Roslyn Bonar - Royal College of Pathologists of Australasia - Update on POCT in Australia
Upload
informa-australiaCategory
view
51download
0
The Role of External Quality Assurance in Improving
Patient Safety
Tony Badrick

EQA – the more you look the more you see!


Date of download: 10/11/2016Copyright © 2016 American Medical
Association. All rights reserved.
From: Diagnostic Error in MedicineAnalysis of 583 Physician-Reported Errors
Arch Intern Med. 2009;169(20):1881-1887. doi:10.1001/archinternmed.2009.333
Classification of diagnostic errors in 583 physician-reported cases using the Diagnostic Error Evaluation and Research project tool
to localize where in the diagnostic process error occurred.
Figure Legend:

Benefits of EQA participation
• Characterise test bias and imprecision across multiple methods
• Correlate specific method variables with bias and imprecision
• Identify interfering substances and quantify their effects across multiple methods


Benefits of EQA participation
• Provide clinical laboratories with reliable information for replacing unsatisfactory methods
• Identify clinical laboratories that are at risk for poor performance
• Satisfy accreditation and regulatory requirements

Benefits of EQA participation
• For most laboratories, EQA and accreditation represent a miniscule cost compared to total budget, rarely exceeding 0.1%.
• Contribute directly to opportunities for continual improvement and continuing education.

14

Benefits of EQA participation
• Provide an opportunity that integrates with preventive action, and with detection of occurrences that lead to appropriate remedial and corrective actions.
• Provide the opportunity to earn certificates that provide the public with visual thus providing a reasonable basis for public and client confidence.


Position of EQA in the Laboratory
Laboratory Quality Management Systemeg ISO 15189
Quality Policy
Quality Assurance
Quality Control
Internal Quality
Control
External Quality
Assurance
Other aspects of good
laboratory practice
All measures taken to assure quality

•Sturgeon C. Best Pract & Res Clin Endo & Metab 2013; 27: 802-822

Laboratory Method Standardisation
Refe
rence m
ate
rials
Refe
rence L
abora
torie
s
Re
fere
nce
Me
tho
ds
Tra
ceable
refe
rence In
terv
als
Exte
rnal Q
uality
Assura
nce

Key Requirements of an EQA
• Specimen distribution frequency and reporting requirements
• Specimen material distributed
• Definition of target values
• Assessment of overall performance
• Assessment of individual method performance

Key Requirements of an EQA
• Assessment of method robustness to clinically relevant interference
• Assessment of individual laboratory performance
• Communication with participating laboratories
• Audit of wider aspects of analytical performance and educational activities

EQA driving Improvement
Improvements in performance in medical diagnostics
tests documented by inter-laboratory comparison
programsTholen DW (2002) Accreditation and Quality Assurance Vol 7, Issue 4:146-152
A survey of clinical genetic laboratories in the United
States indicated that increased participation in PT
correlated directly with fewer PT failures and fewer
incorrect patient test reportsHudson KL, Murphy JA, Kaufman DJ et al (2006) Oversight of US genetic testing laboratories
Nat Biotechnol. 24(9):1083–1090.
There is evidence that EQA failure rates decrease with
increased experience performing EQA.

EQA driving Improvement
Failures in the EQA program over the last five years have helped us to
significantly improve our transfusion service in terms of performance
evaluation, patient care and safety issues, and the overall quality of
laboratory practices.Chaudary R, Das SS. Ojha S, Khetan D, and Sonker A (2010) The external quality assessment
scheme: Five years experience as a participating laboratory. Asian J Transfus Sci. 4(1): 28–30.
External quality assessment (EQA) has been shown to improve laboratory
performance and diagnosis in haemostasis. We report here findings from
the World Federation of Haemophilia EQA programme during the
period 2004–2007.Jennings I, Kitchen DP, Woods TAL, et al (2009) Haemophilia Volume 15, Issue 2:571–577
External quality assessment schemes raise standards: evidence from the
UKNEQAS parasitology subschemesKettlehut MM, Chiodini PL, Edwards H and Moody A (2003) J Clin Pathol 2003;56:927-932
doi:10.1136/jcp.56.12.927
EQA driving Improvement
Poor PT/EQA performance because of interpretation
errors has decreased between 1997 and 2006. This may
be derived from continued participation in PT/EQA.Ramsden SC, Deans Z, Robinson DO, et al (2006) Monitoring standards for
molecular genetic testing in the United Kingdom, The Netherlands and Ireland.
Genetic Test 10(3):147–156.
90% of the EQA problems were resolved after the first round of EQA and 99% were resolved by the third round, suggesting that the laboratories had successfully corrected mistakes identified by EQA performance.Hoeltge FA, Phillips MG, Styer PE, Mockridge P (2005) Detection and correction of systematic laboratory problems by analysis of clustered proficiency testing failures. Arch Pathol Lab Med.129(2):186–189.

