
Tina L. Sumpter and David S. Wilkes Am J Physiol Lung Cell
12
286:1129-1139, 2004. doi:10.1152/ajplung.00330.2003 Am J Physiol Lung Cell Mol Physiol Tina L. Sumpter and David S. Wilkes You might find this additional information useful... 117 articles, 60 of which you can access free at: This article cites http://ajplung.physiology.org/cgi/content/full/286/6/L1129#BIBL 2 other HighWire hosted articles: This article has been cited by [PDF] [Full Text] [Abstract] , October 15, 2005; 172 (8): 944-955. Am. J. Respir. Crit. Care Med. D. S. Wilkes, T. M. Egan and H. Y. Reynolds Lung Transplantation: Opportunities for Research and Clinical Advancement [PDF] [Full Text] [Abstract] , March 15, 2008; 177 (6): 660-668. Am. J. Respir. Crit. Care Med. Cummings, T. Iwata, D. Brand, R. Presson, W. J. Burlingham and D. S. Wilkes Hayney, A. Munoz del Rio, K. Meyer, D. S. Greenspan, J. Torrealba, K. M. Heidler, O. W. J. L. Bobadilla, R. B. Love, E. Jankowska-Gan, Q. Xu, L. D. Haynes, R. K. Braun, M. S. Transplantation Th-17, Monokines, Collagen Type V, and Primary Graft Dysfunction in Lung on the following topics: http://highwire.stanford.edu/lists/artbytopic.dtl can be found at Medline items on this article's topics Medicine .. Homologous Transplantation Physiology .. Lungs Medicine .. Lung Transplantation Oncology .. Alloimmunity Oncology .. Autoimmunity Biochemistry .. Collagen including high-resolution figures, can be found at: Updated information and services http://ajplung.physiology.org/cgi/content/full/286/6/L1129 at: can be found AJP - Lung Cellular and Molecular Physiology about Additional material and information http://www.the-aps.org/publications/ajplung This information is current as of November 12, 2009 . http://www.the-aps.org/. American Physiological Society. ISSN: 1040-0605, ESSN: 1522-1504. Visit our website at year (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by the integrative aspects of normal and abnormal function of cells and components of the respiratory system. It is published 12 times a publishes original research covering the broad scope of molecular, cellular, and AJP - Lung Cellular and Molecular Physiology on November 12, 2009 ajplung.physiology.org Downloaded from
Transcript of Tina L. Sumpter and David S. Wilkes Am J Physiol Lung Cell

286:1129-1139, 2004. doi:10.1152/ajplung.00330.2003 Am J Physiol Lung Cell Mol PhysiolTina L. Sumpter and David S. Wilkes
You might find this additional information useful...
117 articles, 60 of which you can access free at: This article cites http://ajplung.physiology.org/cgi/content/full/286/6/L1129#BIBL
2 other HighWire hosted articles: This article has been cited by
[PDF] [Full Text] [Abstract], October 15, 2005; 172 (8): 944-955. Am. J. Respir. Crit. Care Med.
D. S. Wilkes, T. M. Egan and H. Y. Reynolds Lung Transplantation: Opportunities for Research and Clinical Advancement
[PDF] [Full Text] [Abstract], March 15, 2008; 177 (6): 660-668. Am. J. Respir. Crit. Care Med.
Cummings, T. Iwata, D. Brand, R. Presson, W. J. Burlingham and D. S. Wilkes Hayney, A. Munoz del Rio, K. Meyer, D. S. Greenspan, J. Torrealba, K. M. Heidler, O. W. J. L. Bobadilla, R. B. Love, E. Jankowska-Gan, Q. Xu, L. D. Haynes, R. K. Braun, M. S.
TransplantationTh-17, Monokines, Collagen Type V, and Primary Graft Dysfunction in Lung
on the following topics: http://highwire.stanford.edu/lists/artbytopic.dtlcan be found at Medline items on this article's topics
Medicine .. Homologous Transplantation Physiology .. Lungs Medicine .. Lung Transplantation Oncology .. Alloimmunity Oncology .. Autoimmunity Biochemistry .. Collagen
including high-resolution figures, can be found at: Updated information and services http://ajplung.physiology.org/cgi/content/full/286/6/L1129
at: can be foundAJP - Lung Cellular and Molecular Physiologyabout Additional material and information
http://www.the-aps.org/publications/ajplung
This information is current as of November 12, 2009 .
http://www.the-aps.org/.American Physiological Society. ISSN: 1040-0605, ESSN: 1522-1504. Visit our website at year (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2005 by theintegrative aspects of normal and abnormal function of cells and components of the respiratory system. It is published 12 times a
publishes original research covering the broad scope of molecular, cellular, andAJP - Lung Cellular and Molecular Physiology
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

Invited Review
Role of autoimmunity in organ allograft rejection: a focus on immunity totype V collagen in the pathogenesis of lung transplant rejection
Tina L. Sumpter and David S. WilkesDepartments of Medicine, Microbiology and Immunology, Indiana University School of Medicine,Richard L. Roudebush Veterans Affairs Medicine Center, Indianapolis, Indiana 46202
Sumpter, Tina L., and David S. Wilkes. Role of autoimmunity in organallograft rejection: a focus on immunity to type V collagen in the pathogenesis oflung transplant rejection.Am J Physiol Lung Cell Mol Physiol 286: L1129–L1139,2004; 10.1152/ajplung.00330.2003.—Lung transplantation is the only definitivetreatment modality for many forms of end-stage lung disease. However, the lung isrejected more often than any other type of solid organ allograft due to chronicrejection known as bronchiolitis obliterans (BO). Indeed, BO is the primary reasonwhy the 5- and 7-yr survival rates are worse for the lung than for any othertransplanted organ. Alloimmunity to donor antigens is established as the primarymechanism that mediates rejection responses. However, newer immunosuppressiveregimens designed to abrogate alloimmune activation have not improved survival.Therefore, these data suggest that other antigens, unrelated to donor transplantationantigens, are involved in rejection. Utilizing human and rodent studies of lungtransplantation, our laboratory has documented that a native collagen, type Vcollagen [col(V)], is a target of the rejection response. Col(V) is highly conserved;therefore, these data indicate that transplant rejection involves both alloimmune andautoimmune responses. The role of col(V) in lung transplant rejection is describedin this review article. In addition, the potential role of regulatory T cells that arecrucial to modulating autoimmunity and alloimmunity is also discussed.
bronchiolitis obliterans; regulatory T cell; major histocompatibility complex
LUNG TRANSPLANTATION is the only definitive treatment for manyforms of end-stage lung disease such as emphysema, idiopathicpulmonary fibrosis, and cystic fibrosis. The first lung trans-plants were performed nearly 40 years ago, and currently, over1,400 lung transplants are performed annually (44). Survival ofthe transplant recipients is limited by the development ofchronic rejection known as bronchiolitis obliterans (BO), theleading cause of death in lung allograft recipients (44). Indeed,BO is the primary reason why the 5- and 7-yr survival rates oflung allograft recipients are�50 and 35%, respectively, post-transplantation. Survival statistics following lung transplant arethe worst of all recipients of solid organ allografts (Fig. 1). Thepoor survival statistics take on a new importance when con-sidered in the context of advancements of surgical techniques,immunosuppression, and other supportive measures developedfor the care of these patients over the last 20 years. The currentsophistication in treatment regimens has not translated intoimproved survival of lung transplant recipients.
Repeated acute rejection episodes have been suggested to bethe main risk factor for the development of BO (52). BO alsoarises as a severe pulmonary complication postbone marrowtransplantation. BO has also been described following inhala-tion injury and after viral infections and may be idiopathic,occurring after nonspecific pulmonary injury (56, 92, 103).
Although there are other examples (10), a common themeemerges, suggesting that BO following lung transplant mayactually result from a local response to tissue remodeling thatoccurs postlung injury and not an immune response to alloan-tigens. Patients at risk for BO have higher local levels ofsoluble mediators of repair, such as IL-6, IL-8, monocytechemoattractant protein-1, and other factors, implicating theirrole in BO pathogenesis (85). The link between acute rejectionand BO may be the sustained injury and tissue remodeling thatoccurs during the rejection response. Halloran et al. (34)suggested that the “injury response” is the cause of chronicrejection of solid organs. In accord with this, a cycle of injuryis initiated by either ischemia of the grafted organ or thealloimmune response and marked by release of inflammatorycytokines and other mediators promoting repair of the lung.Immunological repair and tissue remodeling marked by im-mune recognition of foreign and possible sequestered antigenscould result in further injury.
Building on the concept that remodeling may release novelantigens into the lung, one could hypothesize that ischemia/reperfusion injury could release self-antigens that could inducethe onset of BO. Models of retransplantation in which the graftis transplanted back into the original host following the onsetof rejection illustrate this point (50, 97). If recognition ofallogeneic major histocompatibility complexes (MHCs) medi-ated the rejection response, then chronic rejection may cease ordiminish after the graft is retransplanted into a syngeneic host.For example, Izutani et al. (50) studied the vasculopathy ofchronic cardiac rejection in mice. In this report, chronic rejec-
Address for reprint requests and other correspondence: D. S. Wilkes, Depts.of Medicine, Microbiology, and Immunology, Indiana Univ. School of Med-icine, Richard L. Roudebush VA Medicine Center, 1481 W. 10th St. 111P,Indianapolis, IN 46202 (E-mail: [email protected]).
Am J Physiol Lung Cell Mol Physiol 286: L1129–L1139, 2004;10.1152/ajplung.00330.2003.
http://www.ajplung.org L1129
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

tion did not abate once cardiac allografts were retransplantedinto syngeneic hosts. This suggests that chronic allograft re-jection could proceed in the absence of allogenic donor anti-gens, which could indicate that chronic rejection may involvemechanisms other than alloimmunity. A non-MHC antigen,found in both donor and recipient, exposed during the originalrejection response could have a role in the pathogenesis ofchronic rejection. In support of this, myosin and heat shockproteins, which are nonpolymorphic among individuals, medi-ate rejection in experimental models of cardiac and skin graftrejection, respectively, adding an autoimmune component tothe rejection response (8, 15, 16).
