Nerve injury and repair
44
Presented By: Dr Akasha Amber Plastic surgery resident (1 st year) BVH BWP
-
Upload
surgeon-awan -
Category
Health & Medicine
-
view
2.163 -
download
2
Transcript of Nerve injury and repair

Presented By:
Dr Akasha Amber
Plastic surgery resident (1st year)BVH BWP

Principals & Techniques Of
Peripheral Nerve Repair


mesoneuriumFascicles of nerve fibers
perineurium
epineurium
endoneurium


Physiology


Nerve Injury Focal contusion (gunshot wounds) Stretch/traction injury Drug injection injury Compression Crush injuries Avulsion Laceration Electrical burns Idiopathic Others(Viral infections, metabolic and neural disorders)

Nerve Regeneration
Changes at proximal and distal site of injury

Classification Of Nerve Injuries
Seddon, Sunderland and lately by Mackinnon 6 degrees

Degrees Of Nerve Injury
1st degree of injury(neuraparaxia)› Segmental demylination› Axons intact› Recovery in 12 to 16 wks
2nd degree injury(axonotmesis)› Axonal injury/ distal wallerian degeneration› Regeneration at rate of 1 inch per month› Complete slow recovery

Degrees Of Nerve Injury
3rd degree injury› Axonal injury & fibrosis of endoneurium› Incomplete recovery
4th degree injury› Axonal injury› Damage to endo and perineurium with dense
scarring› Needs surgical intervention

Degrees Of Nerve Injury
5th degree injury(neurotmesis)› Complete nerve division
6th degree injury› Variable combination of previous five
degrees of nerve injury


normal
1st degree injury
2nd degree injury
3rd degree injury
4th degree injury
6th degree injury

Diagnosis
Motor function
› Movements, muscle atrophy
sensory function
› Tinel sign, Ten test
› Two point discrimination
› Touch, vibration
•History•Examination

Tinel Sign
Tinel sign: -› peripheral tingling or dysaesthesia'
provoked by percussion of the nerve› Positive in axonal injuries

Electrical Stimulation Tests:
EMG NCS Intra operative nerve action potential
Principals Of Nerve Repair
Microsurgical techniques› Adequate magnification› Microsurgical instruments & sutures
Different techniques:› Primary nerve repair› Nerve grafting› Nerve transfer› Nerve conduits› Nerve allografts

Timing Of The Nerve Repair
Sharply transected nerves› Immediate repair
Crushed, avulsed, blast injuries› Nerve ends tacked together› Repair delayed for 3 weeks or until wound bed permits
Re-exploration Neuroma excision, nerve grafts Acute nerve grafting in the 1st sitting Bleeding control ,trimming of fascicles ,loose epineural suturing
Closed injuries treated expectantly for 12 weeks


Primary Nerve Repair
Primary repair› Tension free repair› Mobilization of nerve ends› Discourage
Facilitation by postural position Extreme range of joint movements

Primary Nerve Repair
Primary nerve repair› Epineural repair› Grouped fascicular repair

Epineural Repair
Standard repair

Fascicular Repair
Restore the continuity of fascicles Internal topography Intra-operative nerve stimulation Neurolysis with the eyes Priority to the motor recovery(radial and
peroneal nerve)


e.g. Ulnar Nerve Fascicular Components

Nerve Grafts
Tension at site of repair Need of postural positioning Alignment of sensory & motor components Maximize number of axons Reversal of graft Exclusion of expendable nerve

Options For Nerve Grafts
Sural nerve› 30-40cm› Lateral peroneal communicating br : 10-20cm
Lateral antebrachial cutaneous nerve(LABC)› 8cm
Medial antebrachial cutaneous nerve (MABC)› Anterior & posterior division› 20 cm
Expendable nerves(peroneal and radial) Sensory branches of ulnar and median nerves Distal anterior interosseous nerve and so on…

