Thyroid Disorders: Hyper and Hypothyroidism Year II, Unit II Unit-directed Activity AMEL ARNAOUT,...
43
Thyroid Disorders: Hyper and Hypothyroidism Year II, Unit II Unit-directed Activity AMEL ARNAOUT, MD
-
Upload
joshua-barton -
Category
Documents
-
view
214 -
download
0
Transcript of Thyroid Disorders: Hyper and Hypothyroidism Year II, Unit II Unit-directed Activity AMEL ARNAOUT,...

Thyroid Disorders: Hyper and Hypothyroidism
Year II, Unit II
Unit-directed Activity
AMEL ARNAOUT, MD

You may only access and use this presentation for educational purposes. You may not post this presentation online or distribute it without the permission of the author.
Disclosure
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Describe important signs & symptoms of hyperthyroidism Describe important signs & symptoms of hypothyroidism Discuss the use of thyroid function tests in the diagnosis of
hypothyroidism Discuss common causes of primary & secondary hypothyroidism Discuss the use of thyroid function tests in the diagnosis of
hyperthyroidism Describe the pathophysiology of hyperthyroid Graves’ disease Outline and describe acute, subacute & chronic thyroiditis Describe the clinical course of postpartum thyroiditis Describe the three phases of subacute thyroiditis
Objectives
Unit II – Thyroid Disorders: Hyper and Hypothyroidism – D. Liu

Case 1
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Ms. Lee is a 56-year old woman who has been your patient for 10 years.
She is normally healthy and active. During a routine check-up, she complains of
fatigue and 10 lb weight gain in 6 months.
Hypothyroidism is on the differential diagnosis. What other information will you ask for on history?
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Additional History: Chronic constipation Hot flashes since menopause Weight increased despite stable diet &
activity PMHx: Borderline HTN & dyslipidemia Meds: Multivitamin, no other supplements FHx: Hypothyroidism in aunts
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

What signs might you expect to find on physical exam?
General appearance: Vitals: Head & neck: Resp: CVS: Abdo: MSK: Neuro:
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
BP 135/90, HR 65
Small, firm thyroid – no nodule

Which of the following tests would you order?
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
TSH Free T3 Total T3 Free T4 Total T4 Thyroid ultrasound Thyroid uptake &
scan
Anti-microsomal antibodies
Anti-thyroglobulin antibodies
Thyroxine binding inhibitory immunoglobulin (TBII)

Investigations
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Test Result Reference Range Units
TSH 34.3 0.35 – 5.0 mU/L
Free T4 5.7 7.0 - 17.0 pmol/L
Free T3 3.2 3.3 – 6.0 pmol/L
What treatment would you recommend?
What is your plan for follow up?
What is the diagnosis?

Diagnosis: Primary hypothyroidism Treatment: Levothyroxine (T4) titrated to achieve a
normal TSH Repeat blood work (TSH) 6 weeks after initiating
treament

What if these were her lab results?
Case 1: Ms. Lee
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Test Result Reference Range Units
TSH 9.5 0.35 – 5.0 mU/L
Free T4 10.8 7.0 - 17.0 pmol/L
Free T3 4.3 3.3 – 6.0 pmol/L
What are the indications for treating subclinical hypothyroidism?

• Indications for treatment of SCH:• TSH >10• Significant symptoms of hypothyroidism• Hyperlipidemia• Depression• Women of childbearing age• Positive anti-TPO antibodies

Case 2
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 2: Mrs. Healthnut
40 yr old female with small goitre (symmetric enlargement, no palpable nodules).
Surgeon advised she does not need surgery.
She read on the internet that taking kelp might shrink her thyroid gland.
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 2: Mrs. Healthnut
What are possible consequences of taking kelp and the mechanisms involved?
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
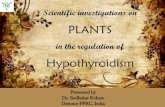
HO O CH2 CHCOOH
NH2
I
I I
I
T4: 4 iodine atomsRemoved when converted to T3

• Kelp contains iodine which acts as a substrate for thyroid hormone synthesis
• An increase in iodine in the diet MAY cause an increase in formation of thyroid hormones T4 and T3 which MAY cause a slight increase in circulating Free T4 and Free T3 levels which MAY suppress TSH.
• A lower TSH causes gland to shrink

Case 3
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 3: Ms. Newmum
Ms. N has a 5-month old baby. She was coping well, but now has symptoms suggestive of thyrotoxicosis.
Describe symptoms of thyrotoxicosis.
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

What signs might you expect to find on physical exam?
General appearance: Vitals: Head & neck:
Resp: CVS: Abdo: MSK: Neuro:
Case3: Ms. Newmum
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
BP 140/80, HR 95
Eyes: Lid lag, no proptosisThyroid 2 x normal size, no nodule
S1 S2 & systolic flow murmur
Fine tremor in hands

Which of the following tests would you order?
Case 3: Ms. Newmum
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
TSH Free T3 Total T3 Free T4 Total T4 Thyroid ultrasound Thyroid uptake &
scan
Anti-microsomal antibodies
Anti-thyroglobulin antibodies
Thyroxine binding inhibitory immunoglobulin (TBII)

Investigations
Case 3: Ms. Newmum
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Test Result Reference Range Units
TSH 0.06 0.35 – 5.0 mU/L
Free T4 33 7.0 - 17.0 pmol/L
Free T3 10.4 3.3 – 6.0 pmol/L
What is the differential diagnosis?
Which test(s) will you order next?