TYPE V COLLAGEN AND IMMUNITY DURING LUNGALLOGRAFT REJECTION
Our laboratory has determined that immunity during lungallograft rejection involves an immune response to anotherself-antigen, type V collagen [col(V)] (37, 65, 114, 115). Allcollagen molecules are triple helices composed of �-chains(101). Col(V) is a 116-kDa heterodimer composed of �1- and�2-chains (57, 101). In the lung, col(V) is considered a minorcollagen located within the perivascular and peribronchiolarconnective tissues, which are sites of rejection activity (57, 63,64). Data showing that col(V) is a target of the immuneresponse during lung allograft rejection (37, 65, 114, 115) andthat recognition of polymorphisms in donor MHC antigensstimulate rejection activity suggested that col(V) may havepartial sequence homology to MHC proteins. Interestingly, theimmune response to col(V) in lung transplantation appears tobe directed against �1-chain of col(V) [�1(V)] and �2(V).�1(V) is nearly 80% homologous to the �2-chain of type XIcollagen [�2(XI)] (14), and the gene for �2(XI) maps within theMHC class II loci in humans and mice (36). Although thesedata suggest col(V) peptides may have sequence homology toMHC antigens, analysis of amino acid sequences did not revealany primary homology between col(V) and MHC molecules.However, primary sequence homology to alloantigens alonemay not be required to induce alloimmunity. For example, Luzet al. (60) recently reported a single amino acid substitution ina peptide bound to MHC molecules altered the affinity of theMHC-peptide complex to the T cell receptors (TCRs). Thissingle amino acid substitution may determine the differencebetween autoreactivity or alloreactivity. Alternatively, priorinfections or other host factors could trigger or perpetuateimmune responses to both autoantigens and alloantigens (1).
These data suggest that secondary or tertiary characteristics ofthe peptide, the peptide-TCR affinity, or other host factors mayexplain the phenomenon of col(V)-induced immunity duringlung allograft rejection.
IMMUNE RESPONSE TO COL(V) CONTRIBUTETO THE REJECTION RESPONSE
The first evidence showing that col(V) was involved in localimmune responses to lung alloantigens was obtained from ourmurine model of acute rejection. In this model, repeatedintrapulmonary instillations of allogeneic lung macrophagesand dendritic cells reproduce the immunology and pathologyanalogous to acute rejection in recipient lungs (108). After fourweekly instillations of allogeneic lung cells, recipient micedevelop lymphocytic perivascular and peribronchiolar infil-trates analogous to grade 1–2 acute rejection and IgG2a anti-body deposits in perivascular and peribronchiolar tissues (108).Our ongoing studies in human lung allograft recipientsundergoing rejection show similar antibody deposits in thetransplanted lung. The antigen recognized by these antibodiesis col(V) (D. S. Wilkes and W. Burlingham, manuscript inpreparation).
During ontogeny of the immune system, negative selectionin the thymus deletes autoreactive T cells, i.e., cells thatexpress TCRs with high affinity for self-antigens (88). How-ever, under normal conditions T cells with low affinity forself-antigens circulate in the periphery or reside in variousorgans (88). It is unlikely that autoreactive T cells will becomeactivated unless there are perturbations involving immunehomeostasis or exposure of sequestered self-antigens. Duringlung allograft rejection, rare self-antigens may be exposedresulting in the development of autoreactive T cells.
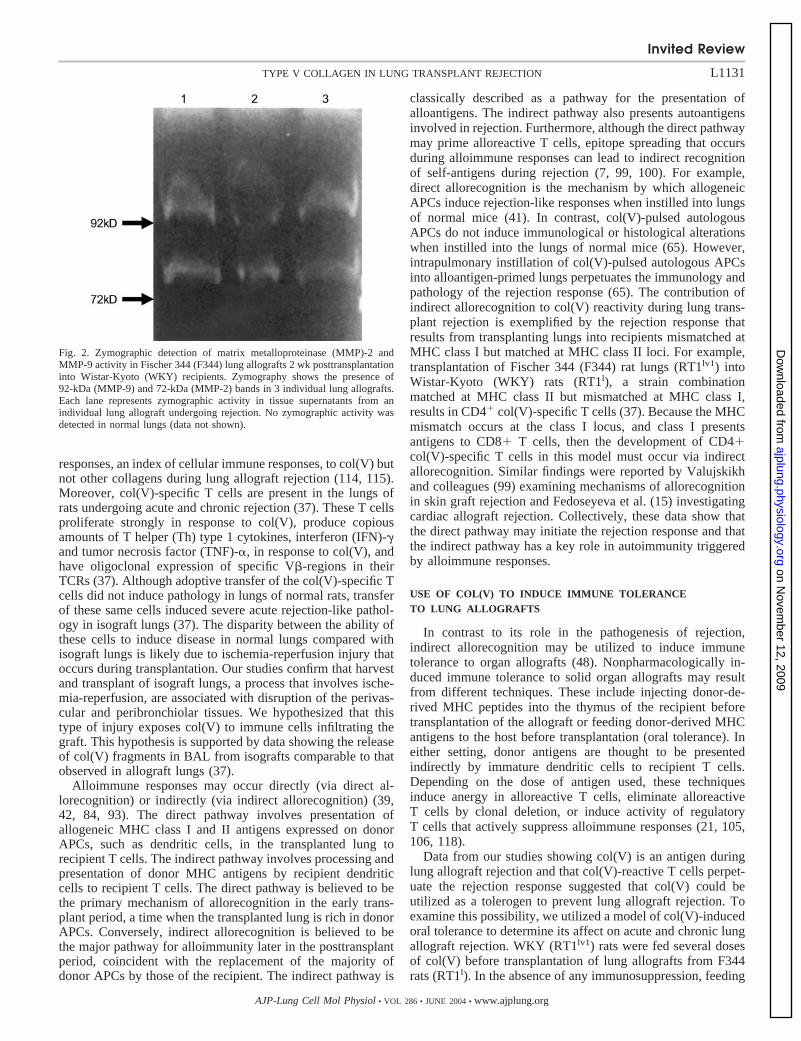
Col(V) is located beneath the basement membrane withinbronchiolar and vascular tissues in the lung and possiblyintercalated with type 1 collagen, the major collagen in thelung (63, 64). The inflammatory responses and architecturalremodeling that occurs in these tissues during the rejectionresponse may expose graft-infiltrating lymphocytes to frag-ments of col(V). Indeed, we reported that lung allograft rejec-tion is associated with the release of col(V) fragments inbronchoalveolar lavage fluid (BAL) (37). Matrix metallopro-teinases (MMPs) may degrade collagen molecules (121).MMP-2 and MMP-9 are capable of degrading col(V), andTrello et al. (96) reported activity of MMP-2 and MMP-9 inlungs of human transplant recipients during rejection. Figure 2shows that MMP-2 and MMP-9 are active in rat lung allograftsduring acute rejection, thus supporting the role of MMPs in therelease of col(V) fragments during the rejection response.These data support the theory that inflammation and remodel-ing occurring during the rejection response may lead to therelease of potentially antigenic col(V) peptides.
However, the aforementioned data are indirect evidence thatimmune responses to col(V) are involved in the pathogenesisof lung allograft rejection. As T cells mediate rejection, col(V)-specific cellular immune activity during the rejection responsewas examined. T cells isolated from the lungs of mice thatreceived instillations of allogeneic antigen-presenting cells(APCs) proliferated in response to col(V), but not col(II), acollagen found in cartilage but not the lung (37, 114, 115).Similarly, rats develop strong delayed type hypersensitivity
Fig. 1. Survival data for recipients of solid organ allografts (2002). Dataadapted from the Collaborative Transplant Study Group with permission.
Invited Review
L1130 TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from
responses, an index of cellular immune responses, to col(V) butnot other collagens during lung allograft rejection (114, 115).Moreover, col(V)-specific T cells are present in the lungs ofrats undergoing acute and chronic rejection (37). These T cellsproliferate strongly in response to col(V), produce copiousamounts of T helper (Th) type 1 cytokines, interferon (IFN)-�and tumor necrosis factor (TNF)-�, in response to col(V), andhave oligoclonal expression of specific V�-regions in theirTCRs (37). Although adoptive transfer of the col(V)-specific Tcells did not induce pathology in lungs of normal rats, transferof these same cells induced severe acute rejection-like pathol-ogy in isograft lungs (37). The disparity between the ability ofthese cells to induce disease in normal lungs compared withisograft lungs is likely due to ischemia-reperfusion injury thatoccurs during transplantation. Our studies confirm that harvestand transplant of isograft lungs, a process that involves ische-mia-reperfusion, are associated with disruption of the perivas-cular and peribronchiolar tissues. We hypothesized that thistype of injury exposes col(V) to immune cells infiltrating thegraft. This hypothesis is supported by data showing the releaseof col(V) fragments in BAL from isografts comparable to thatobserved in allograft lungs (37).
