Tuberculosis - The Filipino Doctor TUBERC… · · 2015-06-18Jose Ibarra Angeles PhilTIPS 7. Ms....
27
Tuberculosis (2005) Department of Health
-
Upload
dangnguyet -
Category
Documents
-
view
215 -
download
3
Transcript of Tuberculosis - The Filipino Doctor TUBERC… · · 2015-06-18Jose Ibarra Angeles PhilTIPS 7. Ms....

Tuberculosis (2005)
Department of Health

Tuberculosis
207
Board of Advisers
1. Dr. Myrna Cabotaje NCDPC, DOH2. Dr. Jaime Lagahid IDO, DOH3. Dr. Jennifer Ann Mendoza-Wi Philippine Coalition Against Tuberculosis (PhilCAT)
Technical Working Group (TWG)
Department of Health
1. Dr. Anna Marie Celina Garfin National Center for Disease Prevention and Control (NCDPC) 2. Dr. Ernesto Bontuyan Jr. NCDPC3. Ms. Agnes del Rosario NCDPC4. Ms. Ferdinand La Puebla NCDPC5. Ms. Ellen Melia Castillo National Tuberculosis Reference Laboratory (NTRL)6. Ms. Edna Nito National Center for Health Promotion (NCHP)
Center for Health Development
1. Dr. Lydia Rogando Center for Health Development (CHD)-Bicol2. Dr. Flor Elona Center for Health Development (CHD)-Eastern Visayas3. Dr. Willie Cabauatan Center for Health Development (CHD)-Cagayan Valley4. Ms. Joy Tabotabo Center for Health Development (CHD)-Central Visayas5. Ms. Gemma Tan Center for Health Development (CHD)-Ilocos
Local Government Units
1. Dr. Niela Jorvina Laguna Provincial Health Office2. Dr. Christina Giango Cebu Provincial Health Office3. Ms. Evangeline Rambuyon Negros Provincial Health Office4. Ms. Letty Rivera Batangas Provincial Health Office
Partners
1. Dr. Michael Voniatis World Health Organization (WHO)2. Dr. Tomohiro Shirahama JICA3. Dr. Arthur Lagos JICA4. Dr. Marilyn Gorra PhilTIPS5. Dr. Charles Yu PhilTIPS6. Mr. Jose Ibarra Angeles PhilTIPS7. Ms. Elaine Umali WVDFI
Department of HealthNational Tuberculosis Control Program
San Lazaro Compound, Rizal Avenue, Sta. Cruz, ManilaTelephone No: 743-8301 loc. 2350/2352

Tuberculosis
208
Technical Review Panel (TRP)
Department of Health
1. Dr. Rosalind Vianzon National Center for Disease Prevention and Control (NCDPC)2. Ms. Cirila Negad NCDPC3. Ms. Arlene Tivera NCDPC4. Dr. Vivian Lofranco Lung Center of the Philippines (LCP)5. Dr. Nora Cruz National Tuberculosis Reference Laboratory (NTRL)6. Ms. Paz Rostrata National Tuberculosis Reference Laboratory (NTRL)
Center for Health Development
1. Dr. Sylvia Somontan Center for Health Development (CHD)-Caraga2. Dr. Eloisa Segura Center for Health Development (CHD)-Davao3. Dr. Amelia Medina Center for Health Development (CHD)-NCR4. Dr. Edith Caloyloy Center for Health Development (CHD)-Western Visayas5. Ms. Marilou Gecosala Center for Health Development (CHD)-Northern Mindanao
Local Government Units
1. Dr. Bernard Caspe Iloilo City Health Office2. Dr. Ma. Lourdes San Juan Pasay City Health Office3. Dr. Marian Isiderio Eastern Samar Provincial Health Office4. Ms. Teresita Puente Pasig City Health Office5. Ms. Myla Espino Pasig City Health Office6. Ms. May Fernando Bulacan Provincial Health Office
Partners
1. Dr. Mariquita Mantala LEAD for Health Project2. Dr. Jubert Benedicto PhilCAT3. Ms. Amelia Sarmiento PhilCAT4. Mr. Albert Angelo Concepcion PhilCAT5. Dr. Maria Rubio MDM6. Dr. Jose Luis Portrero MDM7. Dr. Ma. Imelda Quelapio TDFI/GFATM8. Dr. Melvin Magno WVDFI
Publication Staff
1. Dr. Ma. Theresa Velasco Technical Editor2. Ms. Laila Garcia Assistant Technical Editor3. Ms. Rose Gonzales Creative Director

Tuberculosis
209
N
Y
Y
B. Only One (1) Smear-Positive
N
N
Y
Y
Y
N
Y
Figure 2.1
Algorithm for the Diagnosis of Pulmonary Tuberculosis
Figure 2.1a
1 23
4
5
6
1
2 34
56
7
8
TB symptomatic(cough for 2 weeks or
more)
Three (3) sputum
collection
Classify as Smear-Positive TB
B. Only One (1) Smear-Positive?
C. All 3 Smear-Negative
See Figure 2.1a
See Figure 2.2
A. 2 or 3 Smear-Positive?
Collect another 3 Sputum Specimens
Immediately
If at least one (1)
Smear-Positive?
Request for CXR
Classify as Smear-Positive TB
Consistent with active
TB?
Observation/further exam, if
necessary.
Classify as Smear-Positive
TB

Tuberculosis
210
C. All 3 Smear-Negative
Refer to Physician (Symptomatic Tx for
2-3 wks)
If symptoms persist, request
for CXR
Abnormal findings
on CXR?
Observation/further exam
TB Diagnostic Committee
Consistent with active
TB?
Classify as Smear-
Negative TB
N
Y
Y
N
Figure 2.2
Algorithm for the Diagnosis of Smear-Negative Pulmonary Tuberculosis
Not consistent with active
TB
No Abnormal findings on CXR
1
2
3
45
6 7
8 9
10

Tuberculosis
211
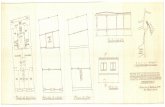
Figure 1.1. Flow of NTP Activities
COMMuNiTY
DOTS FACiLiTY
Case Finding
Diagnosis
initiation of Treatment
Case Holding with DOTS
Treatment Completion
report Treatment Outcome/request Supplies
Monitoring and Supervision
Sputum specimen (3 specimens) with NTP Laboratory Request Form for Direct Sputum Smear Microscopy
MiCrOSCOPY CeNTer
(Result of the DSSm. If results are Smear negative and with chest x-ray suggestive of TB, refer to TBDC for evaluation.)
T B D CSputum specimen (1 specimen) with Laboratory Request Form for DSSM
MiCrOSCOPY CeNTer
Results (DSSM for follow-up)
Symptoms of TBCough for two or more weeks, with or without• Fever• Chest and/or back pains not referable to any musculo-
skeletal disorders• Hemoptysis or recurrent blood-streaked sputum• Other symptoms, such as sweating, fatigue, body
malaise, shortness of breath

