M eM V para o e de H de C a i a : r de e 1 M T S uTiSM: S ...
Upload
harriet-curtisCategory
view
216download
0
Autism Spectrum Disorders:
Research findings and treatment implications
Center for Autism and Related Disorders, Inc
Doreen Granpeesheh, Ph.D. B.C.B.A-D
Today’s Presentations
DSM 5 diagnosis of ASD
A multi-disciplinary treatment model
What is ABA (Applied Behavior Analysis)
Applications of behavior analysis to the treatment of ASD

Autism Spectrum Disorder
Doreen Granpeesheh, PhD, BCBA-D

DSM IVAutistic Disorder: Total of 6 or more symptoms < age 3 Social Deficits (2)
• Eye Contact• Showing/Sharing• Emotional Reciprocity
Communication Deficits• Language• Pretend Play• Conversation
Stereotypic/Repetitive Behaviors• Routines• Preoccupation• Intense focus• Motor
4

DSM IV
Asperger’s Social Deficits: 2 Stereotypic/Repetitive: 1 No Communication Deficit
PDDNOS Same as Autistic Disorder but less than 6
symptoms
5
Autism Spectrum Disorder: DSM-5
Criterion A: Persistent deficits in social communication and social interaction across contexts, not accounted for by general developmental delays, and manifested by all 3 of the following:
1. Deficits in social-emotional reciprocity; ranging from abnormal social approach and failure of normal back and forth conversation through reduced sharing of interests, emotions, and affect and response to total lack of initiation of social interaction,
2. Deficits in non-verbal communicative behaviors used for social interaction; ranging from poorly integrated verbal and nonverbal communication, through abnormalities in eye contact and body-language, or deficits in understanding and use of nonverbal communication, to total lack of facial expression or gestures
3. Deficits in developing and maintaining relationships, appropriate to developmental level (beyond those with caregivers); ranging from difficulties adjusting behavior to suit different social contexts through difficulties in sharing imaginative play and in making friends to an apparent absence of interest in people
Autism Spectrum Disorder: DSM-5
Criterion B: Restricted, repetitive patterns of behavior, interests, or activities as manifested by at least two of the following:
1. Stereotyped or repetitive speech, motor movements, or use of objects; (such as simple motor stereotypies, echolalia, repetitive use of objects, or idiosyncratic phrases)
2. Excessive adherence to routines, ritualized patterns of verbal or nonverbal behavior, or excessive resistance to change; (such as motoric rituals, insistence on same route or food, repetitive questioning or extreme distress at small changes).
3. Highly restricted, fixated interests that are abnormal in intensity or focus; (such as strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
4. Hyper- or hypo-reactivity to sensory input or unusual interest in sensory aspects of environment; (such as apparent indifference to pain/heat/cold, adverse response to specific sounds or textures, excessive smelling or touching of objects, fascination with lights or spinning objects) (APA, 2011)
7

Autism Spectrum Disorder: DSM-5
Criterion C: Symptoms must be present in early childhood (but may not become fully manifest until social demands exceed limited capacities)
Criterion D: Symptoms together limit and impair everyday functioning
8

Key Differences Between DSM-IV-TR
and DSM-5
3 key domains become 2
Shift from categorical to dimensional
Requires 2 repetitive/restrictive behaviors
Language delay is not necessary
Specifiers and modifiers
Level of severity
9

ASD DSM-5 Diagnosis: Specifiers and Modifiers
With the new criteria, the child will receive a diagnosis with the etiology as a specifier ASD with Rett Syndrome ASD with Fragile X
OR with a modifier indicating another important factor ASD with tonic-clonic seizures ASD with intellectual disabilities
10
ASD DSM-5 Diagnosis: Specifiers and Modifiers
Early history is also specified Age of perceived onset Pattern of onset
• Loss of skills (when?)
ASD with onset before 20 months and loss of words
ASD with onset before 32 months and loss of social skills
ASD with no clear onset and no loss ASD – Aspergers type
11

Level of SeveritySeverity Level for ASD Social Communication Restricted interests &
repetitive behaviors
Level 1: Requiring Support
Without support, some significant deficits in social communication
Significant interference in at least one context
Level 2: Requires substantial support
Marked deficits with limited initiations and reduced or atypical responses
Obvious to the casual observer and occur across contexts
Level 3: Requires very substantial support
Minimal social communication
Marked interference in daily life
12
Social Communication Disorder
Impaired pragmatic use of language
Difficulty in the social use of verbal or nonverbal communication Must affect development of relationships, comprehension,
academic achievement, or occupational performance
Cannot be explained by low cognitive ability, word structure, or grammar
Symptoms must be present in early childhood But may not fully manifest until social demands exceed capacities
ASD must be ruled out
13

Clinical Implications
ADHD can now be diagnosed along with ASD
Need to rework assessment measures Screeners and gold standard measures of
assessments are based on DSM-IV criteria
Services and third party billing
14

What does ASD look like?Communication: delayed in language no eye contact
Social Behavior: No interaction with anyone Do not play with others Do not ask for help
Stereotypy: Numerous repetitive behaviors (lining up objects,
opening closing door, turning on and off the lights) Many inflexibilities and repetitive routines
Anything else? Challenging Behaviors!Sensory Sensitivities!Medical Illnesses!

Teach New LearningPatterns
Genetic Predisposition
Physical ConditionsOxidative Stress Decreased Methylation
Immune Dysfunction GI Inflammation
Brain DisordersHypoperfusion
Hypo and Hyper sensitivity to stimuliDifferent Learning Patterns
Behavioral SymptomsDelayed Language
Delayed Social SkillsStereotypy
AUTISMMetals
Pesticides BisphenolAAntibiotics
Minimize ExposureTo Toxins
Treat the Underlying
Medical Disorders
Identify Sensory Issues
Reduce/Eliminate Symptoms
Minimize Exposure to Toxins
Make sure your physician only uses antibiotics when necessary
Avoid pesticides (go organic)
Avoid BPA (plastics)
Spread out vaccinations to reduce stress on immune system
Check for metal toxicity to determine need for chelation (toxic metal assay)

Treat Underlying Medical Illness
Immune Markers Immunoglobulin Subsets (Antibodies that respond to bacteria,
viruses, fungus, etc) Check for Strep Titers (PANDAS) Vaccine Titers
Detoxification markers Redox capacity (Redox SYS™ Diagnostic System). Oxidative Stress Decreased Methylation/transulfation (fasting plasma
cysteine or methionine markers
Discuss Possible Treatments with your physician

