
Thoracic Manifestations of Systemic Autoim- mune Diseases: Radio ...
14
1623 SCIENTIFIC EXHIBIT Thoracic Manifestations of Systemic Autoim- mune Diseases: Radio- graphic and High-Reso- lution CT Findings 1 Jennifer P. Mayberry, MD • Steven L. Primack, MD • Nestor L. Müller, MD, PhD The systemic autoimmune diseases include collagen vascular diseases, the systemic vasculitides, Wegener granulomatosis, and Churg-Strauss syndrome. They can cause a variety of thoracic abnormalities that are influenced by the pathophysiologic characteristics of the underlying disease process. Although many of the abnormalities can be detected at chest radiography, high-resolution computed tomography (CT) has been shown to be superior in depicting parenchymal, airway, and pleu- ral abnormalities. Thoracic manifestations of collagen vascular dis- eases include pleural disease, pulmonary fibrosis, diaphragm weakness, aspiration pneumonia, bronchiolitis obliterans organizing pneumonia, bronchiolitis obliterans, and bronchiectasis. Wegener granulomatosis may be associated with multiple nodules or masses with irregular mar- gins that are frequently cavitated. Patients with Churg-Strauss syn- drome often have consolidation or ground-glass attenuation at chest radiography and CT. Goodpasture syndrome is associated with exten- sive bilateral air-space consolidation. Index terms: Arthritis, rheumatoid, 60.611 • Dermatomyositis, 60.614 • Lung, CT, 60.12118 • Lung, diseases, 60.61, 60.62, 60.691, 60.695 Lupus erythematosus, 60.612 • Scleroderma, 60.613 • Spondylitis, 60.74 • Wegener granulomatosis, 60.622 RadioGraphics 2000; 20:1623–1635 1 From the Department of Radiology, Oregon Health Sciences University, 3181 SW Sam Jackson Park Rd, Mail Code L340, Portland, OR 97201 (J.P.M., S.L.P.); and the Department of Radiology, University of British Columbia and Vancouver Hospital and Health Sciences Centre, Vancouver, British Columbia, Canada (N.L.M.). Presented as a scientific exhibit at the 1999 RSNA scientific assembly. Received February 21, 2000; revision requested March 31 and received May 3; accepted May 4. Address correspondence to S.L.P. (e-mail: [email protected]). © RSNA, 2000 LEARNING OBJECTIVES FOR TEST 5 After reading this article and taking the test, the reader will be able to: ■ Identify the chest radiographic and CT findings in patients with systemic auto- immune diseases. ■ Recognize the dif- ferences in imaging findings among the various systemic au- toimmune diseases. ■ Describe some of the clinical thoracic findings of the sys- temic autoimmune diseases. CME FEATURE See accompanying test at http:// www.rsna.org /education /rg_cme.html
Transcript of Thoracic Manifestations of Systemic Autoim- mune Diseases: Radio ...
1623SCIENTIFIC EXHIBIT
Thoracic Manifestationsof Systemic Autoim-mune Diseases: Radio-graphic and High-Reso-lution CT Findings1
Jennifer P. Mayberry, MD • Steven L. Primack, MD • Nestor L. Müller,MD, PhD
The systemic autoimmune diseases include collagen vascular diseases,the systemic vasculitides, Wegener granulomatosis, and Churg-Strausssyndrome. They can cause a variety of thoracic abnormalities that areinfluenced by the pathophysiologic characteristics of the underlyingdisease process. Although many of the abnormalities can be detectedat chest radiography, high-resolution computed tomography (CT) hasbeen shown to be superior in depicting parenchymal, airway, and pleu-ral abnormalities. Thoracic manifestations of collagen vascular dis-eases include pleural disease, pulmonary fibrosis, diaphragm weakness,aspiration pneumonia, bronchiolitis obliterans organizing pneumonia,bronchiolitis obliterans, and bronchiectasis. Wegener granulomatosismay be associated with multiple nodules or masses with irregular mar-gins that are frequently cavitated. Patients with Churg-Strauss syn-drome often have consolidation or ground-glass attenuation at chestradiography and CT. Goodpasture syndrome is associated with exten-sive bilateral air-space consolidation.
Index terms: Arthritis, rheumatoid, 60.611 • Dermatomyositis, 60.614 • Lung, CT, 60.12118 • Lung, diseases, 60.61, 60.62, 60.691, 60.695Lupus erythematosus, 60.612 • Scleroderma, 60.613 • Spondylitis, 60.74 • Wegener granulomatosis, 60.622
RadioGraphics 2000; 20:1623–1635
1From the Department of Radiology, Oregon Health Sciences University, 3181 SW Sam Jackson Park Rd, Mail Code L340, Portland, OR 97201(J.P.M., S.L.P.); and the Department of Radiology, University of British Columbia and Vancouver Hospital and Health Sciences Centre,Vancouver, British Columbia, Canada (N.L.M.). Presented as a scientific exhibit at the 1999 RSNA scientific assembly. Received February 21,2000; revision requested March 31 and received May 3; accepted May 4. Address correspondence to S.L.P. (e-mail: [email protected]).
©RSNA, 2000
LEARNINGOBJECTIVESFOR TEST 5After reading thisarticle and takingthe test, the reader
will be able to:
� Identify the chestradiographic and CTfindings in patientswith systemic auto-immune diseases.
� Recognize the dif-ferences in imagingfindings among thevarious systemic au-toimmune diseases.
� Describe some ofthe clinical thoracicfindings of the sys-temic autoimmunediseases.
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html
1624 November-December 2000 RG � Volume 20 • Number 6
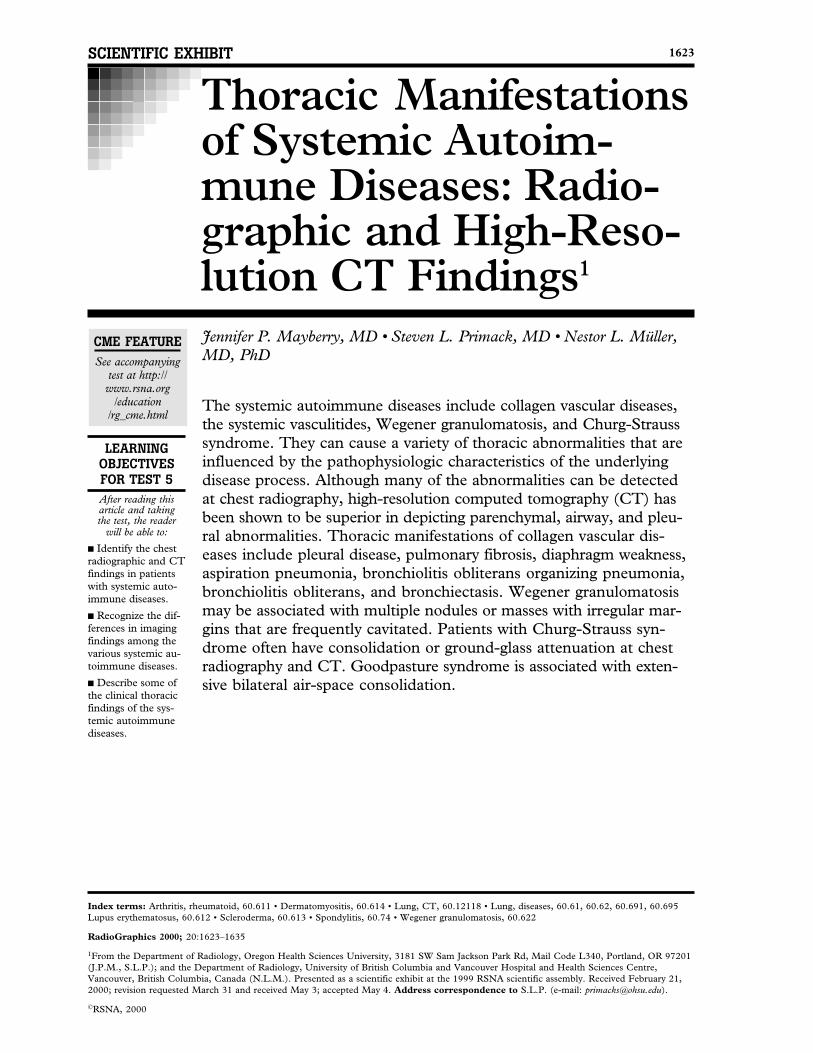
Figure 1. Systemic lupus erythematosus with pleuralinvolvement. CT scan shows pleural effusion of the leftlung, as well as pericardial effusion.
