Treatment for Nausea and Vomiting: Filling up your Toolbox Tod A. Wyn, MD FAAHPM Associate Medical...
50
Treatment for Nausea and Treatment for Nausea and Vomiting: Filling up your Vomiting: Filling up your Toolbox Toolbox Tod A. Wyn, MD FAAHPM Tod A. Wyn, MD FAAHPM Associate Medical Director Associate Medical Director Hospice of Holland Hospice of Holland
-
Upload
benny-hollings -
Category
Documents
-
view
219 -
download
1
Transcript of Treatment for Nausea and Vomiting: Filling up your Toolbox Tod A. Wyn, MD FAAHPM Associate Medical...

Treatment for Nausea and Treatment for Nausea and Vomiting: Filling up your ToolboxVomiting: Filling up your Toolbox
Tod A. Wyn, MD FAAHPMTod A. Wyn, MD FAAHPMAssociate Medical DirectorAssociate Medical Director
Hospice of HollandHospice of Holland
DisclosureDisclosuress
No relevant financial disclosuresNo relevant financial disclosures
Off-label use of medications will be Off-label use of medications will be discusseddiscussed

ObjectivesObjectives
1) Be able to identify the mechanisms involved 1) Be able to identify the mechanisms involved in nausea and the various triggers that induce in nausea and the various triggers that induce nausea and vomiting.nausea and vomiting.
2) Identify the various treatments and 2) Identify the various treatments and remedies for nausea and the indications for remedies for nausea and the indications for their use.their use.
""One of the best temporary cures for pride and affectation is seasickness; a man who wants to vomit never puts on airs.” Josh Billings 1860
""The act of vomiting deserves your respect. It’s an orchestral event of the gut.”Mary Roach, Packing for Mars: The Curious Science of Life in the Void
"Oh, my God! I'm gagging and vomiting at the same time. I'm... I'm gavomiting!" Dr. Cox, Scrubs
Notable QuotesNotable Quotes

HistoryHistory

Famous Vomiting with the Famous Vomiting with the AncientsAncients
Famous Vomiting in PoliticsFamous Vomiting in Politics

Famous Vomiting in Famous Vomiting in SportsSports

Vomiting in Pop Vomiting in Pop CultureCulture

BloodlettingBloodlettingGingerGingerMintMintFrankincenseFrankincense
Q: What's the best food to eat when Q: What's the best food to eat when you're vomiting?you're vomiting? A: Bananas...because they taste the A: Bananas...because they taste the best coming back up!best coming back up!
Historical Historical RemediesRemedies

