Understanding and Treating Anxiety in Individuals with Autism Spectrum Disorders C enter for A utism...
46
Understanding and Treating Anxiety in Individuals with Autism Spectrum Disorders Center for Autism and Related Disorders, I Doreen Granpeesheh, Ph.D., BCBA
-
Upload
laney-launder -
Category
Documents
-
view
216 -
download
1
Transcript of Understanding and Treating Anxiety in Individuals with Autism Spectrum Disorders C enter for A utism...

Understanding and Treating Anxiety
in Individuals with
Autism Spectrum Disorders
Center for Autism and Related Disorders, Inc
Doreen Granpeesheh, Ph.D., BCBA

Todays Lecture:
Exploring Anxiety in ourselves
What is Anxiety?
What are the signs of Anxiety in ASD?
Some ways to assess Anxiety in ASD
Incidence Rates of Anxiety in ASD
Treatments for Anxiety in Individuals with ASD
Exploring Anxiety in Ourselves
How do we define Anxiety? Anxiety is a normal reaction to stress. It helps
one deal with a tense situation in the office, study harder for an exam, keep focused on an important speech. In general, it helps one cope. But when anxiety becomes an excessive, irrational dread of everyday situations, it has become a disabling disorder. (NIMH)

Symptoms we call Anxiety
When I’m Anxious, I …worry
am afraid
don’t sleep
don’t eat
eat too much
obsess about things
have racing thoughts
have heart palpitations
have Irritable bowel syndrome
feel dizzy
How do I deal with Anxiety?I distract myself
I keep myself busy
I talk to my friends/gain reassurance
I pray
I take medications to help me
I exercise
I breath, meditate, do yoga
I practice positive self talk
I try to change my beliefs
I avoid what’s making me anxious
I take drugs/alcohol/other addictions
I try to change what is causing me anxiety
From a behavioral perspective…
Everything we do is to Get something good, or avoid something bad!
Feeling Anxious is something bad!
Sometimes we avoid all situations that may bring on anxiety
And if we cant avoid the situation, we do things to help us cope.
Some of the things we do are good, other things are bad!
How do I deal with Anxiety?
Good Coping Strategies
I distract myself
I keep myself busy
I talk to my friends/gain reassurance
I pray
I take medications to help me
I exercise
I breath, meditate, do yoga
I practice positive self talk
I try to change my beliefs
Bad Coping Strategies
I avoid what’s making me anxious
I take drugs/alcohol/other addictions
I try to change what is causing me anxiety
With all these coping strategies, what are we trying to gain?
Avoid or reduce the anxiety
Find other things that are rewarding so they replace the anxiety
Gain better understanding of what’s causing us anxiety
Change our perceptions and beliefs so we have less anxiety

If our children with ASD felt anxious, Would we know it? How would they show us? What ways do they have to cope? What techniques do they know to calm
themselves? Can we help reduce what causes them anxiety
to begin with?
Our goal is to…
Recognize anxiety in our children
Help them recognize what makes them anxious
Help them find good coping strategies
Help them feel confident enough to approach situations they feel anxious about
Help them overcome their anxieties
Help them find ways to reward themselves

What is Anxiety
Panic Disorder
Separation Anxiety Disorder
Specific Phobia
Social Phobia
Obsessive Compulsive Disorder
Post Traumatic Stress Disorder
Generalized Anxiety Disorder
DSM IV definitions of AnxietyPanic Disorder: Recurrent and unexpected panic attacks.
Separation Anxiety Disorder: Developmentally inappropriate and excessive anxiety surrounding separation from home or from significant attachment figures
Specific Phobia: a significant anxiety provoked by exposure to a feared object, often leads to avoidance

DSM IV definitions of AnxietySocial Phobia: a significant anxiety provoked by exposure to social or performance situations, which often leads to avoidance
Obsessive Compulsive Disorder: obsessions that cause marked distress and/or compulsions which are performed to neutralize anxiety

DSM IV definitions of AnxietyPost Traumatic Stress Disorder: the re-experiencing of an extremely traumatic event accompanied by increased arousal and avoidance of stimuli related to the trauma
Generalized Anxiety Disorder: At least 6 months of persistent and excessive anxiety and worry
How many of these do individuals with ASD experience?

