepest pocket (SDP)) • Presence of a keyhole sign • Bladder wall thickness (mm) • Presence of a thickened bladder wall

8
121
Prediction of postnatal renal function
There were no missing data for the end-point of the study, the eGFR. Ideally, all other candidate parameters should be known in order to be able to build the model. Overall, more than 75 percent of values were available across all variables, which is a well accepted percentage for imputation. On this basis, we performed multiple imputation according to current practice for prediction models.12,13,14 Imputation was performed using SPSS statistics 23 (SPSS Inc. Chicago, IL,USA). Predictive mean matching was applied and twenty imputed datasets were generated.
Statistical analysis
Using the imputed multiple dataset, logistic regression was performed to predict occurrence of the primary end-point. For both dichotomous and continuous variables, univariable pooled odds ratios and 95% confidence intervals (CI) , as well as P-values, were calculated. All predictive variables that had P < .157 in the univariable analysis were considered as potential candidates for inclusion in the multivariable prediction model.14 Multivariable logistic regression with manual backward stepwise selection was used to create the final model using the same cut-off P-value.
To evaluate the discriminative performance of the model, the receiver operator characteristic (ROC) curve was plotted and the area under the curve (AUC or c-statistic) was calculated. This statistic ranges from 0.5 (no discrimination) to 1 (perfect discrimination).
For the calibration of the model, correspondence between the predicted probabilities and the observed proportions was plotted in a calibration plot. Due to the low number of cases, 5 subgroups were created based on the quintiles of the predicted probabilities instead of the recommended 10 subgroups based on deciles of predicted probability. The fit of the logistic regression model was also assessed based on the Hosmer-Lemeshow goodness of fit test. This test is performed on a crosstable of two columns (the observed dichotomous outcome) by ten rows (deciles of the predicted probability). A high P-value is favorable since it indicates that the identification of cases depends on the predicted probability. Internal validation was performed by bootstrap replication for each of the imputed datasets to assess the extent of overfitting of the model.
Using the final prediction model equation, predicted probabilities of renal compromise were calculated for four hypothetical cases with varying chracteristics.
All analyses were performed using IBM SPSS Statistics version 23 (Chicago, IL, USA).

122
Chapter 8
results
During the study period, LUTO was antenatally suspected and confirmed at postmortem or postnatal examination in 222 cases.
In total, 95 fetus with confirmed diagnoses of LUTO and known postnatal eGFR met our criteria for analysis. The description of the total population of fetuses with prenatally diagnosed megacystis, retrieved from the eight University Medical Centers was described previously by Fontanella etal.15
table 1. Descriptive characteristics of the study population
Variable n = 95(%) Mean Min-Max
Gestational age at diagnosis (weeks) - 25 12-42
Gestational age at birth (weeks) - 37 32-42
Birthweight (g) - 3243 1490-4925
Male gender 93 (97.8)
eGFR (ml/min*1.73 m2) 78.1 2.74-162
> 90 44 (46.3)
90-60 17 (17.9)
60-30 18 (18.9)
30-15 8 (8.4)
<15 8 (8.4)
Creatinine 68.13 13-785
Transplantation:
No 84 (88.4)
Yes 6 (6.3)
In preparation 2 (2.1)
Dialysis 3 (3.2)
Descriptive characteristics of the patients used in our model are presented in Table 1. There were 61 (64 %) cases with normal renal function, 9 (9.4 %) with mild to moderately decreased renal function, 9 (9.4 %) cases with moderately to severely impaired renal function, 8 (8.4 %) with severely decreased renal function and 8 (8.4 %)cases with renal failure according to the KDIGO 2012 CKD guideline.10
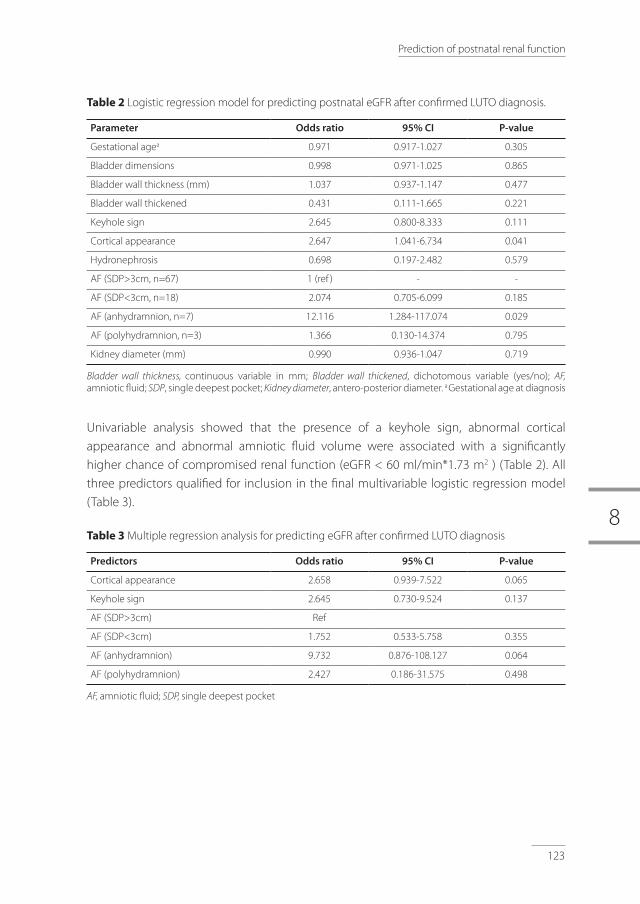
8
123
Prediction of postnatal renal function
table 2 Logistic regression model for predicting postnatal eGFR after confirmed LUTO diagnosis.
Parameter Odds ratio 95% CI P-value
Gestational agea 0.971 0.917-1.027 0.305
Bladder dimensions 0.998 0.971-1.025 0.865
Bladder wall thickness (mm) 1.037 0.937-1.147 0.477
Bladder wall thickened 0.431 0.111-1.665 0.221
Keyhole sign 2.645 0.800-8.333 0.111
Cortical appearance 2.647 1.041-6.734 0.041
Hydronephrosis 0.698 0.197-2.482 0.579
AF (SDP>3cm, n=67) 1 (ref ) - -
AF (SDP<3cm, n=18) 2.074 0.705-6.099 0.185
AF (anhydramnion, n=7) 12.116 1.284-117.074 0.029
AF (polyhydramnion, n=3) 1.366 0.130-14.374 0.795
Kidney diameter (mm) 0.990 0.936-1.047 0.719
Bladder wall thickness, continuous variable in mm; Bladder wall thickened, dichotomous variable (yes/no); AF,amniotic fluid; SDP, single deepest pocket; Kidneydiameter, antero-posterior diameter. a Gestational age at diagnosis
Univariable analysis showed that the presence of a keyhole sign, abnormal cortical appearance and abnormal amniotic fluid volume were associated with a significantly higher chance of compromised renal function (eGFR < 60 ml/min*1.73 m2 ) (Table 2). All three predictors qualified for inclusion in the final multivariable logistic regression model (Table 3).
table 3 Multiple regression analysis for predicting eGFR after confirmed LUTO diagnosis
Predictors Odds ratio 95% CI P-value
Cortical appearance 2.658 0.939-7.522 0.065
Keyhole sign 2.645 0.730-9.524 0.137
AF (SDP>3cm) Ref
AF (SDP<3cm) 1.752 0.533-5.758 0.355
AF (anhydramnion) 9.732 0.876-108.127 0.064
AF (polyhydramnion) 2.427 0.186-31.575 0.498
AF, amniotic fluid; SDP,single deepest pocket

124
Chapter 8
Figure 1 Receiver-operating characteristic curve (ROC) of the multivariable logistic regression model for predicting eGFR in LUTO based on mean predicted probabilities from all imputations. The area under the curve was 0.751 (95% CI 0.651-0.851).
Figure 2 Calibration plot with calculated probability of eGFR on the X-axis and observed proportion of the eGFR on the Y-axis. Error bars indicate standard errors
The developed model had a fair discriminative capacity with a c-statistic of 0.751 (95% CI 0.651-0.851). After bootstrap replication, the mean c-statistic was 0.69 (AUC varied from 0.61-0.73) (Figure 1). The estimated overfitting was calculated to be 8.22 % ((0.73-0.69)/0.73). The model was well-calibrated, as indicated by the Hosmer-Lemeshow goodness-of-fit test (average p-value 0.74) and by the calibration plot (Figure 2). The observed proportion in
Renal compromise quintiles
Predicted probability
Ob
serv
ed p
rob
abili
ty
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.80.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
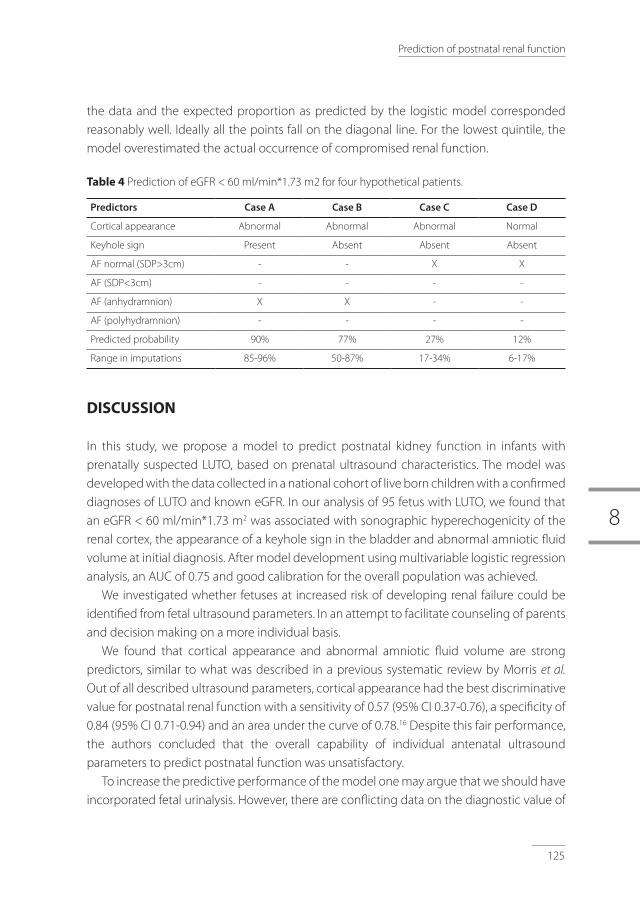
8
125
Prediction of postnatal renal function
the data and the expected proportion as predicted by the logistic model corresponded reasonably well. Ideally all the points fall on the diagonal line. For the lowest quintile, the model overestimated the actual occurrence of compromised renal function.
table 4 Prediction of eGFR < 60 ml/min*1.73 m2 for four hypothetical patients.
Predictors Case A Case B Case C Case D
Cortical appearance Abnormal Abnormal Abnormal Normal
Keyhole sign Present Absent Absent Absent
AF normal (SDP>3cm) - - X X
AF (SDP<3cm) - - - -
AF (anhydramnion) X X - -
AF (polyhydramnion) - - - -
Predicted probability 90% 77% 27% 12%
Range in imputations 85-96% 50-87% 17-34% 6-17%
DISCUSSION
In this study, we propose a model to predict postnatal kidney function in infants with prenatally suspected LUTO, based on prenatal ultrasound characteristics. The model was developed with the data collected in a national cohort of live born children with a confirmed diagnoses of LUTO and known eGFR. In our analysis of 95 fetus with LUTO, we found that an eGFR < 60 ml/min*1.73 m2 was associated with sonographic hyperechogenicity of the renal cortex, the appearance of a keyhole sign in the bladder and abnormal amniotic fluid volume at initial diagnosis. After model development using multivariable logistic regression analysis, an AUC of 0.75 and good calibration for the overall population was achieved.
We investigated whether fetuses at increased risk of developing renal failure could be identified from fetal ultrasound parameters. In an attempt to facilitate counseling of parents and decision making on a more individual basis.
We found that cortical appearance and abnormal amniotic fluid volume are strong predictors, similar to what was described in a previous systematic review by Morris etal.
Out of all described ultrasound parameters, cortical appearance had the best discriminative value for postnatal renal function with a sensitivity of 0.57 (95% CI 0.37-0.76), a specificity of 0.84 (95% CI 0.71-0.94) and an area under the curve of 0.78.16 Despite this fair performance, the authors concluded that the overall capability of individual antenatal ultrasound parameters to predict postnatal function was unsatisfactory.
To increase the predictive performance of the model one may argue that we should have incorporated fetal urinalysis. However, there are conflicting data on the diagnostic value of