Treat Underlying Medical Illness
Evaluate and Treat GI Disorders Nutrition Diet Medication
• Anti-inflammatories• Steroids• Anti-fungals• Anti Chlostridia
Help the child become healthy
Make sure he is sleeping well
Make sure he is getting the right nutrition
Identify Sensory Issues
Everything we learn enters through our sensesHow does your child receive information? Does he perceive visual information correctly?
• Focus versus double vision• Binocularity• Central Vision• Tracking
Does he perceive auditory information correctly?• Figure ground discrimination• Binaural integration and separation• Appropriate hemispheric lateralization
Does he perceive tactile or proprioceptive information correctly?
If we don’t receive information correctly, we cannot learn correctly!
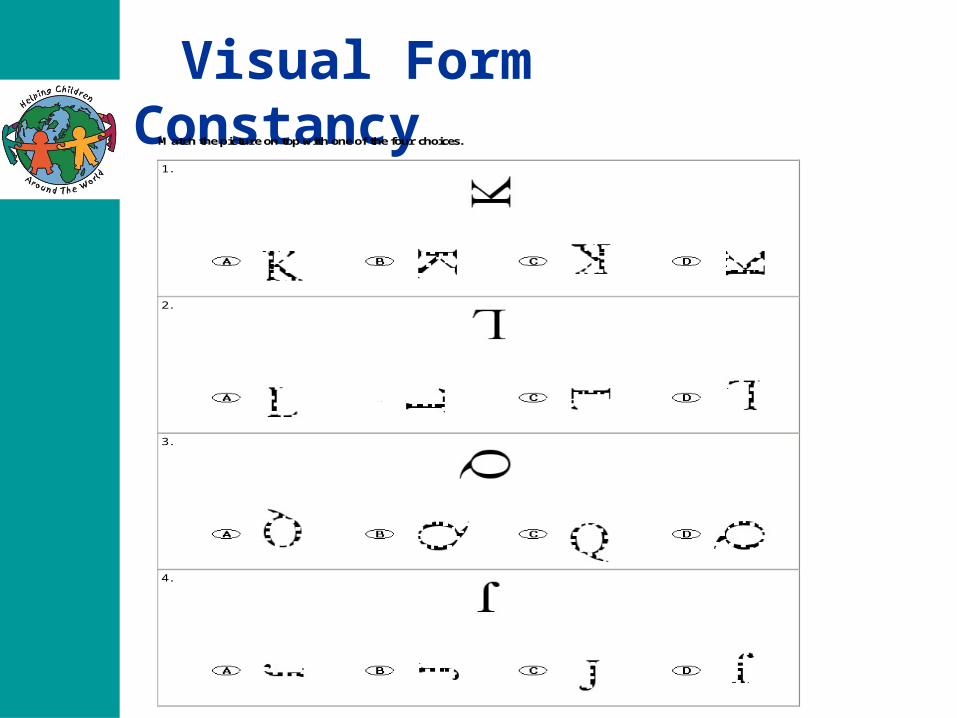
Visual Form ConstancyMatch the picture on top with one of the four choices.
1.
2.
3.
4.

Visual Form Constancy
What is added to the first picture to make the second picture?
1.
First Picture
to
Second Picture
2.
First Picture
to
Second Picture
3.
First Picture
to
Second Picture

Visual Figure-Ground Discrimination
1.
How many times is the number 8 in the above picture?
10 times 7 times 8 times 5 times 2.
How many times is the number 6 in the above picture?
10 times 4 times 5 times 1 time 3.
How many times is the number 9 in the above picture?
9 times 3 times 15 times 2 times
Treating sensory issuesDevelopmental Optometry Tracking Figure ground discrimination Bilateral use exercises
Audiology Pairing with visual input Noise reduction headphones Practice the hemispheric deficit areas
Tactile/Proprioceptive Sensory Integration/OT Sensory Diet to regulate
Sensory Regulation Activities Teaching self soothing activities Using environmental stimuli to prevent sensory overload

Experiencing the world through Autism
Little or no sleep
Stomach pain, bloating, discomfort
Diarrhea and/or constipation
Lights are too strong or piercing
Sounds are too intense
Background noise is loud
Objects are not in focus
Everything is unpredictable
Autism leads to Anxiety

Do individuals with autism experience anxiety?
Signs of Anxiety in Autism Self stimulatory behavior
• Ordering, lining up• Hoarding• Checking• Avoiding
Social Activities Eye Contact Demands
Self injury?

Treat the Anxiety
Reduce demands until skills are mastered
Reward frequently
Teach coping strategies
Allow functional levels of compulsivity
Improve Sleep
Improve Chemistry SSRI SNRI

Teach New Learning Patterns
ABA: Applied Behavior Analysis “30 years of research demonstrated the
efficacy of Applied Behavioral methods in reducing inappropriate behavior and in increasing communication, learning and appropriate social behavior”
Surgeon General, 1999
Outcome Research on ABA for Autism
Lovaas (1987)
Sallows (2005)
Howard (2005)
Cohen (2006)
Eikeseth (2007)
Remington (2007)
Perry (2008)
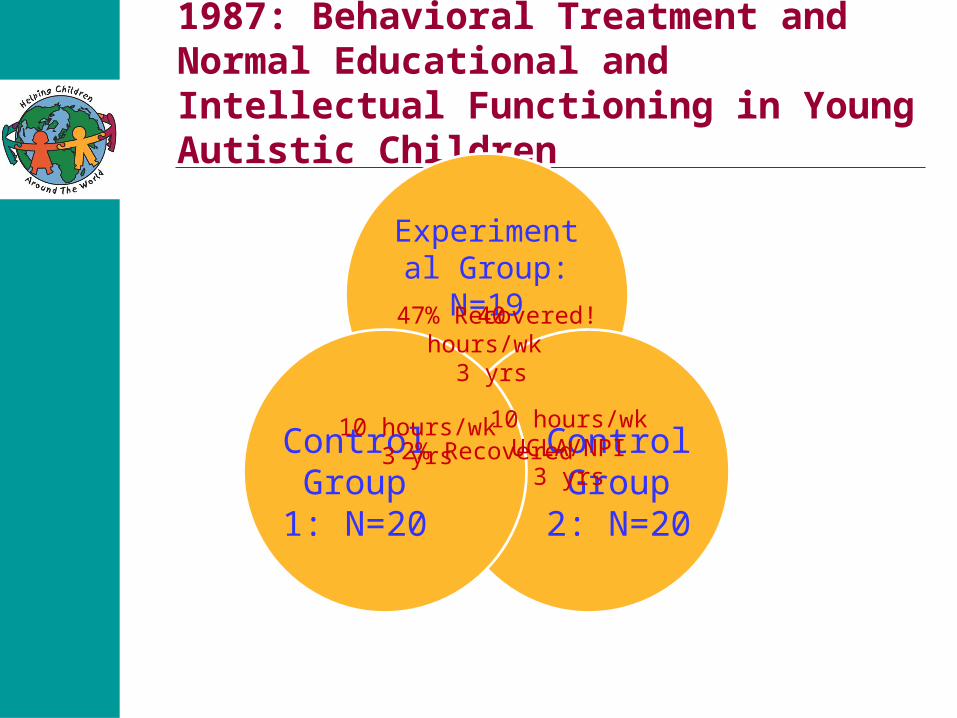
1987: Behavioral Treatment and Normal Educational and Intellectual Functioning in Young Autistic Children
Experimental Group:
N=19
Control Group 2:
N=20
Control Group 1:
N=20
40 hours/wk 3 yrs
10 hours/wk3 yrs
10 hours/wkUCLA/NPI
3 yrs
47% Recovered!
2% Recovered

40 hrs/week ABA for 2 or more years
47% achieved average IQ and required no special education after treatment
McEachin (1993): gains maintained for 8/9 when the children were 12 years old

4 years of ABAResults:
Average IQ: 48% Success in unsupported regular education:
34% Non-impaired communication: 42% Non-impaired socialization: 42% Failure to qualify for autism according to the
ADI-R: 34%
3 years of ABAResults:
Average IQ: 57% Success in unsupported regular
education : 28% Non-impaired on the Vineland adaptive
behavior composite: 38%

Replication in Norway2 years of ABAResults:
Average IQ: 7/13 = 54% Average score on Aechenbach
CBC: 4/13 = 31%

