Transplantation of Muscle-Derived Stem Cells into the ...€¦ · nerve injury group (n=5, group...
5
Korean Journal of Urology Ⓒ The Korean Urological Association, 2011 359 Korean J Urol 2011;52:359-363 www.kjurology.org DOI:10.4111/kju.2011.52.5.359 Investigative Urology Transplantation of Muscle-Derived Stem Cells into the Corpus Cavernosum Restores Erectile Function in a Rat Model of Cavernous Nerve Injury Jang Chun Woo, Woong Jin Bae, Su Jin Kim, Sung Dae Kim 1 , Dong Wan Sohn, Sung Hoo Hong, Ji Youl Lee, Tae-Kon Hwang, Young Chul Sung 2 , Sae Woong Kim Department of Urology, College of Medicine, The Catholic University of Korea, Seoul, 1 Department of Urology, College of Medicine, The Jeju National University of Korea, Jeju, 2 Division of Molecular and Life Science, Integrative Bioscience and Biotechnology, WCU, POSTECH, Pohang, Korea Purpose: Muscle-derived stem cells (MDSCs) harvested from skeletal muscles have the advantage of providing easier access and do not pose the immunogenic risks of embry- onic stem cells. We investigated the effect of intracavernosal transplantation of MDSCs on erectile function in rats with bilateral cavernous nerve injury. Materials and Methods: Adult male white rats underwent experimentation in 3 groups: group I, sham operation; group II, bilateral cavernous nerve injury; group III, bilateral cavernous nerve injury with MDSC injection. MDSCs were harvested from the femoral muscle of rats and were then injected into the cavernosum. Survival of MDSCs and measurement of erectile function was studied after 4 weeks. We checked the intra- cavernosal pressure (ICP) and obtained penile tissue. The expression of cyclic guano- sine monophosphate (cGMP) was analyzed. Results: Four weeks after transplantation, PKH-26-labeled MDSCs were identified in the cavernosal tissues of group III. Peak ICP and the drop rate of group II were 52±8.7 mmHg and 34±6.5 mmHg/min, respectively, whereas peak ICP and the drop rate of group III were 97±15.6 mmHg and 17±4.9 mmHg/min, respectively, showing that erec- tile function improved after MDSC transplantation (p<0.05). The expression of cGMP was significantly lower in group II (21.9±5.8 fmol/well) than in group I and group III (70.2±10.3 and 58.9±10.5 fmol/well, respectively). Conclusions: In a cavernous nerve injury rat model, intracavernosal transplantation of MDSCs showed acceptable survival of MDSCs as well as improvement of erectile function. Key Words: Erectile dysfunction; Stem cells; Transplantation This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. Article History: received 5 April, 2011 accepted 21 April, 2011 Corresponding Author: Sae Woong Kim Department of Urology, Seoul St. Mary’s Hospital, 505, Banpo-dong, Seocho-gu, Seoul 137-701, Korea TEL: +82-2-2258-6226 FAX: +82-2-599-7839 E-mail: [email protected] We acknowledge the financial support of the Healthy Medical Treatment Research and development Program of the Ministry of Health & Welfare (No. A090481) and in part the Catholic Institute of Cell Therapy Basic Science Programs Foundation. INTRODUCTION Erectile dysfunction is a common complication after radi- cal prostatectomy. With detailed understanding of the anatomy of the cavernous nerves [1], nerve-sparing proce- dures have been developed [2] and applied to carefully se- lected patients. Nevertheless, considerable numbers of pa- tients who undergo radical prostatectomy become impotent. In one study, among men who were potent at baseline, the proportion who were impotent 18 or more months after sur- gery was 65.6% of men undergoing non-nerve-sparing pro- cedures, 58.6% of men undergoing unilateral nerve-spar- ing procedures, and 56.0% of men undergoing bilateral nerve-sparing procedures [3]. Recovery of erectile dysfunc- tion is slow, usually taking months to years, and even if the nerve-sparing procedure is done by experienced hands, one third of patients need the aid of medications such as phos- phodiesterase inhibitors [4].