IntroductionThe autoimmune diseases comprise a group ofimmunologic disorders whose common denomi-nator is the presence of an idiopathic systemicautoimmune process. These disorders includethe collagen vascular diseases, the systemic vas-culitides, Wegener granulomatosis, and Churg-Strauss syndrome. The systemic autoimmunediseases can cause a variety of pulmonary paren-chymal, vascular, airway, and pleural abnormali-ties. The characteristic thoracic manifestations ofthese diseases are influenced by the underlyingautoimmune process. Although many of the com-plications can be detected at chest radiography,high-resolution computed tomography (CT) hasbeen shown to be superior to radiography in theassessment of the presence and extent of paren-chymal, airway, and pleural abnormalities.
In this article, we illustrate the radiographicand high-resolution CT manifestations in thechest of systemic autoimmune diseases. Discus-sion of clinical symptoms and patient characteris-tics associated with each of these disorders is ac-companied by description and illustration of thecharacteristic thoracic findings at radiographyand high-resolution CT.
Systemic Lupus ErythematosusSystemic lupus erythematosus is an autoimmunedisease of unknown pathogenesis characterized athistologic examination by deposition of autoanti-bodies and immune complexes that damage tis-sues and cells. The presentation is usually sys-temic and includes fatigue, malaise, anorexia, fe-ver, and weight loss. The disease predominantlyaffects women (F:M, 10:1) aged 20–50 years.
During the course of systemic lupus erythema-tosus, pleural disease develops in 50% of patients(1). The most common radiographic manifesta-
tion is unilateral or bilateral pleural effusion thatfrequently is associated with pericardial effusion(2) (Fig 1).
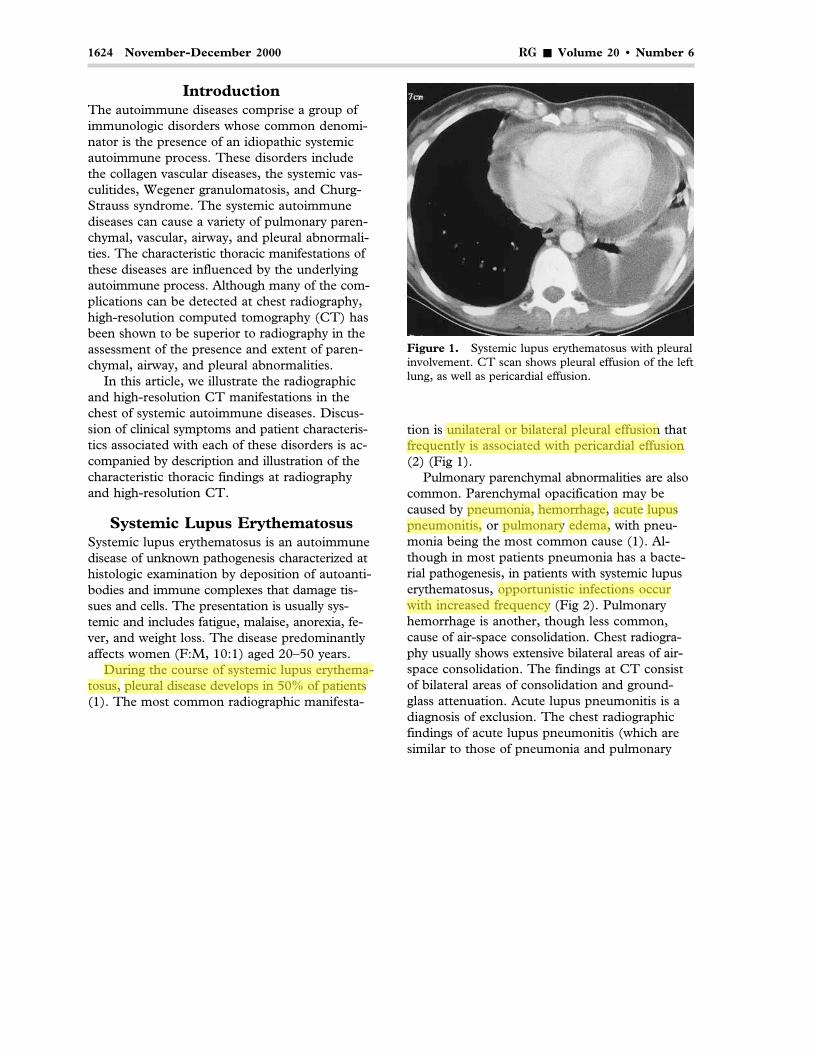
Pulmonary parenchymal abnormalities are alsocommon. Parenchymal opacification may becaused by pneumonia, hemorrhage, acute lupuspneumonitis, or pulmonary edema, with pneu-monia being the most common cause (1). Al-though in most patients pneumonia has a bacte-rial pathogenesis, in patients with systemic lupuserythematosus, opportunistic infections occurwith increased frequency (Fig 2). Pulmonaryhemorrhage is another, though less common,cause of air-space consolidation. Chest radiogra-phy usually shows extensive bilateral areas of air-space consolidation. The findings at CT consistof bilateral areas of consolidation and ground-glass attenuation. Acute lupus pneumonitis is adiagnosis of exclusion. The chest radiographicfindings of acute lupus pneumonitis (which aresimilar to those of pneumonia and pulmonary
takis
During the course of systemic lupus erythematosus,
takis
pleural disease develops in 50% of patients
takis
unilateral or bilateral pleural effusion
takis
frequently is associated with pericardial effusion
takis
pneumonia,
takis
hemorrhage,
takis
acute
takis
lupus
takis
pneumonitis,
takis
edema,
takis
pulmonary
takis
opportunistic infections occur
takis
with increased frequency
RG � Volume 20 • Number 6 Mayberry et al 1625
a. b.Figure 2. Systemic lupus erythematosus with an opportunistic infection. High-resolution CT scans show patchyground-glass attenuation bilaterally and a cavitary nodule in the superior segment of the right lower lobe (a) and fo-cal consolidation in the left lower lobe with multiple areas of cavitation (b). Results of bronchoscopic lavage and bi-opsy were positive for cytomegalovirus and aspergillosis.