What is ASD?
Autism Delays in Communication Delays in Social Skills Stereotyped Repetitive Behaviors
Asperger’s Syndrome No Delays in Communication
Pervasive Developmental Disorder NOS Same as Autism but fewer than 6 symptoms
Why would individuals with ASD have Anxiety?
Symptoms of ASD lead directly to anxiety: Not understanding what’s going on around
them Not being able to attend to important things Fear of failure Feeling like they don’t fit in Not knowing how to handle social situations Not understanding what is expected of them
Underlying reasons in ASD lead to Anxiety: Not getting enough sleep Not feeling well due to underlying GI issues Sensory overload Being on medications that can agitate or cause a
sensation of anxiety Receiving treatments that can increase anxiety Imbalances in neurotransmitters Abnormal activity levels in certain parts of the
brain
Signs of Anxiety in ASDRitualistic Behavior Obsessive Compulsive Behavior
• Lining up objects (control of the environment)• Hoarding (safety)• Body Rocking (parasympathetic activation)
Physiological Responses• No sleep• Irritable bowel or other GI issues• Hives
Avoidant Behaviors• Self isolation• No eye contact• Social avoidance• Self stimulatory behaviors
Anxiety and avoidance in infants and toddlers with autism spectrum disorders: Evidence
for differing symptom severity and presentation
Thompson E Davis III, Jill C. Fodstad,
Whitney S. Jenkins, Julie A. Hess, Brittany N.
Moree, Tim Dempsey, Johnny L. Matson
Research in Autism Spectrum Disorders 4 (2010) 305-313
Results: Toddlers with AD had more severe anxious and avoidant symptoms than those with PDD NOS or with controls (other developmental disorders)

20
Avoidance Behavior
Item Description Autism (n=159),M (SD)
PDD-NOS (n= 154), M (SD)
Control (n =200), M (SD)
Fear of being around others in school, at home, or in social situations
0.27 0.16 0.07
Avoids specific situations, people, or events
0.36 0.12 0.02
Unreasonable fear of approaching or touching specific objects, people, or items
0.39 0.23 0.09
Withdraws or removes him/her self from social situations
0.75 0.28 0.07