25
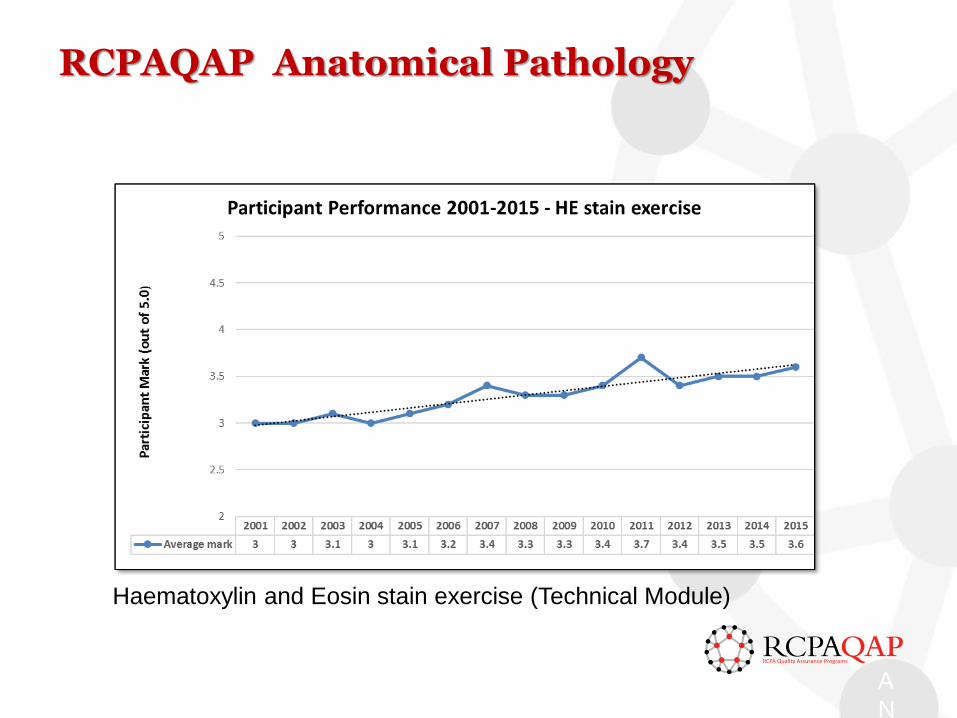
RCPAQAP Anatomical Pathology
26 A
N
A
Haematoxylin and Eosin stain exercise (Technical Module)


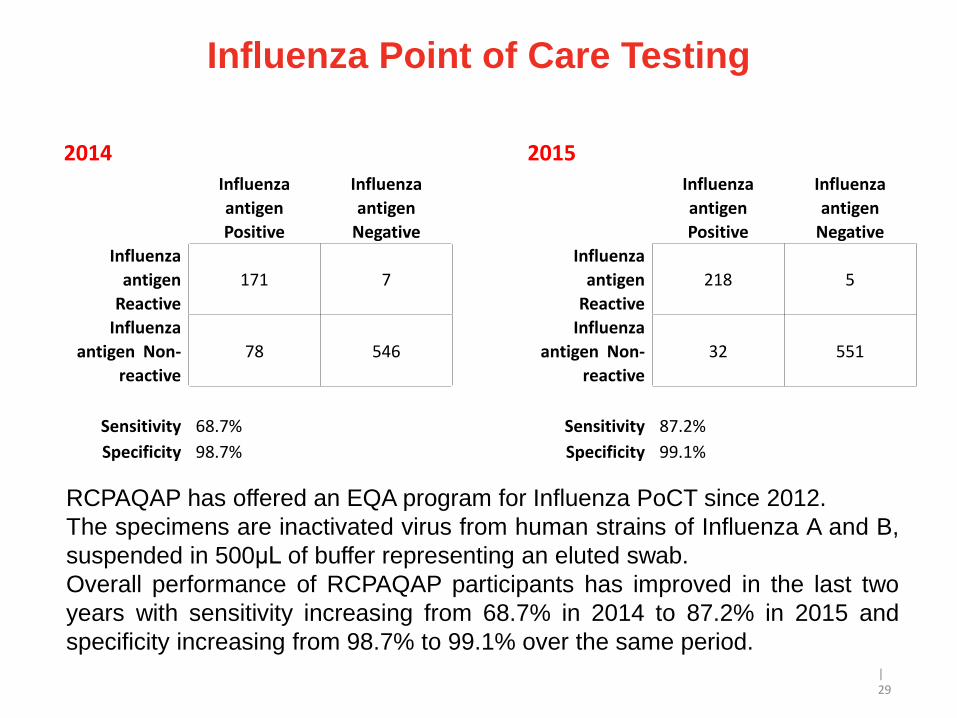
Influenza Point of Care Testing
| 29
2014 2015Influenza
antigen
Positive
Influenza
antigen
Negative
Influenza
antigen
Positive
Influenza
antigen
Negative
Influenza
antigen
Reactive
171 7
Influenza
antigen
Reactive
218 5
Influenza
antigen Non-
reactive
78 546
Influenza
antigen Non-
reactive
32 551
Sensitivity 68.7% Sensitivity 87.2%
Specificity 98.7% Specificity 99.1%
RCPAQAP has offered an EQA program for Influenza PoCT since 2012.
The specimens are inactivated virus from human strains of Influenza A and B,
suspended in 500μL of buffer representing an eluted swab.
Overall performance of RCPAQAP participants has improved in the last two
years with sensitivity increasing from 68.7% in 2014 to 87.2% in 2015 and
specificity increasing from 98.7% to 99.1% over the same period.