Alloimmune responses may occur directly (via direct al-lorecognition) or indirectly (via indirect allorecognition) (39,42, 84, 93). The direct pathway involves presentation ofallogeneic MHC class I and II antigens expressed on donorAPCs, such as dendritic cells, in the transplanted lung torecipient T cells. The indirect pathway involves processing andpresentation of donor MHC antigens by recipient dendriticcells to recipient T cells. The direct pathway is believed to bethe primary mechanism of allorecognition in the early trans-plant period, a time when the transplanted lung is rich in donorAPCs. Conversely, indirect allorecognition is believed to bethe major pathway for alloimmunity later in the posttransplantperiod, coincident with the replacement of the majority ofdonor APCs by those of the recipient. The indirect pathway is
classically described as a pathway for the presentation ofalloantigens. The indirect pathway also presents autoantigensinvolved in rejection. Furthermore, although the direct pathwaymay prime alloreactive T cells, epitope spreading that occursduring alloimmune responses can lead to indirect recognitionof self-antigens during rejection (7, 99, 100). For example,direct allorecognition is the mechanism by which allogeneicAPCs induce rejection-like responses when instilled into lungsof normal mice (41). In contrast, col(V)-pulsed autologousAPCs do not induce immunological or histological alterationswhen instilled into the lungs of normal mice (65). However,intrapulmonary instillation of col(V)-pulsed autologous APCsinto alloantigen-primed lungs perpetuates the immunology andpathology of the rejection response (65). The contribution ofindirect allorecognition to col(V) reactivity during lung trans-plant rejection is exemplified by the rejection response thatresults from transplanting lungs into recipients mismatched atMHC class I but matched at MHC class II loci. For example,transplantation of Fischer 344 (F344) rat lungs (RT1lv1) intoWistar-Kyoto (WKY) rats (RT1l), a strain combinationmatched at MHC class II but mismatched at MHC class I,results in CD4� col(V)-specific T cells (37). Because the MHCmismatch occurs at the class I locus, and class I presentsantigens to CD8� T cells, then the development of CD4�col(V)-specific T cells in this model must occur via indirectallorecognition. Similar findings were reported by Valujskikhand colleagues (99) examining mechanisms of allorecognitionin skin graft rejection and Fedoseyeva et al. (15) investigatingcardiac allograft rejection. Collectively, these data show thatthe direct pathway may initiate the rejection response and thatthe indirect pathway has a key role in autoimmunity triggeredby alloimmune responses.
USE OF COL(V) TO INDUCE IMMUNE TOLERANCETO LUNG ALLOGRAFTS
In contrast to its role in the pathogenesis of rejection,indirect allorecognition may be utilized to induce immunetolerance to organ allografts (48). Nonpharmacologically in-duced immune tolerance to solid organ allografts may resultfrom different techniques. These include injecting donor-de-rived MHC peptides into the thymus of the recipient beforetransplantation of the allograft or feeding donor-derived MHCantigens to the host before transplantation (oral tolerance). Ineither setting, donor antigens are thought to be presentedindirectly by immature dendritic cells to recipient T cells.Depending on the dose of antigen used, these techniquesinduce anergy in alloreactive T cells, eliminate alloreactiveT cells by clonal deletion, or induce activity of regulatoryT cells that actively suppress alloimmune responses (21, 105,106, 118).
Data from our studies showing col(V) is an antigen duringlung allograft rejection and that col(V)-reactive T cells perpet-uate the rejection response suggested that col(V) could beutilized as a tolerogen to prevent lung allograft rejection. Toexamine this possibility, we utilized a model of col(V)-inducedoral tolerance to determine its affect on acute and chronic lungallograft rejection. WKY (RT1lv1) rats were fed several dosesof col(V) before transplantation of lung allografts from F344rats (RT1l). In the absence of any immunosuppression, feeding
Fig. 2. Zymographic detection of matrix metalloproteinase (MMP)-2 andMMP-9 activity in Fischer 344 (F344) lung allografts 2 wk posttransplantationinto Wistar-Kyoto (WKY) recipients. Zymography shows the presence of92-kDa (MMP-9) and 72-kDa (MMP-2) bands in 3 individual lung allografts.Each lane represents zymographic activity in tissue supernatants from anindividual lung allograft undergoing rejection. No zymographic activity wasdetected in normal lungs (data not shown).
Invited Review
L1131TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

col(V) prevented the onset of acute lung allograft rejection(Fig. 3) and, most importantly, abrogated the development ofBO (Fig. 4). The ability of col(V)-induced tolerance to preventrejection was not haplotype specific, in that feeding col(V) waseffective in suppressing acute rejection in another unrelated ratstrain combination undergoing lung transplantation (114). Im-portantly, col(V)-induced tolerance did not induce global im-mune hyporesponsiveness, as cellular immune responses tonominal antigens were not suppressed in col(V)-tolerant recip-ients made tolerant to col(V) (114).
APC-induced immune activation of T cells is dependent onbidirectional signaling between APCs and T cells. Oral toler-ance could affect both T cell and APC function. Therefore,defective antigen presentation could have contributed to theinability of T cells from tolerant rats to respond to alloantigens.However, data showing that APCs isolated from tolerant allo-graft recipients were comparable to APCs from normal rats instimulating proliferation in donor-derived T cells indicate thatcol(V)-induced oral tolerance affected the function of T cellsand not the function of APCs (114).
Fig. 3. Top: gross anatomy of control isograft lungs(A), control allograft lungs (B), and collagen type V[col(V)]-fed allograft lungs (C) 2 wk posttransplan-tation (posterior view). The left (L) lung is thetransplanted lung, and the right (R) is the native lungin each panel. The control allograft lung (L in B) wasdark brown in color and shrunken compared with thenative lung. However, the col(V)-fed allograft lung(L in C) had the appearance of the isograft lung (Lin A). Control isograft lungs (A) show no patholog-ical lesions and are identical to normal WKY lungs(data not shown). Photographs representative of 5rats in each group. Bottom: histology of controlisografts (D), control allografts (E), and col(V)-fedallografts (F) 2 wk posttransplantation. Controlisografts show normal airway and vascular struc-tures (D). Control allografts show extensive perivas-cular, peribronchial, and alveolar mononuclear cellinfiltrates consistent with severe rejection, grade A4(E). In contrast, allografts from rats fed col(V)before transplantation show only mild to moderateperivascular and peribronchial mononuclear cell in-filtrates, grade A1–A2 (F). Photomicrographs repre-sentative of 5 rats in each group (�100 magnifica-tion). [Adapted from Yasufuku et al. (114).]
Fig. 4. Top: gross anatomy of control allograft lungs (A) andcol(V)-fed allograft lungs (B) 10 wk posttransplantation(posterior view). The left lung is the transplanted lung, andthe right is the native lung in each panel. The controlallograft lung (L in A) was dark brown, shrunken, and firm.However, the col(V)-fed allograft lung (L in B) had a nearlynormal appearance. Photographs representative of 5 rats ineach group. Bottom: histology of control allografts (C) andcol(V)-fed allografts (D) 10 wk posttransplantation. Controlallografts show extensive interstitial mononuclear cell infil-trates, fibrosis, and obliteration of small airways by granu-lation tissue (BO). In contrast, allografts from rats fedcol(V) before transplantation show only mild alveolar infil-trates consistent with mild acute rejection (grade A2) (D).Photomicrographs representative of 5 rats in each group(�100 magnification). [Adapted from Yasufuku et al.(115).]
Invited Review
L1132 TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

Presentation of alloantigens is critical for the development ofcol(V)-induced oral tolerance. This is exemplified by datashowing that tolerance could be adoptively transferred by Tcells isolated from lung allograft recipients made tolerant byfeeding col(V) but not by T cells isolated from rats fed col(V)that did not receive lung allografts. Furthermore, the overlap ofautoreactivity with alloreactivity was also shown by experi-ments in which adoptive transfer of col(V)-specific T cellsabrogated col(V)-induced immune tolerance to lung allografts(37). Examination of the immune mechanisms that mediatedsuppression of alloreactivity revealed that feeding col(V) fol-lowed by lung transplantation resulted in elevated systemicactivity of transforming growth factor (TGF)-� that suppressedalloimmune responses during acute and chronic rejection(114). Neutralizing TGF-� recovered activity of alloreactive Tcells (114). Therefore, alloreactive T cells were not lostthrough clonal deletion or through activation-induced celldeath; alloreactive T cells were actively suppressed. These datasuggested that regulatory T cells (Tregs) that produce TGF-�may have a key role in col(V)-induced oral tolerance. Indeed,data showing that tolerance to lung allografts may be adop-tively transferred to naıve rats (67) confirm a role for Tregs incol(V)-induced tolerance.
TREGS IN TOLERANCE: AUTOIMMUNITYAND ALLOIMMUNITY
Immune tolerance inhibits injurious responses against en-dogenous and exogenous antigens (106). Controlling toleranceinduction offers a powerful treatment modality for transplan-tation and autoimmunity. Tregs downregulate harmful immuneresponses and induce tolerance. Tregs block aberrant T cellresponses against both foreign and self-antigens in the periph-ery, preventing proliferation and activation of both autoreac-tive and alloreactive T cells. The immune response during lungallograft rejection appears to be biphasic, initiating with analloimmune response and resulting in an autoimmune re-sponse. Modulating Tregs offers a means for controlling bothof these deleterious phases hypothesized to occur in the lungand cause BO. To exploit the potential of Tregs, their naturalfunction in the lung needs to be better defined and the mech-anisms whereby Tregs can be induced also need to be identi-fied. The purpose of this section is to provide a brief overviewof the phenotype and function of Tregs and their relationship totransplantation tolerance.
CLASSIFICATION OF THE REGULATORS
Tregs are commonly described as belonging to three subsets:Th3 cells, T regulatory type 1 (Tr1) cells, or thymically derivedTregs. These subsets differ in ontogeny and in mechanisms ofaction. Recently, Bluestone and Abbas (9) classified Tregs astwo types: natural Tregs and adaptive Tregs. Natural Tregs areantigen nonspecific thymically derived Tregs that suppress Tcell responses in a contact-driven, antigen-independent man-ner. Adaptive Tregs differentiate either from thymically de-rived Tregs or from CD4� helper T cells following antigenicstimulation in the periphery. Adaptive Tregs suppress T cellresponses in an antigen-specific, cytokine-driven manner. AllTregs work to maintain systemic immune homeostasis.
Tregs arise in the thymus (5) and first emerge at day 10 ofneonatal development (76). Jagged-1, a Notch ligand naturally
found on thymic epithelial cells, is involved in the differenti-ation of Tregs (116). Naturally occurring Tregs with diversephenotypes have been isolated from the thymus, lymph nodes,spleens, and peripheral blood of rodents and humans (4).Naturally occurring Tregs with suppressive properties include��TCR� cells (40), CD8�CD4� cells (17), CD4�DX5�cells (22), and CD4�CD8���TCR� cells (19, 119). Themost extensively studied Tregs constitutively express CD4 andCD25, the IL-2 receptor �-chain, in humans and in mice (82,90, 110) and CD4 and CD45RC in rats (117). Unlike Th3 andTr1 cells, which are clonally derived, natural Tregs are hetero-geneous, evidenced by the diversity expressed in their TCRV�-repertoires (58). Tregs express high levels of CD5, CD54,CD69, CD38 (78), and Fas (90) and express low levels ofCD62L and CD45RB (77). Tregs constitutively express thecostimulatory molecules CD28, 4-1BB, glucocorticoid-in-duced TNF receptor (GITR), CD103, and OX-40 (62). Al-though Tregs express surface markers found on activated Tcells, such as CD25 in mice and humans, it is important to notethat naturally occurring Tregs are a unique lineage of thymi-cally derived cells, independent from T cells activated in theperiphery (49).
