Thyroid & Parathyroid Chapter
94
44 Thyroid and Parathyroid John K. C. Chan The Thyroid Gland NEOPLASTIC LESIONS Classification General Considerations Follicular Adenoma Follicular Carcinoma Papillary Carcinoma Poorly Differentiated Thyroid Carcinoma Anaplastic (Undifferentiated) Carcinoma Columnar Cell Carcinoma Mucoepidermoid Carcinoma Sclerosing Mucoepidermoid Carcinoma with Eosinophilia Mucinous Carcinoma Medullary Thyroid Carcinoma Collision Tumor Mixed Follicular-Parafollicular Carcinoma Thymic and Related Branchial Pouch Tumors of the Thyroid Intrathyroid Parathyroid Tumor Malignant Lymphoma Plasmacytoma of the Thyroid Langerhans Cell Histiocytosis (Histiocytosis X) Angiosarcoma Solitary Fibrous Tumor Other Mesenchymal Tumors Paraganglioma Teratoma Metastatic Malignant Neoplasms in Thyroid Contents of the Final Surgical Pathology Report NON-NEOPLASTIC LESIONS Incidental and Insignificant Findings in the Thyroid Gland Cysts Thyroid Tissue in the Lateral Neck Thyroiditis Graves’ Disease Nodular Goiter Dyshormonogenetic Goiter Fine-Needle Aspiration–Associated Changes in the Thyroid Gland Amyloid Goiter Black Thyroid Uncommon Lesions of the Thyroid Gland The Parathyroid Gland NEOPLASTIC LESIONS Classification General Considerations Parathyroid Adenoma Parathyroid Carcinoma Contents of the Final Surgical Pathology Report NON-NEOPLASTIC LESIONS Primary Parathyroid Chief Cell Hyperplasia Primary Water-Clear Cell Hyperplasia Secondary Parathyroid Hyperplasia Parathyroid Cyst Periparathyroid Salivary Heterotopia–Cyst Unit Amyloidosis A. The Thyroid Gland NEOPLASTIC LESIONS Classification The primary tumors of the thyroid gland, grouped according to the line of differentiation, include the following. 1 Tumors of Thyroid Follicular Epithelium Follicular adenoma, including Hu ¨ rthle cell ade- noma Follicular carcinoma, including Hu ¨ rthle cell car- cinoma Papillary carcinoma 3 Copyright 2003, Elsevier Science (USA). All rights Reserved
-
Upload
shriniwas-rushi -
Category
Documents
-
view
87 -
download
4
description
Thyroid & Parathyroid Chapter
Transcript of Thyroid & Parathyroid Chapter

44
Thyroid and ParathyroidJohn K. C. Chan
The Thyroid GlandNEOPLASTIC LESIONS
ClassificationGeneral ConsiderationsFollicular AdenomaFollicular CarcinomaPapillary CarcinomaPoorly Differentiated Thyroid CarcinomaAnaplastic (Undifferentiated) CarcinomaColumnar Cell CarcinomaMucoepidermoid CarcinomaSclerosing Mucoepidermoid Carcinoma with
EosinophiliaMucinous CarcinomaMedullary Thyroid CarcinomaCollision TumorMixed Follicular-Parafollicular CarcinomaThymic and Related Branchial Pouch Tumors of the
ThyroidIntrathyroid Parathyroid TumorMalignant LymphomaPlasmacytoma of the ThyroidLangerhans Cell Histiocytosis (Histiocytosis X)AngiosarcomaSolitary Fibrous TumorOther Mesenchymal TumorsParagangliomaTeratomaMetastatic Malignant Neoplasms in ThyroidContents of the Final Surgical Pathology Report
NON-NEOPLASTIC LESIONSIncidental and Insignificant Findings in the Thyroid
GlandCystsThyroid Tissue in the Lateral NeckThyroiditisGraves’ DiseaseNodular GoiterDyshormonogenetic GoiterFine-Needle Aspiration–Associated Changes in the
Thyroid GlandAmyloid GoiterBlack ThyroidUncommon Lesions of the Thyroid Gland
The Parathyroid GlandNEOPLASTIC LESIONS
ClassificationGeneral ConsiderationsParathyroid AdenomaParathyroid CarcinomaContents of the Final Surgical Pathology Report
NON-NEOPLASTIC LESIONSPrimary Parathyroid Chief Cell HyperplasiaPrimary Water-Clear Cell HyperplasiaSecondary Parathyroid HyperplasiaParathyroid CystPeriparathyroid Salivary Heterotopia–Cyst UnitAmyloidosis
A. The Thyroid Gland
NEOPLASTIC LESIONS
Classification
The primary tumors of the thyroid gland, groupedaccording to the line of differentiation, include thefollowing.1
Tumors of Thyroid FollicularEpithelium
Follicular adenoma, including Hurthle cell ade-noma
Follicular carcinoma, including Hurthle cell car-cinoma
Papillary carcinoma
3
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
Copyright � 2003, Elsevier Science (USA). All rights Reserved

4
TABLE 44–1. Immunohistochemical Staining Profile of the Various Thyroid Neoplasms
Tumor Type Cytokeratin
Pan-neuroendocrine Markers(such as synaptophysin,chromogranin) Thyroglobulin Calcitonin
Thyroid TranscriptionFactor 1 Other Markers
Papillary carcinoma; follicularadenoma-carcinoma; poorlydifferentiated thyroid carci-noma; columnar cell carci-noma
Positive Negative Positive Negative Positive —
Medullary carcinoma Positive Positive Negative Positive Positive Carcinoembryonic an-tigen (CEA)�; S-100�
sustentacular cellsmay be present inhereditary form
Mixed follicular-parafollicularcarcinoma
Positive Positive Positive Positive Positive —
Anaplastic carcinoma Variable (positive in �50%of cases)
Negative Negative Negative Usually negative —
Angiosarcoma Variable (usually negative,but sometimes positive)
Negative Negative Negative Negative Positive for endothe-lial markers, such asCD31, CD34, factorVIII
Malignant lymphoma Negative Negative Negative Negative Negative Leukocyte commonantigen� and otherlymphoid markers�
Carcinoma showing thymus-like element (CASTLE)
Positive Negative Negative Negative Negative CD5�
Intrathyroid parathyroid tumor Positive Positive Negative Negative Negative Parathyroid hormone�
Paraganglioma Negative Positive Negative Negative Negative S-100� sustentacularcells; CEA�
38419W
eidner
(SAU
NM
)L
EFT
INT
ER
AC
TIV
E
shortstand
ardlong
topof
RH
Copyright
�2003,E
lsevierScience
(USA
).All
rightsR
eserved

Thyroid and Parathyroid 5
Poorly differentiated thyroid carcinoma, includ-ing insular carcinoma
Anaplastic carcinoma, squamous cell carcinoma,and carcinosarcoma
Rare tumor types: columnar cell carcinoma, mu-coepidermoid carcinoma, sclerosing muco-epidermoid carcinoma with eosinophilia,mucinous carcinoma
Tumors Showing C Cell orSimultaneous Follicular and C CellDifferentiation
Medullary carcinomaCollision tumor: follicular and medullary carci-
nomas or papillary and medullary carcino-mas
Mixed follicular-parafollicular carcinoma (differ-entiated thyroid carcinoma, intermediatetype)
Ectopic Tumors
Ectopic thymomaSpindle epithelial tumor with thymus-like ele-
ment (SETTLE)Carcinoma showing thymus-like element (CAS-
TLE)Intrathyroid parathyroid adenoma and carci-
noma
Tumors of Hematolymphoid Cells
Malignant lymphomaPlasmacytomaLangerhans cell histiocytosis
Mesenchymal and Other Tumors
Benign and malignant mesenchymal tumors,such as solitary fibrous tumor, smooth mus-cle tumor, peripheral nerve sheath tumor,angiosarcoma
ParagangliomaTeratoma
The most common primary thyroid cancer ispapillary carcinoma, which accounts for 60% to 80%of all cases, followed by follicular carcinoma, whichaccounts for 10% to 20% of cases. Most thyroid tu-mors can be readily diagnosed on morphologic as-sessment alone. Nonetheless, in some circumstances,especially with medullary carcinoma or unusual-looking tumors, immunohistochemical studies arerequired for a definitive classification. The immuno-histochemical profiles of the more common thyroidtumors are shown in Table 44–1.2–5
General Considerations
PATHOGENESISSome risk factors for development of thyroid cancerhave been identified; radiation exposure is the best
documented factor.6 External radiation was oncepopularly used to treat patients with a variety ofbenign disorders of the head and neck region, suchas acne, tinea capitis, cervical tuberculous lymphad-enitis, and thymic enlargement; such patients havean increased chance of developing thyroid cancer.Cancer patients treated with radiation have beenshown to have an excess of thyroid cancer com-pared with control subjects. Survivors of the Hiro-shima atomic bomb have a high risk for develop-ment of thyroid cancer; persons who were youngerthan 10 years when they were exposed have an ex-cess relative risk of 9.46. The Chernobyl nuclear ac-cident in 1986 provides further evidence of the im-portance of radiation in thyroid carcinogenesis; insome exposed areas, the incidence of thyroid cancerin children increased from 0.5 per million per yearto 96.4 per million per year. The clinicopathologicfeatures of the Chernobyl accident–associated thy-roid cancers are listed in Table 44–2.
Iodine deficiency and endemic goiter are associ-ated with an increased risk of thyroid carcinomaand angiosarcoma. It has been postulated that thetumors may result from prolonged stimulation ofthe thyroid tissues by thyroid-stimulating hormone.7
Hashimoto’s thyroiditis and lymphocytic thy-roiditis are associated with an increased risk for ma-lignant lymphoma. In addition, sclerosing mucoepi-dermoid carcinoma with eosinophilia almost alwaysarises in a setting of fibrosing Hashimoto’s thyroidi-tis. Hashimoto’s thyroiditis may slightly increase therisk for development of papillary carcinoma.8
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–2. Features of Chernobyl Nuclear Accident-Associated Thyroid Cancer
It is caused by exposure to radioactive iodine fallout; the acci-dent occurred on April 26, 1986.
Most cases are papillary carcinomas (�95%). The papillary car-cinomas often show a follicular, solid, or mixed follicular-papillary-solid pattern, contrasting with the typical papillarypattern seen in sporadic papillary carcinomas in children.
The incidence of thyroid cancer in areas around Chernobyl hasincreased 6- to 500-fold compared with previous years, de-pending on the distance from the accident site. The greatestnumber of cases occur in areas where the thyroid radiationdose is �0.5 gy.
The tumors show greater aggressiveness at presentation, suchas extrathyroidal extension, venous invasion, and lymphnode metastasis. Thus, treatment often entails total thyroid-ectomy and lymph node dissection.
Lymphocytic thyroiditis and antithyroperoxidase antibody aremore common than in sporadic cases.
Age at diagnosis is usually �14 years, which is younger thanfor the sporadic thyroid cancers in children not related to anuclear accident.
The time interval between the nuclear accident and the diag-nosis of thyroid cancer is �6–7 years.
Subjects younger than 5 years or in utero at the time of thenuclear accident account for the majority of cases.
Papillary carcinomas occurring in this setting show a muchhigher frequency of RET/PTC (especially RET/PTC3) gene rear-rangement compared with sporadic cases.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

6 Endocrine System
Thyroid cancer can occur as a component ofsome heritable syndromes.8, 9 Medullary carcinomais a key component of multiple endocrine neoplasiatype 2 (MEN 2) or familial medullary thyroid carci-noma. Thyroid adenoma or carcinoma sometimesoccurs as a component of MEN type 1 (MEN 1).Some patients with familial adenomatous polyposisdevelop thyroid cancer, most commonly papillarycarcinoma of the cribriform-morular variant (so-called familial adenomatous polyposis–associatedthyroid carcinoma). Thyroid tumors also constitute a
component of Cowden’s disease and may includefollicular adenoma, follicular carcinoma, and papil-lary carcinoma. There are also less well defined fa-milial nonmedullary thyroid cancer syndromes.
GRADING AND STAGINGThe TNM staging is the most widely used stagingsystem for thyroid cancer (Table 44–3). There are nouniversally accepted grading systems for thyroidcancers, although the histologic grade may be im-plied from the histologic type (e.g., low grade for
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–3. Staging of Thyroid Tumors
TNM Staging
Primary Tumor (T)All categories may be subdivided: (a) solitary; (b) multifocal—the largest is measured for classificationTX Primary tumor cannot be assessedT0 No evidence of primary tumorT1 Tumors �1 cm, limited to the thyroidT2 Tumor 1–4 cm, limited to the thyroidT3 Tumor �4 cm, limited to the thyroidT4 Tumor of any size extending beyond thyroid capsule
Lymp Node (N)NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasisN1a Metastasis in ipsilateral cervical lymph nodesN1b Metastasis in bilateral, midline or contralateral cervical, or upper mediastinal lymph nodes
Distant Metastasis (M)MX Presence of distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Papillary or Follicular Carcinoma
Stage �45 y �45 y
I Any T, any N, M0 T1, N0, M0
II Any T, any N, M1 T2, N0, M0T3, N0, M0
III — T4, N0, M0Any T, N1, M0
IV — Any T, any N, M1
Medullary Carcinoma
Stage TNM status
I T1, N0, M0
II T2, N0, M0T3, N0, M0T4, N0, M0
III Any T, N1, M0
IV Any T, any N, M1
Anaplastic CarcinomaAll cases are stage IV (i.e., any T, any N, any M)
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 7
papillary and follicular carcinomas, and high gradefor anaplastic carcinoma).
PROGNOSTIC FEATURESThe different types of thyroid cancers have a num-ber of significant prognostic factors in common.
• Age younger than 40 years is a highly favorableprognostic factor.10
• Small tumor size (especially is a favorable�1 cm)prognostic factor.
• Tumor stage (intrathyroid tumor versus presenceof extrathyroidal extension; presence or absence ofmetastasis) is a highly significant prognostic fac-tor.10–12
According to the Surveillance, Epidemiology,and End Results study,10 the 10-year relative sur-vival rates of the major thyroid carcinomas are asfollows: papillary carcinoma, 0.98; follicular carci-noma, 0.92; medullary carcinoma, 0.80; and anaplas-tic carcinoma, 0.13. Papillary carcinoma and follicu-lar carcinoma are sometimes lumped together in onecategory of “differentiated thyroid carcinoma” inclinical studies, but this is not advisable becausethey show different clinical and biologic features.
THERAPYThe mainstay of therapy for thyroid tumors is surgi-cal excision, and the extent of surgery depends onthe tumor type. For thyroid carcinomas that cantake up iodine (such as follicular carcinoma, papil-lary carcinoma, and poorly differentiated thyroidcarcinoma), radioactive iodine is sometimes adminis-tered after total thyroidectomy so that residual mi-croscopic tumor can be eradicated. Thyroxine is also
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
commonly given postoperatively to suppress thy-roid-stimulating hormone activity in the hope of re-ducing tumor recurrence. External radiation therapyand chemotherapy are often reserved for uncontrol-lable disease or highly aggressive tumors.
TISSUE PROCUREMENTFine-Needle AspirationIn recent years, fine-needle aspiration cytology
has become the first-line screening or diagnostic pro-cedure for patients presenting with a thyroidmass.13, 14 The technique is popular because the pro-cedure is simple and relatively nontraumatic, withgood acceptance by patients. In experienced hands,the false-positive rate and false-negative rate(� 0%)(7% to 10%) are low.15 The diagnostic categories andtheir rationale are listed in Table 44–4. By use of thecytologic diagnosis for triage, patients with a diag-nosis of tumor or who are suspected of having tu-mor can be selected for early operation. Thoseshown on cytologic assessment to have non-neoplas-tic lesions (such as cyst or colloid nodule) can befollowed up; repeated fine-needle aspiration may berequired during follow-up to rule out a missed neo-plasm.15, 16
Core Needle BiopsyCore or large needle biopsy is performed in
some centers either as the sole procedure or as acomplementary procedure to fine-needle aspirationfor the initial investigation of thyroid nodules.17–22
The procedure is more traumatic than fine-needleaspiration, but the yield is generally higher, permit-ting more accurate diagnosis to be made in somecases.
TABLE 44–4. Diagnostic Categories from Fine-Needle Aspiration Cytology of the Thyroid
Cytologic Diagnosis Rationale
Inadequate for diagnosis With the exception of cyst (which can be hypocellular, with only macrophagesbeing identified), the minimal criterion for adequacy of a specimen is the pres-ence of 5–6 groups of thyroid follicular epithelium with �10 cells per group.
Benign, e.g., nodular goiter, cyst, Hashi-moto’s thyroiditis
Nodular goiter can usually be recognized by features such as abundant thickcolloid, low cellularity, large follicles, and honeycombed arrangement of nucleiin the epithelial fragments.
Follicular lesion It can be difficult to make a distinction between cellular adenomatoid nodule andfollicular neoplasm. In such situations, the descriptive term follicular lesion isapplicable.
Follicular neoplasm It is not possible to make a distinction between follicular carcinoma and follicularadenoma on the basis of fine-needle aspiration cytology because diagnosis offollicular carcinoma requires demonstration of vascular or capsular invasion.
Suspicious of malignancy A diagnosis of “suspicious of malignancy” is justified if there are cytologic fea-tures suggestive of but not diagnostic of malignancy.
Malignant neoplasm, e.g., papillary carci-noma, medullary carcinoma, anaplasticcarcinoma, lymphoma
Papillary carcinoma, medullary carcinoma, anaplastic carcinoma, and malignantlymphoma can often be diagnosed on the basis of fine-needle aspiration sam-ples because they exhibit distinctive cytologic and sometimes architectural fea-tures. Immunohistochemical studies on the aspirate smears or cell blocks pre-pared from the aspirated materials are particularly helpful in supporting adiagnosis of medullary carcinoma or lymphoma. Definitive treatment can pro-ceed on the basis of the cytologic diagnosis. A diagnosis of follicular carcinomacannot be made from fine-needle aspiration cytology.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

8 Endocrine System
Surgical ExcisionSurgical excision is the standard treatment of
thyroid tumors, providing ample tissue for histo-logic examination and special studies. It is most im-portant to sample the specimen adequately so thatan accurate diagnosis can be reached and all prog-nostic information can be provided. Sampling ismost critical for encapsulated follicular neoplasm be-cause a diagnosis of follicular carcinoma can bemissed owing to the focal nature of the invasivefoci. Some authors recommend a minimum of 10blocks.23 Others recommend at least five blocks ini-tially, with five or more additional blocks beingtaken if the tumor is found to be cellular on initialhistologic examination.24 Most blocks should betaken from the peripheral portions of the tumor,including the interface with the normal thyroid,rather than from the central portion. For optimalassessment of the capsule in all histologic sections,after bisection of the nodule through the equator,
Follicular Adenoma
CLINICAL CONSIDERATIONSPresentationFollicular adenoma occurs most commonly in
adult women aged 20 to 50 years, although no ageor sex is exempt. Most patients present with a pain-less thyroid nodule (“cold” nodule on iodine scan).Rare tumors show increased iodine uptake (“hot”nodules) and may be associated with hyperthyroid-ism. Follicular adenomas are benign and are ade-quately treated by lobectomy.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–1. Follicular adenoma. The tumor is enveloped by athin fibrous capsule. There is no capsular or vascular invasion.
radial cuts are made to produce wedge-shapedpieces, like cutting slices of an orange.25
Intraoperative Frozen SectionDiagnosis of thyroid tumors is usually not diffi-
cult on frozen sections; the greatest difficulty lies inthe distinction between follicular adenoma and fol-licular carcinoma because the invasive component isoften focal and thus not seen in random frozen sec-tions. Touch preparations form an important adjunctat intraoperative assessment and are particularlyhelpful for recognizing the characteristic nuclear fea-tures of papillary carcinoma and medullary carci-noma.
The role of intraoperative frozen section hasmuch diminished in recent years because of thewidespread use of fine-needle aspiration cytologyfor preoperative screening or diagnosis. It is cur-rently used mostly when fine-needle aspiration find-ings are suggestive of malignancy or are inconclu-sive. Intraoperative frozen section is of limited useand cost-effectiveness for follicular neoplasms be-cause of the high deferral rate (“follicular neoplasm;defer diagnosis to permanent sections”).26–29 Afterfrozen section is performed, the remaining tissueshould be fixed and further sampled for histologicexamination.
FIGURE 44–2. Follicular adenoma. A. This tumor is composed of small follicles lined by cells withuniform dark nuclei. B. This tumor shows a trabecular to microfollicular growth pattern and com-prises cells with mildly atypical nuclei.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 9
Macroscopic FindingsFollicular adenomas are almost invariably soli-
tary. They are round or oval and are enveloped in afibrous capsule, which is often thin. The cut surfaceshows homogeneous tan-brown fleshy tumor, some-times with a glistening quality. Secondary changessuch as hemorrhage and cystic degeneration may bepresent. Hurthle cell adenomas are typically mahog-any brown.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsFollicular adenoma is typically enclosed in a fi-
brous capsule of variable thickness, often with com-pression of the surrounding thyroid tissue (Fig.44–1). It can show a wide spectrum of architecturalfeatures, but a follicular pattern is most common.
The lining cells often have uniform, dark, round nu-clei, although occasional enlarged hyperchromaticnuclei can be interspersed (Fig. 44–2).
The many histologic variants of follicular ade-noma are listed in Table 44–5 (Figs. 44–3 to 44–10).By definition, capsular or vascular invasion must beabsent; if invasion is found, the tumor has to bediagnosed as follicular carcinoma.23, 30–56 The natureof hyalinizing trabecular adenoma has been mostcontroversial. The hyalinizing trabecular pattern isnot specific for follicular adenoma; it can be ob-served in papillary carcinoma and follicular carci-noma as well as focally in various thyroid lesions,such as colloid nodule and thyroiditis.57–59 Some in-vestigators consider hyalinizing trabecular adenomato represent a peculiar variant of papillary carci-noma because of merging with typical papillarycarcinoma in some cases, similarities in cytologic
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–3. Hyalinizing trabecular adenoma. A. The tumor typically forms wavy trabeculae inter-spersed with lumpy hyaline material. There are interspersed small cystic spaces representing abortivefollicle formation. B. The tumor cells possess pale oval nuclei that are sometimes grooved, mimickingthe cytologic features of papillary carcinoma. Perinucleolar haloes are present. Some tumor cellscontain distinctive cytoplasmic “yellow bodies” that stain dull pink and are surrounded by a halo.
TABLE 44–5. Variants of Follicular Adenoma
Variant* Defining Morphologic FeaturesEntity for Which the Variant May beMistaken
Macrofollicular Most follicles in the neoplasm are large. Nodular goiter
Microfollicular Most follicles in the neoplasm are small. Poorly differentiated (insular) carcinoma
Trabecular (embryonal) The tumor cells form straight trabeculaeseparated by a delicate vasculature.
Poorly differentiated (insular) carcinomaMedullary carcinoma
Hyalinizing trabecular The tumor forms wavy trabeculae with in-terspersed microcystic spaces representingabortive follicle formation.
The elongated tumor cells are aligned per-pendicularly in the trabeculae. The nucleiare often grooved and show pseudoinclu-sions. Unique cytoplasmic yellow bodiesare present.
Lumpy hyaline material is interspersedthroughout the tumor. Calcified colloidmay be present.
Papillary carcinomaParagangliomaMedullary carcinoma
Table continues on following page
Copyright � 2003, Elsevier Science (USA). All rights Reserved
10 Endocrine System
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
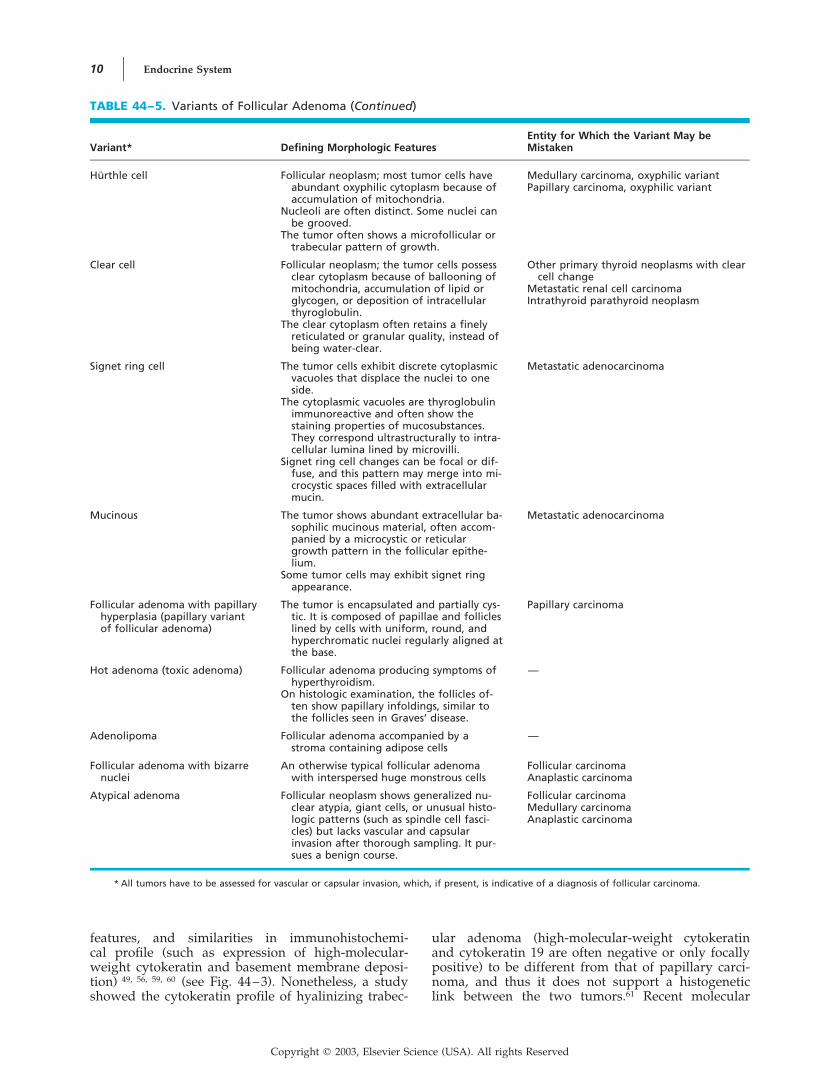
TABLE 44–5. Variants of Follicular Adenoma (Continued)
Variant* Defining Morphologic FeaturesEntity for Which the Variant May beMistaken
Hurthle cell Follicular neoplasm; most tumor cells haveabundant oxyphilic cytoplasm because ofaccumulation of mitochondria.
Nucleoli are often distinct. Some nuclei canbe grooved.
The tumor often shows a microfollicular ortrabecular pattern of growth.
Medullary carcinoma, oxyphilic variantPapillary carcinoma, oxyphilic variant
Clear cell Follicular neoplasm; the tumor cells possessclear cytoplasm because of ballooning ofmitochondria, accumulation of lipid orglycogen, or deposition of intracellularthyroglobulin.
The clear cytoplasm often retains a finelyreticulated or granular quality, instead ofbeing water-clear.
Other primary thyroid neoplasms with clearcell change
Metastatic renal cell carcinomaIntrathyroid parathyroid neoplasm
Signet ring cell The tumor cells exhibit discrete cytoplasmicvacuoles that displace the nuclei to oneside.
The cytoplasmic vacuoles are thyroglobulinimmunoreactive and often show thestaining properties of mucosubstances.They correspond ultrastructurally to intra-cellular lumina lined by microvilli.
Signet ring cell changes can be focal or dif-fuse, and this pattern may merge into mi-crocystic spaces filled with extracellularmucin.
Metastatic adenocarcinoma
Mucinous The tumor shows abundant extracellular ba-sophilic mucinous material, often accom-panied by a microcystic or reticulargrowth pattern in the follicular epithe-lium.
Some tumor cells may exhibit signet ringappearance.
Metastatic adenocarcinoma
Follicular adenoma with papillaryhyperplasia (papillary variantof follicular adenoma)
The tumor is encapsulated and partially cys-tic. It is composed of papillae and follicleslined by cells with uniform, round, andhyperchromatic nuclei regularly aligned atthe base.
Papillary carcinoma
Hot adenoma (toxic adenoma) Follicular adenoma producing symptoms ofhyperthyroidism.
On histologic examination, the follicles of-ten show papillary infoldings, similar tothe follicles seen in Graves’ disease.
—
Adenolipoma Follicular adenoma accompanied by astroma containing adipose cells
—
Follicular adenoma with bizarrenuclei
An otherwise typical follicular adenomawith interspersed huge monstrous cells
Follicular carcinomaAnaplastic carcinoma
Atypical adenoma Follicular neoplasm shows generalized nu-clear atypia, giant cells, or unusual histo-logic patterns (such as spindle cell fasci-cles) but lacks vascular and capsularinvasion after thorough sampling. It pur-sues a benign course.
Follicular carcinomaMedullary carcinomaAnaplastic carcinoma
* All tumors have to be assessed for vascular or capsular invasion, which, if present, is indicative of a diagnosis of follicular carcinoma.
features, and similarities in immunohistochemi-cal profile (such as expression of high-molecular-weight cytokeratin and basement membrane deposi-tion) 49, 56, 59, 60 (see Fig. 44–3). Nonetheless, a studyshowed the cytokeratin profile of hyalinizing trabec-
ular adenoma (high-molecular-weight cytokeratinand cytokeratin 19 are often negative or only focallypositive) to be different from that of papillary carci-noma, and thus it does not support a histogeneticlink between the two tumors.61 Recent molecular
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 11
FIGURE 44–5. Follicular adenoma, clear cell variant. The clearcytoplasm is not water-clear but retains a finely reticulated qual-ity.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
studies demonstrated a high frequency of RET/PTCtranslocation, suggesting a histogenetic relationshipof hyalinizing trabecular adenoma with papillarycarcinoma.61a–61c
ImmunohistochemistryFollicular adenomas are immunoreactive for cy-
tokeratin and thyroglobulin but not for calcitoninand pan-neuroendocrine markers. Hyalinizing tra-becular adenoma is peculiar in that it often showsan unusual cell membrane pattern of staining forKi-67.
Molecular BiologyMutations in the ras gene are found in some
follicular adenomas, at a frequency lower than infollicular Hemizygous deletion of62, 63carcinomas.
FIGURE 44–6. Follicular adenoma, signet ring cell variant.
FIGURE 44–4. Hurthle cell adenoma. A. This tumor shows a follicular growth pattern. The cellspossess abundant eosinophilic granular cytoplasm. Nucleoli are often but not invariably distinct inHurthle cells. B. This tumor shows a solid to trabecular growth pattern. The calcified colloid (left field)can potentially be mistaken for psammoma bodies. In contrast to psammoma bodies, they occurwithin follicular lumina rather than in the stroma.
the Cowden disease gene, PTEN, is found in 26% offollicular adenomas.64 Activating mutations of thegenes coding for the thyrotropin receptor and �-subunit of the stimulatory G protein have been de-tected in some follicular adenomas, especially thehyperfunctioning ones.62, 65–70
Differential Diagnosis
COLLOID (ADENOMATOID) NODULE. It can bedifficult to distinguish between follicular adenomaand adenomatoid nodule (hypercellular colloid nod-ule); the distinction is sometimes arbitrary. In gen-eral, adenomatoid nodules are multiple, lack a well-defined fibrous capsule, and are composed offollicles morphologically similar to those in the sur-rounding thyroid tissue.
PAPILLARY CARCINOMA. Pale or clear nucleiare not uncommonly encountered in follicular ade-
Copyright � 2003, Elsevier Science (USA). All rights Reserved
12 Endocrine System
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
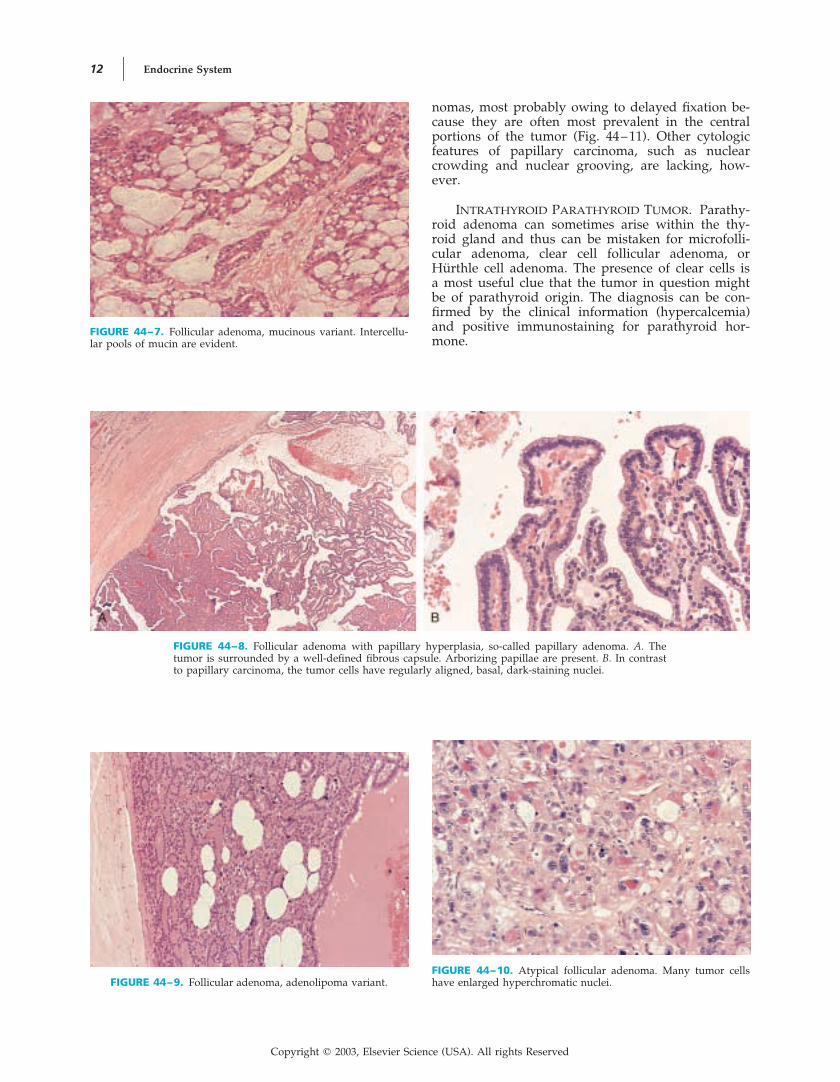
FIGURE 44–8. Follicular adenoma with papillary hyperplasia, so-called papillary adenoma. A. Thetumor is surrounded by a well-defined fibrous capsule. Arborizing papillae are present. B. In contrastto papillary carcinoma, the tumor cells have regularly aligned, basal, dark-staining nuclei.
FIGURE 44–7. Follicular adenoma, mucinous variant. Intercellu-lar pools of mucin are evident.
nomas, most probably owing to delayed fixation be-cause they are often most prevalent in the centralportions of the tumor (Fig. 44–11). Other cytologicfeatures of papillary carcinoma, such as nuclearcrowding and nuclear grooving, are lacking, how-ever.
INTRATHYROID PARATHYROID TUMOR. Parathy-roid adenoma can sometimes arise within the thy-roid gland and thus can be mistaken for microfolli-cular adenoma, clear cell follicular adenoma, orHurthle cell adenoma. The presence of clear cells isa most useful clue that the tumor in question mightbe of parathyroid origin. The diagnosis can be con-firmed by the clinical information (hypercalcemia)and positive immunostaining for parathyroid hor-mone.
FIGURE 44–9. Follicular adenoma, adenolipoma variant.FIGURE 44–10. Atypical follicular adenoma. Many tumor cellshave enlarged hyperchromatic nuclei.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 13
TABLE 44–6. Comparison Between Papillary and Follicular Carcinoma
Papillary Carcinoma Follicular Carcinoma
Frequency �70% of thyroid cancers �20% of thyroid cancers
Age Wide age range (mean, 43 y) Minimally invasive type: mean, 48 yWidely invasive type: mean, 55 y
Presentation Slow-growth thyroid mass; cervical lymphadenopa-thy; incidental finding
Slow-growing thyroid mass; fast-growing thyroidmass (less common); distant metastasis (such asbone)
Multifocal disease Common Uncommon
Clinical behavior Tumor is locally invasive; typically spreads by lym-phatic route to lymph nodes (�40%).
Distant metastasis (such as to lungs) is rare.The tumor is indolent; the cancer-related mortality
is only 6.5%—often confined to older patientswith extensive extrathyroid disease or distant me-tastasis.
Tumor spreads predominantly by bloodstream; boneis the predilection site.
Lymph node metastasis is uncommon.The cumulative mortality rates of the minimally in-
vasive and widely invasive types are 3% and 32%,respectively.
Basis of diagnosis Diagnosis is mostly based on the nuclear characteris-tics (crowded, ground-glass, grooved nuclei withpseudoinclusions), and demonstration of invasionis not required for the diagnosis. Therefore, thistumor is diagnosable by fine-needle aspiration cy-tology.
A follicular neoplasm demonstrating vascular orcapsular invasion, and nuclear features of papil-lary carcinoma must be lacking. Therefore, distinc-tion from follicular adenoma cannot be made onfine-needle aspiration cytology; only a diagnosticlabel of “follicular neoplasm” can be given.
Genetic basis Overexpression of RET proto-oncogene due to fu-sion with PTC1, PTC2, or PTC3 gene, or overex-pression of NTRK1 gene due to fusion with othergenes such as TPM3
Somatic mutation of ras oncogene in �50% ofcases, most commonly involving codon 61 CAA :CGA (Gln : Arg). t(2;3)(q13 5) resulting inPAX8-PPAR�1 fusion is found in �50% of cases.
Follicular Carcinoma
CLINICAL CONSIDERATIONSPresentationFollicular carcinoma is a malignant thyroid neo-
plasm showing follicular cell differentiation but lack-ing the diagnostic features of papillary carcinoma.1It generally occurs in patients with a mean age
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–11. Follicular adenoma showing nuclear clearing.Although the nuclei show clearing, they are not crowded and donot exhibit grooves. This is a common finding confined to thecentral portion of follicular adenoma, where fixation is delayed.
higher than that of those with follicular adenoma. Itusually manifests as a solitary thyroid mass or, lesscommonly, as metastatic tumor, in particular inbone.71–74 The main mode of spread is hematoge-nous (predilection sites are bone and lung) ratherthan lymphatic.75 The differences in clinicopathologicand biologic features between follicular carcinomaand papillary carcinoma are listed in Table 44–6.
Macroscopic Findings and MajorSubtypes of Follicular CarcinomaFollicular carcinoma is categorized into mini-
mally invasive and widely invasive types, whichshow different clinical outcome (Table 44–7). Theminimally invasive type is more common.1, 24, 44, 76–80
Minimally invasive carcinomas are macroscopi-cally indistinguishable from follicular adenoma, al-though the capsule tends to be thicker. Vascular orcapsular invasion is identified only on histologic as-sessment (Fig. 44–12). The prognosis is excellent,and thus treatment can be conservative.24, 72, 73, 81–88
The less common widely invasive follicular car-cinoma shows obvious invasion of the adjacent thy-roid parenchyma (Fig. 44–13). The tumor can ex-tend into the perithyroid tissues, and plugging ofblood vessels by tumor may also be 1, 44evident.There is a significant risk of distant metastasis, andthe prognosis is much worse than for minimally in-vasive follicular carcinoma.44, 89 Of note, many casesreported in the literature as “widely invasive follicu-lar carcinomas” are now reclassifiable as poorly dif-ferentiated thyroid carcinomas.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

14 Endocrine System
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsFollicular carcinomas are often surrounded by a
thick, dense fibrous capsule, although some widelyinvasive follicular carcinomas may not have a fi-brous capsule (see Figs. 44–12 and 44–13). Thetumors comprise cuboid cells forming closelypacked follicles, trabeculae, or solid sheets. The folli-cles are mostly small, but large follicles can also bepresent. The tumor cells often have uniform, dark-staining or pale-staining, round nuclei, but signifi-cant nuclear atypia can be observed in some cases(Fig. 44–14). The cytoplasm is eosinophilic, oxy-philic, or clear. Mitotic figures range from beingscanty to easily found. Secondary changes such ashemorrhage, hemosiderin deposition, sclerosis,edema, necrosis, and cystic change are not uncom-mon. The tumors may show variant histologic fea-
tures like those listed for follicular adenomas31, 34, 90–
93 (see Table 44–5).The only feature that distinguishes a follicular
carcinoma from a follicular adenoma is the presenceof vascular or capsular invasion.1 Strict criteria mustbe applied in the assessment of invasion.94–98 Thehistologic features that should heighten the suspi-cion for follicular carcinoma are listed in Table44–8, but they are by themselves insufficient for adiagnosis of malignancy.
To qualify for vascular invasion, the followingtwo criteria must be satisfied24:
• Involved blood vessels have to be located withinor outside the fibrous capsule.
• The intravascular polypoid tumor plug has to becovered by endothelium; if it is not endothelial-ized, it must be associated with thrombus forma-tion (Fig. 44–15; see also Fig. 44–12).
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–7. Categories of Follicular Carcinoma
Minimally Invasive Widely Invasive
Definition Totally encapsulated tumor with no gross invasion;vascular or capsular invasion is identified on his-tologic examination.
Tumor shows obvious invasion of adjacent thyroid tissue.
Age Younger (mean, �48 y) Older (mean, �56 y)
Metastases Regional lymph node or distant metastasis is rareand occurs late if it does.
Regional lymph node metastasis occurs in 13%–24% ofcases.
Distant metastasis (such as to lung, bone, brain, liver) iscommon (29%–60%).
Outcome Excellent prognosis. The long-term mortality isonly 3%–5%.
Long-term mortality is 30%–50%.
Treatment Curable by lobectomy or subtotal thyroidectomy,with or without suppressive dose of thyroxine.
For high-risk patients, such as old patients andthose with large tumors, total thyroidectomyand radioactive iodine therapy may have to beconsidered.
Total thyroidectomy, radioactive iodine, and suppressivedose of thyroxine
FIGURE 44–12. Follicular carcinoma, minimally invasive type.The tumor is typically surrounded by a thick fibrous capsule.Vascular invasion is present (upper field).
FIGURE 44–13. Follicular carcinoma, widely invasive type.There is frank invasion of the thyroid tissue in the form of multi-ple cellular tumor nodules. The upper field shows vascular inva-sion.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 15
TABLE 44–8. Key Points and Caveats in Diagnosis of Follicular Adenoma and Carcinoma
There is a tendency to overdiagnose follicular carcinoma. To qualify for follicular carcinoma, the following criteria must besatisfied:• Follicular neoplasm lacking nuclear features of papillary carcinoma• Capsular or vascular invasion, which must be unequivocal
Histologic features in a follicular neoplasm warranting more careful sampling to look for invasion (these features are notdiagnostic of carcinoma per se):• Thick fibrous capsule• High cellularity, i.e., tumors that are predominantly solid, trabecular, or microfollicular• Diffuse nuclear atypia (as opposed to presence of occasional bizarre cells)• Readily identifiable mitotic figures• Perpendicularly aligned neoplastic follicles or mushroom-shaped tumor bud in fibrous capsule• Hurthle cell neoplasm (�35% of all Hurthle cell neoplasms are malignant, a percentage higher than that of non–Hurthle cell
neoplasms)
Do not mistake capsular rupture associated with prior fine-needle aspiration as true capsular invasion. Capsular rupture can berecognized by the following features:• Tumor buds within fibrous capsule (at most one or two sites) are tiny and lack a “mushroom” contour.• Tumor buds are associated with blood, chronic inflammatory cells, and hemosiderin deposit.• Tumor cells often have a degenerated appearance.• Hemorrhagic track (with or without reparative features) is often identifiable in the vicinity.
If prominent delicate fibrovascular septa are present, consider the alterantive possibilities:• Medullary carcinoma• Intrathyroid parathyroid neoplasm• Paraganglioma
If a Hurthle cell neoplasm appears unusual, it may represent oxyphilic variant of the following tumors:• Medullary carcinoma• Intrathyroid parathyroid neoplasm• Papillary carcinoma
An invasive bud frequently pushes into the fi-brous capsule and then into a capsular blood vessellumen (Fig. 44–16). Mere bulging of follicles againstthe thin-walled capsular vessels is not sufficient fora designation of vascular invasion (Fig. 44–17). Re-traction spaces around tumor islands should not bemistaken for vascular invasion, and they can be rec-ognized by the lack of endothelial lining. The pres-ence of ragged clusters of nonendothelialized tumorwithin blood vessels does not count for vascularinvasion. This is believed to result from artifactual
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–14. Follicular carcinoma. A. This tumor shows a trabecular growth pattern and com-prises cells with fairly uniform, dark, round nuclei. B. This tumor exhibits generalized nuclear atypia.This is a feature that should alert one to the possibility of carcinoma for a follicular neoplasm.
dislodgment of tumor during sectioning of the speci-men.24 Intravascular endothelial hyperplasia occur-ring in capsular blood vessels should also not bemistaken for vascular invasion; the intravascularpolypoid plug is formed by plump spindly endothe-lial cells and pericytes instead of follicular epithelialcells99 (Fig. 44–18).
To qualify for capsular invasion, there must becomplete transgression of the fibrous capsule by tu-mor. That is, the tumor bud must have extendedbeyond an imaginary line drawn through the exter-
Copyright � 2003, Elsevier Science (USA). All rights Reserved