Transcript of Transplantation of Muscle-Derived Stem Cells into the ...€¦ · nerve injury group (n=5, group...

Korean Journal of UrologyⒸ The Korean Urological Association, 2011 359 Korean J Urol 2011;52:359-363
www.kjurology.orgDOI:10.4111/kju.2011.52.5.359
Investigative Urology
Transplantation of Muscle-Derived Stem Cells into the Corpus Cavernosum Restores Erectile Function in a Rat Model of Cavernous Nerve InjuryJang Chun Woo, Woong Jin Bae, Su Jin Kim, Sung Dae Kim1, Dong Wan Sohn, Sung Hoo Hong, Ji Youl Lee, Tae-Kon Hwang, Young Chul Sung2, Sae Woong KimDepartment of Urology, College of Medicine, The Catholic University of Korea, Seoul, 1Department of Urology, College of Medicine, The Jeju National University of Korea, Jeju, 2Division of Molecular and Life Science, Integrative Bioscience and Biotechnology, WCU, POSTECH, Pohang, Korea
Purpose: Muscle-derived stem cells (MDSCs) harvested from skeletal muscles have the advantage of providing easier access and do not pose the immunogenic risks of embry-onic stem cells. We investigated the effect of intracavernosal transplantation of MDSCs on erectile function in rats with bilateral cavernous nerve injury.Materials and Methods: Adult male white rats underwent experimentation in 3 groups: group I, sham operation; group II, bilateral cavernous nerve injury; group III, bilateral cavernous nerve injury with MDSC injection. MDSCs were harvested from the femoral muscle of rats and were then injected into the cavernosum. Survival of MDSCs and measurement of erectile function was studied after 4 weeks. We checked the intra-cavernosal pressure (ICP) and obtained penile tissue. The expression of cyclic guano-sine monophosphate (cGMP) was analyzed.Results: Four weeks after transplantation, PKH-26-labeled MDSCs were identified in the cavernosal tissues of group III. Peak ICP and the drop rate of group II were 52±8.7mmHg and 34±6.5 mmHg/min, respectively, whereas peak ICP and the drop rate of group III were 97±15.6 mmHg and 17±4.9 mmHg/min, respectively, showing that erec-tile function improved after MDSC transplantation (p<0.05). The expression of cGMP was significantly lower in group II (21.9±5.8 fmol/well) than in group I and group III (70.2±10.3 and 58.9±10.5 fmol/well, respectively). Conclusions: In a cavernous nerve injury rat model, intracavernosal transplantation of MDSCs showed acceptable survival of MDSCs as well as improvement of erectile function.
Key Words: Erectile dysfunction; Stem cells; Transplantation
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article History:received 5 April, 2011accepted 21 April, 2011
Corresponding Author:Sae Woong KimDepartment of Urology, Seoul St. Mary’s Hospital, 505, Banpo-dong, Seocho-gu, Seoul 137-701, KoreaTEL: +82-2-2258-6226FAX: +82-2-599-7839E-mail: [email protected]
We acknowledge the financial support of the Healthy Medical Treatment Research and development Program of the Ministry of Health & Welfare (No. A090481) and in part the Catholic Institute of Cell Therapy Basic Science Programs Foundation.
INTRODUCTION
Erectile dysfunction is a common complication after radi-cal prostatectomy. With detailed understanding of the anatomy of the cavernous nerves [1], nerve-sparing proce-dures have been developed [2] and applied to carefully se-lected patients. Nevertheless, considerable numbers of pa-tients who undergo radical prostatectomy become impotent. In one study, among men who were potent at baseline, the
proportion who were impotent 18 or more months after sur-gery was 65.6% of men undergoing non-nerve-sparing pro-cedures, 58.6% of men undergoing unilateral nerve-spar-ing procedures, and 56.0% of men undergoing bilateral nerve-sparing procedures [3]. Recovery of erectile dysfunc-tion is slow, usually taking months to years, and even if the nerve-sparing procedure is done by experienced hands, one third of patients need the aid of medications such as phos-phodiesterase inhibitors [4].