Case 5: Mrs. New Baby
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Case 3: Ms. Newmum
24 hr uptake: 47% (6-22%)

What is her diagnosis?
What is the pathophysiology of this condition?
How can this condition be treated?
What are potential adverse effects of the treatment options?
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Case 3: Ms. Newmum

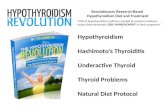
Thyroid Gland
I- I-
MIT T3 T3
Po Po P
DIT T4 T4
Thyroglobin
MIT
I- DIT
ID
T4 5’deiodinase T3Periphery
Periphery
PTU, MMI
Iopanoic Acid, Ipodate
Inorganic Iodine
PTU Steroids
Iodine
Na+ Na+

With plans to have another pregnancy, Ms. N opted to be treated with 131-iodine. She is euthyroid on thyroid hormone replacement 4 months after thyroid ablation.
She is worried about how Graves’ disease will affect her pregnancy and baby. What would you advise?
Unit II – Thyroid Disorders: Hyper and Hypothyroidism
Case 3: Ms. Newmum

Case 4
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 4: Mr. Payne
Mr. Payne is normally stoic
He presents with new neck pain, irritability, rapid weight loss in the last week, heat intolerance and palpitations.
What is the likely cause of his thyrotoxicosis?
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

THYROIDITIS
Thyroiditis with pain and tenderness:
• acute infectious (rare)
• subacute granulomatous thyroiditis (common)

SUBACUTE GRANULOMATISTHYROIDITIS
• subacute thyroiditis or DeQuervains’ thyroiditis, likely viral
• three phases: hyperthyroid,hypothyroid recovery phase
• treatment: NSAID or prednisone for pain, b-blocker for hyperthyroid symptoms, L-T4 not usually necessary

Thyroiditis

Case 4: Mr. Payne
What investigations are appropriate? Discuss the expected results. What treatments would you consider
recommending for this condition? What is the expected clinical course for Mr. N? Discuss the clinical course of acute and chronic
thyroiditis.
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 5
Unit II – Thyroid Disorders: Hyper and Hypothyroidism

Case 5
• 26 yr old woman with 6 wk history of agitation, tremors, palpitations, 20 lb wt loss, diarrhea
• PHX: unremarkable• no meds• O/E
– BP 170/62, HR 132 irreg irreg, RR 23, temp 39o
– agitated, flight of ideas, tremulous– exophthalmus, lid lag, stare, chemosis– thyroid 4x normal, diffuse with bruit– few basilar crackles

Thyroid Storm
• Very rare• high mortality (20-30%)• When to suspect
– often have a history of thyroid disease– have all the usual features of thyrotoxicosis– often have very large goiter– often a ppting illness/event
• surgery, infection, pregnancy, iodinated contrast dye

Thyroid Storm
• Life threatening exacerbation of the hyperthyroid state• Decompensation of organ systems• Fatal if untreated• Mortality rate of 20 - 30%• Most common in patients with thyrotoxicosis secondary to Graves disease

Thyroid Storm:Clinical Presentation
• Features of thyrotoxicosis• History of thyroid disease, or symptoms
consistent with prolonged thyrotoxicosis• Fever• Systolic Hypertension, widened pulse preassure• Tachycardia, Atrial arrythmias• Mental status change• GI, CVS or Neurologic symptoms may
perdominate

Thyroid Storm:Clinical Presentation
• Infection• Surgery• Radioiodine Therapy• Iodonated Contrast
Dyes• Withdrawal of
Antithyroid drug therapy
• Amiodarone
• DKA• CHF• Hypoglycemia• Stroke• Trauma• Tooth extraction• Bowel infarction• Pulmonary embolism
Precipitating event:

THYROID STORMCLINICAL FEATURES
• Hyperpyrexia (>380C) • Tachycardia or cardiac dysrhythmia• Dehydration and dry skin• Restlessness, anxiety, or delirium• Goitre with or without exophthalmos• Stupor, coma or shock• Look for precipitating illness

Laboratory
• Elevated T3 and T4
• Suppressed TSH• Hyper or hypo glycemia• Leukocytosis• Elevated calcium• Increased transaminases, LDH, CK, Alk phos

Diagnosis of thyroid storm
• A clinical diagnosis, no lab criteria• febrile• CNS effects
– agitation, delirium, psychosis, extreme lethargy, seizure, coma
• GI/hepatic effects– diarrhea, N, V, jaundice
• CV effects– tachy, a fib, high output failure

Thermoregulatory DysfunctionTemperature
99-99.91 5100-100.9 10101-101.9 15102-102.9 20103-103.9 25 >=104.0 30
CNS EffectsMild 10AgitationModerate 20 Delerium, PsychosisExtreme lethargySevere 30Seizure, Coma
Precipitant HistoryNegative 0Positive 10
GI/Hepatic DysfunctionModerate 10Diarrhea, N&V Abd. PainSevere 30 Unexplained jaundice
CVS DysfunctionTachycardia99-109 5 110-11910 120-129 15130-139 20 >=140 25CHF Mild 5 Moderate 10 Severe 15Afib 10
Score > 45 Suggest thyroid storm 25-45 impending thyroid storm < 25 unlikely thyroid storm
Burch & Wartofsky 1993.

Treatment
• Monitored bed• Correct the hyperthyroidism
– PTU 600-1000 mg x 1 then 300 mg q. 4h– iodine after 1st dose of PTU– lugols 10 drops tid
• block the effects of thyroid hormone– large doses of B-blockers
• treat ppting event

THYROID STORMTREATMENT
• Lower temperature with cooling blanket, acetaminophen, or chlorpromazine• SSKI 5-10 gtts po tid or qid, or Na I I g iv infusion q12h• Propranolol 1 mg iv/min up to 2-10 mg, or 40-80 mg po q4-6h• PTU 800 mg po, and 200-300 mg q6h, or methimazole 80 mg po, and 40 mg q8h• Hydrocortisone 100 mg iv q8h or equivalent• Fluids and electrolyte replacement• Plasmaphoresis or peritoneal dialysis