Thyroid gland
34
-
Upload
soumyadev-satpathy -
Category
Education
-
view
2.429 -
download
2
description
examination of thyroid gland
Transcript of Thyroid gland


The examination consists of three portions:
Inspection, Palpation, and Synthesis of data from these techniques

AGE:
Puberty- simple goitre,papillary carcinoma,
Middle age- multinodular goitre,colloid goitre,follicular carcinoma. Old age- Anaplastic carcinoma

SEX:Simple goitre is more common in Females
thyrotoxicosis is 8 times more common in females. Thyroid carcinoma is more often seen in females 3:1.
OCCUPATION:Thyrotoxicosis is common in people working under
stress and strain. .

RESIDENCE:Goitre belts in india like Himalayas, Vindyas,
Satpuda ranges. Areas producing chalk or lime stone like Derbyshire

SWELLING;
DURATION;
ASSOCIATED PAIN;

1.DESCRIBE IN DETAILS ONSET AND PROGRESSION OF THE SWELLING, 2.PRESSURE EFFECTS; 3.SYMPOTOMS OF HYPOTHYROIDISM
4.SYMPOTOMS OF HYPERTHYROIDISM; 5.SYMPTOMS OF MALIGANANCY.

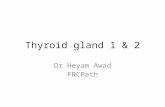
Tilt the patients head back a bit
Use tangential lighting from the tip of the patients chin
Ask for swallowing
Observe the thyroid cartilage, cricoid cartilage and the thyroid gland raising with swallowing

Inspection: Anterior Approach
The patient should be seated or standing in a comfortable position with the neck in a neutral or slightly extended position.
Cross-lighting increases shadows, improving the detection of masses.
To enhance visualization of the thyroid, you can: Extending the neck, which stretches overlying
tissues Have the patient swallow a sip of water, watching
for the upward movement of the thyroid gland.

Inspection: Lateral Approach After completing anterior inspection of the
thyroid, observe the neck from the side. Estimate the smooth, straight contour from
the cricoid cartilage to the suprasternal notch. Measure any prominence beyond this
imagined contour, using a ruler placed in the area of prominence.

• Size : ……X………..• Shape : Ovoid / Spherical / Irregular• Location: One side / mid line / both sides of
mid line• Extent: Horizontal from Sternomastoid…
Vertical from Suprasternal Notch… The swelling is: Under Sternomastoid / Not
under sternum• Surface: Smooth / Nodular / Bosselated

• Skin over the swelling:Redness and edema, Scars of previous surgery, Sinuses, Dilated veins
• Pulsatility : Present / Absent
• Movement with Deglutition: Present / Absent
• Protrusion of Tongue (For midline swellings): Present / Absent

Do not press to much the thyroid
You can loose the sensitivity of your fingers
Try to not strangle your patient

The following information could be obtained
volume consistency mobility of the thyroid gland surface temperature

Palpate the thyroid gland from behind
Localize anatomic boundaries
Thyroid isthmus is often palpable
Thyroid lobes are barely or not palpable
The consistency is rubbery, similar to that of sternomastoid muscle

Temperature: Normal / Raised Tenderness : Present / Absent Size: … X … Shape: Ovoid / Spherical / Irregular Extent: Horizontal from Sternomastoid…
Vertical from Suprasternal Notch… Plane of the swelling : Under Sternomastoid /
Under Strap muscles/ Deep to deep fascia.

A) In case of affection of entire gland,• i) Surface : Smooth / Bosselated• ii) Consistency : Uniform (Soft / Firm / Hard) /
Variable• iii) Retrosternal Extension : Present / AbsentB)In case of Single Nodule Or One Lobe affection• i) Location : Lobe / Isthmus• ii)Consistency: Soft / Firm• iii) Is the rest of the gland palpable ? Yes / No

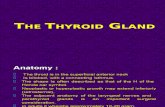
• Stand behind the pt.
• Place your hands around the neck with the thumbs over the occiput and tips of the other fingers over the front of the neck.
• Flex the neck to relax deep cervical fascia.
• Ask the pt to swallow to look for lower border and nodules.
• To palpate anterior surface, incline the head to the side being examined to relax overlying sternomastoid muscle.

Palpation: Anterior Approach
1. The patient is examined in the seated or standing position.
2. Attempt to locate the thyroid isthmus by palpating between the cricoid cartilage and the suprasternal notch.
3. Use one hand to slightly retract the sternocleidomastoid muscle while using the other to palpate the thyroid.
4. Have the patient swallow a sip of water as you palpate, feeling for the upward movement of the thyroid gland.