CD4�CD25� Tregs suppress a plethora of autoimmunediseases. In mice, thymectomy on the third day of neonataldevelopment causes a deficiency of CD4�CD25� Tregs,resulting in systemic autoimmunity (5). Depleting wild-typeadult mice of CD25� cells breaks systemic tolerance, resultingin multiple autoimmune diseases (5). Multiple autoimmunediseases develop following adoptive transfer of lymph node orspleen-derived cells depleted of CD25� cells into nude mice.Thyroiditis, gastritis, insulitis, sialoadenitis, adrenalitis, oopho-ritis, glomerulonephritis, polyarthritis, as well as graft-vs.-hostdisease have all been described in this model (82). In thesemodel systems, naturally occurring Tregs maintain homeosta-sis by inhibiting autoreactive T cells.
In the respiratory and oral mucosa, maintenance of ho-meostasis is crucial. The mucus-lined tracts of the respiratorytract and the gut are continually assaulted with environmentalantigens. Aberrant immune responses in these regions wouldbe systemically detrimental. Tregs maintain homeostasis inthese environments, with Tr1 cells predominating in the drain-ing lymph nodes of the lung and Th3 cells predominating in thegut (3). IL-10, secreted by pulmonary dendritic cells inducesdifferentiation of antigen-specific T cells with regulatory ca-pabilities that differentiate from CD4� cells. These cells,deemed Tr1 cells, secrete IL-10 and IL-4 but not TGF-� (3).Systemic administration of IL-10 increases populations ofTregs in vivo (25). In vitro, Tr1 cells generated by stimulationwith exogenous IL-10 or by engagement of CD3 and comple-ment regulatory protein in the presence of IL-2 have beendescribed (30, 53). IL-10, produced by Tr1 cells, rendersCD4� cells anergic and unable to respond to alloantigen inmixed lymphocyte reactions (29).
Th3 cells generated in a similar manner in the gut maintainoral tolerance. After feeding with low dose of oral antigen,dendritic cells in mucosal gut-associated lymphatic tissue se-crete TGF-�. TGF-� induces antigen-specific CD4� T cells todifferentiate into Th3 cells (3). Ex vivo stimulation withTGF-� generates Th3 cells from CD4� T cells. Th3 cells, inturn, secrete large quantities of TGF-� (106). TGF-�, likeIL-10 produced by Tr1 cells, is a potent immunosuppressant
Invited Review
L1133TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

capable of blocking T cell proliferation. IL-4, also secreted byTh3 cells, acts on the Th3 cells in a positive feedback loop toincrease production of TGF-� and maintain populations of Th3cells (47). Although operating through different cytokines,both Tr1 cells and Th3 cells express markers of activated cells.CD25 has been identified on both populations (53, 120). Bothpopulations express low levels of CD45RB (as reviewed inRef. 29). Oligoclonality of their TCR V�-region indicatesantigen specificity in Tr1 and Th3 cells (13, 58). Tr1 and Th3cells arise in the periphery in response to antigen when stim-ulated with the appropriate cytokines.
Tr1 and Th3 cells have also been exploited in autoimmunemodels. After stimulation with autoantigen, Tr1 cells secretingIL-10 were isolated in a murine model of diabetes. Adoptivetransfer of these Tr1 cells inhibited diabetes in secondaryrecipients (12). Chen et al. (13) induced Th3 cells to protectagainst development of autoimmune encephalomyelitis by oraladministration of myelin basic protein. In our laboratory, Th3cells from rats tolerized orally to col(V) block BO in allograftrecipients (Fig. 4).
The mechanism utilized by Tregs in vivo to suppress cell-mediated immunity has been investigated extensively, butmany questions remain. In vitro, Tregs in the presence of APCsblock CD3-induced proliferation of CD4� Th cells (94),CD8� cytolytic T cells (CTLs) (76), and natural killer T cells(6) in an antigen-independent manner (95). In such a coculturesystem, Tregs suppress transcription of IL-2 mRNA in the Thsand CTLs, resulting in cell cycle arrest (76, 94). The interac-tion occurring among this cellular triad of APCs, Tregs, andresponder T cells is controversial. Th3 and Tr1 cells secretesoluble mediators of immunosuppression. However, in manyreports, Tregs require contact with the APC and the responderT cells to exert their suppressive function. This contact-depen-dent suppression may be due to membrane-bound TGF-� (4,69) identified by expression of latency-associated peptide,which cleaves inactive TGF-� into active TGF-� (69, 73). Analternative mechanism of immune suppression may be relatedto elevated expression of costimulatory molecules, such asCTLA-4, on Tregs, which may compete with the responder Tcells for a limited number of ligating molecules, such as B7.1(CD80) and B7.2 (CD86) on the surface of APCs. If this weretrue, increasing the numbers of APCs would decrease thesuppressor function of Tregs. In fact, in a coculture systemwith Tregs, Ths, and APCs, suppression can be enhanced byincreasing the number of APCs (91). This phenomenon sug-gests that bidirectional signaling between APC and Tregs mayaugment the suppressive function of Tregs. In fact, a recentreport from Grohmann et al. (28) demonstrated that CTLA-4 Igcan induce expression of indoleamine 2,3-dioxygenase (IDO)in dendritic cells. IDO is an enzyme that depletes tryptophan,resulting in suppressed T cell function. CTLA-4 is upregulatedon the surface of Tregs, suggesting that Tregs may suppressother cells indirectly through interactions with APCs. Collec-tively, these reports suggest that there are many potentialmechanisms of Treg-induced immune suppression.
REGULATING THE REGULATORS
Tregs constitutively express CD25, the IL-2 receptor�-chain, suggesting that IL-2-mediated signaling may be im-portant for Treg maintenance. In good agreement, IL-2, IL-
2R�, and IL-2R� knockout mice develop lethal autoimmunedisorders, suggesting that IL-2 is required for the maintenanceof tolerance (20, 75, 79, 89, 109). More importantly, Tregsfrom IL-2 knockout mice regain regulatory function in thepresence of IL-2, whereas T cells from IL-2R knockout micedo not have regulatory function, suggesting that Tregs areregulated by IL-2 signaling (20). In support of this, in vitropriming of Tregs with IL-2 in the presence of TCR ligationenhances their suppressive function (94).
In vitro, Tregs do not proliferate in response to TCR ligation(91). After TCR ligation, Tregs do not synthesize IL-2, whichmay contribute to their anergic state. The addition of exoge-nous IL-2 or ligation of CD28 breaks anergy. This effect isreversible; when IL-2 or anti-CD28 are removed from the cellculture environment, Tregs return to their anergic state. Foxp3,constitutively expressed in Tregs, may maintain anergy. Foxp3encodes scurfin, the forkhead-winged helix transcription factorthat has recently come to light as a key regulator for Tregfunction (18, 43). Foxp3-deficient patients develop severe lym-phoproliferative and autoimmune disorders (107). Overexpres-sion of scurfin in CD4 cells inhibits proliferation and IL-2production following ligation of the TCR (54, 86). Overex-pressing Foxp3 in CD4�CD25� T cells upregulates expres-sion of CD25, CTLA-4, GITR, and CD103 and confers sup-pressive properties in these cells. Foxp3 appears to be crucialfor maintaining the Treg phenotype and suppressive properties.Induction of Foxp3 may be an important event required forgeneration of Tregs in the periphery (18, 43).
TGF-�, a potent immunosuppressive cytokine, may also beimportant for the generation of Tregs in the periphery. TGF-�inhibits the function of Th1 by downregulating the IL-12receptor and inhibits the function of Th2 cells by downregu-lating the expression of GATA-3 (24). Reports showing thatimpaired TGF-� signaling results in autoimmunity in the lungand gut indicate that this cytokine has a key role in maintainingperipheral tolerance (23, 68, 71). For example, mice expressinga dominant-negative TGF-� receptor 1 in T cells developautoimmune disease, localized to the lung and the colon (23).Our studies have shown that TGF-� is upregulated systemi-cally in tolerant lung allograft recipients (115). Moreover,permissiveness to TGF-�-mediated signaling may be a keyfeature of Tregs irrespective of the Treg phenotype. For exam-ple, we recently reported that Tregs mediating col(V)-inducedtolerance to lung allografts do not express Smad7, a moleculethat blocks TGF-�-mediated signaling (67). Furthermore,col(V)-induced oral tolerance to lung allografts results in Tregsthat proliferate in response to TGF-�, consistent with theabsence of Smad7 transcripts in these cells (67).
The importance of permissiveness to TGF-�-mediated sig-naling in the function of Tregs has also been shown by anothergroup of studies in our laboratory. We reported that lungallograft rejection is associated with the development ofcol(V)-reactive CD4� T cells that induce rejection “ like”pathology in isograft lungs after adoptive transfer (37). Thesesame cells, termed lung T cell-1 (LT1), also abrogated col(V)-induced oral tolerance to lung allografts (37). Interestingly,another col(V)-reactive T cell line, termed LT3, did not inducedisease in isograft lungs after adoptive transfer (37). AlthoughLT3 did not have an effect on col(V)-induced tolerance to lungallografts (37), adoptive transfer of LT3 to naıve rats abrogatedrejection of lung allografts, indicating that LT3 cells had
Invited Review
L1134 TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

regulatory function (Fig. 5). Although these cells were pheno-typically identical, examination of Smad7 profiles revealed thatLT1 expressed Smad7, whereas LT3 did not express Smad7(Fig. 6). These data are similar to our prior report of col(V)-induced tolerance to lung grafts showing that absence ofSmad7 identifies the Tregs with true regulatory function (67).Interestingly, Nakao et al. (71) showed that overexpression ofSmad7 in T cells is associated with a normal phenotype in micebut enhanced antigen-induced airway inflammation. Collec-tively, these data suggest Smad7, which determines permis-siveness to TGF-�-mediated signaling, may have key roles inregulating many types of T cell responses in the lung. Smad7expression is induced by IL-7 (45), IFN-� (98), and TGF-�(70). The molecular mechanisms suppressing the expression ofSmad7 transcripts are unknown.