16 Endocrine System
FIGURE 44–16. Follicular carcinoma. The tumor (lower field) ex-tends into the fibrous capsule and then projects into a vascularlumen in the capsule.
FIGURE 44–17. Follicular adenoma. Bulging of tumor againstblood vessels within the tumor proper does not constitute vascu-lar invasion.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–15. Follicular carcinoma showing vascular invasion. A. A tumor plug projects into acapsular blood vessel, and it is clothed by endothelium. B. The intravascular tumor plug has a jaggedoutline and is not clothed by endothelium. However, this satisfies the criterion for vascular invasionbecause there is associated fibrin thrombus (left field).
FIGURE 44–18. Follicular adenoma with intravascular endothelial hyperplasia in the capsule, mim-icking vascular invasion. A. Cellular proliferation is seen in the capsular blood vessel (upper field). B.Closer examination reveals that the intravascular proliferation consists of small blood vessels and nottumor cells.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 17
nal contour of the capsule (Fig. 44–19). The invasivebud may be “naked” (without a fibrous capsule) orclothed by a thinner, newly formed fibrous cap-sule24, 71, 78, 100 (Fig. 44–19). A tumor bud that showsincomplete penetration of the capsule despite exami-nation of multiple levels of the tissue block can bedisregarded. Follicles entrapped in the capsule by asclerotic process are often aligned parallel to the fi-bers of the capsule (Fig. 44–20), whereas folliclesoriented perpendicular to the fibers or forming amushroom-shaped bud are more indicative of anactive invasive process, mandating examination ofmultiple levels and multiple blocks for more definiteevidence of capsular invasion (Fig. 44–21). Fine-nee-dle aspiration can result in capsular rupture, mim-icking capsular invasion; see Table 44–8 for featuressupportive of this interpretation101 (Fig. 44–22).
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–19. Follicular carcinoma showing capsular invasion. A. In this case, there is total pene-tration of the fibrous capsule. The invasive bud does not have a fibrous cap. B. In this case, theinvasive bud has penetrated the fibrous capsule, reaching beyond an imaginary line drawn along theexternal contour of the capsule. This invasive bud is clothed by a newly formed, thin fibrous cap.
FIGURE 44–20. Follicular adenoma. A. Bosselations of the tumor on the inner aspect of the fibrouscapsule should not be interpreted as capsular invasion. B. In the fibrous capsule, there are atrophicfollicles aligned in the direction of the fibrous capsule. This phenomenon results from passive entrap-ment of follicles in the fibrotic process and does not indicate capsular invasion.
Hurthle Cell CarcinomaHurthle cell carcinoma is a variant of follicular
carcinoma characterized by mitochondria-rich cells,75
although some investigators consider it to be a dis-tinct entity.45 There is new evidence that the patternof chromosome allelic alteration in Hurthle cell car-cinomas differs from that of conventional follicularcarcinomas.102
On gross evaluation, the tumor is bright brown.A size of 4 cm or larger is strongly correlated withmalignancy.103 On histologic examination, the tumorshows a trabecular, microfollicular, diffuse, or rarelypapillary growth pattern. The tumor cells possessabundant brightly eosinophilic granular cytoplasm,which can exhibit partial to complete clearing asa result of ballooning of the mitochondria (Fig.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
18 Endocrine System
44–23). The nuclei are round or sometimes grooved.The chromatin is granular to coarse, and nucleoli areoften prominent. Some degree of nuclear pleomor-phism is common. The colloid can undergo calcifica-tion and thus may be mistaken for psammoma bod-ies. Hurthle cell neoplasms are particularly prone toinfarction after fine-needle aspiration.101, 104–106
Some previous studies have proposed aggressivetreatment for all Hurthle cell neoplasms, irrespectiveof whether invasion could be demonstrated histolog-ically, on the basis of the belief that all were poten-tially malignant.107–110 However, many later studieshave challenged this misconception and shown thatthe behavior of Hurthle cell neoplasms can be accu-rately predicted by histologic features (i.e., whetherthere is vascular or capsular invasion, as in follicularneoplasms).* Only those showing invasion are diag-nosed as carcinoma (see Fig. 44–15A). Such tumorscan recur locally, metastasize to regional lymphnodes, or show distant metastasis (especially to boneand lungs).71, 98, 100, 119, 120 When a Hurthle cell neo-plasm shows some but inconclusive evidence of in-vasion, the term Hurthle cell tumor of uncertain malig-nant potential is sometimes applied. Clinicalfollow-up shows a benign evolution in all cases. Itmay therefore be more appropriate to simply labelsuch cases “Hurthle cell adenoma.”100, 121
The overall mortality rate of Hurthle cell carci-nomas is 30% to 70%.71, 98, 100 Compared with con-ventional follicular carcinomas, Hurthle cell carcino-mas take up radioactive iodine less satisfactorily;
they show a higher frequency of extrathyroidal ex-tension, local recurrence, and metastasis to lymphnodes, and the survival rate is lower.75, 96, 100, 122, 123
However, with stratification by the extent of inva-sion, the differences are obliterated.75 It has beensuggested that the presence of a solid or trabecularpattern in more than 75% of the tumor area identi-fies a poorly differentiated subgroup with worseprognosis—30% died of disease or were alivewith recurrent disease, compared with a 2.5% mor-tality rate for the non–poorly differentiated sub-group.124
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
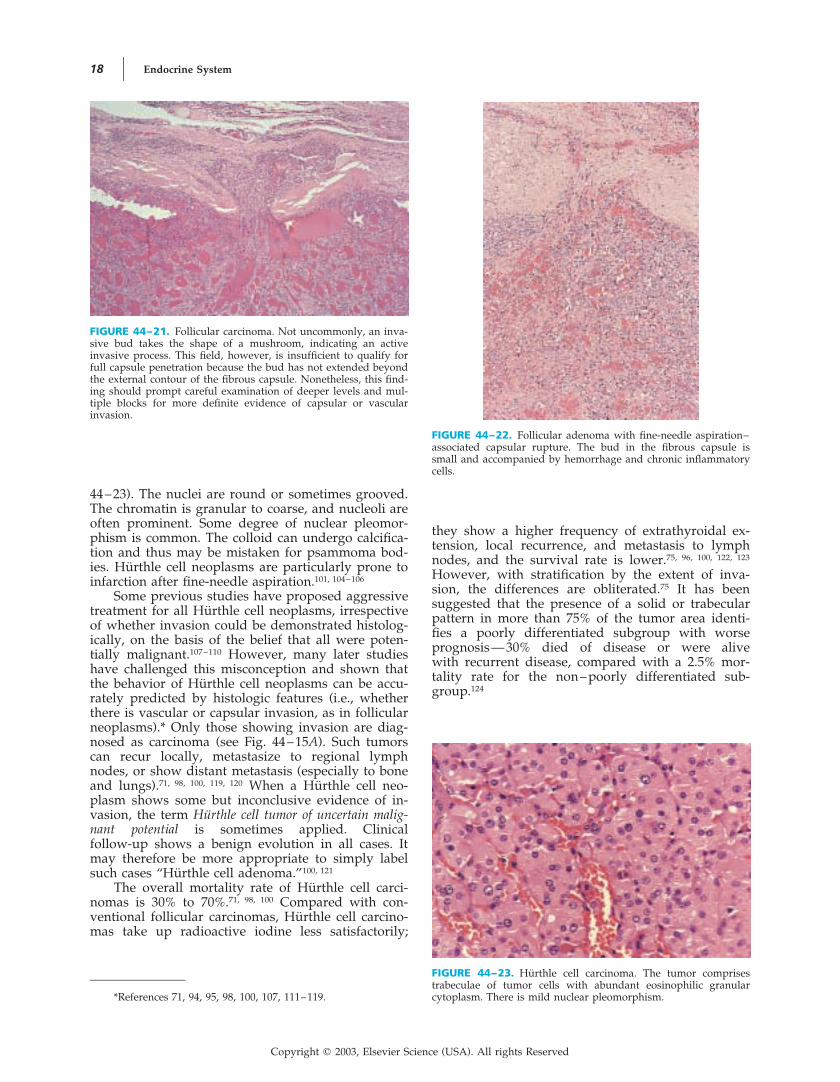
FIGURE 44–21. Follicular carcinoma. Not uncommonly, an inva-sive bud takes the shape of a mushroom, indicating an activeinvasive process. This field, however, is insufficient to qualify forfull capsule penetration because the bud has not extended beyondthe external contour of the fibrous capsule. Nonetheless, this find-ing should prompt careful examination of deeper levels and mul-tiple blocks for more definite evidence of capsular or vascularinvasion.
FIGURE 44–22. Follicular adenoma with fine-needle aspiration–associated capsular rupture. The bud in the fibrous capsule issmall and accompanied by hemorrhage and chronic inflammatorycells.
*References 71, 94, 95, 98, 100, 107, 111–119.
FIGURE 44–23. Hurthle cell carcinoma. The tumor comprisestrabeculae of tumor cells with abundant eosinophilic granularcytoplasm. There is mild nuclear pleomorphism.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 19
ImmunohistochemistryFollicular carcinoma is immunoreactive for cyto-
keratin and thyroglobulin but not for pan-neuroen-docrine markers.125 Immunohistochemical studies arerarely required for diagnosis of this tumor with theexception of two scenarios:
• Unusual-looking thyroid neoplasm—thyroglobulinimmunoreactivity confirms the presence of thyroidfollicular cell differentiation and is helpful for dis-tinction from medullary carcinoma.
• Metastatic neoplasm suspected to represent meta-static follicular carcinoma—thyroglobulin immu-noreactivity confirms the thyroid origin of the car-cinoma.
Molecular Biology and Special StudiesClonal chromosome abnormalities, such as non-
disjunctional chromosome loss and deletions in 3p25: pter, are common in follicular carcinomas.126–129
Comparative genomic hybridization studies revealfrequent DNA copy number changes; loss of chro-mosome 22 is associated with the widely invasivetype and old age at presentation.130 Molecular stud-ies show frequent loss of heterozygosity on chromo-somes 3p (86%), 17p (72%), and 10q (57%); 17pchange is correlated with mortality.131, 132
A high frequency of activating point mutationsin the family of ras genes is found in follicular carci-nomas, although similar mutations can also befound in some follicular adenomas.62, 63 N-ras muta-tion is found in 50% of follicular carcinomas, mostcommonly involving codon 61 with CAA : CGA(Gln : Arg); this mutation is observed in approxi-mately 25% of anaplastic carcinomas but not in pap-illary carcinomas.133 H-ras codon 12 mutation isfound in 33% of follicular carcinomas.134 Alterationin the TP53 gene is uncommon, but its presence isassociated with an increased risk of metastasis.135
Recently, t(2;3)(q13; p25), which results in fusion ofPAX8 gene with peroxisome proliferator-activatedreceptor gamma 1 (PPAR�1) gene, has been shownto be a characteristic genetic aberration of follicularcarcinoma. The fusion transcript is detected in 5 of 8follicular carcinomas, but not in 20 follicular adeno-mas, 10 papillary carcinomas and 10 cases of multi-nodular hyperplasia.135a
Differential Diagnosis
FOLLICULAR ADENOMA. The current “goldstandard” for distinguishing between follicular carci-noma and follicular adenoma is identification of vas-cular or capsular invasion in follicular carcinoma(see “Microscopic Findings”). Although some anti-bodies, such as Leu-7, thyroid peroxidase (monoclo-nal antibody 47), HBME-1, tissue polypeptide anti-gen, dipeptidyl aminopeptidase IV (CD26), andtopoisomerase II, have been reported to stain follicu-lar carcinomas and follicular adenomas with differ-ent frequencies,136–142 the discriminatory power isnot high enough for routine diagnostic application.Various tumor markers, such as carcinoembryonic
antigen, oncogene products (Ras p21, c-Myc), cyclinD1, cyclin-dependent kinase inhibitor (p27), prolifer-ation marker (Ki-67), epidermal growth factor, P-glycoprotein, high-mobility group I HMGI(Y) pro-tein, and telomerase activity, have not been shownto be sufficiently discriminatory 121, 125, 143–149either.DNA ploidy analysis also fails to distinguish follicu-lar carcinoma from follicular adenoma.150–154
HASHIMOTO’S THYROIDITIS AND DYSHORMON-OGENESIS. In Hashimoto’s thyroiditis or dyshor-monogenetic goiter, multiple cellular hyperplasticnodules can be present, raising a concern for follicu-lar carcinoma. However, vascular invasion is notfound, and the different cellular nodules often ex-hibit different cellularities and follicle size.
MEDULLARY CARCINOMA. Some variants ofmedullary carcinoma can mimic follicular or Hurthlecell carcinoma. The presence of prominent delicatefibrovascular septa should always raise the possibil-ity of medullary carcinoma. If there is any uncer-tainty about the diagnosis, immunohistochemicalstudies should be performed.
PAPILLARY CARCINOMA. Some follicular carci-nomas may show nuclear clearing, mimicking papil-lary carcinomas. However, this phenomenon is oftenconfined to the central portion of the tumor, wherethere is delayed fixation. Hurthle cell carcinomascan show nuclear grooving, but this is often a focalphenomenon and other cytologic features of papil-lary carcinoma are lacking.
PROGNOSTIC CONSIDERATIONSThe most important prognostic factors for follicularcarcinoma are age, degree of invasiveness, and pres-ence or absence of distant metastasis.
AGE. The prognosis is excellent for patientsyounger than 30 to 40 years.*
MINIMALLY INVASIVE VERSUS WIDELY INVA-SIVE TYPE. The prognosis of the widely invasivefollicular carcinoma is much worse than that ofthe minimally invasive type (see Table 44–7).Tumor invasion of the soft tissues of the neck isassociated with a particularly unfavorable progno-sis.44, 82, 96, 111, 123
METASTASIS. Distant metastasis at presentationis a highly unfavorable prognostic factor.†
SEX. Some studies have shown the male sex tobe associated with a worse outcome.82, 100, 156
HISTOLOGIC TYPE OR PATTERN. As a group,Hurthle cell carcinomas have a worse progno-sis than that of conventional follicular carcino-mas.71, 75, 100, 123 Presence of a solid or trabecular pat-tern in more than 75% of the tumor area isassociated with a worse prognosis.124
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
*References 44, 71, 78, 82, 100, 111, 123, 155, 156.
†References 44, 71, 81, 100, 111, 123, 156–158.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

20 Endocrine System
TUMOR SIZE. Some studies have reported alarge tumor (�4 cm) to be associated with a worseprognosis.78, 100, 123, 155, 156
VASCULAR INVASION. Follicular carcinomasshowing capsular invasion alone in the absence ofvascular invasion have a negligible risk of metasta-sis.81, 121, 156, 159
E-CE-CADHERIN EXPRESSION. Lack of E-cadherinexpression is reported to be an unfavorable prognos-tic factor.160
DNA ADNA ANEUPLOIDY. Whereas some studies sug-gest that aneuploid follicular carcinomas are moreaggressive, other studies have not been able to con-firm this observation.150, 151, 161
P53 A53 ABERRATION. Presence of p53 aberrationmay confer an increased chance of metastasis.124, 135
Papillary Carcinoma
CLINICAL CONSIDERATIONSPresentationPapillary carcinoma can occur in patients of any
age, including children. The mean age is 43 years,and there is a female predilection162–165 (see Table44–6). The patients usually present with a thyroidmass or cervical lymph node metastasis. Small pap-
illary carcinoma can also be discovered incidentallyin thyroid glands excised for various reasons (latentpapillary carcinoma).166, 167
Macroscopic FindingsThe macroscopic appearances of papillary carci-
noma are highly variable, mirroring the myriad his-tologic patterns that this tumor can assume. Theclassic examples exhibit firm to hard white-tan tu-mors with invasive borders. The tumor often has agranular quality on the cut surface due to the pres-ence of papillae. The presence of psammoma bodiescan impart a gritty sensation on cutting of the tu-mor. Tumors with a predominantly follicular archi-tecture are often tan-brown and fleshy, similar tofollicular neoplasms. Some tumors can be encapsu-lated. Cystic change can occur.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsPapillary carcinoma is defined as a malignant
epithelial tumor showing evidence of follicularcell differentiation, typically with papillary and fol-licular structures as well as characteristic nuclear
The diagnosis is based on the nu-1, 168, 169changes.clear characteristics, which include large size, pallor,ground-glass appearance, irregular outline, deepgrooves, and pseudoinclusions169–172 (Fig. 44–24).
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–24. Papillary carcinoma showing the spectrum ofcytologic features. A. The papillae are covered by cells with palenuclei, some of which are optically clear (left field). The nuclei alsoexhibit crowding. B. The nuclei are comparatively chromatin rich,although still pale. They are ovoid, with grooving and distinctnucleoli. Note the lack of polarity. C. The nuclei are pale, andsome nuclear pseudoinclusions are seen. Portion of a multinucle-ated histiocyte is seen in the lumen (lower field).
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 21
Papillary carcinomas are usually infiltrative, butsome may be circumscribed or even encapsulated(Fig. 44–25).
The papillae are usually arborizing, with deli-cate fibrovascular cores (Fig. 44–26A; see also Fig.44–25). However, the papillae can be broad, withthe cores being formed by fibrocellular, edematous,or hyalinized tissue, which may contain foamy mac-rophages, adipose cells, or small neoplastic folli-cles.38, 173, 174 Micropapillae comprising cellular tuftsare sometimes formed. Follicles are frequentlypresent. They vary in size and contour but are com-monly elongated or irregularly shaped and containdark-staining colloid. Some follicles can be large andmarkedly distended with colloid. Intrafollicularhemorrhage is common. There is often an intricateblending of the follicles and papillae, resulting in acomplex tubulopapillary pattern (Fig. 44–26B). Lesscommon patterns are microglandular, cribriform,
anastomosing tubular, trabecular, and 171, 175solid.Multinucleated histiocytes with deeply eosinophiliccytoplasm can be found in the luminal space ofsome follicles and papillae in approximately 50% ofcases and can aid in the diagnosis of papillary carci-noma because they are extremely rare in other thy-roid lesions or tumors176 (see Fig. 44–24C).
There is commonly an abundant scleroticstroma,177, 178 and desmoplastic stroma is often con-fined to the invasive fronts170 (Fig. 44–27; see alsoFig. 44–25). The stroma commonly shows patchyinfiltration of lymphocytes, plasma cells, and macro-phages. Psammoma bodies are found in the stalksof the papillae, in the fibrous stroma, or amongthe tumor cells in about 50% of cases; they are vir-tually pathognomonic of papillary thyroid carci-noma170, 179, 180 (see Fig. 44–26A).
The nuclei of papillary carcinoma are character-istically large, crowded, ovoid, ground-glass (“Or-phan Annie” eye), and grooved and contain smalldistinct nucleoli171, 181 (see Fig. 44–24). Nuclear pseu-doinclusions may be identified in a small proportionof tumor cells181–184 (see Fig. 44–24C). Mitotic figuresare usually sparse. In some papillary carcinomas,the typical nuclear features may not be well devel-oped, and thus the diagnosis of papillary carcinomawould have to depend on the architectural featuresand on the identification of foci showing more typi-cal nuclear features (Fig. 44–28).
The neoplastic cells are cuboid, polygonal, co-lumnar, flattened, dome shaped, or hobnailed. Thecytoplasm is lightly eosinophilic to amphophilic, butit can be oxyphilic or clear.31, 34, 185–187 Cytoplasmicmucin can be demonstrated by histochemical stainsin a proportion of cases.188, 189 Focal squamous differ-entiation is common, and such foci usually do notexhibit the characteristic nuclear features of papil-lary carcinoma (Fig. 44–29).
Many variants of papillary carcinoma have beenrecognized, but only some are of prognostic signifi-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–25. Papillary carcinoma. A typical example showinginfiltrative growth, prominent branching papillae, and scleroticstroma.
FIGURE 44–26. Papillary carcinoma. A. Arborizing papillae are evident. Psammoma bodies are seenin the cores of some papillae. B. Complex tubulopapillary architecture is a common growth pattern.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

22 Endocrine System
cance.* They are listed in Table 44–9 (Figs. 44–30 to44–42).
Latent Papillary CarcinomaLatent papillary carcinomas are cancers inciden-
tally found in thyroidectomy specimens or at au-topsy. In autopsy series, they are found in approxi-mately 5% to 10% of cases, but the frequency rangesfrom as high as 36% in Finland to as low as 1.2%in Latent papillary carcinomas171, 248–257Switzerland.usually appear after puberty, and the prevalencedoes not show a significant increase with age there-after.250, 258–260 A small proportion of cases can showregional lymph node metastasis, but the deposits areoften microscopic and probably remain dormant
even without excision.261 The lack of female predom-inance in latent papillary carcinomas and the dis-sociation between the prevalence rates of latentand clinical thyroid carcinomas suggest that mostlatent papillary carcinomas remain dormant anddo not grow to become clinically apparent tu-mors.180, 250, 254, 262 Because latent papillary carcinomasare innocuous, no additional therapy is required.
Latent papillary carcinomas are almost alwaystiny and commonly show a predominantly folliculararchitecture. Most cases exhibit an invasive stellatecontour and sclerosis; others comprise a circum-scribed or encapsulated collection of neoplastic folli-cles without intratumoral sclerosis245, 263 (Figs. 44–43and 44–44).
ImmunohistochemistryThe immunohistochemical profile of papillary
carcinoma is listed in Table 44–1. The staining for
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–27. Papillary carcinoma with extrathyroidal exten-sion. The tumor extends into the skeletal muscle of the anteriorneck and is accompanied by a desmoplastic stroma.
FIGURE 44–28. Papillary carcinoma. In this tumor, the nuclearfeatures of papillary carcinoma are poorly developed. A diagnosisof papillary carcinoma is made because the tumor exhibits a pap-illary architecture and frank invasion into the soft tissues of theneck.
FIGURE 44–29. Papillary carcinoma showing focal squamousmetaplasia.
FIGURE 44–30. Papillary carcinoma, follicular variant. This tu-mor is composed exclusively of follicles. It is infiltrative and ac-companied by a sclerotic stroma, and thus recognition of themalignant nature of the neoplasm is easy.
*References 45, 72, 76, 164, 165, 170, 171, 180, 185, 190–247.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 23
TABLE 44–9. Variants of Papillary Carcinoma
Variant* Defining Morphologic FeaturesEntity for Which the VariantMay Be Mistaken Clinical Significance
Follicular variant Composed exclusively or almostexclusively of follicles
The follicles are often elon-gated and irregularly shaped,with abortive papillae.
The colloid is often dark stain-ing.
Follicular adenomaFollicular carcinoma
No prognostic implications
Encapsulated variant Tumor with a distinct fibrouscapsule
Capsular or vascular invasionmay or may not be present.
Follicular adenomaFollicular carcinoma
Highly favorable prognosis: notumor relapse after nodulec-tomy or lobectomy
Cystic variant Prominent cyst formationThere may or may not be neo-
plastic papillae projectinginto the cystic space.
Cystic degeneration of colloidnodule
No prognostic implications
Encapsulated follicu-lar variant
Encapsulated tumor composedexclusively or almost exclu-sively of follicles
Follicular adenomaFollicular carcinoma
Highly favorable prognosis: notumor relapse after treat-ment
Diffuse sclerosingvariant
Diffuse extensive involvementof one or both lobes withoutforming a gross tumor nod-ule
Thyroid parenchyma showssclerosis and lymphoid infil-tration. Tumor islands are of-ten small and dispersed, withmany lying within lymphaticspaces.
Tumor commonly shows squa-mous metaplasia and promi-nent psammoma body for-mation.
Thyroiditis, especially becauseof the diffuse nature of theprocess and frequent pres-ence of circulating antithy-roid antibodies
Some studies have reportedthis variant to be more ag-gressive, with frequentlymph node and sometimesdistant metastases, but out-come is still favorable be-cause of the young age ofpatients (favorable prognos-tic factor).
Some studies have not shownthis variant to exhibit a highmetastatic rate.
Diffuse follicularvariant
Diffuse involvement of the en-tire thyroid without forma-tion of discrete tumor nod-ules, and composed entirelyof follicles
No fibrosis
Colloid goiter More aggressive, with frequentlymph node and distant me-tastases, but outcome is stillfavorable because of theyoung age of patients (favor-able prognostic factor) andgood response to radioactiveiodine therapy.
Macrofollicular vari-ant
Presence of many large folli-cles, mimicking colloid nod-ule
Nodular goiter No prognostic implications
Tall cell variant �50% of tumor cells with aheight of more than twicethe breadth
Tumor cells often possess oxy-philic cytoplasm.
Columnar cell carcinoma As a group, tall cell variant ismore aggressive than con-ventional papillary carci-noma, with larger tumors,more frequent extrathyroidalextension, higher recurrencerate, and higher mortality(reported 9%–25%).
For intrathyroidal tumors oc-curring in young patients,however, the prognosis ap-pears to be similar to that ofconventional papillary carci-noma.
Oxyphil cell variant �50% of tumor cells withabundant oxyphilic cytoplasm
Hurthle cell adenoma or carci-noma
No prognostic implications
Solid variant �50% of tumor showing asolid growth pattern
The sheets and nests of tumorare often traversed by deli-cate fibrovascular septa.
Poorly differentiated (insular)carcinoma
No prognostic implications
Table continued on following page
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

24 Endocrine System
thyroglobulin is patchy, and it is often absent inareas of squamous differentiation. The main applica-tion of immunohistochemical staining is in confirma-tion of the thyroid origin of metastatic carcinoma,such as cystic metastasis of papillary thyroid carci-noma in a cervical lymph node. Although stainingfor high-molecular-weight cytokeratin or cytokeratin19 has been suggested to be of value in supporting adiagnosis of papillary carcinoma versus benign thy-
roid lesions in difficult cases,264–267 the results arenot consistent enough for routine application.
Cytogenetics and Molecular BiologyThe key molecular change in papillary carci-
noma involves activation of the proto-oncogene RETor NTRK1 by intrachromosome inversion or chromo-some translocation.268–270 Constitutive activation ofRET (a receptor tyrosine kinase) occurs through fu-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–9. Variants of Papillary Carcinoma Continued
Variant* Defining Morphologic FeaturesEntity for Which the VariantMay Be Mistaken Clinical Significance
Trabecular variant �5% of tumor showing a tra-becular growth pattern
Follicular adenoma or carci-noma, trabecular (embryonal)type
Some studies have shown thisvariant to have a less favor-able outcome.
Cribriform-morularvariant
An intricate admixture of crib-riform structures, closelypacked small follicles, papil-lae, and squamoid islands(morulas)
Colloid is usually scanty or ab-sent.
Some tumor cells in the morulacontain nuclei with a lightlyeosinophilic homogeneousappearance caused by biotinaccumulation.
The tumor cell nuclei are oftenmore hyperchromatic andpseudostratified comparedwith classic papillary carci-noma.
Columnar cell carcinomaTall cell variant of papillary car-
cinoma
Familial adenomatous polyposisshould be excluded becausethe papillary carcinomas as-sociated with the syndromecommonly exhibit histologicfeatures of this variant.
By itself, the variant has noprognostic implications.
Variant with nodu-lar fasciitis– likestroma
Presence of abundant nodularfasciitis– like or fibromatosis-like reactive stroma
The papillary carcinoma com-ponent can be masked bythe stromal component orshows peculiar architecturalfeatures reminiscent of fibro-cystic disease or phyllodes tu-mor of the breast.
Nodular fasciitisFibromatosisBenign mesenchymal neoplasm
No prognostic implications
Warthin tumor–likevariant
Presence of broad papillae cov-ered by oxyphilic neoplasticcells, with the cores beingpacked with lymphoid cells,reminiscent of Warthin tu-mor of salivary gland
Hashimoto’s thyroiditis No prognostic implications
Papillary microcarci-noma
Small tumor, �1 cm Multifocal fibrosing thyroiditisHyperplastic adenomatoid nod-
ule
Highly favorable prognosisVirtually all patients remain
well on long-term follow-up.The rare patients who have an
unfavorable outcome arethose with lymphadenopathy�3 cm and a nonencapsu-lated type of primary lesion.
Dedifferentiatedpapillary carci-noma
Papillary carcinoma accompa-nied by an anaplastic carci-noma or poorly differenti-ated thyroid carcinoma,indicating transformation toa higher-grade neoplasm
— High mortality rate
* All variants show the typical nuclear characteristics of papillary carcinoma, at least in some areas of the tumor.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 25
FIGURE 44–31. Papillary carcinoma, encapsulated follicular variant. A. The encapsulated tumor iscomposed exclusively of follicles, rendering distinction from follicular adenoma or follicular carcinomadifficult. The clues to diagnosis are dark-staining colloid, elongated follicles, and presence of abortivepapillae. B. The follicles are lined by cells with crowded, pale, and grooved nuclei, compatible withpapillary carcinoma.
FIGURE 44–32. Papillary carcinoma, cystic variant. A. The cysthas a fibrous wall lined by attenuated epithelium and can poten-tially be mistaken for cystic degeneration of colloid nodule. B. Inthe wall, there are occasional follicles lined by cells with active-looking and crowded nuclei. C. Focally, short papillae lined bycells exhibiting features of papillary carcinoma are identified, per-mitting the correct diagnosis to be made.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
sion of the RET gene with a gene commonly ex-pressed in thyroid epithelial cells, such as PTC1through inv(10)(q11.2q21), PTC2 through t(10;17)(q11.2;q23), and PTC3 through cytogenetically unde-tectable paracentric inversion within 10q11.2.271–277
The RET/PTC translocation occurs in approximately30% to 40% of papillary carcinomas, but the fre-quency is higher in children and young patients,Chernobyl accident–associated tumors, and patientswho received external radiation during child-
Copyright � 2003, Elsevier Science (USA). All rights Reserved

26 Endocrine System
FIGURE 44–33. Papillary carcinoma, diffuse sclerosing variant. A. The thyroid gland shows sclerosisand chronic inflammation, mimicking thyroiditis. However, linear scratches on the slide suggest thepresence of calcified psammoma bodies. B. Hiding within the gland are islands of papillary carci-noma. A psammoma body is seen in the left lower field.
FIGURE 44–34. Papillary carcinoma, diffuse follicular variant. A. The neoplasm shows extensiveinvolvement of the thyroid without discrete nodule formation or sclerosis and thus can be mistakenfor a diffuse goiter, especially because some follicles are large. B. Careful examination of the smallerfollicles reveals cytologic features of papillary carcinoma.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–35. Papillary carcinoma, tall cell variant. A. The neoplastic cells are tall columnar andexhibit oncocytic cytoplasmic features. The nuclear features are no different from those of conven-tional papillary carcinoma. B. In this unusual example, the cells show cytoplasmic clearing.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 27
FIGURE 44–36. Papillary carcinoma, oncocytic variant. The cu-boid and polygonal tumor cells possess abundant eosinophilicgranular cytoplasm.
FIGURE 44–38. Papillary carcinoma, trabecular variant.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–37. Papillary carcinoma, solid variant. Solid islandsof tumor are often traversed by delicate capillaries. The character-istic nuclear features of papillary carcinoma are present.
FIGURE 44–39. Papillary carcinoma, cribriform-morular variant. A. There is an intricate blend ofcribriform structures, empty follicles, and solid foci. B. Papillae merge into a morular structure. Highlycharacteristic homogeneous, lightly eosinophilic biotin inclusions are seen in the nuclei of the morula.The tumor cells are often more chromatin rich than in a usual case of papillary carcinoma.
hood.62, 278–296 Activation of the NTRK1 gene product(a receptor for nerve growth factor) occurs throughfusion with widely expressed “housekeeping” genes,such as TPM3 (tropomyosin gene), TPR, andTAG.268, 280, 281, 285, 297–299
Differential DiagnosisThe main criteria and problems in diagnosis of
papillary carcinoma are listed in Table 44–10.300
Some immunohistochemical markers, such asexpression of high-molecular-weight cytokeratin(34�E12, cytokeratin 1), cytokeratin 19, vimentin,mesothelium-associated antibody HBME-1, Leu-7(CD57), CD15 (Leu-M1), or CD44, and loss of ex-pression of thyroid peroxidase or retinoblastomaprotein have been reported to be of value in distin-
Copyright � 2003, Elsevier Science (USA). All rights Reserved

28 Endocrine System
FIGURE 44–41. Papillary carcinoma, Warthin tumor–like vari-ant. The resemblance to Warthin tumor of the salivary gland isstriking. The neoplastic cells show oncocytic change.
FIGURE 44–42. Papillary carcinoma, dedifferentiated variant.Papillary carcinoma component is shown on the left; the anaplas-tic carcinoma comprising pleomorphic spindly cells is shown onthe right.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–40. Papillary carcinoma, variant with nodular fasciitis– like stroma. A. The interaction ofthe abundant fibrocellular stroma with the papillary carcinoma results in a peculiar pattern mimickingsclerosing adenosis of the breast. B. The stroma comprises loose fascicles of active-looking myofibro-blasts, mimicking nodular fasciitis or fibromatosis.
FIGURE 44–43. Latent papillary carcinoma as an incidental finding. A. Near the central field, there isa collection of small follicles representing latent papillary carcinoma. It is not accompanied by asclerotic stroma. B. The follicles are lined by cells with large pale nuclei lacking polarity (left field),characteristic of papillary carcinoma. Note the abrupt difference in nuclear features compared withthe adjoining normal follicles (right field).
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 29
guishing papillary carcinoma from benign thyroidlesions and other thyroid tumors, but so far none ofthese makers is reliable enough to aid in routinediagnosis of papillary 138, 139, 265, 266, 301–314carcinoma.Future studies are required to determine whetheroverexpression of RET by in situ hybridization orimmunohistochemistry can aid in the diagnosis ofpapillary carcinoma. Currently, morphologic assess-ment remains the gold standard in rendering a diag-nosis of papillary carcinoma.
COLLOID NODULE. In contrast to papillary car-cinoma, the papillae found in colloid or adenoma-
toid nodules are often broad, with small follicles inthe loose core. The cells are usually columnar, withdark round nuclei regularly aligned at the base ofthe cells. In some colloid or adenomatoid nodules,there can be collections of follicles with pale or clearnuclei, raising a concern for papillary carcinoma.However, a diagnosis of papillary carcinoma (follic-ular variant) should not be made unless there aretotally convincing nuclear features (see Figs. 44–24and 44–31 and Table 44–10). The neoplastic folliclesof papillary carcinoma should show an abruptchange from the surrounding benign follicles, oftenaccompanied by enlargement of the nuclei (see Fig.44–43). In contrast, the atypical follicles of adenom-atoid nodule typically show gradual transition withthe surrounding benign follicles.
FOLLICULAR ADENOMA WITH PAPILLARY HY-PERPLASIA. Distinguishing features from papil-lary carcinoma are the same as those for colloidnodule.
FOLLICULAR ADENOMA. Some follicular adeno-mas may have some pale or clear nuclei, raising thepossibility of follicular variant of papillary carci-noma. The nuclear clearing is often artifactual be-cause of delayed fixation, with “blowing up” of thenuclei (see Fig. 44–11). Convincing nuclear featuresmust be present in rendering a diagnosis of papil-lary carcinoma in an encapsulated follicular neo-plasm because there is no harm in missing an en-capsulated papillary carcinoma, which has anexcellent prognosis (see Table 44–9).
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–44. Latent papillary carcinoma as an incidental find-ing. This microcarcinoma shows a papillary architecture.
TABLE 44–10. Key Points and Caveats in Diagnosis of Papillary Carcinoma
Diagnostic criteria for papillary carcinoma are based on a constellation of features, no single one of which is pathognomonic. For anoninvasive tumor, the diagnostic label “papillary carcinoma” should be applied only when the typical cytologic features are welldeveloped.
Basic criteria• Cytologic features: ovoid nuclei that are crowded, without polarization, clear or pale, and grooved, with or without pseudoin-
clusions• Demonstration of vascular or capsular invasion is not required
Strong supporting feature, if present• Psammoma bodies
Other supporting histologic features• Papillae (including abortive papillae)• Follicles that are elongated or irregularly shaped• Dark-staining colloid• Multinucleated histiocytes in lumina of follicles or papillae
Deceptively “benign” patterns warranting serious consideration of the possibility of papillary carcinoma:• “Colloid nodule” with delicate papillary budding in some follicles, or psammoma bodies, or many clear nuclei (papillary
carcinoma, macrofollicular variant)• Hashimoto’s or lymphocytic thyroiditis– like picture, but with many “knife marks” on the histologic section due to presence of
psammoma bodies (diffuse sclerosing variant of papillary carcinoma)• “Follicular adenoma” with many elongated follicles and dark-staining colloid or abortive papillae (papillary carcinoma, encapsu-
lated follicular variant)• “Degenerate cyst,” but with occasional small papillary tufts projecting into the lumen or some follicles in the fibrous wall lined
by cells with high nuclear-to-cytoplasmic ratio (cystic variant of papillary carcinoma)• Spindle cell proliferation resembling nodular fasciitis or fibromatosis (papillary carcinoma variant with exuberant nodular
fasciitis– like stroma)
Copyright � 2003, Elsevier Science (USA). All rights Reserved

30 Endocrine System
COLUMNAR CELL CARCINOMA. See later.MEDULLARY CARCINOMA WITH PSEUDOPAPIL-
LARY PATTERN. See later.
PROGNOSTIC CONSIDERATIONSPapillary carcinoma is an indolent neoplasm. Ac-cording to a long-term follow-up study from theMayo Clinic, the cancer-related mortality is only6.5%.164 The tumor is locally invasive and has a pro-pensity to metastasize to regional lymph nodes, butdistant metastasis is uncommon and often late(� 10%).73, 192, 193, 315, 316
The most significant prognostic factors are age,stage, and tumor size. To aid in prediction of out-come and selection of therapy, a number of parame-ters (such as age, metastasis, extent of primary can-cer, and tumor size) are taken into considerationto divide patients into low-risk and high-riskgroups.317–320 The low-risk group has an excellentprognosis, and conservative therapy can be consid-ered. The high-risk group has a worse outcome, andthus more aggressive therapy is required.
AGE. Young age is an important favorable prog-nostic factor. Few patients younger than 40 years dieof papillary carcinoma.164, 165, 241, 321–329
SEX. The male sex is often associated with aworse prognosis.226, 323, 325, 326, 329–332
TUMOR SIZE. Risk of death from papillary carci-noma increases with the size of the primary tu-mor.164 Microcarcinomas (�1 to 1.5 cm) have an ex-cellent prognosis, whereas tumors larger than 4 cmfare worse.78, 164, 241, 325, 333
TUMOR STAGE. Extrathyroidal extension wors-ens the prognosis, which is even worse when thereis invasion of the esophagus or trachea.164, 325, 327, 334, 335
Presence of distant metastasis is a highly unfavor-able prognostic feature.157 Papillary carcinoma isunique among carcinomas in that most studies havenot found lymph node metastasis to be of prognos-tic significance.*
TUMOR ENCAPSULATION. Encapsulated papil-lary carcinomas have an excellent prognosis. Thereis no recurrence after excision of the tumor.72, 192, 196
HISTOLOGIC VARIANTS. The prognostic signifi-cance of the variants is listed in Table 44–9.340
COMPLETENESS OF EXCISION. Incomplete tumorexcision increases the probability of recurrence.319, 341
HISTOLOGIC FEATURES. The histologic featuresshown in some studies to be associated with aworse prognosis are marked cellular atypia (multi-layered cells with marked variation in cellular andnuclear size and shape, uneven distribution of chro-matin) and trabecular growth 237, 331, 332, 342pattern(Fig. 44–45). High tumor grade (grade 2), as definedby the presence of marked nuclear atypia, tumor
necrosis, or vascular invasion, has been reported tobe associated with a worse prognosis.339, 343
STROMAL REACTION. Chronic thyroiditis in thebackground thyroid tissue and stromal bone forma-tion have been reported to be favorable prognosticfactors.178, 329
VASCULAR INVASION. Invasion of sizable bloodvessels is an unfavorable prognostic factor.77, 192
IMMUNOHISTOCHEMICAL FEATURES. High den-sity of S-100 protein–positive histiocytes is a favor-able prognostic factor.344 The features associatedwith a worse prognosis are Leu-M1 positivity, epi-thelial membrane antigen positivity, p53 proteinimmunoreactivity, lack of E-cadherin expression,and low-level expression of retinoblastoma pro-tein.160, 303, 345–348
TUMOR ANGIOGENESIS. Whereas some studieshave suggested that a high microvessel count (intra-tumoral microvessel count as highlighted by immu-nostaining for vascular markers) correlates with aworse prognosis, other studies cannot confirm thisfinding.349–351
DNA PDNA PLOIDY. Multiploidy or aneuploidy is anunfavorable prognostic factor.178, 352
N-N-RAS MUTATION. N-ras mutation at codon 61,which is uncommon, is associated with a more ag-gressive behavior.353
Poorly Differentiated ThyroidCarcinoma
CLINICAL CONSIDERATIONSPresentationPoorly differentiated thyroid carcinoma shows
histologic and biologic features intermediate be-tween differentiated thyroid carcinomas and ana-plastic carcinomas.342, 354–357 It retains sufficient dif-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–45. Papillary carcinoma with marked cellular atypia(grade 2). Some studies have shown this feature to be associatedwith a worse prognosis.
*References 77, 164, 321, 324, 325, 328, 329, 336–339.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 31
ferentiation to form small follicular structures and toproduce thyroglobulin, but it lacks the usual mor-phologic characteristics of papillary and follicularcarcinoma.358 The morphologic spectrum of poorlydifferentiated thyroid carcinoma is broad, and insu-lar carcinoma is the best characterized form.354 Analternative designation of “primordial cell carci-noma” has also been proposed in view of the cy-toarchitectural resemblance to the fetal thyroid.355
Poorly differentiated carcinomas can arise denovo or transform from differentiated thyroid carci-nomas, either after repeated recurrences or with thetwo components being discovered simultaneously atdiagnosis.238, 359 They can further transform to ana-plastic carcinoma.
The tumor predominantly affects middle-aged and elderly adults, with a mean age of 54years.89, 354, 355, 358 Women are more commonly af-fected than are men (male-to-female ratio � 1 : 2).Most patients present with an enlarging thyroidmass, and there may be a preceding history of long-standing goiter. Rare patients present with bone me-tastasis. The disease is often locally advanced at pre-sentation, with extrathyroidal extension in morethan 50% of cases.89 Lymph node and distant metas-tases are already present at presentation in approxi-mately 40% and approximately 30% of cases, respec-tively.89, 354, 358
Macroscopic FindingsThe tumor is partially encapsulated or frankly
invasive. It is often large, with a mean size of4.7 cm.358 The cut surface is solid, firm, and fleshy,often punctuated by areas of necrosis and hemor-rhage.
numbers of small abortive follicles (Fig. 44–46). It iscommon to observe retraction artifacts around thetumor islands. The frequent presence of coagulativenecrosis results in a characteristic “peritheliomatous”appearance. The tumor can also form diffuse sheets,trabeculae, festoons, and papillae (Fig. 44–47). Vas-cular invasion is common.354, 360 Some cases mayshow transition with typical papillary carcinoma orfollicular carcinoma. The tumor cells are relativelysmall, with uniform round, hyperchromatic nuclei,indistinct nucleoli and scanty cytoplasm355 (Fig. 44–48). Some mitotic figures can often be identified.
There is a morphologic range of poorly differen-tiated thyroid carcinomas that do not fit the histo-logic description of insular carcinoma. They arecomposed of large cells growing in a trabecular,cribriform, solid, or focally follicular pattern355 (Fig.44–48B).
ImmunohistochemistryPoorly differentiated thyroid carcinoma is im-
munoreactive for cytokeratin, thyroglobulin, andthyroid transcription factor 1. The positive stainingfor thyroglobulin may be confined to the abortivefollicles and isolated cells in the form of paranuclearglobules.354, 355, 361 There is reduced expression of thecyclin-dependent kinase inhibitor p27 and a higherKi-67 index compared with differentiated thyroidcarcinomas.357, 362 Positive staining for Bcl-2 is com-mon (84%), contrasting with the infrequent positivestaining in anaplastic carcinomas (14%).363
Molecular BiologyApproximately half of the cases of poorly differ-
entiated thyroid carcinomas show immunoreactivityfor p53 protein, whereas this feature is uncommonin well-differentiated thyroid carcinomas but com-mon in anaplastic carcinomas. Thus, it appears thatTP53 gene mutation may play a role in the genesisof some cases.363, 364 The finding of point mutationsin the ras oncogene in a proportion of cases suggests
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsInsular carcinoma typically grows in the form of
large solid nests (insulae) decorated with variable
FIGURE 44–46. Insular carcinoma. A. The tumor is infiltrative and highly cellular. B. The tumorfrequently forms islands punctuated by small follicles.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
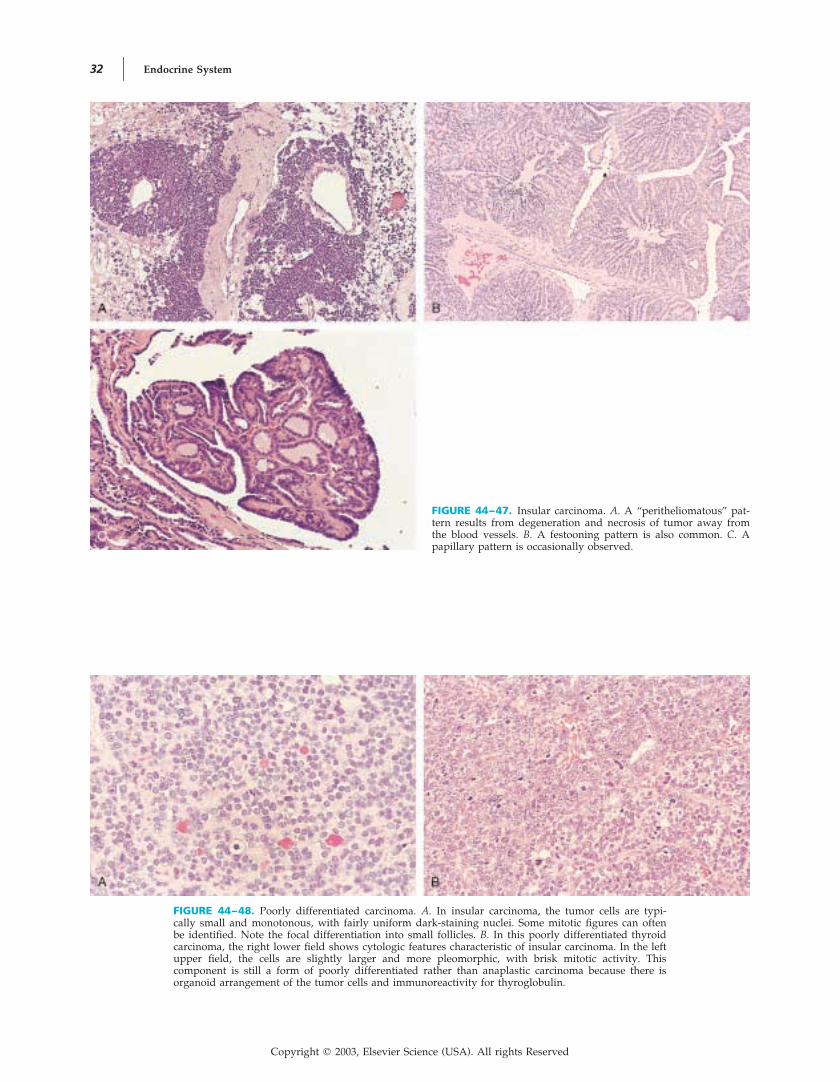
32 Endocrine System
FIGURE 44–47. Insular carcinoma. A. A “peritheliomatous” pat-tern results from degeneration and necrosis of tumor away fromthe blood vessels. B. A festooning pattern is also common. C. Apapillary pattern is occasionally observed.
FIGURE 44–48. Poorly differentiated carcinoma. A. In insular carcinoma, the tumor cells are typi-cally small and monotonous, with fairly uniform dark-staining nuclei. Some mitotic figures can oftenbe identified. Note the focal differentiation into small follicles. B. In this poorly differentiated thyroidcarcinoma, the right lower field shows cytologic features characteristic of insular carcinoma. In the leftupper field, the cells are slightly larger and more pleomorphic, with brisk mitotic activity. Thiscomponent is still a form of poorly differentiated rather than anaplastic carcinoma because there isorganoid arrangement of the tumor cells and immunoreactivity for thyroglobulin.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 33
a relationship with follicular carcinoma in suchcases.89, 365
Differential Diagnosis
MEDULLARY CARCINOMA. Insular carcinomamay mimic medullary carcinoma as a result of thegrowth pattern and amyloid-like sclerosis. The dis-tinction can be readily made by immunostaining forthyroglobulin and calcitonin (see Table 44–1).
ANAPLASTIC THYROID CARCINOMA. Poorly dif-ferentiated carcinoma lacks the prominent nuclearpleomorphism and frequent mitoses of anaplasticcarcinoma and furthermore shows abortive folliclesand thyroglobulin immunoreactivity.
SOLID VARIANT OF PAPILLARY CARCINOMA.See Table 44–9.
PROGNOSTIC CONSIDERATIONSRecurrence or metastasis develops in approximately60% of cases after treatment.89, 354, 355 In contrast tothe rapidly fatal course of anaplastic carcinoma,poorly differentiated carcinoma causes death afterseveral years (mean survival, 3.9 years). The long-term survival rate is around 40%.89, 354–356, 366 Deathis often attributable to metastasis rather than to un-controllable local disease. The treatment usually con-sists of total thyroidectomy, radioactive iodine, andsuppressive thyroxine.354 Radiotherapy and chemo-therapy may also be considered in view of the unfa-vorable prognosis. Poor prognostic factors includeadvanced age, large tumor size, extrathyroidal ex-tension, lymph node metastasis, and presence of ananaplastic carcinoma component.356
Whether the presence of a minor component ofpoorly differentiated carcinoma worsens the progno-sis of an otherwise typical differentiated thyroid car-cinoma remains controversial.360, 367–369 The outcomewill probably be worsened if the poorly differenti-ated carcinoma component is found in the invasiveportions of the tumor but not if the component isconfined to an encapsulated tumor.
Anaplastic (Undifferentiated)Carcinoma
CLINICAL CONSIDERATIONSPresentationAnaplastic carcinoma is predominantly a disease
of older adults with a mean age of 67 years; there isa slight female predominance.238, 370–372 The patientspresent with a rapidly enlarging thyroid mass ormetastatic tumor in cervical lymph nodes or distantsites. The mass lesion is frequently accompanied byhoarseness, dysphagia, and dyspnea. Some patientshave a history of long-standing goiter or well-differ-entiated thyroid carcinoma.238, 359, 370, 373, 374 Squamouscell carcinoma and carcinosarcoma can be consid-ered variants of anaplastic carcinoma.
Macroscopic FindingsAnaplastic thyroid carcinoma typically shows in-
filtration of the perithyroid soft tissues and adjacentstructures, such as the larynx and pharynx. The tu-mor is fleshy, with areas of necrosis and hemor-rhage.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsAnaplastic thyroid carcinoma is characterized by
highly pleomorphic tumor cells that lack any orga-noid growth pattern238, 374 (Fig. 44–49). The tumorgrows in diffuse sheets, irregular islands, cords, andfascicles. The tumor cells are large and are polygo-nal, ovoid, or spindly; some foci can show squa-mous differentiation229 (Fig. 44–50). A pseudoan-giomatoid pattern resembling angiosarcoma can beseen in some cases (Fig. 44–51). Mitotic figures arefrequent, and coagulative tumor necrosis is often ex-tensive (see Fig. 44–49). There is a tendency for thetumor cells to permeate and replace the walls ofblood vessels, obliterating their lumina238 (Fig.44–52). There are commonly some admixed inflam-matory cells, particularly neutrophils.
A component of papillary carcinoma, follicularcarcinoma, or poorly differentiated thyroid carci-noma can be found in approximately 50% of cases,suggesting that the anaplastic carcinoma arisesthrough a process of “dedifferentiation”238, 354, 366, 373–377
(Fig. 44–53).The morphologic variants of anaplastic carci-
noma are listed in Table 44–11 (Figs. 44–54 and44–55).300, 373, 378–391 True “small cell” anaplastic carci-nomas are extremely rare; most cases diagnosed assuch in the past represent malignant lymphoma,medullary carcinoma, or poorly differentiated thy-roid carcinoma.238, 373, 374, 392–396
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–49. Anaplastic carcinoma. The tumor is solid grow-ing, lacking organoid features. Coagulative necrosis is a commonfinding.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
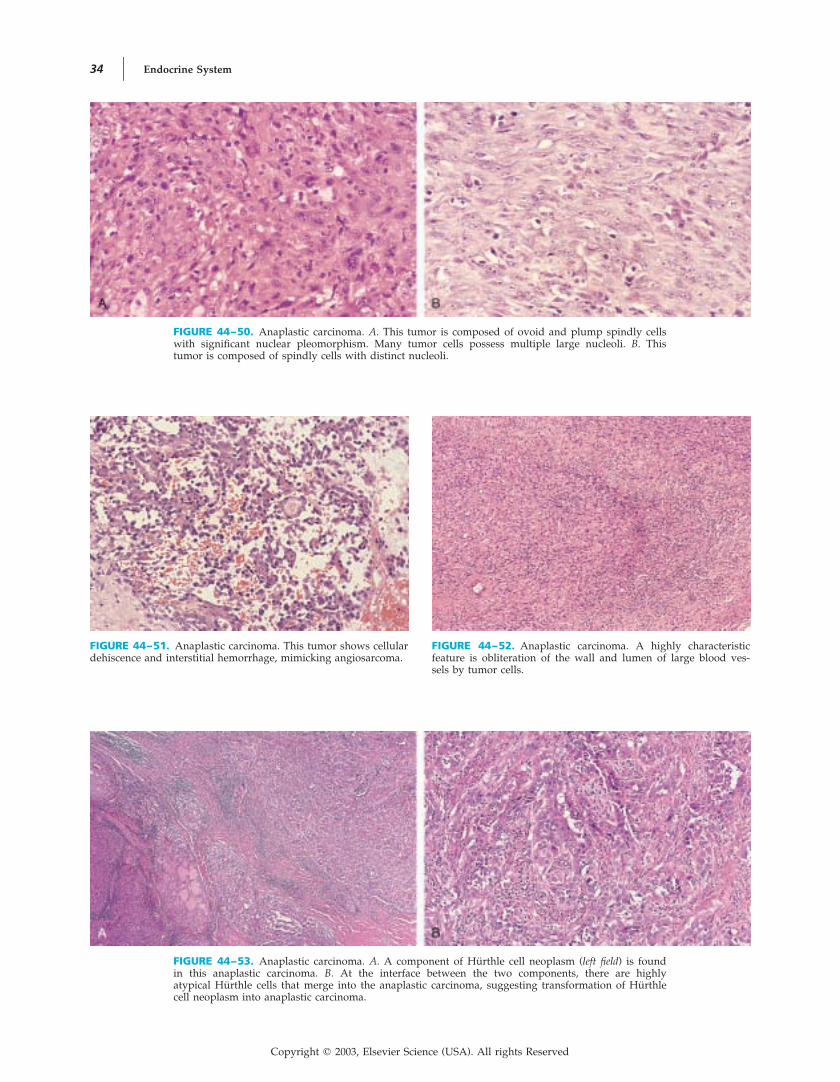
34 Endocrine System
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–51. Anaplastic carcinoma. This tumor shows cellulardehiscence and interstitial hemorrhage, mimicking angiosarcoma.
FIGURE 44–50. Anaplastic carcinoma. A. This tumor is composed of ovoid and plump spindly cellswith significant nuclear pleomorphism. Many tumor cells possess multiple large nucleoli. B. Thistumor is composed of spindly cells with distinct nucleoli.
FIGURE 44–52. Anaplastic carcinoma. A highly characteristicfeature is obliteration of the wall and lumen of large blood ves-sels by tumor cells.
FIGURE 44–53. Anaplastic carcinoma. A. A component of Hurthle cell neoplasm (left field) is foundin this anaplastic carcinoma. B. At the interface between the two components, there are highlyatypical Hurthle cells that merge into the anaplastic carcinoma, suggesting transformation of Hurthlecell neoplasm into anaplastic carcinoma.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 35
ImmunohistochemistryIn anaplastic carcinoma, epithelial markers can-
not be consistently demonstrated, except in areas ofsquamous differentiation. Cytokeratin is positive inonly approximately half of the cases, whereas epi-thelial membrane antigen is positive in only 33% to55%.238, 370, 372, 397, 398 Vimentin is positive in 50% to100% but has no diagnostic value.372, 397
Thyroglobulin and thyroid transcription factor 1are negative in the anaplastic carcinoma component,but immunostaining for these markers can some-times highlight the preexisting differentiated thyroidcarcinoma component if it is present.2, 3, 370, 393, 399
Calcitonin is negative.238, 370 Focal immunoreactivity
for factor VIII–related antigen has been reported,possibly indicating focal divergent endothelial differ-entiation.398
Molecular BiologyAberrations in the p53 pathways have been im-
plicated in the transformation of differentiated thy-roid carcinoma to anaplastic carcinoma.364, 377, 400–404
The anaplastic carcinoma component commonlyshows strong immunoreactivity for p53 protein,whereas the differentiated thyroid carcinoma com-ponent is negative. The �-catenin gene commonlyshows somatic mutations in anaplastic carcinomaand may thus play a key role in the development ofthis tumor type.405
Differential DiagnosisThe main pitfalls in diagnosis of anaplastic car-
cinoma are listed in Table 44–12.SARCOMA. Anaplastic carcinomas composed
predominantly of spindly cells are difficult to distin-guish from sarcomas. However, because primarysarcomas of the thyroid are rare, they should bediagnosed only when there is strong proof of a defi-nite line of differentiation, such as smooth muscle ornerve sheath differentiation.238
LARGE CELL LYMPHOMA. Large cell lymphomacan be distinguished from anaplastic carcinoma bythe poor cellular cohesion, presence of plasmacytoidor amphophilic cytoplasm, infiltration of thyroid fol-licular epithelium, stuffing of follicular lumina bytumor cells, and immunohistochemical expression ofleukocyte markers.
METASTATIC CARCINOMA. Clinical correlationis required to distinguish anaplastic carcinoma from
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–11. Variants of Anaplastic Thyroid Carcinoma
Variant* Defining Morphologic FeaturesEntity for Which the Variant May beMistaken
Angiomatoid variant Presence of irregular cleftlike tumor cell– linedspaces mimicking vascular spaces
Angiosarcoma
Osteoclastic variant Reactive osteoclastic giant cells are interspersed inan otherwise typical anaplastic carcinoma
Giant cell tumor of larynx (thyroid cartilage)
Paucicellular variant Low-cellularity tumor with large areas of sclerosisand infarction. A sprinkling of lymphocytes isoften present. Focally, spindly tumor cells withmild to moderate nuclear atypia can be identi-fied. These spindle cells also obliterate the walland lumina of blood vessels.
Riedel’s thyroiditis
Lymphoepithelioma-likevariant
Irregular infiltrative islands and sheets of syncytial-appearing pleomorphic tumor cells, heavily in-termingled with lymphocytes and plasma cells
CASTLE
Squamous cell carcinoma Identical to squamous cell carcinoma occurring inother sites
CASTLE
Adenosquamous carcinoma Squamous cell carcinoma with areas of mucin pro-duction
—
Carcinosarcoma Anaplastic carcinoma accompanied by a sarcoma-tous component with muscle, fat, cartilage, orbone differentiation
—
* None of these variants has clinical or prognostic significance.
FIGURE 44–54. Anaplastic carcinoma, osteoclastic variant. Non-neoplastic osteoclast giant cells are dispersed among the highlypleomorphic ovoid tumor cells.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