Korean J Urol 2011;52:359-363
360 Woo et al
Cell transplantation and tissue engineering is an emerg-ing field of science. In the field of urology, attempts have been made to engineer urological tissues, including the urethra [5], bladder [6,7], and ureter [8]. These studies used autologous organ-specific cells to regenerate correspon-ding organs, but the use of such cells required a lot of time and material for cell proliferation; also, such cells could not be used in malignant conditions [9]. For these reasons, stem cells have emerged as the current trend in the study of cell transplantation and tissue engineering during the past decade. Muscle-derived stem cells (MDSCs) are adult stem cells located in muscles that are known to not only pro-liferate into muscle cells but also differentiate into various other tissues such as bone, cartilage, and fat [10]. Previously, umbilical cord blood mesenchymal stem cells were used in a rat model of cavernous nerve injury and showed improved erectile function [11]. In this study, we transplanted MDSCs in a rat model of cavernous nerve injury to study the effect on erectile function and also looked at the survival rate of MDSCs through immunohistochemical staining.
MATERIALS AND METHODS
1. Experimental animalsThe Institutional Animal Care and Use Committee of the School of Medicine, the Catholic University of Korea, ap-proved the experimental protocol. Sixteen-week-old adult white rats (Saemtaco Bio Inc., Osan, Korea) weighing about 300 to 350 g were used. Experimental groups were divided into 3: a control group (n=5, group I), a bilateral cavernous nerve injury group (n=5, group II), and a bilateral cav-ernous nerve injury group with MDSC injection (1x106 cells in 20 μl; n=5, group III).
2. Purification and proliferation of MDSCsMDSCs were harvested from the femoral muscles of white rats by use of a modified preplate technique as previously described [12,13]. First, muscle tissue was extracted from the femoral muscle of the white rat and was minced into a coarse slurry with razor blades. Cells were enzymatically dissociated by the addition of collagenase-type XI 0.2% for 1 hour at 37.1oC, dispase (grade II 240 unit) for 45 minutes, and trypsin 0.1% for 30 minutes. The dissociated cells were preplated on a collagen-coated flask for 1 hour and this flask was termed pp1. The nonadhering cells were then transferred to another collagen-coated flask for 2 hours to obtain pp2 and this procedure was repeated at 24-hour in-tervals until pp4. The pp4 population was used for this experiment. The proliferation medium was Dulbecco’s modified Eagle’s medium with 10% fetal bovine serum, 10% horse serum, 0.5% chick embryo extract, and 1% pen-icillin/streptomycin. Proliferation was done for 4 days. All culture media and other supplies were purchased from Gibco Laboratories (Grand Island, NY, USA).
3. Cavernous nerve transection and transplantation of MDSCs
Tiletamine 0.2 ml was administered intraperitoneally for anesthesia. A low-midline abdominal incision was made, exposing the bladder and prostate. The pelvic ganglion was identified at the area lateral to the prostate on both sides. From the pelvic ganglion, cavernous nerves were identified to travel post-laterally into the corpus cavernosum. Group I rats were closed without nerve injury. In group II rats, the cavernous nerves were transected 2 to 3 mm distal to the pelvic ganglion and the wound was sutured. In group III rats, the cavernous nerves were transected and MDSCs (1x106 cells in 20 μl) labeled with PKH-26 fluorescent cell linker (Sigma, St. Louis, MO, USA) were injected into the corpus cavernosum and the wound was then sutured.
4. Measurement of peak intracavernosal pressure and drop rate
After 4 weeks, peak intracavernosal pressure (ICP) and the drop rate were measured for all rats. Tiletamine 0.2 ml was administered intraperitoneally for anesthesia. A low-mid-line abdominal incision was made and the pelvic ganglion and cavernous nerve were exposed on both sides. The penis was also opened and the corpus cavernosum was exposed. A 23 G needle connected to a polyethylene tube was in-serted into the corpus cavernosum to measure peak ICP and the drop rate. Papaverine (5 mg/kg) was injected into the corpus cavernosum to induce erection.