Replication in England25 hrs/week of ABA for 2 years
Gains in language, intelligence, daily living, positive social behavior
No increase in parent stress
Replication in the Middle EastResults:
Scoring in non-ASD range on ADOS after treatment: 4/19 = 21%
Whole province of Ontario, CanadaFree ABA for all young children with autism332 children71% made significant gains11% achieved functioning in the average rangePoor quality control, lots of different providers, still had large good effects
Outcome Research on ABA for Autism
Conclusions of outcome research Every published study demonstrated very
large treatment effects Replicated across research groups, across
university vs. community settings, and across continents
Intensity matters: at least 25 hours per week of one-to-one intervention for more than a year produces best outcomes
Duration matters: two or more years of intervention
Outcome-Level Analysis of ABA Treatment for Autism
Effects of age and treatment intensity on outcomeN = 245More treatment = more gainsPublished in Research in Autism Spectrum Disorders (2009)
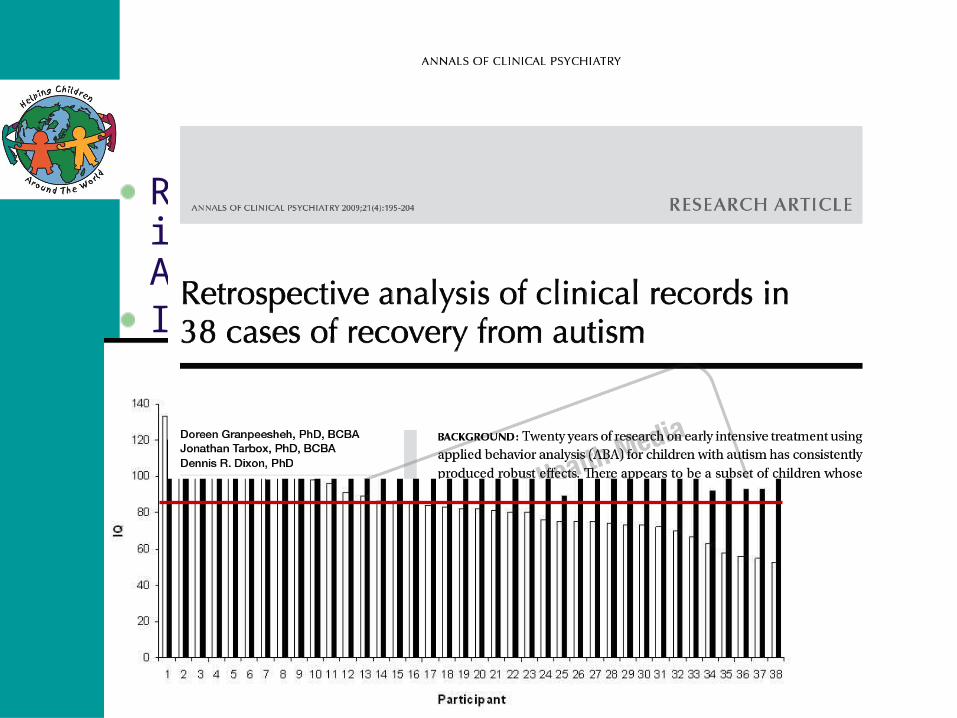
Recovery from Autism
Retrospective analysis of charts in 38 cases of recovery following ABA treatmentIn-press in Annals of Clinical Psychiatry
Acceptability of ABA
The following bodies now recommend ABA as a treatment for autism American Academy of Pediatrics The New York State Department of Health The National Academy of Sciences Surgeon General
• “30 years of research demonstrated the efficacy of Applied Behavioral methods in reducing inappropriate behavior and in increasing communication, learning and appropriate social behavior”
Surgeon General, 1999

Integrative TreatmentSensory
InterventionsDevelop and
Regulatesensory input ability
Behavioral Interventions
Teach new learning patters
Generalize to daily living
Medical InterventionsEliminate Triggers
Stabilize underlying cause
Achieve health
A healthy child feels better, sleeps better
and can learn better!!
Why would a behaviorist care about biomedical interventions?
1990: Andrew was diagnosed with Celiac…we placed him on a diet and he recovered within a year!
1992: I began to notice a pattern of children with extremely high use of antibiotics! This must be leading to some abnormal flora!
1993: Emily had fungus on her nails…treated with antifungals, her behavior changed drastically!

Preliminary Outcome Study:1996
63 boys 16 girls
79 children
Average age at intake: 39.1 months
Average IQ at intake: 76.8 (borderline)
Length of time in treatment: 3 years

Preliminary Outcome Study:1996
High Intensity
More than 25 hours/week
44 children
Low Intensity
Less than 25 hours/week
35 children
Matched on age, IQ, language, adaptive behavior
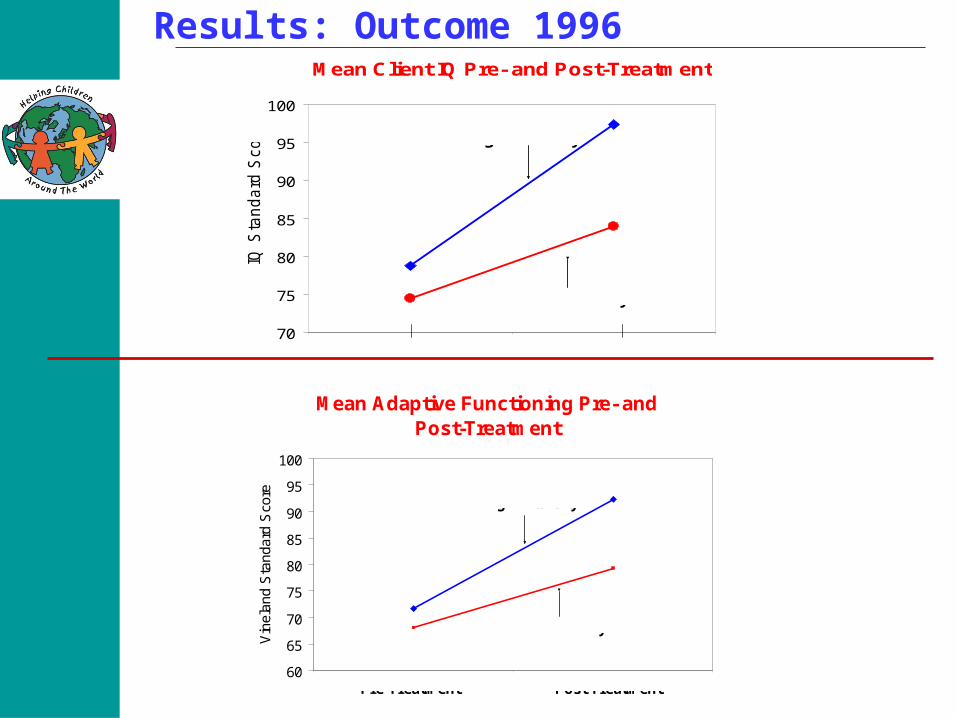
Results: Outcome 1996Mean Client IQ Pre- and Post-Treatment
70
75
80
85
90
95
100
1 2
IQ S
tan
da
rd S
co
re High Intensity
Low Intensity
Pre-Treatment Post Treatment
Mean Adaptive Functioning Pre- and Post-Treatment
60
65
70
75
80
85
90
95
100
1 2
Vin
elan
d S
tand
ard
Sco
re
High Intensity
Low Intensity
Pre-Treatment Post Treatment
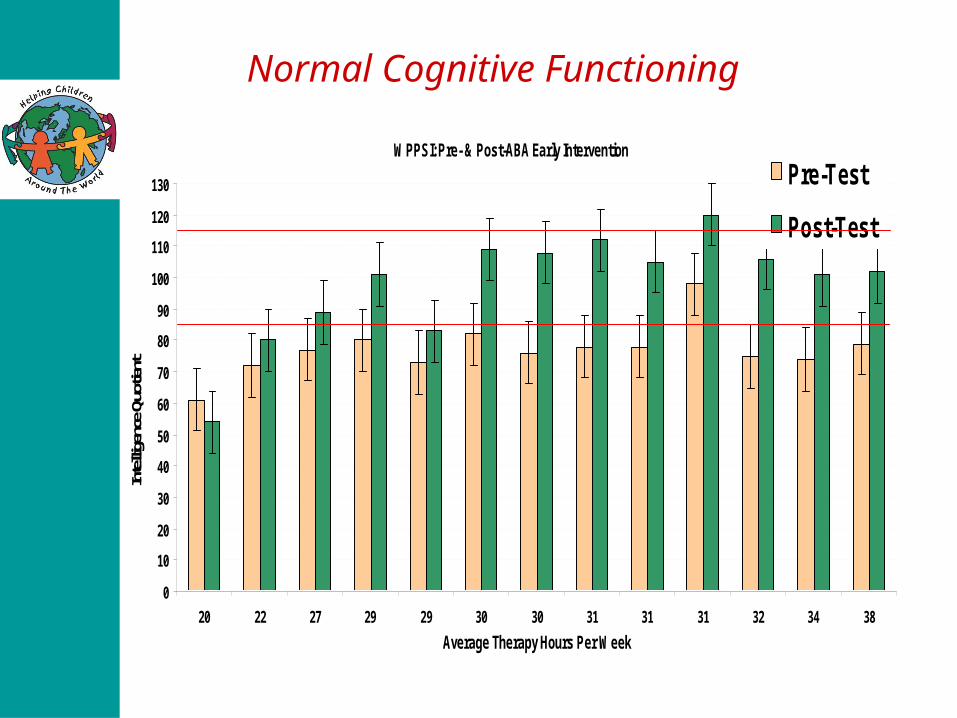
WPPSI: Pre- & Post-ABA Early Intervention
0
10
20
30
40
50
60
70
80
90
100
110
120
130
20 22 27 29 29 30 30 31 31 31 32 34 38
Average Therapy Hours Per Week
Intel
ligen
ce Q
uotie
nt
Pre-Test
Post-Test
Normal Cognitive Functioning

