
The Year in Diabetes- 2016cmetracker.net/PPMC/Files/EventMaterials/12-Diabetes.pdfThe Year in...
16
1 The Year in Diabetes- 2016 Elizabeth Stephens, MD Endocrinology- Medical Education Faculty PMG- Northeast April 2016 [email protected] Disclosures • None
Transcript of The Year in Diabetes- 2016cmetracker.net/PPMC/Files/EventMaterials/12-Diabetes.pdfThe Year in...
1
The Year in Diabetes- 2016
Elizabeth Stephens, MD
Endocrinology- Medical Education Faculty
PMG- Northeast
April [email protected]
Disclosures
• None

2
Goals for Discussion
• Review 2016 Guidelines from American Diabetes Association and discuss:– Role for SGLT-2’s
– New considerations for GLP-1’s
– Alternative insulin formulations
• New isn’t always better– When to use regular and NPH insulin
Key to Medications
• DPP4 inhibitors:– Sitagliptin (Januvia®), Saxagliptin (Onglyza®), Linagliptin
(Tradjenta®), Alogliptin (Nesina®)
• GLP1 agonists:– Exenatide: BID (Byetta®) , weekly (Bydureon®)
– Liraglutide: daily (Victoza®)
– Albiglutide: weekly (Tanzeum®)
– Dulaglutide: weekly (Trulicity® )
• SGLT2 inhibitors:– Canagliflozin (Invokana®), Dapagliflozin (Farxiga®),
Empagliflozin (Jardiance®)

3
Let’s start with a case…
• 54 yo man, diagnosed with type 2 DM 9 years ago
• Initially managed with metformin, then added glimepiride
• A1c now 8.8%, weight 280#, BMI 40• Taking all meds, has a number of questions:
– Is the glimepiride “bad” for him?– Does he need insulin?– On a fixed income- can’t afford “fancy”, but curious
about medicines he has seen on TV– Doesn’t want to gain weight
Diab Care 2016;39(supp 1):S52
4
Issues with Sulfonylureas: Cons
