
Today’s webinar will begin in a few minutes.
35
Today’s webinar will begin in a few minutes. Please press *6 to mute your line or use the “mute” button on your phone. If you have questions for the presenter or need to contact TCPS staff, type your comments into the chat box. Lines will be opened during the call, so attendees may ask questions. Please do not put the conference on hold. Thank you for your patience.
-
Upload
donna-reese -
Category
Documents
-
view
27 -
download
1
description
Today’s webinar will begin in a few minutes. Please press *6 to mute your line or use the “mute” button on your phone. If you have questions for the presenter or need to contact TCPS staff, type your comments into the chat box. - PowerPoint PPT Presentation
Transcript of Today’s webinar will begin in a few minutes.

Today’s webinar will begin in a few minutes.
Please press *6 to mute your line or use the “mute” button on your phone.
If you have questions for the presenter or need to contact TCPS staff, type your comments into the chat box.
Lines will be opened during the call, so attendees may ask questions.
Please do not put the conference on hold.
Thank you for your patience.
Catheter-Associated Urinary Tract Infections (CAUTI)
Tennessee Performance Trends
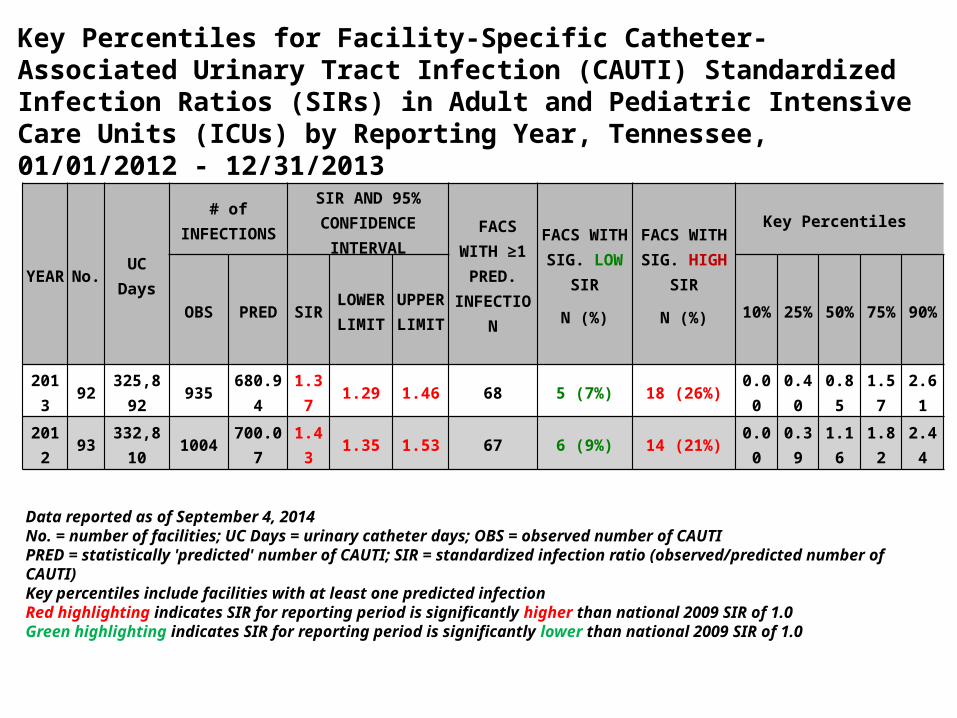
Key Percentiles for Facility-Specific Catheter-Associated Urinary Tract Infection (CAUTI) Standardized Infection Ratios (SIRs) in Adult and Pediatric Intensive Care Units (ICUs) by Reporting Year, Tennessee, 01/01/2012 - 12/31/2013
YEAR No. UC Days
# of INFECTIONS SIR AND 95% CONFIDENCE INTERVAL FACS WITH
≥1 PRED. INFECTION
FACS WITH SIG. LOW SIR
N (%)
FACS WITH SIG. HIGH SIR
N (%)
Key Percentiles
OBS PRED SIR LOWER LIMIT
UPPER LIMIT 10% 25% 50% 75% 90%
2013 92 325,892 935 680.94 1.37 1.29 1.46 68 5 (7%) 18 (26%) 0.00 0.40 0.85 1.57 2.61
2012 93 332,810 1004 700.07 1.43 1.35 1.53 67 6 (9%) 14 (21%) 0.00 0.39 1.16 1.82 2.44
Data reported as of September 4, 2014No. = number of facilities; UC Days = urinary catheter days; OBS = observed number of CAUTIPRED = statistically 'predicted' number of CAUTI; SIR = standardized infection ratio (observed/predicted number of CAUTI)Key percentiles include facilities with at least one predicted infectionRed highlighting indicates SIR for reporting period is significantly higher than national 2009 SIR of 1.0Green highlighting indicates SIR for reporting period is significantly lower than national 2009 SIR of 1.0
CAUTI Performance January – June 2014
• 403 CAUTI events January – June 2014• Of the 18 hospital “outliers” for 2013
– 11 showing some improvement• 4 hospitals showing over 50% reduction
– 3 getting worse – 4 no change in performance
CAUTI Recommendations – Call to Action from Deep Dive Session Fall 2013 with CMO’s
– Focused leadership attention and accountability.– Include CAUTI performance on organizational scorecards and in performance
evaluations of leaders/staff. – Make hospital and unit level data visible to staff and physicians by posting on units.
– Utilize communication strategies such as daily staff huddles, communication boards and bedside shift reports to identify, share and discuss patient safety risks and mitigation plans.
– Define clinical protocols for indications for catheter placement to decrease utilization.
– Develop and utilize nurse-driven protocols for prompt removal of catheters when criteria for use are no longer met.
– Utilize daily multi-disciplinary rounds to assess continued need for any device including urinary catheters.
Tennessee Center for Patient SafetyThe THA Board accepted the recommendations from the THA Quality Committee to address CAUTI performance:
• THA board set a specific goal for a 40 percent reduction in CAUTI within next 12 months (by July 2015)– 371 fewer events July 2014-June 2015 compared to 2013– THA staff focus on outlier hospitals to show clinical and financial
impact of poor performance and provide targeted resources• Hospitals share data on MRSA, C-difficile and healthcare worker
vaccinations with THA to include in TCPS summary reports and hospital scorecards– No new data collection required by hospitals. Hospitals would
confer rights to access in CDC reporting system• THA collect and monitor hospital performance for long-term acute care
(LTAC) and rehabilitation facilities using publicly reported metrics for CAUTI, CLABSI, MRSA, C-difficile and healthcare worker vaccinations