21
Avoidance Behavior
Item Description Autism (n=159),M (SD)
PDD-NOS (n= 154), M (SD)
Control(n =200), M (SD)
Avoids specific objects, persons, or situations causing interference with his/her normal routine
0.23 0.06 0.02
Persistent fear that is not age appropriate
0.13 .012 0.02
Exposure to specific objects/situations provokes immediate distress that is not age appropriate
0.26 0.12 0.02
Presentation of a specific object or situation results in loss of control, panic, or fainting
0.11 0.06 0.01
Trembles or shakes in the presence of specific objects or situations
0.94 0.08 0.06
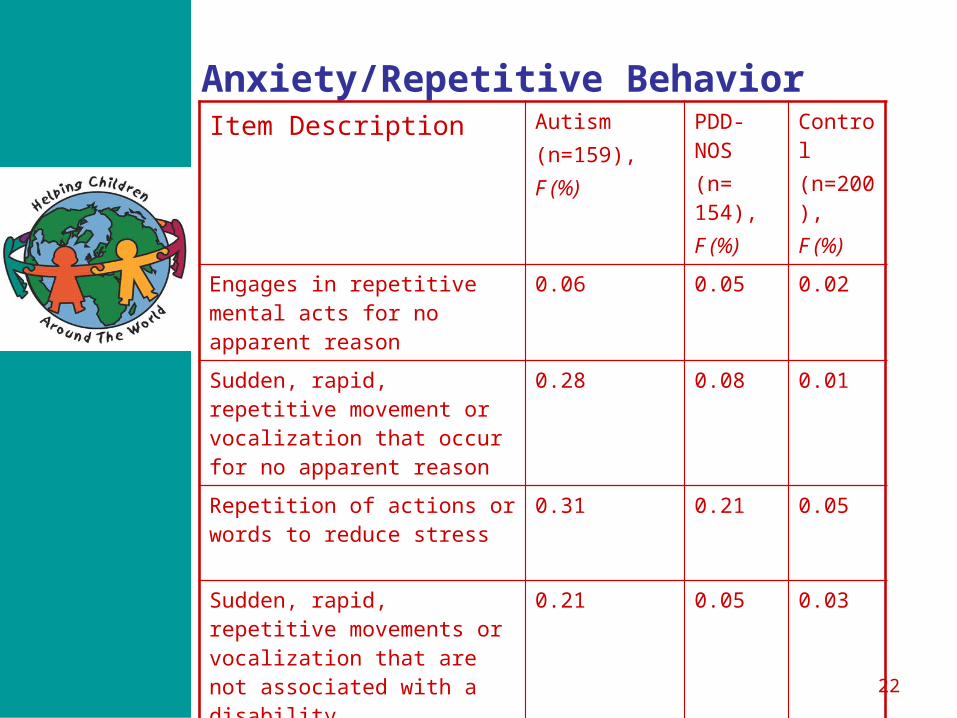
22
Anxiety/Repetitive BehaviorItem Description Autism
(n=159),F (%)
PDD-NOS(n= 154), F (%)
Control (n=200), F (%)
Engages in repetitive mental acts for no apparent reason
0.06 0.05 0.02
Sudden, rapid, repetitive movement or vocalization that occur for no apparent reason
0.28 0.08 0.01
Repetition of actions or words to reduce stress
0.31 0.21 0.05
Sudden, rapid, repetitive movements or vocalization that are not associated with a disability
0.21 0.05 0.03
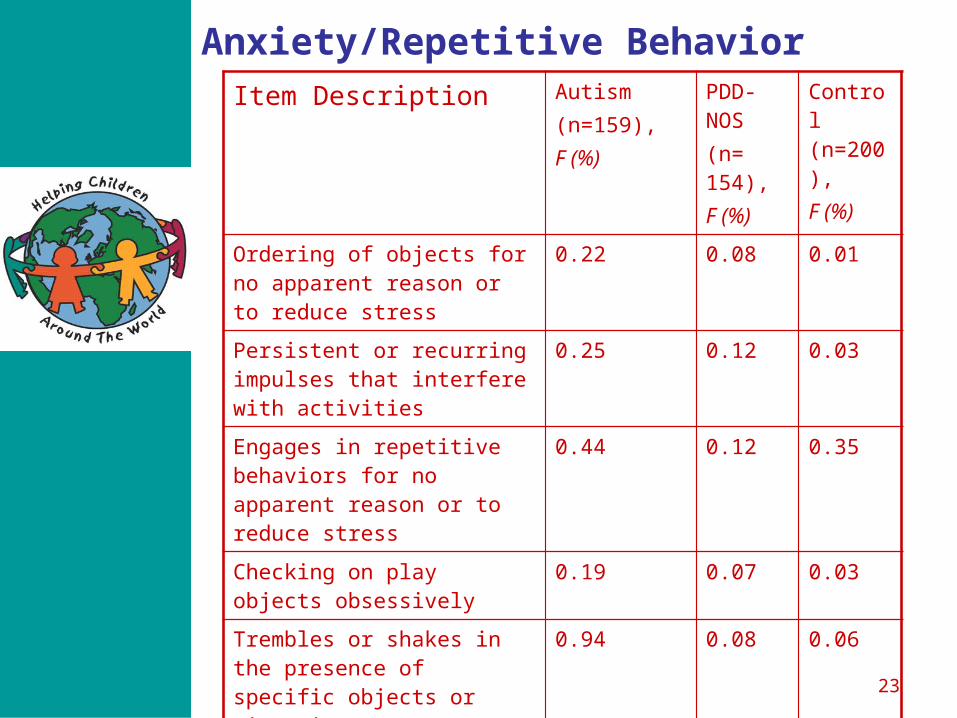
23
Anxiety/Repetitive BehaviorItem Description Autism
(n=159),F (%)
PDD-NOS (n= 154), F (%)
Control (n=200), F (%)
Ordering of objects for no apparent reason or to reduce stress
0.22 0.08 0.01
Persistent or recurring impulses that interfere with activities
0.25 0.12 0.03
Engages in repetitive behaviors for no apparent reason or to reduce stress
0.44 0.12 0.35
Checking on play objects obsessively
0.19 0.07 0.03
Trembles or shakes in the presence of specific objects or situations
0.94 0.08 0.06
Has difficulty organizing tasks, activities, and belongings
0.23 0.10 0.02
Summary of research findingsStudies show that individuals with ASD experience greater levels of anxiety than community populations, regardless of their age!
Individuals with ASD show greater levels of anxiety than individuals within other clinical groups (DD, ADHD, MR)
Individuals with ASD show similar levels of anxiety when compared to individuals with a diagnosis of clinical Anxiety!!
Co-morbidity incidence rates of Anxiety and ASD
Prevalence of Anxiety in ASD ranges from 11% to 84%!!
Most studies estimate prevalence of about 40-50%
Children with more severe ASD have more anxiety than those less affected.
Why is it hard to dx Anxiety in Individuals with ASD?
Diagnostic Overshadowing We attribute the anxiety to the autism We ignore the co-morbid issues because the
main diagnosis of autism is more debilitating
Anxiety is often misunderstood as a behavior problem
The symptoms get mixed up…is he having avoiding the situation because of his autism, or is it anxiety?
Recommended ways to assess for Anxiety
Clinical Interview (may only be possible with higher functioning individuals) Young children with ASD cant identify
emotions well so we need to give them concrete examples, and teach them about emotions
Give forced choice, rather than open ended questions
Use many visual aids such as pictures of emotions, emotional thermometer (Atwood)
Recommended ways to assess for Anxiety
Anxiety Rating Scales Stress Survey Schedule for Persons with
Autism and Developmental Disabilities (Gorden et. al 2001)
The Autism Co-Morbidity Interview: a semi structured parent interview
(Leyfer et al 2006)

Recommended ways to assess for Anxiety
Direct Observations of Anxiety
A Functional Behavior Assessment (FBA) looks at what happened before and after a behavior that may be a sign of anxiety
Time for School….Joe Tantrums….Gets sent homeA challenging behavior (tantrum) may begin due to
anxiety, but then become learned due to reinforcement!!!
Noisy Environment....Tom lines up toys….Tom Avoids
Is it ok to let Tom avoid the social setting, or is it better to help him cope with the noisy environment?