36 Endocrine System
metastatic carcinoma, although metastatic carcinomashould be suspected if the bulk of the tumor lieswithin lymphovascular spaces. The presence of acomponent of differentiated thyroid carcinomastrongly favors the diagnosis of anaplastic carci-noma.
PARATHYROID CARCINOMA. Parathyroid carci-noma presenting as a thyroid mass is not uncom-monly misdiagnosed as anaplastic thyroid carci-noma. The distinction is important becauseparathyroid carcinoma is a much more indolent neo-plasm. Histologic clues to the correct diagnosis arepresence of clear cells, mixture of cell types, paucityof mitotic figures, and prominent delicate vascula-ture.
RIEDEL’S THYROIDITIS. The paucicellular variantof anaplastic carcinoma can be mistaken for Riedel’sthyroiditis, which has a favorable prognosis. Fea-tures favoring the diagnosis of a paucicellular vari-ant of anaplastic carcinoma are presence of infarc-tion, cytologic atypia (albeit focal and often subtle),vascular occlusion by spindle cells, discrete interface
with the adjacent tissue, and cytokeratin immunore-activity.
ANGIOSARCOMA. See later.SOLID VARIANT OF PAPILLARY CARCINOMA.
The solid variant of papillary carcinoma can be dis-tinguished from anaplastic carcinoma by the typicalnuclear features, lack of bizarre cells, and paucity ofmitotic figures.
POORLY DIFFERENTIATED THYROID CARCI-NOMA. Poorly differentiated thyroid carcinoma usu-ally shows definite cellular organization into islandswith microfollicles, relatively small cells, fairly uni-form nuclei, lack of bizarre cells, and thyroglobulinimmunoreactivity.
THYMIC AND RELATED TUMORS. See later.
PROGNOSTIC CONSIDERATIONSAnaplastic carcinoma is inoperable in about half ofthe cases because of extensive local disease. Regionallymph node and distant metastases (mostly lungs,sometimes bones) are common. The cause of death
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–55. Anaplastic carcinoma, paucicellular variant. A. The tumor infiltrates and replaces thethyroid parenchyma. The extremely low cellularity, fibrosis, and sprinkling of chronic inflammatorycells impart an impression of thyroiditis. B. In areas, there is dense fibrous tissue with ghost shadowsof blood vessels, indicating prior infarction of the tissue. C. Careful scrutiny of the less hypocellularareas reveals myofibroblast-like spindly cells that are in fact tumor cells. Mild nuclear atypia isevident. D. Identification of blood vessels showing obliteration by atypical spindly cells provides thebest clue to the diagnosis of anaplastic carcinoma.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 37
is usually upper airway obstruction from extensivelocal disease or a combination of the effects of localand metastatic disease.406 The median survival isonly 3 to 4 months, and the 5-year survival rateis 5% to 10%.366, 377, 407–409 The rare patients whocan achieve a cure usually have relatively small(�5 cm) tumors confined to the thyroid gland andhave been treated with aggressive local interven-tion.374, 406, 407, 410–412 Unfavorable prognostic factors
for anaplastic carcinoma include large tumor size(�6 cm), extension of tumor beyond the neck, oldage at diagnosis, male gender, and dyspnea as apresenting symptom.406
Columnar Cell Carcinoma
CLINICAL AND PROGNOSTICCONSIDERATIONSAlthough columnar cell carcinoma was originally re-ported as an aggressive neoplasm,413 studies haveshown that aggressive behavior is observed only inthe frankly invasive tumors. For invasive tumors,there is slight male predilection and the mean age is55.6 years.413–422 There is a high frequency of re-gional lymph node and distant metastases. The mor-tality rate, which is at least 75%, is high. In contrast,for encapsulated tumors, there is marked femalepredominance and patients are younger (mean,42.7 Most patients remain well on414, 422–425years).follow-up.
There are divergent views on the nature of co-lumnar cell carcinoma: a distinct tumor type versusa variant of thyroid carcinoma. In fact, occasionalcases show merging with tall cell papillary carci-noma.419, 421, 422, 426, 427 There is also some morphologicoverlap with the cribriform-morular variant of papil-lary carcinoma and familial adenomatous polyposis–associated thyroid carcinoma.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsColumnar cell carcinoma shows heterogeneous
growth patterns, including papillary, complex glan-dular, cribriform, and solid. The cells are tall colum-nar and characteristically show marked nuclearpseudostratification and hyperchromasia, reminis-cent of colorectal adenocarcinoma or endometrioidadenocarcinoma (Fig. 44–56). Subnuclear vacuolesand diffuse cytoplasmic clearing can sometimes oc-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–12. Main Pitfalls in Diagnosis of AnaplasticThyroid Carcinoma
Main Diagnostic PitfallEntities That May Cause theDiagnostic Confusion
Benign lesions mimicking an-aplastic thyroid carcinoma
Reparative cellular atypia inbenign tumor attributableto infarction or fine-needleaspiration injury
Florid granulation tissue for-mation resulting from or-ganization of infarcted tu-mor
Inflammatory pseudotumor
Low-grade malignant tumorsmimicking anaplastic thy-roid carcinoma
Papillar carcinoma, solid vari-ant
Mucoepidermoid carcinomaSclerosing mucoepidermoid
carcinoma with eosino-philia
Thymic and branchial pouch–related tumors (ectopicthymoma, SETTLE, CASTLE)
Parathyroid carcinomaMalignant lymphoma
Anaplastic thyroid carcinomavariant potentially misdi-agnosed as benign or low-grade malignant lesions
Paucicellular variant, whichmay be mistaken for Rie-del’s thyroiditis
Lymphoepithelioma-like car-cinoma variant, which maybe mistaken for CASTLE ormalignant lymphoma
FIGURE 44–56. Columnar cell carcinoma. A. Complex tubulopapillary structures characterize thegrowth pattern of this tumor. B. The lining cells are markedly pseudostratified cells and possesschromatin-rich nuclei.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
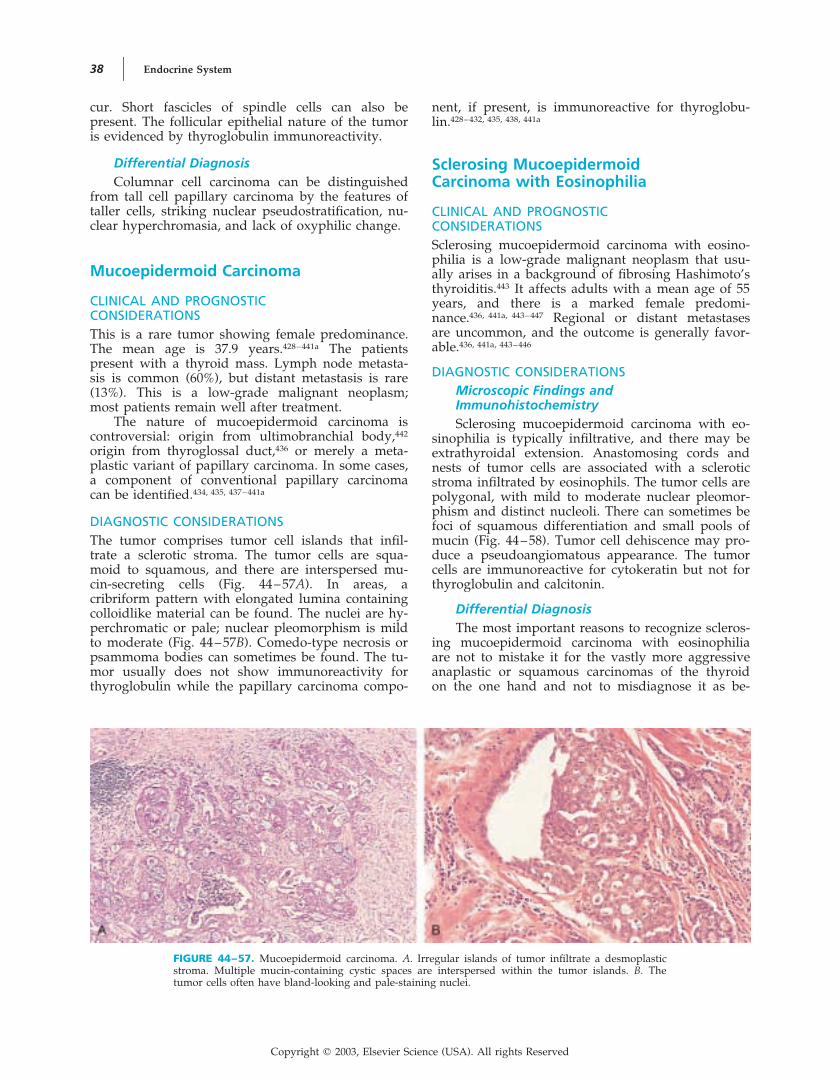
38 Endocrine System
cur. Short fascicles of spindle cells can also bepresent. The follicular epithelial nature of the tumoris evidenced by thyroglobulin immunoreactivity.
Differential DiagnosisColumnar cell carcinoma can be distinguished
from tall cell papillary carcinoma by the features oftaller cells, striking nuclear pseudostratification, nu-clear hyperchromasia, and lack of oxyphilic change.
Mucoepidermoid Carcinoma
CLINICAL AND PROGNOSTICCONSIDERATIONSThis is a rare tumor showing female predominance.The mean age is 37.9 years.428–441a The patientspresent with a thyroid mass. Lymph node metasta-sis is common (60%), but distant metastasis is rare(13%). This is a low-grade malignant neoplasm;most patients remain well after treatment.
The nature of mucoepidermoid carcinoma iscontroversial: origin from ultimobranchial body,442
origin from thyroglossal duct,436 or merely a meta-plastic variant of papillary carcinoma. In some cases,a component of conventional papillary carcinomacan be identified.434, 435, 437–441a
DIAGNOSTIC CONSIDERATIONSThe tumor comprises tumor cell islands that infil-trate a sclerotic stroma. The tumor cells are squa-moid to squamous, and there are interspersed mu-cin-secreting cells (Fig. 44–57A). In areas, acribriform pattern with elongated lumina containingcolloidlike material can be found. The nuclei are hy-perchromatic or pale; nuclear pleomorphism is mildto moderate (Fig. 44–57B). Comedo-type necrosis orpsammoma bodies can sometimes be found. The tu-mor usually does not show immunoreactivity forthyroglobulin while the papillary carcinoma compo-
nent, if present, is immunoreactive for thyroglobu-lin.428–432, 435, 438, 441a
Sclerosing MucoepidermoidCarcinoma with Eosinophilia
CLINICAL AND PROGNOSTICCONSIDERATIONSSclerosing mucoepidermoid carcinoma with eosino-philia is a low-grade malignant neoplasm that usu-ally arises in a background of fibrosing Hashimoto’sthyroiditis.443 It affects adults with a mean age of 55years, and there is a marked female predomi-
Regional or distant metastases436, 441a, 443–447nance.are uncommon, and the outcome is generally favor-able.436, 441a, 443–446
DIAGNOSTIC CONSIDERATIONSMicroscopic Findings andImmunohistochemistrySclerosing mucoepidermoid carcinoma with eo-
sinophilia is typically infiltrative, and there may beextrathyroidal extension. Anastomosing cords andnests of tumor cells are associated with a scleroticstroma infiltrated by eosinophils. The tumor cells arepolygonal, with mild to moderate nuclear pleomor-phism and distinct nucleoli. There can sometimes befoci of squamous differentiation and small pools ofmucin (Fig. 44–58). Tumor cell dehiscence may pro-duce a pseudoangiomatous appearance. The tumorcells are immunoreactive for cytokeratin but not forthyroglobulin and calcitonin.
Differential DiagnosisThe most important reasons to recognize scleros-
ing mucoepidermoid carcinoma with eosinophiliaare not to mistake it for the vastly more aggressiveanaplastic or squamous carcinomas of the thyroidon the one hand and not to misdiagnose it as be-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–57. Mucoepidermoid carcinoma. A. Irregular islands of tumor infiltrate a desmoplasticstroma. Multiple mucin-containing cystic spaces are interspersed within the tumor islands. B. Thetumor cells often have bland-looking and pale-staining nuclei.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 39
nign squamous metaplasia on the other. In contrastto anaplastic or squamous cell carcinoma, thegrowth pattern is more diffuse with formation ofcords or large islands; nuclear atypia is generallynot striking, and the inflammatory component isusually eosinophilic rather than neutrophilic.
Mucinous Carcinoma
Primary mucinous carcinoma of the thyroid is ex-tremely rare; only four cases have been reported inthe literature.448–451 It is histologically identical tocolloid carcinoma of other sites, except that thyro-globulin is usually positive.
Medullary Thyroid Carcinoma
CLINICAL CONSIDERATIONSPresentationMedullary thyroid carcinoma is a malignant
neoplasm exhibiting parafollicular C cell differentia-tion.452 The patients are mostly adults with slightfemale predominance.453–464 Most patients presentwith a thyroid mass or cervical lymphadenopathy.465
Some patients may have diarrhea or, more rarely,Cushing’s syndrome.454, 466 The stage distribution atpresentation is as follows: stage I, 21%; stage II,21%; stage III, 47%; and stage IV, 12%.467 In somecenters, routine screening of the calcitonin level inpatients with nodular thyroid disease allows earlydiagnosis of unsuspected sporadic medullary thy-roid carcinoma.468–470
Approximately 20% to 30% of medullary carci-nomas are heritable (autosomal dominant with highpenetrance).453, 455 The tumor often appears at an ear-lier age, multicentrically and bilaterally, and on abackground of C cell hyperplasia454–461, 471–473 (Table
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–58. Sclerosing mucoepidermoid carcinoma with eosinophilia. A. Cords of polygonal tu-mor cells with distinct nucleoli infiltrate a sclerotic stroma richly infiltrated by eosinophils andlymphocytes. B. Irregular islands of squamoid cells are intermingled with eosinophils and lympho-cytes. The mucinous component is usually difficult to appreciate without recourse to mucin stain.
44–13). Germline mutation in the RET gene is theunderlying molecular event.462–464 Thyroidectomy isusually performed for the mutant RET gene carriersidentified through screening of family members, andthe medullary carcinomas diagnosed in such circum-stances are often small and at an early stage.
Macroscopic FindingsMedullary carcinoma has a predilection for the
middle third of the lateral lobe, where normal Ccells are most prevalent.460 It is infiltrative, circum-scribed, or encapsulated474, 475 (Fig. 44–59). It is firmand grayish white, tan, or reddish brown. Hemor-rhage and necrosis can be seen in larger tumors.476
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsMedullary carcinoma typically grows in the
form of sheets, packets, or irregular islands tra-
FIGURE 44–59. Medullary carcinoma. This tumor exhibits inva-sive borders, but other cases can have circumscribed borders.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

40
TABLE 44–13. Sporadic and Hereditary Forms of Medullary Thyroid Carcinoma (MTC)
Sporadic MTC
Hereditary MTC
Familial MTC MEN 2A MEN 2B
Mean age at diagnosis 44–50 y 29–43 y 21–38 y 12–23 y
Sex ratio Male-female 1 : 1.4 � Male-Female 1 : 1.1 �
Other components of the syn-drome
Nil Nil PheochromocytomaParathyroid hyperplasia
PheochromocytomaMucosal neuromasMarfanoid appearance
Germline mutation in RETproto-oncogene
Nil Mutation involving exon 10,11, 13, or 14
Mutation involving exon 10 or 11 Mutation involving exon 16 (co-don 918), with ATG : ACG (me-thionine : threonine)
Bilaterality and C cell hyperpla-sia in the background
Uncommon � Frequent �
Metastases at diagnosis Lymph node: 40%–50%Distant: 12%
Lymph node: 10%–20%Distant: 0%
Lymph node: 14%Distant: 0%–3%
Lymph node: 38%Distant: 20%
Tumor-related mortality �30% �0% (most indolent amongthe various types)
0%–17% 50% (most aggressive)
MEN, multiple endocrine neoplasia.
38419W
eidner
(SAU
NM
)L
EFT
INT
ER
AC
TIV
E
shortstand
ardlong
topof
RH
Copyright
�2003,E
lsevierScience
(USA
).All
rightsR
eserved
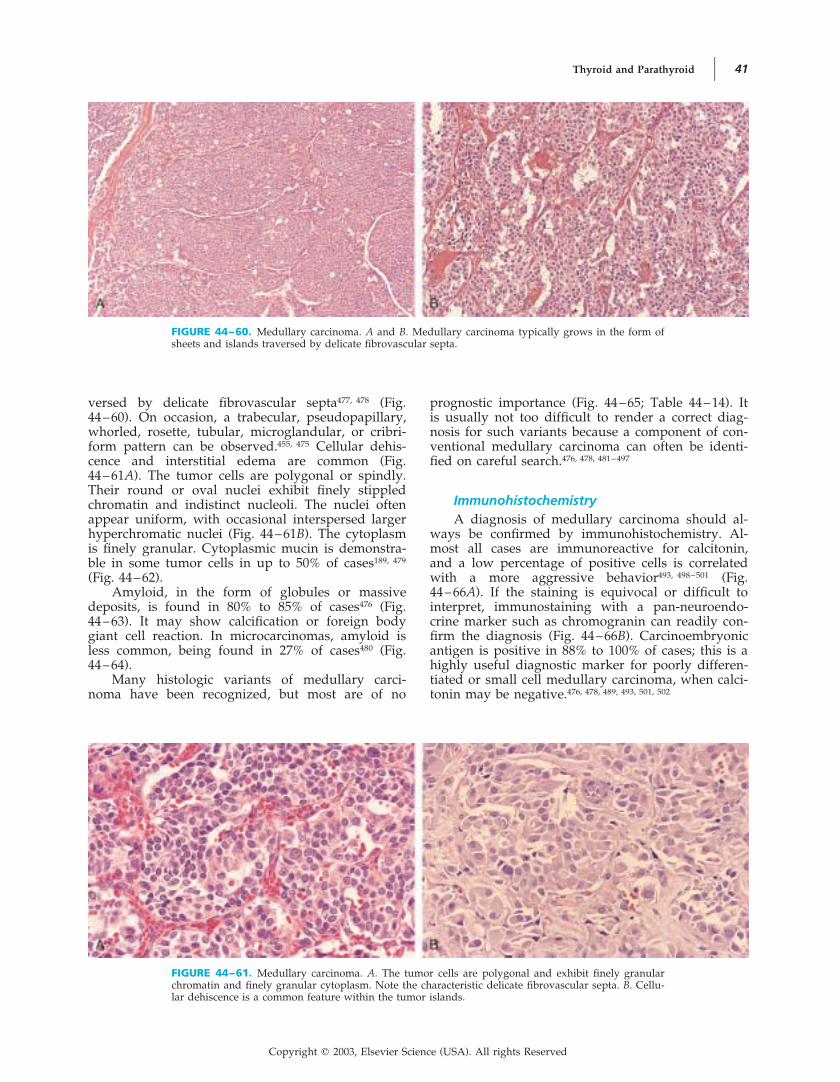
Thyroid and Parathyroid 41
versed by delicate fibrovascular (Fig.477, 478septa44–60). On occasion, a trabecular, pseudopapillary,whorled, rosette, tubular, microglandular, or cribri-form pattern can be Cellular dehis-455, 475observed.cence and interstitial edema are common (Fig.44–61A). The tumor cells are polygonal or spindly.Their round or oval nuclei exhibit finely stippledchromatin and indistinct nucleoli. The nuclei oftenappear uniform, with occasional interspersed largerhyperchromatic nuclei (Fig. 44–61B). The cytoplasmis finely granular. Cytoplasmic mucin is demonstra-ble in some tumor cells in up to 50% of cases189, 479
(Fig. 44–62).Amyloid, in the form of globules or massive
deposits, is found in 80% to 85% of cases476 (Fig.44–63). It may show calcification or foreign bodygiant cell reaction. In microcarcinomas, amyloid isless common, being found in 27% of cases480 (Fig.44–64).
Many histologic variants of medullary carci-noma have been recognized, but most are of no
prognostic importance (Fig. 44–65; Table 44–14). Itis usually not too difficult to render a correct diag-nosis for such variants because a component of con-ventional medullary carcinoma can often be identi-fied on careful search.476, 478, 481–497
ImmunohistochemistryA diagnosis of medullary carcinoma should al-
ways be confirmed by immunohistochemistry. Al-most all cases are immunoreactive for calcitonin,and a low percentage of positive cells is correlatedwith a more aggressive (Fig.493, 498–501behavior44–66A). If the staining is equivocal or difficult tointerpret, immunostaining with a pan-neuroendo-crine marker such as chromogranin can readily con-firm the diagnosis (Fig. 44–66B). Carcinoembryonicantigen is positive in 88% to 100% of cases; this is ahighly useful diagnostic marker for poorly differen-tiated or small cell medullary carcinoma, when calci-tonin may be negative.476, 478, 489, 493, 501, 502
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–60. Medullary carcinoma. A and B. Medullary carcinoma typically grows in the form ofsheets and islands traversed by delicate fibrovascular septa.
FIGURE 44–61. Medullary carcinoma. A. The tumor cells are polygonal and exhibit finely granularchromatin and finely granular cytoplasm. Note the characteristic delicate fibrovascular septa. B. Cellu-lar dehiscence is a common feature within the tumor islands.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

42 Endocrine System
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–62. Medullary carcinoma. Staining with periodicacid–Schiff shows presence of mucin vacuoles in some tumorcells.
TABLE 44–14. Variants of Medullary Thyroid Carcinoma
Variant* Defining Morphologic FeaturesEntities for Which the Variant May BeMistaken
Glandular-follicular Presence of glandular or follicular structures whichmay contain eosinophilic secretion in the lumina
The cytoplasm toward the luminal aspect is oftenmore deeply eosinophilic due to polarization ofneurosecretory granules.
Follicular adenoma or carcinomaPoorly differentiated (insular) thyroid carci-
noma
Papillary Presence of pseudopapillae due to cellular dehis-cence, and only rarely are there true papillary for-mations
Papillary carcinoma
Oxyphilic Tumor cells with abundant eosinophilic granular cyto-plasm due to accumulation of mitochondria
Hurthle cell neoplasm
Clear cell Presence of tumor cells with water-clear cytoplasm Other clear cell tumors
Spindle cell Presence of spindly tumor cells arranged in fasciclesor whorls
Mesenchymal tumors
Pigmented Presence of brown melanin pigment in some tumorcells
—
Squamous Presence of squamous differentiation Squamous cell carcinoma
Small cell Tumor composed predominantly of small cells, oftenwith nuclear molding, resembling small cell carci-noma of lung
Malignant lymphoma
Giant cell (anaplastic) Presence of large cells with bizarre and pleomorphicnuclei, but mitotic figures are rare
Anaplastic carcinoma
Neuroblastoma-like Presence of fibrillary matrix or rosettes, resemblingneuroblastoma
Malignant lymphomaMetastatic neuroblastomaPeripheral primitive neuroectodermal tumor
Carcinoid-like Histologic features resembling intestinal carcinoid,with tumor islands, trabeculae, or glands separatedby fibrohyaline stroma
Metastatic carcinoidParagangliomaFollicular neoplasm
Hyalinizing trabecularadenoma–like
Wavy trabeculae of tumor cells, which merge intoabundant extracellular hyaline material, mimickinghyalinizing trabecular adenoma
Hyalinizing trabecular adenomaParaganglioma
Paraganglioma-like Tumor forming packets delineated by a delicate vas-culature
Paraganglioma
* The listed variants have no clinical or prognostic significance, except the small cell type, which is more aggressive. The prognostic implication ofthe giant cell variant is still unsettled.
FIGURE 44–63. Medullary carcinoma. Abundant amyloid depos-its (upper field) are evident in this tumor.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
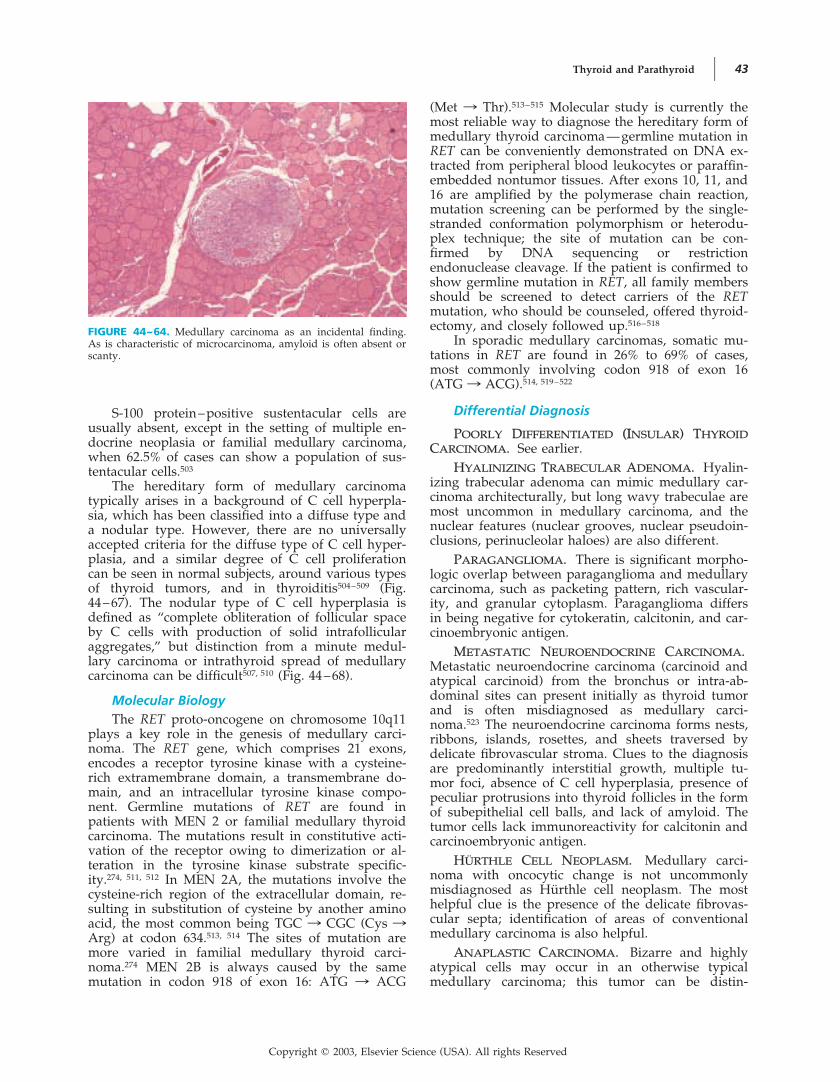
Thyroid and Parathyroid 43
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
S-100 protein–positive sustentacular cells areusually absent, except in the setting of multiple en-docrine neoplasia or familial medullary carcinoma,when 62.5% of cases can show a population of sus-tentacular cells.503
The hereditary form of medullary carcinomatypically arises in a background of C cell hyperpla-sia, which has been classified into a diffuse type anda nodular type. However, there are no universallyaccepted criteria for the diffuse type of C cell hyper-plasia, and a similar degree of C cell proliferationcan be seen in normal subjects, around various typesof thyroid tumors, and in thyroiditis504–509 (Fig.44–67). The nodular type of C cell hyperplasia isdefined as “complete obliteration of follicular spaceby C cells with production of solid intrafollicularaggregates,” but distinction from a minute medul-lary carcinoma or intrathyroid spread of medullarycarcinoma can be difficult507, 510 (Fig. 44–68).
Molecular BiologyThe RET proto-oncogene on chromosome 10q11
plays a key role in the genesis of medullary carci-noma. The RET gene, which comprises 21 exons,encodes a receptor tyrosine kinase with a cysteine-rich extramembrane domain, a transmembrane do-main, and an intracellular tyrosine kinase compo-nent. Germline mutations of RET are found inpatients with MEN 2 or familial medullary thyroidcarcinoma. The mutations result in constitutive acti-vation of the receptor owing to dimerization or al-teration in the tyrosine kinase substrate specific-ity.274, 511, 512 In MEN 2A, the mutations involve thecysteine-rich region of the extracellular domain, re-sulting in substitution of cysteine by another aminoacid, the most common being TGC : CGC (Cys :Arg) at codon 634.513, 514 The sites of mutation aremore varied in familial medullary thyroid carci-noma.274 MEN 2B is always caused by the samemutation in codon 918 of exon 16: ATG : ACG
(Met : Thr).513–515 Molecular study is currently themost reliable way to diagnose the hereditary form ofmedullary thyroid carcinoma—germline mutation inRET can be conveniently demonstrated on DNA ex-tracted from peripheral blood leukocytes or paraffin-embedded nontumor tissues. After exons 10, 11, and16 are amplified by the polymerase chain reaction,mutation screening can be performed by the single-stranded conformation polymorphism or heterodu-plex technique; the site of mutation can be con-firmed by DNA sequencing or restrictionendonuclease cleavage. If the patient is confirmed toshow germline mutation in RET, all family membersshould be screened to detect carriers of the RETmutation, who should be counseled, offered thyroid-ectomy, and closely followed up.516–518
In sporadic medullary carcinomas, somatic mu-tations in RET are found in 26% to 69% of cases,most commonly involving codon 918 of exon 16(ATG : ACG).514, 519–522
Differential Diagnosis
POORLY DIFFERENTIATED (I(INSULAR) THYROIDCARCINOMA. See earlier.
HYALINIZING TRABECULAR ADENOMA. Hyalin-izing trabecular adenoma can mimic medullary car-cinoma architecturally, but long wavy trabeculae aremost uncommon in medullary carcinoma, and thenuclear features (nuclear grooves, nuclear pseudoin-clusions, perinucleolar haloes) are also different.
PARAGANGLIOMA. There is significant morpho-logic overlap between paraganglioma and medullarycarcinoma, such as packeting pattern, rich vascular-ity, and granular cytoplasm. Paraganglioma differsin being negative for cytokeratin, calcitonin, and car-cinoembryonic antigen.
METASTATIC NEUROENDOCRINE CARCINOMA.Metastatic neuroendocrine carcinoma (carcinoid andatypical carcinoid) from the bronchus or intra-ab-dominal sites can present initially as thyroid tumorand is often misdiagnosed as medullary carci-noma.523 The neuroendocrine carcinoma forms nests,ribbons, islands, rosettes, and sheets traversed bydelicate fibrovascular stroma. Clues to the diagnosisare predominantly interstitial growth, multiple tu-mor foci, absence of C cell hyperplasia, presence ofpeculiar protrusions into thyroid follicles in the formof subepithelial cell balls, and lack of amyloid. Thetumor cells lack immunoreactivity for calcitonin andcarcinoembryonic antigen.
HURTHLE CELL NEOPLASM. Medullary carci-noma with oncocytic change is not uncommonlymisdiagnosed as Hurthle cell neoplasm. The mosthelpful clue is the presence of the delicate fibrovas-cular septa; identification of areas of conventionalmedullary carcinoma is also helpful.
ANAPLASTIC CARCINOMA. Bizarre and highlyatypical cells may occur in an otherwise typicalmedullary carcinoma; this tumor can be distin-
FIGURE 44–64. Medullary carcinoma as an incidental finding.As is characteristic of microcarcinoma, amyloid is often absent orscanty.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

44 Endocrine System
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–65. Variants of medullary carcinoma. A. Glandular-follicular variant, which can potentially be mistaken for a follicu-lar neoplasm. B. Papillary variant comprising pseudopapillae pro-duced by cellular dehiscence. The tumor cells lack the typicalnuclear features of papillary carcinoma. C. Oncocytic variant,which can be mistaken for Hurthle cell follicular neoplasm. D.Clear cell variant. E. Spindle cell variant, which may be mistakenfor a mesenchymal neoplasm. F. Small cell variant. G. Giant cellvariant.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 45
FIGURE 44–66. Medullary carcinoma, immunohistochemical staining. A. All tumor cells show posi-tive staining for calcitonin. B. Strong positive granular staining for chromogranin is observed.
guished from anaplastic carcinoma by the presenceof many bland-looking cells among the bizarre cellsand the paucity of mitotic figures.
PARATHYROID NEOPLASM. See later.
PROGNOSTIC CONSIDERATIONSThe tumor tends to spread by lymphatics to lymphnodes of the neck (one third to two thirds) andupper mediastinum.454, 465, 524 Local recurrence devel-ops in about one third of cases after treatment.465
Late in the course, the tumor may metastasize toother sites, such as lungs, liver, adrenal, and bone,although distant metastasis is already present in 8%of patients at presentation.524 Patients may still sur-vive for many years despite the presence of distantmetastases. The 5-year, 10-year, and 15-year survivalrates are 65% to 87%, 51% to 78%, and 65%, respec-tively,453, 465, 525–527 indicating that this tumor is indo-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–67. C cell hyperplasia, diffuse type, found adjacentto a follicular adenoma. This form of C cell hyperplasia cannot beappreciated in conventional histologic sections. Immunostainingfor calcitonin shows increased isolated C cells (stained brown).These cells lie within the basal lamina of the follicles.
lent and not rapidly lethal. However, there is still anexcess mortality 10 years after a diagnosis of medul-lary carcinoma.527 Because medullary carcinoma isnot radiosensitive, adequate surgical clearance (totalthyroidectomy) is the mainstay of primary treat-ment.528, 529
Tumor stage is the single most important prog-nostic factor on multivariate analysis.453, 473, 524–527
STAGE OF DISEASE. Extrathyroidal extension isassociated with a high risk of recurrence, diseaseprogression, and worsened survival.526, 529, 530 Pres-ence of lymph node metastasis at diagnosis greatlyworsens the prognosis, with 10-year survival drop-ping from 86% to 95% (node negative) to 46% to55% (node positive).* Distant metastasis is associatedwith a poor survival.529
AGE. Older patients (�50 to 60 years) have aworse outcome.†
SEX. Some studies have shown the female sex tobe associated with a better prognosis,493, 526 but thisfactor loses prognostic significance on multivariateanalysis according to some series.524, 525
MEDULLARY CARCINOMA OF MEN 2.MEN 2. MEN2A–associated medullary carcinoma has a betterprognosis than the sporadic variety does; MEN 2B–associated medullary carcinoma is associated with aworse prognosis.455, 471, 527, 531 Nonetheless, this factoris apparently not significant after multivariate analy-sis according to one study.453
TUMOR SIZE. Small tumors less than 1 cm havean excellent Unfavorable461, 468, 474, 527, 532prognosis.outcome in microcarcinomas is virtually confined topatients who are symptomatic (such as palpable mi-crocarcinoma, diarrhea, or metastatic disease at pre-sentation).532
*References 455, 465, 493, 524, 526, 528, 530.
†References 453, 455, 465, 473, 493, 524, 526, 528.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

46 Endocrine System
BIOCHEMICAL CURE. Achievement of biochemi-cal cure predicts good survival (98% at 10 yearsversus 70% for those not achieving biochemicalcure).525, 530
HISTOLOGIC FEATURES. Features associatedwith a worse prognosis include high mitotic count(more than 1 mitotic figure per 25 high-powerfields), coagulative necrosis, absence of amyloid, andsmall cell variant474, 475, 486, 526, 527, 533 (Fig. 44–69).
IMMUNOHISTOCHEMICAL FEATURES. Calcitonin-poor medullary carcinomas fare worse than calcito-nin-rich tumors.534–536 The calcitonin content of thetumor may decrease at relapse. Strong expression ofCD15/Leu-M1 is correlated with a higher risk oflocal recurrence and tumor mortality.537, 538 Low ex-pression of chromogranin B or Bcl-2 is associatedwith a more aggressive course.539, 540
N-N-MYC EXPRESSION. Increased expression ofN-myc has been reported to be an unfavorable prog-nostic factor.541
TUMOR ANGIOGENESIS. A high microvesselcount is associated with a poorer prognosis.542
DNA PDNA PLOIDY. Aneuploid tumors behave moreaggressively than diploid ones do.493, 527, 543, 544
Collision Tumor
Collision tumors are neoplasms comprising twocomponents: medullary carcinoma and a carcinomaof follicular cell derivation (follicular carcinoma orpapillary carcinoma).545–552 The two components canbe intermingled, contiguous, or separate. Most prob-ably represent coincidental occurrence of two neo-plasms in proximity.
Mixed Follicular-ParafollicularCarcinoma
CLINICAL CONSIDERATIONSMixed follicular-parafollicular carcinoma, also knownas differentiated carcinoma of intermediate type, isan uncommon tumor of the thyroid comprisingclosely intermingled follicular and parafollicularcells. The follicular cells secrete thyroglobulin, andthe parafollicular cells secrete calcitonin or otherhormone products such as somatostatin and neuro-tensin; on occasion, both hormone products can beproduced by the same cell.553–556 The patients have amedian age of 48 years. They present with a thyroidnodule, and lymph node involvement is common(� 75%). The mean size of the tumor is 3.7 cm.556
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–68. C cell hyperplasia, nodular type, associated with MEN 2A. A. Small nodular clustersof cells are found among the follicles, sometimes obliterating their lumina. B. A corresponding fieldstained for calcitonin clearly delineates the hyperplastic C cells.
FIGURE 44–69. Medullary carcinoma showing “aggressive” his-tologic features, such as diffuse cellular atypia, coagulative necro-sis, and mitotic figures.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 47
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsMixed follicular-parafollicular carcinomas are of-
ten completely or partially encapsulated. They showsolid, nested, or cribriform growth with intermin-gled follicles553, 557–559 (Fig. 44–70). It is importantnot to mistake entrapped thyroid follicles in a con-ventional medullary carcinoma for a mixed follicu-lar-parafollicular carcinoma. Cytologic comparisonof the cells lining the follicles with those of the sur-rounding follicles is most helpful. The most defini-tive evidence of follicular differentiation is identifi-cation of follicles in metastatic deposits. Amyloid isoccasionally present. On ultrastructural examination,neurosecretory granules, follicular cells, cells withintermediate features, and indifferent cells are iden-tified.553
ImmunohistochemistryThyroglobulin immunoreactivity is characteris-
tically seen in the follicular and cribriform areasand sometimes in the solid component; calcitoninimmunoreactivity is most conspicuous in the solidareas553, 555 (Fig. 44–71). Rare cells with dual hor-mone production can be identified in some cases.
Differential DiagnosisThis tumor histologically mimics the less well
differentiated examples of follicular carcinoma or in-sular carcinoma. Immunohistochemical confirmationis therefore essential for diagnosis. However, thepossibilities of entrapped benign follicles and diffu-sion of thyroglobulin from surrounding thyroid tis-sue have to be excluded.
Molecular BiologyAlthough it has been thought that mixed follicu-
lar-parafollicular carcinoma results from an uncom-mitted stem cell capable of differentiating towardboth follicular cells and C cells, molecular studieshave failed to confirm such a hypothesis.556 Studiesof gene mutation, allelic loss, and clonal compositionon microdissected tumor tissue show that the follic-ular and parafollicular components belong to differ-ent clones.560 Furthermore, the follicular componentis often oligoclonal or polyclonal.
PROGNOSTIC CONSIDERATIONSMixed follicular-parafollicular carcinomas spread byboth the lymphatic and hematogenous routes andare more aggressive than differentiated thyroid car-cinomas. In the series of 18 patients reported byLjungberg,553 6 developed metastasis, and 4 died ofthe tumor 1 month to 15 years after surgery. Ac-cording to the review of Papotti and colleagues,556
56% of patients (N � 25) were alive with disease ordead of disease up to 10 years after diagnosis. Theresults contrast with those of otherwise typical med-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–70. Mixed follicular-parafollicular carcinoma. Itshows a solid growth interspersed with follicles.
FIGURE 44–71. Mixed follicular-parafollicular carcinoma, immunohistochemical staining. A. Thesolid component shows immunoreactivity for calcitonin. B. Thyroglobulin immunoreactivity is con-fined to the follicles.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
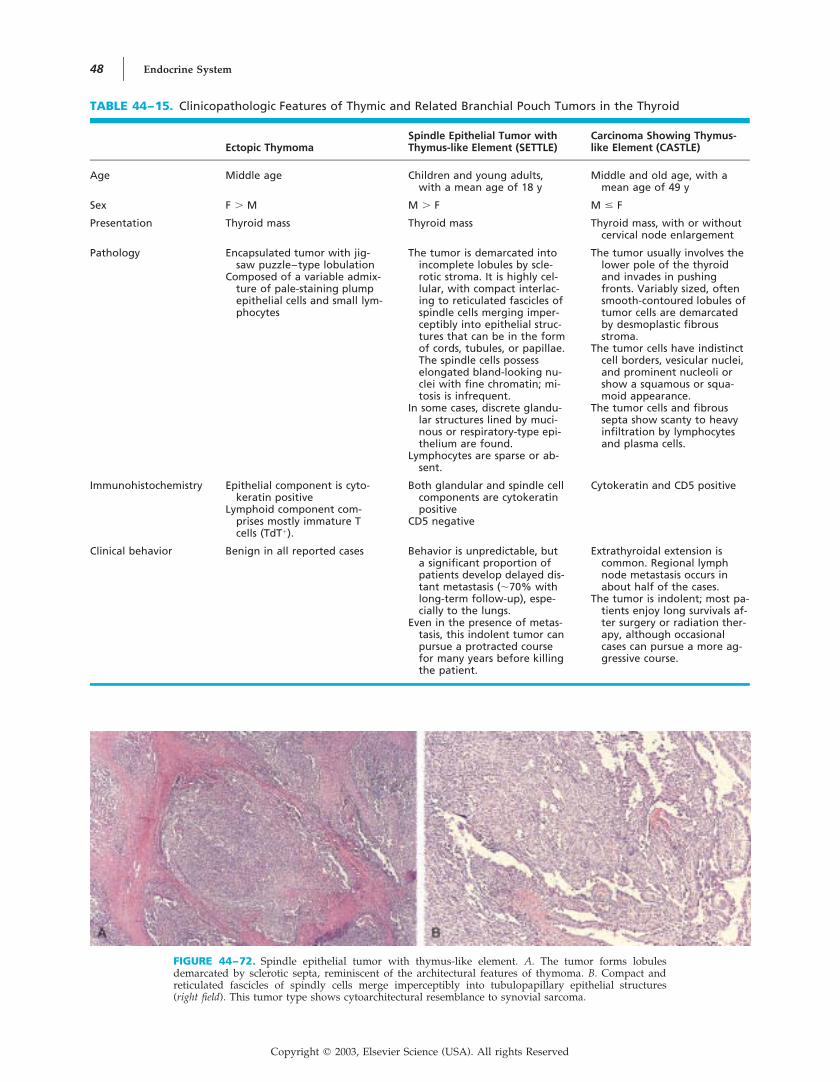
48 Endocrine System
FIGURE 44–72. Spindle epithelial tumor with thymus-like element. A. The tumor forms lobulesdemarcated by sclerotic septa, reminiscent of the architectural features of thymoma. B. Compact andreticulated fascicles of spindly cells merge imperceptibly into tubulopapillary epithelial structures(right field). This tumor type shows cytoarchitectural resemblance to synovial sarcoma.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–15. Clinicopathologic Features of Thymic and Related Branchial Pouch Tumors in the Thyroid
Ectopic ThymomaSpindle Epithelial Tumor withThymus-like Element (SETTLE)
Carcinoma Showing Thymus-like Element (CASTLE)
Age Middle age Children and young adults,with a mean age of 18 y
Middle and old age, with amean age of 49 y
Sex F � M M � F M � F
Presentation Thyroid mass Thyroid mass Thyroid mass, with or withoutcervical node enlargement
Pathology Encapsulated tumor with jig-saw puzzle–type lobulation
Composed of a variable admix-ture of pale-staining plumpepithelial cells and small lym-phocytes
The tumor is demarcated intoincomplete lobules by scle-rotic stroma. It is highly cel-lular, with compact interlac-ing to reticulated fascicles ofspindle cells merging imper-ceptibly into epithelial struc-tures that can be in the formof cords, tubules, or papillae.The spindle cells possesselongated bland-looking nu-clei with fine chromatin; mi-tosis is infrequent.
In some cases, discrete glandu-lar structures lined by muci-nous or respiratory-type epi-thelium are found.
Lymphocytes are sparse or ab-sent.
The tumor usually involves thelower pole of the thyroidand invades in pushingfronts. Variably sized, oftensmooth-contoured lobules oftumor cells are demarcatedby desmoplastic fibrousstroma.
The tumor cells have indistinctcell borders, vesicular nuclei,and prominent nucleoli orshow a squamous or squa-moid appearance.
The tumor cells and fibroussepta show scanty to heavyinfiltration by lymphocytesand plasma cells.
Immunohistochemistry Epithelial component is cyto-keratin positive
Lymphoid component com-prises mostly immature Tcells (TdT�).
Both glandular and spindle cellcomponents are cytokeratinpositive
CD5 negative
Cytokeratin and CD5 positive
Clinical behavior Benign in all reported cases Behavior is unpredictable, buta significant proportion ofpatients develop delayed dis-tant metastasis (�70% withlong-term follow-up), espe-cially to the lungs.
Even in the presence of metas-tasis, this indolent tumor canpursue a protracted coursefor many years before killingthe patient.
Extrathyroidal extension iscommon. Regional lymphnode metastasis occurs inabout half of the cases.
The tumor is indolent; most pa-tients enjoy long survivals af-ter surgery or radiation ther-apy, although occasionalcases can pursue a more ag-gressive course.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 49
ullary carcinoma shown on immunohistochemicalstaining to be thyroglobulin positive, which has aprognosis similar to or better than that of conven-tional medullary carcinoma.561
Thymic and Related BranchialPouch Tumors of the Thyroid
CLINICAL CONSIDERATIONSThe occasional presence of sequestered thymic tissueor branchial pouch remnants in the thyroid glandmay explain the occurrence of ectopic thymic tu-mors in the thyroid. These rare tumors include ec-topic thymoma, spindle epithelial tumor with thy-mus-like element (SETTLE), and carcinoma showingthymus-like element (CASTLE); their clinicopathol-ogic features are summarized in Table 44–15 (Figs.44–72 to 44–74).562–581
DIAGNOSTIC CONSIDERATIONSEctopic thymoma is histologically identical to themediastinal counterpart. For CASTLE, the morpho-logic features and expression of CD5 (a lymphocyte-associated marker commonly expressed in thymiccarcinomas but not in nonthymic carcinomas)strongly suggest that this is an intrathyroid thymiccarcinoma.582–584 The histogenesis of SETTLE cur-rently remains elusive.581
The most important reason for recognizing thisgroup of neoplasms is that they are benign to low-grade malignant and should not be mistaken forlymphoma or the vastly more aggressive anaplasticcarcinoma. Follicular dendritic cell tumor can alsopotentially be misdiagnosed as CASTLE.585
Intrathyroid Parathyroid Tumor
Because the parathyroid glands are close to or areembedded in the thyroid gland, parathyroid ade-noma or carcinoma can occur as primary thyroidtumor.586, 587 These tumors are not uncommonly mis-diagnosed as follicular adenoma, follicular carci-noma, or anaplastic carcinoma (Fig. 44–75A). A para-thyroid origin should be suspected when there areclear cells, prominent delicate vasculature, and regi-mentation of nuclei along the vascular septa. Thediagnosis can be confirmed by immunostaining forparathyroid hormone (Fig. 44–75B).
Malignant Lymphoma
CLINICAL CONSIDERATIONSPresentationPrimary lymphoma of the thyroid accounts for
approximately 5% of all thyroid cancers.588 It affectsmostly adults, and there is a female predominance(male-to-female 589–599 Hashimoto’sratio � 1 : 2.5).
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–73. Spindle epithelial tumor with thymus-like ele-ment. The spindly cells have fairly uniform nuclei and scantycytoplasm. The glandular structures (left upper field) exhibit bland-looking, pale-staining nuclei.
FIGURE 44–74. Carcinoma showing thymus-like element. A. The tumor invades the thyroid predom-inantly in the form of smooth-contoured cell islands, different from the extensive permeative growthof anaplastic carcinoma. B. The tumor island comprises squamoid cells with moderate nuclear atypia.The cytoarchitectural features are identical to those of squamous cell carcinoma of the thymus.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