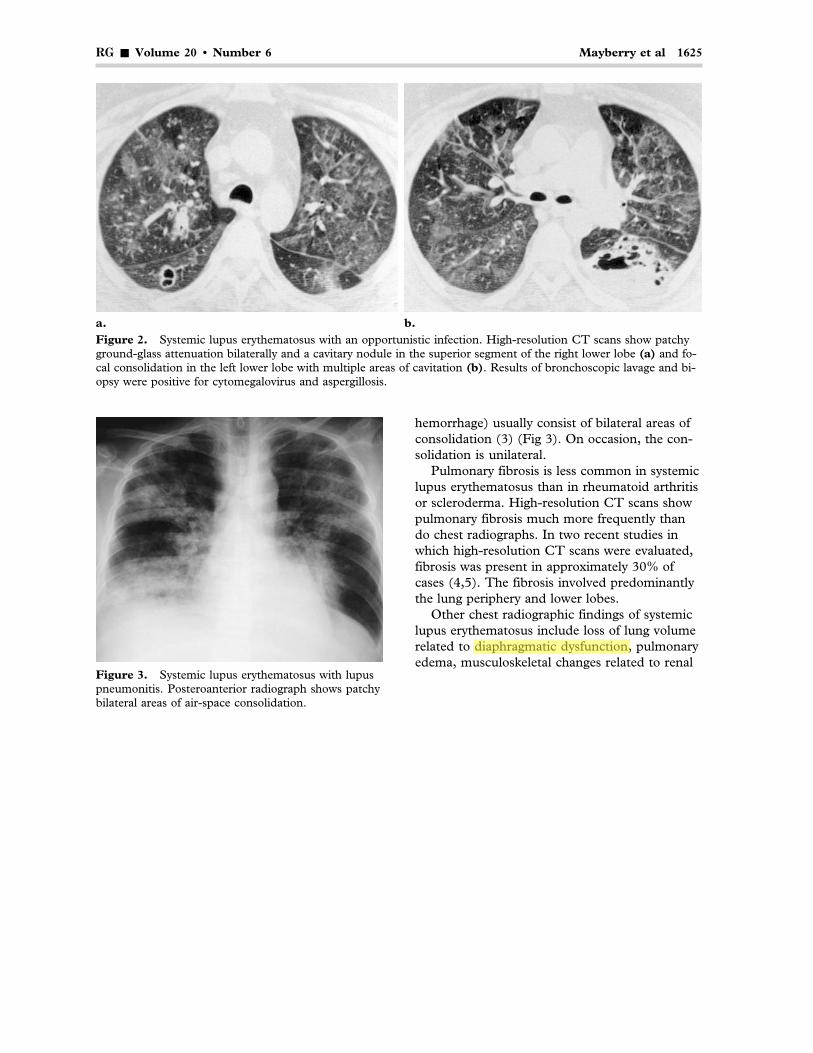
Figure 3. Systemic lupus erythematosus with lupuspneumonitis. Posteroanterior radiograph shows patchybilateral areas of air-space consolidation.
hemorrhage) usually consist of bilateral areas ofconsolidation (3) (Fig 3). On occasion, the con-solidation is unilateral.
Pulmonary fibrosis is less common in systemiclupus erythematosus than in rheumatoid arthritisor scleroderma. High-resolution CT scans showpulmonary fibrosis much more frequently thando chest radiographs. In two recent studies inwhich high-resolution CT scans were evaluated,fibrosis was present in approximately 30% ofcases (4,5). The fibrosis involved predominantlythe lung periphery and lower lobes.
Other chest radiographic findings of systemiclupus erythematosus include loss of lung volumerelated to diaphragmatic dysfunction, pulmonaryedema, musculoskeletal changes related to renal
takis
diaphragmatic dysfunction,
1626 November-December 2000 RG � Volume 20 • Number 6
failure, and bone changes related to corticoster-oid therapy (Figs 4, 5).
Rheumatoid ArthritisRheumatoid arthritis is an autoimmune diseaseof unknown pathogenesis that affects 1% of thepopulation, with a 3:1 predilection for womenbetween the ages of 20 and 50 years. The classicclinical manifestation is chronic symmetric poly-arthritis due to a persistent inflammatory synovi-tis.
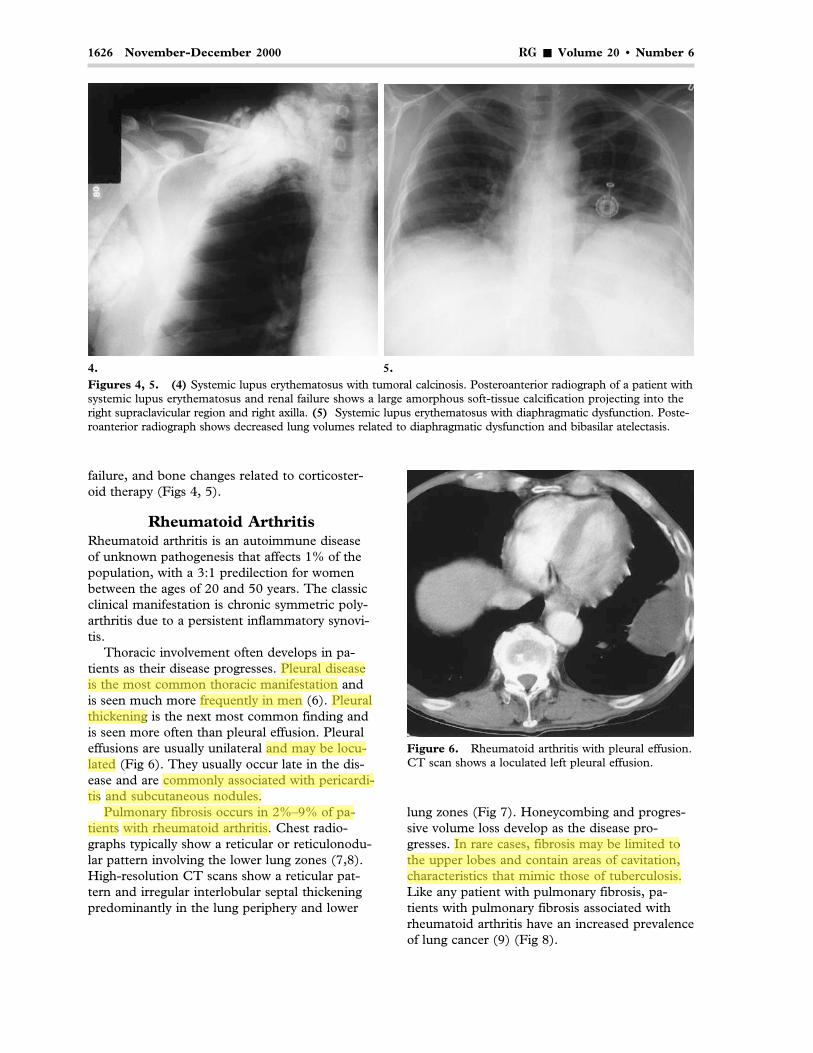
Thoracic involvement often develops in pa-tients as their disease progresses. Pleural diseaseis the most common thoracic manifestation andis seen much more frequently in men (6). Pleuralthickening is the next most common finding andis seen more often than pleural effusion. Pleuraleffusions are usually unilateral and may be locu-lated (Fig 6). They usually occur late in the dis-ease and are commonly associated with pericardi-tis and subcutaneous nodules.