Why didn’t we publish this?
1996 Outcome Study Confounding Variable: • A higher percentage of children in the
high intensity group were receiving biomedical interventions!
• Was the improvement in IQ and adaptive skills due to ABA or due to the medical interventions or a combination???
Let’s look at some case studies of children who improved significantly with a combination of medical and behavioral treatment

D.R. Diagnosis: AutismIntake: Age: 2.11 Deficits: receptive vocabulary of 10 words, 3 expressive words used for
needs (juice, open, ball), no eye contact, severe tantrums, crying, aggression and elopement, ssb included gazing, mouthing objects and toe walking.
Treatment: 1 year 10 months with CARD to date Average intensity of 30 hours/week Specific Carbohydrate Diet
Current: Age: 4.9 In typical preschool with aide 175 mastered receptive labels, mands and tacts with all items using full
sentences, maintains eye contact up to 8 seconds, responds to name by making eye contact and saying “yes” or ‘what”, answers 23 social identification questions, interacts with adults average of 10 minutes/peers 2 minutes. Ssb reduced but still exist, aggression and noncompliance have extinguished.

DR
0
50
100
150
200
250
Nov-03 Dec-03 Jan-04 Feb-04 Mar-04 Apr-04 May-04 Jun-04
Months
Ne
w S
kil
ls p
er
Mo
nth
ABA + IgG Allergy
Elimination Diet +
Feingold Diet +
Rotation diet
ABA + Specific Carbohydrate Diet
D.R.: New Skills per month

DR
0
100
200
300
400
500
600
700
800
Nov Dec Jan Feb Mar April May June
Months
Fre
qu
en
cy
of
Ste
reo
typ
y p
er
Mo
nth
Visual SSB Verbal SSB Oral Motor SSB Tactile SSB
ABA + IgG Allergy
Elimination Diet +
Feingold Diet +
Rotation diet
ABA + Specific Carbohydrate Diet
D.R.: Stereotypy per month

DR
0
10
20
30
40
50
60
70
80
90
100
Nov Dec Jan Feb Mar April May June
Months
ABA + IgG Allergy
Elimination Diet +
Feingold Diet +
Rotation diet
ABA + Specific Carbohydrate Diet F
req
ue
nc
y o
f A
gg
res
sio
n p
er
Mo
nth
D.R.: Aggression per month
EmmaDiagnosis: Asperger’s SyndromeIntake: Age: 3.4 Deficits: poor eye contact, extensive vocabulary but did not use
language with peers, self-isolated at school, severe tantrums, non compliance and aggression with family, visual self-stimulatory behaviors, severe ritualistic behavior, no Theory of Mind
Treatment: 10 months with CARD Average intensity of 10 hours/week Lexapro Pro DHA and CorOmega
Exit: Age: 4.2 In typical kindergarten with no aide Initiated conversations with peers, many friends, no tantrums or
aggression, very advanced in academic skills and very popular in school

Emma
0
1
2
3
4
5
6
7
April May June July Aug Sept Oct Nov Dec
Months
Fre
qu
en
cy
pe
r S
es
sio
n
Tantrums Non-Compliance Ritual SSB
ABA + Lexapro
ABA + ProDHA + Coromega
ABA
Emma: Challenging Behaviors per month
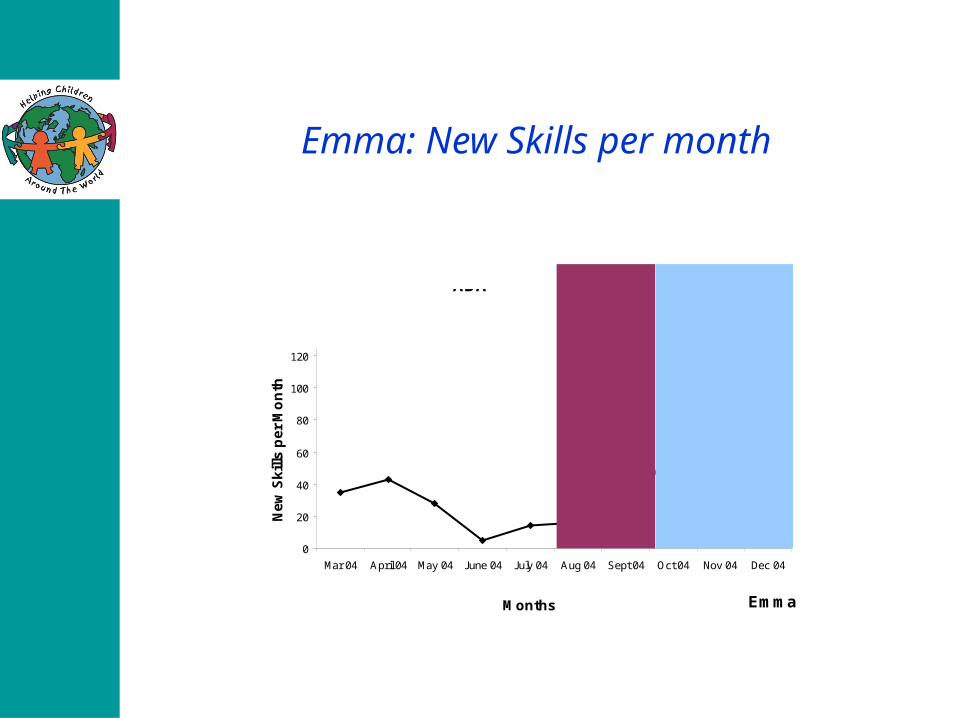
Emma
0
20
40
60
80
100
120
Mar 04 April 04 May 04 June 04 July 04 Aug 04 Sept 04 Oct 04 Nov 04 Dec 04
Months
Ne
w S
kil
ls p
er
Mo
nth
ABA + Lexapro
ABA + ProDHA + Coromega
ABA
Emma: New Skills per month
A. D. Diagnosis: AutismIntake: Age: 2.11 Deficits: had 3-4 word utterances but no spontaneous language, self-
isolated around peers, no safety awareness, toe walking, licking hands, had difficulty inhibiting responses and would often touch people’s hair or clothing.
Treatment: 3 year with CARD Average intensity of 25 hours/week Anti-fungals Chelation
Exit: Age: 5.11 In typical kindergarten without aide Initiates, joins, transitions conversations with peers, has many friends,
good understanding of others perspectives, no challenging or self-stimulatory behaviors present. Normal range on all exit testing (IQ, language, TOM, EF)