Case studyCase study
84 year-old woman diagnosed with ovarian cancer 3 years ago and is s/p surgery and chemo. Has diffuse abdominal metastasis which have caused partial bowel obstruction.
Chief issues have been nausea/vomiting, odynophagia/dysphasia, and GERD.
Wants to keep eating.
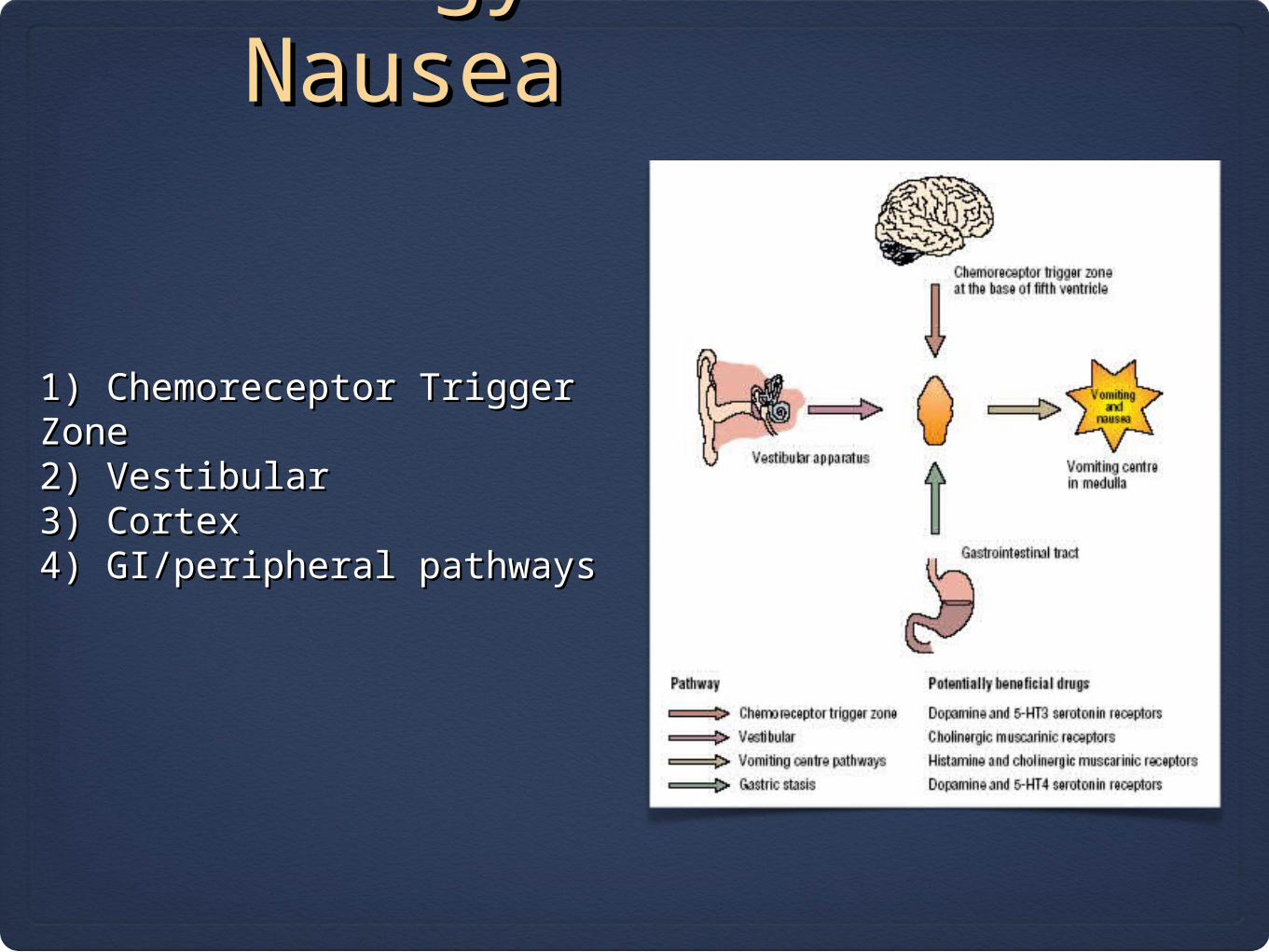
1) Chemoreceptor Trigger Zone1) Chemoreceptor Trigger Zone2) Vestibular2) Vestibular3) Cortex3) Cortex4) GI/peripheral pathways4) GI/peripheral pathways
Etiology of Etiology of NauseaNausea

AssessmentAssessment
OnsetFrequencyRelationship to eatingRelationship to medsCurrent anti-emetics
Chronic vs. ProgressingAlleviating factorsSeverity (scale: 1-10)Goal

Identify Potential Reversible Causes
* Drugs (chemo, opioids, abx, NSAIDS, SSRIs)* Constipation* Gastroparesis* GERD* Uremia* Infection
* Pain* Dehydration* Electrolyte imbalance (high Ca)* Endocrine dysfunction* Increased ICP* Anxiety

Other Causes
* Pregnancy* Cyclic Vomiting Syndrome* Hepatic disease* Migraine headaches* Following surgery* Myocardial infarction* Violent coughing* Hangover* Meniere's disease


Most patients have multi-factorial Most patients have multi-factorial causescauses

Non PharmacologicNon PharmacologicTreatmentTreatment
•Reassurance/relaxation•Correct dehydration, correct electrolyte distrubances•Decompress, correct constipation•Oral hygeine•Reduce portions and use cold food•Reduce or eliminate tube feedings•Avoid odors