50 Endocrine System
thyroiditis and lymphocytic thyroiditis are recog-nized predisposing factors.589, 593, 598
Some patients present with a rapidly enlargingthyroid mass, which may be accompanied by dys-phagia or hoarseness, simulating the presentation ofanaplastic carcinoma. Others present with gradualenlargement of the thyroid gland or a slow-growingthyroid nodule. The tumor can be confined to thethyroid or show extrathyroidal extension. Regionallymph nodes are sometimes involved.
Macroscopic FindingsThe lymphoma forms a noncircumscribed rub-
bery to soft mass in one or both lobes of the thy-roid. The cut surfaces are slightly bulging, fleshy,light tan, and often homogeneous, with or withoutnecrosis and hemorrhage. The size ranges from lessthan 1 cm to 19.5 cm.592, 600
DIAGNOSTIC CONSIDERATIONSHistologic TypesHodgkin’s lymphoma of the thyroid is ex-
tremely rare.601 Among non-Hodgkin’s lymphomas,diffuse large B cell lymphoma and extranodal mar-ginal zone B cell lymphoma of mucosa-associatedlymphoid tissue (MALT) type constitute almost allcases.589, 596, 599, 602 Exceptional examples of follicularlymphoma, intravascular lymphomatosis, and T celllymphomas have been reported.599, 603–607
Extranodal Marginal Zone B CellLymphoma of MALT TypeThe histologic features of extranodal marginal
zone B cell lymphoma involving the thyroid aresimilar to those of this lymphoma type occurringelsewhere. Within the diffuse lymphomatous infil-trate, some reactive lymphoid follicles are often in-terspersed (Fig. 44–76A). The lymphoma cells aresmall to medium sized, resembling small lympho-cytes, centrocytes, or monocytoid B cells; the cellularcomposition is often mixed. Plasma cells, often in
groups, are commonly found among the lymphomacells. Invasion of the thyroid follicles by lymphomacells results in formation of lymphoepithelial lesionsand plugging of the follicular lumina by lymphomacells589, 599, 608 (Fig. 44–77; see also Fig. 44–76B). Col-onization of the reactive lymphoid follicles can re-sult in a pattern reminiscent of follicular lymphoma(see Fig. Immunohistochemical599, 608, 60944–76C).staining shows expression of B markers; CD5, CD10,CD23, and cyclin D1 are negative.599, 607 Monotypicimmunoglobulin can be demonstrated in the plasmacells in approximately 30% of cases.608, 610
Diffuse Large B Cell Lymphoma Withor Without a Component ofExtranodal Marginal Zone B CellLymphomaDiffuse large B cell lymphoma accounts for
more than 60% of all thyroid lymphomas. In somecases, there is a component of extranodal marginalzone B cell lymphoma, suggesting transformationfrom it.590, 591, 593, 599, 611, 612 The lymphomatous growtheffaces the architecture of the thyroid tissue (Fig.44–78A). The lymphoma cells are large, with roundvesicular nuclei, distinct nucleoli, and a moderateamount of amphophilic cytoplasm that may some-times be plasmacytoid (Fig. 44–78B). Mitotic figuresand apoptotic bodies are common. Invasion of thethyroid epithelium to produce lymphoepitheliallesions is common, whereas plugging of follicu-lar lumina by lymphoma cells is much less fre-quent.590, 592, 599, 613 Vascular invasion can sometimesbe identified590, 592 (Fig. 44–78C). Immunohistochemi-cal analysis shows positive staining for leukocytecommon antigen and B markers.
Differential Diagnosis
HASHIMOTO’S THYROIDITIS. When Hashimoto’sthyroiditis shows a florid chronic inflammatory cellinfiltrate, it can be difficult to tell whether there issuperimposed extranodal marginal zone B cell lym-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–75. Intrathyroid parathyroid adenoma. A. The presence of follicle structures creates astrong mimicry of follicular neoplasm. B. The diagnosis can be readily confirmed by positive immuno-reactivity for parathyroid hormone.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 51
FIGURE 44–76. Extranodal marginal zone B cell lymphoma ofthe thyroid. A. An intense lymphoid infiltrate characterizes lym-phoma. B. The infiltrate comprises centrocyte-like cells with irreg-ular nuclei, plasma cells, and plasmacytoid cells. The lymphoidcells infiltrate into the thyroid follicles (lymphoepithelial lesions)and characteristically plug up the lumina of the follicles. C. Thepreexisting reactive lymphoid follicles are colonized by monoto-nous-appearing lymphoma cells, resulting in a resemblance tofollicular lymphoma.
FIGURE 44–77. Extranodal marginal zone B cell lymphoma of the thyroid. A. The lymphoma cellsshow prominent infiltration and expansion of the thyroid follicles to produce lymphoepithelial lesions(right field). B. Cytokeratin immunostaining of a corresponding field clearly shows follicular destruc-tion and expansion by the neoplastic infiltrate.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
phoma.608 A dense lymphoid infiltrate, broad bandsof centrocyte-like cells or clear cells, and prominentlymphoepithelial lesions are histologic featuresstrongly favoring a diagnosis of lymphoma, whichcan be further supported by immunohistochemicalstudies to demonstrate sheets of B cells, aberrantcoexpression of CD43, or light chain restriction.300
ANAPLASTIC CARCINOMA. Features favoring adiagnosis of lymphoma are lack of cellular co-hesion, plasmacytoid cytoplasm, presence of lym-phoepithelial lesions, and plugging of follicular lu-mina by tumor cells. The diagnosis can be readilyconfirmed by immunohistochemical studies (see Ta-ble 44–1).
Copyright � 2003, Elsevier Science (USA). All rights Reserved

52 Endocrine System
PROGNOSTIC CONSIDERATIONSThe 5-year survival rate for thyroid lymphoma is50% to 79%.* The most important prognostic factorsare tumor stage and histologic type.
TUMOR STAGE. Stage IIE or higher is associatedwith a much worse prognosis than is stage IE dis-ease; almost all mortalities are confined to the stageIIE and higher group.591, 592, 599 Most studies have alsoshown extrathyroidal extension to worsen the prog-nosis, with a 5-year survival of 40% compared with85% for intrathyroidal tumor.590–593, 596, 599
HISTOLOGIC TYPE. Although some studies havenot found the histologic type to correlate with prog-nosis,589, 591, 593, 594, 616 other studies have shown theprognosis of extranodal marginal zone B cell lym-phoma of MALT type to be much superior to that ofdiffuse large B cell lymphoma.590, 599, 612, 617 Accordingto the series from the Armed Forces Institute of Pa-thology, none of 30 patients with pure extranodalmarginal zone B cell lymphoma died of lymphoma,whereas 20 (26%) of 77 patients with a diffuse largeB cell lymphoma component died of the disease.599
There is no difference in outcome for diffuse large Bcell lymphoma with or without an identifiable com-
ponent of extranodal marginal zone B cell lym-phoma, similar to the findings in other mucosal sitessuch as the stomach, although conflicting results arereported by Skacel and coworkers.599, 618
AGE. Advanced age (older than 60 to 65 years)has been shown in some studies to be associatedwith a worse prognosis.590, 591
TUMOR SIZE. A large tumor (�10 cm) is re-ported to be associated with a worse prognosis ac-cording to some but not all studies.590, 596, 599
VASCULAR INVASION. Vascular invasion is as-sociated with a worse prognosis.592, 599
HISTOLOGIC FEATURES. High mitotic count andhigh apoptotic count are associated with a worseprognosis.599 Tumor necrosis is associated with aworse prognosis according to one study but not an-other.592, 599
Plasmacytoma of the Thyroid
Plasmacytoma of the thyroid is uncommon, and theprognosis is excellent592, 619 (Table 44–16). The neo-plastic infiltrate comprises a monotonous populationof mature-looking, immature-looking, pleomorphic,or plasmablastic plasma cells. It has been suggestedthat thyroid plasmacytoma may represent an ex-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–78. Diffuse large B cell lymphoma of the thyroid. A.The neoplasm is permeative and destructive. Residual follicles areevident in the left lower field. B. The noncohesive neoplastic cellsare large and possess round or irregular nuclei, distinct nucleoli,and amphophilic cytoplasm. C. The neoplastic cells commonlyinfiltrate the epithelial lining of the follicles, but they rarely ag-gregate within the central colloid material.
*References 589–591, 593, 600, 610, 611, 614, 615.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 53
treme (mature) form of extranodal marginal zoneB cell lymphoma with prominent plasmacytic differ-entiation.600, 620 The major differential diagnoses areinflammatory pseudotumor (plasma cell granu-loma)621, 622 and malignant lymphoma.
Langerhans Cell Histiocytosis(Histiocytosis X)
CLINICAL AND PROGNOSTICCONSIDERATIONSThe thyroid gland can be involved by Langerhanscell histiocytosis as the sole lesion or as part of dis-seminated disease. The patients show a wide agerange (median, 37 years), and there is no sex predi-lection.623–628 The disease presents either as an inci-dental finding in the thyroid removed for other rea-sons or at autopsy or as a large thyroid. Theprognosis is excellent for disease limited to the thy-roid but poor for patients with disseminated disease.
DIAGNOSTIC CONSIDERATIONSThe thyroid is infiltrated by Langerhans cells in apatchy or extensive pattern, and there can be extra-thyroidal extension. The Langerhans cells possessgrooved or highly contorted nuclei, thin nuclearmembrane, delicate chromatin, and moderateamount of eosinophilic cytoplasm. They can infil-trate and destroy the thyroid follicular epithelium.There are variable numbers of admixed eosinophils,sometimes with formation of eosinophil abscesses.The diagnosis should be confirmed by positive im-munostaining for S-100 protein and CD1a.
Angiosarcoma
CLINICAL AND PROGNOSTICCONSIDERATIONS
PresentationAngiosarcoma of the thyroid, also known as ma-
lignant hemangioendothelioma, is rare. It affectsmostly old patients with a slight male predomi-nance.629 The patients usually present with rapid on-set of a neck mass, which may cause difficulties inbreathing and swallowing. They may have a historyof long-standing goiter. Some patients may presentwith distant metastasis.
Angiosarcoma of the thyroid is extremely ag-gressive, and metastatic spread is common, such asto the lung, pleura, lymph node, adrenal, gastroin-testinal tract, and bone.629 The median survival isonly 3.5 months, and the rare survivors all havesmall tumors lacking extrathyroidal extension.630
Macroscopic FindingsThe tumor is usually solitary and infiltrative,
with a fleshy gray-tan appearance punctuated byareas of necrosis and hemorrhage. There can be acentral cavity filled with coagulated or fluidblood.629
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsAngiosarcomas of the thyroid are often poorly
differentiated. The tumors grow in solid sheets andirregular anastomosing channels that contain blood.The tumor cells often exhibit significant nuclearpleomorphism; some of them have cytoplasmic vac-uolation. Some cases can show epithelioid morpho-logic features, with polygonal tumor cells and abun-dant eosinophilic hyaline cytoplasm630–632 (Fig. 44–79).
ImmunohistochemistryA diagnosis of angiosarcoma has to be substanti-
ated by positive immunohistochemical staining for
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–16. Comparison Between Plasmacytoma and Malignant Lymphoma of Thyroid
Plasmacytoma Malignant Lymphoma
Sex Slight male predominance (male-female 1.4 : 1) Female predominance (male-female 1 : 2.5)Age (mean) 58 y 62 yPresentation Usually slowly growing thyroid mass Rapidly or slowly growing thyroid mass5-year survival More favorable: 85% Less favorable: overall �60%, but much more favorable for
extranodal marginal zone B cell lymphoma of MALT type
FIGURE 44–79. Epithelioid angiosarcoma. Cords and islands ofpolygonal cells with voluminous hyaline cytoplasm show cyto-plasmic vacuoles and occasional irregular narrow vascular chan-nels.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

54 Endocrine System
endothelial markers, such as factor VIII–related anti-gen, CD31, and CD34.397, 398 Some cases can exhibitimmunoreactivity for cytokeratin.631
Differential DiagnosisBecause anaplastic carcinoma can exhibit angio-
sarcoma-like morphologic features focally (angioma-toid carcinoma), distinction between anaplastic carci-noma and pure angiosarcoma can be difficult.633–635
The distinction is not too important from a clini-cal point of view, however, because both arehighly aggressive neoplasms with similar survivalfigures.
Fine-needle aspiration changes such as reactivevascular proliferation or pseudoangiosarcomatouschange in the damaged thyroid follicular epitheliumcan mimic angiosarcoma.
Sclerosing mucoepidermoid carcinoma with eo-sinophilia can exhibit a pseudoangiomatous pattern,focally mimicking angiosarcoma.
Solitary Fibrous Tumor
Solitary fibrous tumor can rarely occur as a primarythyroid tumor.636–639 All patients have remained wellafter surgical excision.
The histologic features are identical to those ofthe pleural counterpart. The tumor is well circum-scribed, although some thyroid follicles can be en-trapped in the periphery. It shows alternating hy-percellular and hypocellular areas, with haphazardlydistributed bland-looking spindly or stellate cells in-timately intermingled with delicate to thick collagenfibers (Fig. 44–80). A pericytomatous vascular pat-tern is common. The tumor cells are immunoreactivefor CD34 but are negative for cytokeratin and S-100protein.
Other Mesenchymal Tumors
Smooth muscle tumors of the thyroid gland are rare,and most are malignant.640 Leiomyomas are encap-sulated and confined to the thyroid gland, with nocellular atypia, necrosis, or mitotic activity. Leiomyo-sarcomas often affect older patients and are oftenlarger. On histologic examination, they exhibit cellu-lar pleomorphism, mitotic activity, necrosis, hemor-rhage, invasive growth, and extrathyroidal exten-sion. The diagnosis has to be confirmed byimmunohistochemical or ultrastructural studies, es-pecially for distinction from anaplastic carcinoma.These tumors are aggressive; most patients diewithin 2 years. Metastases to the lungs and othersites develop early in the course of disease.640–645
Rare mesenchymal tumors reported to occur inthe thyroid include hemangioma, lymphangioma,peripheral nerve sheath tumors, fibrosarcoma, lipo-sarcoma, chondrosarcoma, osteosarcoma, and follic-ular dendritic cell sarcoma.624, 646–654
Paraganglioma
CLINICAL CONSIDERATIONSRarely, paragangliomas can occur within the thyroidgland, probably from the inferior laryngeal paragan-glia. There is a female predominance, and most pa-tients are aged between 40 and 60 years.262, 655 Thepatients present with a neck mass. The tumors arecircumscribed or can extend into the adjacent larynxor trachea. All patients have remained well aftersurgical excision.
DIAGNOSTIC CONSIDERATIONSThe tumors usually have a size of approximately 2cm.262, 656 Alveolar packets of ovoid cells with finelygranular cytoplasm are surrounded by an inconspic-uous layer of sustentacular cells (Fig. 44–81; see Ta-ble 44–1). The stroma is typically richly vascular-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–80. Solitary fibrous tumor. Nondescript spindly cellswith scanty cytoplasm and in close interaction with delicate colla-gen fibrils characterize solitary fibrous tumor. Some entrappedfollicles are seen in the peripheral portion of the tumor.
FIGURE 44–81. Paraganglioma. Oval islands of tumor are sepa-rated by a richly vascularized stroma. This tumor can potentiallybe mistaken for medullary carcinoma.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 55
ized. Tumors with enlarged, hyperchromatic, orbizarre nuclei can potentially be misdiagnosed as amalignant neoplasm. Other major differential diag-noses are medullary carcinoma and hyalinizing tra-becular adenoma.
Teratoma
CLINICAL AND PROGNOSTICCONSIDERATIONSThere are two distinct age peaks for the occurrenceof thyroid teratomas. The first and higher peak is inthe newborn period to the age of 2 years; the secondsmaller peak is in older children and adults, mostlybetween the ages of 20 and 50 years.600, 657–662 Thesetumors are more common in females than in males.Most patients present with a large thyroid or neckmass, which may be accompanied by respiratorydifficulties.
Thyroid teratomas occurring before the age of 2years usually pursue a benign course after surgicalexcision, although some patients may die of respira-tory obstruction. Thyroid teratomas occurring inadults are more likely to be malignant, with localrecurrence, cervical lymph node metastasis, and pul-monary metastasis. Nonetheless, long-term survivalis possible with aggressive treatment includingchemotherapy and surgery.600, 663, 664
thyroid, but it can be recognized by the presence ofmultiple tumor nodules, distinct cell membranes,water-clear cytoplasm, sinusoidal vascular pattern,fresh hemorrhage in the glandular lumina, and neg-ative immunostaining for thyroglobulin.31
Contents of the Final SurgicalPathology Report
In the surgical pathology report of thyroid excisionspecimens for tumors, it is important to include allinformation relevant for staging and prognosticationin addition to the diagnosis15, 45, 46 (Table 44–17).
NON-NEOPLASTIC LESIONS
Incidental and InsignificantFindings in the Thyroid Gland
Skeletal muscle fibers may be intermingled with thethyroid follicles in the region beneath the thyroidcapsule. Adipose cells and hyaline cartilage rest areoccasionally found incidentally in the thyroidgland.670 Ectopic parathyroid tissue, ectopic thymictissue, and ectopic salivary gland tissue can alsosometimes be found within the thyroid.
Rarely, there can be columnar ciliated epithe-lium replacing part of the follicular epithelium.670
The thyroid follicular epithelium can also undergosquamous metaplasia or oncocytic metaplasia.671
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
DIAGNOSTIC CONSIDERATIONSThe teratomas are most often immature, althoughsome may be of the mature type. Tissues from thevarious germ layers are present, and neuroectoder-mal tissue may be prominent. The presence of neu-ral tissue provides a strong point against the differ-ential diagnosis of anaplastic carcinoma.
Tumors occurring in neonates and infants areoften immature (grade 1 or 2), but they are some-times mature. Those occurring in adults most oftenshow grade 3 immaturity (“malignant”).600
Metastatic Malignant Neoplasmsin Thyroid
Because the thyroid gland is rich in blood vesselsand lymphatics, it is not infrequently involved bymetastatic cancer in patients with carcinomatosis,most commonly due to pulmonary carcinoma (usu-ally adenocarcinoma), breast carcinoma, malignantmelanoma, and renal cell carcinoma.665–669 The meta-static deposits are often small and asymptomaticand are associated with obvious widespread meta-static tumor elsewhere.665
Renal cell carcinoma can metastasize to the thy-roid gland as the initial manifestation of the tumoror as the first evidence of relapse many years afterresection of the renal primary.31, 665 It can potentiallybe misdiagnosed as primary clear cell tumor of the
✒ TABLE 44–17. Contents of the Final Report:Thyroid Excision Specimens
Specimen type/operation procedure
DiagnosisHistologic type, and variant if applicableHistologic grade, if relevant
Other tumor featuresTumor location (right lobe, left lobe, isthmus)Tumor sizeSolitary or multicentricEncapsulated or nonencapsulatedCapsular invasion (absent, present, extensive)Vascular invasion (absent, present, extensive)Extrathyroidal extension (structures invaded, if applicable)Mitotic activity
Surgical margins: free, close to surgical margin (specify dis-tance), or margin involved (specify site)
Non-neoplastic thyroid: normal, nodular goiter, lymphocyticthyroiditis, Hashimoto’s thyroiditis, atrophy, fibrosis
Lymph nodesNumber of lymph nodes found, and their location (level)Number of involved lymph nodesSize of largest metastatic depositPresence or absence of extracapsular extension
Copyright � 2003, Elsevier Science (USA). All rights Reserved

56 Endocrine System
Crystals are commonly found in the colloid ofthe thyroid follicles. They are most commonly seenin nodular goiters, but they can be seen in variousnon-neoplastic and neoplastic lesions of the thyroid.The crystals vary in geometric shapes and are mostoften composed of calcium oxalate.672–674
Solid cell nests, common incidental findings inthe thyroid, are often detected at low-magnificationscanning as a blue-staining cellular 671, 675–679focus.They appear as a small collection of solid epithelialislands resembling transitional epithelium (Fig.44–82). Some islands can show cystic change andcontain mucinous substance. The epithelial cells pos-sess oval grooved nuclei. The solid cell nests arebelieved to be remnants of ultimobranchial bodies,and many scattered C cells are associated with thesenests.508, 677
Palpation granuloma (palpation thyroiditis) is acommon incidental finding of no consequence and isbelieved to result from the mechanical trauma ofpalpation.680 One or two thyroid follicles appear tohave ruptured and are replaced by histiocytes andmultinucleated histiocytes. They are not associatedwith fibrous scarring.
Cysts
The most common cyst of the thyroid gland is de-generate cyst resulting from cystic degeneration ofnodular goiter. Cystic degeneration can also occur invarious thyroid tumors, such as follicular adenoma.The cystic variant of papillary carcinoma is charac-terized by the presence of a prominent cystic com-ponent lined by neoplastic cells.
Thyroglossal duct cyst represents cystic dilata-tion of the persistent thyroglossal duct. The patientusually present in the first 3 decades of life with aswelling in the midline of the neck that typicallymoves upward with swallowing. The cyst is usually
situated below the hyoid bone but above the thyroidisthmus. When it is complicated by infection, therecan be tenderness and pain. Histologic examinationshows the cyst to be lined by respiratory or strati-fied squamous epithelium. The wall consists of fi-brous tissue, which may be infiltrated by chronicinflammatory cells. Mucous glands can be present inthe wall. Some thyroid follicles are often but notinvariably identified in the vicinity. Rarely, carcino-mas can develop in a thyroglossal duct cyst. Papil-lary carcinoma is the most common histologic type,but squamous cell carcinoma can also rarely occurin this setting.681–683
Multiple branchial cleft– like cysts are rarelyfound in association with Hashimoto’s thyroiditis.The cysts are lined by squamous or respiratory epi-thelium and are surrounded by a band of denselymphoid infiltrate.684 Postulated pathogenetic mech-anisms include metaplastic and cystic change of thethyroid follicles in the setting of thyroiditis andorigin from developmental rests.684, 685
Thyroid Tissue in the Lateral Neck
LATERAL ABERRANT THYROIDThyroid tissue occurring in the lateral neck separatefrom the thyroid gland has often been referred to aslateral aberrant thyroid. This can occur in severalcircumstances46: 1) sequestered nodule in nodulargoiter; the nodule may still be connected by a nar-row strand of tissue to the main gland; 2) regrowthof thyroid tissue that has been implanted in the softtissues of the neck from prior surgery; and 3) se-questered thyroid tissue involved by Hashimoto’sthyroiditis or Graves’ disease. It is most important,however, to rule out the possibility of metastaticthyroid carcinoma (most commonly papillary carci-noma) in cervical lymph nodes.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–82. Solid cell nest of the thyroid. A. Small, blue-staining islands of epithelium aredisposed in a stellate configuration among the thyroid follicles. Occasional epithelial islands show cystformation with secretion. B. The epithelial cells resemble transitional epithelium, and nuclear groovesare common.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 57
THYROID INCLUSIONS IN CERVICALLYMPH NODEBenign thyroid follicles can rarely occur in cervicallymph nodes. Nonetheless, this belief is not univer-sally accepted; some investigators consider all thy-roid tissues within lymph nodes to represent metas-tasis from clinically undetected thyroid carcinoma.686
Because the distinction between benign thyroid in-clusions and metastasis from an occult thyroid carci-noma can be extremely difficult owing to the almostnormal histologic appearances of some thyroid carci-nomas, strict criteria must be used in the diagnosisof benign thyroid inclusions46, 687, 688:
• They consist of only a small conglomerate of thy-roid follicles.
• They are limited to the periphery of one or twolymph nodes.
• Nuclear features of papillary carcinoma are lack-ing, that is, nuclei are not enlarged, with fine chro-matin and inconspicuous nucleoli.
• Psammoma bodies are absent.• There is lack of a desmoplastic reaction.
METASTATIC THYROID CARCINOMA INCERVICAL LYMPH NODEPapillary carcinoma commonly metastasizes tolymph nodes, whereas follicular carcinoma rarelydoes. Cervical lymph node metastasis is sometimes
the first clinical manifestation of an occult papillarythyroid carcinoma—the thyroid primary is almostalways located on the ipsilateral side. The node canbe cystic or show sudden enlargement because ofhemorrhage. On histologic examination, a diagnosisof metastatic papillary thyroid carcinoma can be ob-vious because of presence of recognizable lymphnode tissue and papillary carcinoma. However, insome cases, the cyst wall is formed by dense fibroustissue with scanty lymphoid tissue underneath andlined by attenuated nondescript cells, and thus itmay be mistaken for a branchial cyst (Fig. 44–83).Careful search may be required to uncover smallpapillae projecting into the lumen or some elongatedfollicles in the wall, with the cells exhibiting thetypical nuclear features of papillary carcinoma (Fig.44–83B, C). A diagnosis can be readily confirmed bypositive immunostaining for thyroglobulin.
MIMICKER OF METASTATIC THYROIDCARCINOMA IN CERVICAL LYMPH NODEA sequestered thyroid nodule involved by floridHashimoto’s thyroiditis can potentially be mistakenfor metastatic thyroid carcinoma in lymph node be-cause the lymphoplasmacytic infiltrate with germi-nal center formation imparts a lymph node–like ap-pearance and the thyroid follicles can exhibit nuclearatypia or pallor. However, subcapsular sinuses, ahallmark of lymph node, are lacking.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–83. Cystic metastasis of papillary thyroid carcinomain lymph node. A. This cyst excised from the lateral neck can bemistaken for a developmental cyst because of its innocuous ap-pearance. The wall is formed by fibrous tissue with only focallining by attenuated epithelium. B. In areas, more plump andslightly pseudostratified epithelial cells are seen lining the cyst. C.On careful search, a small focus with papillary structures isfound, clinching the diagnosis of metastatic papillary carcinoma.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

58 Endocrine System
Thyroiditis
ACUTE THYROIDITISAcute thyroiditis is rare. It is caused by bacterialinfection, such as Staphylococcus, Streptococcus pyoge-nes, and Haemophilus influenzae. The patients are of-ten immunosuppressed, or there is a regional infec-tive focus, such as piriform sinus fistula. Theypresent with painful swelling of the thyroid andfever. Histologic examination shows polymorph in-filtration associated with destruction of the thyroidfollicles.
INFECTIOUS GRANULOMATOUSTHYROIDITISGranulomatous inflammation can be produced inthe thyroid by some infective processes, such as tu-
berculosis, actinomycosis, and fungal infection. Thepatients are often immunocompromised. Granulo-mas with or without caseation are found in the thy-roid, although they can be poorly formed in im-munocompromised hosts. The main differentialdiagnoses are sarcoidosis and de Quervain’s thy-roiditis.
DE QUERVAIN’S THYROIDITIS (SUBACUTEGRANULOMATOUS THYROIDITIS)de Quervain’s thyroiditis is thought to be caused byviral infection, although no specific virus has beenincriminated. The main features are summarized inTable 44–18.689, 690 In contrast to the randomly dis-tributed granulomas in infectious granulomatousthyroiditis, the granulomas in de Quervain’s thy-roiditis are centered around residual colloid (Fig.44–84).
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–18. Major Types of Thyroiditis
Hashimotos’ Thyroiditis de Quervain’s Thyroiditis Riedel’s Thyroiditis
Nature of diseaseprocess
Autoimmune thyroiditis, with au-toantibodies against thyro-globulin, thyroid peroxidase,thyrotropin receptor, and io-dine transporter, as well ascell-mediated immunityagainst thyroid tissue compo-nents
A subacute thyroiditisPossibly related to viral infection
or postviral inflammatory pro-cess
An inflammatory fibrosclerosinglesion
A small proportion of patientssubsequently develop inflam-matory fibrosclerosis of othersites, e.g., retroperitoneal fi-brosis, mediastinal fibrosis, or-bital pseudotumor, sclerosingcholangitis
Age Most commonly 45–65 y Most commonly 30–50 y Broad age range, with a meanof 48 y
Sex F �� M (15 : 1) F � M (4 : 1) F � M (5 : 1)
Presentation Painless thyroid swellingSome may have evidence of hy-
pothyroidism, whereas somemay have transient hyperthy-roidism
Sudden or gradual onset of painin the neck
May have transient hyperthyroid-ism
Can be accompanied by feverand systemic symptoms
May have a history of precedingupper respiratory infection
Recent enlargement of thyroidgland, which may be accompa-nied by pressure symptoms,e.g, dyspnea, dysphagia
Most patients are euthyroid, butsome can be hypothyroid
Pattern of in-volvement ofthe thyroidgland
Diffuse, with involvement ofboth lobes
No extrathyroidal extension
Unilateral or bilateral involve-ment
Usually a patchy process (1 cm toseveral centimeters in diame-ter), but there is no extrathy-roidal extension
Focal involvement of thyroid, as-sociated with extrathyroidalextension
Antithyroid anti-bodies in se-rum
Always Usually negative Approximatelly two thirds of pa-tients
Major histologicfeatures
Lymphoplasmacytic infiltrationFollicular infiltration and destruc-
tion by lymphocytesWidespread oncocytic change in
thyroid epithelium
Disrupted folliclesHistiocytes and multinucleated
giant cells around pools of re-sidual colloid
Lymphocytic infiltrationPatchy fibrosis
Invasive process, and may entrapskeletal muscle fibers
Focal replacement of thyroid pa-renchyma by hypocellular fi-brous tissue
Patchy chronic inflammationwith or without lymphoid folli-cle formation
Phlebitis
Clinical outcome Gradual loss of thyroid function,i.e., hypothyroidism
May have transient hyperthyroid-ism
Disease usually resolves in a fewmonths
Disease appears to be self-lim-ited
Prognosis after subtotal removalof the fibrotic mass is excellent
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 59
HASHIMOTO’S THYROIDITISClinical ConsiderationsHashimoto’s thyroiditis, also known as struma
lymphomatosa, is the prototype of autoimmune thy-roiditis. The salient clinical features are summarizedin Table 44–18.689–691 There is an increased risk fordevelopment of malignant lymphoma and papillarycarcinoma.
The thyroid is usually symmetrically enlarged,with a firm or rubbery consistency. The cut surfaceis tan or tan-brown, with a homogeneous or vaguelylobulated appearance.
Diagnostic ConsiderationsOn histologic examination, there is heavy infil-
tration of the interstitium and some thyroid folliclesby lymphocytes and plasma cells. Reactive lymphoidfollicles are often present. There is loss of thyroid
follicles, and the remaining ones are often small. Thethyroid follicular epithelium shows extensive onco-cytic (Hurthle cell) change and can have enlarged orpale nuclei (Fig. 44–85). Those examples with heavylymphoplasmacytic infiltration can be difficult todistinguish from extranodal marginal zone B celllymphoma or plasmacytoma arising in Hashimoto’sthyroiditis; see the relevant sections for distinguish-ing features.
Nodular Hashimoto’s thyroiditis refers to thepresence of superimposed nodules comprisingclosely packed small follicles or trabeculae, most ofwhich are lined by Hurthle cells (Fig. 44–86). Themultiplicity of nodules and the frequent presence ofisolated pleomorphic nuclei can potentially lead toan erroneous diagnosis of Hurthle cell carcinoma.Vascular invasion is absent, however.
The fibrosing variant accounts for 12.5% of allcases of Hashimoto’s thyroiditis. It is defined by thepresence of broad bands of dense hyaline fibrous tis-sue occupying more than one third of the thyroidgland, separating islands of thyroid parenchyma ex-hibiting typical histologic features of Hashimoto’sthyroiditis (oxyphilic change, follicular cell damage,and lymphoid infiltration)692 (Fig. 44–87). Squamousmetaplasia in the thyroid follicles is common. Clini-cally, the thyroid gland feels firm or hard, and pres-sure symptoms can be present. The antithyroid anti-body titers are often high. Clinical evidence ofhypothyroidism is present in approximately 50% ofcases.
LYMPHOCYTIC THYROIDITIS ANDPAINLESS THYROIDITISThe term lymphocytic thyroiditis is often appliedwhen there is diffuse or multifocal lymphoplas-macytic infiltration in the absence of oncocyticchange in the thyroid follicular epithelium. There isno significant atrophy of the thyroid follicles. How-ever, during the active phase, there can be folliculardestruction and hyperplastic change in the follicles.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–84. de Quervain’s thyroiditis. The thyroid shows in-filtration by chronic inflammatory cells and mild fibrosis. Themost characteristic feature is the presence of foreign body–typegiant cells engulfing colloid material, indicating that there hasbeen destruction of follicles.
FIGURE 44–85. Hashimoto’s thyroiditis. A. There is frequently an accentuated lobulated architecture.Lymphoid infiltration with lymphoid follicle formation is evident. The pink appearance in areas notinfiltrated by lymphoid cells results from oncocytic change in the follicular epithelium. B. The folliclesare typically small and lined by oncocytic (Hurthle) cells. There are many intermingled lymphocytesand plasma cells.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

60 Endocrine System
The disease is believed to have an autoimmunebasis.
The clinical counterpart is variously known aspainless thyroiditis, silent thyroiditis, juvenile thy-roiditis, or postpartum thyroiditis, depending on theclinical scenario.693–698 In most patients, there is tran-sient hyperthyroidism followed by hypothyroidismand spontaneous evolution. Some patients presentwith thyroid swelling. The entire clinical course usu-ally lasts less than 1 year. Only rarely do the pa-tients eventually become hypothyroid.
RIEDEL’S THYROIDITISThe main features of Riedel’s thyroiditis are summa-rized in Table 44–18 (Fig. 44–88).689, 699–701 The clini-cal impression is usually that of thyroid cancer be-cause of the presence of a stony hard thyroid mass.Riedel’s thyroiditis is rare; for unknown reasons, itsincidence has decreased dramatically during the
past few decades.701 Although steroid treatment maysometimes be effective, surgical excision is usuallyrequired to relieve the pressure symptoms and toexclude malignancy.
The most important differential diagnosis ispaucicellular variant of anaplastic carcinoma becauseof marked differences in outcome (see “AnaplasticCarcinoma”).381 Riedel’s thyroiditis can also be dis-tinguished from fibrosing Hashimoto’s thyroiditis bythe features of extrathyroidal extension of the fibro-proliferative process, presence of phlebitis, and rela-tively normal surviving thyroid tissue.700
FOCAL LYMPHOCYTIC THYROIDITIS(NONSPECIFIC LYMPHOCYTIC THYROIDITIS)Focal lymphoid infiltration in the thyroid gland is afairly common incidental finding in thyroidectomyspecimens and at autopsy.702–705 This is also a com-mon finding in the vicinity of various thyroid tu-mors, especially papillary carcinoma. The lymphoidcells tend to be localized to the interlobular areas,with little evidence of destruction of thyroid folli-cles. The pathogenesis is unknown, but the lesion isprobably of no consequence.
MULTIFOCAL FIBROSING THYROIDITISMultifocal fibrosing thyroiditis is a peculiar form ofthyroiditis characterized by many microscopic fociof stellate cellular fibrosis with some entrapped thy-roid follicles, mimicking the low-magnification archi-tecture of papillary microcarcinoma.45 The pathogen-esis is not known.
Graves’ Disease
CLINICAL CONSIDERATIONSGraves’ disease is the most common cause of hyper-thyroidism. It is an organ-specific autoimmune dis-ease produced by thyroid-stimulating antibodies—
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–86. Nodular Hashimoto’s thyroiditis. In the back-ground Hashimoto’s thyroiditis, variably sized nodules composedof follicles lined by Hurthle cells are present. These nodules con-tain few lymphoplasmacytic cells.
FIGURE 44–87. Fibrosing Hashimoto’s thyroiditis. Broad fibrousbands traverse the thyroid gland involved by Hashimoto’s thy-roiditis. In contrast to Riedel’s thyroiditis, the process does notextend beyond the thyroid capsule.
FIGURE 44–88. Riedel’s thyroiditis. The fibroproliferative pro-cess replaces the thyroid parenchyma and extends into the sur-rounding tissue. In addition to a sprinkling of chronic inflamma-tory cells, small aggregates of lymphocytes are present.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
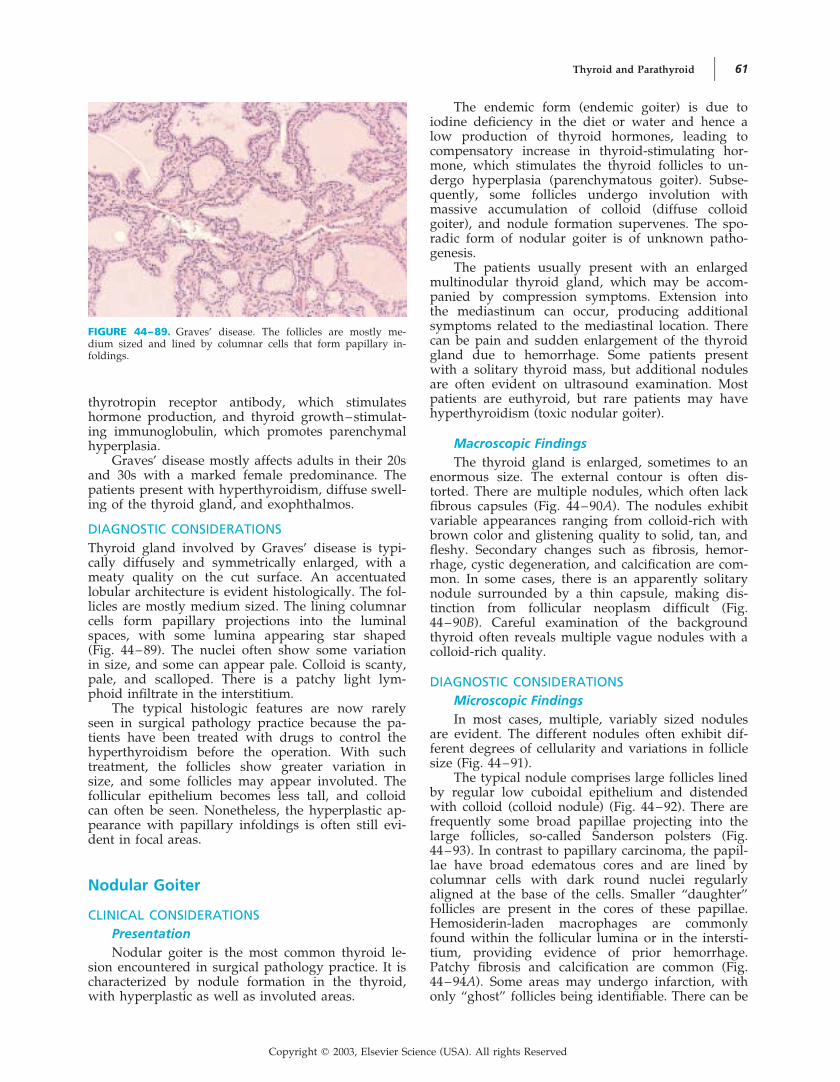
Thyroid and Parathyroid 61
thyrotropin receptor antibody, which stimulateshormone production, and thyroid growth–stimulat-ing immunoglobulin, which promotes parenchymalhyperplasia.
Graves’ disease mostly affects adults in their 20sand 30s with a marked female predominance. Thepatients present with hyperthyroidism, diffuse swell-ing of the thyroid gland, and exophthalmos.
DIAGNOSTIC CONSIDERATIONSThyroid gland involved by Graves’ disease is typi-cally diffusely and symmetrically enlarged, with ameaty quality on the cut surface. An accentuatedlobular architecture is evident histologically. The fol-licles are mostly medium sized. The lining columnarcells form papillary projections into the luminalspaces, with some lumina appearing star shaped(Fig. 44–89). The nuclei often show some variationin size, and some can appear pale. Colloid is scanty,pale, and scalloped. There is a patchy light lym-phoid infiltrate in the interstitium.
The typical histologic features are now rarelyseen in surgical pathology practice because the pa-tients have been treated with drugs to control thehyperthyroidism before the operation. With suchtreatment, the follicles show greater variation insize, and some follicles may appear involuted. Thefollicular epithelium becomes less tall, and colloidcan often be seen. Nonetheless, the hyperplastic ap-pearance with papillary infoldings is often still evi-dent in focal areas.
The endemic form (endemic goiter) is due toiodine deficiency in the diet or water and hence alow production of thyroid hormones, leading tocompensatory increase in thyroid-stimulating hor-mone, which stimulates the thyroid follicles to un-dergo hyperplasia (parenchymatous goiter). Subse-quently, some follicles undergo involution withmassive accumulation of colloid (diffuse colloidgoiter), and nodule formation supervenes. The spo-radic form of nodular goiter is of unknown patho-genesis.
The patients usually present with an enlargedmultinodular thyroid gland, which may be accom-panied by compression symptoms. Extension intothe mediastinum can occur, producing additionalsymptoms related to the mediastinal location. Therecan be pain and sudden enlargement of the thyroidgland due to hemorrhage. Some patients presentwith a solitary thyroid mass, but additional nodulesare often evident on ultrasound examination. Mostpatients are euthyroid, but rare patients may havehyperthyroidism (toxic nodular goiter).
Macroscopic FindingsThe thyroid gland is enlarged, sometimes to an
enormous size. The external contour is often dis-torted. There are multiple nodules, which often lackfibrous capsules (Fig. 44–90A). The nodules exhibitvariable appearances ranging from colloid-rich withbrown color and glistening quality to solid, tan, andfleshy. Secondary changes such as fibrosis, hemor-rhage, cystic degeneration, and calcification are com-mon. In some cases, there is an apparently solitarynodule surrounded by a thin capsule, making dis-tinction from follicular neoplasm difficult (Fig.44–90B). Careful examination of the backgroundthyroid often reveals multiple vague nodules with acolloid-rich quality.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsIn most cases, multiple, variably sized nodules
are evident. The different nodules often exhibit dif-ferent degrees of cellularity and variations in folliclesize (Fig. 44–91).
The typical nodule comprises large follicles linedby regular low cuboidal epithelium and distendedwith colloid (colloid nodule) (Fig. 44–92). There arefrequently some broad papillae projecting into thelarge follicles, so-called Sanderson polsters (Fig.44–93). In contrast to papillary carcinoma, the papil-lae have broad edematous cores and are lined bycolumnar cells with dark round nuclei regularlyaligned at the base of the cells. Smaller “daughter”follicles are present in the cores of these papillae.Hemosiderin-laden macrophages are commonlyfound within the follicular lumina or in the intersti-tium, providing evidence of prior hemorrhage.Patchy fibrosis and calcification are common (Fig.44–94A). Some areas may undergo infarction, withonly “ghost” follicles being identifiable. There can be
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–89. Graves’ disease. The follicles are mostly me-dium sized and lined by columnar cells that form papillary in-foldings.
Nodular Goiter
CLINICAL CONSIDERATIONSPresentationNodular goiter is the most common thyroid le-
sion encountered in surgical pathology practice. It ischaracterized by nodule formation in the thyroid,with hyperplastic as well as involuted areas.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

62 Endocrine System
interspersed cysts comprising a fibrous wall withor without lining by attenuated epithelium (Fig.44–94B). The lining epithelium and entrapped folli-cles in the fibrous wall may show reactive atypia orsquamous metaplasia. In some cysts, collections ofresidual large follicles project into the cyst lumen.
Some nodules can be highly cellular, being com-posed of small follicles and trabeculae (Fig. 44–95;see also Fig. 44–92C). The nuclei of the thyroid epi-thelial cells appear uniform or atypical. Oncocytic,clear cell, and signet ring change can occur. Therecan also be areas resembling hyalinizing trabecularadenoma.57 These cellular nodules (adenomatoidnodules) can be difficult to distinguish from follicu-lar neoplasm or even insular carcinoma. When thefollicles exhibit large pale nuclei, the additional dif-ferential diagnosis of papillary carcinoma may beraised; these follicles show gradual transition withthe normal or benign follicles, and they lack thesharp demarcation from the non-neoplastic folliclesas seen in papillary carcinoma.
Differential Diagnosis
FOLLICULAR ADENOMA. The distinction be-tween nodular goiter presenting as a solitary noduleand follicular adenoma can be difficult and some-times arbitrary. The distinction is not critical, how-ever, as long as there is no capsular or vascularinvasion. In general, an adenoma is solitary, is com-pletely enveloped by a fibrous capsule, is expansileand produces a compression effect on the surround-ing tissues, and shows cytoarchitectural features dis-similar from the surrounding parenchyma.
FOLLICULAR CARCINOMA. See earlier.
PAPILLARY CARCINOMA. See earlier
INSULAR CARCINOMA. See earlier.
DYSHORMONOGENESIS. For young patients notliving in areas of endemic goiter and presentingwith large multinodular goiter, the possibility ofdyshormonogenesis should be entertained.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–90. Nodular goiter. A. In this case, multiple nodules with a glistening colloid (gelati-nous) quality are evident. B. In this case, the nodule is apparently solitary and enveloped by a thincapsule. It has a variegated appearance with colloidlike areas, small cysts, hemorrhagic areas, fibrosis,and calcification.
FIGURE 44–91. Nodular goiter. Multiple nodules with variable cellularities and follicle sizes areseen. A. In this case, most follicles are large. B. In this case, there are large as well as small follicles.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
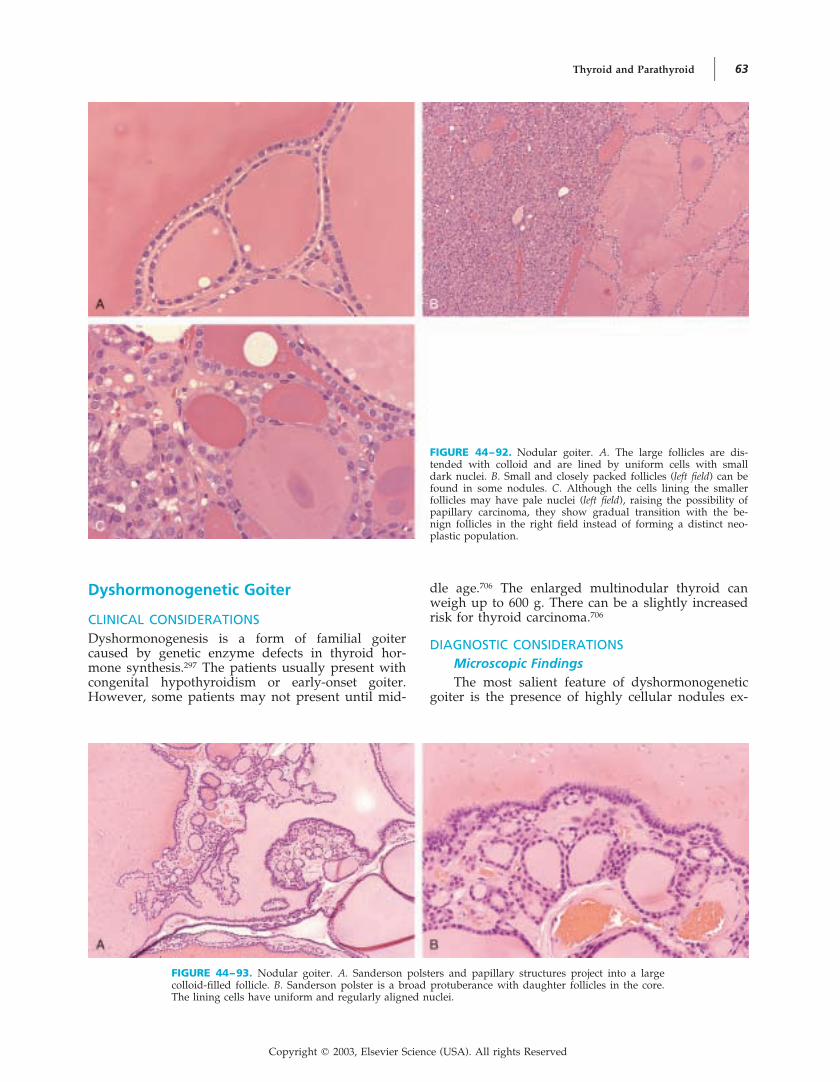
Thyroid and Parathyroid 63
Dyshormonogenetic Goiter
CLINICAL CONSIDERATIONSDyshormonogenesis is a form of familial goitercaused by genetic enzyme defects in thyroid hor-mone synthesis.297 The patients usually present withcongenital hypothyroidism or early-onset goiter.However, some patients may not present until mid-
dle age.706 The enlarged multinodular thyroid canweigh up to 600 g. There can be a slightly increasedrisk for thyroid carcinoma.706
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsThe most salient feature of dyshormonogenetic
goiter is the presence of highly cellular nodules ex-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–92. Nodular goiter. A. The large follicles are dis-tended with colloid and are lined by uniform cells with smalldark nuclei. B. Small and closely packed follicles (left field) can befound in some nodules. C. Although the cells lining the smallerfollicles may have pale nuclei (left field), raising the possibility ofpapillary carcinoma, they show gradual transition with the be-nign follicles in the right field instead of forming a distinct neo-plastic population.
FIGURE 44–93. Nodular goiter. A. Sanderson polsters and papillary structures project into a largecolloid-filled follicle. B. Sanderson polster is a broad protuberance with daughter follicles in the core.The lining cells have uniform and regularly aligned nuclei.
Copyright � 2003, Elsevier Science (USA). All rights Reserved
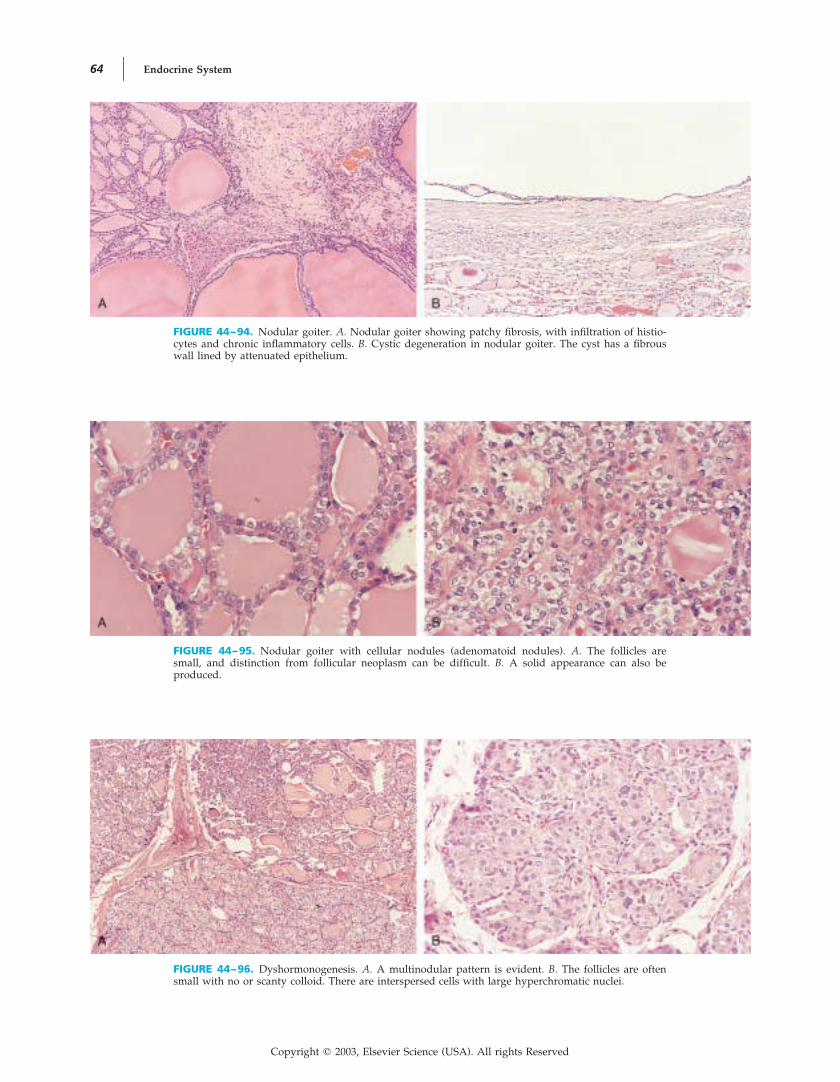
64 Endocrine System
FIGURE 44–95. Nodular goiter with cellular nodules (adenomatoid nodules). A. The follicles aresmall, and distinction from follicular neoplasm can be difficult. B. A solid appearance can also beproduced.
FIGURE 44–96. Dyshormonogenesis. A. A multinodular pattern is evident. B. The follicles are oftensmall with no or scanty colloid. There are interspersed cells with large hyperchromatic nuclei.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–94. Nodular goiter. A. Nodular goiter showing patchy fibrosis, with infiltration of histio-cytes and chronic inflammatory cells. B. Cystic degeneration in nodular goiter. The cyst has a fibrouswall lined by attenuated epithelium.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 65
hibiting a variety of architectural features (Fig.44–96A). The nodules can show a microfollicular,trabecular, solid, papillary, insular, or mixed growthpattern. Follicles, when present, are small and fre-quently devoid of colloid. There are commonly in-terspersed cells with large hyperchromatic nuclei orvesicular nuclei. Cells with hyperchromatic pleomor-phic nuclei are most commonly found in the inter-nodular tissue in association with streaming of folli-cles (Fig. 44–96B). There is often prominent fibrosisbetween the nodules. Because of the presence ofmultiple highly cellular nodules, cellular atypia, andpseudoinfiltrative pattern created by the fibrosis,dyshormonogenetic goiter can be mistaken for follic-ular carcinoma.706
Differential Diagnosis
FOLLICULAR CARCINOMA. In contrast to follicu-lar carcinoma, the different nodules exhibit differentdegrees of cellularity and architectural features, andgenuine vascular invasion is lacking.707
NODULAR GOITER. In contrast to nodulargoiter, there is scanty colloid, less degenerativechange, presence of prominent nuclear atypia, andabsence of normal internodular tissue.706
THYROID TREATED WITH RADIOACTIVE IODINE.The thyroid glands in patients treated with radioac-tive iodine can be indistinguishable from dyshor-monogenetic goiter histologically. The clinical his-tory is essential for making the distinction.
Fine-Needle Aspiration–AssociatedChanges in the Thyroid Gland
Fine-needle aspiration of the thyroid gland can leadto a variety of histologic changes, some mundaneand some potentially causing diagnostic prob-lems.101, 106
TISSUE INJURYIn the track of the needle pass, a linear hemorrhagictrack or an irregularly shaped hematoma is formed(Fig. 44–97A). The thyroid follicles in the vicinitycan undergo partial disruption or necrosis.
REPARATIVE CHANGEOrganization of the hematoma and damaged tissueleads to granulation tissue formation, chronic in-flammatory cell infiltration, hemosiderin deposition,and subsequently fibrous scarring.
TISSUE INJURY OR REPAIR-ASSOCIATEDREACTIVE CHANGES THAT MAY LEAD TOA MISDIAGNOSIS OF MALIGNANCYThe stromal reparative reaction to the trauma offine-needle aspiration can be exuberant. Active-look-ing plump spindly myofibroblasts are admixed withthin-walled blood vessels, histiocytes, and hemosid-erin (Fig. 44–97B). The lesion can be mistaken forKaposi’s sarcoma or other sarcomas; the term post–fine-needle aspiration spindle cell nodule has also beenapplied to this lesion.708
Tumor infarction complicating fine-needle aspi-ration can be accompanied by exuberant fibrogranu-lation tissue that begins in the peripheral zone andgradually extends inward. This reparative processcan potentially be mistaken for anaplastic carcinoma,attributable to the poorly defined contour of thelesion and reactive atypia of the spindly cells (Fig.44–98).
Organization of the fine-needle aspiration–asso-ciated hematoma can result in an exuberant, Massontumor– like reaction, which can potentially be mis-taken for angiosarcoma.709
The follicles around the areas of tissue injury orinfarction can exhibit reactive atypia, such as nuclearenlargement and prominent nucleoli, and can poten-tially be mistaken for high-grade carcinoma. Thesereactive follicles can show anastomosis and intrafol-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–97. Fine-needle aspiration–associated changes in the thyroid. A. A linear hemorrhagicneedle track is evident. B. Exuberant fibroblastic-myofibroblastic reaction in an area of tissue injury,so-called post–fine-needle aspiration spindle cell nodule.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