AD
0
2
4
6
8
10
12
14
May
June
July
Aug
Sep
t
Oct
Nov
Dec Jan
Feb
Mar
ch
Apr
il
May
June
Month
Fre
qu
en
cy
pe
r H
ou
r
Elopement Fidgeting LeaningRunning Grabbing Screaming
ABAABA +
Antifungal + Chelation
A.D.: Challenging Behaviors per month

AD
0
50
100
150
200
250
June
July
Aug
Sep
t
Oct
Nov
Dec Jan
Feb
Mar
ch
Apr
il
May
June
Month
Ne
w S
kill
s p
er
Mo
nth
ABAABA +
Antifungal + Chelation
A.D.: New Skills per month

What do we learn from these Case Studies?
A variety of medical interventions worked for these childrenEach child benefited from a different type of interventionAutism is a “Spectrum Disorder”…children with Autism are very different from each other! Not every intervention will work for every child….except for ABA!

What is Applied Behavior Analysis
ABA is based on the principles of
Operant Conditioning Theory:
“Human Behavior is affected by events that precede it (antecedents) and events that follow it (consequences)”
Change these events…change Behavior!
What does that mean?
In ABA we change behavior by changing antecedents and consequencesWhat is a behavior? Behavior is anything we do
What is an antecedent? An Antecedent is whatever happened just
before the behavior
What is a consequence? A Consequence is whatever happens just after
the behavior
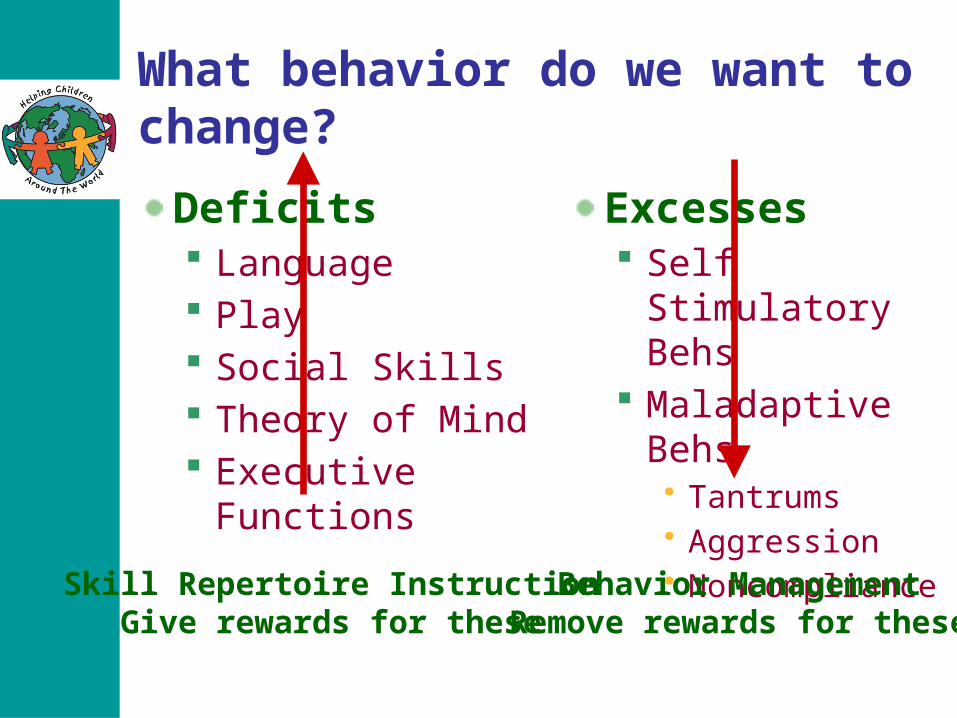
What behavior do we want to change?
Deficits Language Play Social Skills Theory of Mind Executive Functions
Excesses Self Stimulatory
Behs Maladaptive Behs
• Tantrums• Aggression• Noncompliance
Skill Repertoire InstructionGive rewards for these
Behavior ManagementRemove rewards for these

Why does a child have challenging behaviors?
Everything we do is to Get a Reward Avoid a Punishment
Challenging Behavior is the child’s way of telling us what he wantsHe may not realize that his way of telling us is not the “appropriate way”He may not have the skills to tell us the appropriate way!

What is this child trying to get?

Positive things children want:
Attention
good or bad
Tangibles
our favorite foods
fun activities
toys
playground
Negative things children avoid
Having to work Classroom Listening to people telling us what to do Giving up something we want to keep
doing Sensory Overload Getting ready in the morning

How do we change Behavior
Give Remove
positive
Behavior Behavior
negative
Behavior Behavior
+ Reinforcement
- Reinforcement
Response CostExtinction
Punishment
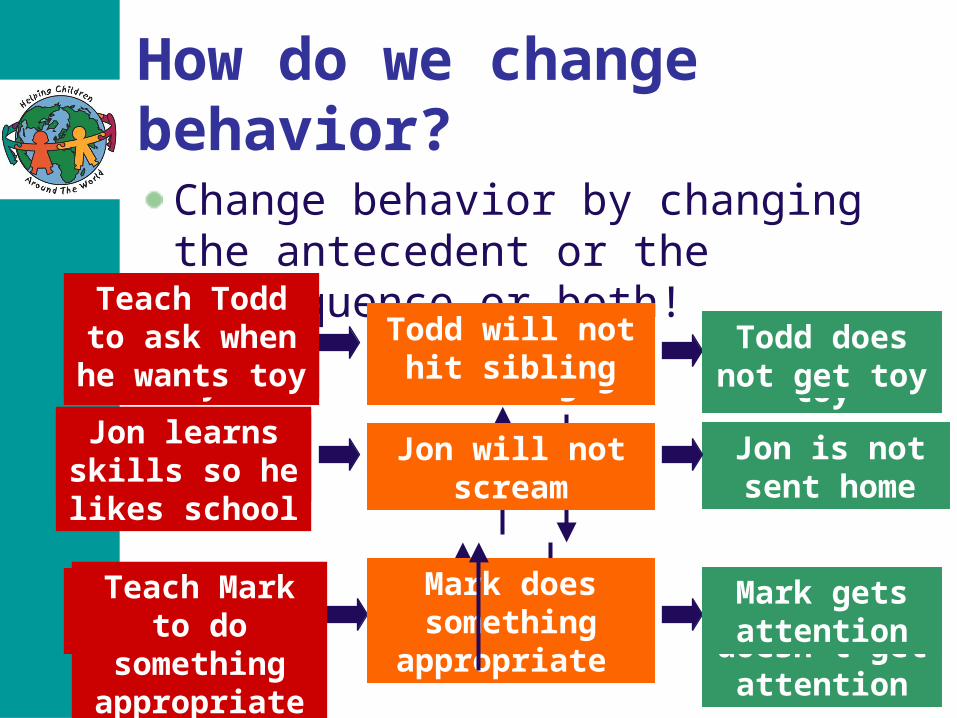
How do we change behavior?
Change behavior by changing the antecedent or the consequence or both!
Todd wants toy Todd hits sibling Todd gets toyTodd does not get toy
Teach Todd to ask when he
wants toyTodd will not hit
sibling
Todd will not hit sibling
Mark wants attention
Mark cries and tantrums
Mark gets attention
Mark doesn’t get attention
Teach Mark to do something appropriate
Mark does something
appropriate
Mark gets attention
Jon hates school
Jon screams Jon is sent home
Jon is not sent home
Jon learns skills so helikes school
Jon will not scream