Pulmonary fibrosis occurs in 2%–9% of pa-tients with rheumatoid arthritis. Chest radio-graphs typically show a reticular or reticulonodu-lar pattern involving the lower lung zones (7,8).High-resolution CT scans show a reticular pat-tern and irregular interlobular septal thickeningpredominantly in the lung periphery and lower
lung zones (Fig 7). Honeycombing and progres-sive volume loss develop as the disease pro-gresses. In rare cases, fibrosis may be limited tothe upper lobes and contain areas of cavitation,characteristics that mimic those of tuberculosis.Like any patient with pulmonary fibrosis, pa-tients with pulmonary fibrosis associated withrheumatoid arthritis have an increased prevalenceof lung cancer (9) (Fig 8).
4. 5.Figures 4, 5. (4) Systemic lupus erythematosus with tumoral calcinosis. Posteroanterior radiograph of a patient withsystemic lupus erythematosus and renal failure shows a large amorphous soft-tissue calcification projecting into theright supraclavicular region and right axilla. (5) Systemic lupus erythematosus with diaphragmatic dysfunction. Poste-roanterior radiograph shows decreased lung volumes related to diaphragmatic dysfunction and bibasilar atelectasis.
Figure 6. Rheumatoid arthritis with pleural effusion.CT scan shows a loculated left pleural effusion.
takis
Pleural disease
takis
is the most common thoracic manifestation
takis
frequently in men
takis
Pleural
takis
thickening
takis
and may be loculated
takis
commonly associated with pericarditis
takis
and subcutaneous nodules.
takis
Pulmonary fibrosis occurs in 2%–9% of patients
takis
with rheumatoid arthritis.
takis
In rare cases, fibrosis may be limited to
takis
the upper lobes and contain areas of cavitation,
takis
characteristics that mimic those of tuberculosis.
RG � Volume 20 • Number 6 Mayberry et al 1627
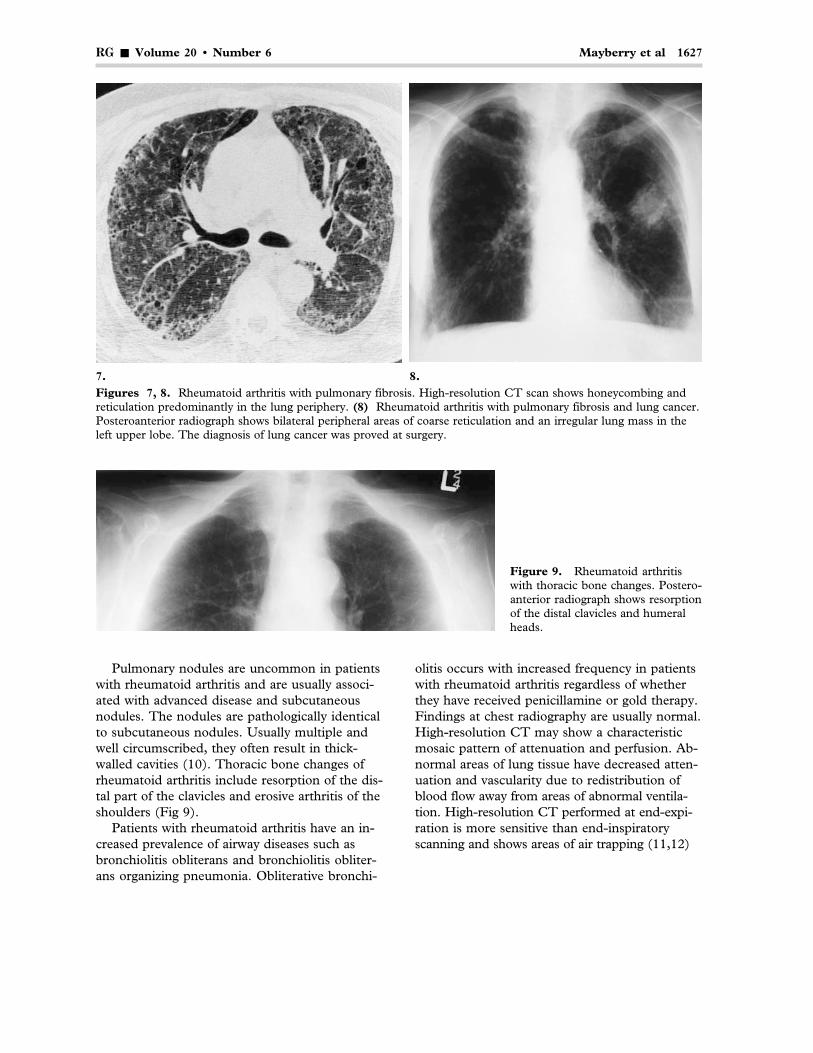
Figure 9. Rheumatoid arthritiswith thoracic bone changes. Postero-anterior radiograph shows resorptionof the distal clavicles and humeralheads.
7. 8.Figures 7, 8. Rheumatoid arthritis with pulmonary fibrosis. High-resolution CT scan shows honeycombing andreticulation predominantly in the lung periphery. (8) Rheumatoid arthritis with pulmonary fibrosis and lung cancer.Posteroanterior radiograph shows bilateral peripheral areas of coarse reticulation and an irregular lung mass in theleft upper lobe. The diagnosis of lung cancer was proved at surgery.
Pulmonary nodules are uncommon in patientswith rheumatoid arthritis and are usually associ-ated with advanced disease and subcutaneousnodules. The nodules are pathologically identicalto subcutaneous nodules. Usually multiple andwell circumscribed, they often result in thick-walled cavities (10). Thoracic bone changes ofrheumatoid arthritis include resorption of the dis-tal part of the clavicles and erosive arthritis of theshoulders (Fig 9).
Patients with rheumatoid arthritis have an in-creased prevalence of airway diseases such asbronchiolitis obliterans and bronchiolitis obliter-ans organizing pneumonia. Obliterative bronchi-
olitis occurs with increased frequency in patientswith rheumatoid arthritis regardless of whetherthey have received penicillamine or gold therapy.Findings at chest radiography are usually normal.High-resolution CT may show a characteristicmosaic pattern of attenuation and perfusion. Ab-normal areas of lung tissue have decreased atten-uation and vascularity due to redistribution ofblood flow away from areas of abnormal ventila-tion. High-resolution CT performed at end-expi-ration is more sensitive than end-inspiratoryscanning and shows areas of air trapping (11,12)

1628 November-December 2000 RG � Volume 20 • Number 6
a. b.Figure 10. Rheumatoid arthritis with obliterative bronchiolitis in a patient who had undergone penicillamine ther-apy. (a) High-resolution CT scan obtained at end-inspiration shows cylindrical bronchiectasis in the right middlelobe (arrow). (b) High-resolution CT scan obtained at end-expiration shows patchy air trapping bilaterally, particu-larly in the right middle lobe and right lower lobe posteriorly (arrows).
(Fig 10). The predominant radiographic andhigh-resolution CT finding in patients with bron-chiolitis obliterans organizing pneumonia is air-space consolidation that is usually bilateral andtends to have a patchy peripheral or peribron-chial distribution.