Kalra clin biochem 37;1052-62: 2004
32

33

PITUS- Australia
A national project for the Standardisation of Pathology Units and Terminology (PUTS) was initiated by the RCPA in July 2011 with support from Government. Around 80 pathologists, scientists, informaticians, and other clinicians worked in 8 working groups to establish guidelines for the use of terminology and standardised units covering each of the pathology disciplines.
34
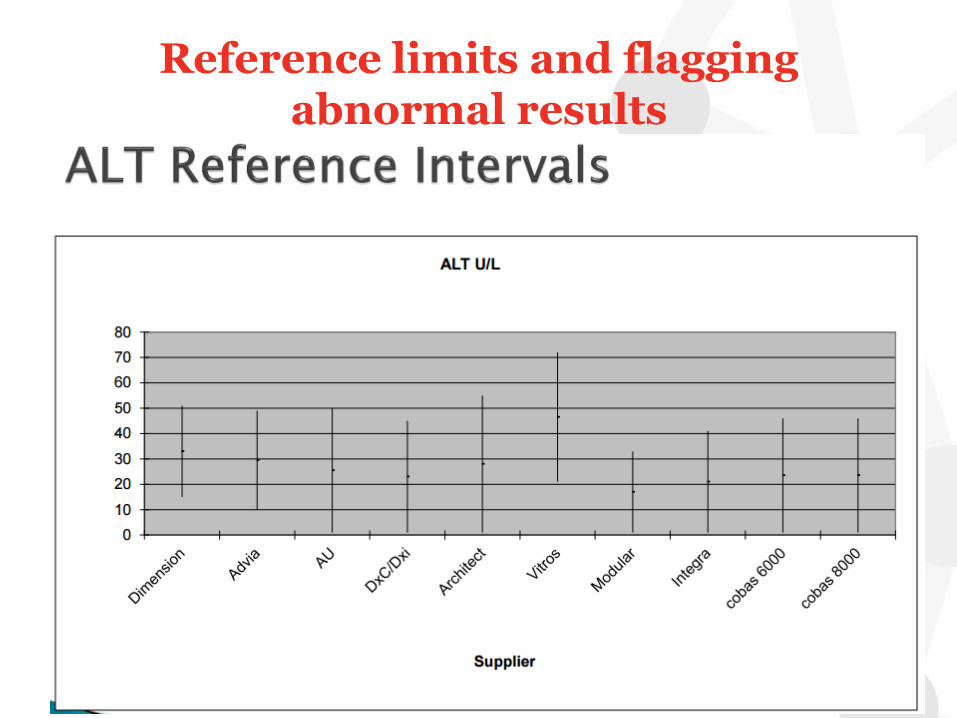
Reference limits and flaggingabnormal results