5. HistologyAfter measurement of peak ICP and the drop rate, the pe-nises were removed and the rats were sacrificed with intra-venous sodium pentobarbital (100 mg/kg). The tissue specimens were fixed in 4% paraformaldehyde solution at 4oC for one day. The next day, the specimens were serially transferred into 10%, 20%, and 30% sucrose that was dis-solved in 0.1 M phosphate buffer (PB), and at each stage, they were left to sink down completely. They were then em-bedded in optimal cutting temperature (OCT) compound (Tissue-Tek, Miles Laboratory, Elkhart, IN, USA) in liquid nitrogen at −80oC and sectioned at 10 μm on a cryostat (Microm, Walldorf, Germany). Sections were mounted on gelatin-coated slides and the slides were stained for hema-toxylin and eosin. To identify PKH-26-labeled MDSCs, DAPI staining was done to group III and the cells were ob-served under a fluorescent microscope.
6. Analysis of cyclic guanosine monophosphateMeasurement of the cyclic guanosine monophosphate (cGMP) level was performed by the use of a commercially available radioimmunoassay kit, the cGMP [125I] assay kit (Amersham International, Amersham, UK). The princi-ples of the current experiment were to induce competitive bonding between 125I-labeled cGMP, which is present at a certain amount in the cells, and intracellular cGMP, to measure the amount of isotopes of 125I-labeled cGMP, and thereby to quantify the level of cGMP that is present in the

Korean J Urol 2011;52:359-363
MDSCs for Erectile Dysfunction in Cavernous Nerve Injury 361
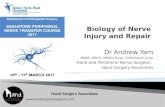
FIG. 1. Measurement of erectile function by Papaverine injection.Peak intracavernous pressure (ICP) was higher in group III thanin group II. Also, the drop rate was lower in group III than in groupII. a: p<0.05.
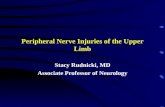
FIG. 2. H&E staining and DAPI staining of group III at week 4. (A) H&E staining. (B) DAPI staining. PKH-26 labeled muscle-derivedstem cells (MDSCs) were identified in DAPI staining of the cavernosum of group III rats. Red spots: PKH-26.
FIG. 3. cGMP expression of group III was higher than that of groupII. a: p<0.05.
sample. Following the preliminary experiment, the level of cGMP was lower in the cells and tissue forming the cor-pus cavernosum. An analysis was therefore performed by using an acetylation assay. Dried cytoplasmic extracts were dissolved by using assay buffer contained in a kit, to which acetylation reagent, antiserum, and [125I]cGMP were added in a sequential manner. Following this, the reaction was performed in compliance with the kit protocol. Eventually, with the use of a gamma scintillation counter, the radioactivity (cpm/min) of each tube was measured. The level of cGMP of each sample was calculated by use of a standard curve.
7. Statistical analysisAll data are presented as means±standard deviations, and p-values<0.05 are reported as significant. Comparisons between groups were performed by using Sigmastat for Windows (Systat Inc., Chicago, IL, USA). The Mann-Whitney test was used to compare results.
RESULTS
1. Change in erectile functionAt 4 weeks, after papaverine injection to induce erection, the peak ICP of group I (control group) was 120±12.8 mmHg, that of group II (bilateral cavernous nerve injury group) was 52±8.7 mmHg, and that of group III [bilateral caver-nous nerve injury group with MDSCs (1x106 cells in 20 ml) injection] was 97±15.6 mmHg. The drop rate of group I was 10±4.1 mmHg/min, that of group II was 34±6.5 mmHg/min, and that of group III was 17±4.9 mmHg/min. The peak ICP and drop rate were significantly higher in group III than in group II (p<0.05) (Fig. 1).