66 Endocrine System
licular hemorrhage, resulting in an angiosarcoma-like appearance106, 709, 710 (Fig. 44–99).
TUMOR IMPLANTATION IN NEEDLE TRACKAt the site of needle puncture of the fibrous capsuleof a thyroid neoplasm, some tumor islands can her-niate into the capsule. This phenomenon (capsularrupture) can potentially lead to an erroneous inter-pretation of capsular invasion (see Fig. 44–22 andTable 44–8).
TUMOR INFARCTIONAmong the various types of thyroid tumors, Hurthlecell tumor is particularly prone to undergo infarc-tion after fine-needle aspiration, probably because ofthe high energy requirements of the mitochondria-rich tumor cells104 (Fig. 44–100). Papillary carcinomaalso occasionally undergoes infarction after fine-nee-
dle aspiration (see Fig. 44–98). It can be difficult toarrive at a definitive diagnosis in the excision speci-men if the tumor shows complete infarction.
Amyloid Goiter
The thyroid gland is a common site for depositionof amyloid in systemic amyloidosis, but this usuallydoes not result in enlargement of the thyroid orclinical symptoms. However, on occasion, amyloiddeposits are so extensive that the patients presentwith a nontender, rapidly enlarging neck mass,which may be associated with dysphagia, dyspnea,and hoarseness. There is usually no clinical or bio-chemical evidence of thyroid dysfunction.711, 712
On histologic examination, amyloid is depositedbetween and around the follicles, accompanied by
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–98. Fine-needle aspiration–associated infarction of papillary carcinoma. A. In most areasof the resection specimen, there is prominent myofibroblastic proliferation associated with histiocytesand deposits of hematoidin and hemosiderin. This represents organization of the infarct. B. Residualpapillary carcinoma is identified focally (right upper field). Note the adjacent reparative reaction andinfarcted tumor (lower field).
FIGURE 44–99. Fine-needle aspiration–associated reactive cellu-lar atypia. Around the hemorrhagic needle track, the folliclesanastomose to produce branching clefts, which in association withthe extravasated blood mimic angiosarcoma.
FIGURE 44–100. Fine-needle aspiration–associated infarction ofHurthle cell adenoma. Virtually the entire tumor has undergoneinfarction. Necrotic ghost cells are seen in the left field, and onlya thin rim of viable tumor is seen in the right field. The interven-ing zone shows histiocytic infiltration and reparative changes.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 67
atrophy of the follicles (Fig. 44–101). Amyloid isalso deposited in the blood vessel walls. Adiposecells are commonly interspersed within the amyloid.The amyloid can be of AA or AL type.
Black Thyroid
Black thyroid is an uncommon but dramatic condi-tion caused by administration of minocycline, aform of tetracycline. There are no clinical symptoms.On gross evaluation, the thyroid is black. On histo-logic examination, the follicular cells contain fine,dark brown granules, and ultrastructural analysisshows the pigment to be located in lysosomes (Fig.
44–102). The pigment is currently believed to resultfrom oxidative interaction between thyroid peroxi-dase and the drug; it resembles neuromelanin inhistochemical properties.713–720 Of interest, when atumor arises in a black thyroid, the tumor is oftennonpigmented.721–723
Uncommon Lesions of the ThyroidGland
Exceptional examples of Rosai-Dorfman disease, ma-lacoplakia, extramedullary hematopoiesis, and in-flammatory pseudotumor (plasma cell granuloma)have been reported in the thyroid.621, 724–730
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–101. Amyloid goiter. There is interstitial depositionof eosinophilic-staining amyloid. Commonly, there are inter-spersed adipose cells. The follicles are atrophic and lined by at-tenuated epithelium.
FIGURE 44–102. Black thyroid associated with minocycline in-take. The follicular epithelial cells contain bright brown granulesin the cytoplasm.
B. The Parathyroid Gland
NEOPLASTIC LESIONS
Classification
Few tumor types are known to affect the parathy-roid gland, and they include the following:
Parathyroid adenomaTypicalVariants
LipoadenomaPapillary variantWater-clear variantFollicular variantOxyphil variant
Parathyroid carcinoma (functional or nonfunc-tional)
Parathyroid neoplasm of uncertain malignantpotential
General Considerations
PATHOGENESISParathyroid adenomas and carcinomas usually occursporadically, but they can sometimes occur as acomponent of multiple endocrine neoplasia (MEN 1and MEN 2) or familial idiopathic hyperparathy-roidism.731–733 Radiation to the head and neck regionhas also been implicated as a possible etiologic fac-tor of parathyroid adenoma.734, 735 Parathyroid carci-noma can occasionally supervene on parathyroid ad-enoma or parathyroid hyperplasia.736
Copyright � 2003, Elsevier Science (USA). All rights Reserved

68 Endocrine System
HYPERPARATHYROIDISM AS THE MAINCLINICAL MANIFESTATION OFPARATHYROID NEOPLASMSParathyroid neoplasms typically present with fea-tures of hyperparathyroidism, although some pa-tients are asymptomatic. There are three forms ofhyperparathyroidism: primary, secondary, and terti-ary. Only the primary and tertiary forms are associ-ated with hypercalcemia and its related complica-tions, such as polyuria and polydipsia, muscleweakness, renal stone, and mental disturbance, butall three forms can be associated with hyperparathy-roid bone disease manifesting as bone pain or frac-ture.733, 737–748
Primary HyperparathyroidismPrimary hyperparathyroidism is defined as over-
production of parathyroid hormone as a result ofintrinsic abnormality of the parathyroid glands. Inmore than 85% of cases, the underlying pathologicprocess is a parathyroid neoplasm. The remainingcases result from primary parathyroid hyperplasia,which can be sporadic or syndromatic (Table44–19).
Secondary HyperparathyroidismSecondary hyperparathyroidism is defined as
compensatory hyperplasia of parathyroid glandswith overproduction of parathyroid hormone due tohypocalcemia. As a result, the serum calcium con-centration is often normalized. Nonetheless, the para-thyroid hormone can stimulate bone resorption, re-sulting in parathyroid bone disease. Underlyingdisorders include chronic renal failure (the most
common), malabsorption, vitamin D deficiency, andrenal tubular acidosis.
Tertiary HyperparathyroidismTertiary hyperparathyroidism is defined as au-
tonomous parathyroid hyperfunction superveningon secondary hyperparathyroidism. As a result, theserum calcium concentration is elevated. The auton-omous parathyroid hyperfunction is most oftencaused by nodular hyperplasia; it is only uncom-monly due to superimposed parathyroid adenomaor carcinoma.
Parathyroid Adenoma
CLINICAL CONSIDERATIONSPresentationParathyroid adenoma is the most common cause
of primary hyperparathyroidism (�85%).749, 750 It oc-curs in patients with a mean age of 56 to 62 years.Women are more commonly affected than are men.Approximately 50% of patients are asymptomatic,being incidentally found to have hypercalcemia onroutine blood chemistry.750, 751 Others present withrenal stone (30%) or parathyroid bone disease (20%),but simultaneous renal and skeletal disease is ex-tremely rare.750–755 Surgical excision of the single in-volved parathyroid gland is curative.749, 756
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–19. Syndromes Associated with Hyperparathyroidism
MEN 1 MEN 2AFamilial IsolatedHyperparathyroidism
Endocrine organdisease
Parathyroid hyperplasia or neo-plasm
Thyroid nodule or follicular ade-noma
Adrenal nodule or adenomaIslet cell tumorPituitary adenomaThymic carcinoidBronchial carcinoid
Parathyroid hyperplasia or neo-plasm
Thyroid medullary carcinomaPheochromocytoma
Parathyroid hyperplasia or neo-plasm
Other clinicalfeatures
Facial angiofibromasCollagenomasMultiple lipomas
Lichen amyloidosis (some cases) Some kindreds also have jaw tu-mors (hyperparathyroidism–jaw tumor syndrome)
Natural historyof hyperpara-thyroidism
Hyperparathyroidism is com-monly the first presentation.
Serum calcium level tends to belower than that of parathyroidadenoma, but incidence of re-nal or bone involvement issimilar.
Hyperparathyroidism occurs in20%–30% of cases and is usu-ally mild and asymptomatic.
Hyperparathyroidism is often di-agnosed at an early age.
Incidence of renal stone is high.Recurrent or persistent hyper-
parathyroidism is common.
Genetic basis Germline mutation in MEN1 lo-cus on chromosome 11q13
Germline gain-of-function muta-tion in RET proto-oncogene onchromosome 10q11
Genetic locus linked to 1q21–32(HPT-JT or HRPT2 gene)
Although parathyroid adenoma typically in-volves a single gland, occasionally two of the fourglands are simultaneously involved (double ade-noma) on both sides or on the same side of the
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 69
neck.751, 757–760 These patients are often symptomaticand have a significantly higher parathyroid hor-mone level and tumor weight than with solitary ad-enoma. Because distinction from asymmetric pri-mary hyperplasia of the parathyroid glands can bedifficult, strict criteria must be applied for its diag-nosis757, 758:
• Two enlarged parathyroid glands are confirmedhistologically to be hypercellular.
• The remaining parathyroid glands are confirmedintraoperatively to be normal (preferably con-firmed histologically by biopsy).
• No clinical evidence or family history of multipleendocrine neoplasia or familial hyperparathyroid-ism is found.
• Permanent cure of hypercalcemia is achieved byexcision of the two enlarged glands alone.
Parathyroid adenomas can sometimes causeproblems in their localization because of occurrence
in ectopic locations, such as the mediastinum, thy-roid, or esophagus.761–766 When they occur withinthe thyroid gland, they can potentially be mistakenfor thyroid follicular adenoma or medullary carci-noma.761, 767
Macroscopic FindingsParathyroid adenomas usually weigh less thanwith size ranging from less than 1 cm to several1 g,
centimeters.768 The degree of hypercalcemia is gener-ally correlated with the weight of the tumor.768 Para-thyroid adenoma forms a solitary circumscribednodule, which is usually soft and orange-brown orreddish yellow to mahogany brown. Hemorrhage orcystic degeneration can sometimes be seen. The un-affected parathyroid glands are normal in size orsmall.
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsParathyroid adenomas are typically well circum-
scribed and solitary, although exceptionally theymay be multinodular (Fig. 44–103). Vague lobula-tion may be present.769, 770 A thin rim of compressedparathyroid tissue can be present at the periphery.In contrast to the normal parathyroid gland, inter-spersed adipose cells are absent or scanty.
The tumor cells form solid sheets, cords, acini,follicles, and microcysts traversed by a delicate cap-illary or sinusoidal network (Fig. 44–104). They arepolygonal, and the cytoplasm can be clear, eosino-philic, or oxyphilic. The nuclei are usually dark,round, and uniform, but there can be interspersednuclei that are large, hyperchromatic, or even bi-zarre768 (Fig. 44–105). The nuclei also show a ten-dency to be polarized toward the vascular aspect ofthe cells (Fig. 44–106). Mitotic figures are rare orabsent. Vague nodular foci are sometimes seenwithin the tumor.771
Fibrosis, hemorrhage, infarction, or cystic changecan occur, but there should not be coagulative tu-mor necrosis; if it is present, coagulative tumor ne-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–103. Parathyroid adenoma. The well-circumscribedtumor exhibits a solid growth pattern punctuated by edematousareas (left field). Residual normal parathyroid tissue is seen in theright upper field.
FIGURE 44–104. Parathyroid adenoma. A. Clear cells grow in a diffuse pattern and are characteristi-cally traversed by delicate blood vessels. B. The tumor shows a complex acinar growth pattern.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

70 Endocrine System
FIGURE 44–106. Parathyroid adenoma. A characteristic featurecommonly seen in the normal parathyroid gland, parathyroid ad-enoma, and parathyroid carcinoma is palisading of nuclei alongthe vascular pole of the cells.
crosis strongly suggests parathyroid carcinoma. Rarecases show a lymphoid infiltrate in the peripheralportion in the form of lymphoid follicles or in theparenchyma in the form of isolated 772, 773cells.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–105. Parathyroid adenoma. A. The tumor cells pos-sess clear or eosinophilic cytoplasm. The nuclei appear uniformand dark staining. B. In focal areas, there are cells with largehyperchromatic nuclei. Presence of these large nuclei is not indic-ative of malignancy. C. In this example, most nuclei are mildlyatypical.
Rarely, intrafollicular or interstitial amyloid can befound767, 774, 775 (Fig. 44–107). The morphologic vari-ants are listed in Table 44–20 (Figs. 44–107 to44–109).775–788
ImmunohistochemistryThe tumor cells of parathyroid adenoma are im-
munoreactive for cytokeratin, pan-neuroendocrinemarkers (such as synaptophysin, chromogranin, andneurofilament), and parathyroid hormone.789–791 TheKi-67 proliferative index is low (0.5% to 5.1%, with amean of 2% to 3%), but the nodular foci may showa higher index.771, 792–794
Immunohistochemical staining for parathyroidhormone is rarely required for diagnostic purposes,except when there are difficulties in distinction froma thyroid follicular adenoma or when the tumor oc-curs in an ectopic location.
Molecular Biology and GeneticsMolecular evidence of monoclonality can be
demonstrated in most parathyroid adenomas by useof X-linked restriction fragment length polymor-phism studies.795–797 Furthermore, some cases exhibittumor-specific DNA alterations in the parathyroidhormone gene.795
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 71
FIGURE 44–107. Parathyroid adenoma, oxyphilic type. A. The tumor cells form trabeculae and acini.Amyloid is found in the lumina of the acini. B. This example shows a diffuse growth pattern. Incontrast to Hurthle (oxyphilic) cells of the thyroid, the cell membranes are typically distinct.
FIGURE 44–108. Parathyroid lipoadenoma. Islands of parathy-roid parenchymal cells are interspersed among abundant adiposecells. The circumscribed border of the large tumor is seen in theleft upper field.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–20. Morphologic Variants of Parathyroid Adenoma
Variant Major Pathologic Findings Potential Diagnostic Pitfall
Lipoadenoma(“parathyroidhamartoma”)
Often large size; chief and oxyphil cells are intermingledwith many mature adipose cells, which occupy 20%–90% of the tissue area; loose fibromyxoid stroma canbe present in some cases
Without information on the gross appearance(circumscribed and large), it can be mis-taken histologically for normal parathyroid
Papillary Prominent papillary pattern May be mistaken for papillary thyroid carci-noma
Water-clear cell Composed of tumor cells with clear cytoplasm and dis-tinct cell membranes
—
Follicular Prominent follicular-acinar pattern May be mistaken for follicular thyroid neo-plasm
Oxyphilic Composed entirely of oxyphilic cells with abundant eo-sinophilic granular cytoplasm
May be mistaken for Hurthle cell neoplasmsof thyroid
FIGURE 44–109. Parathyroid adenoma, papillary variant. Thepapillary processes are not genuine papillae but represent pseu-dopapillae formed by dehiscence of the tumor tissue.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

72 Endocrine System
On cytogenetic analysis, rare cases of parathy-roid adenoma show pericentric inversion of chromo-some 11, which results in translocation of the cyclinD1 (PRAD1) gene with the parathyroid hormonegene, causing overexpression of cyclin D1 and henceincreased cellular proliferation.795, 796, 798–801 Immu-nohistochemical expression of cyclin D1 occurs at ahigher frequency (� 25% of cases), suggestingderegulation of cyclin D1 by mechanisms otherthan pericentric chromosome inversion in such
The MEN 1–associated MEN1 gene798, 802cases.shows somatic mutation in 10% to 23% of sporadicparathyroid adenomas.803, 804 Chromosome abnormal-ities identified by comparative genomic hybridiza-tion include loss of 11p, 11q, 1p, and 1q and gain of16p and 19p.805
Differential Diagnosis
PRIMARY OR SECONDARY PARATHYROID HY-PERPLASIA. In parathyroid hyperplasia, all the para-thyroid glands should be enlarged, although theyare unevenly enlarged in some cases. Not uncom-monly, the individual enlarged glands have a multi-nodular appearance.
PARATHYROID CARCINOMA. See subsequentsection.
THYROID FOLLICULAR ADENOMA. When theparathyroid tumor is inside the thyroid gland andshows a microfollicular pattern, it can be mistakenfor a follicular adenoma. Parathyroid adenoma isimmunoreactive for parathyroid hormone, whereasthyroid follicular adenoma is immunoreactive forthyroglobulin.
OXYPHIL CELL NODULE. Oxyphil cell nodulesare a common incidental finding in the parathyroidgland, especially in an older subject. They are smalland commonly multifocal (Fig. 44–110).
Intraoperative Frozen SectionDiagnosis of Parathyroid AdenomaIntraoperative frozen section evaluation of pa-
tients presenting with hyperparathyroidism aims toachieve the following806, 807:
• Confirm that the tissue removed for examinationindeed represents parathyroid tissue, not lymphnode, thyroid, or ectopic thymus.
• Determine whether the abnormal parathyroid tis-sue represents parathyroid adenoma (removal ofthe diseased gland alone is sufficient), parathyroidhyperplasia (removal of 3.5 glands is required), orparathyroid carcinoma (en bloc radical excision isrequired).749, 756
The gland should be measured, weighed, andexamined histologically. It is usually easy to confirmthat the excised tissue is parathyroid gland on histo-logic examination, except that a small biopsy speci-men of lymph node may occasionally be misinter-preted as parathyroid tissue because of artifactualspaces created by freezing that mimic adiposecells.808 A parathyroid gland with few or no inter-spersed adipose cells is supportive of a diagnosis of“hypercellular parathyroid gland, consistent withparathyroid adenoma or hyperplasia” (Table44–21). Some investigators consider lipid staining(Sudan II or IV, oil red O) on frozen sections orimprint smears to be helpful in identifying an ab-normal parathyroid gland797, 809–812 because the nor-mal parathyroid cells contain abundant intracyto-plasmic lipid droplets, whereas the hyperplastic oradenomatous cells are often devoid of intracyto-plasmic lipid. An exception is the oxyphil cell,which always contains no or scanty intracytoplasmiclipid droplets.770 Adenomatous or hyperplasticglands may occasionally contain intracytoplasmiclipid, albeit weakly and focally.813–816
After it is confirmed that the parathyroid glandis hypercellular, the next step is to determinewhether it represents an adenoma or hyperplasticprocess. Although a compressed rim of normal para-thyroid gland is characteristic of parathyroid ade-noma, it is not always found and it can be mim-icked by the compressed intervening parenchyma inmultinodular parathyroid The817, 818hyperplasia.most reliable way to make the distinction is by de-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–110. Oxyphil cell nodule. Small nodule composedentirely of oxyphilic cells is a common incidental finding in theparathyroid gland.
TABLE 44–21. Features Indicative of a Hypercellular(Neoplastic or Hyperplastic) ParathyroidGland
Weight: single gland weighing �100 mg (normal weight, �30mg)
Adipose cells in gland: few or absent (on average, �17% of anormal parathyroid gland is composed of adipose cells)
Intracytoplasmic lipid droplets as demonstrated by lipid stain:absent or scanty
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 73
termining the status of the other parathyroid glands.If they are all normal in size or small, a diagnosis ofadenoma is favored. If all are enlarged, a diagnosisof parathyroid hyperplasia is favored. Simple in-spection is not reliable because some hyperplasticprocesses affect the glands unequally; it is preferableto take an incisional biopsy specimen of one ormore glands for histologic confirmation to ascertainwhether they are normal-suppressed or hyper-plastic.819
Intraoperative assay of the parathyroid hormonelevel is an alternative way for guiding the extent ofsurgery, taking advantage of the fact that the hor-mone has a short half-life.807, 820–822 If preoperativeimaging studies can identify an enlarged parathy-roid gland, a more limited unilateral procedure canbe performed in place of bilateral neck exploration.Approximately 15 minutes after removal of the en-larged gland, a serum sample is taken for parathy-roid hormone assay. A significant drop in the hor-mone level (�50%) suggests successful removal ofthe hypersecreting tissue, and thus cure is reasona-bly ensured. The other parathyroid glands have tobe explored for hyperplasia if the parathyroid hor-mone level remains elevated after removal of oneenlarged gland.
Parathyroid Carcinoma
CLINICAL CONSIDERATIONSPresentationParathyroid carcinomas are rare, constituting
only about 2% of all parathyroid neoplasms. Com-pared with parathyroid adenoma, the patients withparathyroid carcinoma have a lower mean age (45 to54 years), there is no sex predilection, and virtuallyall patients are symptomatic because of the high se-rum calcium level (3.5 to 4 mmol/L). Only rare tu-
mors are nonfunctional.* The clues for recognizingthe malignant nature of a parathyroid neoplasm arelisted in Table 44–22.
Macroscopic FindingsThe carcinomas are usually hard because of the
presence of fibrous trabeculae. The size ranges from1 cm to several centimeters.752 They are often muchlarger than parathyroid adenomas, with an averageweight of 12 g (versus less than 1 g for parathyroidadenoma).768 They can be circumscribed or invasive.Necrosis and calcification can be present.834
DIAGNOSTIC CONSIDERATIONSMicroscopic FindingsThe tumor shows frank invasive features or is
surrounded by a thick fibrous capsule736 (Fig.44–111). It comprises polygonal cells forming solidsheets, trabeculae, acini, and packets.755 In some
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–22. Clues for Recognizing ParathyroidCarcinoma Versus Parathyroid Adenoma
Clinical Clues* Clues at Operation
High serum calcium level(�3.5 mmol/L or 14 mg/dL)
Simultaneous parathyroidbone disease and renalstone (found in �40%)
Palpable neck mass (found in�40%)
Vocal cord paralysisPresence of metastasis
Firm consistencyThick capsuleAdherence and invasion to
adjacent organs, e.g., thy-roid, muscle, nerve, esoph-agus
* The clinical clues actually reflect a large tumor or a tumor withinvasive properties.
*References 731, 736, 752–754, 767, 823–833.
FIGURE 44–111. Parathyroid carcinoma. A. The tumor shows frank infiltration into the surroundingfibrofatty tissue. B. In this example, the tumor grows in the form of irregular infiltrative islands. Thestroma is desmoplastic.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

74 Endocrine System
cases, the nuclei are uniform and bland-looking,with or without interspersed large hyperchromaticor bizarre nuclei731 (Fig. 44–112). In other cases, thenuclei are overtly pleomorphic (Fig. 44–112C). Nu-cleoli are sometimes prominent.835 The cytoplasm isclear, lightly eosinophilic, or oxyphilic.834, 836, 837 Onoccasion, monotonous small cells with high nuclear-
to-cytoplasmic ratio can dominate (Fig. 44–113). Co-agulative necrosis can be present.835
The features for diagnosing parathyroid carci-noma are outlined in Table 44–23.838 Stringent crite-ria must be used in the assessment of capsular orvascular invasion, similar to those applied for follic-ular neoplasms of the thyroid. Broad fibrous septa
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–112. Parathyroid carcinoma showing the spectrumof cytologic features. A. In this example, the cells have fairlyuniform nuclei. B. In this example, interspersed cells with largehyperchromatic nuclei are present. Mitotic figures are also evi-dent. C. In this example, many tumor cells are atypical and havemacronucleoli.
FIGURE 44–113. Parathyroid carcinoma. A. Monotonous small cells are seen in the left field of thistumor. B. Higher magnification shows small cells with high nuclear-to-cytoplasmic ratio. A mitoticfigure is seen near the central field.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 75
traversing the tumor must be accompanied by ex-pansile nodules before they are considered signifi-cant to distinguish them from the focal scarring dueto previous hemorrhage or surgery752 (Fig. 44–114).Although mitotic figures have been emphasized asbeing the single most important criterion of malig-nancy,752 they are now recognized as being signifi-cant only when they are present in considerablenumbers736, 838–840 (see Fig. 44–112B). Conversely,some carcinomas may show no or few mitotic fig-ures.752, 835, 838
ImmunohistochemistryThe tumor cells of parathyroid carcinoma are
immunoreactive for cytokeratin, pan-neuroendocrine
markers, and parathyroid hormone. Immunostainingfor parathyroid hormone is most helpful for con-firming a diagnosis of nonfunctioning or ectopicparathyroid carcinoma.
Molecular BiologyIn most parathyroid carcinomas, allelic loss of
the retinoblastoma (RB) tumor suppressor gene isfound.800, 838, 841 On immunohistochemical staining,lack of immunoreactivity for the RB protein occursin 20% to 88% of cases.792, 841, 842 Cyclin D1 overex-pression is also common (91% of cases).798, 802 Thereis commonly reduced expression of the cyclin-de-pendent kinase inhibitor protein p27 (mean labelingindex of 14% versus 57% for parathyroid ade-noma).794
Differential DiagnosisThe main problem in diagnosis of parathyroid
carcinoma is to recognize its malignant nature. Thedifficulty lies in the fact that some apparently bland-looking tumors may declare themselves to be malig-nant by subsequent recurrence or metastasis.836, 843 Insome cases, the malignant nature of the tumor isobvious by virtue of the frankly invasive growth,significant cellular pleomorphism, and frequent mi-toses. However, in other cases, it is essential to con-sider a number of features to render a diagnosis ofmalignancy (see Table 44–23).
Immunostaining for the proliferation markerKi-67 can sometimes be helpful because the index ishigher in parathyroid carcinoma than in ade-noma.792–794 Nonetheless, it cannot be used as thesole criterion because there is overlap in the countsbetween adenomas and carcinomas.844 Whereas ahigh Ki-67 index (�5%) suggests a diagnosis of car-cinoma, a low index does not exclude this possibil-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
TABLE 44–23. Histologic Criteria for Diagnosis of Parathyroid Carcinoma in a Parathyroid Neoplasm
Absolute Criteria of Malignancy Features Associated with Malignancy
Presence of any one of the following criteria is sufficient for adiagnosis of malignancy:
—Invasion into surrounding tissues● Thyroid● Esophagus● Nerves● Soft tissues—Regional or distant metastasis
When the absolute criteria are lacking, at least 2 and prefera-bly 3 or more of the following features have to be presentto establish a diagnosis of malignancy:—Vascular invasion—Capsular invasion—Broad fibrous bands splitting the parenchyma and de-
lineating expansile nodules—Coagulative tumor necrosis—Mitotic count �5 per 10 high-power fields—Sheetlike monotonous small cells with high nuclear-to-cy-
toplasmic ratio—Generalized cellular atypia—Frequent macronucleoli
Ancillary studies that may help in supporting a diagnosis of parathyroid carcinoma over adenoma:Immunostaining for Ki-67: high Ki-67 index (mean Ki-67 index for carcinoma is 6.1%–8.4%; that for adenoma is 2.0%–3.3%)Immunostaining for retinoblastoma protein (lack of nuclear staining in tumor cells, provided that appropriate internal positive
control is found) or molecular analysis of retinoblastoma gene in tumor (allelic loss)Immunostaining for p27: low percentage of positive cells (mean labeling index 13.9% for carcinoma versus 56.8% for adenoma)
In some cases, there are some features associated with malignancy, but they are insufficient for a definite diagnosis of carcinomato be made. A designation “parathyroid neoplasm of uncertain malignant potential” may be appropriate in such circumstances.
FIGURE 44–114. Parathyroid carcinoma. The tumor is traversedby dense fibrous bands associated with expansile nodules of tu-mor tissue.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

76 Endocrine System
ity. The role of flow cytometric analysis of DNA inthe diagnosis of parathyroid carcinoma remains con-troversial.845–848 A study employing a static DNAfluorometric method has reported a high nuclearDNA content and aneuploidy to favor a diagnosis ofparathyroid carcinoma over parathyroid adenoma.849
When there are some but inconclusive featuresassociated with malignancy, the designation “para-thyroid neoplasm of uncertain malignant potential”or “atypical parathyroid adenoma” can be ap-plied.850 Follow-up with regular monitoring of theserum calcium level will be helpful for such pa-tients. Firm data on the outcome of these cases arelacking.
PROGNOSTIC CONSIDERATIONSGeneral BehaviorParathyroid carcinoma generally pursues an in-
dolent clinical course. It can invade contiguousstructures, particularly the thyroid.754, 830, 851 Surgeryis the mainstay of treatment. Local recurrence devel-ops in approximately one third of patients, usuallywithin 3 years833; this occurrence may be reduced bypostoperative radiotherapy.826 About one third ofpatients develop metastasis, usually relatively late inthe course; the favored sites are regional lymphnodes of the neck and mediastinum, lungs, liver,and bones. The relapse usually manifests as recur-rent hypercalcemia, and symptomatic control oreven occasionally cure can still be achieved by fur-ther operations.* The 5-year and 10-year survivalrates are 60% and 40%, respectively. Death is usu-ally caused by metabolic complications of hyper-calcemia rather than by organ replacement bytumor.752–754, 834, 853
Prognostic FactorsData on prognostic factors of parathyroid carci-
noma are limited. Adequate en bloc excision (re-moval of the tumor, adjacent thyroid lobe, paratra-cheal soft tissues and lymph nodes, and ipsilateralthymus) on recognition of the malignant nature ofthe tumor at the initial operation offers the bestchance of cure.824, 827, 833, 852 Nonfunctioning parathy-roid carcinomas appear to behave more aggressivelythan functioning ones.823 The triad of macronucleoli,more than 5 mitoses per 50 high-power fields, andnecrosis is correlated with a more aggressive out-come. High nuclear DNA content is correlated witha less favorable survival.835
Contents of the Final SurgicalPathology Report
The checklist of contents of the final report of para-thyroid carcinoma excision specimens is listed inTable 44–24.
NON-NEOPLASTIC LESIONS
Primary Parathyroid Chief CellHyperplasia
CLINICAL CONSIDERATIONSPrimary parathyroid chief cell hyperplasia is a denovo hyperplastic process involving all the parathy-roid glands, producing the clinical features of pri-mary Approxi-737, 756, 769, 854hyperparathyroidism.mately 80% of cases are sporadic; the other casesoccur as a component of MEN 1, MEN 2, familialisolated hyperparathyroidism, or hyperparathyroid-ism–jaw tumor syndrome. The condition is morecommon in females than in males. Treatment con-sists of subtotal parathyroidectomy (removal of 3.5glands); the remaining gland is sometimes autoim-planted in the forearm.
DIAGNOSTIC CONSIDERATIONSAlthough all parathyroid glands are involved, theymay be unevenly enlarged, with some glands appar-ently having a “normal size”—and hence leading toa misdiagnosis of parathyroid neoplasm. The com-bined weight of the parathyroid glands ranges fromless than 1 g to 10 g.
In primary chief cell hyperplasia, the parathy-roid glands are hypercellular, with marked reduc-tion in interposed adipose cells. The proliferatedparathyroid cells include predominantly chief cells,but water-clear cells and oxyphil cells are oftenpresent. The parathyroid cells show a solid, trabecu-lar, follicular, or cordlike growth. In areas, it is com-mon to see the characteristic palisading of the nuclei
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
*References 753, 754, 823, 828, 830, 843, 852.
✒ TABLE 44–24. Contents of the Final Report:Parathyroid Excision Specimens
Specimen type/operation procedure
DiagnosisHistologic diagnosis
Other tumor featuresTumor locationTumor sizeEncapsulated or nonencapsulatedCapsular invasion (absent, present, extensive)Vascular invasion (absent, present, extensive)Tissues or structures invaded by the carcinomaMitotic countImmunohistochemical expression of RB, cyclin D1, p27 (op-
tional)
Surgical margins: free, close to surgical margin, or margin in-volved (specify site)
Non-neoplastic parathyroid: normal, diffuse hyperplasia, nodu-lar hyperplasia
Lymph nodesNumber of lymph nodes found, and their location (level)Number of involved lymph nodesSize of largest metastatic depositPresence or absence of extracapsular extension
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 77
along the vascular septa. The pathologic process isinitially diffuse, but with time, nodules will super-vene on the background of diffuse hyperplasia. Thevarious nodules often show different cellular compo-sitions and different patterns of cellular organiza-tion.
Primary Water-Clear CellHyperplasia
CLINICAL CONSIDERATIONSWater-clear cell hyperplasia is a rare form of pri-mary parathyroid hyperplasia. It shows no familialincidence or association with multiple endocrineneoplasia. Of interest, for unknown reasons, thisentity has virtually disappeared in the past fewdecades.737, 738, 855, 856
The condition occurs mostly in older adults, butany age can be affected. It is slightly more commonin males than in females. The patients present withfeatures of primary hyperparathyroidism. In general,the hypercalcemia is more severe than in chief cellhyperplasia.
DIAGNOSTIC CONSIDERATIONSIn water-clear cell hyperplasia, the parathyroidglands are usually markedly enlarged; the combined
weight of the gland is frequently above 10 g. Theupper glands are often larger than the lower ones.On histologic examination, the hyperplastic parathy-roid cells are large and possess water-clear cyto-plasm. They form solid sheets and acini.
Secondary Parathyroid Hyperplasia
CLINICAL CONSIDERATIONSSecondary parathyroid hyperplasia is a hyperplasticcondition of the parathyroid glands in response tohypocalcemia or hyperphosphatemia. The most com-mon cause is chronic renal failure. The patientspresent with features of secondary hyperparathy-roidism (mostly with parathyroid bone disease) ortertiary hyperparathyroidism (mostly with complica-tions of hypercalcemia). Treatment consists of subto-tal parathyroidectomy.
DIAGNOSTIC CONSIDERATIONSThere is uniform or uneven enlargement of all para-thyroid glands, indistinguishable from that seen inprimary parathyroid hyperplasia. A multinodularpattern is seen in the majority of cases. The prolifer-ation involves chief cells, clear cells, and oxyphilcells, which are arranged in sheets, trabeculae, oracini (Fig. 44–115). There can be fibrous bands
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–115. Secondary parathyroid hyperplasia in chronicrenal failure. A. The enlarged parathyroid gland is converted intomultiple hyperplastic nodules. B. The nodules show different cellcompositions. This field may give a false impression of an ade-noma surrounded by compressed residual parathyroid tissue. C.The nodules often show a mixture of cell types.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

78 Endocrine System
around the nodules, hemosiderin deposition, andcystic change. Calcification can be present.
Parathyroid Cyst
Parathyroid cyst manifests clinically as a mass lesionor hypercalcemia, but it can also be an incidentalfinding. Its size can range from a few millimeters to10 cm. The wall is thin and translucent.857 A diagno-sis can be made by fine-needle aspiration, either byidentification of parathyroid cells or by demonstra-tion of elevated levels of parathyroid hormone inthe cystic fluid.858 On histologic examination, it isoften lined by attenuated parathyroid cells and sur-rounded by islands of normal, hyperplastic, or ade-nomatous parathyroid tissue (Fig. 44–116). That is,some cases represent cystic change of a parathyroidadenoma and are thus associated with hypercal-cemia.
Periparathyroid SalivaryHeterotopia–Cyst Unit
An uncommon lesion occurring in a periparathyroidlocation is the salivary heterotopia–cyst unit.859 It isusually small, measuring 1 to 6 mm, comprisingsmall lobules of salivary acini and cysts. The cystsare lined by flattened, ciliated, or columnar cells,without parathyroid cell lining. The salivary hetero-topia–cyst unit has been postulated to be of thirdand fourth-fifth branchial pouch derivation.
Amyloidosis
The parathyroid glands can be involved in systemicamyloidosis. The glands are enlarged and histologi-cally show deposition of amyloid in blood vesselwalls and the interstitium.860 When there is abun-
dant amyloid deposition, parenchymal cells may belost, leading to the development of mild hypocal-cemia.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
FIGURE 44–116. Parathyroid cyst. The cyst is lined by a singlelayer of parathyroid cells. Normal parathyroid tissue is identifiedin the wall (lower field).
REFERENCES
1. Hedinger C, Williams ED, Sobin LH: Histological Typing ofThyroid Tumors. WHO International Histological Classifica-tion of Tumors. 2nd ed. Berlin, Springer-Verlag, 1988.
2. Ordonez NG: Thyroid transcription factor-1 is a marker oflung and thyroid carcinomas. Adv Anat Pathol 7:123–127,2000.
3. Katoh R, Kawaoi A, Miyagi E, et al: Thyroid transcriptionfactor-1 in normal, hyperplastic, and neoplastic follicular thy-roid cells examined by immunohistochemistry and nonra-dioactive in situ hybridization. Mod Pathol 13:570–576, 2000.
4. Chan JKC: Tumors of the thyroid and parathyroid glands. InFletcher CDM (ed): Diagnostic Histopathology of Tumors.2nd ed. Edinburgh, Churchill Livingstone, 2000, pp 959–1056.
5. Katoh R, Miyagi E, Nakamura N, et al: Expression of thyroidtranscription factor-1 (TTF-1) in human C cells and medul-lary thyroid carcinomas. Hum Pathol 31:386–393, 2000.
6. Figge J, Jennings T, Gerasimov G: Radiation and thyroidcancer. In Wartofsky L (ed): Thyroid Cancer, A Comprehen-sive Guide to Clinical Management. Totowa, NJ, HumanaPress, 2000, pp 85–116.
7. Figge J: Epidemiology of thyroid cancer. In Wartofsky L (ed):Thyroid Cancer, A Comprehensive Guide to Clinical Man-agement. Totowa, NJ, Humana Press, 2000, pp 77–81.
8. Williams ED: The aetiology of thyroid tumours. Clin Endo-crinol Metab 8:193–207, 1979.
9. Feilotter H, Mulligan L: Endocrine cancers. In Foulkes WD,Hodgson SV (eds): Inherited susceptibility to cancer: clinical,predictive and ethical perspectives. Cambridge, UK, Cam-bridge University Press, 1998, pp 326–354.
10. Gilliland FD, Hunt WC, Morris DM, Key CR: Prognosticfactors for thyroid carcinoma. A population-based study of15,698 cases from the Surveillance, Epidemiology and EndResults (SEER) program 1973–1991. Cancer 79:564–573, 1997.
11. Brierley JD, Panzarella T, Tsang RW, et al: A comparison ofdifferent staging systems predictability of patient outcome.Thyroid carcinoma as an example. Cancer 79:2414–2423,1997.
12. Gemsenjager E, Heitz PU, Martina B: Selective treatment ofdifferentiated thyroid carcinoma. World J Surg 21:546–551,discussion 551–552, 1997.
13. Oertel YC, Oertel JE: Diagnosis of malignant epithelial thy-roid lesions: fine needle aspiration and histopathologic corre-lation. Ann Diagn Pathol 2:377–400, 1998.
14. Oertel YC: Fine-needle aspiration and the diagnosis of thy-roid cancer. Endocrinol Metab Clin North Am 25:69–91,1996.
15. Silver CE, Owen RP: Year 2000 update: what the head andneck surgeon expects of the pathologist. Pathol Case Rev 5:183–188, 2000.
16. Chang HY, Lin JD, Chen JF, et al: Correlation of fine needleaspiration cytology and frozen section biopsies in the diag-nosis of thyroid nodules. J Clin Pathol 50:1005–1009, 1997.
17. Quinn SF, Nelson HA, Demlow TA: Thyroid biopsies: fine-needle aspiration biopsy versus spring-activated core biopsyneedle in 102 patients. J Vasc Interv Radiol 5:619–623, 1994.
18. Munn JS, Castelli M, Prinz RA, Walloch JL: Needle biopsy ofnodular thyroid disease. Am Surg 54:438–443, 1988.
19. Lo Gerfo P: The value of coarse needle biopsy in evaluatingthyroid nodules. Thyroidology 6:1–4, 1994.
20. Wang C, Guyton SP, Vickery AL Jr: A further note on thelarge needle biopsy of the thyroid gland. Surg Gynecol Ob-stet 156:508–510, 1983.
21. Miller JM: Evaluation of thyroid nodules. Accent on needlebiopsy. Med Clin North Am 69:1063–1077, 1985.
22. Broughan TA, Esselstyn CB Jr: Large-needle thyroid biopsy:still necessary. Surgery 100:1138–1141, 1986.
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 79
23. Lang W, Georgii A, Stauch G, Kienzle E: The differentiationof atypical adenomas and encapsulated follicular carcinomasin the thyroid gland. Virchows Arch Pathol Anat 385:125–141, 1980.
24. Franssila KO, Ackerman LV, Brown CL: Follicular carci-noma. Semin Diagn Pathol 2:101–122, 1985.
25. Yamashina M: Follicular neoplasms of the thyroid. Total cir-cumferential evaluation of the fibrous capsule. Am J SurgPathol 16:392–400, 1992.
26. McHenry CR, Raeburn C, Strickland T, Marty JJ: The utilityof routine frozen section examination for intraoperative diag-nosis of thyroid cancer. Am J Surg 172:658–661, 1996.
27. Gibb GK, Pasieka JL: Assessing the need for frozen sections:still a valuable tool in thyroid surgery. Surgery 118:1005–1009, discussion 1009–1010, 1995.
28. Sabel MS, Staren ED, Gianakakis LM, et al: Use of fine-needle aspiration biopsy and frozen section in the manage-ment of the solitary thyroid nodule. Surgery 122:1021–1026,discussion 1026–1027, 1997.
29. Mulcahy MM, Cohen JI, Anderson PE, et al: Relative accu-racy of fine-needle aspiration and frozen section in the diag-nosis of well-differentiated thyroid cancer. Laryngoscope108:494–496, 1998.
30. Deligdisch L, Subhani Z, Gordon RE: Primary mucinous car-cinoma of the thyroid gland: report of a case and ultrastruc-tural study. Cancer 45:2564–2567, 1980.
31. Carcangiu ML, Sibley RK, Rosai J: Clear cell change in pri-mary thyroid tumors. A study of 38 cases. Am J Surg Pathol9:705–722, 1985.
32. Schroder S, Husselmann H, Bocker W: Lipid-rich cell ade-noma of the thyroid gland. Report of a peculiar thyroidtumour. Virchows Arch A Pathol Anat Histopathol 404:105–108, 1984.
33. Toth K, Peter I, Kremmer T, Sugar J: Lipid-rich cell thyroidadenoma: histopathology with comparative lipid analysis.Virchows Arch A Pathol Anat Histopathol 417:273–276,1990.
34. Schroder S, Bocker W: Clear-cell carcinomas of thyroidgland: a clinicopathological study of 13 cases. Histopathol-ogy 10:75–89, 1986.
35. Vuitch F, Leavitt A: Papillary variant of follicular adenomaof thyroid (abstract). Mod Pathol 3:104A, 1990.
36. Hjorth L, Thomsen LB, Nielsen VT: Adenolipoma of thethyroid gland. Histopathology 10:91–96, 1986.
37. Laforga JB, Vierna J: Adenoma of thyroid gland containingfat (thyrolipoma). Report of a case. J Laryngol Otol 110:1088–1089, 1996.
38. Gnepp DR, Ogorzalek JM, Heffess CS: Fat-containing lesionsof the thyroid gland. Am J Surg Pathol 13:605–612, 1989.
39. Gherardi G: Signet ring cell ’mucinous’ thyroid adenoma: afollicle cell tumour with abnormal accumulation of thyro-globulin and a peculiar histochemical profile. Histopathology11:317–326, 1987.
40. Mendelsohn G: Signet-cell–simulating microfollicular ade-noma of the thyroid. Am J Surg Pathol 8:705–708, 1984.
41. Rigaud C, Peltier F, Bogomoletz WV: Mucin producing mi-crofollicular adenoma of the thyroid. J Clin Pathol 38:277–280, 1985.
42. Alsop JE, Yerbury PJ, O’Donnell PJ, Heyderman E: Signet-ring cell microfollicular adenoma arising in a nodular ectopicthyroid. A case report. J Oral Pathol 15:518–519, 1986.
43. Hazard JB, Kenyon R: Atypical adenoma of the thyroid.Arch Pathol 58:554–563, 1954.
44. Lang W, Choritz H, Hundeshagen H: Risk factors in follicu-lar thyroid carcinomas. A retrospective follow-up study cov-ering a 14-year period with emphasis on morphological find-ings. Am J Surg Pathol 10:246–255, 1986.
45. Rosai J, Carcangiu ML, DeLellis RA: Tumors of the ThyroidGland. Atlas of Tumor Pathology. Third Series, Fascicle 5.Washington, DC, Armed Forces Institute of Pathology, 1992.
46. Rosai J: Ackerman’s Surgical Pathology. 8th ed. St. Louis, CVMosby, 1996.
47. Hirokawa M, Carney JA: Cell membrane and cytoplasmicstaining for MIB-1 in hyalinizing trabecular adenoma of thethyroid gland. Am J Surg Pathol 24:575–578, 2000.
48. Hirokawa M, Shimizu M, Manabe T, et al: Hyalinizing tra-becular adenoma of the thyroid: its unusual cytoplasmic im-munopositivity for MIB1. Pathol Int 45:399–401, 1995.
49. Papotti M, Riella P, Montemurro F, et al: Immunophenotypicheterogeneity of hyalinizing trabecular tumours of the thy-roid. Histopathology 31:525–533, 1997.
50. Rothenberg HJ, Goellner JR, Carney JA: Hyalinizing trabecu-lar adenoma of the thyroid gland: recognition and character-ization of its cytoplasmic yellow body. Am J Surg Pathol23:118–125, 1999.
51. Carney JA, Ryan J, Goellner JR: Hyalinizing trabecular ade-noma of the thyroid gland. Am J Surg Pathol 11:583–591,1987.
52. Sambade C, Sarabando F, Nesland JM, Sobrinho-Simoes M:Hyalinizing trabecular adenoma of the thyroid (case of theUllensvang course). Hyalinizing spindle cell tumor of thethyroid with dual differentiation (variant of the so-calledhyalinizing trabecular adenoma). Ultrastruct Pathol 13:275–280, 1989.
53. Katoh R, Jasani B, Williams ED: Hyalinizing trabecular ade-noma of the thyroid. A report of three cases with immuno-histochemical and ultrastructural studies. Histopathology15:211–224, 1989.
54. Bronner MP, LiVolsi VA, Jennings TA: PLAT: paragangli-oma-like adenoma of the thyroid. Surg Pathol 1:383–389,1988.
55. Schmid KW, Mesewinkel F, Bocker W: Hyalinizing trabecu-lar adenoma of the thyroid—morphology and differentialdiagnosis. Acta Med Austriaca 23:65–68, 1996.
56. Chetty R, Beydoun R, LiVolsi VA: Paraganglioma-like (hy-alinizing trabecular) adenoma of the thyroid revisited. Pa-thology 26:429–431, 1994.
57. Chan JKC, Tse CCH, Chiu HS: Hyalinizing trabecular ade-noma–like lesion in multinodular goiter. Histopathology16:611–614, 1990.
58. Li M, Rosai J, Carcangiu ML: Hyalinizing trabecular ade-noma of the thyroid: a distinct tumor type or a pattern ofgrowth? Evaluation of 28 cases (abstract). Mod Pathol 8:54A,1995.
59. Fonseca E, Nesland JM, Sobrinho-Simoes M: Expression ofstratified epithelial-type cytokeratins in hyalinizing trabecu-lar adenomas supports their relationship with papillary car-cinomas of the thyroid. Histopathology 31:330–335, 1997.
60. Li M, Carcangiu ML, Rosai J: Abnormal intracellular andextracellular distribution of basement membrane material inpapillary carcinoma and hyalinizing trabecular tumors of thethyroid: implication for deregulation of secretory pathways.Hum Pathol 28:1366–1372, 1997.
61. Hirokawa M, Carney JA, Ohtsuki Y: Hyalinizing trabecularadenoma and papillary carcinoma of the thyroid glandexpress different cytokeratin patterns. Am J Surg Pathol24:877–881, 2000.
61a. Papotti M, Volante M, Giuliano A, et al: RET/PTC activa-tion in hyalinizing trabecular tumors of the thyroid. Am JSurg Pathol 24:1515–1621, 2000.
61b. Cheung CC, Boerner SL, MacMillan CM, et al: Hyalinizingtrabecular tumor of the thyroid: a variant of papillary carci-noma proved by molecular genetics. Am J Surg Pathol 24:1622–1626, 2000.
61c. LiVolsi VA: Hyalinizing trabecular adenoma of the thyroid:adenoma, carcinoma or neoplasm of uncertain malignant po-tential? Am J Surg Pathol 24:1683–1684, 2000.
62. Schlumberger MJ: Papillary and follicular thyroid carcinoma(review). N Engl J Med 338:297–306, 1998.
63. Wright PA, Lemoine NR, Mayall ES, et al: Papillary andfollicular thyroid carcinomas show a different pattern of rasoncogene mutation. Br J Cancer 60:576–577, 1989.
64. Dahia PL, Marsh DJ, Zheng Z, et al: Somatic deletions andmutations in the Cowden disease gene, PTEN, in sporadicthyroid tumors. Cancer Res 57:4710–4713, 1997.
65. Porcellini A, Ciullo I, Pannain S, et al: Somatic mutations inthe VI transmembrane segment of the thyrotropin receptorconstitutively activate cAMP signalling in thyroid hyperfunc-tioning adenomas. Oncogene 11:1089–1093, 1995.
66. Porcellini A, Ciullo I, Laviola L, et al: Novel mutations of
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