Step 1: Identifying what the child wants to communicateStep 2: Teaching the child more appropriate ways to communicate
If we teach appropriate communication skills, they will replace challenging behaviors in our kids
Challenging behaviors are NOT part of the Autism diagnosis! They are just a form of communication!
Summary
Identify the behavior you want to changeIdentify why it is happening What is your child trying to communicate? What does he want to have or avoid?
Now that you know the function, you can change the behaviorHow?By changing either the antecedent or the consequence…or both! The FUNCTION of the behavior tells you what to do!

Extinction for Tangible Function
Example of DRA

The Secret to successful ABA
The key is to teach appropriate skills!
If a child has appropriate skills, and they are easy to do, he will not engage in challenging behaviors!
We cannot simply “extinguish” challenging behaviors without replacing them first, with appropriate skills!

We learned how to use ABA to change behavior
Now lets look at how we can use ABA to teach skills
Same principles

What behavior do we want to change?
Deficits Language Play Social Skills Theory of Mind Executive Functions
Excesses Self Stimulatory
Behs Maladaptive Behs
• Tantrums• Aggression• Noncompliance
Skill Repertoire InstructionGive rewards for these
Behavior ManagementRemove rewards for these
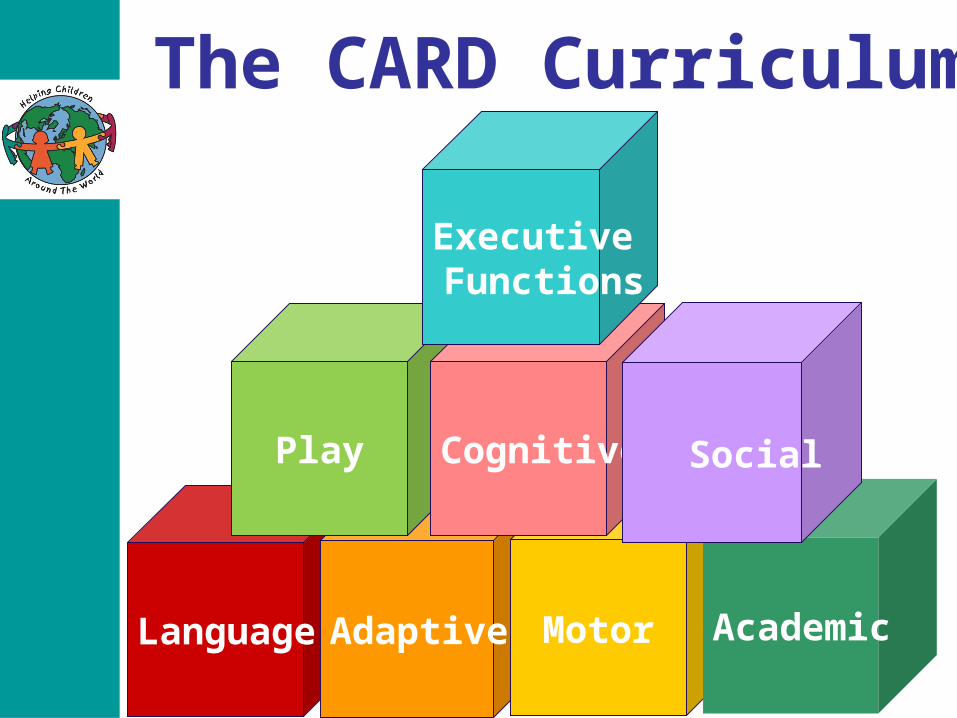
The CARD Curriculum
Language Adaptive Motor Academic
Play Cognitive
Executive Functions
Social

The CARD Curriculum
0-11 mos.Body PartsFollowing InstructionsGesturesMaking RequestsPeopleSound DiscriminationVerbal ImitationYes/No
1:0 – 1:11 yrs.ActionsAsking for InformationCategories
Language
ChoicesFast MappingFunctionsObjectsOppositesPrepositionsPronouns
2:0-2:11 yrs.AdverbsAttribute-ObjectConditionalityDeliver a MessageFeaturesGenderI Have/ISee
Listen to/Tell a StoryLocationsNegationPluralsRecalling EventsSound Speed & DurationSyllable SegmentationWh-Discrimination
3:0-3:11 yrs.Minimal PairsSame/DifferentSequencesSound Changes
Statement-Statement
4:0-4:11 yrs.Describe by Category/Feature/
FunctionPhonic Same/ DifferentStatement- QuestionWhat Goes With
5:0-5:11 yrs.Observational LearningSyntax
By Emerging Age and Verbal Operant:
Mixed Operants

Play Curriculum PlayDomains
Electronic Play
Beginning Play
Interactive Play
PretendPlay
Constructive Play
Sensorimotor PlayTask Completion Play
Initiating and Sustaining Play
Early Social GamesRead-to-Me Books & Nursery Rhymes
Music and MovementTreasure Hunt
Card and Board GamesLocomotor Play
Peer Play
Functional Pretend PlaySymbolic PlayImaginary Play
Sociodramatic Play
Block ImitationStructure Building
Sand and Water ConstructionsClay Constructions
Arts and Crafts
Audio and Video PlayComputer PlayVideo Games

Interactive Play: Nursery Rhymes
Adaptive CurriculumAdaptive
DomesticPet Care
Setting & Clearing TableTelephone Skills
TidyingMeal Preparation
CleaningGardeningLaundry
School Backpack PrepMaking a Bed
PersonalFeedingToileting
UndressingUnfastening
DressingPreventing Spread of Germs
BathingFasteningTeeth CareHair CareNail Care
Health Care

Motor CurriculumMotor
Gross
Fine
Oral
Visual

The CARD Curriculum School Skills
MathNumber Concepts
Rote CountingReading Numerals
Numeral ComprehensionOrdinal Position
Numerals in SequenceAddition
SubtractionAdvanced Counting
MoneyTime
Language Arts 1Reading
Visual Discrimination of SymbolsReciting AlphabetUppercase LettersLowercase LettersWord Recognition
Reading OrallyReading Comprehension
Book TopographyStory Comprehension
Story SummarizingText Comprehension
Language Arts 2Manuscript Writing
Printing SymbolsPersonal Data
Lowercase LettersUppercase Letters
Letters in SequenceLetters Dictated
Simple SentencesQuality of Printing
Physical EducationScience
HistorySocial Studies
NonAcademicSkills

The CARD Curriculum
Cognition: Meta-cognition: Identifying your own … Social Cognition: Inferring others’…
EmotionsThoughts
Knowledge
Desires
Beliefs
Intentions
Cognition

Classic Test of Social Cognition
“Sally-Anne” or False-Belief Task
Where will Sally look for her ball?
Where does she think her ball is?
Cognition