Matching Etiology with Matching Etiology with MechanismMechanism
1) Chemoreceptor Trigger Zone2) Vestibular3) Cortex4) GI/peripheral pathways
1) D2 and 5HT3 antagonists2) Antihistamines and Anti-muscarinics 3) Antihistamines and Anxiolytics4) D2 and 5HT3 antagonists
Matching Medication to Matching Medication to MechanismMechanism
D2 Antagonists: Haldol, Reglan, Compazine, Thorazine
5HT3 Antagonists: Zofran, Emend, Remeron
Anti-histamines: Benadryl, Phenergan, Antivert, Cyclizine
Anti-cholinergics/anti-muscarinics : Hyoscyamine, Scopolamine
Others: Decadron, Ativan
Pro-motility: Reglan, Propulsid
Opioid-Opioid-InducedInduced
Primarily hits CTZPrimarily hits CTZ
Think D2 Antagonist:Think D2 Antagonist:Reglan, Haldol, Compazine, ThorazineReglan, Haldol, Compazine, Thorazine
Consider opioid-rotationConsider opioid-rotation
Chemotherapy-Chemotherapy-InducedInduced
Primarily from 5HT3 stimulating gut/peripheral Primarily from 5HT3 stimulating gut/peripheral pathwayspathways
Think 5HT3 antagonists: Zofran, Emend, RemeronThink 5HT3 antagonists: Zofran, Emend, Remeron
Malignant Bowel Malignant Bowel ObstructionObstruction
• Primarily from stimulation of CTZ
• Think D2-antagonists: Reglan, Compazine, Haldol
• Consider Octreotide
• Remember Decadron
• Don’t forget to decompress
Motion-InducedMotion-Induced
Primarily from stimulation of vestibular systemPrimarily from stimulation of vestibular system
Think anti-muscarinics: Scopolamine, HyoscyamineThink anti-muscarinics: Scopolamine, Hyoscyamine
Think anti-histamines: Antivert, Phenergan Think anti-histamines: Antivert, Phenergan

Increased ICPIncreased ICP
Steroids act to decrease pressureSteroids act to decrease pressure
Directly stimulates the Vomiting CenterDirectly stimulates the Vomiting Center
Think anti-histamines Think anti-histamines

Most patients have multi-factorial Most patients have multi-factorial causescauses
DosingDosing"Go hard or go home" "Go hard or go home"
Appropriate doses...Appropriate doses... scheduled around-the-clockscheduled around-the-clock

Case study Case study revisitedrevisited
Patient was placed on Reglan (10 mg BID), Zofran (4 mg QID), and a PPI.
Initially seemed to respond well, but then had worsening nausea. No emesis, and symptom description complicated by confusion between nausea and GERD.
Added Phenergan (25 mg q6 hrs) and an H2 blocker, but had minimal improvement.

Intractable Intractable VomitingVomiting
Poly-Drug Regimens Poly-Drug Regimens and Routes of and Routes of DeliveryDelivery
General guidelines:General guidelines: * Don't use more than one drug from each class* Don't use more than one drug from each class * Consider less traditional medications: Decadron, Ativan* Consider less traditional medications: Decadron, Ativan * May need to consider alternate routes: topical, rectal, SQ* May need to consider alternate routes: topical, rectal, SQ * Be alert for drug interactions* Be alert for drug interactions * May need to consider "palliative sedation" (eg Propofol)* May need to consider "palliative sedation" (eg Propofol)

ABHR (Ativan, Benadryl, ABHR (Ativan, Benadryl, Haldol, Reglan)Haldol, Reglan)
Can be given topically or rectallyCan be given topically or rectally
But does it work?But does it work?

Continuous InfusionsContinuous InfusionsHave the potential to provide very quick and Have the potential to provide very quick and effective relief of intractable nauseaeffective relief of intractable nausea
Benadryl/Ativan/Decadron (BAD drip): (0.2-2.0 ml/hr)(50 cc D5W, 200 mg Benadryl, 8 mg Ativan, 20 mg Decadron)
Can be transitioned over to an oral regimen Can be transitioned over to an oral regimen
Could consider Haldol/Ativan/Decadron, or Reglan/Ativan/Decadron
Reglan/Benadryl/Decadron (RBD drip): (0.5-1.5 ml/hr) (50 cc NS, 80 mg Reglan, 100 mg Benadryl, 8 mg Decadron)
Alternative Alternative TherapiesTherapies

AcupressureAcupressure
Thought to work at the P6 Thought to work at the P6 (Neiguan) point.(Neiguan) point.Examples include "sea bands"Examples include "sea bands"
Five Phases (Wu Xing) TheoryFive Phases (Wu Xing) Theory

Acupuncture Acupuncture
In nausea, stimulation of point In nausea, stimulation of point P6 (forearm) is believed to P6 (forearm) is believed to offer relief.offer relief.
Generally believed to be more Generally believed to be more helpful in setting of chemotherapy helpful in setting of chemotherapy and post-op nauseaand post-op nausea