Chris Edwards, MD, FHMChief Medical Officer
Maury Regional Medical Center
Lynnelle Murrell, RN,BSN,CICDirector, Infection Prevention
Maury Regional Medical Center
8
ON THE CUSP:A CAUTI Prevention Project
September 26, 2014
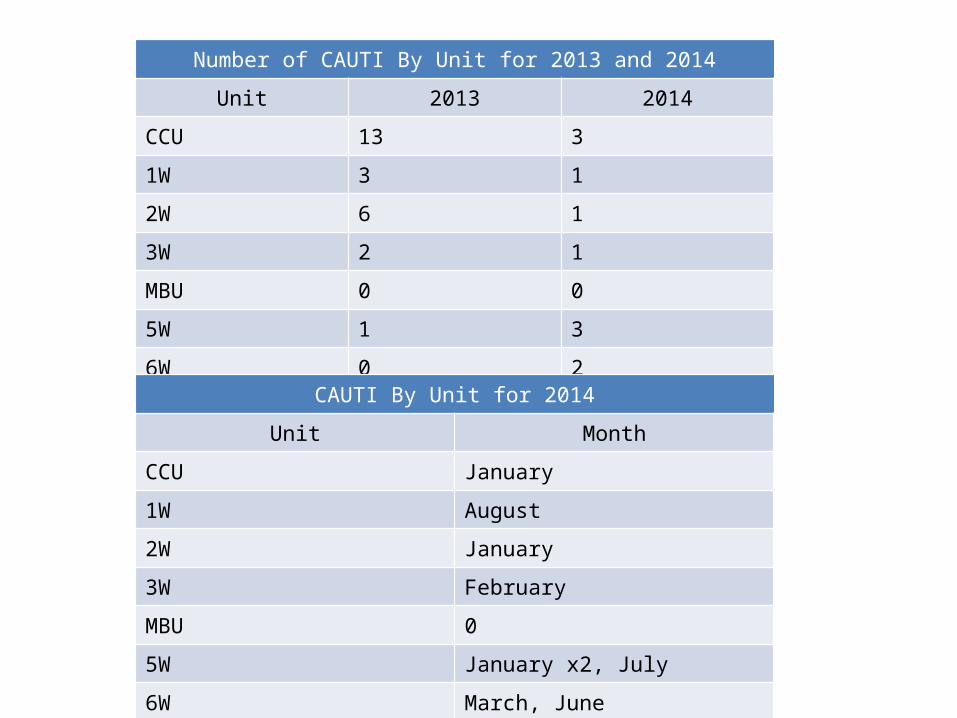
Number of CAUTI By Unit for 2013 and 2014Unit 2013 2014
CCU 13 31W 3 12W 6 13W 2 1MBU 0 05W 1 36W 0 2
CAUTI By Unit for 2014Unit Month
CCU January1W August2W January3W FebruaryMBU 05W January x2, July6W March, June
Project Kickoff
oInvolved the whole facility
oIdentified Champions: multidisciplinary and house wide
oPresented data in a personal form
oDeclared Zero Infections Tolerated
oA culture change regarding how
wethink about urinary catheters
Measureso Science of Safety video mandatory for staffo Added Patient Safety Rounding for inpatient and
outpatient areas ando Daily Multidisciplinary Rounds
– Included how many patients have urinary catheters
– What is the plan for removal?– Do you feel comfortable using the nurse
driven protocol for removal?