80 Endocrine System
thyrotropin receptor gene in thyroid hyperfunctioning ade-nomas. Rapid identification by fine needle aspiration biopsy.J Clin Endocrinol Metab 79:657–661, 1994.
67. Krohn K, Fuhrer D, Holzapfel HP, Paschke R: Clonal originof toxic thyroid nodules with constitutively activating thyro-tropin receptor mutations. J Clin Endocrinol Metab 83:130–134, 1998.
68. Pinducciu C, Borgonovo G, Arezzo A, et al: Toxic thyroidadenoma: absence of DNA mutations of the TSH receptorand Gs alpha. Eur J Endocrinol 138:37–40, 1998.
69. Tonacchera M, Chiovato L, Pinchera A, et al: Hyperfunction-ing thyroid nodules in toxic multinodular goiter share acti-vating thyrotropin receptor mutations with solitary toxic ad-enoma. J Clin Endocrinol Metab 83:492–498, 1998.
70. Esapa C, Foster S, Johnson S, et al: G protein and thyrotro-pin receptor mutations in thyroid neoplasia. J Clin Endocri-nol Metab 82:493–496, 1997.
71. Crile G Jr, Pontius KI, Hawk WA: Factors influencing thesurvival of patients with follicular carcinoma of the thyroidgland. Surg Gynecol Obstet 160:409–413, 1985.
72. Schroder S, Bocker W, Dralle H, et al: The encapsulatedpapillary carcinoma of the thyroid. A morphologic subtypeof the papillary thyroid carcinoma. Cancer 54:90–93, 1984.
73. Shaha AR, Shah JP, Loree TR: Differentiated thyroid cancerpresenting initially with distant metastasis. Am J Surg174:474–476, 1997.
74. Lo CY, Lorentz TG, Wan KY: Follicular carcinoma of thethyroid gland in Hong Kong Chinese. Br J Surg 82:1095–1097, 1995.
75. Evans HL, Vassilopoulou-Sellin R: Follicular and Hurthle cellcarcinomas of the thyroid: a comparative study. Am J SurgPathol 22:1512–1520, 1998.
76. Woolner LB: Thyroid carcinoma: pathologic classificationwith data on prognosis. Semin Nucl Med 1:481–502, 1971.
77. Franssila KO: Prognosis in thyroid carcinoma. Cancer36:1138–1146, 1975.
78. Schroder S, Pfannschmidt N, Dralle H, et al: The encapsu-lated follicular carcinoma of the thyroid. A clinicopathologicstudy of 35 cases. Virchows Arch A Pathol Anat Histopathol402:259–273, 1984.
79. Lang W, Georgii A: Minimal invasive cancer in the thyroid.Clin Oncol 1:527–537, 1982.
80. Crile G Jr, Hawk WA: Carcinomas of the thyroid. Cleve ClinQ 38:97–104, 1971.
81. van Heerden JA, Hay ID, Goellner JR, et al: Follicular thy-roid carcinoma with capsular invasion alone: a nonthreaten-ing malignancy. Surgery 112:1130–1136, discussion 1136–1138, 1992.
82. Rossi RL, Nieroda C, Cady B, Wool MS: Malignancies of thethyroid gland. The Lahey Clinic experience. Surg Clin NorthAm 65:211–230, 1985.
83. Brooks JR, Starnes HF, Brooks DC, et al: Surgical therapy forthyroid carcinoma: a review of 1249 solitary thyroid nodules.Surgery 104:940–946, 1988.
84. Van Nguyen K, Dilawari RA: Predictive value of AMESscoring system in selection of extent of surgery in well dif-ferentiated carcinoma of thyroid. Am Surg 61:151–155, 1995.
85. Shah JP, Loree TR, Dharker D, Strong EW: Lobectomy ver-sus total thyroidectomy for differentiated carcinoma of thethyroid: a matched-pair analysis. Am J Surg 166:331–335,1993.
86. Wax MK, Briant TD: Completion thyroidectomy in the man-agement of well-differentiated thyroid carcinoma. Otolaryn-gol Head Neck Surg 107:63–68, 1992.
87. Loh KC: Familial nonmedullary thyroid carcinoma: a meta-review of case series. Thyroid 7:107–113, 1997.
88. Lerch H, Schober O, Kuwert T, Saur HB: Survival of differ-entiated thyroid carcinoma studied in 500 patients. J ClinOncol 15:2067–2075, 1997.
89. Pilotti S, Collini P, Mariani L, et al: Insular carcinoma: adistinct de novo entity among follicular carcinomas of thethyroid gland. Am J Surg Pathol 21:1466–1473, 1997.
90. Molberg K, Albores-Saavedra J: Hyalinizing trabecular carci-noma of the thyroid gland. Hum Pathol 25:192–197, 1994.
91. Gonzalez-Campora R, Fuentes-Vaamonde E, Hevia-Vazquez
A, et al: Hyalinizing trabecular carcinoma of the thyroidgland: report of two cases of follicular cell thyroid carcinomawith hyalinizing trabecular pattern. Ultrastruct Pathol 22:39–46, 1998.
92. McCluggage WG, Sloan JM: Hyalinizing trabecular carci-noma of thyroid gland. Histopathology 28:357–362, 1996.
93. Ishimaru Y, Fukuda S, Kurano R, et al: Follicular thyroidcarcinoma with clear cell change showing unusual ultra-structural features. Am J Surg Pathol 12:240–246, 1988.
94. LiVolsi VA: Current concepts in follicular tumors of the thy-roid. Monogr Pathol 35:118–137, 1993.
95. Gosain AK, Clark OH: Hurthle cell neoplasms. Malignantpotential. Arch Surg 119:515–519, 1984.
96. Watson RG, Brennan MD, Goellner JR, et al: InvasiveHurthle cell carcinoma of the thyroid: natural history andmanagement. Mayo Clin Proc 59:851–855, 1984.
97. Evans HL: Follicular neoplasms of the thyroid. A study of 44cases followed for a minimum of 10 years, with emphasis ondifferential diagnosis. Cancer 54:535–540, 1984.
98. Bronner MP, LiVolsi VA: Oxyphilic (Askanazy/Hurthle cell)tumors of the thyroid: microscopic features predict biologicbehavior. Surg Pathol 1:137–150, 1988.
99. Baloch ZW, LiVolsi VA: Intravascular Kaposi’s-like spindlecell proliferation of the capsular vessels of follicular-derivedthyroid carcinomas. Mod Pathol 11:995–998, 1998.
100. Carcangiu ML, Bianchi S, Savino D, et al: Follicular Hurthlecell tumors of the thyroid gland. Cancer 68:1944–1953, 1991.
101. Chan JK, Tang SK, Tsang WY, et al: Histologic changes in-duced by fine-needle aspiration. Adv Anat Pathol 3:71–90,1996.
102. Segev DL, Saji M, Phillips GS, et al: Polymerase chain reac-tion–based microsatellite polymorphism analysis of follicularand Hurthle cell neoplasms of the thyroid. J Clin EndocrinolMetab 83:2036–2042, 1998.
103. Chen H, Nicol TL, Zeiger MA, et al: Hurthle cell neoplasmsof the thyroid: are there factors predictive of malignancy?Ann Surg 227:542–546, 1998.
104. Kini SR, Miller JM: Infarction of thyroid neoplasms followingaspiration biopsy (abstract). Acta Cytol 30:591, 1986.
105. Jones JD, Pittman DL, Sandes LR: Necrosis of thyroid nod-ules after fine needle aspiration. Acta Cytol 29:29–31, 1985.
106. LiVolsi VA, Merino MJ: Worrisome histologic alterations fol-lowing fine-needle aspiration of the thyroid (WHAFFT).Pathol Annu 29:99–120, 1994.
107. Flint A, Lloyd RV: Hurthle-cell neoplasms of the thyroidgland. Pathol Annu 25:37–52, 1990.
108. Thompson NW, Dunn EL, Batsakis JG, Nishiyama RH:Hurthle cell lesions of the thyroid gland. Surg Gynecol Ob-stet 139:555–560, 1974.
109. Gundry SR, Burney RE, Thompson NW, Lloyd R: Total thy-roidectomy for Hurthle cell neoplasm of the thyroid. ArchSurg 118:529–532, 1983.
110. Miller RH, Estrada R, Sneed WF, Mace ML: Hurthle celltumors of the thyroid gland. Laryngoscope 93:884–888, 1983.
111. Jorda M, Gonzalez-Campora R, Mora J, et al: Prognosticfactors in follicular carcinoma of the thyroid. Arch PatholLab Med 117:631–635, 1993.
112. Rosen IB, Luk S, Katz I: Hurthle cell tumor behavior: di-lemma and resolution. Surgery 98:777–783, 1985.
113. Heppe H, Armin A, Calandra DB, et al: Hurthle cell tumorsof the thyroid gland. Surgery 98:1162–1165, 1985.
114. Arganini M, Behar R, Wu TC, et al: Hurthle cell tumors: atwenty-five-year experience. Surgery 100:1108–1115, 1986.
115. Caplan RH, Abellera RM, Kisken WA: Hurthle cell tumorsof the thyroid gland. A clinicopathologic review and long-term follow-up. JAMA 251:3114–3117, 1984.
116. Gonzalez-Campora R, Herrero-Zapatero A, Lerma E, et al:Hurthle cell and mitochondrion-rich cell tumors. A clinico-pathologic study. Cancer 57:1154–1163, 1986.
117. Saull SC, Kimmelman CP: Hurthle cell tumors of the thyroidgland. Otolaryngol Head Neck Surg 93:58–62, 1985.
118. Bondeson L, Bondeson AG, Ljungberg O, Tibblin S: Oxyphiltumors of the thyroid: follow-up of 42 surgical cases. AnnSurg 194:677–680, 1981.
119. Wasvary H, Czako P, Poulik J, Lucas R: Unilateral lobectomy
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 81
for Hurthle cell adenoma. Am Surg 64:729–732, discussion732–733, 1998.
120. Grant CS, Barr D, Goellner JR, Hay ID: Benign Hurthle celltumors of the thyroid: a diagnosis to be trusted? World JSurg 12:488–495, 1988.
121. Erickson LA, Jin L, Goellner JR, et al: Pathologic features,proliferative activity, and cyclin D1 expression in Hurthlecell neoplasms of the thyroid. Mod Pathol 13:186–192, 2000.
122. Tollefsen HR, Shah JP, Huvos AG: Hurthle cell carcinoma ofthe thyroid. Am J Surg 130:390–394, 1975.
123. Shaha AR, Loree TR, Shah JP: Prognostic factors and riskgroup analysis in follicular carcinoma of the thyroid. Surgery118:1131–1136, discussion 1136–1138, 1995.
124. Papotti M, Torchio B, Grassi L, et al: Poorly differentiatedoxyphilic (Hurthle cell) carcinomas of the thyroid. Am J SurgPathol 20:686–694, 1996.
125. Davila RM, Bedrossian CW, Silverberg AB: Immunocyto-chemistry of the thyroid in surgical and cytologic specimens.Arch Pathol Lab Med 112:51–56, 1988.
126. Roque L, Clode A, Belge G, et al: Follicular thyroid carci-noma: chromosome analysis of 19 cases. Genes Chromo-somes Cancer 21:250–255, 1998.
127. Pierotti MA, Bongarzone I, Borello MG, et al: Cytogeneticsand molecular genetics of carcinomas arising from thyroidepithelial follicular cells. Genes Chromosomes Cancer 16:1–14, 1996.
128. Tung WS, Shevlin DW, Kaleem Z, et al: Allelotype of follicu-lar thyroid carcinomas reveals genetic instability consistentwith frequent nondisjunctional chromosomal loss. GenesChromosomes Cancer 19:43–51, 1997.
129. Roque L, Castedo S, Clode A, Soares J: Deletion of 3p25 :pter in a primary follicular thyroid carcinoma and its metas-tasis. Genes Chromosomes Cancer 8:199–203, 1993.
130. Hemmer S, Wasenius VM, Knuutila S, et al: DNAcopy number changes in thyroid carcinoma. Am J Pathol154:1539–1547, 1999.
131. Grebe SK, McIver B, Hay ID, et al: Frequent loss of hetero-zygosity on chromosomes 3p and 17p without VHL or p53mutations suggests involvement of unidentified tumor sup-pressor genes in follicular thyroid carcinoma. J Clin Endocri-nol Metab 82:3684–3691, 1997.
132. Zedenius J, Wallin G, Svensson A, et al: Deletions of thelong arm of chromosome 10 in progression of follicular thy-roid tumors. Hum Genet 97:299–303, 1996.
133. Oyama T, Suzuki T, Hara F, et al: N-ras mutation of thyroidtumor with special reference to the follicular type. Pathol Int45:45–50, 1995.
134. Bouras M, Parvaz P, Berger N, et al: Ha-ras oncogene (codon12) mutation in thyroid carcinogenesis: analysis of 60 benignand malignant thyroid tumors. Ann Biol Clin 53:549–555,1995.
135. Sapi Z, Lukacs G, Sztan M, et al: Contribution of p53 genealterations to development of metastatic forms of follicularthyroid carcinoma. Diagn Mol Pathol 4:256–260, 1995.
135a. Kroll TG, Sarraf P, Pecciarini L, et al: PAX8-PPAR gamma 1fusion oncogene in human thyroid carcinoma. Science 289:1357–1360, 2000.
136. Ghali VS, Jimenez EJ, Garcia RL: Distribution of Leu-7 anti-gen (HNK-1) in thyroid tumors: its usefulness as a diagnos-tic marker for follicular and papillary carcinomas. HumPathol 23:21–25, 1992.
137. De Micco C, Ruf J, Chrestian MA, et al: Immunohistochemi-cal study of thyroid peroxidase in normal, hyperplastic, andneoplastic human thyroid tissues. Cancer 67:3036–3041, 1991.
138. Sack MJ, Astengo-Osuna C, Lin BT, et al: HBME-1 immuno-staining in thyroid fine-needle aspirations: a useful markerin the diagnosis of carcinoma. Mod Pathol 10:668–674, 1997.
139. Miettinen M, Karkkainen P: Differential reactivity of HBME-1 and CD15 antibodies in benign and malignant thyroidtumours. Preferential reactivity with malignant tumours. Vir-chows Arch 429:213–219, 1996.
140. Tuccari G, Barresi G: Tissue polypeptide antigen in thyroidtumours of follicular cell origin: an immunohistochemical re-evaluation for diagnostic purposes. Histopathology 16:377–381, 1990.
141. Kotani T, Asada Y, Aratake Y, et al: Diagnostic usefulness ofdipeptidyl aminopeptidase IV monoclonal antibody in paraf-fin-embedded thyroid follicular tumours. J Pathol 168:41–45,1992.
142. Aratake Y, Kotani T, Tamura K, et al: Dipeptidyl aminopep-tidase IV staining of cytologic preparations to distinguishbenign from malignant thyroid diseases. Am J Clin Pathol96:306–310, 1991.
143. Johnson TL, Lloyd RV, Thor A: Expression of ras oncogenep21 antigen in normal and proliferative thyroid tissues. Am JPathol 127:60–65, 1987.
144. Johnson TL, Lloyd RV, Burney RE, Thompson NW: Hurthlecell thyroid tumors. An immunohistochemical study. Cancer59:107–112, 1987.
145. Mizukami Y, Nonomura A, Hashimoto T, et al: Immunohis-tochemical demonstration of epidermal growth factor andc-myc oncogene product in normal, benign and malignantthyroid tissues. Histopathology 18:11–18, 1991.
146. Erickson LA, Jin L, Wollan PC, et al: Expression of p27kip1and Ki-67 in benign and malignant thyroid tumors. ModPathol 11:169–174, 1998.
147. Loy TS, Gelven PL, Mullins D, Diaz-Arias AA: Immunostain-ing for P-glycoprotein in the diagnosis of thyroid carcinomas[see comments]. Mod Pathol 5:200–202, 1992.
148. Chiappetta G, Tallini G, De Biasio MC, et al: Detection ofhigh mobility group I HMGI(Y) protein in the diagnosis ofthyroid tumors: HMGI(Y) expression represents a potentialdiagnostic indicator of carcinoma. Cancer Res 58:4193–4198,1998.
149. Umbricht CB, Saji M, Westra WH, et al: Telomerase activity:a marker to distinguish follicular thyroid adenoma from car-cinoma. Cancer Res 57:2144–2147, 1997.
150. Backdahl M, Wallin G, Akensten U, et al: Nuclear DNAmeasurements in follicular thyroid adenomas. Eur J SurgOncol 15:125–129, 1989.
151. Hruban RH, Huvos AG, Traganos F, et al: Follicular neo-plasms of the thyroid in men older than 50 years of age. ADNA flow cytometric study. Am J Clin Pathol 94:527–532,1990.
152. Schurmann G, Mattfeldt T, Feichter G, et al: Stereology,flow cytometry, and immunohistochemistry of follicularneoplasms of the thyroid gland. Hum Pathol 22:179–184,1991.
153. Oyama T, Vickery AL Jr, Preffer FI, Colvin RB: A compara-tive study of flow cytometry and histopathologic findings inthyroid follicular carcinomas and adenomas. Hum Pathol25:271–275, 1994.
154. Joensuu H, Klemi P, Eerola E: DNA aneuploidy in follicularadenomas of the thyroid gland. Am J Pathol 124:373–376,1986.
155. Schmidt RJ, Wang CA: Encapsulated follicular carcinomaof the thyroid: diagnosis, treatment and results. Surgery100:1068–1076, 1986.
156. Segal K, Arad A, Lubin E, et al: Follicular carcinoma of thethyroid. Head Neck 16:533–538, 1994.
157. Zohar Y, Strauss M: Occult distant metastases of well-differentiated thyroid carcinoma. Head Neck 16:438–442,1994.
158. Marcocci C, Pacini F, Eliseri R, et al: Clinical and biologicbehavior of bone metastasis from differentiated thyroid car-cinoma. Surgery 106:960–966, 1989.
159. Goldstein NS, Czako P, Neill JS: Metastatic minimally inva-sive (encapsulated) follicular and Hurthle cell thyroid carci-noma: a study of 34 patients. Mod Pathol 13:123–130, 2000.
160. von Wasielewski R, Rhein A, Werner M, et al: Immunohisto-chemical detection of E-cadherin in differentiated thyroidcarcinomas correlates with clinical outcome. Cancer Res57:2501–2507, 1997.
161. Joensuu H, Klemi P, Eerola E, Tuominen J: Influence ofcellular DNA content on survival in differentiated thyroidcancer. Cancer 58:2462–2467, 1986.
162. Beaugie JM, Brown CL, Doniach I, Richardson JE: Primarymalignant tumours of the thyroid: the relationship betweenhistological classification and clinical behaviour. Br J Surg63:173–181, 1976.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

82 Endocrine System
163. Hirabayashi RN, Lindsay S: Carcinoma of the thyroid gland:a statistical study of 390 patients. J Clin Endocrinol Metab21:1596–1610, 1961.
164. McConahey WM, Hay ID, Woolner LB, et al: Papillary thy-roid cancer treated at the Mayo Clinic, 1946 through 1970:initial manifestations, pathologic findings, therapy, and out-come. Mayo Clin Proc 61:978–996, 1986.
165. Meissner WA, Adler A: Papillary carcinoma of the thyroid, astudy of the pattern in 226 patients. Arch Pathol 66:518–525,1958.
166. Verge J, Guixa J, Alejo M, et al: Cervical cystic lymph nodemetastasis as first manifestation of occult papillary thyroidcarcinoma: report of seven cases. Head Neck 21:370–374,1999.
167. al-Talib RK, Wilkins BS, Theaker JM: Cystic metastasis ofpapillary carcinoma of the thyroid—an unusual presenta-tion. Histopathology 20:176–178, 1992.
168. Hedinger C, Sobin L: Histological Typing of Thyroid Tu-mors. Geneva, World Health Organization, 1974.
169. Hedinger C, Williams ED, Sobin LH: The WHO histologicalclassification of thyroid tumors: a commentary on the secondedition. Cancer 63:908–911, 1989.
170. Carcangiu ML, Zampi G, Rosai J: Papillary thyroid carci-noma: a study of its many morphologic expressions andclinical correlates. Pathol Annu 20:1–44, 1985.
171. Chan JK: Papillary carcinoma of thyroid: classical and vari-ants. Histol Histopathol 5:241–257, 1990.
172. Rosai J, Carcangiu ML: Pitfalls in the diagnosis of thyroidneoplasms. Pathol Res Pract 182:169–179, 1987.
173. Bruno J, Ciancia EM, Pingitore R: Thyroid papillary adeno-carcinoma; lipomatous-type. Virchows Arch A Pathol AnatHistopathol 414:371–373, 1989.
174. Vestfrid MA: Papillary carcinoma of the thyroid gland withlipomatous stroma: report of a peculiar histological type ofthyroid tumour. Histopathology 10:97–100, 1986.
175. Chan JK, Loo KT: Cribriform variant of papillary thyroidcarcinoma. Arch Pathol Lab Med 114:622–624, 1990.
176. Guiter GE, DeLellis RA: Multinucleate giant cells in papillarythyroid carcinoma. A morphologic and immunohistochemi-cal study. Am J Clin Pathol 106:765–768, 1996.
177. Isarangkul W: Dense fibrosis. Another diagnostic criterionfor papillary thyroid carcinoma. Arch Pathol Lab Med117:645–646, 1993.
178. Yamashita H, Noguchi S, Murakami N, et al: DNA ploidyand stromal bone formation as prognostic indicators of thy-roid papillary carcinoma in aged patients: a retrospectivestudy. Acta Pathol Jpn 43:22–27, 1993.
179. Johannessen JV, Sobrinho-Simoes M: The origin and signifi-cance of thyroid psammoma bodies. Lab Invest 43:287–296,1980.
180. Vickery AL, Carcangiu ML, Johannessen JV: Papillary carci-noma. Semin Diagn Pathol 2:90–100, 1985.
181. Chan JK, Saw D: The grooved nucleus. A useful diagnosticcriterion of papillary carcinoma of the thyroid. Am J SurgPathol 10:672–679, 1986.
182. Glant MD, Berger EK, Davey DD: Intranuclear cytoplasmicinclusions in aspirates of follicular neoplasms of the thyroid.A report of two cases. Acta Cytol 28:576–580, 1984.
183. Oyama T: A histopathological, immunohistochemical and ul-trastructural study of intranuclear cytoplasmic inclusions inthyroid papillary carcinoma. Virchows Arch A Pathol AnatHistopathol 414:91–104, 1989.
184. Scopa CD, Melachrinou M, Saradopoulou C, Merino MJ: Thesignificance of the grooved nucleus in thyroid lesions. ModPathol 6:691–694, 1993.
185. Hazard JB: Nomenclature of thyroid tumors. In Young S,Inman DR (eds): Thyroid Neoplasia. London, AcademicPress, 1968, pp 3–37.
186. Dickersin GR, Vickery AL Jr, Smith SB: Papillary carcinomaof the thyroid, oxyphil cell type, “clear cell” variant: a light-and electron-microscopic study. Am J Surg Pathol 4:501–509,1980.
187. Variakojis D, Getz ML, Paloyan E, Straus FH: Papillary clearcell carcinoma of the thyroid gland. Hum Pathol 6:384–390,1975.
188. Chan JK, Tse CC: Mucin production in metastatic papillarycarcinoma of the thyroid. Hum Pathol 19:195–200, 1988.
189. Mlynek ML, Richter HJ, Leder LD: Mucin in carcinomas ofthe thyroid. Cancer 56:2647–2650, 1985.
190. Chen KT, Rosai J: Follicular variant of thyroid papillary car-cinoma: a clinicopathologic study of six cases. Am J SurgPathol 1:123–130, 1977.
191. Rosai J, Zampi G, Carcangiu ML: Papillary carcinoma of thethyroid. A discussion of its several morphologic expressions,with particular emphasis on the follicular variant. Am J SurgPathol 7:809–817, 1983.
192. Carcangiu ML, Zampi G, Pupi A, et al: Papillary carcinomaof the thyroid. A clinicopathologic study of 241 cases treatedat the University of Florence, Italy. Cancer 55:805–828,1985.
193. Franssila KO: Is the differentiation between papillary andfollicular thyroid carcinoma valid? Cancer 32:853–864, 1973.
194. Moreno A, Rodriguez JM, Sola J, et al: Encapsulated papil-lary neoplasm of the thyroid: retrospective clinicopathologi-cal study with long term follow up. Eur J Surg 162:177–180,1996.
195. Vickery AL Jr: Thyroid papillary carcinoma. Pathologicaland philosophical controversies. Am J Surg Pathol 7:797–807, 1983.
196. Evans HL: Encapsulated papillary neoplasms of the thyroid.A study of 14 cases followed for a minimum of 10 years.Am J Surg Pathol 11:592–597, 1987.
197. Chan JK, Carcangiu ML, Rosai J: Papillary carcinoma of thy-roid with exuberant nodular fasciitis– like stroma. Report ofthree cases. Am J Clin Pathol 95:309–314, 1991.
198. Michal M, Chlumska A, Fakan F: Papillary carcinoma ofthyroid with exuberant nodular fasciitis– like stroma. Histo-pathology 21:577–579, 1992.
199. Mizukami Y, Nonomura A, Matsubara F, et al: Papillarycarcinoma of the thyroid gland with fibromatosis-likestroma. Histopathology 20:355–357, 1992.
200. Terayama K, Toda S, Yonemitsu N, et al: Papillary carci-noma of the thyroid with exuberant nodular fasciitis– likestroma. Virchows Arch 431:291–295, 1997.
201. Acosta J, Rodriguez JM, Sola J, et al: Nodular fasciitis–typepapillary thyroid carcinoma. Presentation of a new case. EurJ Surg Oncol 24:80–81, 1998.
202. Mizukami Y, Kurumaya H, Kitagawa T, et al: Papillary car-cinoma of the thyroid gland with fibromatosis-like stroma: acase report and review of the literature. Mod Pathol 8:366–370, 1995.
203. Chan JK, Tsui MS, Tse CH: Diffuse sclerosing variant ofpapillary carcinoma of the thyroid: a histological and immu-nohistochemical study of three cases. Histopathology 11:191–201, 1987.
204. Hayashi Y, Sasao T, Takeichi N, et al: Diffuse sclerosingvariant of papillary carcinoma of the thyroid. A histopatho-logical study of four cases. Acta Pathol Jpn 40:193–198, 1990.
205. Fujimoto Y, Obara T, Ito Y, et al: Diffuse sclerosing variantof papillary carcinoma of the thyroid. Clinical importance,surgical treatment, and follow-up study. Cancer 66:2306–2312, 1990.
206. Albareda M, Puig-Domingo M, Wengrowicz S, et al: Clinicalforms of presentation and evolution of diffuse sclerosingvariant of papillary carcinoma and insular variant of follicu-lar carcinoma of the thyroid. Thyroid 8:385–391, 1998.
207. Carcangiu ML, Bianchi S: Diffuse sclerosing variant of papil-lary thyroid carcinoma. Clinicopathologic study of 15 cases[see comments]. Am J Surg Pathol 13:1041–1049, 1989.
208. Carcangiu ML, Bianchi S, Rosai J: Diffuse sclerosing papil-lary carcinoma: report of 8 cases of a distinctive variant ofthyroid malignancy (abstract). Lab Invest 56:10A, 1987.
209. Soares J, Limbert E, Sobrinho-Simoes M: Diffuse sclerosingvariant of papillary thyroid carcinoma. A clinicopathologicstudy of 10 cases. Pathol Res Pract 185:200–206, 1989.
210. Schroder S, Bay V, Dumke K, et al: Diffuse sclerosing variantof papillary thyroid carcinoma. S-100 protein immunocyto-chemistry and prognosis. Virchows Arch A Pathol Anat His-topathol 416:367–371, 1990.
211. Gomez-Morales M, Aneiros J, Alvaro T, Navarro N: Langer-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 83
hans’ cells and prognosis of thyroid carcinoma (letter). Am JClin Pathol 91:628–629, 1989.
212. Gomez-Morales M, Alvaro T, Munoz M, et al: Diffuse scle-rosing papillary carcinoma of the thyroid gland: immunohis-tochemical analysis of the local host immune response. His-topathology 18:427–433, 1991.
213. Sobrinho-Simoes M, Soares J, Carneiro F: Diffuse follicularvariant of papillary carcinoma of the thyroid: report of eightcases of a distinct aggressive type of thyroid tumor. SurgPathol 3:189–203, 1990.
214. Mizukami Y, Nonomura A, Michigishi T, et al: Diffuse follic-ular variant of papillary carcinoma of the thyroid. Histopa-thology 27:575–577, 1995.
215. Hawk WA, Hazard JB: The many appearances of papillarycarcinoma of the thyroid. Cleve Clin Q 43:207–215, 1976.
216. Johnson TL, Lloyd RV, Thompson NW, et al: Prognosticimplications of the tall cell variant of papillary thyroid carci-noma. Am J Surg Pathol 12:22–27, 1988.
217. Ostrowski ML, Merino MJ: Tall cell variant of papillary thy-roid carcinoma: a reassessment and immunohistochemicalstudy with comparison to the usual type of papillary carci-noma of the thyroid. Am J Surg Pathol 20:964–974, 1996.
218. Ruter A, Dreifus J, Jones M, et al: Overexpression of p53in tall cell variants of papillary thyroid carcinoma. Surgery120:1046–1050, 1996.
219. Apel RL, Asa SL, LiVolsi VA: Papillary Hurthle cell carci-noma with lymphocytic stroma. “Warthin-like tumor” of thethyroid [see comments]. Am J Surg Pathol 19:810–814, 1995.
220. Vera-Sempere FJ, Prieto M, Camanas A: Warthin-like tumorof the thyroid: a papillary carcinoma with mitochondrion-rich cells and abundant lymphoid stroma. A case report.Pathol Res Pract 194:341–347, 1998.
221. Ozaki O, Ito K, Mimura T, et al: Papillary carcinoma of thethyroid. Tall-cell variant with extensive lymphocyte infiltra-tion. Am J Surg Pathol 20:695–698, 1996.
221a. Baloch ZW, LiVolsi VA: Warthin-like papillary carcinomaof the thyroid. Arch Pathol Lab Med 124:1192–1195, 2000.
222. Nakamura T, Moriyama S, Nariya S, et al: Macrofollicularvariant of papillary thyroid carcinoma. Pathol Int 48:467–470, 1998.
223. Albores-Saavedra J, Gould E, Vardaman C, Vuitch F: Themacrofollicular variant of papillary thyroid carcinoma: astudy of 17 cases. Hum Pathol 22:1195–1205, 1991.
224. Albores-Saavedra J, Housini I, Vuitch F, Snyder WH 3rd:Macrofollicular variant of papillary thyroid carcinoma withminor insular component. Cancer 80:1110–1116, 1997.
225. Sobrinho-Simoes MA, Nesland JM, Holm R, et al: Hurthlecell and mitochondrion-rich papillary carcinomas of the thy-roid gland: an ultrastructural and immunocytochemicalstudy. Ultrastruct Pathol 8:131–142, 1985.
226. Tscholl-Ducommun J, Hedinger CE: Papillary thyroid carci-nomas. Morphology and prognosis. Virchows Arch PatholAnat 396:19–39, 1982.
227. Beckner ME, Heffess CS, Oertel JE: Oxyphilic papillary thy-roid carcinomas. Am J Clin Pathol 103:280–287, 1995.
228. Berho M, Suster S: The oncocytic variant of papillary carci-noma of the thyroid: a clinicopathologic study of 15 cases.Hum Pathol 28:47–53, 1997.
229. Katoh R, Sakamoto A, Kasai N, Yagawa K: Squamous differ-entiation in thyroid carcinoma. With special reference to his-togenesis of squamous cell carcinoma of the thyroid. ActaPathol Jpn 39:306–312, 1989.
230. Cameselle-Teijeiro J, Chan JK: Cribriform-morular variant ofpapillary carcinoma: a distinctive variant representing thesporadic counterpart of familial adenomatous polyposis–as-sociated thyroid carcinoma? Mod Pathol 12:400–411, 1999.
231. Yamashita T, Hosoda Y, Kameyama K, et al: Peculiar nuclearclearing composed of microfilaments in papillary carcinomaof the thyroid. Cancer 70:2923–2928, 1992.
232. Harach HR, Williams GT, Williams ED: Familial adenoma-tous polyposis associated thyroid carcinoma: a distinct typeof follicular cell neoplasm. Histopathology 25:549–561, 1994.
233. Cetta F, Toti P, Petracci M, et al: Thyroid carcinoma associ-ated with familial adenomatous polyposis. Histopathology31:231–236, 1997.
234. Perrier ND, van Heerden JA, Goellner JR, et al: Thyroidcancer in patients with familial adenomatous polyposis.World J Surg 22:738–742, discussion 743, 1998.
235. Soravia C, Sugg SL, Berk T, et al: Familial adenomatouspolyposis–associated thyroid cancer: a clinical, pathological,and molecular genetics study. Am J Pathol 154:127–135,1999.
236. Cetta F, Pelizzo MR, Curia MC, Barbarisi A: Genetics andclinicopathological findings in thyroid carcinomas associatedwith familial adenomatous polyposis. Am J Pathol 155:7–9,1999.
237. Mizukami Y, Noguchi M, Michigishi T, et al: Papillary thy-roid carcinoma in Kanazawa, Japan: prognostic significanceof histological subtypes. Histopathology 20:243–250, 1992.
238. Carcangiu ML, Steeper T, Zampi G, Rosai J: Anaplastic thy-roid carcinoma. A study of 70 cases. Am J Clin Pathol83:135–158, 1985.
239. Kawahara E, Ooi A, Oda Y, et al: Papillary carcinoma of thethyroid gland with anaplastic transformation in the meta-static foci. An immunohistochemical study. Acta Pathol Jpn36:921–927, 1986.
240. D’Antonio A, De Chiara A, Santoro M, et al: Warthin-liketumour of the thyroid gland: RET/PTC expression indicatesit is a variant of papillary carcinoma. Histopathology 36:493–498, 2000.
241. Ito J, Noguchi S, Murakami N, Noguchi A: Factors affectingthe prognosis of patients with carcinoma of the thyroid. SurgGynecol Obstet 150:539–544, 1980.
242. Chen KT: Minute (less than 1 mm) occult papillary thyroidcarcinoma with metastasis (letter). Am J Clin Pathol 91:746,1989.
243. Kasai N, Sakamoto A: New subgrouping of small thyroidcarcinomas. Cancer 60:1767–1770, 1987.
244. Laskin WB, James LP: Occult papillary carcinoma of thethyroid with pulmonary metastases. Hum Pathol 14:83–85,1983.
245. Sampson RJ, Key CR, Buncher CR, Iijima S: Smallest formsof papillary carcinoma of the thyroid. A study of 141 micro-carcinomas less than 0.1 cm in greatest dimension. ArchPathol 91:334–339, 1971.
246. Strate SM, Lee EL, Childers JH: Occult papillary carcinomaof the thyroid with distant metastases. Cancer 54:1093–1100,1984.
247. Sugitani I, Yanagisawa A, Shimizu A, et al: Clinicopathologicand immunohistochemical studies of papillary thyroid mi-crocarcinoma presenting with cervical lymphadenopathy.World J Surg 22:731–737, 1998.
248. Fukunaga FH, Yatani R: Geographic pathology of occult thy-roid carcinomas. Cancer 36:1095–1099, 1975.
249. Harach HR, Franssila KO, Wasenius VM: Occult papillarycarcinoma of the thyroid. A “normal” finding in Finland. Asystematic autopsy study. Cancer 56:531–538, 1985.
250. Sampson RJ: Prevalence and significance of occult thyroidcancer. In DeGroot LJ, Frohman LA, Kaplan DL (eds): Radia-tion-Associated Thyroid Carcinoma. New York, Grune &Stratton, 1977, pp 137–153.
251. Arellano L, Ibarra A: Occult carcinoma of the thyroid gland.Pathol Res Pract 179:88–91, 1984.
252. Bondeson L, Ljungberg O: Occult thyroid carcinoma at au-topsy in Malmo, Sweden. Cancer 47:319–323, 1981.
253. Fukunaga FH, Lockett LJ: Thyroid carcinoma in the Japanesein Hawaii. Arch Pathol 92:6–13, 1971.
254. Lang W, Borrusch H, Bauer L: Occult carcinomas of thethyroid. Evaluation of 1,020 sequential autopsies. Am J ClinPathol 90:72–76, 1988.
255. Ludwig G, Nishiyama RH: The prevalence of occult papil-lary thyroid carcinoma in 100 consecutive autopsies in anAmerican population. Lab Invest 34:320–321, 1976.
256. Ottino A, Pianzola HM, Castelletto RH: Occult papillary thy-roid carcinoma at autopsy in La Plata, Argentina. Cancer64:547–551, 1989.
257. Sobrinho-Simoes MA, Sambade MC, Goncalves V: Latentthyroid carcinoma at autopsy: a study from Oporto, Portu-gal. Cancer 43:1702–1706, 1979.
258. Mills SE, Allen MS Jr: Congenital occult papillary carcinomaof the thyroid gland. Hum Pathol 17:1179–1181, 1986.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved
84 Endocrine System
259. Komorowski RA, Hanson GA: Occult thyroid pathology inthe young adult: an autopsy study of 138 patients withoutclinical thyroid disease. Hum Pathol 19:689–696, 1988.
260. Franssila KO, Harach HR: Occult papillary carcinoma of thethyroid in children and young adults. A systemic autopsystudy in Finland. Cancer 58:715–719, 1986.
261. Rassel H, Thompson LD, Heffess CS: A rationale for con-servative management of microscopic papillary carcinoma ofthe thyroid gland: a clinicopathologic correlation of 90 cases.Eur Arch Otorhinolaryngol 255:462–267, 1998.
262. LaGuette J, Matias-Guiu X, Rosai J: Thyroid paraganglioma:a clinicopathologic and immunohistochemical study of threecases. Am J Surg Pathol 21:748–753, 1997.
263. Schroder S, Pfannschmidt N, Bocker W, et al: Histopatho-logic types and clinical behaviour of occult papillary carci-noma of the thyroid. Pathol Res Pract 179:81–87, 1984.
264. Fonseca E, Nesland JM, Hoie J, Sobrinho-Simoes M: Patternof expression of intermediate cytokeratin filaments in thethyroid gland: an immunohistochemical study of simpleand stratified epithelial-type cytokeratins. Virchows Arch430:239–245, 1997.
265. Raphael SJ, McKeown-Eyssen G, Asa SL: High-molecular-weight cytokeratin and cytokeratin-19 in the diagnosis ofthyroid tumors. Mod Pathol 7:295–300, 1994.
266. Raphael SJ, Apel RL, Asa SL: Brief report: detection of high-molecular-weight cytokeratins in neoplastic and non-neoplas-tic thyroid tumors using microwave antigen retrieval. ModPathol 8:870–872, 1995.
267. Schelfhout LJ, Van Muijen GN, Fleuren GJ: Expression ofkeratin 19 distinguishes papillary thyroid carcinoma fromfollicular carcinomas and follicular thyroid adenoma. Am JClin Pathol 92:654–658, 1989.
268. Pierotti MA, Vigneri P, Bongarzone I: Rearrangements ofRET and NTRK1 tyrosine kinase receptors in papillary thy-roid carcinomas. Recent Results Cancer Res 154:237–247,1998.
269. Smanik PA, Furminger TL, Mazzaferri EL, Jhiang SM: Break-point characterization of the ret/PTC oncogene in humanpapillary thyroid carcinoma. Hum Mol Genet 4:2313–2318,1995.
270. Santoro M, Carlomagno F, Hay ID, et al: Ret oncogene acti-vation in human thyroid neoplasms is restricted to the papil-lary cancer subtype. J Clin Invest 89:1517–1522, 1992.
271. Sozzi G, Bongarzone I, Miozzo M, et al: A t(10;17) transloca-tion creates the RET/PTC2 chimeric transforming sequencein papillary thyroid carcinoma. Genes Chromosomes Cancer9:244–250, 1994.
272. Minoletti F, Butti MG, Coronelli S, et al: The two genesgenerating RET/PTC3 are localized in chromosomal band10q11.2. Genes Chromosomes Cancer 11:51–57, 1994.
273. Fugazzola L, Pierotti MA, Vigano E, et al: Molecular andbiochemical analysis of RET/PTC4, a novel oncogenic rear-rangement between RET and ELE1 genes, in a post-Cherno-byl papillary thyroid cancer. Oncogene 13:1093–1097, 1996.
274. Ponder BAJ: Multiple endocrine neoplasia type 2. In Vogel-stein B, Kinzler KW (eds): The Genetic Basis of Human Can-cer. New York, McGraw-Hill, 1998, pp 475–487.
275. Klugbauer S, Demidchik EP, Lengfelder E, Rabes HM: Mo-lecular analysis of new subtypes of ELE/RET rearrange-ments, their reciprocal transcripts and breakpoints in papil-lary thyroid carcinomas of children after Chernobyl.Oncogene 16:671–675, 1998.
276. Klugbauer S, Demidchik EP, Lengfelder E, Rabes HM: Detec-tion of a novel type of RET rearrangement (PTC5) in thyroidcarcinomas after Chernobyl and analysis of the involvedRET-fused gene RFG5. Cancer Res 58:198–203, 1998.
277. Bongarzone I, Butti MG, Fugazzola L, et al: Comparison ofthe breakpoint regions of ELE1 and RET genes involved inthe generation of RET/PTC3 oncogene in sporadic and inradiation-associated papillary thyroid carcinomas. Genomics42:252–259, 1997.
278. Williams GH, Rooney S, Thomas GA, et al: RET activation inadult and childhood papillary thyroid carcinoma using areverse transcriptase-n-polymerase chain reaction approachon archival-nested material. Br J Cancer 74:585–589, 1996.
279. Lam AK, Montone KT, Nolan KA, Livolsi VA: Ret oncogeneactivation in papillary thyroid carcinoma: prevalence andimplication on the histological parameters. Hum Pathol29:565–568, 1998.
280. Delvincourt C, Patey M, Flament JB, et al: Ret and trk proto-oncogene activation in thyroid papillary carcinomas inFrench patients from the Champagne-Ardenne region. ClinBiochem 29:267–271, 1996.
281. Kitamura Y, Minobe K, Nakata T, et al: Ret/PTC3 is themost frequent form of gene rearrangement in papillary thy-roid carcinomas in Japan. J Hum Genet 44:96–102, 1999.
282. Santoro M, Dathan NA, Berlingieri MT, et al: Molecularcharacterization of RET/PTC3; a novel rearranged version ofthe RET proto-oncogene in a human thyroid papillary carci-noma. Oncogene 9:509–516, 1994.
283. Lee CH, Hsu LS, Chi CW, et al: High frequency of rear-rangement of the RET protooncogene (RET/PTC) in Chinesepapillary thyroid carcinomas. J Clin Endocrinol Metab83:1629–1632, 1998.
284. Bongarzone I, Butti MG, Coronelli S, et al: Frequent activa-tion of ret protooncogene by fusion with a new activatinggene in papillary thyroid carcinomas. Cancer Res 54:2979–2985, 1994.
285. Bongarzone I, Fugazzola L, Vigneri P, et al: Age-related acti-vation of the tyrosine kinase receptor protooncogenes RETand NTRK1 in papillary thyroid carcinoma. J Clin Endocri-nol Metab 81:2006–2009, 1996.
286. Zou M, Shi Y, Farid NR: Low rate of ret proto-oncogeneactivation (PTC/retTPC) in papillary thyroid carcinomasfrom Saudi Arabia. Cancer 73:176–180, 1994.
287. Tallini G, Ghossein RA, Emanuel J, et al: Detection of thyro-globulin, thyroid peroxidase, and RET/PTC1 mRNA tran-scripts in the peripheral blood of patients with thyroid dis-ease. J Clin Oncol 16:1158–1166, 1998.
288. Mayr B, Potter E, Goretzki P, et al: Expression of Ret/PTC1,-2, -3, -delta3 and -4 in German papillary thyroid carcinoma.Br J Cancer 77:903–906, 1998.
289. Mayr B, Potter E, Goretzki P, et al: Expression of wild-typeret, ret/PTC and ret/PTC variants in papillary thyroid carci-noma in Germany. Langenbecks Arch Surg 384:54–59, 1999.
290. Soares P, Fonseca E, Wynford-Thomas D, Sobrinho-SimoesM: Sporadic ret-rearranged papillary carcinoma of the thy-roid: a subset of slow growing, less aggressive thyroid neo-plasms? J Pathol 185:71–78, 1998.
291. Nikiforov YE, Rowland JM, Bove KE, et al: Distinct patternof ret oncogene rearrangements in morphological variants ofradiation-induced and sporadic thyroid papillary carcinomasin children. Cancer Res 57:1690–1694, 1997.
292. Sugg SL, Ezzat S, Zheng L, et al: Oncogene profile of papil-lary thyroid carcinoma. Surgery 125:46–52, 1999.
293. Klugbauer S, Lengfelder E, Demidchik EP, Rabes HM: Highprevalence of RET rearrangement in thyroid tumors of chil-dren from Belarus after the Chernobyl reactor accident. On-cogene 11:2459–2467, 1995.
294. Fugazzola L, Pilotti S, Pinchera A, et al: Oncogenic rear-rangements of the RET proto-oncogene in papillary thyroidcarcinomas from children exposed to the Chernobyl nuclearaccident. Cancer Res 55:5617–5620, 1995.
295. Pisarchik AV, Ermak G, Demidchik EP, et al: Low preva-lence of the ret/PTC3r1 rearrangement in a series of papil-lary thyroid carcinomas presenting in Belarus ten years post-Chernobyl. Thyroid 8:1003–1008, 1998.
296. Bounacer A, Wicker R, Schlumberger M, et al: Oncogenicrearrangements of the ret proto-oncogene in thyroid tumorsinduced after exposure to ionizing radiation. Biochimie79:619–623, 1997.
297. Kopp P, Jameson JL: Thyroid disorders. In Jameson JL (ed):Principles of Molecular Medicine. Totowa, NJ, HumanaPress, 1998, pp 459–473.
298. Bongarzone I, Vigneri P, Mariani L, et al: RET/NTRK1 rear-rangements in thyroid gland tumors of the papillary carci-noma family: correlation with clinicopathological features.Clin Cancer Res 4:223–228, 1998.
299. Beimfohr C, Klugbauer S, Demidchik EP, et al: NTRK1 rear-rangement in papillary thyroid carcinomas of children after
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved
Thyroid and Parathyroid 85
the Chernobyl reactor accident. Int J Cancer 80:842–847,1999.
300. Chan JKC, Tsang WYW: Endocrine malignancies that maymimic benign lesions. Semin Diagn Pathol 12:45–63, 1995.
301. Cheifetz RE, Davis NL, Robinson BW, et al: Differentiationof thyroid neoplasms by evaluating epithelial membrane an-tigen, Leu-7 antigen, epidermal growth factor receptor, andDNA content. Am J Surg 167:531–534, 1994.
302. Viale G, Dell’Orto P, Coggi G, Gambacorta M: Coexpressionof cytokeratins and vimentin in normal and diseased thyroidglands. Lack of diagnostic utility of vimentin immunostain-ing. Am J Surg Pathol 13:1034–1040, 1989.
303. Yamamoto Y, Izumi K, Otsuka H: An immunohistochemicalstudy of epithelial membrane antigen, cytokeratin, and vi-mentin in papillary thyroid carcinoma. Recognition of lethaland favorable prognostic types [see comments]. Cancer70:2326–2333, 1992.
304. Damiani S, Fratamico F, Lapertosa G, et al: Alcian blue andepithelial membrane antigen are useful markers in differenti-ating benign from malignant papillae in thyroid lesions. Vir-chows Arch A Pathol Anat Histopathol 419:131–135, 1991.
305. Lucas SD, Ek B, Rask L, et al: Aberrantly expressed cytoker-atin 1, a tumor-associated autoantigen in papillary thyroidcarcinoma. Int J Cancer 73:171–177, 1997.
306. Miettinen M, Kovatich AJ, Karkkainen P: Keratin subsetsin papillary and follicular thyroid lesions. A paraffin sec-tion analysis with diagnostic implications. Virchows Arch431:407–413, 1997.
307. Tanaka T, Umeki K, Yamamoto I, et al: Immunohistochemi-cal loss of thyroid peroxidase in papillary thyroid carcinoma:strong suppression of peroxidase gene expression. J Pathol179:89–94, 1996.
308. Umeki K, Tanaka T, Yamamoto I, et al: Differential expres-sion of dipeptidyl peptidase IV (CD26) and thyroid peroxi-dase in neoplastic thyroid tissues. Endocr J 43:53–60, 1996.
309. Khan A, Baker SP, Patwardhan NA, Pullman JM: CD57(Leu-7) expression is helpful in diagnosis of the follicularvariant of papillary thyroid carcinoma. Virchows Arch432:427–432, 1998.
310. Loy TS, Darkow GV, Spollen LE, Diaz-Arias AA: Immuno-staining for Leu-7 in the diagnosis of thyroid carcinoma.Arch Pathol Lab Med 118:172–174, 1994.
311. Chhieng DC, Ross JS, McKenna BJ: CD44 immunostaining ofthyroid fine-needle aspirates differentiates thyroid papillarycarcinoma from other lesions with nuclear grooves and in-clusions. Cancer 81:157–162, 1997.
312. Ross JS, del Rosario AD, Sanderson B, Bui HX: Selectiveexpression of CD44 cell-adhesion molecule in thyroid papil-lary carcinoma fine-needle aspirates. Diagn Cytopathol14:287–291, 1996.
313. van Hoeven KH, Kovatich AJ, Miettinen M: Immunocyto-chemical evaluation of HBME-1, CA 19-9, and CD-15 (Leu-M1) in fine-needle aspirates of thyroid nodules. Diagn Cyto-pathol 18:93–97, 1998.
314. Anwar F, Emond MJ, Schmidt RA, et al: Retinoblastomaexpression in thyroid neoplasms. Mod Pathol 13:562–569,2000.
nation of risk groups and outcome of treatment. Arch Surg133:419–425, 1998.
321. Woolner LB, Beahrs OH, Black BM, et al: Thyroid carcinoma:general considerations and follow-up data on 1181 cases. InYoung S, Inman DR (eds): Thyroid Neoplasia. London, Aca-demic Press, 1968, pp 51–76.
322. Tubiana M, Schlumberger M, Rougier P, et al: Long-termresults and prognostic factors in patients with differentiatedthyroid carcinoma. Cancer 55:794–804, 1985.
323. Mazzaferri EL: Papillary thyroid carcinoma: factors influenc-ing prognosis and current therapy. Semin Oncol 14:315–332,1987.
324. Beenken S, Guillamondegui O, Shallenberger R, et al: Prog-nostic factors in patients dying of well-differentiated thyroidcancer. Arch Otolaryngol Head Neck Surg 115:326–330,1989.
325. Shaha AR, Shah JP, Loree TR: Risk group stratification andprognostic factors in papillary carcinoma of thyroid. AnnSurg Oncol 3:534–538, 1996.
326. Salvesen H, Njolstad PR, Akslen LA, et al: Papillary thyroidcarcinoma: a multivariate analysis of prognostic factors in-cluding an evaluation of the p-TNM staging system. Eur JSurg 158:583–589, 1992.
327. Bellantone R, Lombardi CP, Boscherini M, et al: Prognosticfactors in differentiated thyroid carcinoma: a multivariateanalysis of 234 consecutive patients. J Surg Oncol 68:237–241, 1998.
328. Noguchi S, Murakami N, Kawamoto H: Classification ofpapillary cancer of the thyroid based on prognosis. World JSurg 18:552–557, discussion 558, 1994.
329. Kashima K, Yokoyama S, Noguchi S, et al: Chronic thyroidi-tis as a favorable prognostic factor in papillary thyroid carci-noma. Thyroid 8:197–202, 1998.
330. Frauenhoffer CM, Patchefsky AS, Cobanoglu A: Thyroid car-cinoma: a clinical and pathologic study of 125 cases. Cancer43:2414–2421, 1979.
331. Tennvall J, Biorklund A, Moller T, et al: Prognostic factors ofpapillary, follicular and medullary carcinomas of the thyroidgland. Retrospective multivariate analysis of 216 patientswith a median follow-up of 11 years. Acta Radiol Oncol24:17–24, 1985.
332. Tennvall J, Biorklund A, Moller T, et al: Is the EORTC prog-nostic index of thyroid cancer valid in differentiated thyroidcarcinoma? Retrospective multivariate analysis of differenti-ated thyroid carcinoma with long follow-up. Cancer 57:1405–1414, 1986.
333. Rodriguez JM, Moreno A, Parrilla P, et al: Papillary thyroidmicrocarcinoma: clinical study and prognosis. Eur J Surg163:255–259, 1997.
334. Vickery AL Jr, Wang CA, Walker AM: Treatment of in-trathyroidal papillary carcinoma of the thyroid. Cancer60:2587–2595, 1987.
335. McCaffrey TV, Bergstralh EJ, Hay ID: Locally invasive papil-lary thyroid carcinoma: 1940–1990 [see comments]. HeadNeck 16:165–172, 1994.
336. Yasumoto K, Miyagi C, Nakashima T, et al: Papillary andfollicular thyroid carcinoma: the treatment results of 357 pa-tients at the National Kyushu Cancer Centre of Japan. JLaryngol Otol 110:657–662, 1996.
337. Hughes CJ, Shaha AR, Shah JP, Loree TR: Impact of lymphnode metastasis in differentiated carcinoma of the thyroid: amatched-pair analysis. Head Neck 18:127–132, 1996.
338. Scheumann GF, Gimm O, Wegener G, et al: Prognostic signif-icance and surgical management of locoregional lymph nodemetastases in papillary thyroid cancer. World J Surg 18:559–567, discussion 567–568, 1994.
339. Akslen LA, LiVolsi VA: Prognostic significance of histologicgrading compared with subclassification of papillary thyroidcarcinoma [see comments]. Cancer 88:1902–1908, 2000.
340. Pilotti S, Collini P, Manzari A, et al: Poorly differentiatedforms of papillary thyroid carcinoma: distinctive entities ormorphological patterns? Semin Diagn Pathol 12:249–255,1995.
341. Andersen PE, Kinsella J, Loree TR, et al: Differentiated carci-noma of the thyroid with extrathyroidal extension. Am JSurg 170:467–470, 1995.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
315. Gimm O, Rath FW, Dralle H: Pattern of lymph node metas-tases in papillary thyroid carcinoma. Br J Surg 85:252–254,1998.
316. Lindsay A: Papillary thyroid carcinoma revisited. In Hedin-ger CE (ed): Thyroid Cancer. Berlin, Springer-Verlag, 1969,pp 29–32.
317. Cady B, Rossi R: An expanded view of risk-group definitionin differentiated thyroid carcinoma. Surgery 104:947–953,1988.
318. Cady B: Papillary carcinoma of the thyroid gland: treatmentbased on risk group definition. Surg Oncol Clin North Am7:633–644, 1998.
319. Hay ID, Bergstralh EJ, Goellner JR, et al: Predicting outcomein papillary thyroid carcinoma: development of a reliableprognostic scoring system in a cohort of 1779 patients surgi-cally treated at one institution during 1940 through 1989.Surgery 114:1050–1057, discussion 1057–1058, 1993.
320. Sanders LE, Cady B: Differentiated thyroid cancer: reexami-
Copyright � 2003, Elsevier Science (USA). All rights Reserved