126
Chapter 8
biochemical analysis of the fetal urine in predicting fetal renal outcome.17,18 Furthermore, ultrasound parameters of the fetal kidney and urinary biochemistry are not correlated and should be taken separately into account when making a risk assessment for fetuses with LUTO.19
Incorporation of urinalysis in the model might have contributed to a better risk stratification of fetuses candidate for fetal interventions, unfortunately due to the retrospective nature of this cohort, these result were only available in a minority of cases. Another limitation of our study is the lack of external validation20. External validation is a crucial aspect in estimating the applicability of a prognostic model in a population outside the scope where the data were derived from. One could apply the prognostic model on an external population, or split the initial data set in a training and validation sample or retrieve data from a different time frame. However, owing to the low incidence of LUTO, the retrospective design of the nationwide study with inevitable missing data and the need for imputation, external validation was not yet possible. It will be of paramount importance to test this prognostic model in another population in the future, especially to assess if it is capable of identifying cases with a good eGFR. This is in fact where the predicted probability may overestimate the observed probability of renal impairment. This is also the subgroup of fetuses amenable to prenatal intervention.
A recently published classification system with selection criteria for eligibility for fetal intervention by Ruano et al, approaches the fetus on an individual basis to provide the current best management. This classification system uses fetal renal ultrasound parameters, amniotic fluid volume and fetal urinalysis separately.21,22,23 However an individualized estimate of the postnatal renal function is not attempted. To improve selection of a group of fetuses eligible for prenatal therapy, an approach could be to further refine the information inferred from the ultrasound parameters and diminish the subjectivity of, for instance, assessing hyperechogenicity of the renal cortex. A novel approach that needs investigation could be the use of objective tools, such as a gray-scale histogram to infer the residual renal function.24 The other remaining challenge is to investigate the best therapeutic modality after risk stratification. Previous studies have compared VAS versus no fetal therapy, or fetal cystoscopy versus no fetal intervention.25 The aims of the randomized controlled PLUTO trail were to determine the efficacy and safety of vesico-amniotic shunting in lower urinary tract obstruction. Unfortunately the trial was prematurely stopped because of low inclusion rates. Although power for significant results was not achieved, the study suggested a potential benefit for survival in the intervention group (VAS placement) versus the expectant management one.26,27,28 The non-randomized cohort of Ruano etal confirmed these results showing improvement of the survival rate in the first 6 months in cases of severe LUTO after fetal intervention as VAS or cystoscopy.29 However, as suggested by the recent review of Nassr et al, including the above mentioned studies, it may well be that only cystoscopy,

8
127
Prediction of postnatal renal function
rather that VAS, may contribute to prevention of renal function impairment and increase perinatal survival.30 However, it must be stressed that, in spite of this encouraging short-term results, the degree of renal impairment after 1-2 year survival remains uncertain and needs further investigation.
In conclusion, our study has shown that a prediction model, incorporating ultrasound parameters such as cortical appearance, keyhole sign of the bladder and abnormal amniotic fluid volume can make a fairly accurate prediction of an eGFR above or below 60 ml/min*1.73m2, considered as the critical cut-off between acceptable and expected poor renal function. Once the predictive ability of the model is validated in another set of data, this tool could be used to provide parents with tailored counseling and possibly give a better risk stratification of fetuses with LUTO eligible for fetal interventions. Future research is needed to improve the efficacy of renal kidney function predictors and answer the question regarding which therapeutic modality has to be applied in order to preserve and prevent further deterioration of the fetal renal function.

128
Chapter 8
references
1. Queisser-Luft A, Stolz G, Wiesel A, Schlaefer K, Spanger J. Malformations in newborn: results based on 30,940 infants and fetuses from the Mainz congenital birth defect monitoring system (1990-1998). Arch GynecolObstet 2002; 266: 163-167.
2. Wong H, Mylrea K, Feber J, Drukker A, Filler G. Prevalence of complications in children with chronic kidney disease according to KDOQI. KidneyInt2006; 70(3):585-590.
3. Chesnaye N. Bonthuis M, Schaefer F, Groothoff JW et al. Demographics of paediatric renal replacement therapy in Europe: a report of the ESPN/ERA-EDTA registry. PediatrNephrol 2014; 29: 2403-2410.
4. Wuhl E. Timing and outcome of renal replacement therapy in patients with congenital malformations of the kidney and urinary tract. ClinJAmSocNephrol 2013; 8: 67-74
5. Anumba DO, Scott JE, Plant ND, Robson SC. Diagnosis and outcome of lower urinary tract obstruction in the northern region of England. PrenatDaign2005;25:7-13.
6. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction:a population-based epidemiological study. BJOG 2012;119:1455-1464.
7. Muller F, Dommergues M, Bussières L, Lortat-Jacob S, Loirat C, Oury J, Aigrain Y, Niaudet P, Aegerter P, Dumez Y. Development of human renal function: reference intervals for 10 biochemical markers in fetal urine. ClinChem1996;42(11):1855-1860.
8. Muller F, Dommergues M, Mandelbrot L, Aubry M, Nihoul-Fekete C, Dumez Y. Fetal urinary biochemistry predicts postnatal renal function in children with bilateral obstructive uropaties. ObstetGynecol1993;82:813-820.
9. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL. New equations to estimate GFR in children with CKD. JAmSocNephrol2009;20:629-637.
10. Levin A, Stevens PE. Summary of KDIGO 2012 CKD Guideline: behind the scenes, need for guidance, and a framework for moving forward. KidneyInt. 2014;85(1):49-61.
11. Grignon A. Filion R, Filiatrault D. Urinary tract dilatation in utero. Classification and clinical applications. Radiology 1986;160:645-647.
12. Collins GS, Reitsma JB, Altman DG, Moons KGM. Transparent reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. AnnInternMed.2015;162:55-63.
13. Moons KGM, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ2009;338:b375.
14. Royston P, Moons KGM, Altman DG, Vergouwe Y. Prognosis and prognostic research: Developing a prognostic model. BMJ2009;338:b604.
15. Fontanella F, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Bilardo CM. Fetal megacystis: prediction of spontaneous resolution and outcome. UltrasoundObstetGynecol 2017;50(4):458-463.
16. Morris RK, Malin GL,Khan KS, Kilby MD. Antenatal ultrasound to predict postnatal renal function in congenital lower urinary tract obstruction: systematic review of test accuracy. BJOG 2009; 116:1290-1299.
17. Morris RK, Quinlan-Jones E, Kilby MD, Khan KS. Systematic review of accuracy of fetal urine analysis to predict poor postnatal renal function in cases of congenital urinary tract obstruction. PrenatDiagn 2007; 27:900-911.
18. Abdennadher W, Chalouhi G, dreux S, Rosenblatt J, Favre R, Guimiot F, Salomon LJ, Oury JF, Ville Y, Muller F. Fetal urine biochemistry at 13-23 weeks of gestation in lower urinary tract obstruction: criteria for in-utero treatment. UltrasoundObstetGynecol2015;46:306-311.
19. Nassr A, Koh Koh C, Shamshirsaz AA, Espinoza J, Sangi-Haghpeykar H, Sharhan D, Welty S, Angelo J, Roth D, Belfort MA, Braun M, Ruano R. Are ultrasound renal aspects associated with urinary biochemistry in fetuses with lower urinary tract obstruction? PrenatDiagn2016;36:1206-1210.
20. Kleinrouweler CE, Cheong-See FM, Collins GS, Kwee A, Thangaratinam S, Khan KS, Mol BWJ, Pajkrt E, Moons KGM, Schuit E. Prognostic models in obstetrics: available but far from applicable. Am J Obstet Gynecol 2016;214(1):79-90.e36.
8
129
Prediction of postnatal renal function
21. Ruano R, Sananes N, Wilson C, Au J, Koh CJ, Gargollo P, Shamshirsaz AA, Espinoza J, Safdar A, Moaddab A, Meyer N, Cass DL, Olutoye OO, Olutoye OA, welty S, Roth DR, Braun MC, Belfort MA. Fetal lower urinary tract obstruction: proposal for standardized multidisciplinary prenatal management based on disease severity. UltrasoundObstetGynecol2016;48:476-482.
22. Ruano R, Dunn T, Braun MC, Angelo JR, Safdar A. Lower urinary tract obstruction: fetal intervention based on prenatal staging. PediatrNephrol 2017;21
23. Farrugia MK, Braun MC, Peters CA, Ruano R, Herndon CD. Report on The Society for Fetal Urology panel discussion on the selection criteria and intervention for fetal bladder outlet obstruction. JPediatrUrol 2017, http://dx.doi.org/10.1016/j.jpurol.2017.02.021
24. Murata S, Sugiyama N, Maemura K Otsuki Y. Quantified kidney echogenicity in mice with renal ischemia reperfusion injury: evaluation as a noninvasive biomarker of acute kidney injury. Med Mol Morphol2017;50(3):161-169.
25. Smith-Harrison L, Hougen H, Timberlake M, Corbett S. Current applications of in utero intervention for lower urinary tract obstruction. JPediatrUrol2015;11:341-347.
26. Morris MK, Malin GL, Quinlan-Jones E, Middleton LJ,Hemming K, Burk D, Daniels DB, Khan KS, Deeks J, Kilby MD. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): a randomized trial. Lancet2013; 382:1496-1506.
27. Morris R, Kilby M. An overview of the literature on congenital lower urinary tract obstruction and introduction to the PLUTO trail: percutaneous shunting in lower urinary tract obstruction. ANZJOG2009;49:6-10.
28. Diwakar L, Morris R, Barton P, Middleton L, Kilby, Roberts T. Evaluation of the cost effectiveness of vesico-amniotic shunting in the management of congenital lower urinary tract obstruction (Based on data from the PLUTO trail). PLoSONE2013;8(12):1-10
29. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: a multicenter case – control study comparing fetal cystoscopy with vesicoamniotic shunting. UltrasoundObstetGynecol 2015;45:452-458.
30. Nassr AA, Shazly SAM, Abdelmagied AM, Aroujo Júnior E, Tonni G, Kilby MD, Ruano R. Effectiveness of vesicoamniotic shunt in fetuses with congenital lower urinary tract obstruction: an updated systematic review and meta-analysis. UltrasoundObstetGynecol2017;49:696-703.