Policy Changes
o Added observer when inserting UCo Implemented Nurse Driven Removal Protocol
• Tightened the indications for insertion, maintenance,and removal to mirror the 2009 HICPAC guidelines
• Updated GU Shift assessment to include a hard stop where staff would assess whether UC still appropriate
o With rounding learned some staff were not comfortable using protocol for removal without physician’s order• have to keep checking back with, educating staff
Measures
o Maintenance Bundle– Monthly Point Prevalence Study with feedback
• Changed our ED to stock only urimeter kits so admissions to CC would already have urimeter in place
• Beds do not have an appropriate hanger forcatheter bag while in the low position
• CT Table no place to hang catheter bag• Catheter Care charting not being done in EMR
– Educated Nurse Techs and added to charting
Measureso Education and competencies
• Every area that had the potential to touch a UC - Nsg, Nurse techs, Radiology, Transportation, PT/OT
• Developed a checklist and standard work related tourinary catheter insertion
• Required demonstration for all licensed staff that will insert and care for urinary catheters• We know that practices change over the years• Puts all staff on same page (standard
work) when observing insertions
Measures
o CHG bathing for critical care patients• Survey about bathing practices before and after implementation• People’s mindsets changed about the need for a daily soap
andwater bath
• Has branched out to other areas of the hospital after seeing outcomes
o Physician IP Education – contains HICPAC
indications for UC placement to put everyone on the
same page

Measures
o Status board built in Meditech – PCS charting to quickly access UC related data• Used by lead charge nurse for rounding on all
patients each shift• To ensure interventions in place: Is it
hanging in the right place? Secured to leg? Is it still needed?
Internal Reporting
o Event Analysis presentations at IP Council• All HAI device infections and C. difficile are
reviewed by frontline staff involved in the patient’s care.
• Frontline staff bring opportunities to meetingto be discussed
• Frontline engagement and buy-in for IP measures
• Leadership buy-in needed to make sure FLScan get to the meeting
Internal Reporting
o Help staff connect the dots• Standing agenda item on staff nurse, charge
nurse meetings
o Event analysis sent to Nurse Manager inreal time
o Monthly scorecard to individual unitso Data reported to Infection Control
Committee, Patient Safety Committee and Quality Council

Real Time Reporting
Lean initiative: Visual Management Boards posted on the units contain number of days infection free

Attachments• Hospitalist Multidisciplinary Round Guide.doc• Urinary Catheter Insertion Care and Removal.pdf• Urinary Catheter Removal Nurse Clinical Practice
Guideline.pdf• MRH Urinary Catheter Insertion Assessment.doc• CAUTI Prevention Pocket Card.doc• Female Foley (insertion) Checklist.doc• Physician IP Education.doc

Questions?