Follicular bronchiolitis occurs with increasedfrequency in patients with rheumatoid arthritis.In a recent serial evaluation of high-resolutionCT findings in 12 patients with follicular bron-chiolitis, eight patients (66%) had rheumatoidarthritis (13). The major CT findings were smallcentrilobular nodules associated with patchy ar-eas of ground-glass attenuation.
Progressive Systemic SclerosisProgressive systemic sclerosis (scleroderma) is aconnective-tissue disease of unknown pathogen-esis that affects 30- to 50-year-old women threetimes as often as it affects men. This type of scle-rosis is characterized by overproduction of col-lagen, which leads to fibrosis of the lungs, skin,vasculature, and visceral organs. Patients presentwith thickening and tightening of the skin; mus-culoskeletal manifestations; Raynaud phenom-enon; and fibrosis of the lungs, kidneys, and gas-trointestinal tract. Two-thirds of patients withprogressive systemic sclerosis have clinical pul-monary symptoms, the most common of whichare exertional dyspnea and dry, nonproductivecough.
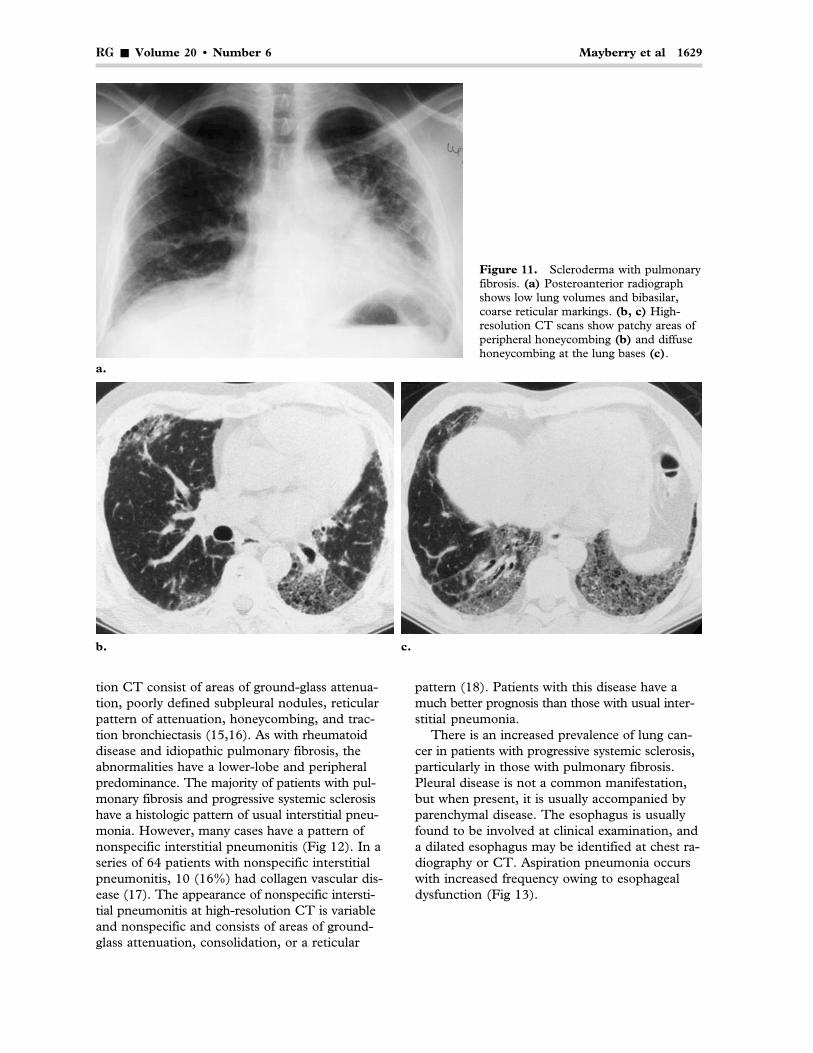
Pulmonary fibrosis is the most common radio-graphic finding, present in 20%–65% of patients(14,15). The fibrosis usually has a basilar pre-dominance and appears initially as a fine reticularpattern that progresses to coarse reticulation andhoneycombing (14) (Fig 11).
High-resolution CT may show evidence of fi-brosis in patients with normal findings at radiog-raphy (15). In a prospective study of 23 patientswith progressive systemic sclerosis, fibrosis wasidentified at chest radiography in 39% of patientsand at high-resolution CT in 91% of patients (15).The predominant abnormalities at high-resolu-
Figure 12. Scleroderma with nonspecific interstitialpneumonitis. High-resolution CT scan obtainedthrough the lung bases shows bibasilar areas of consoli-dation. Video-assisted thoracoscopic surgical biopsyshowed nonspecific interstitial pneumonitis.
RG � Volume 20 • Number 6 Mayberry et al 1629
b. c.
a.
Figure 11. Scleroderma with pulmonaryfibrosis. (a) Posteroanterior radiographshows low lung volumes and bibasilar,coarse reticular markings. (b, c) High-resolution CT scans show patchy areas ofperipheral honeycombing (b) and diffusehoneycombing at the lung bases (c).
tion CT consist of areas of ground-glass attenua-tion, poorly defined subpleural nodules, reticularpattern of attenuation, honeycombing, and trac-tion bronchiectasis (15,16). As with rheumatoiddisease and idiopathic pulmonary fibrosis, theabnormalities have a lower-lobe and peripheralpredominance. The majority of patients with pul-monary fibrosis and progressive systemic sclerosishave a histologic pattern of usual interstitial pneu-monia. However, many cases have a pattern ofnonspecific interstitial pneumonitis (Fig 12). In aseries of 64 patients with nonspecific interstitialpneumonitis, 10 (16%) had collagen vascular dis-ease (17). The appearance of nonspecific intersti-tial pneumonitis at high-resolution CT is variableand nonspecific and consists of areas of ground-glass attenuation, consolidation, or a reticular
pattern (18). Patients with this disease have amuch better prognosis than those with usual inter-stitial pneumonia.
There is an increased prevalence of lung can-cer in patients with progressive systemic sclerosis,particularly in those with pulmonary fibrosis.Pleural disease is not a common manifestation,but when present, it is usually accompanied byparenchymal disease. The esophagus is usuallyfound to be involved at clinical examination, anda dilated esophagus may be identified at chest ra-diography or CT. Aspiration pneumonia occurswith increased frequency owing to esophagealdysfunction (Fig 13).