Final discussion and future perspectives
9

132
Chapter 9

9
133
Final discussion and future perspectives
Summary
Fetal megacystis and congenital LUTO are severe conditions with challenging diagnostic work-up and controversial antenatal management (1)(2)(3)(4). In the previous chapters, we have reported in detail the results of a retrospective multicenter national study and a cross-sectional prospective study, with the main aim of providing clinicians with robust data regarding the differential diagnosis and management of fetal megacystis and LUTO. In summary, we firstly focused on the definition and differential diagnosis of megacystis (part 1); secondly, we aimed at optimizing patient selection in cases with isolated LUTO, theoretically eligible for antenatal intervention (part 2); finally, we concentrated on the antenatal prediction of prognosis in LUTO, both in terms of survival and postnatal renal function (part 3). In this last chapter, we provide a general overview of our results and present three management algorithms (figure 1, 2 and 3), developed on the base of our findings. To conclude, future perspectives and limitations of this thesis will be discussed.
From fetal megacystis to LUtO
The suspicion of LUTO typically arises from the evidence of an enlarged fetal bladder, also known as megacystis (1)(2). However, whenever faced with either early (diagnosed before or at the 17th week of gestation) or late megacystis (diagnosed after the 17th week of gestation), a number of underlying conditions and associated structural anomalies need to be considered and excluded (2)(6).
In chapter 3, the etiologies of megacystis were investigated and in 33% of cases an underlying chromosomal abnormality, genetic syndrome or developmental anomaly cases was found. Fetal medicine specialists should be aware that fetal megacystis may appear as a corollary finding of an underlying genetic disorder and that associated structural anomalies can be detected in 30-34% of cases (chapter 3)(2)(6)(7).
At the light of this evidence, as shown in figure 1 and 2, we recommend to perform a detailed ultrasound scan, with special attention for the spine, skeleton and hear. It is also crucial to verify fetal sex as early as possible, since female fetuses carry a much worse prognosis, due to the common involvement of other abnormally developed organs. Moreover, amniocentesis or chorionic villus sampling (CVS) with QF-PCR should be offered more liberally in view of the well-known association between megacystis and chromosomal abnormalities, of which trisomy18 is the most frequent. Furthermore, in case of negative QF-PCR result and depending on the detected structural anomalies, arrays CHG and even prenatal WES or fetal MRI may be considered.
Fetal Magnetic Resonance Imaging (MRI), using single-shot fast-spin ECHO techniques,

134
Chapter 9
Early megacystis (≤17th weeks’ gestation)
Detailed ultrasound examination with full anatomic survey + karyotyping (QF-PCR with fetal sex)
Presence of associated anomalies
Absence of associated anomalies
Consider further investigations (array CHG, fetal MRI) for excluding:
ANM, cloacal anomalies VACTERL association OEIS and CRS
Measure LBD
LBD > 12 mm LBD ≤ 12 mm
Repeat weekly US scan (resolution in 70% of cases)
Resolution before 23 weeks
Resolution after 23 weeks
Good prognosis
Recheck postnatal
Consider: - UA (in case of associated UCC) - PUV - MMHIS
See next flowchart (figure 3)
Figure 1. Clinical algorithm to guide fetal specialists in the diagnostic work-up and management of early megacystis.
NT, nuchal translucency; LBD longitudinal bladder diameter; MRI, magnetic resonance imaging; UA, urethral atresia; PUV, posterior urethral valves; MMIHS, megacystis microcolon intestinal hypoperistalsis syndrome.

9
135
Final discussion and future perspectives
Consider further investigations (array CHG, fetal MRI) for excluding:
22q11 deletion Overgrowth syndromes MMHIS
Measure LBD
LBD ≤ 22 mm LBD > 22 mm
Measure AFI, ureteral diameters, bladder volume and calculate LUTO score
Late megacystis (>17th weeks’ gestation)
Good prognosis
No Resolution before 23 weeks
Score ≥ 9.5 .5
Score < 9.5
Consider isolated LUTO
Consider VUR and MMHIS See next flowchart (figure 3)
Check growth charts (Chapter 1) + Detailed fetal ultrasound + fetal echocardiography + karyotyping (QF-PCR with fetal sex)
Presence of associated anomalies
Absence of associated anomalies
Resolution before 23 weeks
Figure 2. Clinical algorithm to guide fetal specialists in the diagnostic work-up and management of late megacystis.
LBD longitudinal bladder diameter; MRI, magnetic resonance imaging; VUR, vesicoureteral reflux; MMIHS, megacystis microcolon intestinal hypoperistalsis syndrome.

136
Chapter 9
can in fact provide better imaging of fetal anatomy in case of severe oligo- or anhydramnios or suspicion of an anorectal malformation (8)(9). Array CHG should be in particular offered when heart defects are detected in order to exclude a 22q11 deletion syndrome (chapter 3)(10)(11).Other miscellaneous non-classic chromosomal abnormalities (e.g. duplication 19q13.33; deletion 5q.35.2; etc.) can be detected by array CGH in fetuses with isolated megacystis, however their clinical significance is uncertain for most of them (chapter 3).
Once complex megacystis and associated anomalies have been ruled out, the possibility of spontaneous resolution should be considered (12). From chapter 4, it can be inferred that the LBD measurement can reliably estimate the chance of resolution. In particular, the bladder enlargement will spontaneously regress in 70% of fetuses with early megacystis and LBD ≤12 mm (chapter 4), and cases of megacystis resolving before 23weeks’ gestation have generally a favorable outcome without major urological sequelae. The underlying cause for this transitory bladder enlargement may be sought, as previously suggested, in the immaturity of autonomic innervation and smooth muscle fibers in early gestation (12).
antenatal diagnosis of LUtO and eligibility for fetal therapy
In order to offer parents appropriate therapeutic options for LUTO and avoid meaningless interventions, only cases theoretically eligible for antenatal intervention should be selected (13). Although this concept may seem trivial and the diagnosis of LUTO may be considered straightforward, previous studies have highlighted that one third of all prenatally suspected LUTO are reclassified postnatally, with the majority of them reclassified to vesico-ureteral reflux (VUR)(14). Such cases would not benefit from in utero treatment and need to be identified prenatally (13).
In chapter 5, we investigated the best antenatal criteria for identifying, among fetuses with early megacystis, those with isolated posterior urethral valves (PUV), theoretically eligible for early fetal treatment. This approach demonstrated good accuracy with a sensitivity of 82% and a specificity of 68% (chapter 4). As shown in figure 1, we also found that the finding of an associated umbilical cord cyst (UCC) carried a high risk of urethral atresia (OR 15; p=0.3), which is an unfavorable form of LUTO, not eligible for early fetal cystoscopy (chapter 4). This finding confirms the hypothesis of Sepulveda et al., who speculated that an abnormally distended bladder may prevent the closure of the allantois in the first stages of life, when bladder is connected with the umbilical cord (15)(16), and may eventually lead to a cystic dilatation of the umbilical cord. This is more likely to occur in fetuses with an early and severe bladder enlargement, as it is the case in the setting of urethral atresia (17)(chapter 5).
As shown in the second algorithm in figure 2, a standardized US approach with the assessment of bladder volume, ureters, amniotic fluid (AF) amount and fetal gender, should

9
137
Final discussion and future perspectives
be carried out in fetuses with late megacystis. This recommendation originates from our findings in chapter 6, where the optimal combination of US parameters for diagnosing LUTO has been investigated (chapter 6). The assessment of these five antenatal parameters, and their combination in a clinical score, showed good discriminative capacity for predicting LUTO and reducing the number of false positive diagnoses (chapter 6). However, an external validation of these results is essential before endorsing this statement and supporting its clinical applicability.
Clinical heterogeneity and underlying pathophysiology of LUtO
In fetuses highly suspected for isolated LUTO, antenatal counseling and management should be individualized on the base of the expected outcome. This is made problematic by the highly variable natural history and outcome of LUTO. In fact, severe forms of LUTO can lead to early and massive bladder distention, renal dysplasia, oligohydramnios, and eventual soft tissue deformities (Potter sequence) (18)(19). Conversely, fetuses with milder forms of LUTO can even preserve normal AF amount throughout pregnancy and favorable renal function after birth (20). This heterogeneity in the clinical presentation of LUTO can be partially explained by two factors: the type of obstruction, and the reaction to the obstructive insult, with the occasional occurrence of a pressure ‘pop-off’ mechanism.
The term LUTO refers to a heterogeneous group of anatomical defects, that includes urethral atresia, urethral valves and urethral stenosis. Urethral atresia (UA), defined as complete infravesical obstruction that obliterates the distalmost portion of the prostatic urethra, represents the most severe form of LUTO with very poor prognosis (21). Urethral stenosis constitutes a less common and less severe variant of UA and presents with narrowing of the urethral lumen. Urethral valves can be distinguished in anterior urethral valves (AUV), caused by a mucosal fold arising from the floor of the urethra (22)(23), and posterior urethral valves (PUV), that constitute the most common cause of LUTO with a birth prevalence of 1 to 2 per 10,000 live male births (24)(25). Three types of PUV have been described by Hugh Hampton Young (26)(27). Type I valves are the most frequent and appear as leaflets originating from verumontanum and extending in an inferior and anterior direction. Type II valves are not obstructive and represent mucosal folds extending superiorly from the verumontanum to the bladder neck. Type III valves appear as an annular ring or membrane in the posterior urethra (26).
Irrespective of obstruction type, LUTO can progress differently case per case: with megacystis or bladder wall fibrosis, with unilateral or bilateral hydronephrosis, with renal dysplasia or severe vesicoureteral reflux (28). This clinical heterogeneity can be partially explained also by the occurrence of a number of “pop-off” mechanisms, developed as