WEST TENNESSEE HEALTHCARESHERRI MCALEXANDER, RN, IP
JACKSON MADISON COUNTY GENERAL HOSPITAL
635-bed tertiary care center Serves 17-county area of rural
West Tennessee 5 adult intensive care units as well
as a neonatal intensive care unit Not-for-profit organization
CAUTI PREVENTION INITIATIVE
We began in September 2012 Started out with a CAUTI Bundle following
the HICPAC recommendations for CAUTI Prevention: appropriate catheter usage, proper insertion and maintenance, and prompt removal interventions
Rolled out education to the staff CHG usage in ICUs Bard Stat-lock Rochester Medical Spirit condom catheters

NO
YES
YES
NO
Catheters NOT indicated for:
Incontinence with no skin breakdown Unable to ambulate Close monitoring of urine output outside ICUs Morbid obesity Patient request Confusion or dementia
Urinary catheter in place?
No action necessary. Reassess daily. Avoid catheter placement.
Does the patient meet
criteria for the catheter?
Remove catheter
Criteria to continue:
*Urinary retention
*Urinary obstruction
*Assessment of UOP in critically ill ICU patients: I&O q hour, chemically sedated on a vent, pregnant pts on Magnesium drips
*Patients having selected surgeries: gynecological, genitourinary, or surgeries on contiguous (adjacent) structures such as colorectal or abdominal/pelvic surgeries
*Assist in healing of perineal/sacral wounds in incontinent patients
*Required immobilization for trauma or surgery
*Hospice/Comfort/Palliative care patients
*Chronic indwelling urinary catheters present on admission
Continue to monitor catheter need on a DAILY
basis.

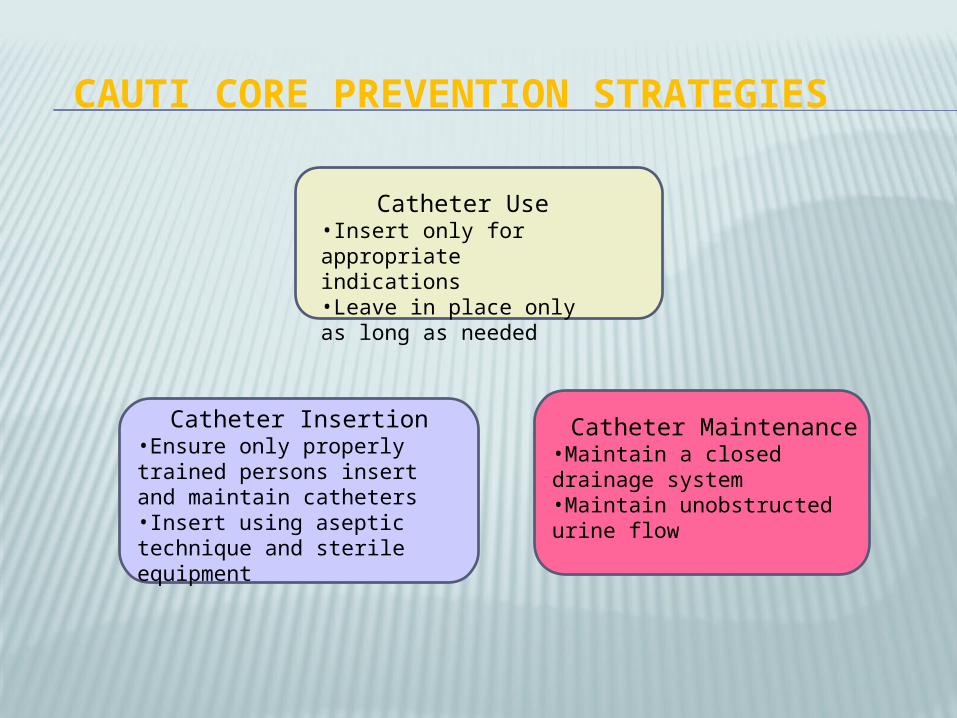
CAUTI CORE PREVENTION STRATEGIES
Catheter Use•Insert only for appropriate indications•Leave in place only as long as needed
Catheter Insertion•Ensure only properly trained persons insert and maintain catheters•Insert using aseptic technique and sterile equipment
Catheter Maintenance•Maintain a closed drainage system•Maintain unobstructed urine flow
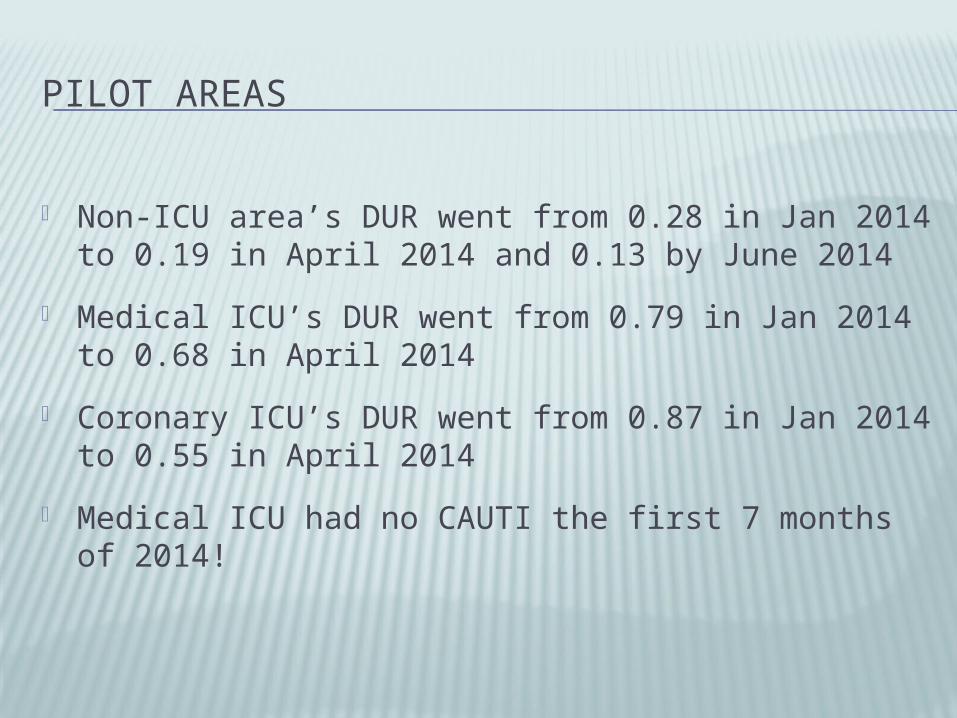
PILOT AREAS
Non-ICU area’s DUR went from 0.28 in Jan 2014 to 0.19 in April 2014 and 0.13 by June 2014
Medical ICU’s DUR went from 0.79 in Jan 2014 to 0.68 in April 2014
Coronary ICU’s DUR went from 0.87 in Jan 2014 to 0.55 in April 2014
Medical ICU had no CAUTI the first 7 months of 2014!