1630 November-December 2000 RG � Volume 20 • Number 6
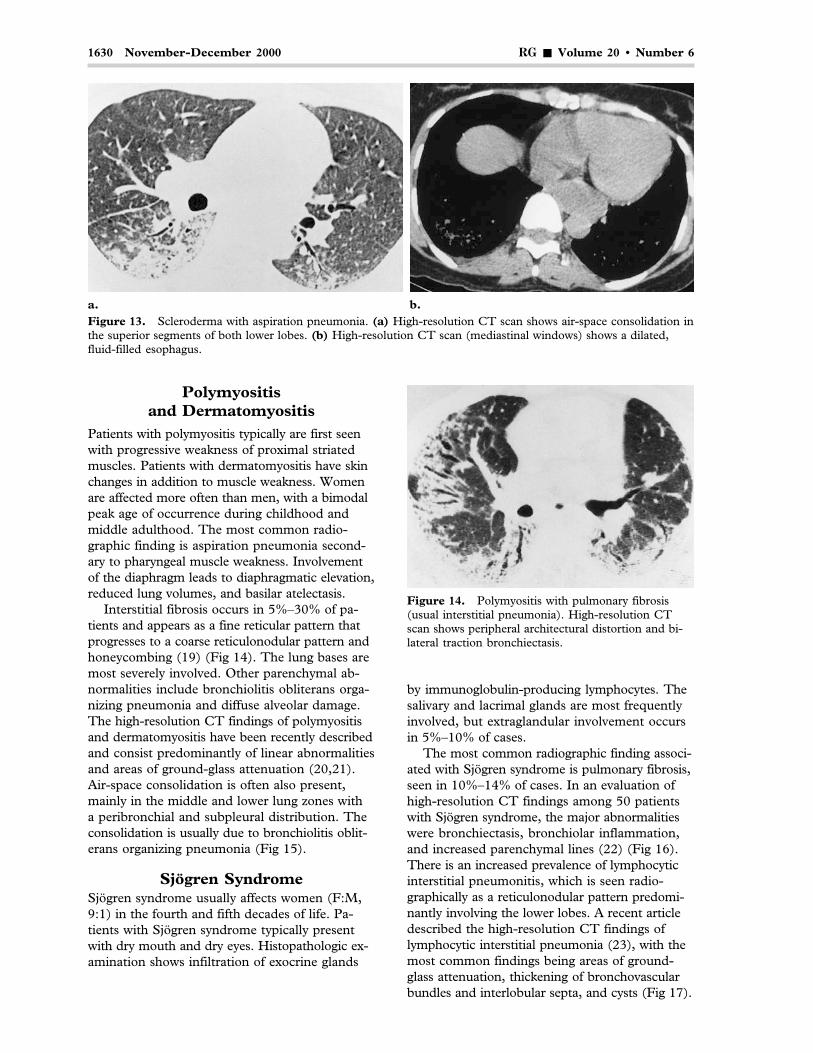
Figure 14. Polymyositis with pulmonary fibrosis(usual interstitial pneumonia). High-resolution CTscan shows peripheral architectural distortion and bi-lateral traction bronchiectasis.
a. b.Figure 13. Scleroderma with aspiration pneumonia. (a) High-resolution CT scan shows air-space consolidation inthe superior segments of both lower lobes. (b) High-resolution CT scan (mediastinal windows) shows a dilated,fluid-filled esophagus.
Polymyositisand Dermatomyositis
Patients with polymyositis typically are first seenwith progressive weakness of proximal striatedmuscles. Patients with dermatomyositis have skinchanges in addition to muscle weakness. Womenare affected more often than men, with a bimodalpeak age of occurrence during childhood andmiddle adulthood. The most common radio-graphic finding is aspiration pneumonia second-ary to pharyngeal muscle weakness. Involvementof the diaphragm leads to diaphragmatic elevation,reduced lung volumes, and basilar atelectasis.
Interstitial fibrosis occurs in 5%–30% of pa-tients and appears as a fine reticular pattern thatprogresses to a coarse reticulonodular pattern andhoneycombing (19) (Fig 14). The lung bases aremost severely involved. Other parenchymal ab-normalities include bronchiolitis obliterans orga-nizing pneumonia and diffuse alveolar damage.The high-resolution CT findings of polymyositisand dermatomyositis have been recently describedand consist predominantly of linear abnormalitiesand areas of ground-glass attenuation (20,21).Air-space consolidation is often also present,mainly in the middle and lower lung zones witha peribronchial and subpleural distribution. Theconsolidation is usually due to bronchiolitis oblit-erans organizing pneumonia (Fig 15).
Sjögren SyndromeSjögren syndrome usually affects women (F:M,9:1) in the fourth and fifth decades of life. Pa-tients with Sjögren syndrome typically presentwith dry mouth and dry eyes. Histopathologic ex-amination shows infiltration of exocrine glands
by immunoglobulin-producing lymphocytes. Thesalivary and lacrimal glands are most frequentlyinvolved, but extraglandular involvement occursin 5%–10% of cases.
The most common radiographic finding associ-ated with Sjögren syndrome is pulmonary fibrosis,seen in 10%–14% of cases. In an evaluation ofhigh-resolution CT findings among 50 patientswith Sjögren syndrome, the major abnormalitieswere bronchiectasis, bronchiolar inflammation,and increased parenchymal lines (22) (Fig 16).There is an increased prevalence of lymphocyticinterstitial pneumonitis, which is seen radio-graphically as a reticulonodular pattern predomi-nantly involving the lower lobes. A recent articledescribed the high-resolution CT findings oflymphocytic interstitial pneumonia (23), with themost common findings being areas of ground-glass attenuation, thickening of bronchovascularbundles and interlobular septa, and cysts (Fig 17).

RG � Volume 20 • Number 6 Mayberry et al 1631
a. b.Figure 15. Dermatomyositis with bronchiolitis obliterans organizing pneumonia. High-resolution CT scans showa peripheral area of consolidation in the right middle lobe (a) and peribronchial consolidation in both lung bases (b).
16. 17.Figures 16, 17. Sjögren syndrome with bronchiectasis. High-resolution CT scan shows extensive bilateral cylin-drical bronchiectasis. (17) Sjögren syndrome with lymphocytic interstitial pneumonitis. High-resolution CT scanshows scattered bilateral thin-walled cysts.
Patients with Sjögren syndrome also have anincreased risk of lymphoma. Lymphoma shouldbe suspected if a chest radiograph shows medias-tinal lymphadenopathy or a pulmonary mass.
Ankylosing SpondylitisAnkylosing spondylitis is an autoimmune diseaseof unknown pathogenesis that primarily affectsthe axial skeleton. It has a male-to-female pre-dominance of 3:1.
In a study of chest radiographic findings in2,080 patients with ankylosing spondylitis, 26(1.2%) had fibrosis in the upper lobes (24). Theradiographic findings of ankylosing spondylitisconsist of reticulonodular opacities in the lung
apices, which become confluent as the diseaseprogresses (24). Common associated abnormali-ties include apical bullae and cavitation, poten-tially mimicking tuberculosis. The high-resolu-tion CT findings in 26 patients with ankylosingspondylitis were recently described (25). Themost common abnormalities are peripheral inter-stitial lung disease, bronchiectasis, paraseptalemphysema, and apical fibrosis (Fig 18). Radio-graphic changes of the spine, consisting of sym-metric marginal syndesmophytes (“bamboospine”), are usually evident when there is apicalfibrosis. Restriction of the chest wall may resultfrom fusion of the costovertebral joints.

1632 November-December 2000 RG � Volume 20 • Number 6
a. b.
c.
Figure 18. Ankylosing spondylitis. (a) Posteroanteri-or radiograph shows severe bilateral scarring in the up-per lobes and volume loss. (b) Lateral radiograph showsflowing syndesmophytes of the thoracic spine. (c) CTscan shows severe volume loss of the lung apices withtraction cystic bronchiectasis.