138
Chapter 9
response to the increased intraluminal pressure within the urinary tract. Pop-off mechanisms could protect the urinary system from the deleterious effects of elevated bladder pressure by allowing urine to extravasate: into the peritoneal cavity (urinary ascites), within the perirenal space or retroperitoneum (urinomas) or in the umbilical cord (umbilical cord cyst and patent urachus). Another pop-off mechanisms is represented by the cystic dilatation of the ureter (ureterocele), that in some cases can expand into the bladder and obstruct the urine outflow, thus constituting a non-classic and infrequent cause of LUTO (obstructive ureterocele) (26). The development of bladder diverticula or unilateral vesico-ureteral reflux have been also defined as pop-off mechanisms (29)(30).
To date, antenatal pop-off mechanisms of LUTO have been little studied and their role in terms of perinatal and long-term outcome has not been yet elucidated. It still not clear whether they could protect the urinary system from the deleterious effects of an elevated vesical pressure or they could rather indicate the presence of a severe insult that will anyway entail bladder and urinary dysfunctions later in life (30). Hereby in Table1, we report on the incidence of some of these pop-off mechanisms in our retrospective cohort.
table 1. Incidence and GA at diagnosis in fetuses developing or not a pop-off mechanism.
Incidence GA at diagnosis of megacystis
Urinary Ascites 41 (8%) 20 ±6
UCC 41 (8%) 16 ±6*
Urinomas/ureterocele 27 (5%) 24 ±7
Rest of the population 432 (80%) 21 ±8
UCC, umbilical cord cyst; GA, gestational age; ANM, anorectal malformations; TOP, terminations of pregnancy; IUFD, intrauterine fetal death; eGFR, estimated glomerular filtration rate.
Staging of LUtO
The type of obstruction and the occasional development of pop-off mechanisms can partially account for the erratic variability in the clinical presentation of LUTO, that leads to a different timing and severity of urinary distension, oligohydramnios and renal impairment. Although the anatomical details of the urinary obstruction cannot be established during fetal life, their effects in term of urinary distension and progression to oligohydramnios can be more easily assessed.
For this reason, in the last part of the thesis, we focused on a series of US parameters to predict perinatal mortality and postnatal renal function of LUTO (chapter 7 and 8). Figure 3 summarizes our results in the form of a management algorithm, specifically formulated for male fetuses at high risk of LUTO, selected by following the two previous algorithms

9
139
Final discussion and future perspectives
(figure 1 and 2). However, it is probably essential to specify that female fetuses with LUTO are generally anyway excluded from fetal therapeutic interventions, since they almost invariably have a poor prognosis and extensive anomalies in the genitourinary region, including bowel, uterus and pelvic floor.
In chapter 6, we have shown that the risk of perinatal mortality can be estimated by considering gestational age at first evidence of oligo- or anhydramnios, and the bladder volume at diagnosis. According to these two criteria, the severity of LUTO can be classified as severe, moderate of mild, entailing a perinatal mortality of 55%, 26% or 9%, respectively (chapter 7).
Antenatal determination of renal injury in obstructive uropathy has been so far considered problematic (31). Previous observational studies reported that the accuracy of prenatal ultrasound for predicting renal function has low sensitivity and specificity (31)(32).
In chapter 5, we tried to elaborate a model based on prenatal US examination to predict postnatal renal function. We found that evidence of keyhole sign, hyperechogenicity of the renal cortex and abnormal amniotic fluid volume at diagnosis were associated with poor postnatal renal function (chapter 8).
On the basis of the proposed staging system and the predicted postnatal renal function, the parents can be extensively counseled on the management options. In the majority of cases, parents will opt for terminating the pregnancy or for an expectative management (33)(4)(34). In a minority of cases, fetal intervention can be attempted.
Management of LUtO
As discussed in the introduction of the thesis, the first antenatal therapeutically attempt for LUTO consisted in a bilateral utererostomies performed in open fetal surgery (35). This technique was promptly abandoned in favor of percutaneous vesico-amniotic shunting (VAS), that currently represents the most commonly used method to relieve the obstruction (36)(37). VAS has been widely used for at least 25 years and more than 300 cases of shunt-treatment have been reported in the literature (37). During these years, different types of shunts have been developed, and a number of complications, such as shunt displacement, shunt blockage, preterm labor, chorio-amnionitis, iatrogenic gastroschisis and urinary ascites, have been reported (13).
Few studies have analyzed the pro and con of each shunt, therefore hereby, in table 2, we report an overview of their main characteristics.
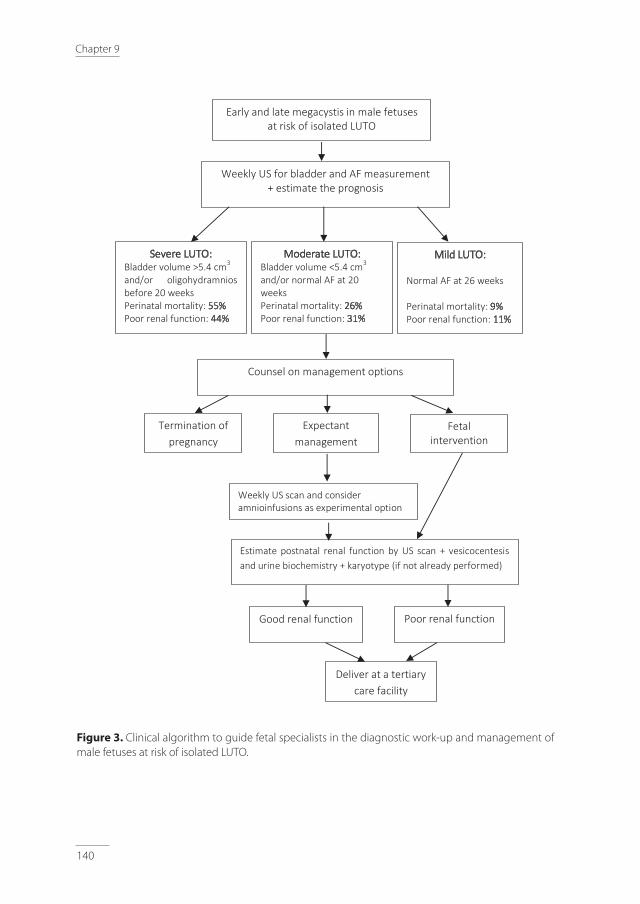
140
Chapter 9
Weekly US for bladder and AF measurement + estimate the prognosis
Severe LUTO: Bladder volume >5.4 cm3 and/or oligohydramnios before 20 weeks Perinatal mortality: 55% Poor renal function: 44%
Moderate LUTO: Bladder volume <5.4 cm3 and/or normal AF at 20 weeks Perinatal mortality: 26% Poor renal function: 31%
Mild LUTO: Normal AF at 26 weeks Perinatal mortality: 9% Poor renal function: 11%
Counsel on management options
Expectant management
Fetal intervention
Estimate postnatal renal function by US scan + vesicocentesis and urine biochemistry + karyotype (if not already performed)
Good renal function
Poor renal function
Early and late megacystis in male fetuses at risk of isolated LUTO
Weekly US scan and consider amnioinfusions as experimental option
Termination of pregnancy
Deliver at a tertiary care facility
Figure 3. Clinical algorithm to guide fetal specialists in the diagnostic work-up and management of male fetuses at risk of isolated LUTO.
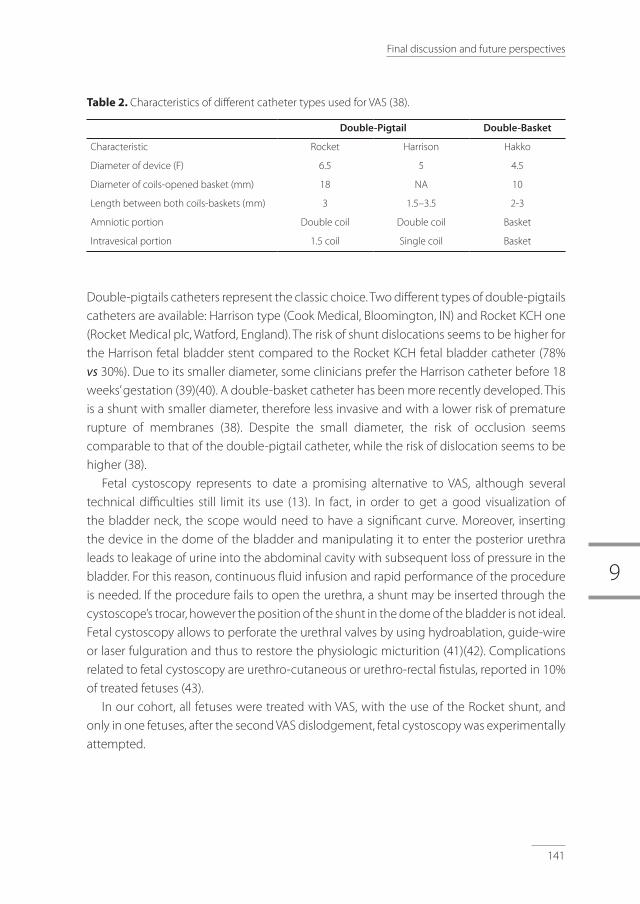
9
141
Final discussion and future perspectives
table 2. Characteristics of different catheter types used for VAS (38).
Double-Pigtail Double-Basket
Characteristic Rocket Harrison Hakko
Diameter of device (F) 6.5 5 4.5
Diameter of coils-opened basket (mm) 18 NA 10
Length between both coils-baskets (mm) 3 1.5–3.5 2-3
Amniotic portion Double coil Double coil Basket
Intravesical portion 1.5 coil Single coil Basket
Double-pigtails catheters represent the classic choice. Two different types of double-pigtails catheters are available: Harrison type (Cook Medical, Bloomington, IN) and Rocket KCH one (Rocket Medical plc, Watford, England). The risk of shunt dislocations seems to be higher for the Harrison fetal bladder stent compared to the Rocket KCH fetal bladder catheter (78% vs 30%). Due to its smaller diameter, some clinicians prefer the Harrison catheter before 18 weeks’ gestation (39)(40). A double-basket catheter has been more recently developed. This is a shunt with smaller diameter, therefore less invasive and with a lower risk of premature rupture of membranes (38). Despite the small diameter, the risk of occlusion seems comparable to that of the double-pigtail catheter, while the risk of dislocation seems to be higher (38).
Fetal cystoscopy represents to date a promising alternative to VAS, although several technical difficulties still limit its use (13). In fact, in order to get a good visualization of the bladder neck, the scope would need to have a significant curve. Moreover, inserting the device in the dome of the bladder and manipulating it to enter the posterior urethra leads to leakage of urine into the abdominal cavity with subsequent loss of pressure in the bladder. For this reason, continuous fluid infusion and rapid performance of the procedure is needed. If the procedure fails to open the urethra, a shunt may be inserted through the cystoscope’s trocar, however the position of the shunt in the dome of the bladder is not ideal. Fetal cystoscopy allows to perforate the urethral valves by using hydroablation, guide-wire or laser fulguration and thus to restore the physiologic micturition (41)(42). Complications related to fetal cystoscopy are urethro-cutaneous or urethro-rectal fistulas, reported in 10% of treated fetuses (43).
In our cohort, all fetuses were treated with VAS, with the use of the Rocket shunt, and only in one fetuses, after the second VAS dislodgement, fetal cystoscopy was experimentally attempted.