Disadvantages
Donor site scarring Donor site sensory loss
› Patient education
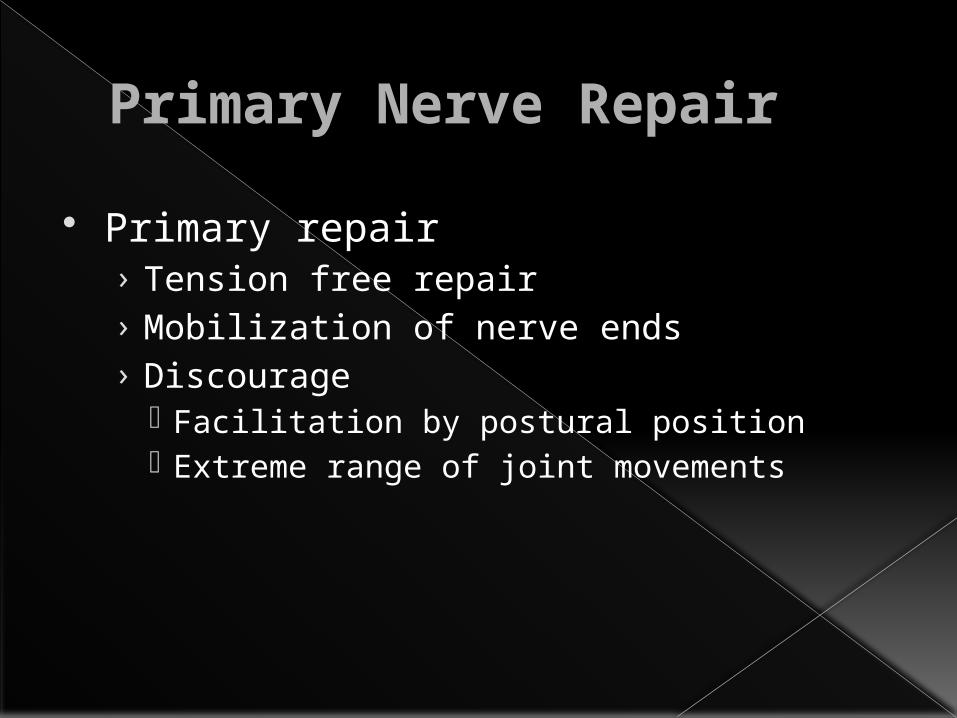
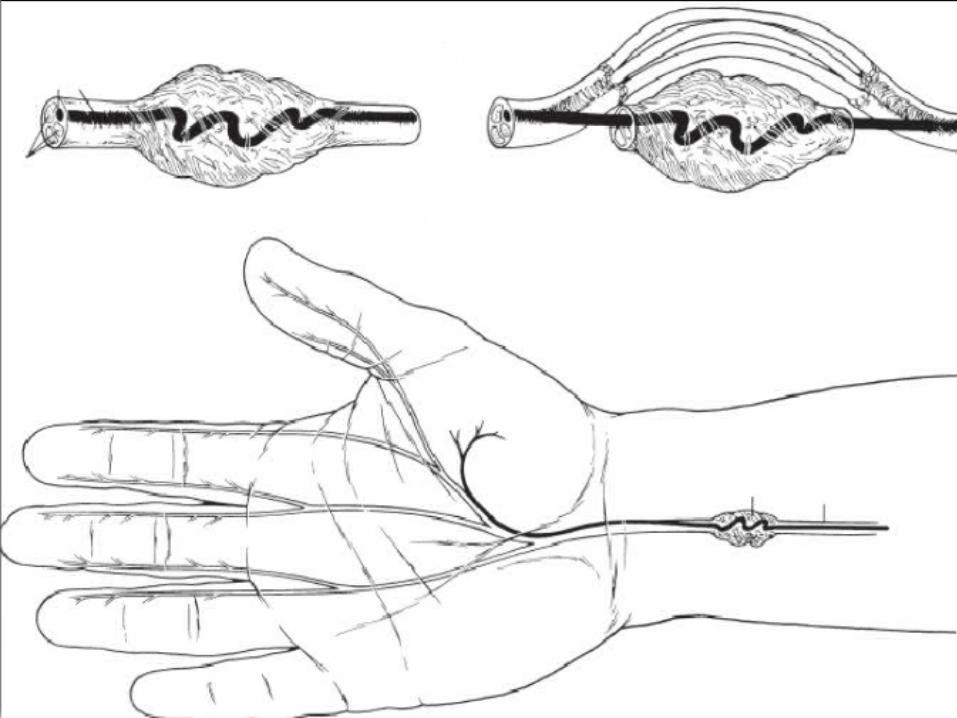
Neuroma In Continuity
Complete : resection and repair with graft