Little is known about mechanisms for maintaining andexpanding Tregs in the periphery. Human peripheral blood Tcells with regulatory function have been expanded ex vivo inresponse to allogeneic stimulation in the presence of TGF-�,and these cells have regulatory activity when adoptively trans-ferred in vivo (113, 120). Several pharmacological interven-tions enhance the function or quantity of Tregs. For example,intratracheal administration of Flt-3 ligand, a potent mobilizerof dendritic cells, also results in an increase in Tregs in theBAL (74). Similarly, tolerant dendritic cells generated phar-macologically with 15-deoxyspergualin or 1, 25-dihydroxyvi-tamin D3 and mycophenolate mofetil expand and induce Tregsin models of cardiac transplant and diabetes, respectively (2,66). A secondary function of Tregs may be to induce tolero-genic dendritic cells, initiating a positive feedback loop for themaintenance of homeostasis (66).
TREGS IN TRANSPLANTATION TOLERANCE
Before the acceptance of Tregs as a true entity, Hall et al.(32) described the “CD4� suppressor cell” in an MHC mis-match model of cardiac transplantation. In these studies, sup-pressor cells isolated from the spleen or the lymph nodes ofcyclosporine-treated rats surviving 75 days following cardiactransplant blocked cardiac rejection in a second recipient for100 days. The CD4� suppressor cells isolated in thesestudies were CD25� and CD45RC� (33), matching the phe-notype of what was later identified as a Treg. Following thispioneering work, Tregs with diverse phenotypes have beenidentified in a number of experimental transplant model mod-els, including models of skin, cardiac, islet, and lung trans-plants (61, 67, 104). Tregs derived from these model systemsregulate alloreactive T cells through IL-10 and CTLA-4(38, 54), TGF-� (64), IL-4 (11), or a cytokine-independentmanner (27).
As mentioned previously, transplant tolerance can be in-duced by a number of protocols. These treatments includeusing antibodies to deplete CD4 cells or immunosuppressiveagents such as cyclosporine A (CsA), followed by a regimentolerizing the recipient to donor antigen, such as infusion withdonor blood or oral administration of donor MHC (72). Othermethods include blockade of costimulatory molecules (CD40,CD154) (102). These protocols result in the generation ofTregs. Many of these methods interfere with the normal func-tion of T cells themselves and may alter Treg efficiency. Forexample, Kinglsey et al. (55) have demonstrated that a second-ary exposure to alloantigen increases percentages of Tregsoriginally generated following exposure to alloantigen throughimmunization with donor strain blood in conjunction with ananti-CD4 antibody.
Because of the reliance on artificial regimens to generateTregs in transplant, questions arise as to the relationship ofthese cells with naturally arising Tregs. Like natural Tregs,those generated using these regimens rely on the thymus. Forexample, removal of the thymus diminishes but does notabrogate Treg-induced tolerance following a tolerization pro-tocol of oral donor splenocytes administration and depletinganti-CD4 antibody (72). To determine the efficacy of natural,thymically derived T cells in inhibiting graft rejection, Graca etal. (27) compared CD4�CD25� splenocytes from mice ren-dered tolerant to MHC-incompatible skin grafts with naıveCD4�CD25� splenocytes. Although both sets of regulatorswere able to block alloresponses, fewer regulator cells from
Fig. 5. Adoptive transfer of lung T cell-3 (LT3),but not LT1, suppresses allograft rejection.Twenty-four hours before transplantation ofF344 allograft lungs, 4 � 106 LT1 or LT3 cellswere injected into the tail vein of recipient WKYrats. Two weeks later, native and transplantedlungs were harvested. A: adoptive transfer ofLT1 had no effect on the development of severeacute rejection in transplanted lungs (grade 4),as manifest by extensive mononuclear cell infil-trates. B: adoptive transfer of LT3 suppressedallograft rejection (grade 1) as shown by fewperivascular infiltrates and no interstitial infiltra-tion. Data are shown from a representativeexperiment in each group (�100 originalmagnification).
Fig. 6. Smad7 expression in col(V)-specific T cell lines: LT1 and LT3. Smad7transcripts were detected by RT-PCR. Data is shown from a representativeexperiment.
Invited Review
L1135TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

tolerized mice were required for transferring graft tolerancecompared with regulators from naıve mice. Notably in thissystem, CD4�CD25� cells also transferred tolerance.
An interesting facet of Tregs isolated from graft recipients isdonor antigen specificity. In our studies of lung transplant,splenic Tregs from tolerant animals could adoptively transfertolerance to donor, but not third-party, antigen-MHC com-plexes (T. Mizobuchi and D. S. Wilkes, manuscript in prepa-ration). Similarly, Tregs have been isolated from skin graftswith the potential of inhibiting donor-specific rejection (26, 27,102, 104). These Tregs had no effect on the rejection ofthird-party grafts (26, 27, 102, 104). Antigen specificity andclonal origin of these Tregs are further demonstrated by anal-ysis of their TCRs. Tregs generated from rats tolerized tocol(V) exhibit a limited V�-repertoire compared with the Tregsfrom untolerized graft recipients and from untreated controls(T. Mizobuchi and D. S. Wilkes, manuscript in preparation).Graft-infiltrating T cells from tolerized rats in a model ofcardiac transplantation also had altered V�-repertoire com-pared with nontolerized controls (31, 112). In these grafts,tolerance may be induced against non-MHC antigens througha mechanism of linked suppression (111), suggesting thatgraft-infiltrating Tregs could block both alloimmune and auto-immune responses.
NOVEL APPROACH TO UNDERSTANDING CHRONIC LUNGALLOGRAFT REJECTION: THE ROLE OF TREGS
The presence of Tregs has been established in humans (90,110). They may function to suppress several immune func-tions, including autoimmunity and alloimmunity. Lung allo-graft rejection involves both alloimmunity to donor antigensand autoimmunity to col(V). Therefore, a dysregulation inTregs may be involved in the pathogenesis causing rejection.
Acute rejection is believed to be the major risk factor for thedevelopment of chronic rejection (10). Tregs, by inhibitingallo- and autoimmune responses, could modulate the develop-ment of chronic lung rejection known as BO, suggesting thatmodalities that either preserve or augment Treg function maysuppress the rejection response. In their “pool size model,”Sanchez-Fueyo et al. (83) hypothesized that the Tregs fail topromote graft survival because they are overpowered by allo-reactive T cells in the absence of immunosuppressive thera-pies. Alternatively, the failure of Tregs may be linked to theimmunosuppressive regimens utilized to treat and prevent therejection response. In a recent review, Wood and Sakaguchi(112) suggest that calcineurin inhibitors block development ofTregs and allograft tolerance. Immunosuppressants such asCsA and FK506 inhibit T cell function and alloreactivitythrough a calcineurin-dependent pathway (35, 51, 59). Al-though calcineurin may induce several functions in T cells, akey activity is the induction of IL-2. As Tregs require IL-2 tofunction optimally (94), calcineurin inhibitors that block IL-2transcription may have the untoward effect of suppressing oreliminating Tregs. Accordingly, the absence of Tregs couldlead to augmented autoimmunity, possibly accounting forcol(V)-induced cellular immunity in human lung allograftrecipients and increase risk of BO. In support of this theory,short courses of CsA induce autoimmune disease in experi-mental models (46, 81). Adoptive transfer of thymocytes fromCsA-treated mice into nude mice results in systemic autoim-
munity (80). Brief treatments of CsA reverse tolerance andinduce allograft rejection in a rat cardiac transplant model (87).Observations in our laboratory (T. L. Sumpter and D. S.Wilkes, unpublished data) also suggest that CsA may havedetrimental effects on Tregs in vitro. These data suggest thatimmunosuppressants, administered early in transplant, mayblock Treg development. In turn, blocking Tregs could aid thedevelopment of autoimmunity that contributes to the rejectionresponse.
FUTURE DIRECTIONS
Data showing that col(V) is an antigen during lung allograftrejection and col(V)-induced oral tolerance prevents lung al-lograft rejection raise several issues. The most important issueyet to be resolved lies in identifying the epitopes of col(V) thatare either tolerogenic or antigenic. This is intriguing, in that notall col(V)-reactive T cells induce pathology after adoptivetransfer (37). This suggests that there may be different anti-genic regions within col(V) that are recognized as antigensduring the rejection response. The difference between anti-genic and potentially tolerogenic peptides of col(V) could berelated to their primary sequence or affinity for TCRs. Datashowing that not all col(V)-reactive T cells induce diseasecould also be related to differential expression of costimulatorymolecules on these cells, rendering them less susceptible toactivation or more resistant to active suppression by Tregs.These questions are currently under investigation. Alterna-tively, strategies designed to block expression of Smad7 in Tcells could be a novel approach used to enhance Treg function.Finally, having been demonstrated in renal (8), heart (16), andlung allografts (37), the role of autoimmunity in the rejectionresponse is established. Because Tregs are believed to functionprimarily as suppressors of autoimmunity, more investigationsare needed to develop immunosuppressive regimens that pre-serve and enhance Treg function, resulting in the blockade ofalloimmunity and autoimmunity in the transplant recipient.
GRANTS
This work was supported by National Institutes of Health Grants HL-69727,HL-60797, and HL/AI-67177 (to D. S. Wilkes).