Tuberculosis
212
examinations alone. Likewise, results of the skin test for TB infection (PPD skin test) should not be used as bases for TB diagnosis in adults.
5. All municipal and city health offices shall be encour-aged to establish and maintain at least one sputum microscopy unit in their areas of jurisdiction.
6. Private-initiated Public-Private Mix DOTS (PPMD) units shall each have an in-house microscopy service.
7. Passive case finding shall be implemented in all DOTS facilities. Concomitant active case finding shall be encouraged only in areas where a cure rate of 85 per cent or higher has been achieved, or in areas where no sputum-smear positive case has been reported in the last three months.
8. Only trained medical technologists or microscopists shall perform DSSM (smearing, fixing, and staining of sputum specimens, as well as reading, recording, and reporting of results). However, in far flung areas, BHWs or other community health volunteers may be allowed to do smearing and fixing of specimens, as long as they have been trained and are supervised by their respective NTP medical technologists/micro-scopists.
iV. PrOCeDureS
A. Identification of TB Symptomatics (To be accomplished by DOTS facility staff)
1. Identify TB symptomatics consulting at the DOTS facility. Look out for those having cough for two or more weeks, with or without one or more of the fol-lowing signs and symptoms:
a. fever; b. chest and/or back pains not referable to any
musculo-skeletal disorders; c. hemoptysis or recurrent blood-streaked sputum; d. significant weight loss; and e. other symptoms, such as sweating, fatigue, body
malaise, and shortness of breath. 2. Motivate TB symptomatic to undergo DSSM. Explain
importance of the procedure and that of submitting three sputum specimens. Obtaining results from three sputum specimens increases the probability of finding acid fast bacilli.
3. Record details of each specimen submission (name of TB symptomatic, date of submission, and result) in the TB Symptomatics Masterlist/TB Symptomatics Target Client List.
4. Encourage household members of identified TB cas-es, who are also TB symptomatics, to undergo DSSM.
B. Collection and Transport of Sputum Specimens to the Microscopy Center
(To be accomplished by DOTS facility staff) 1. Explain the importance of submitting three sputum
specimens taken within two days. a. First specimen, also referred to as spot specimen,
is collected at the time of consultation, or as soon as the TB symptomatic is identified.
b. Second specimen is the very first sputum pro-duced early in the morning immediately after waking up. It is collected by the patient according to instructions given by the DOTS facility staff.
c. Third specimen, or second spot specimen, is col-lected when the TB symptomatic comes back to the DOTS facility to submit the second specimen.
d. All specimens should be collected according to
National Tuberculosis Control Program Manual of Procedures, 2005
CASe FiNDiNg
Case finding, which is the identification and diagnosis of TB cases among individuals with suspected signs and symptoms of TB, is a basic step in TB control. Funda-mental to case finding is the diagnostic methodadopted by the NTP because:
1. It provides a definitive diagnosis of active TB; 2. The procedure is simple; 3. It is economical; and 4. A microscopy center could be put up even in remote
areas.
DSSM results serve as bases for categorizing TB symp-tomatics according to standard case definition. These are also used to: a) monitor progress of patients with sputum smear-positive TB while they are receiving anti–TB treat-ment; and b) confirm cure at the end of treatment.
i. OBJeCTiVe
Early identification and diagnosis of TB cases
ii. DeFiNiTiON OF TerMS
TB symptomatic – any person with cough for two or more weeks with or without the following symptoms: fever; chest and/or back pains not referable to any musculo-skeletal disorders; hemoptysis or recurrent blood-streaked sputum; significant weight loss; and other symptoms, such as sweating, fatigue, body malaise, shortness of breath
Active case finding – a health worker’s purposive effort to find TB cases (among TB symptomatics in the communi-ty) who do not consult with personnel in a DOTS facility
Passive case finding – finding TB cases among TB symptomatics who present themselves in a DOTS facility
iii. POLiCieS
1. DSSM shall be the primary diagnostic tool in NTP case finding.
2. All TB symptomatics identified shall be asked to un-dergo DSSM for diagnosis before start of treatment, regardless of whether or not they have available X-ray results or whether or not they are suspected of having extra-pulmonary TB. The only contraindication for sputum collection is hemoptysis; in which case, DSSM will be requested after control of hemopty-sis.
3. Pulmonary TB symptomatics shall be asked to under-go other diagnostic tests (X-ray and/or culture), if necessary, only after they have undergone DSSM for diagnosis with three sputum specimens yielding negative results. The TBDC will evaluate the results of the chest X-ray, together with the clinical history and findings, and will recommend whether or not the case will be started on treatment.
4. Since DSSM is the primary diagnostic tool, no TB diagnosis shall be made based on the results of X-ray

Tuberculosis
213
instructions given by the DOTS facility staff. The first and third specimen collections are supervised by the DOTS facility staff to ensure quality sputum specimen collection. If quality sputum is not col-lected within two days, the patient is given one week to complete the three-specimen collection. If the patient fails to complete the three-specimen collection within one week, another set of three should be collected.
2. Prepare sputum cup, indicating patient’s complete name, and order of specimen (1st, 2nd, or 3rd).
3. Demonstrate how to produce quality sputum. Advise patient to:
a. Rinse his/her mouth with water. b. Breathe deeply, hold breath, then exhale slowly.
Repeat the entire sequence twice. c. Cough strongly at the height of deep inspiration
after inhaling deeply for the third time, and spit the sputum in the container.
Observe precautions against infection during the demonstration. Stay behind the patient. Collect specimen outside the DOTS facility where aerosols containing TB bacilli are diluted and sterilized by direct sunlight.
4. Collect specimen and check quantity and quality of sputum.
5. Seal sputum specimen container, pack it securely, and transport it to a microscopy center or laboratory, together with the completely filled up NTP Laboratory Request Form for DSSM. Do this as soon as possible or within four days after collection.
6. If specimen cannot be sent to a microscopy unit early enough, store it in a cool, dark, and safe place. No specimen shall remain unexamined over the week-end.
C. Smearing, Fixing, and Staining of Sputum Speci-men and reading, recording, and reporting of results
(To be accomplished by medical technologist or microscopist)
1. Record the information in the NTP Laboratory Regis-ter, including the type of sputum specimen submitted, i.e., mucoid, purulent, blood-streaked, or salivary.
2. Smear, fix, and stain each slide. 3. Read each slide and interpret the result as follows: 0- No AFB seen in 300 oil immersion field (OIF) +n – 1-9 AFB seen in 100 OIF 1+ - 10 – 99 AFB seen in 100 OIF 2+ - 1-10AFB /OIF in at least 50 fields 3 + -more than 10 AFB/OIF in at least 20 fields 4. Interpret the results of the three specimens and write
the final laboratory diagnosis in the lower portion of the NTP Laboratory Request Form for DSSM and on the Remarks column of the NTP Laboratory Register. Laboratory diagnoses are classified as follows:
a. Smear-positive - at least two positive sputum smear results
b. Doubtful -only one positive out of three sputum specimens examined (Request for another set of three sputum specimens).
• If at least one specimen from the second set of specimens is positive, laboratory diagnosis is positive.
• If all three specimens from the second set of specimens are negative, laboratory diagnosis is negative.
c. Smear-negative - all three sputum smear results
negative 5. Send request form back to requesting unit.
D. Decision on Patient’s Diagnosis Based on Labo-ratory results
(To be accomplished by DOTS facility staff) 1. Inform patient of result. • If positive, refer patient to physician for assessment
and initiation of treatment; and, • Encourage household members with signs and
symptoms of TB to consult at DOTS facility. • If doubtful, ask patient to submit another three
sputum specimens within one week. • If negative, refer patient to physician for further
assessment.
e. Diagnosis of Smear-negative Patients with Per-sistent Symptoms
(To be accomplished by physician) 1. Re-assess smear-negative patients with persistent
symptoms of TB. (Refer to Flow Chart 2.1 & 2.2) 2. Refer patient for X-ray examination, if warranted. 3. If X-ray findings are suggestive of TB, refer patient to
the TBDC. In areas where there is no TBDC, physi-cian may manage the patient.
F. referral to TBDC (To be accomplished by physician) 1. Fill up TBDC Referral Form and send it to TBDC,
together with all available chest X-ray films. 2. Wait for TBDC evaluation of results, which is sent
back to the DOTS facility. 3. Carry out TBDC recommendations.
g. Summary of Procedure The following four flow charts summarize the proce-
dure for TB case finding: 1. Flow Chart for the Diagnosis of Pulmonary Tubercu-
losis; 2. Flow Chart for the Diagnosis of Smear-Negative
Pulmonary Tuberculosis; 3. Guide to Case Finding; and 4. Guide to Diagnosis and Initiation of Treatment.
V. QuALiTY ASSurANCe FOr DSSM
The quality assurance (QA) program is a series of regular activities carried out to monitor the laboratory’s overall performance towards maintaining high quality results. DSSM results are highly significant not only to the patient but also to the entire NTP. As such, it is essential for the QA program to: 1) ensure that the reported results are accurate; 2) identify practices that are potential sources of error; and 3) ensure that appropriate corrective actions are initiated.
A. OBJeCTiVe Assurance of high quality DSSM services in NTP
B. COMPONeNTS QA for DSSM includes the following: 1. Quality Control (QC) is the systematic internal
monitoring of working practices, technical procedure, equipment, and materials, including quality of stains. These are performed regularly by the NTP medical technologist or microscopist.
2. External Quality Assessment (EQA) is a system of periodic independent measurement of performance