Korean Hand Korean Hand TherapyTherapy

AromatherapyAromatherapy
Oil of Mint

Non-traditional MedsNon-traditional Meds
5HT4 AgonistProlonged QT Available only for "compassionate use"
Anti-histamine, sedatingNO evidence of causing birth defects (thank you William McBride)
Bendectin (pyridoxine/doxylamine)
Propulsid (cisapride)
Ginger lollipops
MarijuanMarijuana a
Active ingredient: Nine-delta-Active ingredient: Nine-delta-tetrahydrocannabinol (THC)tetrahydrocannabinol (THC)
Demonstrated effectiveness in:Demonstrated effectiveness in: Amelioration of nausea and vomitingAmelioration of nausea and vomiting Inducement of hunger in settings of chemotherapy and Inducement of hunger in settings of chemotherapy and AIDSAIDS AnalgesiaAnalgesia Lowering intra-occular pressureLowering intra-occular pressure ? Multiple Sclerosis? Multiple Sclerosis ? Depression? Depression
Legal Legal Issues:Issues:
Michigan Law vs. FDAMichigan Law vs. FDA
On Dec.4, 2008, the Michigan Medical On Dec.4, 2008, the Michigan Medical Marihuana Act was enacted into law Marihuana Act was enacted into law allowing patients with debilitating allowing patients with debilitating medical conditions such as medical conditions such as HIV,cancer, and Hepatitis C to legally HIV,cancer, and Hepatitis C to legally possess and use marijuana. The possess and use marijuana. The patient can have up to two and a half patient can have up to two and a half ounces of usable marijuana and twelve ounces of usable marijuana and twelve plants that are kept in an enclosed plants that are kept in an enclosed and locked facility.and locked facility.Cannabis is classified as a Schedule I Cannabis is classified as a Schedule I drug under the federal Controlled drug under the federal Controlled Substances Act of 1970 and is deemed Substances Act of 1970 and is deemed to have a high potential for abuse and to have a high potential for abuse and no legitimate medical usesno legitimate medical uses

Administration and Administration and DosingDosing
• Smoking – associated with exposure to CO and tar, similar to smoking nicotine. Peaks at 2.5 minutes and then declines over 30 minutes
• Vaporizing – no elevation of CO or tar. Safer, more predictable
• Ingesting – peaks at 2.5 hours (and at a much lower level) and then declines over 25 hours. Can still produce psycho-active metabolite.

Principal psychoactive component of cannabis
Tetrahydrocannabinol
Dronabinol (Marinol) - a Schedule III drug
Nabilone (Casemet) - a Schedule II drug available in Canada
Sativex (THC + canabidiol) mouth spray for M.S. patients

Who does it Help?Who does it Help?
• Those with symptoms un-relieved by traditional meds
• Those with history of recreational use of marijuana

Thoughts on MJThoughts on MJ
• May offer some benefit for nausea, appetite, and pain
• Other drugs probably at least as good or better
• MJ does have side effects and drug interactions
• Those most likely to benefit are those who’ve done poorly on traditional meds and have prior experience
• Those least likely to benefit are the elderly with no prior experience

• Research data is poor
• High risk for diversion and abuse
• Michigan’s Medical marijuana law is not based on current science, is confusing , and is in opposition to Federal Law


Case study Case study conclusionconclusion
Patient was placed on subcutaneous BAD drip which was gradually increased to 1.2 ml per hour with 0.4ml bolus prn.
She continued her H2 blocker and PPI, but seemed to get her best GERD relief from a GI cocktail.
Patient responded well with nearly complete resolution of both symptoms. Within a couple of weeks, she stopped eating and gradually became less responsive. She passed away comfortably.

Random Random ThoughtsThoughts* Reglan (metoclpramide) 1st drug of choice: has GI effects and CTZ effects
* Haldol is a great anti-emetic
* Steroids too
* NG tube may be necessary
* Combination drugs of different mechanisms may be helpful
* Anticipatory dosing most beneficial
* Use of 5-HT3 antagonists of questionable benefit in non-chemotherapy-induce N/V

Successful Successful Strategies Strategies
Attempt to identify the most likely etiology and mechanism involvedAttempt to identify the most likely etiology and mechanism involved
Choose the medication based on that mechanismChoose the medication based on that mechanism
Dose appropriately and on a scheduled basis Dose appropriately and on a scheduled basis
If ineffective, consider multi-drug regimensIf ineffective, consider multi-drug regimens
Consider continuous infusions (RBD, BAD)Consider continuous infusions (RBD, BAD)
Consider less traditional interventions/medicationsConsider less traditional interventions/medications