“Typical” Meta and SocialCognitive Development
First few months: Sense of Self
9 months: Joint Attention / Social Referencing
15 months: Pretence
18 months: Desire / Intention
2 years: Emotion
3 years: Knowing / Thinking
4 years: Belief / False-Belief
5 years: Intention – Accident vs. Purpose
Cognition
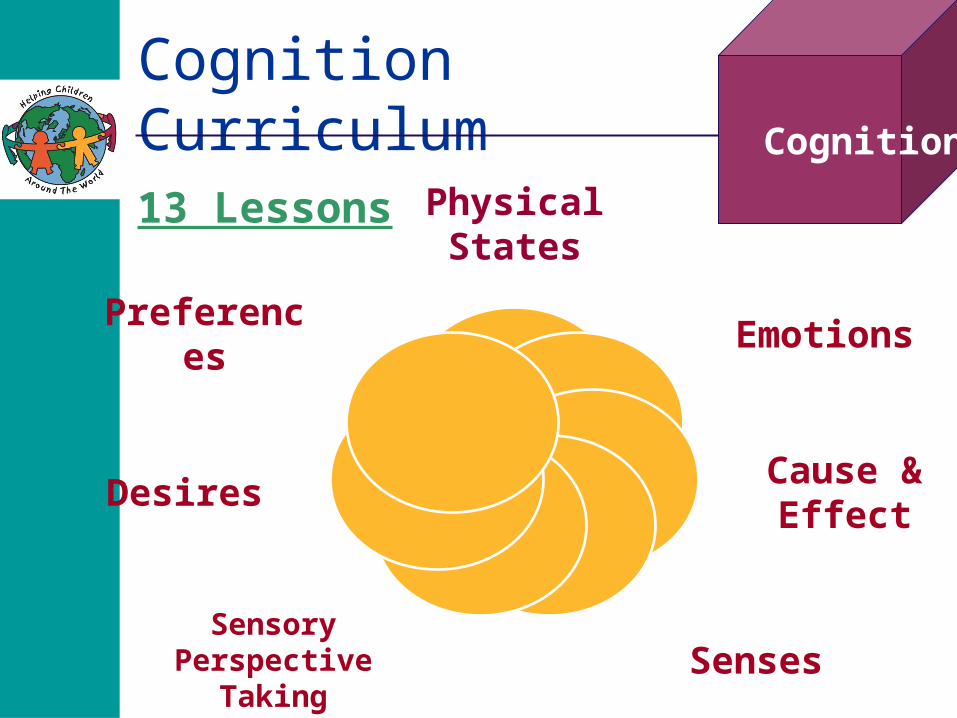
Cognition Curriculum
13 Lessons Physical States
Emotions
Cause & Effect
SensesSensory
Perspective Taking
Desires
Preferences
Cognition

Understanding other perspectives
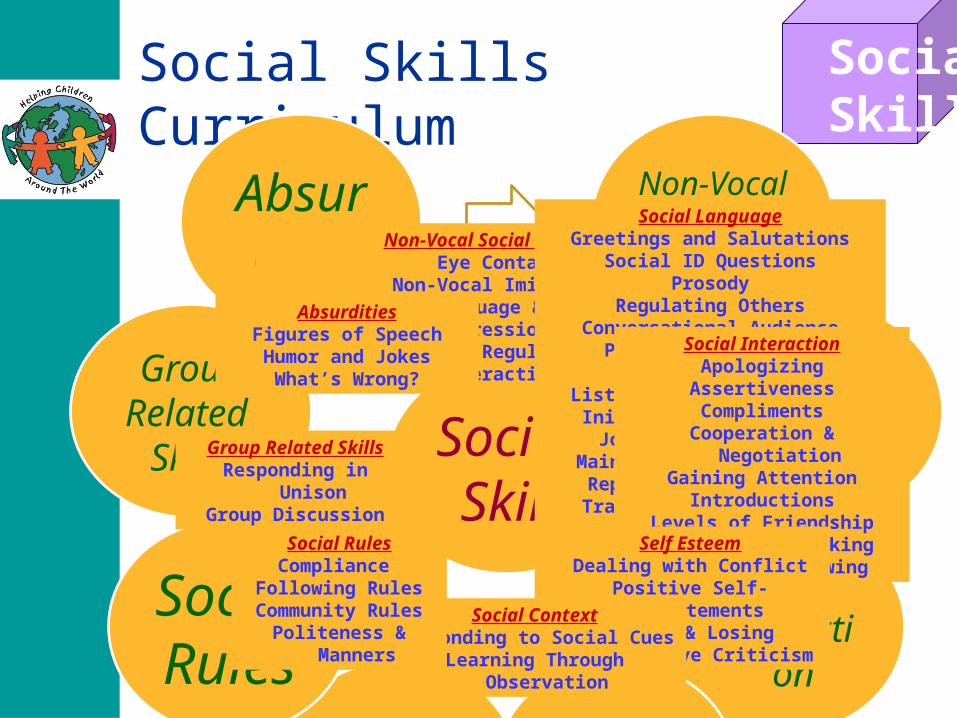
Social Skills CurriculumSocial Skills
Social Skills
Non-VocalSocial
Behavior
SocialLangua
ge
Social Interacti
onSelf Estee
m
Social Context
Social Rules
GroupRelated
Skills
Absurdities
Group Related SkillsResponding in Unison
Group Discussion
Non-Vocal Social BehaviorEye Contact
Non-Vocal ImitationBody Language & Facial Expressions
Gestures to Regulate Social Interaction
Social LanguageGreetings and Salutations
Social ID QuestionsProsody
Regulating OthersConversational Audience
Physical Context of ConversationListening to Conversation
Initiating ConversationJoining Conversation
Maintaining ConversationRepairing Conversation
Transitioning Topics of ConversationEnding Conversation
Social InteractionApologizing
AssertivenessCompliments
Cooperation & NegotiationGaining Attention
IntroductionsLevels of Friendship
Sharing & Turn Taking Lending & BorrowingSelf Esteem
Dealing with ConflictPositive Self-Statements
Winning & Losing Constructive Criticism
Social ContextResponding to Social Cues
Learning Through Observation
Social RulesCompliance
Following RulesCommunity Rules
Politeness & Manners
AbsurditiesFigures of SpeechHumor and JokesWhat’s Wrong?