142
Chapter 9
Limitations and strength of this thesis.
A number of potential limitations of this thesis needs to be acknowledged. Firstly, our results, except those from chapter 1, have been based on a retrospective study. The retrospective study design nature has limited the possibility to obtain specific measurements (such as urinary biochemistry, serial measurements, 3D bladder volume, echogenicity of renal parenchyma) in all cases. Despite this major limitation, the nationwide setting of this project constitutes a major strength of the thesis, and makes of this study the largest thus far published datasets on this topic.
In this thesis, the bladder volume showed to have a central role for the diagnostic and prognostic assessment of megacystis and LUTO. Based on our results, we strongly recommended to incorporate the bladder measurement in the standard assessment of fetal megacystis and congenital LUTO. In the study the bladder volume was mathematically calculated from the three bladder diameters, rather than directly measured by the 3D US. This implied a bias due to the inaccuracy of the available formulas for measuring the fetal bladder (45)(46). We speculate that the bladder volume, measured by using 3D US, could have an even stronger prognostic and diagnostic value and future studies in this direction are needed. Moreover, for defining second and third trimester megacystis, we did not used a specific cut-off for the bladder enlargement but rather the most commonly used definition of a bladder failing to empty within 40 minutes. In fact, when our retrospective data collection was started, no reference range for defining an abnormally enlarged bladder was available. For this reason, we started to construct prospectively fetal bladder growth charts in Chapter 1.
Another crucial limitation of this study is the lack of an external validation for our proposed prediction models (chapter 5, 6 and 7). External validation is of paramount importance to judge the applicability of a prognostic model in a population outside the scope where the data have been derived from.
Future perspectives and challenges
Improvements in diagnostic accuracy of LUTO: Fetal MRI, grey-scale histogram, urine analysis and combined approaches.In this thesis we relied upon clinical data from antenatal US investigations. However, further attention to other additional diagnostic tools should be paid.
For instance, MRI, a technique increasingly used in fetal imaging (9)(8), may be explored for its value in assessing more accurately renal cortex integrity and lung development, as suggested by Craig Peters in a panel discussion at the Society of Fetal Urology (47).

9
143
Final discussion and future perspectives
Alternatively to the MRI, the use of grey-scale histogram may be tested for a more objective evaluation of the echogenicity of fetal renal parenchyma, which has proven to be, among all the other US parameters, the most reliable to predict postnatal renal function (32)(chapter 8).
To date, fetal urine analysis following serial vesicocentesis is standardly performed to estimate renal function before proceeding with any further intervention. Commonly, sodium, chloride, calcium, osmolarity and β2-microglobulin are evaluated, however data on their diagnostic ability are still conflicting (48)(49) and a systematic review reported that none of those analytes yields sufficient clinical accuracy for predicting renal function (48). Moreover, age-based reference ranges are to date available only for sodium and calcium (29), while the current established thresholds for the other analytes are only intended for fetuses undergoing fetal therapy (29). There has been an increasing interest in investigating a number of biochemical marker, such as α1-microglobulin, retinal binding protein, transforming growth factor-β, epidermal growth factor (29)(50), and more recently, the cystatine C and matrix metalloproteinase (MMP-9), independent predictors of severity of renal fibrosis. However, their clinical application has never been validated (31).
Future studies are recommended to combine measurement of the above mentioned analytes with a more standardized US evaluation of LUTO.
Improvements in for future RCT: patient selection, data sharing and technical advancements.At this moment to be able to identify the best candidates and timing for fetal therapy is of pivotal importance to improve clinical outcome in LUTO. The logic continuation of the studies published in this thesis will be to select cases by using our diagnostic and prognostic criteria and, according to the baseline LUTO severity, ascertain when fetal therapy would be more successful. We deliberately did not evaluate the success of fetal therapy in our cohort, due to the small sample of treated fetuses (n = 24). However, future investigations in this direction are recommended, preferably in the setting of an adequately powered randomized controlled trial.
For this purpose, it must borne in mind that the low prevalence of LUTO and the high rate of terminations of pregnancy is likely to limit again the recruitment process, as it happened in the PLUTO trial (51). Therefore, more attention should also be paid on building large collaboration worldwide among the principal fetal surgery centers and on creating a more systematic approach to data sharing and frank disclosure of treatment failures.
Besides the refinements of the diagnostic criteria and patient selection of LUTO, more effort should be aimed at improving in the technical aspects of the procedures, in terms of minimizing the risks of shunt migration and blockage in VAS and develop new cystoscopes capable of making easier the visualization and entrance into the posterior urethra (13).

144
Chapter 9
9.8.3 Change of perspectives in fetal surgery. Classically, fetal surgery has been reserved to those fetuses with life-threatening conditions
and few chances of survival (52). With technical advancements, antenatal surgery has been offered not only as ultimate attempt to rescue cases with otherwise fatal prognosis, but also to improve long-term outcome in fetuses with non-life-threatening conditions. This approach is now already used in the antenatal management of myelomeningocele. In fact, prenatal surgical repair of this non-lethal condition aims at improving the neurological outcome compared to the post-natal repair (53)(54). Similarly, also the TOTAL trial offers tracheal occlusion more liberally to diaphragmatic hernia cases at the less severe end of the spectrum in the attempt to improve long-term outcome (55).
Concerning LUTO, fetal specialists still tend to treat cases with markedly reduced amniotic fluid and severe forms of LUTO. However, the severe deterioration of renal reserve among the severest phenotypes of LUTO may prevent an appropriate ‘rescue’ by fetal therapy. Conversely, the milder phenotypes may benefit more from fetal intervention (33). Timing is the central overarching theme in congenital LUTO and the best timing of in-utero therapy for preserving fetal renal function has not been yet clarified (26).
Concluding remarks
We hope that the results of this thesis, with the proposed stepwise management algorithms, will contribute to refine the diagnostic work-up and the prognostic assessment of fetuses suspected with LUTO. We also hope that this may encourage a new trial where fetal surgery, in the form of refined shunts or cystoscopy, may be offered also to fetuses with good chances of survival but high risk of postnatal morbidity and renal insufficiency. This change in perspective is probably the necessary step in order to make an impact on the overall outcome of fetuses prenatally diagnosed with LUTO.

9
145
Final discussion and future perspectives
references
1. Taghavi K, Sharpe C, Stringer MD. Fetal megacystis: A systematic review. J Pediatr Urol. 2017;13(1):7–15.
2. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, El-Ghoneimi A, Oury JF, Muller F.Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn. 2013;33(12):1162–6.
3. Fievet L, Faure A, Coze S, Harper L, Panait N, Braunstein D, Carson J, Gorincour G, Chaumoitre K, Guys JM, Alessandrini P, D’Ercole C, Merrot T. Fetal megacystis: Etiologies, management, and outcome according to the trimester. Urology. 2014;84(1):185–90.
4. Lissauer D, Morris RK, Kilby MD. Fetal lower urinary tract obstruction. Semin Fetal Neonatal Med. 2007;12(6):464–70.
5. Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol. 1996;8(6):387–90.
6. Fievet L, Faure A, Coze S, Harper L, Panait N, Braunstein D, Carson J, Gorincour G, Chaumoitre K, Guys JM, Alessandrini P, D’Ercole C, Merrot T. Fetal megacystis: Etiologies, management, and outcome according to the trimester. Urology. 2014;84(1):185–90.
7. Müller Brochut A-C, Thomann D, Kluwe W, Di Naro E, Kuhn A, Raio L. Fetal megacystis: experience of a single tertiary center in Switzerland over 20 years. Fetal Diagn Ther. 2014;36(3):215–22.
8. Calvo-Garcia MA. Imaging Evaluation of Fetal Megacystis: How Can Magnetic Resonance Imaging Help? Semin Ultrasound, CT MRI. 2015;36(6):537–49.
9. Abdelazim IA, Belal MM. The role of magnetic resonance imaging (MRI) in refining the diagnosis of suspected fetal renal anomalies. Asian Pacific J Reprod. 2012;1(3):193–7.
10. Wu HY, Rusnack SL, Bellah RD, Plachter N, McDONALD-McGINN DM, Zackai EH,Canning DA. Genitourinary malformations in chromosome 22q11. 2 deletion. J Urol. 2002;168(December):2564–2565.
11. Hacıhamdioğlu B, Hacıhamdioğlu D, Delil K. 22Q11 Deletion Syndrome: Current Perspective. Appl Clin Genet. 2015;8:123–32.
12. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 weeks of gestation: Chromosomal defects and outcome according to bladder length. Ultrasound Obstet Gynecol. 2003;21(4):338–41.
13. Kilby MD, Morris RK. Fetal therapy for the treatment of congenital bladder neck obstruction. Nat Rev Urol. 2014;11(7):412–9.
14. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: A population-based epidemiological study. BJOG An Int J Obstet Gynaecol. 2012;119(12):1455–64.
15. Sepulveda W, Rompel SM, Cafici D, Carstens E, Dezerega V. Megacystis associated with an umbilical cord cyst: a sonographic feature of a patent urachus in the first trimester. J Ultrasound Med. 2010;29(2):295–300.
16. Riddell JVB, Houle AM, Franc-Guimond J, Barrieras D. Prenatal vesico-allantoic cyst outcome - a spectrum from patent urachus to bladder exstrophy. Prenat Diagn. 2015;35(13):1342–6.
17. Robyr R, Benachi A, Daikha-Dahmane F, Martinovich J, Dumez Y, Ville Y. Correlation between ultrasound and anatomical findings in fetuses with lower urinary tract obstruction in the first half of pregnancy. Ultrasound Obstet Gynecol. 2005 May;25(5):478–82.
18. Wu S, Johnson MP. Fetal Lower Urinary Tract Obstruction. Clin Perinatol. 2009;36(2):377–90. Available from: http://dx.doi.org/10.1016/j.clp.2009.03.010
19. Christianson C, Huff D, McPherson E. Limb deformations in oligohydramnios sequence: Effects of gestational age and duration of oligohydramnios. Am J Med Genet. 1999;86(5):430–3.
20. Johnson MP, Danzer E, Koh J, Polzin W, Harman C, O ’shaughnessy R, Brown R, Zaretsky MV; North American Fetal Therapy Network (NAFTNet). Natural History of Fetal Lower Urinary Tract Obstruction with Normal Amniotic Fluid Volume at Initial Diagnosis.
21. Gonzalez R, De Filippo R, Jednak R, Barthold JS. Urethral atresia: long-term outcome in 6 children who survived the neonatal period. J Urol. 2001;165(6 Pt 2):2241–4.
22. Arena S, Romeo C, Borruto FA, Racchiusa S, Di Benedetto V, Arena F. Anterior urethral valves in children: An uncommon multipathogenic cause of obstructive uropathy. Pediatr Surg Int. 2009;25(7):613–6.