2. Survival of MDSCsPHK-26 labeled MDSCs were identified by DAPI staining of the cavernosum of group III rats (Fig. 2).
3. Expression of cGMPThe expression of cGMP was significantly lower in group II (21.9±5.8 fmol/well) than in group I and group III (70.2± 10.3 and 58.9±10.5 fmol/well, respectively) (Fig. 3).

Korean J Urol 2011;52:359-363
362 Woo et al
DISCUSSION
Radical prostatectomy is the mainstay of treatment for lo-calized prostate cancer. The number of prostatectomies performed in Korea is increasing as a result of prostate-spe-cific antigen (PSA) screening and a younger age at diagnosis of prostate cancer [14]. Advances in surgical techniques and scientific technology have led to the advent of laparo-scopic or robotic radical prostatectomy, but despite these developments, erectile dysfunction is still a major compli-cation after radical prostatectomy and it compromises the quality of life of many patients undergoing this procedure [15,16]. The primary cause of erectile dysfunction after rad-ical prostatectomy is injury to the cavernous nerves. The injury leads to a decrease in elastic and smooth muscle fi-bers and a progressive increase in collagen fibers [17], re-sulting in fibrosis of the corpus cavernosum. Nerve-sparing procedures have been proven to be beneficial to sexual func-tion after radical prostatectomy [18-20], but not all pa-tients become potent and many patients depend on phos-phodiesterase-5 inhibitors for satisfactory erection [4]. In this study, MDSCs were injected into a rat model of transected cavernous nerves to investigate the effect on erectile function after cavernous nerve injury. MDSCs are adult stem cells found in muscle tissues. They are free from the ethical problems frequently encountered in the use of embryonic stem cells [21], adequate amounts are easily ob-tained from autologous muscle biopsies in a short period of time, and they pose lower immunogenic and carcinogenic risks than do embryonic stem cells. These qualities make MDSCs a good material for recent studies involving cell transplantation and tissue engineering. In this study, 4 weeks after injecting MDSCs into the cor-pus cavernosum of bilateral cavernous nerve injury rats, we observed a stable survival rate of MDSCs by immuno-staining. In the functional study, the group with bilateral cavernous nerve injury with MDSCs injection showed im-proved erectile function, as peak ICP was significantly higher and the drop rate was lower compared with the bi-lateral cavernous nerve injury group. Also, the increased cGMP expression of group III suggested that MDSCs pro-tected the penile nerve or muscle from atrophy after cav-ernous nerve transection. It is postulated that the MDSCs converted into muscle cells or neuronal cells, thereby re-versing or preventing the fibrotic effect of the cavernous nerve transection seen in the bilateral cavernous nerve in-jury group. It is these muscle cells that are thought to be involved in improving the erectile function. In a similar study, Kim et al injected skeletal-muscle derived cells (MDCs) into the corpora cavernosa of bilateral cavernous nerve injury rats [22]. Maximal ICP was significantly high-er in the MDC injection group than in the sham injection group. This study further demonstrated nerve fiber re-generation in the MDC injection group by staining for neu-ronal marker. The investigators postulated that either the MDCs protected the penile nerve from atrophy after cav-ernous nerve transection or the MDCs differentiated into
a neuronal phenotype. Growth factors may also have a role in improving erectile function after MDSC injection. There are several reports of improved erectile function after growth factor therapy. Chen et al reported an erectile recovery effect of brain-de-rived neurotrophic factor and vascular endothelial growth factor in a rat model of bilateral cavernous nerve injury, and Fandel et al reported similar results with intracaver-nosal growth differentiation factor-5 [23,24]. These types of growth factors are thought to improve erectile function by regenerating injured nerve fibers. Stem cell injection may facilitate the activities of these growth