Date of Birth
15%
48%
5%
32%
0% 10% 20% 30% 40% 50% 60%
dd/mm/yy
dd/mm/yyyy
dd/month/yy
dd/month/yyyy01 April 1980
01 April 80
01/04/1980
01/04/80
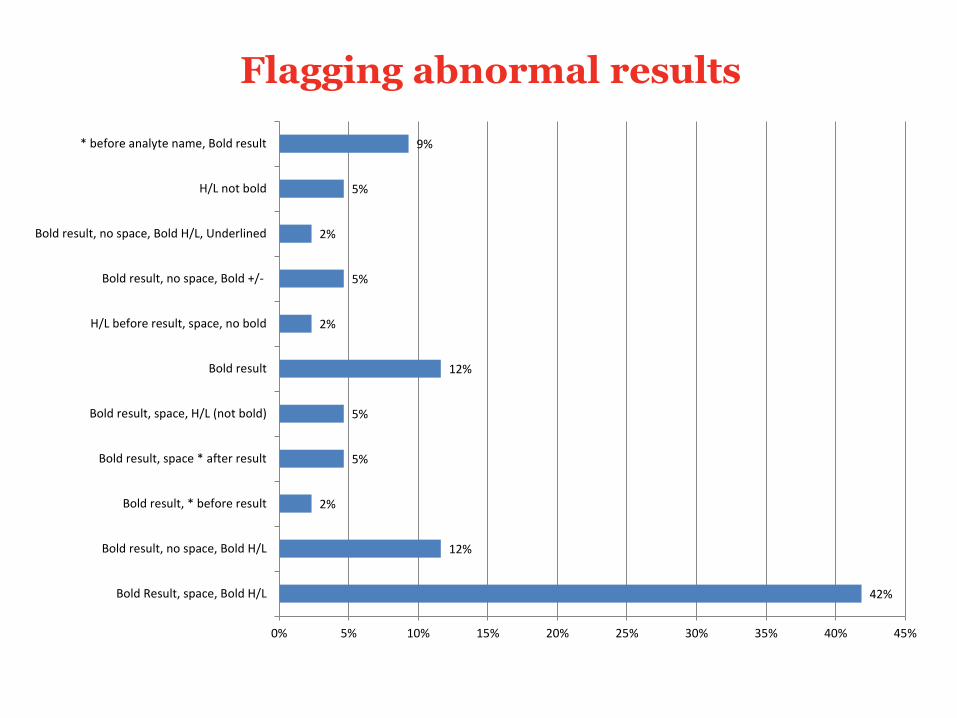
Flagging abnormal results
42%
12%
2%
5%
5%
12%
2%
5%
2%
5%
9%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45%
Bold Result, space, Bold H/L
Bold result, no space, Bold H/L
Bold result, * before result
Bold result, space * after result
Bold result, space, H/L (not bold)
Bold result
H/L before result, space, no bold
Bold result, no space, Bold +/-
Bold result, no space, Bold H/L, Underlined
H/L not bold
* before analyte name, Bold result
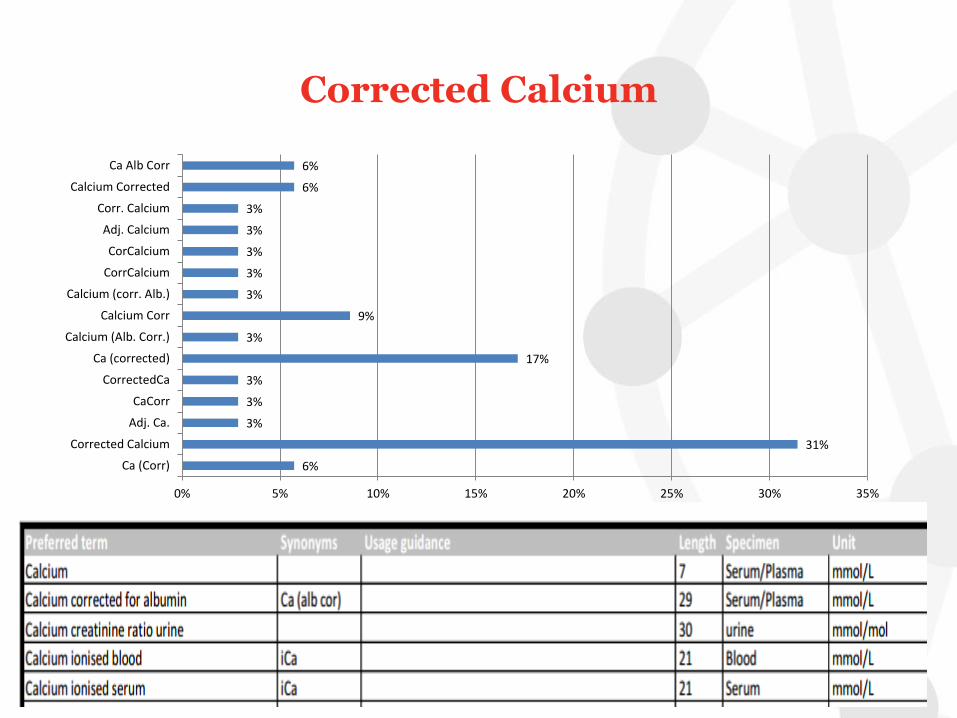
Corrected Calcium
6%
31%
3%
3%
3%
17%
3%
9%
3%
3%
3%
3%
3%
6%
6%
0% 5% 10% 15% 20% 25% 30% 35%