86 Endocrine System
342. Sakamoto A, Kasai N, Sugano H: Poorly differentiated carci-noma of the thyroid. A clinicopathologic entity for a high-risk group of papillary and follicular carcinomas. Cancer52:1849–1855, 1983.
343. Akslen LA: Prognostic importance of histologic grading inpapillary thyroid carcinoma. Cancer 72:2680–2685, 1993.
344. Schroder S, Schwarz W, Rehpenning W, et al: Dendritic/Langerhans cells and prognosis in patients with papillarythyroid carcinomas. Immunocytochemical study of 106 thy-roid neoplasms correlated to follow-up data. Am J ClinPathol 89:295–300, 1988.
345. Schroder S, Schwarz W, Rehpenning W, et al: Prognosticsignificance of Leu-M1 immunostaining in papillary carcino-mas of the thyroid gland. Virchows Arch A Pathol AnatHistopathol 411:435–439, 1987.
346. Goldenberg JD, Portugal LG, Wenig BL, et al: Well-differen-tiated thyroid carcinomas: p53 mutation status and micro-vessel density. Head Neck 20:152–158, 1998.
347. Godballe C, Asschenfeldt P, Jorgensen KE, et al: Prognosticfactors in papillary and follicular thyroid carcinomas: p53expression is a significant indicator of prognosis. Laryngo-scope 108:243–249, 1998.
348. Omura K, Nagasato A, Kanehira E, et al: Retinoblastomaprotein and proliferating-cell nuclear antigen expression aspredictors of recurrence in well-differentiated papillary thy-roid carcinoma. J Clin Oncol 15:3458–3463, 1997.
349. Dhar DK, Kubota H, Kotoh T, et al: Tumor vascularity pre-dicts recurrence in differentiated thyroid carcinoma. Am JSurg 176:442–447, 1998.
350. Ishiwata T, Iino Y, Takei H, et al: Tumor angiogenesis as anindependent prognostic indicator in human papillary thyroidcarcinoma. Oncol Rep 5:1343–1348, 1998.
351. Akslen LA, Livolsi VA: Increased angiogenesis in papillarythyroid carcinoma but lack of prognostic importance [seecomments]. Hum Pathol 31:439–442, 2000.
352. Hamming JF, Schelfhout LJ, Cornelisse CJ, et al: Prognosticvalue of nuclear DNA content in papillary and follicularthyroid cancer. World J Surg 12:503–508, 1988.
353. Hara H, Fulton N, Yashiro T, et al: N-ras mutation: an inde-pendent prognostic factor for aggressiveness of papillarythyroid carcinoma. Surgery 116:1010–1016, 1994.
354. Carcangiu ML, Zampi G, Rosai J: Poorly differentiated (“in-sular”) thyroid carcinoma. A reinterpretation of Langhans’“wuchernde Struma.” Am J Surg Pathol 8:655–668, 1984.
355. Papotti M, Botto Micca F, Favero A, et al: Poorly differenti-ated thyroid carcinomas with primordial cell component. Agroup of aggressive lesions sharing insular, trabecular, andsolid patterns. Am J Surg Pathol 17:291–301, 1993.
356. van den Brekel MW, Hekkenberg RJ, Asa SL, et al: Prognos-tic features in tall cell papillary carcinoma and insular thy-roid carcinoma. Laryngoscope 107:254–259, 1997.
357. Tallini G, Garcia-Rostan G, Herrero A, et al: Downregulationof p27KIP1 and Ki67/Mib1 labeling index support the classi-fication of thyroid carcinoma into prognostically relevant cat-egories. Am J Surg Pathol 23:678–685, 1999.
358. Ringel MD, Burman KD, Shmookler BM: Clinical aspects ofmiscellaneous and unusual types of thyroid cancers. In War-tofsky L (ed): Thyroid Cancer, A Comprehensive Guideto Clinical Management. Totowa, NJ, Humana Press, 2000,pp 421–451.
359. Kapp DS, LiVolsi VA, Sanders MM: Anaplastic carcinomafollowing well-differentiated thyroid cancer: etiological con-siderations. Yale J Biol Med 55:521–528, 1982.
360. Flynn SD, Forman BH, Stewart AF, Kinder BK: Poorly differ-entiated (“insular”) carcinoma of the thyroid gland: an ag-gressive subset of differentiated thyroid neoplasms. Surgery104:963–970, 1988.
361. Pietribiasi F, Sapino A, Papotti M, Bussolati G: Cytologicfeatures of poorly differentiated ’insular’ carcinoma of thethyroid, as revealed by fine-needle aspiration biopsy. Am JClin Pathol 94:687–692, 1990.
362. Resnick MB, Schacter P, Finkelstein Y, et al: Immunohisto-chemical analysis of p27/kip1 expression in thyroid carci-noma. Mod Pathol 11:735–739, 1998.
363. Pilotti S, Collini P, Del Bo R, et al: A novel panel of antibod-
ies that segregates immunocytochemically poorly differenti-ated carcinoma from undifferentiated carcinoma of the thy-roid gland. Am J Surg Pathol 18:1054–1064, 1994.
364. Dobashi Y, Sakamoto A, Sugimura H, et al: Overexpressionof p53 as a possible prognostic factor in human thyroidcarcinoma. Am J Surg Pathol 17:375–381, 1993.
365. Manenti G, Pilotti S, Re FC, et al: Selective activation of rasoncogenes in follicular and undifferentiated thyroid carcino-mas. Eur J Cancer 7:987–993, 1994.
366. Lam KY, Lo CY, Chan KW, Wan KY: Insular and anaplasticcarcinoma of the thyroid: a 45-year comparative study at asingle institution and a review of the significance of p53 andp21. Ann Surg 231:329–338, 2000.
367. Johnson MW, Hunnicutt JW, Bilbao JE, et al: Poorly differen-tiated thyroid carcinoma with focal insular pattern: clinico-pathologic correlation (abstract). Am J Clin Pathol 94:497–498, 1990.
368. Sasaki A, Daa T, Kashima K, et al: Insular component as arisk factor of thyroid carcinoma. Pathol Int 46:939–946, 1996.
369. Ashfaq R, Vuitch F, Delgado R, Albores-Saavedra J: Papillaryand follicular thyroid carcinomas with an insular compo-nent. Cancer 73:416–423, 1994.
370. LiVolsi VA, Brooks JJ, Arendash-Durand B: Anaplastic thy-roid tumors. Immunohistology. Am J Clin Pathol 87:434–442,1987.
371. Nishiyama RH, Dunn EL, Thompson NW: Anaplastic spin-dle-cell and giant-cell tumors of the thyroid gland. Cancer30:113–127, 1972.
372. Venkatesh YS, Ordonez NG, Schultz PN, et al: Anaplasticcarcinoma of the thyroid. A clinicopathologic study of 121cases. Cancer 66:321–330, 1990.
373. Rosai J, Saxen EA, Woolner L: Undifferentiated and poorlydifferentiated carcinoma. Semin Diagn Pathol 2:123–126,1985.
374. Aldinger KA, Samaan NA, Ibanez M, Hill CS Jr: Anaplasticcarcinoma of the thyroid: a review of 84 cases of spindle andgiant cell carcinoma of the thyroid. Cancer 41:2267–2275,1978.
375. Spires JR, Schwartz MR, Miller RH: Anaplastic thyroid carci-noma. Association with differentiated thyroid cancer. ArchOtolaryngol Head Neck Surg 114:40–44, 1988.
376. Galera-Davidson H, Bibbo M, Dytch HE, et al: Nuclear DNAin anaplastic thyroid carcinoma with a differentiated compo-nent. Histopathology 11:715–722, 1987.
377. Lo CY, Lam KY, Wan KY: Anaplastic carcinoma of the thy-roid. Am J Surg 177:337–339, 1999.
378. Cibull ML, Gray GF: Ultrastructure of osteoclastoma-like gi-ant cell tumor of thyroid. Am J Surg Pathol 2:401–405, 1978.
379. Silverberg SG, DeGiorgi LS: Osteoclastoma-like giant cell tu-mor of the thyroid. Report of a case with prolonged survivalfollowing partial excision and radiotherapy. Cancer 31:621–625, 1973.
380. Gaffey MJ, Lack EE, Christ ML, Weiss LM: Anaplastic thy-roid carcinoma with osteoclast-like giant cells. A clinicopath-ologic, immunohistochemical, and ultrastructural study. AmJ Surg Pathol 15:160–168, 1991.
381. Wan SK, Chan JK, Tang SK: Paucicellular variant of anaplas-tic thyroid carcinoma. A mimic of Reidel’s thyroiditis. Am JClin Pathol 105:388–393, 1996.
382. Blasius S, Edel G, Grunert J, et al: Anaplastic thyroid carci-noma with osteosarcomatous differentiation. Pathol Res Pract190:507–510, discussion 511–512, 1994.
383. Bakri K, Shimaoka K, Rao U, Tsukada Y: Adenosquamouscell carcinoma of the thyroid after radiotherapy for Hodg-kin’s disease. Cancer 52:465–470, 1983.
384. Harada T, Katagiri M, Tsukayama C, et al: Squamous cellcarcinoma with cyst of the thyroid. J Surg Oncol 42:136–143,1989.
385. Huang TY, Assor D: Primary squamous cell carcinoma ofthe thyroid gland: a report of four cases. Am J Clin Pathol55:93–98, 1971.
386. Huang TY, Lin SG: Primary squamous cell carcinoma of thethyroid. Indiana Med 79:763–764, 1986.
387. Sarda AK, Bal S, Arunabh, et al: Squamous cell carcinoma ofthe thyroid. J Surg Oncol 39:175–178, 1988.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 87
388. Simpson WJ, Carruthers J: Squamous cell carcinoma of thethyroid gland. Am J Surg 156:44–46, 1988.
389. Shimaoka K, Tsukada Y: Squamous cell carcinomas and ade-nosquamous carcinomas originating from the thyroid gland.Cancer 46:1833–1842, 1980.
390. Theander C, Loden B, Berglund J, Seidal T: Primary squa-mous carcinoma of the thyroid—a case report. J LaryngolOtol 107:1155–1158, 1993.
391. Harada T, Shimaoka K, Katagiri M, et al: Rarity of squamouscell carcinoma of the thyroid: autopsy review. World J Surg18:542–546, 1994.
392. Burt A, Goudie RB: Diagnosis of primary thyroid carcinomaby immunohistological demonstration of thyroglobulin. His-topathology 3:279–286, 1979.
393. Ralfkiaer N, Gatter KC, Alcock C, et al: The value of immu-nocytochemical methods in the differential diagnosis of ana-plastic thyroid tumours. Br J Cancer 52:167–170, 1985.
394. Myskow MW, Krajewski AS, Dewar AE, et al: The role ofimmunoperoxidase techniques on paraffin embedded tissuein determining the histogenesis of undifferentiated thyroidneoplasms. Clin Endocrinol 24:335–341, 1986.
395. Eusebi V, Damiani S, Riva C, et al: Calcitonin free oat-cellcarcinoma of the thyroid gland. Virchows Arch A PatholAnat Histopathol 417:267–271, 1990.
396. Wolf BC, Sheahan K, DeCoste D, et al: Immunohistochemicalanalysis of small cell tumors of the thyroid gland: an EasternCooperative Oncology Group study. Hum Pathol 23:1252–1261, 1992.
397. Totsch M, Dobler G, Feichtinger H, et al: Malignant heman-gioendothelioma of the thyroid. Its immunohistochemicaldiscrimination from undifferentiated thyroid carcinoma [seecomments]. Am J Surg Pathol 14:69–74, 1990.
398. Eckert F, Schmid U, Gloor F, Hedinger C: Evidence of vascu-lar differentiation in anaplastic tumours of the thyroid—animmunohistological study. Virchows Arch A Pathol AnatHistopathol 410:203–215, 1986.
399. Albores-Saavedra J, Nadji M, Civantos F, Morales AR: Thy-roglobulin in carcinoma of the thyroid: an immunohisto-chemical study. Hum Pathol 14:62–66, 1983.
400. Matias-Guiu X, Villanueva A, Cuatrecasas M, et al: p53 in athyroid follicular carcinoma with foci of poorly differentiatedand anaplastic carcinoma. Pathol Res Pract 192:1242–1249,discussion 1250–1251, 1996.
401. Holm R, Nesland JM: Retinoblastoma and p53 tumour sup-pressor gene protein expression in carcinomas of the thyroidgland. J Pathol 172:267–272, 1994.
402. Soares P, Cameselle-Teijeiro J, Sobrinho-Simoes M: Immu-nohistochemical detection of p53 in differentiated, poorlydifferentiated and undifferentiated carcinomas of the thy-roid. Histopathology 24:205–210, 1994.
403. Dobashi Y, Sugimura H, Sakamoto A, et al: Stepwise partici-pation of p53 gene mutation during dedifferentiation of hu-man thyroid carcinomas. Diagn Mol Pathol 3:9–14, 1994.
404. Pollina L, Pacini F, Fontanini G, et al: bcl-2, p53 and prolifer-ating cell nuclear antigen expression is related to the degreeof differentiation in thyroid carcinomas. Br J Cancer 73:139–143, 1996.
405. Garcia-Rostan G, Tallini G, Herrero A, et al: Frequent muta-tion and nuclear localization of beta-catenin in anaplasticthyroid carcinoma. Cancer Res 59:1811–1815, 1999.
406. Sherman SI: Anaplastic carcinoma: prognosis. In Wartofsky L(ed): Thyroid Cancer, A Comprehrensisve Guide to ClinicalManagement. Totowa, NJ, Humana Press, 2000, pp 345–348.
407. Kobayashi T, Asakawa H, Umeshita K, et al: Treatment of 37patients with anaplastic carcinoma of the thyroid. HeadNeck 18:36–41, 1996.
408. Passler C, Scheuba C, Prager G, et al: Anaplastic (undifferen-tiated) thyroid carcinoma (ATC). A retrospective analysis.Langenbecks Arch Surg 384:284–293, 1999.
409. Lu WT, Lin JD, Huang HS, Chao TC: Does surgery improvethe survival of patients with advanced anaplastic thyroidcarcinoma? Otolaryngol Head Neck Surg 118:728–731, 1998.
410. Nel CJ, van Heerden JA, Goellner JR, et al: Anaplastic carci-noma of the thyroid: a clinicopathologic study of 82 cases.Mayo Clin Proc 60:51–58, 1985.
411. Tan RK, Finley RK 3rd, Driscoll D, et al: Anaplastic carci-noma of the thyroid: a 24-year experience. Head Neck 17:41–47, discussion 47–48, 1995.
412. Nilsson O, Lindeberg J, Zedenius J, et al: Anaplastic giantcell carcinoma of the thyroid gland: treatment and survivalover a 25-year period. World J Surg 22:725–730, 1998.
413. Evans HL: Columnar-cell carcinoma of the thyroid. A reportof two cases of an aggressive variant of thyroid carcinoma.Am J Clin Pathol 85:77–80, 1986.
414. Ferreiro JA, Hay ID, Lloyd RV: Columnar cell carcinoma ofthe thyroid: report of three additional cases. Hum Pathol27:1156–1160, 1996.
415. Sobrinho-Simoes M, Nesland JM, Johannessen JV: Columnar-cell carcinoma. Another variant of poorly differentiated car-cinoma of the thyroid. Am J Clin Pathol 89:264–267, 1988.
416. Mizukami Y, Nonomura A, Michigishi T, et al: Columnarcell carcinoma of the thyroid gland: a case report and reviewof the literature. Hum Pathol 25:1098–1101, 1994.
417. Berends D, Mouthaan PJ: Columnar-cell carcinoma of thethyroid. Histopathology 20:360–362, 1992.
418. Gaertner EM, Davidson M, Wenig BM: The columnar cellvariant of thyroid papillary carcinoma. Case report and dis-cussion of an unusually aggressive thyroid papillary carci-noma. Am J Surg Pathol 19:940–947, 1995.
419. Akslen LA, Varhaug JE: Thyroid carcinoma with mixed tall-cell and columnar-cell features. Am J Clin Pathol 94:442–445,1990.
420. Genton CY, Dutoit M, Portmann L, et al: Pathologic fractureof the femur neck as first manifestation of a minute colum-nar cell carcinoma of the thyroid gland. Pathol Res Pract194:861–863, 1998.
421. Shimizu M, Hirokawa M, Manabe T: Tall cell variant ofpapillary thyroid carcinoma with foci of columnar cell com-ponent. Virchows Arch 434:173–175, 1999.
422. Wenig BM, Thompson LD, Adair CF, et al: Thyroid papillarycarcinoma of columnar cell type: a clinicopathologic study of16 cases. Cancer 82:740–753, 1998.
423. Hui PK, Chan JK, Cheung PS, Gwi E: Columnar cell carci-noma of the thyroid. Fine needle aspiration findings in acase. Acta Cytol 34:355–358, 1990.
424. Evans HL: Encapsulated columnar-cell neoplasms of the thy-roid. A report of four cases suggesting a favorable prognosis.Am J Surg Pathol 20:1205–1211, 1996.
425. Fukunaga M, Shinozaki S, Miyazawa Y, Ushigome S: Colum-nar cell carcinoma of the thyroid. Pathol Int 47:489–492,1997.
426. Putti TC, Bhuiya TA, Wasserman PG: Fine needle aspirationcytology of mixed tall and columnar cell papillary carcinomaof the thyroid. A case report. Acta Cytol 42:387–390, 1998.
427. Smith AE, Couch M, Argani P: Pathologic quiz case 1. Papil-lary thyroid carcinoma (PTC), combined tall cell and colum-nar variants. Arch Otolaryngol Head Neck Surg 124:1170,1172, 1998.
428. Franssila KO, Harach HR, Wasenius VM: Mucoepidermoidcarcinoma of the thyroid. Histopathology 8:847–860, 1984.
429. Katoh R, Sugai T, Ono S, et al: Mucoepidermoid carcinomaof the thyroid gland. Cancer 65:2020–2027, 1990.
430. Rhatigan RM, Roque JL, Bucher RL: Mucoepidermoid carci-noma of the thyroid gland. Cancer 39:210–214, 1977.
431. Mizukami Y, Matsubara F, Hashimoto T, et al: Primary mu-coepidermoid carcinoma in the thyroid gland. A case reportincluding an ultrastructural and biochemical study. Cancer53:1741–1745, 1984.
432. Harach HR, Day ES, de Strizic NA: Mucoepidermoid carci-noma of the thyroid. Report of a case with immunohisto-chemical studies. Medicina (B Aires) 46:213–216, 1986.
433. Tanda F, Massarelli G, Bosincu L, et al: Primary mucoepider-moid carcinoma of the thyroid gland. Surg Pathol 3:317–324,1990.
434. Bondeson L, Bondeson AG, Thompson NW: Papillary carci-noma of the thyroid with mucoepidermoid features. Am JClin Pathol 95:175–179, 1991.
435. Sambade C, Franssila K, Basilio-de-Oliveirz C: Mucoepider-moid carcinoma of the thyroid revisited. Surg Pathol 3:271–280, 1990.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

88 Endocrine System
436. Wenig BM, Adair CF, Heffess CS: Primary mucoepidermoidcarcinoma of the thyroid gland: a report of six cases and areview of the literature of a follicular epithelial-derived tu-mor. Hum Pathol 26:1099–1108, 1995.
437. Arezzo A, Patetta R, Ceppa P, et al: Mucoepidermoid carci-noma of the thyroid gland arising from a papillary epithelialneoplasm. Am Surg 64:307–311, 1998.
438. Viciana MJ, Galera-Davidson H, Martin-Lacave I, et al: Papil-lary carcinoma of the thyroid with mucoepidermoid differ-entiation. Arch Pathol Lab Med 120:397–398, 1996.
439. Miranda RN, Myint MA, Gnepp DR: Composite follicularvariant of papillary carcinoma and mucoepidermoid carci-noma of the thyroid. Report of a case and review of theliterature. Am J Surg Pathol 19:1209–1215, 1995.
440. Cameselle-Teijeiro J, Febles-Perez C, Sobrinho-Simoes M:Papillary and mucoepidermoid carcinoma of the thyroidwith anaplastic transformation: a case report with histologicand immunohistochemical findings that support a provoca-tive histogenetic hypothesis. Pathol Res Pract 191:1214–1221,1995.
441. Cameselle-Teijeiro J, Febles-Perez C, Sobrinho-Simoes M: Cy-tologic features of fine needle aspirates of papillary and mu-coepidermoid carcinoma of the thyroid with anaplastic trans-formation. A case report. Acta Cytol 41:1356–1360, 1997.
441a. Baloch ZW, Solomon AC, LiVolsi VA: Primary mucoepider-moid carcinoma and sclerosing mucoepidermoid carcinomawith eosinophilia of the thyroid gland: a report of ninecases. Mod Pathol 13:802–807, 2000.
442. Harach HR: A study on the relationship between solid cellnests and mucoepidermoid carcinoma of the thyroid. Histo-pathology 9:195–207, 1985.
443. Chan JK, Albores-Saavedra J, Battifora H, et al: Sclerosingmucoepidermoid thyroid carcinoma with eosinophilia. A dis-tinctive low-grade malignancy arising from the metaplasticfollicles of Hashimoto’s thyroiditis. Am J Surg Pathol 15:438–448, 1991.
444. Sim SJ, Ro JY, Ordonez NG, et al: Sclerosing mucoepider-moid carcinoma with eosinophilia of the thyroid: report oftwo patients, one with distant metastasis, and review of theliterature. Hum Pathol 28:1091–1096, 1997.
445. Geisinger KR, Steffee CH, McGee RS, et al: The cytomorpho-logic features of sclerosing mucoepidermoid carcinomaof the thyroid gland with eosinophilia. Am J Clin Pathol109:294–301, 1998.
446. Chung J, Lee SK, Gong G, et al: Sclerosing mucoepidermoidcarcinoma with eosinophilia of the thyroid glands: a casereport with clinical manifestation of recurrent neck mass. JKorean Med Sci 14:338–341, 1999.
447. Cavazza A, Toschi E, Valcavi R, et al: Sclerosing mucoepi-dermoid carcinoma with eosinophilia of the thyroid: descrip-tion of a case. Pathologica 91:31–35, 1999.
448. Diaz-Perez R, Quiroz H, Nishiyama RH: Primary mucinousadenocarcinoma of thyroid gland. Cancer 38:1323–1325,1976.
449. Sobrinho-Simoes M, Stenwig AE, Nesland JM, et al: A muci-nous carcinoma of the thyroid. Pathol Res Pract 181:464–471,1986.
450. Sobrinho-Simoes MA, Nesland JM, Johannessen JV: A mu-cin-producing tumor in the thyroid gland. Ultrastruct Pathol9:277–281, 1985.
451. Cruz MC, Marques LP, Sambade CC, et al: Primary muci-nous carcinoma of the thyroid gland. Surg Pathol 4:266–273,1991.
452. Williams ED: Histogenesis of medullary carcinoma of thethyroid. J Clin Pathol 19:114–118, 1966.
453. Raue F, Kotzerke J, Reinwein D, et al: Prognostic factors inmedullary thyroid carcinoma: evaluation of 741 patientsfrom the German Medullary Thyroid Carcinoma Register.Clin Invest 71:7–12, 1993.
454. Williams ED: Medullary carcinoma of the thyroid. In De-Groot LJ (ed): Endocrinology. New York, Grune & Stratton,1979, pp 777–792.
455. Saad MF, Ordonez NG, Rashid RK, et al: Medullary carci-noma of the thyroid. A study of the clinical features andprognostic factors in 161 patients. Medicine (Baltimore)63:319–342, 1984.
456. Rosenberg-Bourgin M, Gardet P, de Sahb R, et al: Compari-son of sporadic and hereditary forms of medullary thyroidcarcinoma. Henry Ford Hospital J 37:141–143, 1989.
457. Donovan DT, Levy ML, Frust EJ: Familial cutaneous lichenamyloidosis in association with MEN2A: a new variant.Henry Ford Hospital J 37:147–150, 1989.
458. Sobol H, Narod SA, Schuffenecker I, et al: Hereditary medul-lary thyroid carcinoma: genetic analysis of three related syn-dromes. Henry Ford Hospital J 37:109–111, 1989.
459. Farndon JR, Leight GS, Dilley WG: Familial medullary thy-roid carcinoma without associated endocrinopathies: a dis-tinct clinical entity. Br J Surg 73:278–281, 1986.
460. Wolfe HJ, DeLellis RA: Familial medullary thyroid carci-noma and C cell hyperplasia. Clin Endocrinol Metab 10:351–365, 1981.
461. Carney JA, Sizemore GW, Hayles AV: C-cell disease of thethyroid gland in multiple endocrine neoplasia, type 2b. Can-cer 44:2173–2183, 1979.
462. Mulligan LM, Kwok JB, Healey CS, et al: Germ-line muta-tions of the RET proto-oncogene in multiple endocrine neo-plasia type 2A. Nature 363:458–460, 1993.
463. Mulligan LM, Eng C, Healey CS, et al: Specific mutations ofthe RET proto-oncogene are related to disease phenotype inMEN 2A and FMTC. Nat Genet 6:70–74, 1994.
464. Hofstra RM, Landsvater RM, Ceccherini I, et al: A mutationin the RET proto-oncogene associated with multiple endo-crine neoplasia type 2B and sporadic medullary thyroid car-cinoma [see comments]. Nature 367:375–376, 1994.
465. Chong GC, Beahrs OH, Sizemore GW, Woolner LH: Medul-lary carcinoma of the thyroid gland. Cancer 35:695–704,1975.
466. Mure A, Gicquel C, Abdelmoumene N, et al: Cushing’s syn-drome in medullary thyroid carcinoma. J Endocrinol Invest18:180–185, 1995.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
467. Modigliani E: Medullary thyroid carcinoma. Curr Ther En-docrinol Metab 5:112–117, 1994.
468. Henry JF, Denizot A, Puccini M, et al: Latent subclinicalmedullary thyroid carcinoma: diagnosis and treatment.World J Surg 22:752–756, discussion 756–757, 1998.
469. Rieu M, Lame MC, Richard A, et al: Prevalence of sporadicmedullary thyroid carcinoma: the importance of routinemeasurement of serum calcitonin in the diagnostic evalua-tion of thyroid nodules [see comments]. Clin Endocrinol(Oxf) 42:453–460, 1995.
470. Kaserer K, Scheuba C, Neuhold N, et al: C-cell hyperplasiaand medullary thyroid carcinoma in patients routinelyscreened for serum calcitonin. Am J Surg Pathol 22:722–728,1998.
471. Kakudo K, Carney JA, Sizemore GW: Medullary carcinomaof thyroid. Biologic behavior of the sporadic and familialneoplasm. Cancer 55:2818–2821, 1985.
472. Carney JA, Sizemore GW, Hayles AB: Multiple endocrineneoplasia, type 2b. Pathobiol Annu 8:105–153, 1978.
473. Kebebew E, Ituarte PH, Siperstein AE, et al: Medullarythyroid carcinoma: clinical characteristics, treatment, prog-nostic factors, and a comparison of staging systems. Cancer88:1139–1148, 2000.
474. Bigner SH, Cox EB, Mendelsohn G, et al: Medullary carci-noma of the thyroid in the multiple endocrine neoplasia IIAsyndrome. Am J Surg Pathol 5:459–472, 1981.
475. Ibanez ML: Medullary carcinoma of the thyroid gland.Pathol Annu 9:263–290, 1974.
476. Albores-Saavedra J, LiVolsi VA, Williams ED: Medullary car-cinoma. Semin Diagn Pathol 2:137–146, 1985.
477. Hazard JB: The C cells (parafollicular cells) of the thyroidgland and medullary thyroid carcinoma. A review. Am JPathol 88:213–250, 1977.
478. Uribe M, Fenoglio-Preiser CM, Grimes M, Feind C: Medul-lary carcinoma of the thyroid gland. Clinical, pathological,and immunohistochemical features with review of the litera-ture. Am J Surg Pathol 9:577–594, 1985.
479. Zaatari GS, Saigo PE, Huvos AG: Mucin production in med-ullary carcinoma of the thyroid. Arch Pathol Lab Med107:70–74, 1983.
480. Krueger JE, Maitra A, Albores-Saavedra J: Inherited medul-
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 89
lary microcarcinoma of the thyroid: a study of 11 cases. AmJ Surg Pathol 24:853–858, 2000.
481. Harach HR, Williams ED: Glandular (tubular and follicular)variants of medullary carcinoma of the thyroid. Histopathol-ogy 7:83–97, 1983.
482. Sambade C, Baldaque-Faria A, Cardoso-Oliveira M, Sob-rinho-Simoes M: Follicular and papillary variants of medul-lary carcinoma of the thyroid. Pathol Res Pract 184:98–107,1988.
483. Dominguez-Malagon H, Delgado-Chavez R, Torres-NajeraM, et al: Oxyphil and squamous variants of medullary thy-roid carcinoma. Cancer 63:1183–1188, 1989.
484. Harach HR, Bergholm U: Medullary (C cell) carcinoma ofthe thyroid with features of follicular oxyphilic cell tumours.Histopathology 13:645–656, 1988.
485. Kakudo K, Miyauchi A, Ogihara T, et al: Medullary carci-noma of the thyroid. Giant cell type. Arch Pathol Lab Med102:445–447, 1978.
486. Mendelsohn G, Baylin SB, Bigner SH, et al: Anaplastic vari-ants of medullary thyroid carcinoma: a light-microscopic andimmunohistochemical study. Am J Surg Pathol 4:333–341,1980.
487. Bussolati G, Monga G: Medullary carcinoma of the thyroidwith atypical patterns. Cancer 44:1769–1777, 1979.
488. Landon G, Ordonez NG: Clear cell variant of medullarycarcinoma of the thyroid. Hum Pathol 16:844–847, 1985.
489. Holm R, Sobrinho-Simoes M, Nesland JM, et al: Medullarycarcinoma of the thyroid gland: an immunocytochemicalstudy. Ultrastruct Pathol 8:25–41, 1985.
490. Marcus JN, Dise CA, LiVolsi VA: Melanin production in amedullary thyroid carcinoma. Cancer 49:2518–2526, 1982.
491. Beerman H, Rigaud C, Bogomoletz WV, et al: Melanin pro-duction in black medullary thyroid carcinoma (MTC). Histo-pathology 16:227–233, 1990.
492. Ikeda T, Satoh M, Azuma K, et al: Medullary thyroid carci-noma with a paraganglioma-like pattern and melanin pro-duction: a case report with ultrastructural and immunohisto-chemical studies. Arch Pathol Lab Med 122:555–558, 1998.
493. Schroder S, Bocker W, Baisch H, et al: Prognostic factors inmedullary thyroid carcinomas. Survival in relation to age,sex, stage, histology, immunocytochemistry, and DNA con-tent. Cancer 61:806–816, 1988.
494. Kakudo K, Miyauchi A, Takai S, et al: C cell carcinoma ofthe thyroid—papillary type. Acta Pathol Jpn 29:653–659,1979.
495. Harach HR, Bergholm U: Small cell variant of medullarycarcinoma of the thyroid with neuroblastoma-like features.Histopathology 21:378–380, 1992.
496. Huss LJ, Mendelsohn G: Medullary carcinoma of the thyroidgland: an encapsulated variant resembling the hyalinizingtrabecular (paraganglioma-like) adenoma of thyroid. ModPathol 3:581–585, 1990.
497. Harach HR, Bergholm U: Medullary carcinoma of the thy-roid with carcinoid-like features. J Clin Pathol 46:113–117,1993.
498. Butler M, Khan S: Immunoreactive calcitonin in amyloid fi-brils of medullary carcinoma of the thyroid gland. An im-munogold staining technique. Arch Pathol Lab Med 110:647–649, 1986.
499. Krisch K, Krisch I, Horvat G, et al: The value of immunohis-tochemistry in medullary thyroid carcinoma: a systematicstudy of 30 cases. Histopathology 9:1077–1089, 1985.
500. Schmid KW, Fischer-Colbrie R, Hagn C, et al: ChromograninA and B and secretogranin II in medullary carcinomas of thethyroid. Am J Surg Pathol 11:551–556, 1987.
501. Lloyd RV, Sisson JC, Marangos PJ: Calcitonin, carcinoembry-onic antigen and neuron-specific enolase in medullary thy-roid carcinoma. Cancer 51:2234–2239, 1983.
502. Schroder S, Kloppel G: Carcinoembryonic antigen and non-specific cross-reacting antigen in thyroid cancer. An immu-nocytochemical study using polyclonal and monoclonal anti-bodies. Am J Surg Pathol 11:100–108, 1987.
503. Matias-Guiu X, Machin P, Pons C, et al: Sustentacular cellsoccur frequently in the familial form of medullary thyroidcarcinoma. J Pathol 184:420–423, 1998.
504. Emmertsen K, Ernø H, Henriques U, Schrøder HD: C-cells
for differentiation between familial and sporadic medullarythyroid carcinoma. Dan Med Bull 30:353–356, 1983.
505. Albores-Saavedra J, Monforte H, Nadji M, Morales AR:C-cell hyperplasia in thyroid tissue adjacent to follicular celltumors. Hum Pathol 19:795–799, 1988.
506. Santensanio G, Iafrate E, Partenzi A, et al: A critical reassess-ment of the concept of C-cell hyperplasia of the thyroid—aquantitative immunohistochemical study. Appl Immunohis-tochem 5:160–172, 1997.
507. DeLellis RA, Wolfe HJ: The pathobiology of the human calci-tonin (C)–cell: a review. Pathol Annu 16:25–52, 1981.
508. Chan JKC, Tse CCH: Solid cell nest-associated C-cells: an-other possible explanation for “C-cell hyperplasia” adjacentto follicular cell tumors (letter). Hum Pathol 10:498, 1989.
509. Baschieri L, Castagna M, Fierabracci A, et al: Distribution ofcalcitonin- and somatostatin-containing cells in thyroid lym-phoma and in Hashimoto’s thyroiditis. Appl Pathol 7:99–104, 1989.
510. Perry A, Molberg K, Albores-Saavedra J: Physiologic versusneoplastic C-cell hyperplasia of the thyroid: separation ofdistinct histologic and biologic entities. Cancer 77:750–756,1996.
511. Komminoth P: The RET proto-oncogene in medullary andpapillary thyroid carcinoma. Molecular features, pathophysi-ology and clinical implications. Virchows Arch 431:1–9,1997.
512. Lloyd RV: RET proto-oncogene mutations and rearrange-ments in endocrine diseases. Am J Pathol 147:1539–1544,1995.
513. Mulligan LM, Marsh DJ, Robinson BG, et al: Genotype-phenotype correlation in multiple endocrine neoplasia type2: report of the International RET Mutation Consortium. JIntern Med 238:343–346, 1995.
514. Komminoth P, Kunz EK, Matias-Guiu X, et al: Analysis ofRET protooncogene point mutations distinguishes heritablefrom nonheritable medullary thyroid carcinomas. Cancer76:479–489, 1995.
515. Eng C, Mulligan LM: Mutations of the RET protooncogenein the multiple endocrine neoplasia type 2 syndromes, re-lated sporadic tumors, and Hirschsprung disease. Hum Mu-tat 9:97–109, 1997.
516. Lallier M, St-Vil D, Giroux M, et al: Prophylactic thyroidec-tomy for medullary thyroid carcinoma in gene carriers ofMEN2 syndrome. J Pediatr Surg 33:846–848, 1998.
517. Hinze R, Holzhausen HJ, Gimm O, et al: Primary hereditarymedullary thyroid carcinoma—C-cell morphology and corre-lation with preoperative calcitonin levels. Virchows Arch433:203–208, 1998.
518. Dralle H, Gimm O, Simon D, et al: Prophylactic thyroidec-tomy in 75 children and adolescents with hereditary medul-lary thyroid carcinoma: German and Austrian experience.World J Surg 22:744–750, discussion 750–751, 1998.
519. Eng C, Mulligan LM, Smith DP, et al: Mutation of the RETprotooncogene in sporadic medullary thyroid carcinoma.Genes Chromosomes Cancer 12:209–212, 1995.
520. Bugalho MJ, Frade JP, Santos JR, et al: Molecular analysis ofthe RET proto-oncogene in patients with sporadic medullarythyroid carcinoma: a novel point mutation in the extracellu-lar cysteine-rich domain. Eur J Endocrinol 136:423–426, 1997.
521. Romei C, Elisei R, Pinchera A, et al: Somatic mutations ofthe ret protooncogene in sporadic medullary thyroid carci-noma are not restricted to exon 16 and are associated withtumor recurrence. J Clin Endocrinol Metab 81:1619–1622,1996.
522. Marsh DJ, Learoyd DL, Andrew SD, et al: Somatic mutationsin the RET proto-oncogene in sporadic medullary thyroidcarcinoma. Clin Endocrinol (Oxf) 44:249–257, 1996.
523. Matias-Guiu X, LaGuette J, Puras-Gil AM, Rosai J: Metastaticneuroendocrine tumors to the thyroid gland mimicking med-ullary carcinoma: a pathologic and immunohistochemicalstudy of six cases. Am J Surg Pathol 21:754–762, 1997.
524. Girelli ME, Nacamulli D, Pelizzo MR, et al: Medullary thy-roid carcinoma: clinical features and long-term follow-up ofseventy-eight patients treated between 1969 and 1986. Thy-roid 8:517–523, 1998.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

90 Endocrine System
525. Modigliani E, Cohen R, Campos JM, et al: Prognostic factorsfor survival and for biochemical cure in medullary thyroidcarcinoma: results in 899 patients. The GETC Study Group.Groupe d’etude des tumeurs a calcitonine. Clin Endocrinol(Oxf) 48:265–273, 1998.
526. Scopsi L, Sampietro G, Boracchi P, et al: Multivariate analy-sis of prognostic factors in sporadic medullary carcinoma ofthe thyroid. A retrospective study of 109 consecutive pa-tients. Cancer 78:2173–2183, 1996.
527. Bergholm U, Bergstrom R, Ekbom A: Long-term follow-up ofpatients with medullary carcinoma of the thyroid. Cancer79:132–138, 1997.
528. Rossi RL, Cady B, Meissner WA, et al: Nonfamilial medul-lary thyroid carcinoma. Am J Surg 139:554–560, 1980.
529. Fuchshuber PR, Loree TR, Hicks WL Jr, et al: Medullarycarcinoma of the thyroid: prognostic factors and treatmentrecommendations. Ann Surg Oncol 5:81–86, 1998.
530. Brierley J, Tsang R, Simpson WJ, et al: Medullary thyroidcancer: analyses of survival and prognostic factors and therole of radiation therapy in local control. Thyroid 6:305–310,1996.
531. Norton JA, Froome LC, Farrell RE, et al: Multiple endocrineneoplasia type IIb: the most aggressive form of medullarythyroid carcinoma. Surg Clin North Am 59:109–118, 1979.
532. Guyetant S, Dupre F, Bigorgne JC, et al: Medullary thyroidmicrocarcinoma: a clinicopathologic retrospective study of 38patients with no prior familial disease. Hum Pathol 30:957–963, 1999.
533. Williams ED, Brown CL, Doniach I: Pathological and clinicalfindings in a series of 67 cases of medullary carcinoma of thethyroid. J Clin Pathol 19:103–113, 1966.
534. Ruppert JM, Eggleston JC, deBustros A, Baylin SB: Dissemi-nated calcitonin-poor medullary thyroid carcinoma in a pa-tient with calcitonin-rich primary tumor. Am J Surg Pathol10:513–518, 1986.
535. Saad MF, Ordonez NG, Guido JJ, Samaan NA: The prognos-tic value of calcitonin immunostaining in medullary carci-noma of the thyroid. J Clin Endocrinol Metab 59:850–856,1984.
536. Mendelsohn G, Wells SA Jr, Baylin SB: Relationship of tissuecarcinoembryonic antigen and calcitonin to tumor virulencein medullary thyroid carcinoma. An immunohistochemicalstudy in early, localized, and virulent disseminated stages ofdisease. Cancer 54:657–662, 1984.
537. Schroder S, Schwarz W, Rehpenning W, et al: Leu-M1 im-munoreactivity and prognosis in medullary carcinomas ofthe thyroid gland. J Cancer Res Clin Oncol 114:291–296,1988.
538. Langle F, Soliman T, Neuhold N, et al: CD15 (LeuM1) im-munoreactivity: prognostic factor for sporadic and hereditarymedullary thyroid cancer? Study Group on Multiple Endo-crine Neoplasia of Austria. World J Surg 18:583–587, 1994.
539. Viale G, Roncalli M, Grimelius L, et al: Prognostic value ofbcl-2 immunoreactivity in medullary thyroid carcinoma.Hum Pathol 26:945–950, 1995.
540. Scopsi L, Sampietro G, Boracchi P, Collini P: Argyrophiliaand chromogranin A and B immunostaining in patients withsporadic medullary thyroid carcinoma. A critical appraisal oftheir prognostic utility. J Pathol 184:414–419, 1998.
541. Roncalli M, Viale G, Grimelius L, et al: Prognostic value ofN-myc immunoreactivity in medullary thyroid carcinoma.Cancer 74:134–141, 1994.
542. Fontanini G, Vignati S, Pacini F, et al: Microvessel count: anindicator of poor outcome in medullary thyroid carcinomabut not in other types of thyroid carcinoma. Mod Pathol9:636–641, 1996.
543. el-Naggar AK, Ordonez NG, McLemore D, et al: Clinico-pathologic and flow cytometric DNA study of medullarythyroid carcinoma. Surgery 108:981–985, 1990.
544. Ekman ET, Bergholm U, Backdahl M, et al: Nuclear DNAcontent and survival in medullary thyroid carcinoma. Swed-ish Medullary Thyroid Cancer Study Group. Cancer 65:511–517, 1990.
545. Gonzalez-Campora R, Lopez-Garrido J, Martin-Lacave I, etal: Concurrence of a symptomatic encapsulated follicular car-
cinoma, an occult papillary carcinoma and a medullary car-cinoma in the same patient. Histopathology 21:380–382,1992.
546. Sobrinho-Simoes M: Mixed medullary and follicular carci-noma of the thyroid. Histopathology 23:287–289, 1993.
547. Pfaltz M, Hedinger CE, Muhlethaler JP: Mixed medullaryand follicular carcinoma of the thyroid. Virchows Arch APathol Anat Histopathol 400:53–59, 1983.
548. Parker LN, Kollin J, Wu SY, et al: Carcinoma of the thyroidwith a mixed medullary, papillary, follicular, and undifferen-tiated pattern. Arch Intern Med 145:1507–1509, 1985.
549. Apel RL, Alpert LC, Rizzo A, et al: A metastasizing compos-ite carcinoma of the thyroid with distinct medullary andpapillary components. Arch Pathol Lab Med 118:1143–1147,1994.
550. Lax SF, Beham A, Kronberger-Schonecker D, et al: Coexis-tence of papillary and medullary carcinoma of the thyroidgland—mixed or collision tumour? Clinicopathological anal-ysis of three cases. Virchows Arch 424:441–447, 1994.
551. Albores-Saavedra J, Gorraez de la Mora T, de la Torre-Ren-don F, Gould E: Mixed medullary-papillary carcinoma of thethyroid: a previously unrecognized variant of thyroid carci-noma. Hum Pathol 21:1151–1155, 1990.
552. Pastolero GC, Coire CI, Asa SL: Concurrent medullary andpapillary carcinomas of thyroid with lymph node metastases.A collision phenomenon. Am J Surg Pathol 20:245–250, 1996.
553. Ljungberg O: Biopsy Pathology of the Thyroid and Parathy-roid. London, Chapman & Hall, 1992.
554. Burt AD, MacGuire J, Lindop GB, et al: Mixed follicular-parafollicular carcinoma of the thyroid. Scott Med J 32:50–51, 1987.
555. Papotti M, Negro F, Carney JA, et al: Mixed medullary-follicular carcinoma of the thyroid. A morphological, immu-nohistochemical and in situ hybridization analysis of 11cases. Virchows Arch 430:397–405, 1997.
556. Papotti M, Volante M, Komminoth P, et al: Thyroid carcino-mas with mixed follicular and C-cell differentiation patterns.Semin Diagn Pathol 17:109–119, 2000.
557. Ljungberg O, Ericsson UB, Bondeson L, Thorell J: A com-pound follicular-parafollicular cell carcinoma of the thyroid:a new tumor entity? Cancer 52:1053–1061, 1983.
558. Ljungberg O, Bondeson L, Bondeson AG: Differentiated thy-roid carcinoma, intermediate type: a new tumor entity withfeatures of follicular and parafollicular cell carcinoma. HumPathol 15:218–228, 1984.
559. Mizukami Y, Nonomura A, Michigishi T, et al: Mixed med-ullary-follicular carcinoma of the thyroid gland: a clinico-pathologic variant of medullary thyroid carcinoma. ModPathol 9:631–635, 1996.
560. Volante M, Papotti M, Roth J, et al: Mixed medullary-follicu-lar thyroid carcinoma. Molecular evidence for a dual originof tumor components. Am J Pathol 155:1499–1509, 1999.
561. Holm R, Sobrinho-Simoes M, Nesland JM, et al: Medullarythyroid carcinoma with thyroglobulin immunoreactivity. Aspecial entity? Lab Invest 57:258–268, 1987.
562. Chan JK, Rosai J: Tumors of the neck showing thymic orrelated branchial pouch differentiation: a unifying concept.Hum Pathol 22:349–367, 1991.
563. Lewis JE, Wick MR, Scheithauer BW, et al: Thymoma, aclinicopathologic review. Cancer 60:2727–2743, 1987.
564. Murao T, Nakanishi M, Toda K, et al: Malignant teratoma ofthe thyroid gland in an adolescent female. Acta Pathol Jpn29:109–117, 1979.
565. Levey M: An unusual thyroid tumor in a child. Laryngo-scope 86:1864–1868, 1976.
566. Weigensberg C, Dalsley H, Asa SL, et al: Thyroid thymomain childhood. Endocrinol Pathol 1:123–127, 1990.
567. Harach HR, Saravia Day E, Franssila KO: Thyroid spindle-cell tumor with mucous cysts. An intrathyroid thymoma?Am J Surg Pathol 9:525–530, 1985.
568. Kingsley DPE, Elton A, Bennett MH: Malignant teratoma ofthe thyroid, case report and a review of the literature. Br JCancer 22:7–11, 1968.
569. Hofman P, Mainguene C, Michiels JF, et al: Thyroid spindleepithelial tumor with thymus-like differentiation (the “SET-
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