146
Chapter 9
23. Kibar Y, Coban H, Irkilata HC, Erdemir F, Seckin B, Dayanc M. Anterior urethral valves: An uncommon cause of obstructive uropathy in children. Vol. 3, Journal of Pediatric Urology. 2007. p. 350–3.
24. Lloyd JC, Wiener JS, Gargollo PC, Inman BA, Ross SS, Routh JC. Contemporary epidemiological trends in complex congenital genitourinary anomalies. J Urol. 2013;190(4 SUPPL):1590–5.
25. Hodges SJ, Patel B, McLorie G, Atala A. Posterior urethral valves. ScientificWorldJournal. 2009;9:1119–26.
26. Clayton DB, Brock JW. Lower Urinary Tract Obstruction in the Fetus and Neonate. Clin Perinatol. 2014;41(3):643–59.
27. Wainwright J. Congenital obstruction of the posterior urethra. Arch Dis Child. 1951;26(126):162–3.
28. Clayton DB, Brock JW. Lower Urinary Tract Obstruction in the Fetus and Neonate. Clin Perinatol. 2014;
29. Freedman a L, Johnson MP, Gonzalez R. Fetal therapy for obstructive uropathy: past, present.future? Pediatr Nephrol. 2000;14(2):167–76.
30. Kaefer M, Keating MA, Adams MC, Rink RC. Hydronephrosis: Clinical POSTERIOR URETHRAL VALVES, PRESSURE POP-OFFS AND BLADDER FUNCTION.
31. M. D. Kilby, D. Oepkes AJ. Fetal Therapy: Scientific Basis and Critical Appraisal of Clinical Benefits.
32. Morris RK, Malin GL, Khan KS, Kilby MD. Antenatal ultrasound to predict postnatal renal function in congenital lower urinary tract obstruction: Systematic review of test accuracy. Vol. 116, BJOG: An International Journal of Obstetrics and Gynaecology. 2009. p. 1290–9.
33. Morris RK, Kilby MD. An overview of the literature on congenital lower urinary tract obstruction and introduction to the PLUTO trial: Percutaneous shunting in lower urinary tract obstruction. Aust New Zeal J Obstet Gynaecol. 2009;49(1):6–10.
34. Morris RK, Kilby MD. Congenital urinary tract obstruction. Best Pract Res Clin Obstet Gynaecol. 2008;22(1):97–122.
35. Harrison MR, Golbus MS, Filly RA, Callen PW, Katz M, de Lorimier AA, Rosen M, Jonsen AR. Fetal surgery for congenital hydronephrosis. N Engl J Med. 1982;306(10):591–3.
36. Quintero R a, Gomez Castro LA, Bermudez C, Chmait RH, Kontopoulos E V. In utero management of fetal lower urinary tract obstruction with a novel shunt: a landmark development in fetal therapy. J Matern Fetal Neonatal Med. 2010;23(8):806–12.
37. Ruano R. Fetal surgery for severe lower urinary tract obstruction. Vol. 31, Prenatal Diagnosis. 2011. p. 667–74.
38. Jeong B-D, Won H-S, Lee M-Y. Perinatal Outcomes of Fetal Lower Urinary Tract Obstruction After Vesicoamniotic Shunting Using a Double-Basket Catheter. J Ultrasound Med. 2018;
39. Kurtz MP, Koh CJ, Jamail GA, Sangi-Haghpeykar H, Shamshirsaz AA, Espinoza J, Cass DL, Olutoye OO, Olutoye OA, Braun MC, Roth DR, Belfort MA, Ruano R. Factors associated with fetal shunt dislodgement in lower urinary tract obstruction. Prenat Diagn. 2016;36(8):720–5.
40. Ruano R, Sananes N, Wilson C, Au J, Koh CJ, Gargollo P,Shamshirsaz AA, Espinoza J, Safdar A, Moaddab A, Meyer N, Cass DL, Olutoye OO, Olutoye OA, Welty S, Roth DR, Braun MC, Belfort MA. Fetal lower urinary tract obstruction: proposal for standardized multidisciplinary prenatal management based on disease severity. Ultrasound Obstet Gynecol. 2016;48(4):476–82.
41. Haeri S. Fetal Lower Urinary Tract Obstruction (LUTO): a practical review for providers. Matern Heal Neonatol Perinatol. 2015;1:26.
42. Morris RK, Ruano R, Kilby MD. Effectiveness of fetal cystoscopy as a diagnostic and therapeutic intervention for lower urinary tract obstruction: a systematic review. Ultrasound Obs Gynecol. 2011;37:629–37.
43. Sananes N, Favre R, Koh CJ, Zaloszyc A, Braun MC, Roth DR,Moog R, Becmeur F, Belfort MA, Ruano R. Urological fistulas after fetal cystoscopic laser ablation of posterior urethral valves: Surgical technical aspects. Ultrasound Obstet Gynecol. 2015;45(2):183–9.
44. Carr MC. Commentary to “Report on the Society for Fetal Urology panel discussion on the selection criteria and intervention for fetal bladder outlet obstruction.” J Pediatr Urol. 2017;1–7.
45. Fägerquist M, Fägerquist U, Odén A, Blomberg SG. Estimation of fetal urinary bladder volume using the sum-of-cylinders method vs. the ellipsoid formula. Ultrasound Obstet Gynecol. 2003;22(1):67–73.
46. Hedriana HL, Moore TR. Accuracy limits of ultrasonograhic estimation of human fetal urinary flow rate. Am J Obstet Gynecol. 1994 Oct 1 [cited 2018 Jan 24];171(4):989–92.

9
147
Final discussion and future perspectives
47. Carr MC. Commentary to “Report on the Society for Fetal Urology panel discussion on the selection criteria and intervention for fetal bladder outlet obstruction.” J Pediatr Urol. 2017;5131.
48. Morris RK, Quinlan-Jones E, Kilby MD, Khan KS. Systematic review of accuracy of fetal urine analysis to predict poor postnatal renal function in cases of congenital urinary tract obstruction. Vol. 27, Prenatal Diagnosis. 2007. p. 900–11.
49. Abdennadher W, Chalouhi G, Dreux S, Rosenblatt J, Favre R, Guimiot F, Salomon LJ, Oury JF, Ville Y, Muller F. Fetal urine biochemistry at 13-23 weeks of gestation in lower urinary tract obstruction: Criteria for in-utero treatment. Ultrasound Obstet Gynecol. 2015;46(3):306–11.
50. Cobet G, Gummelt T, Bollmann R, Tennstedt C, Brux B. Assessment of serum levels of alpha-1-microglobulin, beta-2-microglobulin, and retinol binding protein in the fetal blood. A method for prenatal evaluation of renal function. Prenat Diagn. 1996;16(4):299–305.
51. Morris RK, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan SK, Deeks J., Kilby M., Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): A randomised trial. Lancet. 2013;
52. Luks FI. Requirements for fetal surgery: The diaphragmatic hernia model. Vol. 92, European Journal of Obstetrics Gynecology and Reproductive Biology. 2000. p. 115–8.
53. Adzick S, Thom E, Spong C, Brock J, Burrows P, Johnson M, Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB, D’Alton ME, Farmer DL; MOMS Investigators.A Randomized Trial of Prenatal versus Postnatal Repair of Myelomeningocele. N Engl J Med. 2011;365:883–91.
54. Adzick NS. Prospects for fetal surgery. Early Hum Dev. 2013 Nov 1 [cited 2018 Mar 19];89(11):881–6.
55. DeKoninck P, Gratacos E, Van Mieghem T, Richter J, Lewi P, Ancel AM,Allegaert K, Nicolaides K, Deprest J.Results of Fetal Endoscopic Tracheal Occlusion for congenital diaphragmatic hernia and the set up of the randomized controlled TOTAL trial. Early Hum Dev. 2011;87(9):619–24.