IN SUMMARY
House-wide, our device utilization ratio has dropped from 0.36 in June of 2012 to 0.27 in April 2014
In our ICUs we have dropped our CAUTI rate from 7.03 in December 2013 to 1.51 as of August 2014!
• OB Monthly Team Webinar- September 29, 2014; 10:00am CST
• TCPS October Monthly Webinar- October 17, 2014; 9:00am CST
• OB Monthly Team Webinar- October 27, 2014; 10:00am CST
• 2014 THA Leadership Summit– Wednesday November 5th at the Gaylord Opryland Hotel and Convention
Center in conjunction with THA’s Annual Meeting. Make plans to showcase your improvement work by submitting a poster for presentation. Contact Chris Clarke at [email protected] for details
Upcoming Events
• Webinar Evaluation: Earn contact hours for webinar participation after completing
• TCPS Newsletter: Sent every Tuesday afternoon
• IHI Open School: THA is providing free access to the IHI Open School curriculum for 2014 to employees and trustees of our safety partner hospitals.
• AHRQ Hospital Survey on Patient Safety (HSOPS): The Tennessee Center for Patient Safety offers the survey to all safety partners at NO COST. Go to www.tnpatientsafety.comTools and Resources AHRQ Culture Survey for more information.
Other Reminders

IHI Open School 2014• THA is providing free access to the IHI Open School curriculum to
employees and trustees of our safety partner hospitals.• 21 online, self-paced courses including 72 lessons and corresponding
resources—videos, case studies, podcasts, featured articles, exercises, networking
• Free app for the iPhone and iPad by logging onto iTunes• Over 25 contact hours available for CME, CNE, CPHQ and ACPE credit• Certificate of completion
1. Register using instructions. Type “Tennessee Hospital Association” as your facility to receive free membership.
2. Once registered, go to the course page: www.ihi.org/lms
3. Click the online learning tab and choose a lesson
4. Click Begin Lesson
34

Questions


