Tuberculosis
214
through collaboration with another competent labora-tory at a higher level (province or city). The trained NTP provincial or city coordinators and controllers are responsible for EQA.
3. Quality Improvement (QI) is a process by which the components of smear microscopy diagnostic services are analyzed by trained NTP provincial or city coor-dinators. This is a continuous undertaking designed to identify and address problem areas, which in turn will help ensure quality of DSSM services.
C. POLiCieS 1. In the DOTS facility, the NTP-trained medical tech-
nologist/microscopist shall maintain QC of routine work.
2. A Quality Assurance Center shall be established in every province and highly urbanized city to ensure that QA activities are maintained in all DOTS facili-ties. Provincial/city health offices are responsible for EQA, which includes blinded slide rechecking and on-site evaluations by persons identified to perform such activities.
3. CHDs and their regional laboratories shall support the provincial/city QA centers.
Procedures and forms are found in the Manual on the Quality Assurance for Sputum Smear Microscopy, March 2004.
CASe HOLDiNg
Case holding is the procedure which ensures that patients complete their treatment. Chemotherapy is currently the only way to stop the transmission of TB. While effective anti-TB drugs are available in the country, there are still many TB patients who are not cured. This is because many patients stop taking anti-TB drugs or they take their drugs irregularly. Patients are usually remiss in drug intake due to the long duration of treatment. The shortest duration of treatment is six months.
Treatment compliance is necessary to cure TB and avoid development of drug resistance. It is useless to search for cases if they could not be treated properly after they have been found. It would only encourage false hopes on the part of the patient.
Poor treatment compliance may lead to the following outcomes: chronic infectious illness; drug resistance; or death. Second-line anti-TB drugs for drug resistant cases are very expensive and most are not available in the country. The best way to prevent the occurrence of drug resistance is through regular intake of drugs for the prescribed duration. The strategy developed to ensure treatment compliance is called Directly Observed Treat-ment (DOT). It is one of the key components of DOTS towards achieving sufficient cure rate and preventing drug-resistant TB. DOT works by assigning a responsible person to observe or watch the patient take the correct medications daily during the whole course of treatment.
i. OBJeCTiVeEffective and complete treatment of TB cases, especially pulmonary sputum smear-positive cases
ii. DeFiNiTiON of TerMS
A. Classification of TB cases - TB cases shall be
classified based on the location of lesions, as well as the result of DSSM (Table 3.1).
B. Types of TB cases - TB cases shall be categorized based on the history of anti-TB treatment (Table 3.2). A thorough understanding of the types of TB cases is necessary in determining the correct category of treatment regimen.
C. Directly Observed Treatment (DOT) - DOT is a method developed to ensure treatment compliance by providing constant and motivational supervision to TB patients. DOT works by having a responsible person, referred to as treatment partner, watch the TB patient take medicines everyday during the whole course of treatment.
Any of the following could serve as treatment partner: a) DOTS facility staff, such as the midwife or the nurse; or b) a trained community member, such as the BHW, local government official, or former TB patient. A member of the patient’s family may not be as reliable as a health worker in serving as treatment partner, but he/she may be assigned as treatment partner during weekends and holidays.
DOT can be done in any accessible and convenient place for the patient (e.g., DOTS facility, treatment partner’s house, patient’s place of work, or patient’s house) as long as the treatment partner can effectively ensure the patient’s intake of the prescribed drugs and monitor his/her reactions to the drugs. It is important to supervise the smear-positive TB patients’ daily anti-TB drug intake during the intensive and continuation phases of short-course chemotherapy.
iii. POLiCieS
a. Aside from clinical findings, treatment of all TB cases shall be based on a reliable diagnostic technique, namely, DSSM.
b. Domiciliary treatment shall be the preferred mode of care.
c. Patients with the following conditions shall be recommended for hospitalization:
1. massive hemoptysis; 2. pleural effusion obliterating more than one-half
of a lung field; 3. miliary TB; 4. TB meningitis; 5. TB pneumonia; and 6. those requiring surgical intervention or with
complications. d. All patients undergoing treatment shall be super-
vised (DOT). No patient shall initiate treatment unless the patient and DOTS facility staff have agreed upon a case holding mechanism for treat-ment compliance.
e. The national and local government units shall ensure provision of drugs to all smear positive TB cases.
There are two formulations of anti-TB drugs: 1. Fixed–dose combination (FDCs) – Two or more
first-line anti-TB drugs are combined in one tablet. There are 2-, 3-, or 4-drug fixed-dose combinations.
2. Single drug formulation (SDF) – Each drug is pre-pared individually: INH, ethambutol, and pyrazina-

Tuberculosis
215
TB Symptomatics are thosewith cough for 2 or more weeks with or without 1 or more of the following:• Fever• Chest and/or Back pains• Hemoptysis• Significant weight loss• Other symptoms, such as sweating, fatigue, body malaise, shortness of breath
SPuTuM COLLeCTiON uNiT(To be accomplished by DOTS facility staff)
1. (Optional) Record results in the TB Symptoma-tics Masterlist (or TB Symptomatics Target Client List)
2. Explain result to the patient (If doubtful, immediately collect another 3 specimens for confirmation).
3. Refer to physician/nurse.
Figure 2.3 guide to Case Finding
DiAgNOSiS ANDiNiTiATiON OF TreATMeNT
SPuTuM COLLeCTiON uNiT
(To be accomplished by DOTS facility staff)
1. (Optional) Register patient in TB Symptomatics Masterlist (or TB Symp-
tomatics Target Client List) 2. Explain the importance of three sputum collections to the TB sympto-
matics. 3. Label each sputum container (name and order no. 1, 2, 3). 4. Collect three quality sputum specimens (1st spot, early morning, 2nd
spot). 5. Fill-up NTP Laboratory Request Form for DSSM 6. Pack and send specimen/s to the Microscopy Center, together with the
completely filled up NTP Laboratory Request Form for DSSM.
MiCrOSCOPY CeNTer(To be accomplished by the medical technologist/microscopist)
1. Register in the NTP Laboratory Register 2. Record date received and Laboratory Serial No. in the Laboratory Request
Form for DSSM 3. Perform DSSM: smearing, fixing, staining, and reading slides. 4. Record results in the Laboratory Request Form for DSSM and in the NTP
Laboratory Register 5. Send back accomplished Laboratory Request Form for DSSM to the collec-
tion unit