REFERENCES
1. Adams AB, Williams MA, Jones TR, Shirasugi N, Durham MM,Kaech SM, Wherry J, Onami T, Lanier JG, Kokko KE, PearsonTC, Ahmed R, and Larsen CP. Heterologous immunity provides apotent barrier to transplantation tolerance. J Clin Invest 111: 1887–1895, 2003.
2. Adorini L, Penna G, Giarratana N, and Uskokovic M. Tolerogenicdendritic cells induced by vitamin D receptor ligands enhance regulatoryT cells inhibiting allograft rejection and autoimmune diseases. J CellBiochem 88: 227–233, 2003.
3. Akbari O, DeKruyff RH, and Umetsu DT. Pulmonary dendritic cellsproducing IL-10 mediate tolerance induced by respiratory exposure toantigen. Nat Immun 2: 725–731, 2001.
4. Annunziato FL, Cosmi F, Liotta E, Lazzeri R, Manetti V, Vanini P,Romagnani E, Maggi S, and Romagnani S. Phenotype, localization,and mechanism of suppression of CD4�CD25� human thymocytes. JExp Med 196: 379–387, 2002.
5. Asano M, Toda M, Sakaguchi N, and Sakaguchi S. Autoimmunedisease as a consequence of developmental abnormality of a T cellsubpopulation. J Exp Med 184: 387–396, 1996.
6. Azuma T, Takahashi T, Kunisato A, Kitamura JT, and Hirai H.Human CD4�CD25� regulatory T cells suppress NKT function. CancerRes 63: 4516–4520, 2003.
Invited Review
L1136 TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

7. Benichou G, Valujskikh A, and Heeger PS. Contributions of direct andindirect T cell alloreactivity during allograft rejection in mice. J Immunol162: 352–358, 1999.
8. Birk OS, Gur SL, Elias D, Margalit R, Mor F, Carmi P, Bockova J,Altmann DM, and Cohon IR. The 60-kDa heat shock protein modulatesallograft rejection. Proc Natl Acad Sci USA 96: 5159–5163, 1999.
9. Bluestone JA and Abbas AK. Natural versus adaptive regulatory Tcells. Nat Rev Immunol 3: 253–257, 2003.
10. Boehler A, Kesten S, Weder W, and Speich R. Bronchiolitis obliteransafter lung transplantation. Chest 114: 1411–1426, 1998.
11. Bushnell A, Niimi M, Morris PJ, and Wood KJ. Evidence for immuneregulation in the induction of transplantation tolerance: a conditional butlimited role for IL-4. J Immunol 162: 1359–1366, 1999.
12. Chen C, Lee WH, Yun P, Snow P, and Liu CP. Induction ofautoantigen specific Th2 and Tr1 regulatory T cells and modulation ofautoimmune diabetes. J Immunol 171: 733–744, 2003.
13. Chen Y, Kuchroo VK, Inobe J, Hafler DA, and Weiner HL. Regu-latory T cell clones induced by oral tolerance: suppression of autoim-mune encephalomyelitis. Science 265: 1237–1240, 1994.
14. Cremer MA, Ye XJ, Terato K, Owens SW, Seyer JM, and Kang AH.Type XI collagen-induced arthritis in the Lewis rat. Characterization ofcellular and humoral immune responses to native types XI, V, and IIcollagen and constituent alpha-chains. J Immunol 153: 824–832, 1994.
15. Fedoseyeva EV, Kishimoto K, Rolls HK, Illigens BM, Dong VM,Valujskikh A, Heeger PS, Sayegh MH, and Benichou G. Modulationof tissue-specific immune response to cardiac myosin can prolong sur-vival of allogeneic heart transplants. J Immunol 169: 1168–1174, 2002.
16. Fedoseyeva EV, Zhang F, Orr PL, Levin D, Bunke HJ, and BenichouG. De novo autoimmunity to cardiac myosin after heart transplantationand its contribution to the rejection process. J Immunol 162: 6836–6842,1999.
17. Filaci G and Suciu-Foca N. CD8� T suppressor cells are back to thegame: are they players in autoimmunity? Autoimmun Rev 1: 279–283,2002.
18. Fontenot JD, Gavin MA, and Rudensky AY. Foxp3 programs thedevelopment and function of CD4�CD25� regulatory T cells. NatImmun 4: 330–336, 2003.
19. Ford MS, Young KJ, Zhang Z, Ohashi PS, and Zhang L. The immuneregulatory function of lymphoproliferative double negative T cells invitro and in vivo. J Exp Med 196: 261–267, 2002.
20. Furtado G, Curotto de Lafaille MA, and Kutchukhidze N. Interleukin2 signaling is required for CD4� regulatory T cell function. J Exp Med196: 851–857, 2002.
21. Garcia G and Weiner HL. Manipulation of Th responses by oraltolerance. Curr Top Microbiol Immunol 238: 123–145, 1999.
22. Gonzalez A, Andre-Schmutz I, Carnaud C, Mathis D, and Benoist C.Damage control, rather than unresponsiveness, effected by protectiveDX5� T cells in autoimmune diabetes. Nat Immun 2: 1117–1125, 2001.
23. Gorelik L and Flavell RA. Abrogation of TGFbeta signaling in T cellsleads to spontaneous T cell differentiation and autoimmune disease.Immunity 12: 171–181, 2000.
24. Gorelik L and Flavell RA. Transforming growth factor-� in T-cellbiology. Nat Rev Immunol 2: 46–53, 2002.
25. Goudy KS, Burkhardt BR, Wasserfall C, Song S, Campbell-Thomp-son ML, Brusko T, Powers MA, Clare-Salzler MJ, Sobel ES, EllisTM, Flotte TR, and Atkinson MA. Systemic overexpression of IL-10induces CD4�CD25� cell populations in vivo and ameliorates type 1diabetes in nonobese diabetic mice in a dose-dependent fashion. J Im-munol 171: 2270–2278, 2003.
26. Graca L, Cobbold SP, and Waldman H. Identification of regulatory Tcells in tolerated allografts. J Exp Med 195: 1641–1646, 2002.
27. Graca L, Thompson S, Lin CY, Adams E, Cobbold SP, and Wald-mann H. Both CD4�CD25� and CD4�CD25� regulatory cells me-diate dominant transplantation tolerance. J Immunol 168: 5558–5564,2002.
28. Grohmann U, Orabona C, Fallarino F, Vacca C, Calcinaro F,Falorni A, Candeloro P, Belladonna ML, Bianchi R, Fioretti MC,and Puccetti P. CTLA-4-Ig regulates tryptophan catabolism in vivo. NatImmun 3: 1097–1101, 2002.
29. Groux H. Type 1 T-regulatory cells: their role in the control of immuneresponses. Transplantation 15: 8S–12S, 2003.
30. Groux H, Bigler M, de Vries JE, and Roncarolo MG. Interleukin-10induces a long-term antigen-specific anergic state in human CD4� Tcells. J Exp Med 184: 19–29, 1996.
31. Guillet M, Brouard S, Gagne K, Sebille F, Cuturi MC, Delsuc MA,and Soulillou JP. Different qualitative and quantitative regulation of V�TCR transcripts during early acute allograft rejection and toleranceinduction. J Immunol 168: 5088–5095, 2002.
32. Hall BM, Jelbart ME, Gurley KE, and Dorsch S. Specific unrespon-siveness in rats with prolonged cardiac allograft survival after treatmentwith cyclosporine. Mediation of specific suppression by T helper/inducedcells. J Exp Med 162: 1683–1694, 1985.
33. Hall BM, Pearce NW, Gurley KE, and Dorsch SE. Specific unrespon-siveness in rats with prolonged cardiac allograft survival after treatmentwith cyclosporine. III. Further characterization of the CD4� suppressorcell and its mechanisms of action. J Exp Med 171: 141–157, 1990.
34. Halloran PF, Homik J, Goes N, Lui SL, Urmson J, Ramassar V, andCockfield SM. The “ injury response” : a concept linking nonspecificinjury, acute rejection, and long-term transplant outcomes. TransplantProc 29: 79–81, 1997.
35. Halloran PF, Kung L, and Noujaim J. Calcineurin and the biologicaleffect of cyclosporine and tacrolimus. Transplant Proc 30: 2167–2170,1998.
36. Hanson IM, Gorman P, Lui VC, Cheah KS, Solomon E, and Trows-dale J. The human alpha 2(XI) collagen gene (COL11A2) maps to thecentromeric border of the major histocompatibility complex on chromo-some 6. Genomics 5: 925–931, 1989.
37. Haque MA, Mizobuchi T, Yasufuku K, Fujisawa T, Brutkiewicz RR,Zheng Y, Woods K, Smith GN, Cummings OW, Heidler KM, BlumJS, and Wilkes DS. Evidence for immune responses to a self-antigen inlung transplantation: role of type V collagen-specific T cells in thepathogenesis of lung allograft rejection. J Immunol 169: 1542–1549,2002.
38. Hara M, Kingsley CI, Niimi M, Read S, Turvey SE, Bushell AR,Morris PJ, Powrie F, and Wood KJ. IL-10 is required for regulatory Tcells to mediate tolerance to alloantigens in vivo. J Immunol 166:3789–3796, 2001.
39. Harris PE, Cortesini R, and Suciu-Foca N. Indirect allorecognition insolid organ transplantation. Rev Immunogenet 1: 297–308, 1999.
40. Hayday A and Tigelaar R. Immunoregulation in the tissues by gamma-delta T cells. Nat Rev Immunol 3: 233–242, 2003.
41. Heidler KM, Baker K, Woods K, Schnizlein-Bick C, Cummings OW,Sidner R, Foresman B, and Wilkes DS. Instillation of allogeneic lungantigen-presenting cells deficient in expression of major histocompati-bility complex class I or II antigens have differential effects on localcellular and humoral immunity and on pathology in recipient murinelungs. Am J Respir Cell Mol Biol 23: 499–505, 2000.
42. Hernandez-Fuentes MP, Baker RJ, and Lechler RI. The alloresponse.Rev Immunogenet 1: 282–296, 1999.
43. Hori S, Takashi N, and Sakaguchi S. Control of regulatory T celldevelopment by the transcription factor Foxp3. Science 299: 1057–1061,2003.