Ca (Corr)
Corrected Calcium
Adj. Ca.
CaCorr
CorrectedCa
Ca (corrected)
Calcium (Alb. Corr.)
Calcium Corr
Calcium (corr. Alb.)
CorrCalcium
CorCalcium
Adj. Calcium
Corr. Calcium
Calcium Corrected
Ca Alb Corr
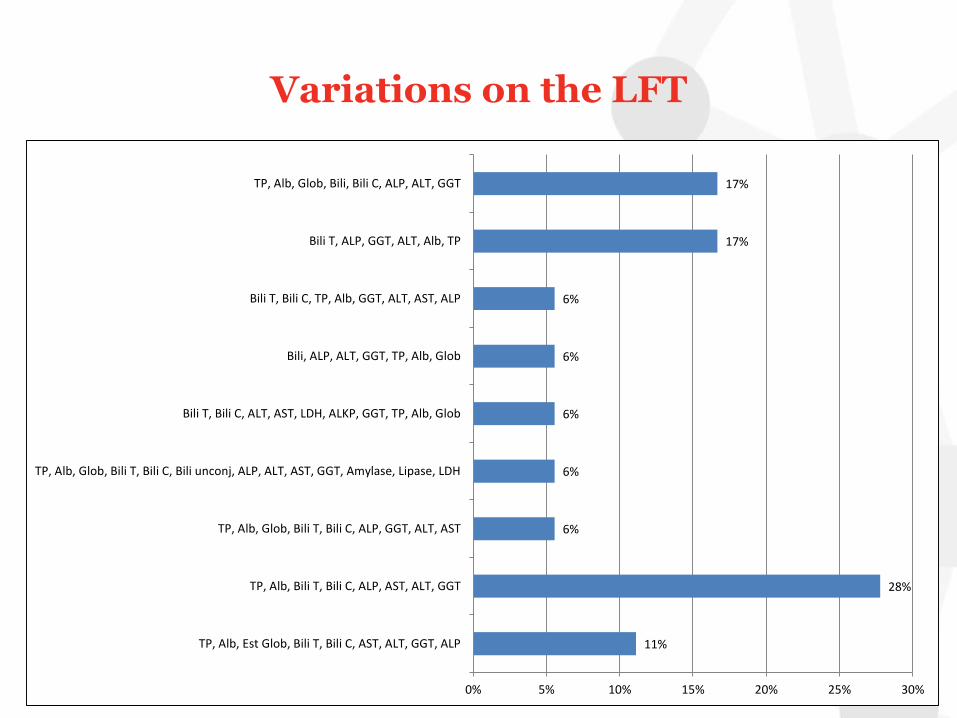
11%
28%
6%
6%
6%
6%
6%
17%
17%
0% 5% 10% 15% 20% 25% 30%
TP, Alb, Est Glob, Bili T, Bili C, AST, ALT, GGT, ALP
TP, Alb, Bili T, Bili C, ALP, AST, ALT, GGT
TP, Alb, Glob, Bili T, Bili C, ALP, GGT, ALT, AST
TP, Alb, Glob, Bili T, Bili C, Bili unconj, ALP, ALT, AST, GGT, Amylase, Lipase, LDH
Bili T, Bili C, ALT, AST, LDH, ALKP, GGT, TP, Alb, Glob
Bili, ALP, ALT, GGT, TP, Alb, Glob
Bili T, Bili C, TP, Alb, GGT, ALT, AST, ALP
Bili T, ALP, GGT, ALT, Alb, TP
TP, Alb, Glob, Bili, Bili C, ALP, ALT, GGT
Variations on the LFT