factors. Bochinski et al showed improved erectile function in a rat model of cavernosal nerve injury after intracavernosally injecting embryonic stem cells that had differentiated along the neural cell line [25]. One of the mechanisms they postulated was that embryonic stem cells acted by produc-ing growth factors. One of the drawbacks of this study, as in other studies using MDSCs, is the need for a longer period of observation and ways to prolong the functional effect of MDSCs. Nolazco et al compared the stimulatory effect of MDSCs at week 2 and week 4 and showed that erectile function was higher at week 2, suggesting that new research is warranted to im-prove the survival of MDSCs and prolong the salutary func-tional effects for at least 3 to 6 months [26]. This means that a stable marker to detect donor cells for a long period would be required, rather than the short-lived fluorescent mark-ers currently being used. Another drawback is that we need further study of the results of the differentiated cells from MDSCs in corpus cavernosum, even though we demon-strated improvement in erectile function. Future studies in stem cell therapy would involve combi-nation with other treatment modalities. Currently, phos-phodiesterase-5 inhibitors are one of the main medical treatments of erectile dysfunction after radical prostatec-tomy. Combining stem cell therapy with medical therapy could produce a synergistic effect and warrants further study. In addition, combination with gene therapy is al-ready producing promising results. Bivalacqua et al dem-onstrated improved age-related erectile dysfunction with the use of mesenchymal stem cells in which gene expression was modified by endothelial nitric oxide synthase [27]. Other applications of gene transfer in stem cell therapy may include transcription of growth factors for nerve re-generation or modifying the differentiation capacity of stem cells to the experimenters’ desire.
CONCLUSIONS
MDSCs can improve erectile function in a cavernous nerve injury rat model. Erectile dysfunction resulting from radi-cal prostatectomy may be treated with intracavernosal in-jection of MDSCs.
Conflicts of InterestThe authors have nothing to disclose.

Korean J Urol 2011;52:359-363
MDSCs for Erectile Dysfunction in Cavernous Nerve Injury 363
REFERENCES
1. Lepor H, Gregerman M, Crosby R, Mostofi FK, Walsh PC. Precise localization of the autonomic nerves from the pelvic plexus to the corpora cavernosa: a detailed anatomical study of the adult male pelvis. J Urol 1985;133:207-12.
2. Walsh PC. Radical retropubic prostatectomy with reduced mor-bidity: an anatomic approach. NCI Monogr 1988;7:133-7.
3. Stanford JL, Feng Z, Hamilton AS, Gilliland FD, Stephenson RA, Eley JW, et al. Urinary and sexual function after radical prosta-tectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA 2000;283:354-60.
4. Walsh PC, Marschke P, Ricker D, Burnett AL. Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. Urology 2000;55:58-61.
5. Bach AD, Bannasch H, Galla TJ, Bittner KM, Stark GB. Fibrin glue as matrix for cultured autologous urothelial cells in urethral reconstruction. Tissue Eng 2001;7:45-53.
6. Oberpenning F, Meng J, Yoo JJ, Atala A. De novo reconstitution of a functional mammalian urinary bladder by tissue engineering. Nat Biotechnol 1999;17:149-55.
7. Fraser M, Thomas DF, Pitt E, Harnden P, Trejdosiewicz LK, Southgate J. A surgical model of composite cystoplasty with cul-tured urothelial cells: a controlled study of gross outcome and ur-othelial phenotype. BJU Int 2004;93:609-16.
8. Matsunuma H, Kagami H, Narita Y, Hata K, Ono Y, Ohshima S, et al. Constructing a tissue-engineered ureter using a decellular-ized matrix with cultured uroepithelial cells and bone marrow- derived mononuclear cells. Tissue Eng 2006;12:509-18.
9. Becker C, Jakse G. Stem cells for regeneration of urological struc-tures. Eur Urol 2007;51:1217-28.
10. Cao B, Huard J. Muscle-derived stem cells. Cell Cycle 2004;3:104-7.11. Choi A, Kim SD, Sohn DW, Kim DB, Kim HW, Cho SY, et al. The
effect of human umbilical cord blood derived mesenchymal stem cell therapy in rat model of cavernosal nerve injury. Korean J Androl 2008;26:136-41.