44. Hosenpud JD, Bennett LE, Keck BM, Boucek MM, and Novick RJ.The registry of the International Society for Heart and Lung Transplan-tation: eighteenth official report–2001. J Heart Lung Transplant 20:805–815, 2001.
45. Huang M, Sharma S, Zhu LX, Keane MP, Luo J, Zhang L, BurdickMD, Lin YQ, Dohadwala M, Gardner B, Batra RK, Strieter RM, andDubinett SM. IL-7 inhibits fibroblast TGF-beta production and signalingin pulmonary fibrosis. J Clin Invest 109: 931–937, 2002.
46. Huss R. In vitro determination of self-reactivity in the early postcyclos-porine period. Transpl Immunol 1: 228–245, 1993.
47. Inobe J, Slavin AJ, Komagata Y, Chen Y, Liu L, and Weiner HL.IL-4 is a differentiation factor for transforming growth factor-beta se-creting Th3 cells and oral administration of IL-4 enhances oral tolerancein experimental allergic encephalomyelitis. Eur J Immunol 28: 2780–2790, 1998.
48. Ishido N, Matsuoka J, Matsuno T, Nakagawa K, and Tanaka N.Induction of donor-specific hyporesponsiveness and prolongation ofcardiac allograft survival by jejunal administration of donor splenocytes.Transplantation 68: 1377–1382, 1999.
49. Itoh M, Takahashi T, Sakaguchi N, Kuniyasu Y, Shimizu J, OtsukaF, and Sakaguchi S. Thymus and autoimmunity: production ofCD25�CD4� naturally anergic and suppressive T cells as a key functionof the thymus in maintaining immunologic self-tolerance. J Immunol162: 5317–5326, 1999.
50. Izutani H, Miyagawa S, Shirakura R, Matsumiya G, Nakata S,Shimazaki Y, and Matsuda H. Evidence that graft coronary arterio-
Invited Review
L1137TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from

sclerosis begins in the early phase after transplantation and progresseswithout chronic immunoreaction. Transplantation 60: 1073–1079, 1995.
51. Jørgensen KA, Koefoed-Nielsen PB, and Karamperis N. Calcineurinphosphatase activity and immunosuppression. A review on the role ofcalcineurin phosphatase activity and the immunosuppressive effect ofcyclosporin A and tacrolimus. Scand J Immunol 57: 93–98, 2003.
52. Keenan RJ and Zeevi A. Immunologic consequences of transplantation.Chest Surg Clin N Am 5: 107–120, 1995.
53. Kemper C, Chan AC, Green JM, Brett KA, Murphy KM, andAtkinson JP. Activation of human CD4� cells with CD3 and CD46induces a T-regulatory cell 1 phenotype. Nature 421: 388–392, 2003.
54. Khattri R, Kasprowicz D, Cox T, Mortrud M, Appleby MW,Brunkow ME, Ziegler SF, and Ramsdell F. The amount of scurfinprotein determines peripheral T cell number and responsiveness. J Im-munol 167: 6312–6320, 2001.
55. Kingsley CI, Karim M, Bushnell AR, and Wood KJ. CD25�CD4�regulatory T cells prevent graft rejection: CTLA-4 and IL-10-dependentimmunoregulation of alloresponses. J Immunol 168: 1080–1086, 2002.
56. Konichezky S, Schattner A, Ezri T, Bokenboim P, and Geva D.Thionyl-chloride-induced lung injury and bronchiolitis obliterans. Chest104: 971–973, 1993.
57. Konomi H, Hayashi T, Nakayasu K, and Arima M. Localization oftype V collagen and type IV collagen in human cornea, lung, and skin.Immunohistochemical evidence by anti-collagen antibodies character-ized by immunoelectroblotting. Am J Pathol 116: 417–426, 1984.
58. Levings MK, Sangregorio R, Sartirana C, Moschin AL, Battaglia M,Orban PC, and Roncarolo MG. Human CD25�CD4� T suppressorcell clones produce transforming growth factor beta, but not interleukin10 and are distinct from type 1 T regulatory cells. J Exp Med 196:1335–1346, 2002.
59. Liu J. FK506 and cyclosporin, molecular probes for studying intracel-lular signal transduction. Immunol Today 14: 290–295, 1993.
60. Luz JG, Huang M, Garcia KC, Rudolph MG, Apostolopoulos V,Teyton L, and Wilson IA. Structural comparison of allogeneic andsyngeneic T cell receptor-peptide-major histocompatibility complexcomplexes: a buried alloreactive mutation subtly alters peptide presen-tation substantially increasing V(beta) interactions. J Exp Med 195:1175–1186, 2002.
61. McHugh RS and Shevach EM. The role of suppressor T cells inregulation of immune responses. J Allergy Clin Immunol 110: 693–702,2002.
62. McHugh RS, Whitters MJ, Piccirillo CA, Young DA, Shevach EM,Collins M, and Byrne MC. CD4�CD25� immunoregulatory T cells:gene expression analysis reveals a functional role for the glucocorticoid-induced TNF receptor. Immunity 16: 311–323, 2002.
63. Madri JA and Furthmayr H. Isolation and tissue localization of typeAB2 collagen from normal lung parenchyma. Am J Pathol 94: 3323–3331, 1979.
64. Madri JA and Furthmayr H. Collagen polymorphism in the lung. Animmunochemical study of pulmonary fibrosis. Hum Pathol 11: 353–366,1980.
65. Mares DC, Heidler KM, Smith GN, Cummings OW, Harris ER,Foresman B, and Wilkes DS. Type V collagen modulates alloantigen-induced pathology and immunology in the lung. Am J Respir Cell MolBiol 23: 62–70, 2000.
66. Min WP, Zhou D, Ichin TE, Strejan GH, Xia X, Yang J, Huang X,Garcia B, White D, Dutartre P, Jevnikar AM, and Zhong R. Inhib-itory feedback loop between tolerogenic dendritic cells and regulatory Tcells in transplant tolerance. J Immunol 170: 1304–1312, 2003.
67. Mizobuchi T, Yasufuku K, Zheng Y, Haque MA, Heidler KM,Woods K, Smith GN Jr, Cummings OW, Fujisawa T, Blum JS, andWilkes DS. Differential expression of Smad7 transcripts identifies theCD4(�)CD45RC(high) regulatory T cells that mediate type V collagen-induced tolerance to lung allografts. J Immunol 171: 1140–1147, 2003.
68. Monteleone G, Kumberova A, Croft NM, McKenzie C, Steer HW,and MacDonald TT. Blocking Smad7 restores TGF-beta1 signaling inchronic inflammatory bowel disease. J Clin Invest 108: 601–609, 2001.
69. Nakamura K, Kitani A, and Strober W. Cell contact-dependentimmunosuppression by CD4(�)CD25(�) regulatory T cells is mediatedby cell surface-bound transforming growth factor beta. J Exp Med 194:629–644, 2001.
70. Nakao A, Afrakhte M, Moren A, Nakayama T, Christian JL,Heuchel R, Itoh S, Kawabata M, Heldin NE, Heldin CH, and ten
Dijke P. Identification of Smad7, a TGFbeta-inducible antagonist ofTGF-beta signalling. Nature 389: 631–635, 1997.
71. Nakao A, Milke S, Hatano M, Okumura K, Tokuhisa T, Ra C, andIwamato I. Blockade of transforming growth factor �/Smad signaling inT cells by overexpression of Smad7 enhances antigen-induced airwayinflammation and airway reactivity. J Exp Med 192: 151–158, 2000.
72. Niimi M, Ikeda Y, Shirasugi N, Shatari T, Takami H, Kodaira S,Matsumoto K, Hamano K, Esato K, Hara M, and Wood KJ. Oraldelivery of alloantigen combined with non-depleting anti-CD4 monoclo-nal antibody induces indefinite survival of cardiac allografts and gener-ates CD4� regulatory T cells. Transplant Proc 32: 2035, 2000.
73. Oida T, Zhang X, Goto M, Hachimura S, Totsuka M, KaminogawaS, and Weiner HL. CD4�CD25� T cells that express latency-associ-ated peptide on the surface suppress CD4�CD45RB high-induced colitisby a TGF-beta-dependent mechanism. J Immunol 170: 2516–2522, 2003.
74. Pabst R, Luhrmann A, Steinmetz I, and Tschernig T. A singleintratracheal dose of the growth factor Fms-like tyrosine kinase recep-tor-3 ligand induces a rapid differential increase of dendritic cells andlymphocyte subsets in lung tissue and bronchoalveolar lavage, resultingin an increased local antibody production. J Immunol 171: 325–330,2003.
75. Papiernik M, de Moraes ML, Pontoux C, Vasseur F, and Penit C.Regulatory CD4 T cells: expression of IL-2R� chain, resistance to clonaldeletion and IL-2 dependency. Int Immunol 10: 371–378, 1998.
76. Piccirillo CA and Shevach EM. Control of CD8� T cell activation byCD4�CD25� immunoregulatory cells. J Immunol 167: 1137–1140,2001.
77. Powrie F, Correa-Oliveira R, Mauze S, and Coffman R. Regulatoryinteractions between CD45RB high and CD45RB low CD4� T cells areimportant for the balance between protective and pathogenic cell-medi-ated immunity. J Exp Med 179: 589–600, 1994.
78. Read S, Mauze S, Asseman C, Bean A, Coffman R, and Powrie F.CD38�CD45RB low CD4� T cells: a population of T cells withimmune regulatory activities in vitro. Eur J Immunol 28: 3435–3447,1998.
79. Sadlack BJ, Lohler J, Schorle H, Klebb G, Haber H, Sickel E, NoelleRJ, and Horak I. Generalized autoimmune disease in interleukin-2-deficient mice is triggered by an uncontrolled activation and proliferationof CD4� T cells. Eur J Immunol 25: 3053–3059, 1995.
80. Sakaguchi S and Sakaguchi N. Thymus and autoimmunity. Transplan-tation of the thymus from cyclosporin A-treated mice causes organ-specific autoimmune disease in athymic nude mice. J Exp Med 167:1479–1485, 1988.