Summary in EnglishNederlandse samenvattingAbbreviationsAcknowledgmentsAbout the authorList of publications
10

150
Chapter 10

10
151
Summary in Englis
English summary
The term LUTO refers to a heterogeneous group of anatomical anomalies characterized by an obstruction in the urethra and by an increased intraluminal pressure along the urinary tract. During fetal life, LUTO leads to the development of an enlarged urinary bladder (also known as megacystis), severe hydronephrosis and oligohydramnios with high risk of early renal damage and perinatal mortality. Over the last 20 years, fetal therapy, in the form of vesico-amniotic shunt or fetal cystoscopy, has been attempted on the assumption that by relieving the intrauterine pressure caused by the obstruction, mortality and renal damage could be possible prevented. However, to date, whether and when the in-utero treatment should be offered is still a matter of debate, and the eventual selection of candidates remains suboptimal owing to the disappointing diagnostic accuracy of fetal LUTO.
Aim of this thesis was to gather at a national level, clinical data that would elucidate the natural history from fetal megacystis to congenital LUTO and guide fetal specialists in the challenging counseling, diagnostic work-up and antenatal management. The thesis is divided in three main parts.
Part I includes chapter 2, chapter 3 and chapter 4, and focuses on the differential diagnosis and definition of fetal megacystis. In chapter 2, we report for the first time in the literature reference values for the dimension of a normal urinary bladder in the second and third trimester of pregnancy. Chapter 3 presents an overview of the structural anomalies and congenital disorders associated with fetal megacystis. From this chapter we also conclude that fetal megacystis does not only occur in fetuses with LUTO, but it can be observed also as corollary finding of miscellaneous genetic syndromes, developmental disorders and chromosomal abnormalities. In chapter 4 we investigates the natural history of megacystis and demonstrates that the longitudinal bladder diameter and the gestational age at resolution of megacystis are reliable predictors of spontaneous resolution and outcome, respectively.
In Part II, we develop two management algorithms for optimizing the antenatal diagnosis of isolated LUTO with the aim of more accurately selecting those fetuses theoretically eligible for in-utero treatment. In chapter 5, we propose an algorithm for identifying fetuses with early megacystis and isolated posterior urethral valves. The visualization of an umbilical cord cyst appears to be a strong marker of the more severe urethral atresia. In chapter 6, we propose a clinical score for the optimal antenatal diagnosis of LUTO in the second and third trimester of pregnancy, as alternative to the commonly used LUTO triad (megacystis, keyhole sign and hydronephrosis). This score can accurately discriminate fetuses with LUTO from those with non-obstructive megacystis, a group non eligible to in-utero treatment.

152
Chapter 10
Finally, Part III of this thesis aims at predicting antenatally the prognosis of LUTO cases, in terms of survival and postnatal renal function. In chapter 7, we propose a staging system for congenital LUTO capable of predicting the severity of the condition and its prognosis in terms of perinatal survival. In chapter 8, a prediction model for postnatal renal function is presented.
The thesis ends with a general discussion of the implications of our findings and future perspective (chapter 9).

10
153
Nederlandse samenvatting
Nederlandse samenvatting
Bij een Lower Urinary Tract Obstruction (LUTO) is er sprake van een groep van anatomische afwijkingen gekenmerkt door een vernauwing of afsluiting van de plasbuis. Foetale LUTO leidt tot de ontwikkeling van een foetale megablaas met ernstige hydronefrose en oligohydramnion. Hierdoor is een LUTO geassocieerd met vroege nierbeschadiging en perinatale sterfte. In de afgelopen 20 jaar werd door middel van foetale therapie getracht om de obstructie in utero op te heffen door de plaatsing van een vesico-amniotische shunt of door foetale cystoscopie. Echter, op dit moment zijn de effectiviteit en de timing voor de in-utero therapie nog steeds niet duidelijk. Bovendien blijft de antenatale selectie van kandidaten nog steeds suboptimaal ten gevolge van de beperkte diagnostische nauwkeurigheid van foetale LUTO tijdens de zwangerschap.
Dit proefschrift richt zich op de differentiële diagnose, counseling en management van een foetale megablaas en LUTO. Het doel van dit proefschrift was om het pathofysiologische verloop van de foetale megablaas te presenteren op basis van landelijke data, en specialisten te begeleiden in de uitdagende counseling en prenatale behandeling van de foetale megablaas en LUTO.
Deel I van dit proefschrift richt zich op de differentiële diagnose en definitie van een foetale megablaas. In hoofdstuk 2 worden prospectieve referentiewaarden voor de dimensie van een normale urineblaas in het tweede en derde trimester van de zwangerschap gepresenteerd. Hoofdstuk 3 beschrijft de structurele anomalieën en aangeboren aandoeningen die geassocieerd zijn met een megablaas. Er kan geconcludeerd worden dat de foetale megablaas niet alleen een marker is voor LUTO maar ook is geassocieerd met een breed spectrum aan genetische syndromen, structurele en chromosomale afwijkingen. Hoofdstuk 4 richt zich op het fysiologische verloop van een foetale megablaas tijdens de zwangerschap. Waarbij de zwangerschapsduur bij de eventueel spontane resolutie van megablaas en de longitudinale blaasdiameter betrouwbare voorspellers zijn van respectievelijk de uitkomst en van de kans op resolutie van een megablaas.
Het doel van deel II van dit proefschrift was om de nauwkeurigheid van de prenatale diagnose van een geïsoleerde LUTO te optimaliseren. In hoofdstuk 5 hebben wij de antenatale criteria voor de optimale selectie van foetussen met een vroege megablaas en urethrakleppen die in theorie in aanmerking voor in-utero interventie komen, onderzocht. Tevens is aangetoond dat een navelstreng cyste in combinatie met een vroege megablaas een sterke marker is voor een urethrale atresie. Hoofdstuk 6 definieert een klinische echografische score om de nauwkeurigheid van de prenatale diagnostiek voor LUTO in het tweede en derde trimester te verbeteren.

154
Chapter 10
Deel III van dit proefschrift richt zich op prenatale voorspellers voor de postnatale en perinatale prognose. In hoofdstuk 7 presenteren we een echografisch stadiëringssysteem om de ernst van LUTO en het risico op perinatale sterfte te voorspellen. Hoofdstuk 8 gaat in op prenatale echografische voorspellers voor de postnatale nierfunctie.
Het proefschrift eindigt met een algemene discussie over de implicaties van onze bevindingen en toekomstperspectief (hoofdstuk 9).

10
155
Abbreviation
abbreviations
LUTO lower urinary tract obstructions LBD longitudinal bladder diameterUS ultrasoundVAS vesico-amniotic shuntPUV posterior urethral valvesRCT randomized controlled trial3D US three-dimensional ultrasoundSonoAVC Automated Volume CalculationsVOCAL Virtual Organ Computer-aided AnaLysisBV bladder volumeGE General electricsSD standard deviationGA gestational ageHUFP hourly urinary fetal productionAUC area under the curveUCC umbilical cord cystANM anorectal malformationsMCA multiple congenital anomaliesNT nucal translucency OR odds ratiocfDNA cell-free DNAPPV positive predictive valueNPV negative predictive valueROC-curve receiver operating characteristic curve AF amniotic fluideGFR estimated glomerular filtration rate TOTAL trial tracheal occlusion to accelerate lung growth trialPLUTO trial Percutaneous vesico-amniotic shunting versus conservative management for fetal lower urinary tract obstruction

10
157
Acknowledgments
acknowledgments
My first meeting with Prof. Bilardo took place in Groningen during my last year of Medical School. We met with the idea of carrying out a very short research project for my master’s thesis. This project did not start with the intention of publishing seven papers and writing a PhD thesis. Our idea was simply retrieving data on fetal megacystis between Groningen and Amsterdam. The situation got a bit out of hand; email by email Catia managed to involve all the academic centers in the Netherlands, months by months we managed to finish our prospective study, and so we ended up here. Dear Catia, it has been a beautiful adventure. Thank you for having firmly invested in this project and in me from that first meeting onwards, thank you for all the learning moments and for your constant and sincere support. The mutual affection of two human beings can be measured by the number of words they exchange, says M. Kundera, and I feel lucky for the amount of words exchanged with you, in the form of manuscripts, drafts, revisions, calls and meetings every time I needed. Grazie!
Once we focused on the natural history of fetal megacystis, many questions related to the antenatal management and treatment of LUTO easily came out. For this purpose, the collaboration and the expertise of the LUMC has been essential and I would like to sincerely thank Prof. Oepkes for his expertise and scientific contribution to this thesis, and Phebe Adama van Scheltema for having me helped from the beginning of this project with the data collection.
I would also like to sincerely thank Leonie Duin, who has guided me since day one of my arrival in Groningen: from the first short explanation about Astraia, to the first 3D ultrasound, to each practical help and encouragements for the clinical practice. Thanks a lot for your support!
My sincere gratitude goes to the reading committee and all the committee members for their time in reviewing this thesis, and thanks to Prof. Mark Kilby for his scientific contribution and availability in traveling twice from Birmingham up to Groningen.
-Science is the name but collaboration is the game- To Eva Pajkrt, Titia Cohen-Overbeek, Christine Willekes, Mireille Bekker and Caroline Bax goes my sincere acknowledgment for their collaboration during these years that made possible to conduct this research.
Thanks also to dr. Suresh Seshadri who allowed me to spend the last period of my PhD life in India. Thanks for the inspiring experience and for your warm hospitality at Mediscan!

158
Chapter 10
I would like to express my gratitude to Prof. Scherjon for his help and support in arranging my PhD trajectory.
To Henk Groen, thanks for your time, answers and supervision to all my questions in statistics.
To Valentina Gracchi, thanks for having always gladly shared your expertise in this field.
A sincere acknowledgment also goes to all the patients who agreed to participate to the FEBLA study and to Rixt and Sofia for their collaboration on working on the 3D images.
A special thanks also goes to my mentors from Rome, Prof. Di Iorio and dr. Margherita Pace for having me helped in arranging the first exchange period to Groningen.
To all the PND staff of UMCG, what a great team! Thanks for everything you taught me about antenatal ultrasound, for your help with the administration behind the FEBLA study, and thanks for your patience with my very first shy and reticent words in Dutch!! To Merel, thanks for your time in correcting the most difficult texts in Dutch and thanks for your precious reliability as colleague, friend and belayer!
Years can pass very fast when they are cheered by nice colleagues around you. Thanks Jan, Tom, Nastaran, Eva, Rikst Nynke, Violeta and whoever has worked on room Y4.228 even just for a while. Thanks for that atmosphere of caring and sharing both our failures and achievements. Thanks Laura and Luana for bringing to Groningen your spontaneity, enthusiasm and the best of our beautiful country. My deep gratitude goes to my colleague, friend and lovely paranymph Francesca. Thanks for having provided with a daily amount of jokes and uncontrollable laughter during these years, for all your help in organizing this day and still more thanks for being supportive every time I needed it.
From Groningen to Delft, I have been lucky to come across many new friends without whom my daily life would have been bleak. Thanks to Gabbia di Matti! A very heterogeneous group of people which has seen a number of people passing by Groningen as well a number of kingdoms succeeding year by year: from the vibrant authentic era of Queen Kappi the First, to the extravagant years of Queen Storm, until our current era guided by Queen Giuls the Lion and characterized by a huge amount of political debates on WhatsApp (sorry for the spam!). During these years, two things have never changed: our bond with this amazing city and our mayor doc Gabri. To Gabri goes my thanks for mentoring me during my first steps in Groningen until my first clinical stage at UMCG. To my sweet Pinkies goes my sincere love and gratitude for the warm and spontaneous pinky-atmosphere of sharing, caring