Tuberculosis
216
Figure 2.4. guide to Diagnosis and initiation of Treatment
CLiNiCAL DiAgNOSiSTo determine patient type and classification; done by DOTS facility staff
1. Verify information gathered on case finding. • Symptoms/condition of patient • Results of sputum examinations • Results of further examination (i.e., CXR, TBDC’s recommendations, culture, etc.) • Source of infection
2. Verify DSSM results.
3. review history of previous treatment. • When was previous treatment taken? For how long? • Where was the previous treatment taken? • What anti-TB drugs were taken? • What was the DSSM result? • What was the treatment outcome?
To be done by iNiTiATiON OF TreATMeNT
Physician 1. Physical assessment and prescription of appropriate category of treatment regimen for TB patient according to
patient classification and type Nurse 2. registration • Fill up NTP Treatment Card • Fill up two NTP ID Cards, one for treatment partner and
one for patient. • Register in the TB Register Designated DOTS Facility Staff 3. Health education with emphasis on key messages, such as: • TB is infectious. • TB can be cured but cure requires regular drug intake. • Irregular drug intake impedes cure and results in chronic
cases. • Anti-TB drugs have side-effects. • It is important to have follow-up DSSM examinations. • Family/treatment partner support is important. Nurse 4. Intake of first dose • Record date when treatment started. • Record due date of the first DSSM follow-up in the NTP Treatment Card and NTP ID Cards Designated DOTS Facility Staff/ 5. DOT Treatment Partners • Assign a treatment partner. • Do DOT for both intensive and continuation phases of treatment. • Conduct weekly consultation meetings at the DOTS facility
during the whole course of treatment. Nurse/Midwife 6. record keeping • Maintain and update TB Register. • Maintain and update NTP Treatment Card at the DOTS
facility. • See to it that both treatment partner and patient maintain,
update, and keep NTP ID Cards.

Tuberculosis
217
mide are in tablet form while rifampicin is in capsule form. These drugs are usually in blister packs good for one week.
The Department of Health shall ensure the provision of FDC drugs to LGUs and other DOTS facilities for all TB cases, giving priority to smear-positive cases. How-ever, LGUs shall procure a portion (at least 5% of the expected cases) of the requirements for SDF for those with adverse reactions necessitating withdrawal of FDC and for Category III cases.
f. Quality of FDCs must be ensured. FDCs must be ordered from a source with a track record of producing FDCs according to WHO-prescribed strength and standard of quality.
g. Treatment shall be based on recommended cat-egory of treatment regimen (Table 3.3).
h. Dosage per Category of Treatment Regimen
a. Fixed-Dose Formulation The number of tablets of FDCs per patient will
depend on the body weight. Hence, all patients must be weighed (using kilogram as a unit) be-fore treatment is started. Tables 3.4 and 3.5 show the treatment regimens for specific categories.
b. Single Drug Formulation Simply add one tablet of INH (100 mg), PZA
(500 mg), and E (400 mg) each for the patient weighing more than 50 kg before treatment initiation. Modify drug dosage within accept-able limits according to patient’s body weight, particularly those weighing less than 30 kg at the time of diagnosis (Table 3.8).
iV. PrOCeDureS
A. initiation of Treatment and registration1. Inform the patient that he/she has TB and motivate
him/her to undergo treatment.2. Refer patient living outside the catchment area to
the most accessible DOTS facility where his/her treatment can be supervised.
3. Weigh the patient.4. Refer patient to a physician for pre-treatment evalu-
ation. 5. Open the NTP Treatment Card and two NTP ID Cards
(one for treatment partner and one for patient) and start the treatment.
6. Watch patient swallow the initial dose. 7. Register patient in the TB Register.
B. ensuring Treatment Compliance through DOT
1. Together with the patient, identify a treatment partner.
2. Explain the importance of treatment compliance to the patient.
3. Administer patient’s drugs daily. Emphasize the fol-lowing to both patient and treatment partner:
a. Patient and treatment partner should meet at their agreed treatment unit everyday.
b. Drugs should be taken 2-3 hours after a regular meal. c. Treatment partner should make sure that the
patient swallows his/her drugs daily. d. After intake of drugs, treatment partner should
sign the treatment partner’s NTP ID Card, as well
as the patient’s NTP ID Card.4. Motivate treatment partner to be vigilant about pa-
tient’s treatment regimen. a. On Saturdays, Sundays, and holidays, when the
DOTS facility is closed, Treatment could be done at home but should be supervised by a trained family member.
b. Treatment partner should emphasize key mes-sages, such as:
• TB can be cured but cure requires regular drug intake for the prescribed duration.
• Patient should report any adverse drug reaction.
• Patient should undergo follow-up sputum examination on specified dates. Schedule of DSSM follow-up for Categories I and III patients is shown in Table 3.9 while Table 3.9.a shows the schedule for those in Category II.
5. Conduct regular (preferably weekly) consultation meetings with patient and treatment partner for treat-ment evaluation at the DOTS facility.
6. Exert effort to contact patient when he/she fails to report on due date.
C. Monitoring response to Treatment
1. Monitor sputum smear status of all patients under treatment, including initially sputum-smear negative patients, according to the standard schedule (Tables 3.9 and 3.9.a).
2. Modify treatment based on DSSM follow-up results (Tables 3.10, 3.10.a, 3.10.b, and 3.10.c, and Figures 3.1, 3.2, and 3.3).
Treatment Modifications Based on Results of DSSM Follow-up
Category i Treatment regimen
1. Do DSSM follow-up towards the end of the second month of treatment.
2. If the result is negative, start continuation phase (HR) and follow recommendations in Table 3.10.
3. If the result is positive, extend intensive phase (HRZE) for another month.
Refer to Table 3.10.a for treatment modifications of smear-positive patients after follow-up examination.
Category ii Treatment regimen
1. Do DSSM follow-up towards the end of the third month of treatment.
2. If DSSM result is negative, start continuation phase (HRE) and refer to Table 3.10.b.
3. If DSSM result is positive, extend intensive phase (HRZE) treatment for another month. Refer to Table 3.10.c.
Category ii Treatment regimen
1. Do DSSM follow-up towards the end of 2nd month of
treatment. 2. If the result is negative, start continuation phase (HR). 3. If the result is positive, declare as Failed, re-register
as Other, and start Category II treatment regimen.
D. Management of Adverse reactions to Drugs Closely monitor the occurrence of minor and major

Tuberculosis
218
Table 3.1 Classification of TB Cases
Location of Lesion DSSM Results Definition of Terms
1. A patient with at least two sputum specimens positive for AFB, with or without radiographic abnormalities consistent with active TB Smear-Positive Or 2. A patient with one sputum specimen positive for AFB and with radiographic abnormalities consistent with active pulmonary TB as determined by a physician Pulmonary TB Or or (PTB) 3. A patient with one sputum specimen positive for AFB and sputum culture positive for M. tuberculosis
A patient with at least three sputum specimens negative for AFB with radiographic abnormalities consistent with Smear-Negative active TB, and there has been no response to a course of antibiotics and/or symptomatic medications, and there is a decision by a physician and/or TBDC to treat the patient with a full course of anti- TB chemotherapy
1. A patient with at least one mycobacterial smear/culture positive from an extra- pulmonary site (organs other than the lungs: pleura, lymph nodes, genito-urinary tract, skin, joints and bones, meninges, intestines, peritoneum, and pericardium, among others)
extra-Pulmonary OrTB (eP) 2. A patient with histological and/or clinical evidence consistent with active extra pulmonary
TB and there is a decision by a physician to treat the patient with anti-TB drugs
Note: All EP cases shall undergo DSSM prior to treatment.
Table 3.2. Types of TB Cases
Types of TB Cases Definition of Terms
New A patient who has never had treatment for TB or who has taken anti-TB drugs for less than one month
relapse A patient previously treated for TB, who has been declared cured or treatment
completed, and is diagnosed with bacteriologically positive (smear or culture) TB Treatment Failure A patient who, while on treatment, is sputum smear-positive at five months or later
during the course of treatment
return After A patient who returns to treatment with positive bacteriology (smear or culture), Default (rAD) following interruption of treatment for two months or more
Transfer-in A patient who has been transferred from another facility adopting NTP policies with proper referral slip to continue treatment
Other All cases who do not fit into any of the above definitions. This may also include the following: 1. Other (positive) – a patient who was initially registered as a new smear-negative
case and turned out to be smear-positive during treatment; 2. Other (negative) – a patient who interrupted treatment for two or more months
and has remained or become smear-negative upon return for treatment; and 3. Chronic case – a patient who remains sputum-positive at the end of a re-treatment
regimen.
Note: *Treatment for primary and latent tuberculosis infection should not be considered as a previous TB treatment.