12. Qu Z, Balkir L, van Deutekom JC, Robbins PD, Pruchnic R, Huard J. Development of approaches to improve cell survival in myoblast transfer therapy. J Cell Biol 1998;142:1257-67.
13. Lee JY, Paik SY, Yuk SH, Lee JH, Ghil SH, Lee SS. The isolation and characterization of muscle derived stem cells from gastro-cnemius muscle of rats using the modified preplate method. Korean J Urol 2004;45:1279-84.
14. Yoo SH, Kim SJ, Shin KY, Choi DY, Park HY, Lee TY, et al. Comparative study on diagnostic value of digital rectal examina-tion, serum prostate specific antigen and transrectal ultrasound
in prostate cancer. Korean J Urol 1997;38:1325-32.15. Talcott JA, Rieker P, Propert KJ, Clark JA, Wishnow KI, Loughlin
KR, et al. Patient-reported impotence and incontinence after nerve-sparing radical prostatectomy. J Natl Cancer Inst 1997;89: 1117-23.
16. Choe JH, Choi YS, Choi HJ, Choi HY, Lee SW. Quality of life and sexual outcomes: radical prostatectomy and external beam radia-tion therapy for prostate cancer. Korean J Urol 2005;46:962-9.
17. Iacono F, Giannella R, Somma P, Manno G, Fusco F, Mirone V. Histological alterations in cavernous tissue after radical prosta-tectomy. J Urol 2005;173:1673-6.
18. Quinlan DM, Epstein JI, Carter BS, Walsh PC. Sexual function following radical prostatectomy: influence of preservation of neu-rovascular bundles. J Urol 1991;145:998-1002.
19. Ayyathurai R, Manoharan M, Nieder AM, Kava B, Soloway MS. Factors affecting erectile function after radical retropubic prosta-tectomy: results from 1620 consecutive patients. BJU Int 2008; 101:833-6.
20. Noldus J, Michl U, Graefen M, Haese A, Hammerer P, Huland H. Patient-reported sexual function after nerve-sparing radical retropubic prostatectomy. Eur Urol 2002;42:118-24.
21. Peault B, Tavian M. Hematopoietic stem cell emergence in the hu-man embryo and fetus. Ann N Y Acad Sci 2003;996:132-40.
22. Kim Y, de Miguel F, Usiene I, Kwon D, Yoshimura N, Huard J, et al. Injection of skeletal muscle-derived cells into the penis im-proves erectile function. Int J Impot Res 2006;18:329-34.
23. Chen KC, Minor TX, Rahman NU, Ho HC, Nunes L, Lue TF. The additive erectile recovery effect of brain-derived neurotrophic fac-tor combined with vascular endothelial growth factor in a rat mod-el of neurogenic impotence. BJU Int 2005;95:1077-80.
24. Fandel TM, Bella AJ, Tantiwongse K, Garcia M, Nunes L, Thüroff JW, et al. The effect of intracavernosal growth differentiation fac-tor-5 therapy in a rat model of cavernosal nerve injury. BJU Int 2006;98:632-6.
25. Bochinski D, Lin GT, Nunes L, Carrion R, Rahman N, Lin CS, et al. The effect of neural embryonic stem cell therapy in a rat model of cavernosal nerve injury. BJU Int 2004;94:904-9.
26. Nolazco G, Kovanecz I, Vernet D, Gelfand RA, Tsao J, Ferrini MG, et al. Effect of muscle-derived stem cells on the restoration of cor-pora cavernosa smooth muscle and erectile function in the aged rat. BJU Int 2008;101:1156-64.
27. Bivalacqua TJ, Deng W, Kendirci M, Usta MF, Robinson C, Taylor BK, et al. Mesenchymal stem cells alone or ex vivo gene modified with endothelial nitric oxide synthase reverse age-associated erectile dysfunction. Am J Physiol Heart Circ Physiol 2007;292: H1278-90.