10
159
Acknowledgments
and laughing out loud, to Ciccio for our genuine friendship and for my favorite idiotic and brilliant moments in Groningen, and to Prof. Giuma thanks for our inspiring mid-afternoon lunches and calls. Thanks to all the people who felt part of this group for even just a short period: I have learned something from each of you!
From Groningen to Delft, I have also found good friends who supported me 24/7, even when a mouse comes to visit your bedside table in the middle of the night, or when suddenly your window collapses: one of the most surreal beer moments ever, with you there Giulia! thanks to both Alessandri, Elly, Giulia and Joe! To my friends, big family, colleagues, and to the Magnifici Dieci spread across Europe, thanks for every plane, train ticket, message and call aimed at let growing and strengthening our long-distance friendships. A special thanks goes to my Miks for the lifelong and silent emotional support and to Antonietta for making me feel at home every time I came back.
And here comes to the acknowledgements for my beautiful and strong family, who still support me whenever and from wherever. Thank you, mum, for your eternal example. Thanks for passing like clouds in the sky, for whispering to me how strong I can still be, and for reminding me that our love, kindness and knowledge is the best thing we can leave to this world. Dear Papa and Ala, your quiet presence during these years have preciously accompanied me step by step, from the first move to Groningen to the last moving out, thank you for staying silently always on my side and for being such a precious source of encouragements. Thanks, Papi for your support in taking that first plane and for your message once I landed, thanks for always desiring the best for me, and even at the cost of your own convenience. To my sister Laura: a tough woman, brilliant researcher, talented artist (thanks for your patience in painting cover and illustration of this thesis) and wonderful mother. You never stopped exceling in doing what you love and I am looking forward to seeing you shining again and again! And thanks to Giulio and Chow-Nadia for making me feel home even in Cachan.
Last but not least, thanks to Dems, my paranymph, best friend and favorite human being in this world. Sharing my days with you means genuinely enjoying life beyond any pre-packaged form of happiness, and seeking a balance in the midst of that dissatisfaction feeling that long drove us - always eager and never set -. Thanks for your endless and unconditional support, love and presence. Thank you for being my sourest critic and my most hardcore fan, for bringing out the best of me and for encouraging me to climb the most challenging routes together. Thanks, because no matter how far you can be, the first call is always for you.
Thank you, all folks!

160
Chapter 10

10
161
About the author
about the author
Federica was born on the 13th of November, 1989 in Rome, Italy. She grew up in Rome with her parents Teresa and Giampietro and her elder sister Laura. In 2008, she graduated from the scientific Liceum Malpighi and she was admitted to the Medical School in La Sapienza, University of Rome. During her third year of University, Federica started to attend the department of gynecology and obstetrics at San Peter Hospital, in Rome under the supervision of Prof. Di Iorio and in 2012 she obtained an Erasmus scholarship to study six months at the Medical University of Innsbruck. There, Federica had the possibility to observe for the first time in her life a procedure of fetal therapy in a twin pregnancy with twin-to-twin transfusion syndrome and her interest in gynecology and prenatal diagnosis grew further. Just after her return from Innsbruck, she obtained a scholarship that took her abroad once again, this time to write her Master’s thesis at the university of Groningen under the supervision of Prof. Bilardo. In 2014, she graduated in Medicine at the La Sapienza University with the highest marks and decided to come back to Groningen for a PhD trajectory. From 2015 to 2018, she collected data from the Netherlands to India, independently performed more than 300 three-dimensional ultrasounds for her research project, and managed to write this PhD thesis.

162
Chapter 10

10
163
List of publications
Publications
Fetal Megacystis: Prediction of spontaneous resolution and outcome. Fontanella F, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, Bilardo CM. Ultrasound in Obstetr and Gynecol 2017.
Yield of a 12-13-week scan for the early diagnosis of fetal congenital anomalies in the cell-free DNA era. Kenkhuis MJ, Bakker M, Bardi F, Fontanella F, Bakker MK, Fleurke-Rozema H, Bilardo CM. Ultrasound in Obstetr and Gynecol 2017.
Prenatal Evidence of Persistent Notochord and Absent Sacrum Caused by a Mutation in the T (Brachyury) Gene. Fontanella F, van Maarle MC, Robles de Medina P, Oostra RJ, van Rijn RR,Pajkrt E, Bilardo CM. Report in Obstetrics and Gynecology 2016.
Prenatal diagnosis of LUTO: how to improve diagnostic accuracy. Fontanella F, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, V. Gracchi, D. Oepkes and Bilardo CM. Ultrasound in Obstetr and Gynecol 2017.
Fetal megacystis: a lot more than LUTO. Fontanella F, L. Maggio, J. B. G. M. Verheij, Duin L,Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, D. Oepkes, Bilardo CM. Ultrasound in Obstetr and Gynecol. 2018
Antenatal work-up of early megacystis and selection of candidates for fetal therapy Fontanella F, L. Maggio, J. B. G. M. Verheij, Duin L, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, D. Oepkes, Bilardo CM. Fetal Diagnosis and Therapy 2018
Prediction model of postnatal renal function in fetuses with Lower Urinary Tract Obstruction: development and internal validation. Duin L, Fontanella F, Groen H, Adama van Scheltema PN, Cohen-Overbeek TE, Pajkrt E, Bekker M, Willekes C, Bax CJ, V. Gracchi, D. Oepkes and Bilardo CM. Submitted
Prediction of perinatal mortality and disease severity in congenital LUTO. Fontanella F, P. N. Adama van Scheltema, L. Duin, T. E. Cohen-Overbeek, E. Pajkrt, M. Bekker, C. Willekes, C. J. Bax, D. Oepkes and C.M. Bilardo. Ultrasound in Obstetr and Gynecol 2018
Reference curves for fetal urinary bladder in the second and third trimester of pregnancy. Fontanella F, H. Groen, Duin L, Bilardo CM. Submitted

164
Chapter 10
Oral communications at international conferencesMegacystis: risk stratification. F. Fontanella, L. Duin, Bilardo C. 16th World Conference in Fetal Medicine
Maggio, L., Elvan, A., Fontanella, F., & Bilardo, C. M. Grading the fetal echogenic bowel (EB): correlation between quantitative computerissed gray-scale analysis and subjective qualitative evaluation. 27th ISUOG World Conference
Fetal Megacystis: a lot more than LUTO, F. Fontanella, P. Adama Van Scheltema, V. Gracchi, T.E. Cohen-Overbeek, C. Willekes, M.N. Bekker, E. Pajkrt, D. Oepkes and C.M. Bilardo. 15th World Conference in Fetal Medicine
Vesico-amniotic shunting versus conservative management in fetal lower urinary tract obstruction: a 10-year registry, F. Fontanella, P. Adama Van Scheltema, V. Gracchi, T.E. Cohen-Overbeek, C. Willekes, M.N. Bekker, E. Pajkrt, D. Oepkes and C.M. Bilardo. 26th ISUOG World Conference
Spontaneous resolution of fetal megacystis: when and why? F. Fontanella, L. Duin, T.E. Cohen-Overbeek, M.N. Bekker, P. Adama Van Scheltema, C. Willekes, E. Pajkrt, C. Bax and C.M. Bilardo. 26th ISUOG World Conference
Prognostic value of umbilical cord cysts in fetal megacystisF. Fontanella, L. Duin, T.E. Cohen-Overbeek, M.N. Bekker, P. Adama Van Scheltema, C. Willekes, E. Pajkrt, C. Bax and C.M. Bilardo. 26th ISUOG World Conference
Antenatal Ultrasound prediction of postnatal renal function in congenital lower urinary tract obstruction F. Fontanella, P. Adama Van Scheltema, V. Gracchi, T.E. Cohen-Overbeek, C. Willekes, M.N. Bekker, E. Pajkrt, D. Oepkes and C.M. Bilardo. 24th ISUOG World Conference
Prices and grantsTop Publication Award 2018, SHARE institute - Rijksuniversiteit Groningen Top Publication Award 2017, SHARE institute - Rijksuniversiteit GroningenBest Oral Communication Award, ISUOG 24th World CongressShortlisted for Young Investigator Award, ISUOG 24th World CongressUniversity Scholarship for International Research Projects, La Sapienza UniversityUniversity Fellowship for International Research Projects, La Sapienza University

10
165
Research Institute SHARE
research Institute SHarE
This thesis is published within the Research Institute SHARE (Science in Healthy Ageing and healthcaRE) of the University Medical Center Groningen / University of Groningen.Further information regarding the institute and its research can be obtained from our internet site: http://www.share.umcg.nl/
More recent theses can be found in the list below.((co-) supervisors are between brackets)
2018
Dorland-Pel HFWork functioning in cancer patients: looking beyond return to work(profUBültmann,profAVRanchor,drFIAbma,drCAMRoelen)
Simoons MSomatic monitoring of patients with mood and anxiety disorders; problem definition, implementation and further explorations(profENvanRoon,profRASchoevers,drHMulder,drHGRuhé)
Bouma AJThe barrier-belief approach; a new perspective of changing behavior in primary care(profRLDiercks,profADijkstra,profCPvanWilgen)
Looijmans ALifestyle interventions in patients with a severe mental illness; addressing self-management and living environment to improve health(profRASchoevers,profRPStolk,drFJörg,drECorpeleijn)
Phí XABreast cancer screening in women at elevated risk; comparative evaluation of screening modalities to inform practice(profGHdeBock,profNHoussami,drMJWGreuter)
Kooiman TJMThe use of self-tracking technology for health(profCPvanderSchans,drMdeGroot,drAKooy)

166
Chapter 10
Schulz TAdjustment to kidney transplantation; predictors of perceived health and psychological distress(profAVRanchor,profRJPloeg,profJJHoman-vanderHeide,drJNiesing)
Verburg PEPregnancy outcome in South Australia; population and cohort studies(profJJHMErwich,profGADekker,profCTRoberts)
Krops LAPhysical activity in hard-to-reach physically disabled people; development, implementation and effectiveness of a community-based intervention(profJHBGeertzen,profPUDijkstra,drRDekker)
Golenia LA new perspective on the development of motor variability during middle childhood(profEOtten,drMMSchoemaker,drRMBongers)
Bebber J vanComputerized adaptive testing in primary care: CATja(profRRMeijer,drJTWWardenaar-Wigman,drAWunderink)
Drenth JCMotor function, paratonia and glycation cross-linked in older people; motor function decline and paratonia and their relation with Advanced Glycation End-products(profCPvanderSchans,profSUZuidema,profIBautmans,drJSMHobbelen)
Selivanova AHealth-state valuation using discrete choice models(profEBuskens,drPFMKrabbe)
For more 2018 and earlier theses visit our website