Tuberculosis
219
reactions to drugs, especially during the intensive phase. (Table 3.11). There are major side effects that necessitate withdrawal of the responsible drug. Since FDC drugs are already used, there is a need to switch to SDF whenever side effects to one or more components of the FDC are suspected.
e. Management of Cases Who interrupted Treatment
1. Perform routine DSSM on defaulters who come back for chemotherapy. Refer patients to DOTS physician for re-evaluation and re-treatment.
2. Manage new smear-positive patients who interrupted treatment according to recommended treatment modification (Table 3.12).
3. Manage Relapse and Treatment failure cases who interrupted treatment according to recommended treatment modification (Table 3.12.a).
4. Continue treatment for patients who were referred or transferred with proper referral slip.
However, do DSSM on patients without properly accom-plished referral slip.
F. Management of referred Cases 1. Assess and categorize all TB cases properly referred
for continuation of treatment by other DOTS facilities as Trans-in and manage them in accordance with NTP policies and guidelines.
Return the duplicate referral form to the referring unit.
2. Evaluate all other referred patients in accordance with NTP policies and guidelines.
g. Management of TB in Special Situations*1. Pregnancy Ascertain whether or not a woman is pregnant before
she starts TB treatment. Most anti-tuberculosis drugs are safe for pregnant women, except Streptomycin, which is ototoxic to the fetus. Advise a pregnant woman that successful treatment of TB with the recommended standardized treatment regimen is important for a successful outcome of pregnancy.
2. Breastfeeding A breastfeeding woman afflicted with TB should re-
ceive a full course of TB treatment. Timely and prop-erly applied chemotherapy is the best way to prevent transmission of tubercle bacilli to the baby. All anti-tuberculosis drugs are compatible with breastfeeding. A woman taking these drugs can safely continue to breastfeed. Mother and baby should stay together and the baby may be breastfed in the normal way. Give the baby prophylactic isoniazid for at least three months beyond the time the mother is considered to be non-infectious. Defer BCG vaccination of the newborn until the end of isoniazid prophylaxis.
3. Oral Contraceptives Rifampicin interacts with oral contraceptive medica-
tions with a risk of decreased protective efficacy against pregnancy. Advise a woman receiving oral contraceptives while on rifampicin treatment that she has the following options: 1) take an oral con-traceptive pill containing a higher dose of estrogen
(50), following consultation with a clinician; or 2) use another form of contraception.
4. Liver Disorders Isoniazid, rifampicin, and pyrazinamide are all associ-
ated with hepatitis. Of the three drugs, rifampicin is least likely to cause hepatocellular damage, although it is associated with cholestatic jaundice. Of the three agents, pyrazinamide is the most hepatotoxic.
Patients with the following conditions can receive the
usual short course chemotherapy regimens provided there is no clinical evidence of chronic liver disease: hepatitis virus carriage; a past history of acute hepa-titis; and excessive alcohol consumption. However, hepatotoxic reactions to antituberculosis drugs may be more common among these patients and should therefore be anticipated.
5. Established Chronic Liver Disease Patients with liver disease should not receive pyrazi-
namide. Isoniazid plus rifampicin plus one or two non-hepatotoxic drugs, such as streptomycin and ethambutol, can be used for a total duration of eight months. Alternative regimens are 9RE or 9SHE in the intensive phase, followed by HE in the continuation phase, with a total treatment duration of 12 months. Recommended treatment regimens are therefore 2SHRE/6HR, 9RE, or 2SHE/10HE.
6. Acute Hepatitis (e.g., Acute Viral Hepatitis) It is not common for a patient to have TB concurrently
with acute hepatitis unrelated to TB or TB treatment. Clinical judgment is necessary. In some cases, it is possible to defer TB treatment until the acute hepatitis has been resolved. In other cases, when it is necessary to treat TB during acute hepatitis, the combination of SE for three months is the safest option. If the hepatitis has been resolved, then put the patient on a continuation phase of six months isoniazid and rifampicin (6HR). If the hepatitis has not been resolved, SE should be continued for a total of 12 months.
7. Renal Failure Isoniazid, rifampicin, and pyrazinamide are either
eliminated almost entirely by biliary excretion or metabolized into non-toxic compounds. These drugs, therefore, can be given in normal dosages to patients with renal failure. Patients with severe renal failure should receive isoniazid with pyridoxine to prevent peripheral neuropathy.
Streptomycin and ethambutol are excreted by the kidney. Where facilities are available to monitor renal function closely, streptomycin and ethambutol may be given in reduced doses. The safest treatment regi-men for patients with renal failure is 2HRZ/4HR.
8. Treating TB and HIV* In patients with HIV-related TB, the priority is to treat
TB, especially smear-positive PTB to stop transmis-sion. However, patients with HIV-related TB can have Anti-Retroviral Therapy (ART) and anti-TB treatment at the same time, if managed carefully. Careful evaluation is necessary in judging when to start ART. In the case, for example, of a patient with a high risk of death during the period of TB treatment
* Source: Treatment of Tuberculosis: Guidelines for National Programs WHO/CDS/TB 2003.313

Tuberculosis
220
Table 3.4. Treatment regimen for Categories i & iii: 2HrZe/4Hr (FDC)
Body Weight No. of Tabs/Day No. of Tabs/Day (kg) intensive Continuation Phase Phase (2 months) (4 months) FDC-A (HrZe) FDC-B (Hr) 30-37 2 2 38-54 3 3 55-70 4 4 >70 5 5
Table 3.5. Treatment regimen for Categories ii: 2HrZeS/HrZe/5Hre (FDC)
intensive Continuation Body Phase Phase Wt. 1st Two Month 3rd month FDC-B e (kg) FDC-A STrePTO- FDC-A (Hr) 400 mg (HrZe) MYCiN (HrZe) 30-37 2 750 2 2 1 38-54 3 750 3 3 2 55-70 4 750 4 4 3 >70 5 750 5 5 3
Table 3.6. Treatment regimen for Categories i & iii: 2HrZe/4Hr (SDF)
No.of Tabs No.of Tabs /Day /Day ANTi-TB intensive Continuation Drugs Phase Phase (2 months) (4 months) Isoniazid (H) 300 mg 1 1 Rifampicin (R) 450 mg 1 1 Pyrazinamide (Z) 500 mg 2 Ethambutol (E) 400 mg 2
Table 3.3. recommended Category of Treatment regimen
TB Treatment regimens Category Type of TB Patient intensive Phase Continuation Phase i New smear-positive PTB, New smear-negative 2HRZE 4HR PTB with extensive parenchymal lesions on CXR as assessed by the TBDC, EPTB, and severe concomitant HIV disease
ii Treatment Failure, Relapse, RAD, Other 2HRZES/HRZE 5HRE iii New smear-negative PTB with minimal parenchymal lesions on CXR as assessed 2HRZE 4HR 4HR by the TBDC
iV Chronic (still smear-positive after supervised Refer to specialized facility or re-treatment) DOTS Plus Center
Refer to Provincial/City NTP Coordinator
Table 3.7. Treatment regimen for Categories ii: 2HrZeS/HrZe/5Hre (SDF) No. of Tabs No. of Tabs /Day /Day intensive Continuation ANTi-TB Drugs Phase Phase (3 months) (5 months) 1st Two 3rd Months Months Isoniazid (H) 300 mg 1 1 1 Rifampicin (R) 450 mg 1 1 1 Pyrazinamide(Z) 500 mg 2 2 Ethambutol (E) 400 mg 2 2 2 Streptomycin (S) 1 gm 1 vial/ day*
* 56 vials for two months
Table 3.8. Drug Dosage per Kg Body Weight
Drug Dose per kg body weight and maximum dose
Isoniazid 5 (4-6) mg/kg, and not to exceed 400 mg daily
Rifampicin 10 (8-12) mg/kg, and not exceed 600 mg daily
Pyrazinamide 25 (20-30) mg/kg, and not to exceed 2 g daily
Ethambutol 15 (15-20) mg/kg, and not to exceed 1.2 g daily
Streptomycin 15 (12-18) mg/kg, and not to exceed 1 g daily