Wegener GranulomatosisPredominantly affecting male patients, Wegenergranulomatosis is a systemic autoimmune diseasecharacterized by granulomatous vasculitis of theupper and lower respiratory tracts, glomerulone-phritis, and small-vessel vasculitis. The histo-pathologic hallmark of Wegener granulomatosisis a necrotizing vasculitis of small arteries andveins with granuloma formation.
Lung disease develops in most patients. Themost common radiographic manifestation ofWegener granulomatosis is multiple nodules orirregularly marginated masses with no zonal pre-dominance (26,27). The nodules or masses areusually multiple but can be solitary in up to 25%of cases (27). Cavitation of the nodules occurs inapproximately 50% of cases. The cavities usuallyhave irregular, thick walls. With treatment, thenodules or cavities may resolve completely or re-sult in a scar. At CT, the nodules typically haveirregular margins and often have a peribroncho-vascular distribution (28,29) (Fig 19). Periph-eral, wedge-shaped areas of consolidation repre-senting infarcts may also be seen. Pleural effu-sions occur in less than 10% of cases. Mediastinaland hilar adenopathy are relatively uncommon.
Localized or diffuse areas of air-space consoli-dation may be present. These areas usually repre-sent pulmonary hemorrhage, although pneu-monia causes similar findings. Pulmonary hemor-rhage can result in a focal area of dense
consolidation, patchy bilateral areas of consolida-tion, or diffuse air-space consolidation (27).
Involvement of the tracheal or bronchial wallsusually consists of mucosal or submucosal granu-lomatous thickening. CT scans show smooth ornodular thickening of the tracheal or bronchialwall (Fig 20). The thickening may become se-vere, causing narrowing of the lumen and pos-sible eventual calcification.
Churg-Strauss SyndromeChurg-Strauss syndrome is an allergic angiitis andgranulomatous necrotizing vasculitis that occuralmost exclusively in patients with asthma. Thesyndrome is most common in patients aged 30–50years and has no gender predilection. Patients aretypically asthmatic and present with eosinophilia,fever, and allergic rhinitis. Findings of chest radi-ography are usually abnormal and most often con-sist of patchy, nonsegmental areas of consolida-tion with no zonal predominance (30) (Fig 21a).

RG � Volume 20 • Number 6 Mayberry et al 1633
19a. 19b.Figures 19, 20. (19) Wegener granulomatosis. (a) Pos-teroanterior radiograph shows bilateral irregular nodulesand a mass in the right lower lobe. (b) High-resolution CTscan shows multiple irregular nodules in a peribroncho-vascular distribution. (20) Wegener granulomatosis withtracheal involvement. CT scan shows diffuse thickening ofthe tracheal wall.
20.
a. b.Figure 21. Churg-Strauss syndrome. (a) Posteroanterior radiograph shows patchy bilateral areas of consolidationpredominantly in the right lung. (b) High-resolution CT scan shows patchy bilateral ground-glass attenuation andconsolidation of the right lower lobe.
1634 November-December 2000 RG � Volume 20 • Number 6
The areas of consolidation may have a peripheraldistribution and are often transient. Nodules mayoccur, but cavitation is rare. Pleural effusions arepresent in approximately 30% of patients (30).
CT findings in 17 patients were recently de-scribed (31). The predominant findings were con-solidation or ground-glass attenuation, seen in 10(59%) patients (Fig 21b). Other, less commonfindings included pulmonary nodules, interlobularseptal thickening, and bronchial wall thickening.
Anti–Glomerular BasementMembrane Antibody Disease
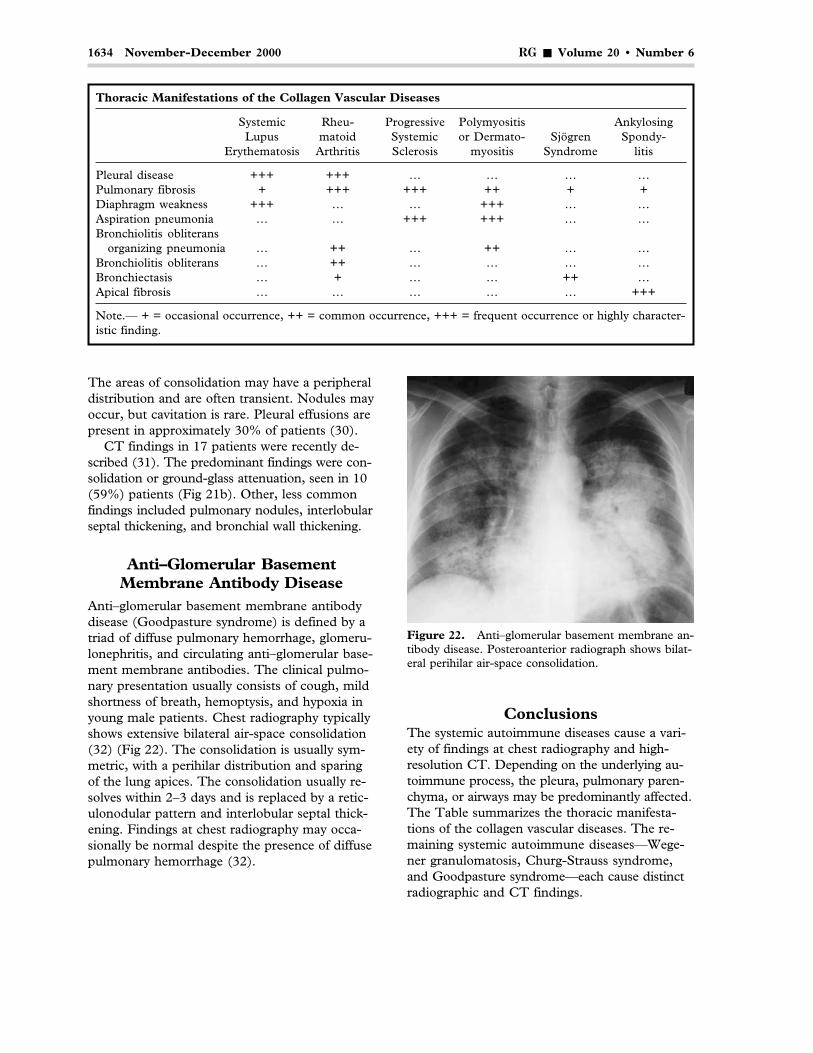
Anti–glomerular basement membrane antibodydisease (Goodpasture syndrome) is defined by atriad of diffuse pulmonary hemorrhage, glomeru-lonephritis, and circulating anti–glomerular base-ment membrane antibodies. The clinical pulmo-nary presentation usually consists of cough, mildshortness of breath, hemoptysis, and hypoxia inyoung male patients. Chest radiography typicallyshows extensive bilateral air-space consolidation(32) (Fig 22). The consolidation is usually sym-metric, with a perihilar distribution and sparingof the lung apices. The consolidation usually re-solves within 2–3 days and is replaced by a retic-ulonodular pattern and interlobular septal thick-ening. Findings at chest radiography may occa-sionally be normal despite the presence of diffusepulmonary hemorrhage (32).