81. Sakaguchi S and Sakaguchi N. Organ-specific autoimmune diseaseinduced in mice by elimination of T cell subsets. V. Neonatal adminis-tration of cyclosporin A causes autoimmune disease. J Immunol 14:2471–2480, 1989.
82. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, and Toda M. Immu-nologic self-tolerance maintained by activated T cells expressing IL-2receptor �-chains (CD25). J Immunol 155: 1151–1164, 1995.
83. Sanchez-Fueyo A, Weber M, Domenig C, Strom TB, and Zheng XX.Tracking the immunoregulatory mechanisms active during allograft tol-erance. J Immunol 168: 2274–2281, 2002.
84. Sayegh MH. Why do we reject a graft? Role of indirect allorecognitionin graft rejection. Kidney Int 56: 1967–1979, 1999.
85. Scholma J, Slebos DJ, Boezen HM, van den Berg JWK, van der BIJ,de Boer WJ, Koeter GH, Timens W, Kauffman HF, and Postma DS.Eosinophilic granulocytes and interleukin-6 level in bronchoalveolarlavage fluid are associated with the development of obliterative bronchi-olitis after lung transplantation. Am J Respir Crit Care Med 162:2221–2225, 2000.
86. Schubert LA, Jeffrey E, Zhang Y, Ramsdell F, and Zeigler SF.Scurfin (Foxp3) acts as a repressor of transcription and regulates T cellactivation. J Biol Chem 40: 37672–37679, 2001.
87. Smith CR, Mohanakumar T, Shimuizu Y, Yu S, Otomo N, Kaleem Z,and Fly MW. Brief cyclosporine treatment prevents intrathymic (IT)tolerance induction and precipitates acute rejection in an IT rat cardiacallograft model. Transplantation 69: 294–299, 2000.
88. Starr TK, Jameson SC, and Hogquist KA. Positive and negativeselection of T cells. Annu Rev Immunol 21: 139–176, 2003.
89. Suzuki H, Kundig TM, Furlonger C, Wakeham A, Timms E, Mat-suyama T, Schmits R, Simard JJL, Ohashi PS, Griesser H, Tanigu-chi T, Paige CJ and Mak TW. Deregulated T cell activation and
Invited Review
L1138 TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from
autoimmunity in mice lacking interleukin-2 receptor beta. Science 268:1472–1476, 1995.
90. Taams LS, Smith J, Rustin MH, Salmon M, Poulter LW, and AkbarAN. Human anergic/suppressive CD4�CD25� T cells: a highly differ-entiated and apoptosis-prone population. Eur J Immunol 31: 1122–1131,2001.
91. Takahashi T, Kuniyasu Y, Toda M, Sakaguchi N, Itoh M, Iwata M,Shimizu J, and Sakaguchi S. Immunological self-tolerance maintainedby CD35�CD4� naturally anergic and suppressive T cells: induction ofautoimmune disease by breaking their anergic state. Int Immunol 10:969–1980, 1998.
92. Tasaka S, Kanazawa M, Mori M, Fujishima S, Ishizaka A, Yama-sawa F, and Kawashiro T. Long-term course of bronchiectasis andbronchiolitis obliterans as a late complication of smoke inhalation.Respiration 62: 40–42, 1995.
93. Tejani A and Emmett L. Acute and chronic rejection. Semin Nephrol21: 498–507, 2001.
94. Thorton AM and Shevach EM. CD4�CD25� immunoregulatory Tcells suppress polyclonal T cell activation in vitro by inhibiting interleu-kin 2 production. J Exp Med 188: 287–296, 1998.
95. Thornton AM and Shevach EM. Suppressor effector function ofCD4�CD25� immunoregulatory T cells is antigen non-specific. J Im-munol 164: 183–190, 2000.
96. Trello CA, Williams DA, Keller CA, Crim C, Webster RO, and OharJA. Increased gelatinolytic activity in bronchoalveolar lavage fluid instable lung transplant recipients. Am J Respir Crit Care Med 156:1978–1986, 1997.
97. Tullius SG, Hancock WW, Heemann U, Azuma H, and Tilney NL.Reversibility of chronic renal allograft rejection. Transplantation 58:93–99, 1994.
98. Ulloa L, Doody J, and Massague J. Inhibition of transforming growthfactor-beta/SMAD signalling by the interferon-gamma/STAT pathway.Nature 397: 710–713, 1999.
99. Valujskikh A, Fedoseyeva E, Benichou G, and Heeger PS. Develop-ment of autoimmunity after skin graft rejection via an indirect allore-sponse. Transplantation 73: 1130–1137, 2002.
100. Valujskikh A, Lantz O, Celli S, Matzinger P, and Heeger PS.Cross-primed CD8� T cells mediate graft rejection via a distinct effectorpathway. Nat Immun 3: 844–851, 2002.
101. Van Kuppevelt TH, Veerkamp JH, and Timmermans JA. Immuno-quantification of type I, III, IV and V collagen in small samples of humanlung parenchyma. Int J Biochem Cell Biol 27: 775–782, 1995.
102. Van Maurik A, Herver M, Wood KJ, and Jones ND. CD4�CD25�alloantigen-specific immunoregulatory cells that can prevent CD8� Tcell-mediated graft rejection: implications for anti-CD154 immunother-apy. J Immunol 169: 5401–5404, 2002.
103. Vilchez RA, Dauber J, and Kusne S. Infectious etiology of bronchi-olitis obliterans: the respiratory viruses connection-myth or reality? Am JTransplant 3: 245–249, 2003.
104. Waldmann H and Cobbold S. Regulating the immune response totransplants: a role for CD4� regulatory cells? Immunity 14: 399–406,2001.
105. Weiner HL. Oral tolerance, an active immunologic process mediated bymultiple mechanisms. J Clin Invest 106: 935–937, 2000.
106. Weiner HL. Oral tolerance: immune mechanisms and the generation ofTh3-type TGF-beta-secreting regulatory cells. Microbes Infect 3: 947–954, 2001.
107. Wildin RS, Smyk-Pearson S, and Filipovich AH. Clinical and molec-ular features of the immunodysregulation, polyendocrinopathy, enterop-athy, X linked (IPEX) syndrome. J Med Genet 39: 537–545, 2002.
108. Wilkes DS, Heidler KM, Bowen LK, Quinlan WM, Doyle NA,Cummings OW, and Doerschuk CM. Allogeneic bronchoalveolarlavage cells induce the histology of acute lung allograft rejection, anddeposition of IgG2a in recipient murine lungs. J Immunol 155: 2775–2783, 1995.
109. Willerford DM, Chen J, Ferry JA, Davidson L, Ma A, and Alt FW.Interleukin-2 receptor alpha chain regulates the size and content of theperipheral lymphoid compartment. Immunity 3: 521–530, 1995.
110. Wing K, Ekmark A, Karlsson H, Rudin A, and Suri-Payer E.Characterization of human CD25�CD4� T cells in thymus, cord andadult blood. Immunology 106: 190–199, 2002.
111. Wise MP, Bemelman F, Cobbold SP, and Waldmann H. Cutting edge:linked suppression of skin graft rejection can operate through indirectrecognition. J Immunol 161: 5813–5816, 1998.
112. Wood KJ and Sakaguchi S. Regulatory T cells in transplantationtolerance. Nat Rev Immunol 3: 199–210, 2003.
113. Yamagiwa S, Gray JD, Hashimoto S, and Horwitz DA. A role forTGF-beta in the generation and expansion of CD4�CD25� regulatory Tcells from human peripheral blood. J Immunol 166: 7282–7289, 2001.
114. Yasufuku K, Heidler KM, O’Donnell PW, Smith GN Jr, CummingsOW, Foresman BH, Fujisawa T, and Wilkes DS. Oral toleranceinduction by type V collagen downregulates lung allograft rejection.Am J Respir Cell Mol Biol 25: 26–34, 2001.
115. Yasufuku K, Heidler KM, Woods KA, Smith GN Jr, Cummings OW,Fujisawa T, and Wilkes DS. Prevention of bronchiolitis obliterans in ratlung allografts by type V collagen-induced oral tolerance. Transplanta-tion 73: 500–505, 2002.
116. Yvon ES, Vigouroux S, Rousseau RF, Biagi E, Amrolia P, Dotti G,Wagner HJ, and Brenner MK. Overexpression of the Notch ligand,Jagged-1, induces alloantigen-specific human regulatory T cells. Blood102: 3815–3821, 2003.
117. Zhai Y, Li J, Hammer M, Busuttil RW, Volk HD, and Kupiec-Weglinski JW. Evidence of cells clonality in the infectious tolerancepathway: implications toward identification of regulatory T cells. Trans-plantation 12: 1701–1708, 2001.
118. Zhang X, Izikson L, Liu L, and Weiner HL. Activation ofCD25(�)CD4(�) regulatory T cells by oral antigen administration.J Immunol 167: 4245–4253, 2001.
119. Zhang ZX, Yang L, Young KJ, DuTemple B, and Zhang L. Identi-fication of a previously unknown antigen-specific regulatory T cell andits mechanism of suppression. Nat Med 6: 782–789, 2000.
120. Zheng SG, Gray JD, Ohtsuka K, Yamagiwa S, and Horwitz DA.Generation ex vivo of TGF-beta-producing regulatory T cells fromCD4�CD25� precursors. J Immunol 169: 4183–4189, 2002.
121. Zucker S, Hymowitz M, Conner C, Zarrabi HM, Hurewitz AN,Matrisian L, Boyd D, Nicolson G, and Montana S. Measurement ofmatrix metalloproteinases and tissue inhibitors of metalloproteinases inblood and tissues. Clinical and experimental applications. Ann NY AcadSci 878: 212–227, 1999.
Invited Review
L1139TYPE V COLLAGEN IN LUNG TRANSPLANT REJECTION
AJP-Lung Cell Mol Physiol • VOL 286 • JUNE 2004 • www.ajplung.org
on Novem
ber 12, 2009 ajplung.physiology.org
Dow
nloaded from


