4%
4%
13%
13%
13%
4%
4%
4%
4%
4%
4%
4%
4%
4%
4%
4%
4%
0% 2% 4% 6% 8% 10% 12% 14%
Chol, Trig, LDL-Chol, HDL-Chol, Total/HDL Ratio
Chol, Trig, HDL Chol, nonHDL chol, LDL Chol, Cholesterol/HDL Ratio
Chol, Trig, HDL Chol, LDL Chol
Chol, Trig, LDL Chol, HDL Chol, Chol/HDL Ratio
Chol, Trig, HDL-C, LDL-C, Ratio,
LDL, Chol/HDL
Chol, Trig, LDL Chol (calc), HDL Chol
Chol, HDL, Trig, LDL, Chol/HDL Ratio, CR Index
Chol, Trig, HDL Chol, LDL (calc)
HDL Chol, Chol, Trig, LDL Chol, Non-HDL Chol
Chol, Trig, HDL Chol, LDL Chol (calc), Non-HDL Chol, Chol/HDL Ratio
LDL Chol, Non HDL Chol, Trig
Chol HDL, Chol LDL, Trig
T Chol , LDL Chol, HDL Chol, Trig
Chol, Trig, HDL, Chol/HDL Ratio, LDL, Non HDLC
Chol, Trig, HDLC, LDL Chol, TC/HDLC, LDL/HDL
Chol, Trig, HDL Chol, Chol/HDL, Non HDL-Chol, LDL Chol
Variations on the lipids
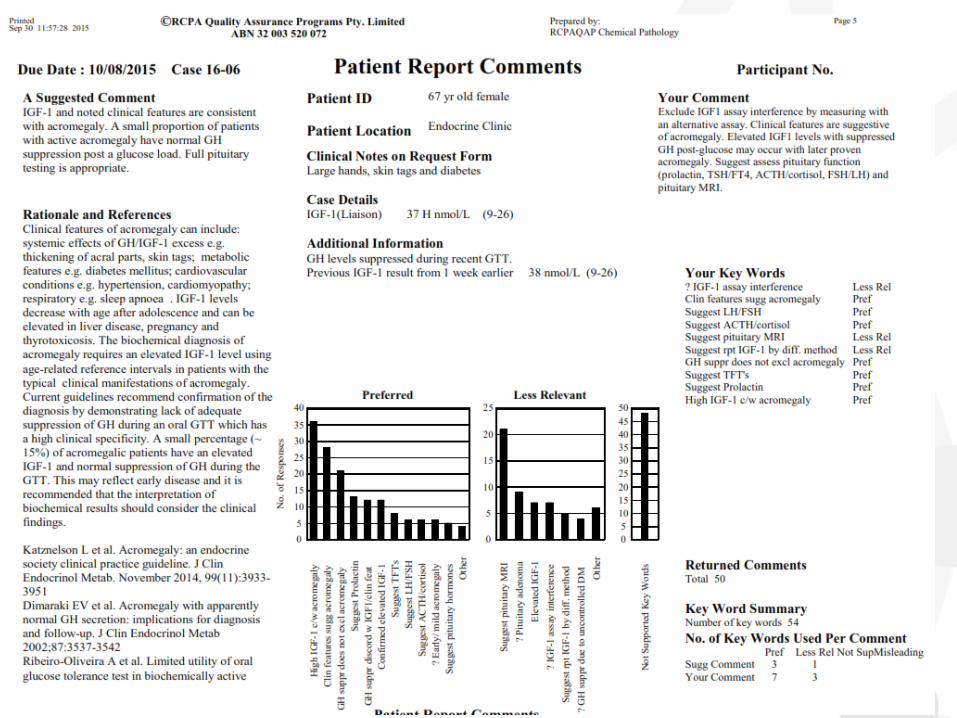
Interpretative Comments
• Commenting on Results of EQA
• Often occurs as part of an normal EQA
– Anatomical Pathology
– Transfusion
– Haematology
• Model for all Reported Comments?
41

Interpretative Comments
The ideal interpretive comment:
(i) describes the abnormalities in the technical
data,
(ii) interprets that information including the
clinical implications such as for diagnosis, and
(iii) provides knowledge for follow-up
including further testing or specialist referral.

Informatics EQA
• EQA is usually an artificial process
– No normal request
– Sample added
– Report not generated
• Should test the entire cycle
– Request
– Result
– Report
44

IT EQA
45

EQA for Referring Doctors

Quality is here to stay
• We need to ensure that EQA is fit for the future
• A systematic approach should be taken to educating, training and developing the skills of the pathology workforce in quality management systems and quality improvement methodology