Thyroid and Parathyroid 91
TLE” tumor). An immunohistochemical and electron micro-scopic study. Eur Arch Otorhinolaryngol 252:316–320, 1995.
570. Saw D, Wu D, Chess Q, Shemen L: Spindle epithelial tumorwith thymus-like element (SETTLE), a primary thyroid tu-mor. Int J Surg Pathol 4:169–174, 1997.
571. Chetty R, Goetsch S, Nayler S, Cooper K: Spindle epithelialtumour with thymus-like element (SETTLE): the predomi-nantly monophasic variant. Histopathology 33:71–74, 1998.
572. Kirby PA, Ellison WA, Thomas PA: Spindle epithelial tumorwith thymus-like differentiation (SETTLE) of the thyroidwith prominent mitotic activity and focal necrosis. Am JSurg Pathol 23:712–716, 1999.
573. Asa SL, Dardick I, Van Nostrand AW, et al: Primary thyroidthymoma: a distinct clinicopathologic entity. Hum Pathol19:1463–1467, 1988.
574. Kakudo K, Mori I, Tamaoki N, Watanabe K: Carcinoma ofpossible thymic origin presenting as a thyroid mass: a newsubgroup of squamous cell carcinoma of the thyroid. J SurgOncol 38:187–192, 1988.
575. Miyauchi A, Kuma K, Matsuzuka F, et al: Intrathyroidalepithelial thymoma: an entity distinct from squamous cellcarcinoma of the thyroid. World J Surg 9:128–135, 1985.
576. Miyauchi A, Ishikawa H, Maedea M: Intrathyroid epithelialthymoma: a report of six cases with immunohistochemicaland ultrastructural studies [in Japanese]. Endocrinol Surg6:289–295, 1989.
577. Mizukami Y, Kurumaya H, Yamada T, et al: Thymic carci-noma involving the thyroid gland: report of two cases. HumPathol 26:576–579, 1995.
578. Watanabe I, Tezuka F, Yamaguchi M, et al: Thymic carci-noma of the thyroid. Pathol Int 46:450–456, 1996.
579. Attaran SY, Omrani GH, Tavangar SM: Lymphoepithelial-like intrathyroidal thymic carcinoma with foci of squamousdifferentiation. Case report. APMIS 104:419–423, 1996.
580. Damiani S, Filotico M, Eusebi V: Carcinoma of the thyroidshowing thymoma-like features. Virchows Arch A PatholAnat Histopathol 418:463–466, 1991.
581. Cheuk W, Jacobson AA, Chan JKC: Spindle epithelial tumorwith thymus-like element: a distinctive malignant thyroidtumor with significant metastatic potential. Mod Pathol 13:1150–1155, 2000.
582. Dorfman DM, Shahsafaei A, Miyauchi A: Intrathyroidal epi-thelial thymoma (ITET)/carcinoma showing thymus-like dif-ferentiation (CASTLE) exhibits CD5 immunoreactivity: newevidence for thymic differentiation. Histopathology 32:104–109, 1998.
583. Berezowski K, Grimes MM, Gal A, Kornstein MJ: CD5 im-munoreactivity of epithelial cells in thymic carcinoma andCASTLE using paraffin-embedded tissue. Am J Clin Pathol106:483–486, 1996.
584. Tse LLY, Shek TWH, Lam KY, et al: Carcinoma showingthymus-like differentiation (CASTLE) of the thyroid: an in-trathyroid thymic carcinoma (abstract). Int J Surg Pathol(in press).
585. Choi P, To KF, Lai FM, et al: Follicular dendritic cell tumorof the neck: a report of two cases complicated by pulmonarymetastasis. Cancer 89:664–672, 2000.
586. Sawady J, Mendelsohn G, Sirota RL, Taxy JB: The intrathy-roidal hyperfunctioning parathyroid gland. Mod Pathol2:652–657, 1989.
587. de la Cruz Vigo F, Ortega G, Gonzalez S, et al: Pathologicintrathyroidal parathyroid glands. Int Surg 82:87–90, 1997.
588. Freeman C, Berg JW, Cutler SJ: Occurrence and prognosis ofextranodal lymphomas. Cancer 29:252–260, 1972.
589. Anscombe AM, Wright DH: Primary malignant lymphomaof the thyroid—a tumour of mucosa-associated lymphoidtissue: review of seventy-six cases. Histopathology 9:81–97,1985.
590. Aozasa K, Inoue A, Tajima K, et al: Malignant lymphomasof the thyroid gland. Analysis of 79 patients with emphasison histologic prognostic factors. Cancer 58:100–104, 1986.
591. Burke JS, Butler JJ, Fuller LM: Malignant lymphomas of thethyroid: a clinical pathologic study of 35 patients includingultrastructural observations. Cancer 39:1587–1602, 1977.
592. Compagno J, Oertel JE: Malignant lymphoma and other lym-
phoproliferative disorders of the thyroid gland. A clinico-pathologic study of 245 cases. Am J Clin Pathol 74:1–11,1980.
593. Devine RM, Edis AJ, Banks PM: Primary lymphoma of thethyroid: a review of the Mayo Clinic experience through1978. World J Surg 5:33–38, 1981.
594. Rasbach DA, Mondschein MS, Harris NL, et al: Malignantlymphoma of the thyroid gland: a clinical and pathologicstudy of twenty cases. Surgery 98:1166–1170, 1985.
595. Woolner LB, McConahey WM, Beahrs OH, Black BM: Pri-mary malignant lymphoma of the thyroid. Review of forty-six cases. Am J Surg 111:502–523, 1966.
596. Singer JA: Primary lymphoma of the thyroid. Am Surg64:334–337, 1998.
597. Pledge S, Bessell EM, Leach IH, et al: Non-Hodgkin’s lym-phoma of the thyroid: a retrospective review of all patientsdiagnosed in Nottinghamshire from 1973 to 1992. Clin Oncol8:371–375, 1996.
598. Hamburger JI, Miller JM, Kini SR: Lymphoma of the thyroid.Ann Intern Med 99:685–693, 1983.
599. Derringer GA, Thompson LD, Frommelt RA, et al: Malignantlymphoma of the thyroid gland: a clinicopathologic study of108 cases. Am J Surg Pathol 24:623–639, 2000.
600. Thompson LD, Rosai J, Heffess CS: Primary thyroid terato-mas: a clinicopathologic study of 30 cases. Cancer 88:1149–1158, 2000.
601. Luboshitzky R, Dharan M, Nachtigal D, et al: Syncytial vari-ant of nodular sclerosing Hodgkin’s disease presenting as athyroid nodule. A case report. Acta Cytol 39:543–546, 1995.
602. Aozasa K, Inoue A, Yoshimura H, et al: Intermediate lym-phocytic lymphoma of the thyroid. An immunologic andimmunohistologic study. Cancer 57:1762–1767, 1986.
603. Coltrera MD: Primary T-cell lymphoma of the thyroid. HeadNeck 21:160–163, 1999.
604. Abdul-Rahman ZH, Gogas HJ, Tooze JA, et al: T-cell lym-phoma in Hashimoto’s thyroiditis. Histopathology 29:455–459, 1996.
605. Yamaguchi M, Ohno T, Kita K: Gamma/delta T-cell lym-phoma of the thyroid gland (letter). N Engl J Med 336:1391–1392, 1997.
606. Shanks JH, Harris M, Howat AJ, Freemont AJ: Angiotropiclymphoma with endocrine involvement. Histopathology31:161–166, 1997.
607. Isaacson PG: Lymphomas of mucosa-associated lymphoidtissue (MALT). Histopathology 16:617–619, 1990.
608. Hyjek E, Isaacson PG: Primary B cell lymphoma of the thy-roid and its relationship to Hashimoto’s thyroiditis. HumPathol 19:1315–1326, 1988.
609. Isaacson PG, Androulakis-Papachristou A, Diss TC, et al:Follicular colonization in thyroid lymphoma. Am J Pathol141:43–52, 1992.
610. Mizukami Y, Michigishi T, Nonomura A, et al: Primary lym-phoma of the thyroid: a clinical, histological and immunohis-tochemical study of 20 cases. Histopathology 17:201–209,1990.
611. Rosen IB, Sutcliffe SB, Gospodarowicz MK, et al: The role ofsurgery in the management of thyroid lymphoma. Surgery104:1095–1099, 1988.
612. Maurer R, Taylor CR, Terry R, et al: Non-Hodgkin’s lym-phoma of the thyroid, a clinicopathological review of 29cases applying the Lukes-Collins classification and an immu-noperoxidase method. Virchows Arch A Pathol Anat Histo-pathol 383:293–317, 1979.
613. Bateman AC, Wright DH: Epitheliotropism in high-gradelymphomas of mucosa-associated lymphoid tissue. Histopa-thology 23:409–415, 1993.
614. Tennvall J, Cavallin-Stahl E, Akerman M: Primary localizednon-Hodgkin’s lymphoma of the thyroid: a retrospectiveclinicopathological review. Eur J Surg Oncol 13:297–302,1987.
615. Stone CW, Slease RB, Brubaker D, et al: Thyroid lymphomawith gastrointestinal involvement: report of three cases. AmJ Hematol 21:357–365, 1986.
616. Pedersen RK, Pedersen NT: Primary non-Hodgkin’s lym-phoma of the thyroid gland: a population based study. His-topathology 28:25–32, 1996.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

92 Endocrine System
617. Laing RW, Hoskin P, Hudson BV, et al: The significance ofMALT histology in thyroid lymphoma: a review of patientsfrom the BNLI and Royal Marsden Hospital. Clin Oncol (RColl Radiol) 6:300–304, 1994.
618. Skacel M, Ross CW, Hsi ED: A reassessment of primarythyroid lymphoma: high-grade MALT-type lymphoma as adistinct subtype of diffuse large B-cell lymphoma. Histopa-thology 37:10–18, 2000.
619. Aozasa K, Inoue A, Yoshimura H, et al: Plasmacytoma of thethyroid gland. Cancer 58:105–110, 1986.
620. Hussong JW, Perkins SL, Schnitzer B, et al: Extramedullaryplasmacytoma. A form of marginal zone cell lymphoma?Am J Clin Pathol 111:111–116, 1999.
621. Yapp R, Linder J, Schenken JR, Karrer FW: Plasma cell gran-uloma of the thyroid. Hum Pathol 16:848–850, 1985.
study of five cases of anaplastic carcinoma. Cancer 62:2558–2563, 1988.
642. Iida Y, Katoh R, Yoshioka M, et al: Primary leiomyosarcomaof the thyroid gland. Acta Pathol Jpn 43:71–75, 1993.
643. Chetty R, Clark SP, Dowling JP: Leiomyosarcoma of the thy-roid: immunohistochemical and ultrastructural study. Pathol-ogy 25:203–205, 1993.
644. Ozaki O, Sugino K, Mimura T, et al: Primary leiomyosar-coma of the thyroid gland. Surg Today 27:177–180, 1997.
645. Tulbah A, Al-Dayel F, Fawaz I, Rosai J: Epstein-Barr virus–associated leiomyosarcoma of the thyroid in a child withcongenital immunodeficiency: a case report. Am J SurgPathol 23:473–476, 1999.
646. Andrion A, Bellis D, Delsedime L, et al: Leiomyoma andneurilemoma: report of two unusual non-epithelial tumoursof the thyroid gland. Virchows Arch A Pathol Anat Histo-pathol 413:367–372, 1988.
647. Galati LT, Barnes EL, Myers EN: Dendritic cell sarcoma ofthe thyroid. Head Neck 21:273–275, 1999.
648. Pickleman JR, Lee JF, Straus FHd, Paloyan E: Thyroid he-mangioma. Am J Surg 129:331–333, 1975.
649. Andrion A, Gaglio A, Dogliani N, et al: Liposarcoma of thethyroid gland. Fine-needle aspiration cytology, immunohis-tology, and ultrastructure. Am J Clin Pathol 95:675–679,1991.
650. Nielsen VT, Knudsen N, Holm IE: Liposarcoma of the thy-roid gland. Tumori 72:499–502, 1986.
651. Tseleni-Balafouta S, Arvanitis D, Kakaviatos N, Paraske-vakou H: Primary myxoid chondrosarcoma of the thyroidgland. Arch Pathol Lab Med 112:94–96, 1988.
652. Nitzsche EU, Seeger LL, Klosa B, et al: Primary osteosar-coma of the thyroid gland. J Nucl Med 33:1399–1401, 1992.
653. Sichel JY, Wygoda M, Dano I, et al: Fibrosarcoma of thethyroid in a man exposed to fallout from the Chernobylaccident. Ann Otol Rhinol Laryngol 105:832–834, 1996.
654. Berthelsen A: Fibrosarcoma in the thyroid gland: recurrencetreated with radiotherapy. J Laryngol Otol 92:933–936, 1978.
655. Heffess CS, Adair FF, Wenig BM: Paragangliomas of thethyroid gland (abstract). Int J Surg Pathol 2(suppl):188, 1995.
656. de Vries EJ, Watson CG: Paraganglioma of the thyroid. HeadNeck 11:462–465, 1989.
657. Bale GF: Teratoma of the neck in the region of the thyroidgland, a review of the literature and report of four cases.Am J Pathol 26:565–580, 1950.
658. Fisher JE, Cooney DR, Voorhess ML, Jewett TC Jr: Teratomaof thyroid gland in infancy: review of the literature and twocase reports. J Surg Oncol 21:135–140, 1982.
659. Kimler SC, Muth WF: Primary malignant teratoma of thethyroid: case report and literature review of cervical terato-mas in adults. Cancer 42:311–317, 1978.
660. Hajdu SI, Hajdu EO: Malignant teratoma of the neck. ArchPathol 83:567–570, 1967.
661. Bowker CM, Whittaker RS: Malignant teratoma of the thy-roid: case report and literature review of thyroid teratoma inadults. Histopathology 21:81–83, 1992.
662. Buckley NJ, Burch WM, Leight GS: Malignant teratoma inthe thyroid gland of an adult: a case report and a review ofthe literature. Surgery 100:932–937, 1986.
663. Ueno NT, Amato RJ, Ro JJ, Weber RS: Primary malignantteratoma of the thyroid gland: report and discussion of twocases. Head Neck 20:649–653, 1998.
664. Chen JS, Lai GM, Hsueh S: Malignant thyroid teratoma of anadult: a long-term survival after chemotherapy. Am J ClinOncol 21:212–214, 1998.
665. Ivy HK: Cancer metastatic to the thyroid: a diagnostic prob-lem. Mayo Clin Proc 59:856–859, 1984.
666. McCabe DP, Farrar WB, Petkov TM, et al: Clinical and path-ologic correlations in disease metastatic to the thyroid gland.Am J Surg 150:519–523, 1985.
667. Lam KY, Lo CY: Metastatic tumors of the thyroid gland: astudy of 79 cases in Chinese patients. Arch Pathol Lab Med122:37–41, 1998.
668. Nakhjavani MK, Gharib H, Goellner JR, van Heerden JA:Metastasis to the thyroid gland. A report of 43 cases. Cancer79:574–578, 1997.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
622. Mizukami Y, Nonomura A, Michigishi T, et al: Pseudolym-phoma of the thyroid gland. A case report. Pathol Res Pract192:166–169, discussion 170–171, 1996.
623. Thompson LD: Langerhans cell histiocytosis isolated to thethyroid gland. Eur Arch Otorhinolaryngol 253:62–65, 1996.
624. Thompson LDR, Wenig BM, Adair CF, Heffess CS: Periph-eral nerve sheath tumors of the thyroid gland, a series offour cases and a review of the literature. Endocr Pathol7:309–318, 1996.
625. Tsang WY, Lau MF, Chan JK: Incidental Langerhans’ cellhistiocytosis of the thyroid. Histopathology 24:397–399, 1994.
626. Coode PE, Shaikh MU: Histiocytosis X of the thyroid mas-querading as thyroid carcinoma. Hum Pathol 19:239–241,1988.
627. Wang WS, Liu JH, Chiou TJ, et al: Langerhans’ cell histiocy-tosis with thyroid involvement masquerading as thyroid car-cinoma. Jpn J Clin Oncol 27:180–184, 1997.
628. Kitahama S, Iitaka M, Shimizu T, et al: Thyroid involvementby malignant histiocytosis of Langerhans’ cell type. Clin En-docrinol (Oxf) 45:357–363, 1996.
629. Egloff B: The hemangioendothelioma of the thyroid. Vir-chows Arch A Pathol Anat Histopathol 400:119–142, 1983.
630. Maiorana A, Collina G, Cesinaro AM, et al: Epithelioid an-giosarcoma of the thyroid. Clinicopathological analysis ofseven cases from non-Alpine areas. Virchows Arch 429:131–137, 1996.
631. Eusebi V, Carcangiu ML, Dina R, Rosai J: Keratin-positiveepithelioid angiosarcoma of thyroid. A report of four cases.Am J Surg Pathol 14:737–747, 1990.
632. Lamovec J, Zidar A, Zidanik B: Epithelioid angiosarcoma ofthe thyroid gland. Report of two cases. Arch Pathol Lab Med118:642–646, 1994.
633. Ritter JH, Mills SE, Nappi O, Wick MR: Angiosarcoma-likeneoplasms of epithelial organs: true endothelial tumors orvariants of carcinoma? Semin Diagn Pathol 12:270–282,1995.
634. Mills SE, Stallings RG, Austin MB: Angiomatoid carcinomaof the thyroid gland. Anaplastic carcinoma with follicularand medullary features mimicking angiosarcoma. Am J ClinPathol 86:674–678, 1986.
635. Mills SE, Gaffey MJ, Watts JC, et al: Angiomatoid carcinomaand ’angiosarcoma’ of the thyroid gland. A spectrum of en-dothelial differentiation. Am J Clin Pathol 102:322–330,1994.
636. Taccagni G, Sambade C, Nesland J, et al: Solitary fibroustumour of the thyroid: clinicopathological, immunohisto-chemical and ultrastructural study of three cases. VirchowsArch A Pathol Anat Histopathol 422:491–497, 1993.
637. Cameselle-Teijeiro J, Varela-Duran J: CD34 and thyroid fi-brous tumor (letter). Am J Surg Pathol 19:1096, 1995.
638. Cameselle-Teijeiro J, Varela-Duran J, Fonseca E, et al: Soli-tary fibrous tumor of the thyroid. Am J Clin Pathol 101:535–538, 1994.
639. Kie JH, Kim JY, Park YN, et al: Solitary fibrous tumour ofthe thyroid. Histopathology 30:365–368, 1997.
640. Thompson LD, Wenig BM, Adair CF, et al: Primary smoothmuscle tumors of the thyroid gland. Cancer 79:579–587,1997.
641. Kawahara E, Nakanishi I, Terahata S, Ikegaki S: Leiomyosar-coma of the thyroid gland. A case report with a comparative
Copyright � 2003, Elsevier Science (USA). All rights Reserved
Thyroid and Parathyroid 93
669. Shimaoka K, Sokal JE, Pickren JW: Metastatic neoplasms ofthe thyroid. Cancer 15:557–565, 1962.
670. Carpenter GR, Emery JL: Inclusions in the human thyroid. JAnat 122:77–89, 1976.
671. LiVolsi VA, Merino MJ: Squamous cells in the human thy-roid gland. Am J Surg Pathol 2:133–140, 1978.
672. Reid JD, Choi CH, Oldroyd NO: Calcium oxalate crystals inthe thyroid. Their identification, prevalence, origin, and pos-sible significance. Am J Clin Pathol 87:443–454, 1987.
673. Katoh R, Suzuki K, Hemmi A, Kawaoi A: Nature and signif-icance of calcium oxalate crystals in normal human thyroidgland. A clinicopathological and immunohistochemicalstudy. Virchows Arch A Pathol Anat Histopathol 422:301–306, 1993.
674. Katoh R, Kawaoi A, Muramatsu A, et al: Birefringent (cal-cium oxalate) crystals in thyroid diseases. A clinicopathologi-cal study with possible implications for differential diagno-sis. Am J Surg Pathol 17:698–705, 1993.
675. Yamaoka Y: Solid cell nest (SCN) of the human thyroidgland. Acta Pathol Jpn 23:493–506, 1973.
676. Harach HR: Solid cell nests of the thyroid. J Pathol 155:191–200, 1988.
677. Ozaki O, Ito K, Sugino K, et al: Solid cell nests of the thy-roid gland. Virchows Arch A Pathol Anat Histopathol418:201–205, 1991.
678. Beckner ME, Shultz JJ, Richardson T: Solid and cystic ulti-mobranchial body remnants in the thyroid [see comments].Arch Pathol Lab Med 114:1049–1052, 1990.
679. Harach HR: Solid cell nests of the human thyroid in earlystages of postnatal life. Systematic autopsy study. Acta Anat127:262–264, 1986.
680. Carney JA, Moore SB, Northcutt RC, et al: Palpation thyroid-itis (multifocal granulomatous folliculitis). Am J Clin Pathol64:639–647, 1975.
681. Fernandez JF, Ordonez NG, Schultz PN, et al: Thyroglossalduct carcinoma. Surgery 110:928–934, discussion 934–935,1991.
682. Heshmati HM, Fatourechi V, van Heerden JA, et al: Thyro-glossal duct carcinoma: report of 12 cases. Mayo Clin Proc72:315–319, 1997.
683. O’Connell M, Grixti M, Harmer C: Thyroglossal duct carci-noma: presentation and management, including eight casereports. Clin Oncol 10:186–190, 1998.
684. Louis DN, Vickery AL Jr, Rosai J, Wang CA: Multiple bran-chial cleft– like cysts in Hashimoto’s thyroiditis [see com-ments]. Am J Surg Pathol 13:45–49, 1989.
685. Wenig BM, Heffess CS, Adair CF: Atlas of Endocrine Pathol-ogy. Philadelphia, WB Saunders, 1997.
686. Sampson RJ, Oka H, Key CR, et al: Metastases from occultthyroid carcinoma. An autopsy study from Hiroshima andNagasaki, Japan. Cancer 25:803–811, 1970.
687. Meyer JS, Steinberg LS: Microscopically benign thyroid folli-cles in cervical lymph nodes. Serial section study of lymphnode inclusions and entire thyroid glands in 5 cases. Cancer24:302–311, 1969.
688. Gerard-Marchant R, Caillou B: Thyroid inclusions in cer-vical lymph nodes. Clin Endocrinol Metab 10:337–349,1981.
689. Hazard JB: Thyroiditis: a review. Part II. Am J Clin Pathol25:399–423, 1955.
690. Volpe R: The pathology of thyroiditis. Hum Pathol 9:429–438, 1978.
691. Woolner LB, McConahey WM, Beahrs OH: Struma lym-phomatosa (Hashimoto’s thyroiditis) and related thyroidaldisorders. J Clin Endocrinol Metab 19:53–83, 1959.
692. Katz SM, Vickery AL: The fibrous variant of Hashimoto’sthyroiditis. Hum Pathol 5:161–170, 1974.
693. Greenberg AH, Czernichow P, Hung W, et al: Juvenilechronic lymphocytic thyroiditis: clinical, laboratory and his-tological correlations. J Clin Endocrinol Metab 30:293–301,1970.
694. Rallison ML, Dobyns BM, Keating FR, et al: Occurrence andnatural history of chronic lymphocytic thyroiditis in child-hood. J Pediatr 86:675–682, 1975.
695. Mizukami Y, Michigishi T, Nonomura A, et al: Postpartum
thyroiditis. A clinical, histologic, and immunopathologicstudy of 15 cases. Am J Clin Pathol 100:200–205, 1993.
696. Roti E, Emerson CH: Clinical review 29: Postpartum thyroid-itis. J Clin Endocrinol Metab 74:3–5, 1992.
697. Mizukami Y, Michigishi T, Hashimoto T, et al: Silent thy-roiditis: a histologic and immunohistochemical study. HumPathol 19:423–431, 1988.
698. Inada M, Nishikawa M, Naito K, et al: Reversible changes ofthe histological abnormalities of the thyroid in patients withpainless thyroiditis. J Clin Endocrinol Metab 52:431–435,1981.
699. Woolner LB, McConahey WM, Beahrs OH: Invasive fibrousthyroiditis (Riedel’s struma). J Clin Endocrinol Metab17:201–220, 1957.
700. Harach HR, Williams ED: Fibrous thyroiditis—an immuno-pathological study. Histopathology 7:739–751, 1983.
701. Schwaegerle SM, Bauer TW, Esselstyn CB Jr: Riedel’s thy-roiditis. Am J Clin Pathol 90:715–722, 1988.
702. Williams ED, Doniach I: The postmortem incidence of focalthyroiditis. J Pathol 83:255–264, 1962.
703. Mitchell JD, Kirkham N, Machin D: Focal lymphocytic thy-roiditis in Southampton. J Pathol 144:269–273, 1984.
704. Okayasu I, Hatakeyama S, Tanaka Y, et al: Is focal chronicautoimmune thyroiditis an age-related disease? Differencesin incidence and severity between Japanese and British. JPathol 163:257–264, 1991.
705. Weaver DR, Deodhar SD, Hazard JB: A characterization offocal lymphocytic thyroiditis. Cleve Clin Q 33:59–72, 1966.
706. Ghossein RA, Rosai J, Heffess C: Dyshormonogenetic goiter:a clinicopathologic study of 56 cases. Endocr Pathol 8:283–292, 1998.
707. Fadda G, Baloch ZW, LiVolsi VA: Dyshormonogenetic goiterpathology, a review. Int J Surg Pathol 7:125–131, 1999.
708. Baloch ZW, Wu H, LiVolsi VA: Post–fine-needle aspirationspindle cell nodules of the thyroid (PSCNT). Am J ClinPathol 111:70–74, 1999.
709. Tsang K, Duggan MA: Vascular proliferation of the thyroid.A complication of fine-needle aspiration. Arch Pathol LabMed 116:1040–1042, 1992.
710. Axiotis CA, Merino MJ, Ain K, Norton JA: Papillary endo-thelial hyperplasia in the thyroid following fine-needle aspi-ration. Arch Pathol Lab Med 115:240–242, 1991.
711. Hamed G, Heffess CS, Shmookler BM, Wenig BM: Amyloidgoiter. A clinicopathologic study of 14 cases and review ofthe literature. Am J Clin Pathol 104:306–312, 1995.
712. Villamil CF, Massimi G, D’Avella J, Cole SR: Amyloid goiterwith parathyroid involvement: a case report and review ofthe literature. Arch Pathol Lab Med 124:281–283, 2000.
713. Landas SK, Schelper RL, Tio FO, et al: Black thyroid syn-drome: exaggeration of a normal process? Am J Clin Pathol85:411–418, 1986.
714. Saul SH, Dekker A, Lee RE, Breitfeld V: The black thyroid.Its relation to minocycline use in man. Arch Pathol Lab Med107:173–177, 1983.
715. Reid JD: The black thyroid associated with minocycline ther-apy. A local manifestation of a drug-induced lysosome/sub-strate disorder. Am J Clin Pathol 79:738–746, 1983.
716. Medeiros LJ, Federman M, Silverman ML, Balogh K: Blackthyroid associated with minocycline therapy. Arch PatholLab Med 108:268–269, 1984.
717. Matsubara F, Mizukami Y, Tanaka Y: Black thyroid. Mor-phological, biochemical and geriatric studies on the browngranules in the thyroid follicular cells. Acta Pathol Jpn32:13–22, 1982.
718. Barsoum GH, Ryley NG, Barros D’Sa AA: Minocycline andblack thyroid. J R Coll Surg Edinb 35:387–388, 1990.
719. Senba M, Toda Y, Yamashita H: Black thyroid associatedwith minocycline therapy: histochemical and ultrastructuralstudies on the brown pigment. Isr J Med Sci 24:51–53, 1988.
720. Hecht DA, Wenig BM, Sessions RB: Black thyroid: a collabo-rative series. Otolaryngol Head Neck Surg 121:293–296,1999.
721. Landas SK, Marsh WL Jr, Schuller DE, et al: Nonpigmentedpapillary carcinoma in a black thyroid gland. Arch Otolaryn-gol Head Neck Surg 116:735–737, 1990.
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

94 Endocrine System
722. Onyia JN, Forrest LA, Forsthoefel K: Papillary carcinomaassociated with black thyroid gland. Am J Otolaryngol17:299–302, 1996.
723. Thompson AD, Pasieka JL, Kneafsey P, DiFrancesco LM: Hy-popigmentation of a papillary carcinoma arising in a blackthyroid. Mod Pathol 12:1181–1185, 1999.
724. Katoh R, Ishizaki T, Tomichi N, et al: Malacoplakia of thethyroid gland. Am J Clin Pathol 92:813–820, 1989.
725. Larkin DFP, Dervan PA, Munnelly J, et al: Sinus histiocytosiswith massive lymphadenopathy simulating subacute thyroid-itis. Hum Pathol 17:321–324, 1986.
726. Chan KW, Poon GP, Choi CH: Plasma cell granuloma of thethyroid. J Clin Pathol 39:1105–1107, 1986.
727. Holck S: Plasma cell granuloma of the thyroid. Cancer48:830–832, 1981.
728. Zingrillo M, Tardio B, Bisceglia M: Plasma cell granuloma ofthe thyroid associated with Hashimoto’s thyroiditis. J Endo-crinol Invest 18:460–464, 1995.
729. Schmid C, Beham A, Seewann HL: Extramedullary haemato-poiesis in the thyroid gland. Histopathology 15:423–425,1989.
730. Larsimont D, Hamels J, Fortunati D: Thyroid-gland malako-plakia with autoimmune thyroiditis. Histopathology 23:491–494, 1993.
731. Wynne AG, van Heerden J, Carney JA, Fitzpatrick LA: Para-thyroid carcinoma: clinical and pathologic features in 43 pa-tients. Medicine (Baltimore) 71:197–205, 1992.
732. Jenkins PJ, Satta MA, Simmgen M, et al: Metastatic parathy-roid carcinoma in the MEN2A syndrome. Clin Endocrinol(Oxf) 47:747–751, 1997.
733. Yoshimoto K, Endo H, Tsuyuguchi M, et al: Familial isolatedprimary hyperparathyroidism with parathyroid carcinomas:clinical and molecular features. Clin Endocrinol (Oxf) 48:67–72, 1998.
734. Prinz RA, Barbato AL, Braithwaite SS, et al: Prior irradiationand the development of coexistent differentiated thyroid can-cer and hyperparathyroidism. Cancer 49:874–877, 1982.
735. Russ JE, Scanlon EF, Sener SF: Parathyroid adenomas follow-ing radiation. Cancer 43:1078–1083, 1979.
736. Evans HL: Criteria for diagnosis of parathyroid carcinoma: acritical study. Surg Pathol 4:244–265, 1991.
737. DeLellis RA: Tumors of the Parathyroid Gland. Atlas of Tu-mor Pathology. Third Series, Fascicle 6. Washington, DC,Armed Forces Institute of Pathology, 1993.
738. Grimelius L, Akerstrom G, Johansson H, et al: The parathy-roid glands. In Kovacs K, Asa SL (eds): Functional EndocrinePathology. 2nd ed. Malden, MA, Blackwell Science, 1998,pp 381–414.
739. Matsushita H: Pathology of the parathyroid glands. In Lech-ago J, Gould VE (eds): Bloodworth’s Endocrine Pathology.3rd ed. Baltimore, Williams & Wilkins, 1997, pp 249–272.
740. Tominaga Y, Kohara S, Namii Y, et al: Clonal analysis ofnodular parathyroid hyperplasia in renal hyperparathyroid-ism. World J Surg 20:744–750, discussion 750–752, 1996.
741. Barry MK, van Heerden JA, Grant CS, et al: Is familial hy-perparathyroidism a unique disease? Surgery 122:1028–1033,1997.
742. Teh BT, Farnebo F, Twigg S, et al: Familial isolated hyper-parathyroidism maps to the hyperparathyroidism–jaw tumorlocus in 1q21–q32 in a subset of families. J Clin EndocrinolMetab 83:2114–2120, 1998.
743. Huang SM, Duh QY, Shaver J, et al: Familial hyperparathy-roidism without multiple endocrine neoplasia. World J Surg21:22–28, discussion 29, 1997.
744. Harach HR, Jasani B: Parathyroid hyperplasia in tertiary hy-perparathyroidism: a pathological and immunohistochemicalreappraisal. Histopathology 21:513–519, 1992.
745. Dotzenrath C, Goretzki PE, Farnebo F, et al: Molecular ge-netics of primary and secondary hyperparathyroidism. ExpClin Endocrinol Diabetes 104:105–107, 1996.
746. Agarwal SK, Kester MB, Debelenko LV, et al: Germline mu-tations of the MEN1 gene in familial multiple endocrineneoplasia type 1 and related states. Hum Mol Genet 6:1169–1175, 1997.
747. Kraimps JL, Denizot A, Carnaille B, et al: Primary hyper-
parathyroidism in multiple endocrine neoplasia type IIa: ret-rospective French multicentric study. Groupe d’Etude desTumeurs a Calcitonine (GETC, French Calcitonin TumorsStudy Group), French Association of Endocrine Surgeons.World J Surg 20:808–812, discussion 812–813, 1996.
748. Fitzpatrick LA: Hypercalcemia in the multiple endocrineneoplasia syndromes. Endocrinol Metab Clin North Am18:741–752, 1989.
749. Wang CA, Castleman B, Cope O: Surgical management ofhyperparathyroidism due to primary hyperplasia. Ann Surg195:384–392, 1982.
750. Dolgin C, Lo Gerfo P, LiVolsi V, Feind C: Twenty-five yearexperience with primary hyperparathyroidism at ColumbiaPresbyterian Medical Center. Head Neck Surg 2:92–98, 1979.
751. Heath H, Hodgson SF, Kennedy MA: Primary hyperparathy-roidism, incidence, morbidity and potential economic impactin a community. N Engl J Med 302:189–193, 1980.
752. Schantz A, Castleman B: Parathyroid carcinoma. A study of70 cases. Cancer 31:600–605, 1973.
753. Holmes EC, Morton DL, Ketcham AS: Parathyroid carci-noma: a collective review. Ann Surg 169:631–640, 1969.
754. Shane E, Bilezikian JP: Parathyroid carcinoma: a review of 62patients. Endocr Rev 3:218–226, 1982.
755. van Heerden JA, Weiland LH, ReMine WH, et al: Cancer ofthe parathyroid glands. Arch Surg 114:475–480, 1979.
756. Roth SI, Wang CA, Potts JT: The team approach to primaryhyperparathyroidism. Hum Pathol 6:645–648, 1975.
757. Harness JK, Ramsburg SR, Nishiyama RH, Thompson NW:Multiple adenomas of the parathyroids: do they exist? ArchSurg 114:468–474, 1979.
758. Verdonk CC, Edias AJ: Parathyroid “double adenomas”: factor fiction? Surgery 90:523–526, 1981.
759. Bartsch D, Nies C, Hasse C, et al: Clinical and surgical as-pects of double adenoma in patients with primary hyper-parathyroidism. Br J Surg 82:926–929, 1995.
760. Szabo E, Lundgren E, Juhlin C, et al: Double parathyroidadenoma, a clinically nondistinct entity of primary hyper-parathyroidism. World J Surg 22:708–713, 1998.
761. Sawady J, Mendelsohn G, Sirota RL, et al: The intrathyroidhyperfunctioning parathyroid gland. Mod Pathol 2:652–657,1989.
762. Russell CF, Edis AJ, Scholz DA, et al: Mediastinal parathy-roid tumors: experience with 38 tumors requiring mediasti-notomy for removal. Ann Surg 193:805–809, 1981.
763. Spiegel AM, Marx SJ, Doppman JL, et al: Intrathyroidalparathyroid adenoma or hyperplasia. An occasionally over-looked cause of surgical failure in primary hyperparathy-roidism. JAMA 234:1029–1033, 1975.
764. Nathaniels EK, Nathaniels AM, Wang C: Mediastinal para-thyroid tumours: a clinical and pathological study of 84cases. Ann Surg 171:165–170, 1970.
765. de la Cruz Vigo F, Ortega G, Gonzalez S, et al: Pathologicintrathyroidal parathyroid glands. Int Surg 82:87–90, 1997.
766. Summers GW: Parathyroid update: a review of 220 cases.Ear Nose Throat J 75:434–439, 1996.
767. Ordonez NG, Ibanez ML, Samaan NA, Hickey RC: Immuno-peroxidase study of uncommon parathyroid tumors. Reportof two cases of nonfunctioning parathyroid carcinoma andone intrathyroid parathyroid tumor producing amyloid. AmJ Surg Pathol 7:535–542, 1983.
768. Castleman B, Roth S: Tumors of the Parathyroid Glands.Atlas of Tumor Pathology. Second Series, Fascicle 14. Wash-ington, DC, Armed Forces Institute of Pathology, 1978.
769. Castleman B, Schantz A, Roth S: Parathyroid hyperplasia inprimary hyperparathyroidism: a review of 85 cases. Cancer38:1668–1675, 1976.
770. Grimelius L, Bondeson L: Histopathological diagnosis ofparathyroid diseases. Pathol Res Pract 191:353–365, 1995.
771. Loda M, Lipman J, Cukor B, et al: Nodular foci in parathy-roid adenomas and hyperplasias: an immunohistochemicalanalysis of proliferative activity. Hum Pathol 25:1050–1056,1994.
772. Lawton TJ, Feldman M, LiVolsi VA: Lymphocytic infiltratesin solitary parathyroid adenomas, a report of four cases withreview of the literature. Int J Surg Pathol 6:5–10, 1998.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved
Thyroid and Parathyroid 95
773. Veress B, Nordenstrom J: Lymphocytic infiltration and de-struction of parathyroid adenomas: a possible tumour-spe-cific autoimmune reaction in two cases of primary hyper-parathyroidism. Histopathology 25:373–377, 1994.
774. Leedham PW, Pollock DJ: Intrafollicular amyloid in primaryhyperparathyroidism. J Clin Pathol 23:811–817, 1970.
775. Sahin A, Robinson RA: Papillae formation in parathyroidadenoma, a source of possible diagnostic error. Arch PatholLab Med 122:99–100, 1988.
776. Abdul-Haj SK, Conklin H, Hewitt WC: Functioning lipoad-enoma of the parathyroid gland, report of a unique case. NEngl J Med 266:121–123, 1962.
777. Daroca PJ Jr, Landau RL, Reed RJ, Kappelman MD: Func-tioning lipoadenoma of the parathyroid gland. Arch PatholLab Med 101:28–29, 1977.
778. Obara T, Fujimoto Y, Ito Y, et al: Functioning parathyroidlipoadenoma—report of four cases: clinicopathological andultrasonographic features. Endocrinol Jpn 36:135–145, 1989.
779. Perosio P, Brooks JJ, LiVolsi VA: Orbital brown tumor asinitial manifestation of parathyroid lipoadenoma. SurgPathol 1:77–82, 1988.
780. Turner WJ, Baergen RN, Pellitteri PK, Orloff LA: Parathyroidlipoadenoma: case report and review of the literature. Otola-ryngol Head Neck Surg 114:313–316, 1996.
781. Weiland LH, Garrison RC, ReMine WH, Scholz DA: Lipoad-enoma of the parathyroid gland. Am J Surg Pathol 2:3–7,1978.
782. Wolff M, Goodman EN: Functioning lipoadenoma of a su-pernumerary parathyroid gland in the mediastinum. HeadNeck Surg 2:302–307, 1980.
783. Ho KJ: Papillary parathyroid adenoma. A rare occurrenceand its importance in differentiation from papillary carci-noma of the thyroid. Arch Pathol Lab Med 120:883–884,1996.
784. Roth SI: Water-clear cell ’adenoma.’ A new entity in thepathology of primary hyperparathyroidism (editorial; com-ment). Arch Pathol Lab Med 119:996–997, 1995.
785. Grenko RT, Anderson KM, Kauffman G, Abt AB: Water-clear cell adenoma of the parathyroid. A case report withimmunohistochemistry and electron microscopy. Arch PatholLab Med 119:1072–1074, 1995.
786. Bedetti CD, Dekker A, Watson CG: Functioning oxyphil celladenoma of the parathyroid gland: a clinicopathologic studyof ten patients with hyperparathyroidism. Hum Pathol 15:1121–1126, 1984.
787. Natsui K, Tanaka K, Suda M, et al: Oxyphil parathyroidadenoma associated with primary hyperparathyroidism andmarked postoperative hungry bone syndrome. Intern Med35:545–549, 1996.
788. Wolpert HR, Vickery AL Jr, Wang CA: Functioning oxyphilcell adenomas of the parathyroid gland. A study of 15 cases.Am J Surg Pathol 13:500–504, 1989.
789. Weiler R, Fischer-Colbrie R, Schmid KW, et al: Immunologi-cal studies on the occurrence and properties of chromo-granin A and B and secretogranin II in endocrine tumors.Am J Surg Pathol 12:877–884, 1988.
790. Miettinen M, Clark R, Lehto VP, et al: Intermediate-filamentproteins in parathyroid glands and parathyroid adenomas.Arch Pathol Lab Med 109:986–989, 1985.
791. Mendelsohn G: Pathology of the parathyroid glands. In Men-delsohn G (ed): Diagnosis and Pathology of Endocrine Dis-eases. Philadelphia, JB Lippincott, 1988, pp 139–177.
792. Vargas MP, Vargas HI, Kleiner DE, Merino MJ: The role ofprognostic markers (MiB-1, RB, and bcl-2) in the diagnosis ofparathyroid tumors. Mod Pathol 10:12–17, 1997.
793. Abbona GC, Papotti M, Gasparri G, Bussolati G: Proliferativeactivity in parathyroid tumors as detected by Ki-67 immuno-staining. Hum Pathol 26:135–138, 1995.
794. Erickson LA, Jin L, Wollan P, et al: Parathyroid hyperplasia,adenomas, and carcinomas: differential expression ofp27/KipI protein. Am J Surg Pathol 23:288–295, 1999.
795. Arnold A, Staunton CE, Kim HG, et al: Monoclonality andabnormal parathyroid hormone genes in parathyroid adeno-mas. N Engl J Med 318:658–662, 1988.
796. Marx SJ: Genetic defects in primary hyperparathyroidism(editorial). N Engl J Med 318:699–701, 1988.
797. Grimelius L, Johansson H: Pathology of parathyroid tumors.Semin Surg Oncol 13:142–154, 1997.
798. Hsi ED, Zukerberg LR, Yang WI, Arnold A: Cyclin D1/PRAD1 expression in parathyroid adenomas: an immunohis-tochemical study. J Clin Endocrinol Metab 81:1736–1739,1996.
799. Abati A, Skarulis MC, Shawker T, Solomon D: Ultrasound-guided fine-needle aspiration of parathyroid lesions: a mor-phological and immunocytochemical approach. Hum Pathol26:338–343, 1995.
800. Arnold A: Molecular mechanisms of parathyroid neoplasia.Endocrinol Metab Clin North Am 23:93–107, 1994.
801. Arnold A, Motokura T, Bloom T, et al: PRAD1 (cyclin D1): aparathyroid neoplasia gene on 11q13. Henry Ford Hosp MedJ 40:177–180, 1992.
802. Vasef MA, Brynes RK, Sturm M, et al: Expression of cyclinD1 in parathyroid carcinomas, adenomas, and hyperplasias:a paraffin immunohistochemical study. Mod Pathol 12:412–416, 1999.
803. Heppner C, Kester MB, Agarwal SK, et al: Somatic mutationof the MEN1 gene in parathyroid tumours. Nat Genet16:375–378, 1997.
804. Shan L, Nakamura Y, Nakamura M, et al: Somatic mutationsof multiple endocrine neoplasia type 1 gene in the sporadicendocrine tumors. Lab Invest 78:471–475, 1998.
805. Palanisamy N, Imanishi Y, Rao PH, et al: Novel chromo-somal abnormalities identified by comparative genomic hy-bridization in parathyroid adenomas. J Clin Endocrinol Me-tab 83:1766–1770, 1998.
806. LiVolsi VA, Hamilton R: Intraoperative assessment of para-thyroid gland pathology. A common view from the surgeonand the pathologist. Am J Clin Pathol 102:365–373, 1994.
807. Silver CE, Owen RP: Year 2000 update: what the head andneck surgeon expects of the pathologist. Pathol Case Rev5:183–188, 2000.
808. Westra WH, Pritchett DD, Udelsman R: Intraoperative con-firmation of parathyroid tissue during parathyroid explora-tion: a retrospective evaluation of the frozen section. Am JSurg Pathol 22:538–544, 1998.
809. Dekker A, Watson CG, Barnes EL: The pathologic assess-ment of primary hyperparathyroidism and its impact ontherapy, a prospective evaluation of 50 cases with oil-red-Ostain. Ann Surg 190:671–675, 1979.
810. Ljungberg O, Tibblin S: Perioperative fat staining of frozensections in primary hyperparathyroidism. Am J Pathol95:633–641, 1979.
811. Roth SI, Gallagher MJ: The rapid identification of “normal”parathyroid glands by the presence of intracellular fat. Am JPathol 84:521–528, 1976.
812. Sasano H, Geelhoed GW, Silverberg SG: Intraoperative cyto-logic evaluation of lipid in the diagnosis of parathyroid ade-noma. Am J Surg Pathol 12:282–286, 1988.
813. Dufour DR, Durkowski C: Sudan IV stain. Its limitations inevaluating parathyroid functional status. Arch Pathol LabMed 106:224–227, 1982.
814. Kasdon EJ, Rosen S, Cohen RB, Silen W: Surgical pathologyof hyperparathyroidism. Usefulness of fat stain and prob-lems in interpretation. Am J Surg Pathol 5:381–384, 1981.
815. King DT, Hirose FM: Chief cell intracytoplasmic fat used toevaluate parathyroid disease by frozen section. Arch PatholLab Med 103:609–612, 1979.
816. Clarke MR, Hoover WW, Carty SE, et al: Atypical fat stain-ing patterns in hyperparathyroidism. Int J Surg Pathol 3:163–168, 1996.
817. Black WC, Utley JR: The differential diagnosis of parathyroidadenoma and chief cell hyperplasia. Am J Pathol 49:761–775,1968.
818. Kay S: The abnormal parathyroid. Hum Pathol 7:127–138,1976.
819. Black WC, Haff RC: The surgical pathology of parathyroidchief cell hyperplasia. Am J Clin Pathol 53:565–579, 1970.
820. Sofferman RA, Standage J, Tang ME: Minimal-access para-thyroid surgery using intraoperative parathyroid hormoneassay. Laryngoscope 108:1497–1503, 1998.
821. Garner SC, Leight GS Jr: Initial experience with intraopera-
38419 Weidner (SAUNM) RIGHT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved

96 Endocrine System
tive PTH determinations in the surgical management of 130consecutive cases of primary hyperparathyroidism. Surgery126:1132–1137, discussion 1137–1138, 1999.
822. Chapuis Y, Fulla Y, Bonnichon P, et al: Values of ultrasonog-raphy, sestamibi scintigraphy, and intraoperative measure-ment of 1–84 PTH for unilateral neck exploration of primaryhyperparathyroidism. World J Surg 20:835–839, discussion839–840, 1996.
823. Aldinger KA, Hickey RC, Ibanez ML, Samaan NA: Parathy-roid carcinoma: a clinical study of seven cases of functioningand two cases of nonfunctioning parathyroid cancer. Cancer49:388–397, 1982.
824. Shortell CK, Andrus CH, Phillips CE Jr, Schwartz SI: Carci-noma of the parathyroid gland: a 30-year experience. Sur-gery 110:704–708, 1991.
825. Park ST, Condemi G, Shakir KM, et al: Parathyroid carci-noma: report of three cases and review of the literature. MilMed 163:246–249, 1998.
826. Chow E, Tsang RW, Brierley JD, Filice S: Parathyroid carci-noma—the Princess Margaret Hospital experience. Int J Ra-diat Oncol Biol Phys 41:569–572, 1998.
827. Cohn K, Silverman M, Corrado J, Sedgewick C: Parathyroidcarcinoma: the Lahey Clinic experience. Surgery 98:1095–1100, 1985.
828. Cordeiro AC, Montenegro FL, Kulcsar MA, et al: Parathy-roid carcinoma. Am J Surg 175:52–55, 1998.
829. McPheeters GO, Bender CA: Parathyroid carcinoma: a casereport and review. Hawaii Med J 44:104–108, 1985.
830. Shane E: Parathyroid carcinoma. Curr Ther Endocrinol Me-tab 6:565–568, 1997.
831. Vetto JT, Brennan MF, Woodruff J, Burt M: Parathyroid car-cinoma: diagnosis and clinical history. Surgery 114:882–892,1993.
832. Vazquez-Quintana E: Parathyroid carcinoma: diagnosis andmanagement. Am Surg 63:954–957, 1997.
833. Wang CA, Gaz RD: Natural history of parathyroid carci-noma. Diagnosis, treatment, and results. Am J Surg 149:522–527, 1985.
834. Anderson BJ, Samaan NA, Vassilopoulou-Sellin R, et al: Par-athyroid carcinoma: features and difficulties in diagnosis andmanagement. Surgery 94:906–915, 1983.
835. Bondeson L, Sandelin K, Grimelius L: Histopathological vari-ables and DNA cytometry in parathyroid carcinoma. Am JSurg Pathol 17:820–829, 1993.
836. Obara T, Fujimoto Y, Yamaguchi K, et al: Parathyroid carci-noma of the oxyphil cell type. A report of two cases, lightand electron microscopic study. Cancer 55:1482–1489, 1985.
837. Nasser G, Loberant N, Salameh A, et al: Oxyphil cell carci-noma of the parathyroid: a rare cause of hyperparathyroid-ism. Clin Oncol 7:323–324, 1995.
838. Chan JK, Tsang WY: Endocrine malignancies that maymimic benign lesions. Semin Diagn Pathol 12:45–63, 1995.
839. Chaitin BA, Goldman RL: Mitotic activity in benign parathy-roid disease (letter). Am J Clin Pathol 76:363–364, 1981.
840. Snover DC, Foucar K: Mitotic activity in benign parathyroiddisease. Am J Clin Pathol 75:345–347, 1981.
841. Cryns VL, Thor A, Xu HJ, et al: Loss of the retinoblastomatumor-suppressor gene in parathyroid carcinoma [see com-ments]. N Engl J Med 330:757–761, 1994.
842. Cryns VL, Rubio MP, Thor AD, et al: p53 abnormalities in
human parathyroid carcinoma. J Clin Endocrinol Metab78:1320–1324, 1994.
843. Vainas IG, Tsilikas C, Grecu A, et al: Metastatic parathyroidcarcinoma (mPCa): natural history and treatment of a case. JExp Clin Cancer Res 16:429–432, 1997.
844. DeLellis RA: Proliferation markers in neuroendocrine tu-mors: useful or useless? A critical reappraisal. Verh DtschGes Pathol 81:53–61, 1997.
845. Bowlby LS, DeBault LE, Abraham SR: Flow cytometric DNAanalysis of parathyroid glands. Relationship between nuclearDNA and pathologic classifications. Am J Pathol 128:338–344, 1987.
846. Bocsi J, Perner F, Szucs J, et al: DNA content of parathyroidtumors. Anticancer Res 18:2901–2904, 1998.
847. Obara T, Fujimoto Y, Hirayama A, et al: Flow cytometricDNA analysis of parathyroid tumors with special referenceto its diagnostic and prognostic value in parathyroid carci-noma. Cancer 65:1789–1793, 1990.
848. Obara T, Fujimoto Y, Kanaji Y, et al: Flow cytometric DNAanalysis of parathyroid tumors. Implication of aneuploidyfor pathologic and biologic classification. Cancer 66:1555–1562, 1990.
849. Levin KE, Chew KL, Ljung BM, et al: Deoxyribonucleic acidcytometry helps identify parathyroid carcinomas. J Clin En-docrinol Metab 67:779–784, 1988.
850. Levin KE, Galante M, Clark OH: Parathyroid carcinoma ver-sus parathyroid adenoma in patients with profound hyper-calcemia. Surgery 101:649–660, 1987.
851. Fujimoto Y, Obara T, Ito Y, et al: Surgical treatment of tencases of parathyroid carcinoma: importance of an initial enbloc tumor resection. World J Surg 8:392–400, 1984.
852. Obara T, Okamoto T, Kanbe M, Iihara M: Functioning para-thyroid carcinoma: clinicopathologic features and rationaltreatment. Semin Surg Oncol 13:134–141, 1997.
853. Stevenson HU: Malignant tumours of the parathyroid gland:a review of the literature with report of a case. Arch Surg60:247–266, 1950.
854. Palmer M, Ljunghall S, Akerstrom G, et al: Patients withprimary hyperparathyroidism operated on over a 24-year pe-riod: temporal trends of clinical and laboratory findings. JChronic Dis 40:121–130, 1987.
855. Roth SI: The ultrastructure of primary water-clear cell hyper-plasia of the parathyroid glands. Am J Pathol 61:233–248,1970.
856. Dawkins RL, Tashjian AH Jr, Castleman B, Moore EW: Hy-perparathyroidism due to clear cell hyperplasia. Serial deter-minations of serum ionized calcium, parathyroid hormoneand calcitonin. Am J Med 54:119–126, 1973.
857. Rangnekar N, Bailer WJ, Ghani A, et al: Parathyroid cysts.Report of four cases and review of the literature. Int Surg81:412–414, 1996.
858. Alvi A, Myssiorek D, Wasserman P: Parathyroid cyst: cur-rent diagnostic and management principles. Head Neck18:370–373, 1996.
859. Carney JA: Salivary heterotopia, cysts, and the parathyroidgland: branchial pouch derivatives and remnants. Am J SurgPathol 24:837–845, 2000.
860. Koelmeyer TD: Generalised amyloidosis with involvementof the parathyroids: case report. N Z Med J 85:372–373,1977.
38419 Weidner (SAUNM) LEFT INTERACTIVE
shortstandardlong
top of RH
Copyright � 2003, Elsevier Science (USA). All rights Reserved