Tuberculosis
221
Table 3.9 Schedule of DSSM Follow-up (Categories i and iii)
Schedule of Category i Category iii DSSM (2HrZe/4Hr) (2HrZe/4Hr) Follow-up regular With One- Treatment Month regular extension Treatment (HrZe) Towards end of YES (If positive) YES 2nd month Towards end of (If negative) YES 3rd month
Towards end of YES 4th month
Towards end of YES 5th month
Beginning of YES1
6th month
Beginning of YES1
7th month
1Check DSSM follow-up results at the end of treatment (during the last week of treatment) for patients who were smear-positive in the last DSSM follow-up and smear-negative in the repeated DSSM (Tables 3.10, and 3.10.a, and Figures 3.1, and 3.3).
Table 3.9.a Schedule of DSSM Follow-up (Category ii) Category ii (2HrZeS/HrZe/5Hre)
Schedule of DSSM regular Treatment With One-Month Follow-up extension (HrZe)
Towards end of 2nd month
Towards end of YES (If positive) 3rd month
Towards end of (If negative) YES 4th month
Towards end of YES 5th month
Towards end of YES 6th month
Towards end of 7th month
Beginning of YES1
8th month
Beginning of 9th month YES1
1Check DSSM follow-up results at the end of treatment (during the last week of treatment) for patients who were smear-positive in the last DSSM follow-up and smear-negative in the repeated DSSM (Tables 3.10.b, and 3.10.c, and Figures 3.2).

Tuberculosis
222
(i.e. disseminated TB and/or CD4 count <200/mm3), it may be necessary to start ART concomitantly with TB treatment. On the other hand, for a patient with smear-positive PTB as the first manifestation of HIV infection, who does not appear to be at risk of dying, it may be safer to defer ART until the initial phase of TB treatment has been completed. This decreases the risk of immune reconstitution syndrome and avoids the risk of drug interaction between Rifampicin and a Protease Inhibitor (PI).
Possible options for ArT in patients with TB includes the following:
• Defer ART until completion of TB treatment. • Treat TB with a rifampicin-containing regimen and
use efavirenz + two Nucleoside Reverse Tran-scriptase Inhibitors (NsRTIs).
• Defer ART until the completion of the initial phase of TB treatment and then use ethambutol and isoniazid in the continuation phase.
* Source: TB/HIV A Clinical Manual, 2nd Edition WHO/HTM/TB/2004.329
V. Treatment Outcome
A. Cured - a sputum smear-positive patient who has completed treatment and is sputum smear negative in the last month of treatment and on at least one previous occasion in the continuation phase
B. Completed Treatment - a patient who has completed treatment but has not met the criteria for cure or failure
This group includes: • A sputum smear-positive patient who has com-
pleted treatment but without DSSM follow -up during the treatment, or with only one negative DSSM during the treatment, or without DSSM in the last month of treatment.
• A sputum smear-negative patient who has com-pleted treatment
C. Died - a patient who died for any reason during the course of treatment
D. Failed • A patient who is sputum smear-positive at five
months or later during the treatment • An initially sputum smear-negative patient before
starting treatment who becomes smear-positive during the treatment. (Note: This case will be re-registered as Other with a new TB case number).
e. Defaulted - a patient who interrupted treatment for two consecutive months or more
F. Transferred out: A patient who transferred to an-other DOTS facility with proper referral slip for con-tinuation of treatment and whose treatment outcome is not known

Tuberculosis
223
Table 3.10. Treatment Modification for New PTB Smear-Positive Cases Based on the Results of DSSM Follow-up for Category i Treatment regimen Without extension
Towards Beginning Towards end of of end of 4th Month 6th Month 6th Month1
If smear-negative, continue If smear-negative, complete continuation continuation phase (HR). phase until end of treatment course and declare as cured. If smear-positive, If smear-negative in the If smear-negative, repeated DSSM, continue continuation declare as cured. immediately for phase (HR) and do confirmation and DSSM towards end of If smear-positive, declare consult DOTS 6th month of treatment. as Failed; re-register as Physician Treatment Failure and start with Category II treatment regimen.
If smear-positive again in the repeated DSSM, declare as Failed; re- register as Treatment Failure and start with Category II treatment regimen.
If smear-positive, If smear-negative, continue continuation If smear-negative, continue continuation phase (HR) and do DSSM towards end declare as cured. phase (HR). of 6th month of treatment. If smear-positive, declare as Failed; re-register as Treatment Failure and start with Category II treatment regimen.
If smear-positive, declare as Failed, re-register as Treatment Failure and start with Category II treatment regimen.
1Check DSSM follow-up results towards the end of the sixth month of treatment only for patients who are: 1) smear-positive in the beginning of the 6th month and smear-negative in the repeated DSSM; and 2) smear-positive towards the end of the fourth month but turned out to be negative in the beginning of the 6th month.

Tuberculosis
224
Table 3.10.a Treatment Modification for New PTB Smear-Positive Cases Based on the Results of DSSM Follow-up for Category i Treatment regimen With extension
Towards end Towards end Beginning of Towards end of 7th of 3rd Month of 5th 7th Month Month
If smear-negative, If smear-negative, If smear-negative, complete continuation start continuation continue continua- phase until end of treatment course and phase (HR). tion phase (HR). declare as cured. If smear-positive, If smear-negative in If smear-negative, repeat DSSM the repeated declare as cured immediately for examination, continue confirmation and continuation phase consult DOTS (HR) and do DSSM If smear-positive, declare as physician. towards end of 7th failed; re-register as month of treatment treatment failure and start Category II treatment regimen.
If smear-positive in the repeated examination, declare as failed; re- register as treatment failure and start Category II treatment regimen.
If smear-positive, If smear-negative, continue continuation If smear-negative, continue phase (HR) and do DSSM towards end of declare as cured. continuation 7th month of treatment. If smear-positive, declare as phase (HR). failed; re-register as treat- ment failure and start Cate- gory II treatment regimen.
If still smear-positive, declare as failed; re-register as treatment failure and start Category II treatment regimen.
If smear-positive, If smear negative, If smear-negative, complete continuation start continue phase until end of treatment course and continuation continuation declare as cured. phase (HR). phase (HR). If smear-positive, If smear-negative in If smear-negative, declare repeat DSSM the repeated as cured. immediately for examination, continue If still smear positive, declare confirmation and continuation phase as failed; re-register as consult DOTS (HR) and do DSSM treatment failure and physician. towards end of 7th and start Category II month of treatment. treatment regimen. If smear-positive in the repeated examination, declare as failed; re- register as treatment failure and start Catego- ry II treatment regimen.
If smear-positive, declare as failed; re- register as treatment failure and start Category II treat- ment regimen.1 Check DSSM follow-up results towards the end of the seventh month of treatment only for patients who are: 1) smear-positive in the beginning of the seventh month and smear-negative in the repeated DSSM; and 2) smear-positive towards the end of the fifth month and turned out to be negative in the beginning of the seventh month.