Three part contingency
In behavioral theory, every behavior can be changed if we change the antecedents (what happened before the behavior) and the consequences (what happened right after the behavior!
If we change the antecedents and consequences, can we reduce the anxiety?
Can we reduce the anxiety without rewarding challenging behaviors?
Treatments for AnxietyPsychopharmacology SSRI’s SNRI’s Azaspirones Benzodiazepines Tricyclics Monoamine Oxidase Inhibitors
All these medications influence our neurotransmitters and control our ability to feel anxious
Treatments for Anxiety
Medications that may improve underlying causes of Anxiety GI meds to calm gastrointestinal distress Sleep medications to help alleviate sleep
deprivation

Treatments for Anxiety
Cognitive Behavior Therapy Aims to create new coping templates by using
behavioral techniques such as • Modeling• Exposure• Relaxation Training
And teaches cognitive techniques to reduce cognitive distortions and deficiencies
4 Components of CBT
Assessment
Psychoeducation
Restructuring
Exposure
CBT: Assessment Need to determine what is causing the anxiety (real or imagined, concrete or abstract)
Need to determine when it is occurring (what are the environmental triggers or antecedents?)
Need to determine how it is being maintained (consequences)
Need to establish a hierarchy from most anxiety provoking to least.
CBT: PsychoeducationTeaching New Skills
Skills that help us cope with Anxiety Relaxation exercises/ deep breathing Guided Meditation Contingency Management
Skills that help us understand better so we do not experience Anxiety Social skills training Cognitive reasoning Planning Perspective Taking
CBT: Cognitive Restructuring
Identifying our negative thoughts
Identifying anxious self talk
Identifying perceived threats
Identifying negative self evaluation
Understanding that our thoughts influence our feelings!

CBT: Exposure
Eliciting the anxiety provoking thought (or situation) while practicing extinction of avoidance behavior and habituation to excessive or maladaptive physiological responses!!
Which means: Facing the Fear!

ExposureSystematic Desensitization 3 components
• Exposure to a hierarchy of anxiety provoking images or experiences
• Relaxation, imagery and breathing • Pairing
Begin with lowest item on hierarchy Begin with imagination not in vivo Pair with relaxation until mastered Go up the hierarchy gradually until all mastered Then do in vivo
Copy Cat Workbook (Kendall 1992)
5 sessions assessment and psychoeducation Building rapport Orienting to treatment Explaining, in child language, the nature of the problem Identifying anxious feelings and responses Teaching child relaxation techniques
5 sessions on cognitive restructuring Identifying anxious self talk Identifying challenging thoughts Teaching Self evaluation Teaching Self reward
5 sessions of graduated exposure
1 session on generalization

Applying CBT to Autism With more affected individuals, the preferred order is Exposure Relaxation Cognitive Restructuring Modeling
Along with Social skills training Goal setting Parent Psychoeducation
CBT Modifications for ASD
Pay attention to the deficits caused by the ASD If the individual doesn’t have social skills,
teach them If the individual would be less anxious with
better adaptive skills, teach them If the individual would be less anxious with
better regulation of sensory input, work on this
CBT Modifications for ASDUse many Visual stimuli Toolbox (can hold strategies) Written Schedules (reduce anxiety of not knowing what
is coming next) Narratives (I am the boss, anxiety is not the boss) Stories Role Play Choice Lists Drawings (thought bubbles, cartoons) Visual Worksheets with response lists Rules lists of emotion to coping Rules lists of what’s normal and what’s excessive
CBT Modifications for ASDUse concepts that the individual likes or is interested in Astronauts exploring a new planet Harrison Ford obsession: what would he do/Star wars cartoons
Use Self Stimulatory behavior as a way to reward/self calm: The Premack Principle Allow non preferred activities to reward preferred activities
Develop socially acceptable compulsions Organizing

Finally…
Parent Anxiety perpetuates Child Anxiety!
Heal yourselves
Stress is when we don’t agree with reality! Our minds find a way to obsess over how
reality is different from what we wanted Our minds find a way to obsess about how
present reality can lead to a worse reality in the future!
We all have something we are afraid of!!

What is Fear?
Fear only comes when we allow our past experiences to color our perceptions of the present, and produce apprehension about the future!
Question the beliefs you have. You will find that the universe has a plan for you. One that is far greater than what you had imagined.