Thoracic Manifestations of the Collagen Vascular Diseases
Systemic Rheu- Progressive Polymyositis AnkylosingLupus matoid Systemic or Dermato- Sjögren Spondy-
Erythematosis Arthritis Sclerosis myositis Syndrome litis
Pleural disease +++ +++ … … … …Pulmonary fibrosis + +++ +++ ++ + +Diaphragm weakness +++ … … +++ … …Aspiration pneumonia … … +++ +++ … …Bronchiolitis obliterans
organizing pneumonia … ++ … ++ … …Bronchiolitis obliterans … ++ … … … …Bronchiectasis … + … … ++ …Apical fibrosis … … … … … +++
Note.— + = occasional occurrence, ++ = common occurrence, +++ = frequent occurrence or highly character-istic finding.
Figure 22. Anti–glomerular basement membrane an-tibody disease. Posteroanterior radiograph shows bilat-eral perihilar air-space consolidation.
ConclusionsThe systemic autoimmune diseases cause a vari-ety of findings at chest radiography and high-resolution CT. Depending on the underlying au-toimmune process, the pleura, pulmonary paren-chyma, or airways may be predominantly affected.The Table summarizes the thoracic manifesta-tions of the collagen vascular diseases. The re-maining systemic autoimmune diseases—Wege-ner granulomatosis, Churg-Strauss syndrome,and Goodpasture syndrome—each cause distinctradiographic and CT findings.

RG � Volume 20 • Number 6 Mayberry et al 1635
References1. Wiedemann HP, Matthay RA. Pulmonary mani-
festations of systemic lupus erythematosus. JThorac Imaging 1992; 7:1–18.
2. Turner-Stokes L, Turner-Warwick M. Intratho-racic manifestations of SLE. Clin Rheum Dis 1982;8:229–242.
3. Matthay RA, Schwarz MI, Petty TL, et al. Pulmo-nary manifestations of systemic lupus erythemato-sus: review of twelve cases of acute lupus pneu-monitis. Medicine 1974; 54:397–409.
4. Bankier AA, Kiner HP, Wiesmayr MN, et al. Dis-crete lung involvement in systemic lupus erythe-matosus: CT assessment. Radiology 1995; 196:835–840.
5. Fenlon HM, Doran M, Sant SM, et al. High-reso-lution chest CT in systemic lupus erythematosus.AJR Am J Roentgenol 1996; 166:301–307.
6. Hunninghake GW, Fauci AS. Pulmonary involve-ment in the collagen vascular diseases. Am RevRespir Dis 1979; 119:471–503.
7. Locke CB. Rheumatoid lung. Clin Radiol 1963;14:43–47.
8. Gamsu G. Radiographic manifestations of thoracicinvolvement by collagen vascular diseases. J ThoracImaging 1992; 7:1–12.
9. Fraser RS, Müller NL, Paré PD, et al. Diagnosisof diseases of the chest. 4th ed. Vol 3. Philadel-phia, Pa: Saunders, 1999; 1608.
10. Martel W, Abell MR, Mikkelsen WM, et al. Pul-monary and pleural lesions in rheumatoid disease.Radiology 1968; 90:641–653.
11. Aquino SL, Webb RW, Golden J. Bronchiolitisobliterans associated with rheumatoid arthritis:findings on HRCT and dynamic expiratory CT. JComput Assist Tomogr 1994; 18:555–558.
12. Hansell DM, Rubens MB, Padley SPG, et al.Obliterative bronchiolitis: individual CT signs ofsmall airways disease and functional correlation.Radiology 1997; 203:721–726.
13. Howling SJ, Hansell DM, Wells AV, et al. Follicu-lar bronchiolitis: thin-section CT and histologicfindings. Radiology 1999; 212:637–642.
14. Arroliga AC, Podell DN, Matthay RA. Pulmonarymanifestations of scleroderma. J Thorac Imaging1990; 7:30–45.
15. Schurawitzki H, Stiglbauer R, Graninger W, et al.Interstitial lung disease in progressive systemicsclerosis: CT versus radiography. Radiology 1990;176:755–759.
16. Remy-Jardin M, Remy J, Wallaert B, et al. Pulmo-nary involvement in progressive systemic sclerosis:sequential evaluation with CT, pulmonary func-tion tests, and bronchoalveolar lavage. Radiology1993; 188:499–506.
17. Katzenstein AA, Fiorelli RF. Non-specific intersti-tial pneumonia/fibrosis: histologic patterns andclinical significance. Am J Surg Pathol 1994; 18:136–147.
18. Johkoh T, Müller NL, Cartier Y, et al. Idiopathicinterstitial pneumonias: diagnostic accuracy ofthin-section CT in 129 patients. Radiology 1999;211:555–560.
19. Dickey BF, Myers AR. Pulmonary disease in poly-myositis/dermatomyositis. Semin Arthritis Rheum1984; 14:60–76.
20. Ikezoe J, Johkoh T, Nohno N, et al. High-resolu-tion CT findings of lung disease in patients withpolymyositis and dermatomyositis. J Thorac Imag-ing 1996; 11:250–259.
21. Mino M, Noma S, Taguchi Y, et al. Pulmonaryinvolvement in polymyositis and dermatomyositis:sequential evaluation with CT. AJR Am J Roent-genol 1997; 169:83–87.
22. Franquet T, Gimenez A, Monill JM, Diaz C, GeliC. Primary Sjögren’s syndrome and associatedlung disease: CT findings in 50 patients. AJR Am JRoentgenol 1997; 169:655–658.
23. Johkoh T, Müller NL, Pickford HA, et al. Lym-phocytic interstitial pneumonia: thin-section CTfindings in 22 patients. Radiology 1999; 212:567–572.
24. Rosenow EC, Strimlan CV, Muhm JR, et al. Pleu-ropulmonary manifestations of ankylosingspondylitis. Mayo Clin Proc 1977; 52:641–649.
25. Fenlon HM, Casserly I, Sant SM, et al. Plain ra-diographic and thoracic high-resolution CT in pa-tients with ankylosing spondylitis. AJR Am JRoentgenol 1997; 168:1067–1072.
26. Aberle DR, Gamsu G, Lynch D. Thoracic mani-festations of Wegener granulomatosis: diagnosisand course. Radiology 1990; 174:703–709.
27. Cordier JF, Valeyre D, Guillevin L, et al. Pulmo-nary Wegener’s granulomatosis: a clinical and im-aging study of 77 cases. Chest 1990; 97:906–912.
28. Kuhlman JE, Hruban RH, Fishman ER.Wegener’s granulomatosis: CT features of paren-chymal lung disease. J Comput Assist Tomogr1991; 15:948–952.
29. Maskell GF, Lockwood CM, Flower CDR. Com-puted tomography of the lung in Wegener’s granu-lomatosis. Clin Radiol 1993; 48:377–380.
30. Lanham JG, Elkon KB, Pusey CD, et al. Systemicvasculitis with asthma and eosinophilia: a clinicalapproach to the Churg-Strauss syndrome. Medi-cine 1984; 63:65–81.
31. Worthy SA, Müller NL, Hansell DM, et al.Churg-Strauss syndrome: the spectrum of pulmo-nary CT findings in 17 patients. AJR Am JRoentgenol 1998; 170:297–300.
32. Bowley NB, Steiner RE, Chin WS. The chest x-ray in antiglomerular basement membrane anti-body disease (Goodpasture’s syndrome). ClinRadiol 1979; 30:419–429.
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.



