Palpation: Posterior Approach
1. The patient is examined in the seated or standing position.
2. Standing behind the patient, attempt to locate the thyroid isthmus by palpating between the cricoid cartilage and the suprasternal notch.
3. Move your hands laterally to try to feel under the sternocleidomstoids for the fullness of the thyroid.
4. Have the patient swallow a sip of water as you palpate, feeling for the upward movement of the thyroid gland.

Stand in front of the patient. Extend the neck slightly. Keep a thumb over the lobe to be examined. Ask the pt to swallow. Feel for small nodules.

• In short and flat neck ————Pizillo’s Method makes gland prominent
• Ask pt to clasp his hands over the occiput• Push the head backwards against the resistance
of the clasped hand

Done to palpate deep or postero medial surface of the gland.
Stand in front of the patient. Extend the neck slightly. Push the thyroid gland laterally to displace it
from tracheo esophageal groove. Palpate the posterior surface for nodules with
other hand.

• Done in large, bilateral goiter to rule out tracheal narrowing.
• Extend the neck.• Ask the patient to take deep breaths through the
mouth.• Compress the swelling from both the sides.• Appearance of stridor with slight compression of
lateral lobes due to Narrowing of trachea ( Scabbard trachea).it is seen in case of large and longstanding multinodular goiter and Ca thyroid infiltrating trachea.

Lahey’s Method of Palpation of Thyroid: Nodules Present / Absent,If present consistency of nodule
Crile’s Method of Palpation of Thyroid: Nodules Present / Absent
Palpabale Thrill : Present / Absent Fixity to skin : Fixed / Not Fixed Mobility : Horizontally Mobile / Fixed ;Vertically
Mobile / Fixed Palpation of Trachea : Palpable / Not Palpable,
Deviated / Not deviated Kocher’s Test : Positive / Negative Palpation of carotids : Berry’s Sign Positive / Negative

Percussion over sternum : Resonant / Dull
Ascultaion of gland : where to ascultate? Lower pole or
Upper pole? why?

Hoarseness of voice : Present / Absent Edema of face and legs: Present / Absent Delayed relaxation of deep reflexes : Ankle
jerk ,Knee jerk History of lethargy: Present / Absent

Dilated veins : Present / Absent Congestion and puffiness of face: Present / Absent Palpate for tracheal rings: Present / Absent Percuss over sternum: Resonant / Dull Pemberton’s sign: Positive / Negative Horners syndrome: (Ptosis,Constricted pupil,
Enophthalmos, Absent cilio-spinal reflex, Anhydrosis) : Present / Absent

Eye signs Lid retraction : Dalrymple’s sign : Present / Absent Lid lag : Von Graeffe’s sign: Present / Absent Incomplete, infrequent blinking: Stellwag’s sign : Present /
Absent Exophthalmos : strip of sclera under inf limbus: Present /
Absent Naffziger’s Method : Present / Absent Wrinkling of forehead : Joffroy’s sign : Present / Absent Eversion of upper eye lid : Gifford’s sign: Positive / Negative Convergence : Mobius’ sign : Present / Absent Chemosis: Congestion and edema of conjunctiva, Corneal ulcers, diminished vision , Ophthalmoplegia

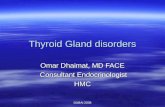
To note the amount and the degree of exophthalmos.
Stand behind the patient. See from above. Observe the eyes in supraorbital plane,if corneal
limbus is visible then it is exophthalmos.

Tremors : Outstretched Hand : Present / Absent Protruded tongue: Present / Absent Tachycardia : Heart rate = …. Bounding pulse:
Present / Absent Warm and moist skin : Present / Absent Pretibial Myxoedema : Present / Absent Bruit, Thrill: Present / Absent

Neck : Enlarged and hard lymph nodes. Skull surface : Hard nodules. Long bones : Deformity and tenderness. Chest : Effusion and consolidation. Abdomen : Nodular Liver and ascites.

Berry’s sign: Palpate the Carotid pulsations against the transverse process of the 6th cervical vertebra b/w post border of thyroid and sternomastiod.
In Ca thyroid, Carotid pulsations is weak or absent. Due to Infiltration of carotid sheath .
In benign goiter pulsations are well felt as carotid sheath pushed backwards.