Neuroma In Continuity
Incomplete neuroma Intra-operative nerve stimulation Black boxing around neuroma

Nerve Transfer
Indications:› Very proximal peripheral nerve injuries› Root avulsions› Excessive scarring› Level of injury unclear
Idiopathic neuritides Radiation induced nerve injury

Nerve Transfer
Motor nerve transfer› Pure motor axons› Close proximity› expendable› Synergistic supply
Sensory nerve transfer› pure sensory axons› Innervates non critical area› Expendable and lying in close proximity

Most Common Uses Of Nerve Transfer
elbow flexion Shoulder abduction Ulnar-innervated intrinsic hand function Forearm pronation Radial nerve function

Transfer of radial nerve to axillary nerve

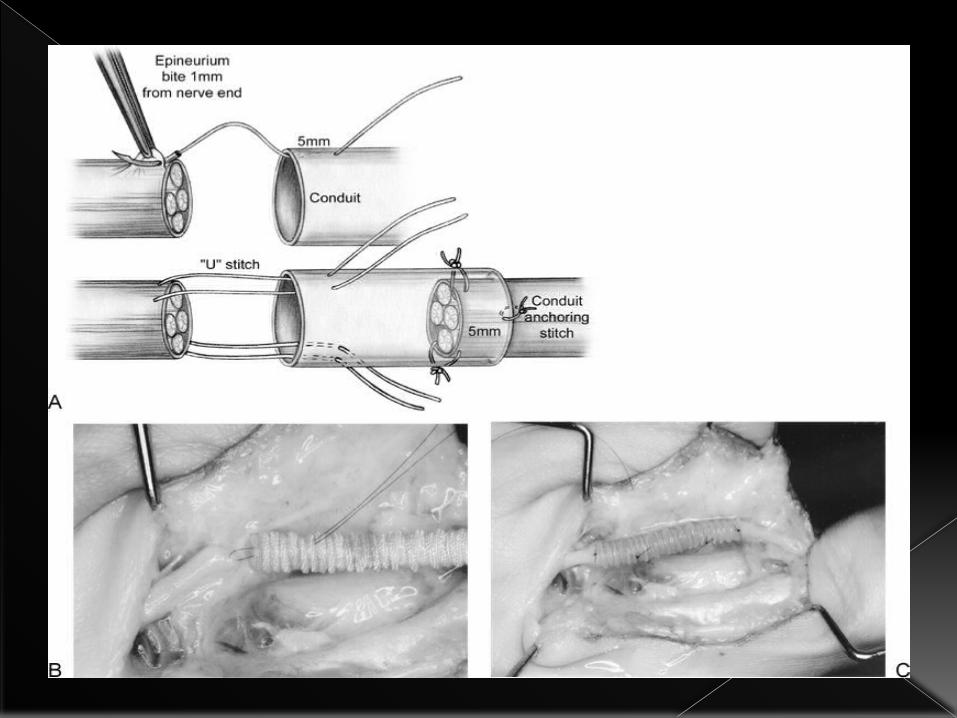
Nerve Conduits
Veins, pseudo-sheaths, bioabsorbable tubes short nerve gaps ≤ 3cm Low antigenicity , biodegradability Trials to add a nerve graft inside the conduit
› neurotrophic factors

Nerve Allografts
Extensive injuries Limited donor material Immunosuppressive agents
› FK506( tacrolimus )› Prednisone , azathioprine
Processed acellular cadaveric nerve allografts› AxoGen, Inc. ,Alachua, FL.

Thank you