Tuberculosis
225
Table 3.10.b Treatment Modification for PTB Smear-Positive Cases Based on the Results of DSSM Follow-up for Category ii Treatment regimen Without extension Towards Beginning Towards end of end of 5th Month 8th Month 8th Month1 If smear- negative, continue If smear-negative, complete continuation continuation phase phase until the end of the treatment (HRE). course and declare as cured. If smear-positive, If smear-negative If smear-negative, declare repeat DSSM in the repeated as cured immediately for DSSM, continue confirmation and continuation phase If smear-positive, declare consult DOTS (HRE) and do DSSM as failed physician. towards end of 8th month. If smear-positive again in the repeated DSSM, complete continuation phase (HRE) until end of treatment course and declare as failed. If smear- positive, continue If smear-negative, continue continuation If smear-negative, declare continuation phase (HRE). phase (HRE) and do DSSM towards end. as cured of 8th month If smear positive, declare as failed. If smear-positive, complete continuation phase (HRE) until end of treatment course and declare as failed. 1 Check DSSM follow-up results towards the end of the 8th month of treatment only for patients who are: 1) smear-positive in the beginning of the 8th
month and smear-negative in the repeated DSSM; 2) smear-positive towards the
end of the 5th month and turned out to be negative in the beginning of the 8th month.
Table 3.10.c Treatment Modifications for PTB Smear-Positive Cases Based on DSSM Follow-up for Cat-egory ii Treatment regimen With extension
Towards end Towards end Beginning of Towards end of 4th Month of 6th Month 9th Month of 9th Month1
If smear-positive If smear-negative, If smear-negative, complete or smear-negative, continue continua- continuation phase until end of start continuation tion phase (HRE). treatment course and declare as cured phase (HRE). If smear-positive, If smear-negative If smear-negative, repeat DSSM in the repeated declare as cured. immediately for DSSM ,continue confirmation and continuation phase If smear- positive, consult DOTS (HRE) and do DSSM declare as failed. physician. towards end of 9th month of treatment. If smear positive again in the repeated DSSM, complete continuation phase (HRE) until end of treatment and declare as failed. If smear- positive, If smear negative, continue continuation If smear- negative, continue continua- phase (HRE) and do DSSM towards end declare as cured. tion phase (HRE). of 9th month of treatment. If smear-positive, complete continuation phase (HRE) until end of treatment course and declare as failed. If still smear-positive, complete conti- nuation phase (HRE) until end of treat- ment and declare as failed. 1Check DSSM follow-up results towards the end of the ninth month of treatment only for patients who are: 1) smear-positive in the beginning of the ninth month and smear-negative in the repeated DSSM; and 2) smear-positive towards the end of the sixth month and turned out to be negative in the beginning of the ninth month.

Tuberculosis
226
*
*
*
Figure 3.1. Category I Treatment Modification Based on DSSM Follow-up Results*
CATegOrY - i
1st mo. 2nd mo. 3rd mo. 4th mo. 5th mo. 6th mo. 7th mo.
H R Z E H R
If negative,
If positive, H R Z E H R with Extension
Figure 3.2. Category II Treatment Modification Based on DSSM Follow-up Results*
CATegOrY ii
1st mo. 2nd mo. 3rd mo. 4th mo. 5th mo. 6th mo. 7th mo. 8th mo. 9th mo.
H R Z ES H R Z E H R E
If negative, If positive,
H R Z E H R E
w/ Extension
Figure 3.3. Category III Treatment Modification Based on DSSM Follow-up Results*
CATegOrY – iii
1st mo. 2nd mo. 3rd mo. 4th mo. 5th mo. 6th mo.
H R Z E H R
*Check DSSM follow-up results at the end of treatment for patients who were smear-positive in the last DSSM follow-up and smear-negative in the repeated DSSM.

Tuberculosis
227
Table 3.11. guide in Managing Adverse reactions to Anti-TB Drugs
Adverse reactions Drug(s) probably Management responsible
Minor 1. Gastro-intestinal intolerance Rifampicin/INH Give medication at bedtime or give small
meals. 2. Mild skin reactions Any kind of drugs Give anti-histamines
3. Orange/red colored urine Rifampicin Reassure the patient
4. Pain at the injection site Streptomycin Apply warm compress. Rotate sites of injection.
5. Burning sensation in the feet Isoniazid Give pyridoxine (vitamin B6): due to peripheral neuropathy 100-200 mg daily for treatment 10 mg daily for prevention.
6. Arthralgia due to hyper- Pyrazinamide Give aspirin or NSAID. uricemia If symptoms persist, consider gout and
request for blood chemistry (uric acid determination and manage accordingly).
7. Flu-like symptoms Rifampicin Give antipyretics. (fever, muscle pains, inflam- mation of the respiratory tract) Major 1. Severe skin rash due to Any kind of drugs Discontinue anti-TB drugs and refer to hypersensitivity (especially streptomycin) DOTS physician.
2. Jaundice due to hepatitis Any kind of drugs Discontinue anti-TB and refer to DOTS (especially isoniazid, physician. If symptoms subside, resume rifampicin, and treatment and monitor clinically. pyrazinamide) 3. Impairment of visual acuity Ethambutol Discontinue ethmbutol and refer to an and color vision due to optic ophthalmologist. neuritis
4. Hearing impairment, ringing of Streptomycin Discontinue streptomycin and refer to the ear, and dizziness due to DOTS physician. damage of the eight cranial nerve 5. Oliguria or albuminuria due to Streptomycin Discontinue anti-TB drugs and refer to renal disorder Rifampicin DOTS physician.
6. Psychosis and convulsion Isoniazid Discontinue isoniazid refer to DOTS physician.
7. Thrombocytopenia, anemia, Rifampicin Discontinue anti-TB drugs and refer to shock DOTS physician.
For details on the management of adverse drug reactions, refer to the Interventions for Tuberculosis Control and Elimination [International Union Against Tuberculosis and Lung Disease (2002), pp. 87-91].

Tuberculosis
228
Table 3.12 Treatment Modifications for New Smear-Positive Cases Who Interrupted Treatment
Length of Length of Do a result of register again? Treatment treatment Interruption smear? smear modification
Less than one Less than 2 No No, use same treatment Continue Category I month weeks card. Treatment Regimen
2 weeks or Yes Positive No, open a new treatment Restart Category I more card (Use same TB case Treatment Regimen number). again Negative No, use same treatment Continue Category I card. Treatment Regimen
One to two Less than 2 No No, use same treatment Continue Category I months weeks card. Treatment Regimen
2 to 8 weeks Yes Positive No, use same treatment Complete remaining intensive phase; add one extra month of intensive phase.
Negative No, use same treatment Continue Category I card. Treatment Regimen.
More than 8 Positive Close previous regis- Start Category II weeks but still Yes tration as Defaulted; Treatment Regimen within 6-month re-register as RAD treatment and open a new treat- regimen ment card (new TB case number). Negative Close previous regis- Start Category II tration as Defaulted; Treatment Regimen re-register under Other and open a new treatment card. (New TB case number).
More than two Less than 2 No No, use same treatment Continue Category I months weeks card. Treatment Regimen
2 to 8 weeks Yes Positive Close previous registration Start Category II as Defaulted; re-register as Treatment Regimen RAD and open a new treat- ment card. (New TB case number). Negative No, use same treatment Continue Category I card. Treatment Regimen. More than 8 Positive Close previous registration Start Category II weeks but still as Defaulted; re-register as Treatment Regimen within 6-month RAD and open a new treat- treatment ment card. (New TB case regimen Yes number). Negative Close previous registration Start Category II as Defaulted; re-register Treatment Regimen under Other and open a new treatment card (New TB case number).
1This is the exceptional case categorizing as Defaulted a patient who interrupted treatment at less than 8 weeks.