Responding to Social Cues
The CARD Curriculum
Process that underlies goal directed behavior
Goal Directed Behavior Involves…
Visualizing situation
Identifying desired objective
Determining plan to meet objective
Monitoring progress to goal
Inhibiting distractions
Executive FunctionsWhat is Executive Function?
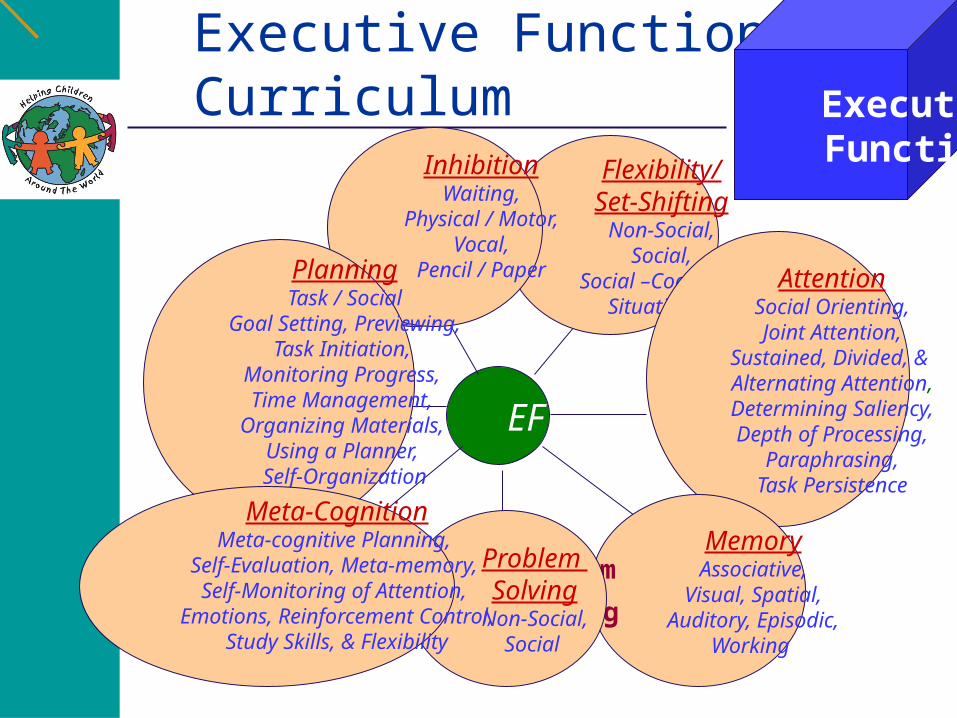
Executive Functions Curriculum
Executive Functions
Planning
Meta-CognitivePlanning
Inhibition Flexibility
Attention
Memory
EF
Flexibility/Set-Shifting
Non-Social,Social,
Social –Cognitive,Situational
AttentionSocial Orienting,Joint Attention,
Sustained, Divided, & Alternating Attention,Determining Saliency,Depth of Processing,
Paraphrasing,Task Persistence
MemoryAssociative,
Visual, Spatial,Auditory, Episodic,
Working
InhibitionWaiting,
Physical / Motor,Vocal,
Pencil / Paper
Problem
Solving
Problem Solving
Non-Social,Social
PlanningTask / Social
Goal Setting, Previewing,Task Initiation,
Monitoring Progress, Time Management,
Organizing Materials, Using a Planner, Self-Organization
Meta-CognitionMeta-cognitive Planning,
Self-Evaluation, Meta-memory, Self-Monitoring of Attention,
Emotions, Reinforcement Control,Study Skills, & Flexibility

Children’s Color Trail Test
Stroop Activities

Problem Solving: clarification

Telling Jokes

Summary
A good ABA program requires good assessment to determine exactly what your child needs to learn!
A good ABA program needs a lot of hours!
Don’t do 5 hours of ABA when 40 hours are recommended! This is like taking 5 mgs of a drug that has shown to be effective at 40 mgs! It wont work!
A 4 year progression
Year 1: Child entering at age 2-3 25 hours per week building to 40 hours Emphasis on
• Building a relationship with child • Replacing challenging behaviors with
functional communication Mands (Requests) Tacts (labels)
• Receptive identification (objects, actions, body parts, colors, shapes)
• Receptive instructions• Verbal and Non-verbal Imitation• Identical Matching• Play Skills (toy play)• Adaptive Skills (toilet training)• Fine and Gross Motor• Dietary restrictions/medical compliance
0
10
20
30
40
Year1
Year2
Year3
Year4
Allocation of Hours
Home-based School-based
A 4 year progressionYear 2:
Child age 3-4 40 hours (in home with partial transition to school) Emphasis on
• Building Expressive Language Objects, Actions, Attributes, Prepositions, Pronouns Categories, Functions, Occupations, Locations
• Beginning Conversation Intraverbals Reciprocal Statements Asking Questions
• Developing Observational Learning I See Sequences Tell me about/Describe
• Emotion Recognition• Inferring others desires• Play Skills (functional pretend, symbolic, imaginary)• Adaptive Skills (dressing, grooming, feeding)• Fine and Gross Motor• Sharing and Turn taking• Attention (dual and divided)
0
10
20
30
40
Year1
Year2
Year3
Year4
Allocation of Hours
Home-based School-based
A 4 year progressionYear 3: Child age 4-5 40 hours (20 hours at home; 20 hours at school) Sample Programs
• Advanced Language Concepts Pragmatic Language Maintaining Conversation (topic initiation, repair,
maintenance)• Meta and Social Cognition
Identifying and Managing own emotions Understanding other’s Perspectives, Knowledge
and Beliefs Inferences
• Executive Function Attention Saliency Flexibility with Routines Inhibition and Self Monitoring Planning
• Social Skills Levels of Friendship Recognizing Social Cues
• Problem Solving• Play Skills (peer play dates)• Adaptive Skills • Fine and Gross Motor
0
10
20
30
40
Year1
Year2
Year3
Year4
Allocation of Hours
Home-based School-based
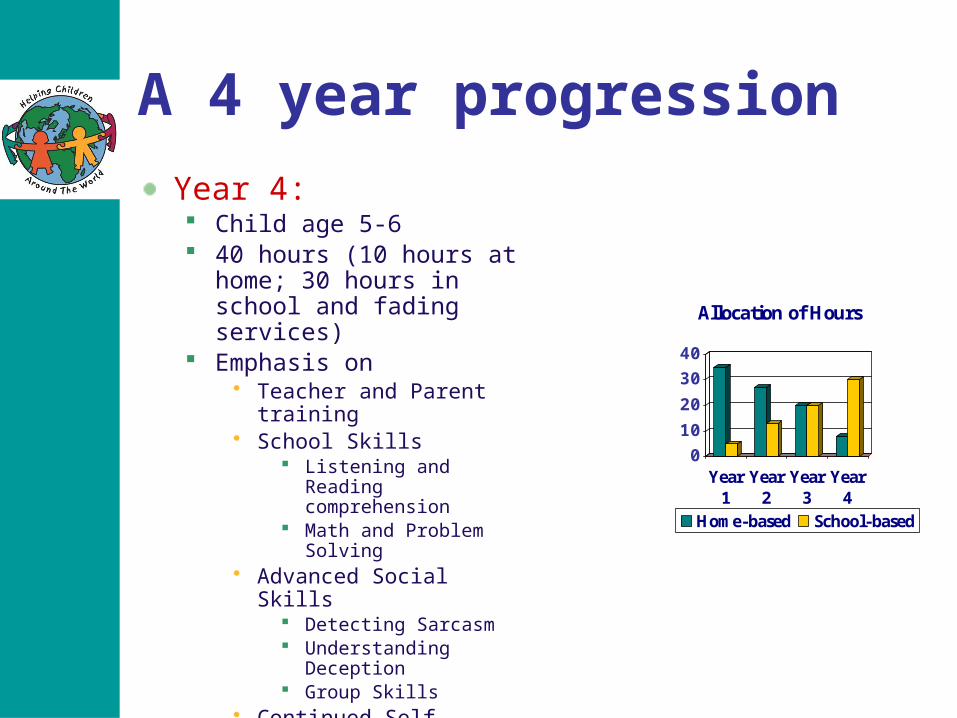
A 4 year progression
Year 4: Child age 5-6 40 hours (10 hours at home; 30
hours in school and fading services)
Emphasis on• Teacher and Parent training• School Skills
Listening and Reading comprehension
Math and Problem Solving• Advanced Social Skills
Detecting Sarcasm Understanding Deception Group Skills
• Continued Self Regulation Self Esteem and
Confidence Task and Social Planning
0
10
20
30
40
Year1
Year2
Year3
Year4
Allocation of Hours
Home-based School-based
Summary
Treat each child differently
Identify the medical issues that need treatment and treat them so that the child is medically stable, sleeping well and attending
Identify the sensory deficits that may be prohibiting normal learning so that you can modify the way you teach
Use ABA techniques to teach the child all the things he is lacking