Tuberculosis
229
Table 3.12.a Treatment Modifications for Relapse and Treatment Failure Cases Who Interrupted Treatment
Length of Length of Do a result of register again? Treatment treatment Interruption DSSM? DSSM modification
Less than one Less than 2 No No, use same treatment Continue Category II month weeks card. Treatment Regimen 2 weeks or Yes Positive No, open a new treatment Restart Category II more card. Treatment Regimen
Negative No, use same treatment Continue Category II card. Treatment Regimen
One to two Less than 2 No No, use same treatment Continue Category II months weeks card. Treatment Regimen
2 to 8 weeks Yes Positive No, use same treatment Complete remaining card. intensive phase; add one extra month of intensive phase.
Negative No, use same treatment Continue Category II card. Treatment Regimen. More than 8 Yes Positive Close previous registration Restart Category II weeks but still as Defaulted; re-register as Treatment Regimen within 8-month RAD and open a new treatment treatment card. regimen Negative Close previous registration Restart Category II as Defaulted; re-register Treatment Regimen under Other and open a new treatment card.
More than Less than 2 No No, use same treatment Continue Category II two months weeks card. Treatment Regimen 2 to 8 weeks Yes Positive Close previous registration Restart Category II as Defaulted; re-register Treatment Regimen as RAD and open a new treatment card.
Negative No, use same treatment Continue Category II card. Treatment Regimen.
More than 8 Yes Positive Close previous registration Restart Category II weeks but still as Defaulted; re-register as Treatment Regimen within 8-month RAD and open a new treatment treatment card. regimen Negative Close previous registration Restart Category II as Defaulted; re-register Treatment Regimen under Other and open a new treatment card.
1 This is the exceptional case categorizing as Defaulted a patient who interrupted treatment at less than 8 weeks.

Tuberculosis
230
AT THe TreATMeNT uNiT (DOTS Facility)
To be done by DOTS 1. Conduct health education for both patient and his/her family. facility staff Emphasize the following key messages: • Importance of regular drug intake; • Results of irregular drug intake; • Side effects of anti-TB drugs; • Necessity of DSSM follow-up; and • Importance of family and treatment partner support. 2. Conduct regular consultation meetings with patient and treatment partner during the course of treatment.
To be accomplished DOTS 3. Monitor and record treatment regularity. facility staff and treatment • TB Register (nurse) and partner • NTP Treatment Card (midwife) • NTP ID Card (Treatment Partner and TB patient)
To be accomplished 4. Do DSSM follow-up on time. by DOTS facility staff • Label container with the name of the patient. • Collect 1 sputum specimen (preferably early morning specimen). • Fill up the NTP Laboratory Request Form for DSSM. Pack the specimens securely and send to microscopy center, together with duly accomplished NTP Laboratory Request Form for DSSM
AT THe MiCrOSCOPY CeNTer(To be accomplished by the Medical Technologist or Microscopist)
Register in the NTP Laboratory Register. Smear, fix, stain, and do microscopic examination. Record the results in the NTP Laboratory Request Form for DSSM. and in the NTP Laboratory Register Send the NTP Laboratory Request Form for DSSM to the treatment unit.
AT THe TreATMeNT uNiT (DOTS Facility) To be accomplished Record DSSM results and due date of DSSM follow-up examination by DOTS facility staff in the NTP Treatment Card. Any follow-up examination with smear positive results must be referred to the physician. To be accomplished Record the results in the TB Register. by DOTS facility staff To be accomplished Inform treatment partner of DSSM results so that he/she can by DOTS facility staff update the NTP ID Card. To be accomplished Upon Treatment Completion: by DOTS facility staff 1. Evaluate and record treatment outcome in the TB Register and NTP Treatment Card. 2. Prepare and submit the Quarterly Report on Treatment Outcome.
Vi. Summary guides
The case holding procedure is summarized in the following Guide to Case Holdings and the accompanying Guide to Ensuring Treatment.
Figure 3.4. guide to Caseholding

Tuberculosis
231
Figure 3.5 guide to ensuring Treatment
Recorded information should be checked to ensure consistency of records of TB patients
NTP Treatment Card(To be accomplished by DOTS facility staff)Record of Individual patients• TB Case number• Classification, type, and regimen• DSSM results on diagnosis, for follow-up• Drug collection• Defaulter action• Treatment outcome
NTP Laboratory register(To be accomplished by the MT)Record of laboratory examination results- 2 types of sputum collections (for diagnosis and for follow-up)- DSSM results on diagnosis/for follow-up
The nurse should check the following NTP Laboratory Register information weekly:- is diagnosis correct?- is treatment regimen appropriate?- are all smear-positive cases reg-
istered and treated properly with DOT?
- are drugs collected on time?- are follow-up exams done on time?- are treatments regular and effec-
tive?- are actions taken to retrieve default-
ers?
TB register(To be accomplished by the DOTS facility staff)Record of Treatment Activity in the DOTS Facility• TB Case number• Classification, type, and regimen• DSSM results on diagnosis, and for follow-up• Defaulter action• Treatment outcome TB Register - DSSM results on diagnosis / - for follow up

Tuberculosis
232
Recommended Therapeutics(Drugs Mentioned in the Treatment Guideline)The following index lists therapeutic classifications as recommended by the treatment guideline. For the prescriber's reference, available drugs are listed under each therapeutic class.
ANTiTuBerCuLOSiS
Ethambutol Am-Europharma
Ethambutol HCl Odetol Pharex Ethambutol
Ethambutol/Isoniazid + Vit B6 Ebutol Ethamizid Forbutol
Isoniazid Am-Europharma Isoniazid Pharex Isoniazid
Isoniazid + Vit B6
Comprilex Pediatric Syrup Curazid Forte (Reformulated)
In-Tbex Isoxin Nicetal Odinah
Pyrazinamide Am-Europharma Pyrazinamide Drugmaker's Biotech
Pyrazinamide Pharex Pyrazinamide Pyramin PZA-Ciba Tub-Mix Zapedia Zcure Zinaplex
Rifampicin Am-Europharma Rifampicin Crisarfarm Drugmaker's Biotech Rifampicin Framacin Medifam Natricin Forte
Pharex Rifampicin PMI Rifampicin Refam Rexilan Rifadin Rifamax Rimactane Rimaped RiteMED Rifampicin Tub-Raxin
Streptomycin Biolab Streptomycin Sulfate
Rifampicin/Isoniazid Bifix Rifinah Rifzin Rimactazid 300/
Rimactazid 450 Rimactazid Paed
Rifampicin/Isoniazid + Vit B6 Kidz Kit 2
Refam Duo
Rifampicin/Isoniazid +Vit B6/Pyrazinamide Kidz Kit 3
Rifampicin/Isoniazid/Ethambutol Continukit Fixcom 3 Myrin Tres
Tritab
Rifampicin/Isoniazid/Pyrazinamide Combi Pack Econopack Rifater
Rimcure Paed Triofix
Rifampicin/Isoniazid/Pyrazinamide/Ethambutol 4D Econokit Econokit-MDR
Fixcom 4 Myrin-P Forte Quadtab Rimstar 4
Ethambutol/Rifampicin/Pyrazinamide/Isoniazid/Vits & Minerals Viper
Rifampicin/Isoniazid/Ethambutol/Multivitamins & Minerals Continukit Plus




![Indian Journal of Tuberculosis - tbassnindia.orgtbassnindia.org/forms/IJT_4.pdf · Indian Journal of Tuberculosis [Indian J Tuberc 2008; 55:175-178] ... NTM and the disease is not](https://static.fdocuments.us/doc/165x107/5af51edf7f8b9a9e598d9a83/indian-journal-of-tuberculosis-journal-of-tuberculosis-indian-j-tuberc-2008.jpg)