• Beta cell burnout:– ADOPT: lost glucose control at 45months with
metformin vs 33 months with glyburide
– No difference in UKPDS
– Over 6 yrs, 34% with SU needed insulin, c/w 27% with DPP4
• Weight gain: 2-5kg on average
• Hypoglycemia: – 6x more hypoglycemia c/w other DM meds
Kahn S, NEJM 2006;355:427; UKPDS 1995;11:1249; Inzucchi S, Diab Obes Metab 2015; Cefalu W, Diab Care 2015
Issues with Sulfonylureas: Pros
• Effective: A1c lowers A1c 1-2% – More effect with higher baseline A1c
• Cost: inexpensive
• Easy: Oral, not injected
• History: Lots of experience
5
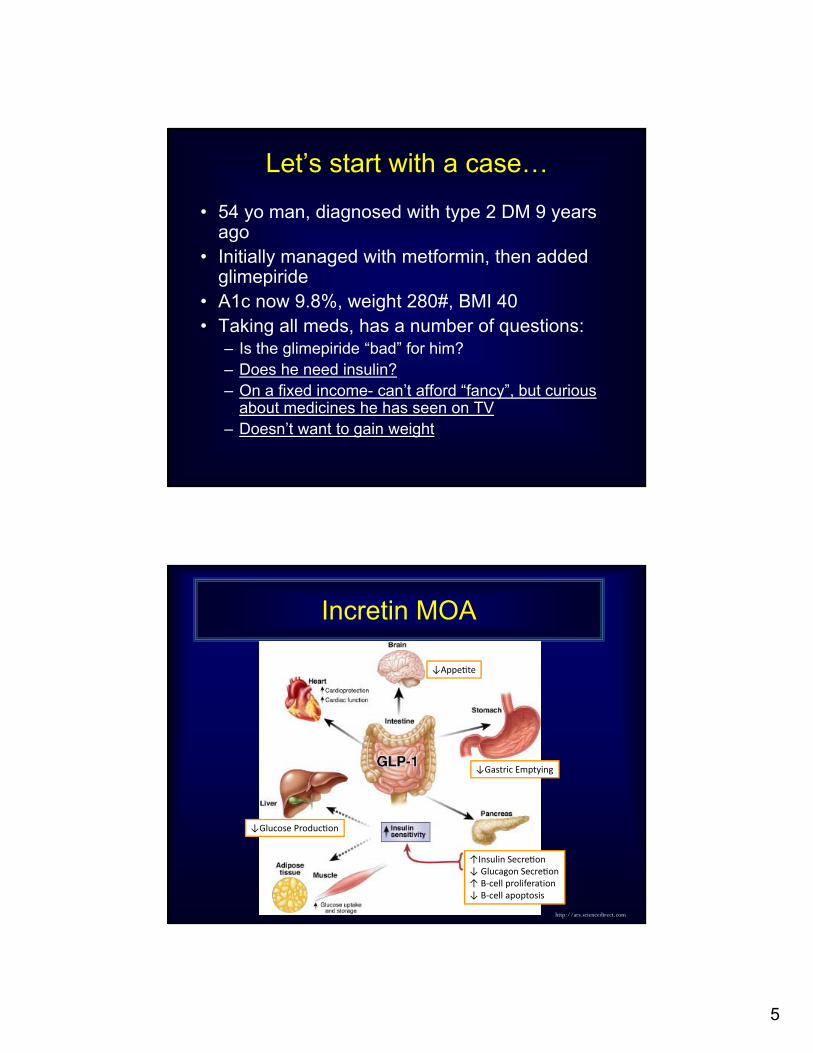
Let’s start with a case…
• 54 yo man, diagnosed with type 2 DM 9 years ago
• Initially managed with metformin, then added glimepiride
• A1c now 9.8%, weight 280#, BMI 40• Taking all meds, has a number of questions:
– Is the glimepiride “bad” for him?– Does he need insulin?– On a fixed income- can’t afford “fancy”, but curious
about medicines he has seen on TV– Doesn’t want to gain weight
Incretin MOA
http://ars.sciencedirect.com
↓Appe te
↓Gastric Emptying
↑Insulin Secre on↓ Glucagon Secre on↑ Β‐cell proliferation↓ Β‐cell apoptosis
↓Glucose Produc on
6
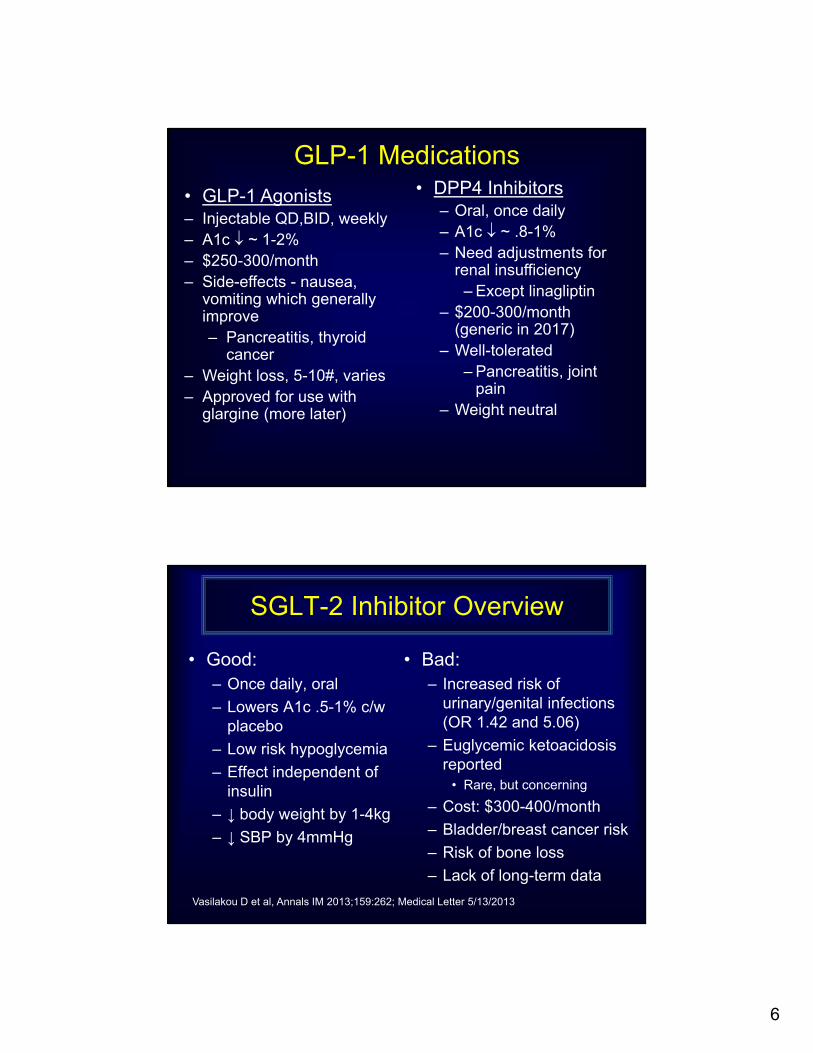
GLP-1 Medications
• GLP-1 Agonists– Injectable QD,BID, weekly– A1c ~ 1-2%– $250-300/month– Side-effects - nausea,
vomiting which generally improve– Pancreatitis, thyroid
cancer – Weight loss, 5-10#, varies– Approved for use with
glargine (more later)
• DPP4 Inhibitors – Oral, once daily– A1c ~ .8-1%– Need adjustments for
renal insufficiency– Except linagliptin
– $200-300/month (generic in 2017)
– Well-tolerated– Pancreatitis, joint
pain – Weight neutral
SGLT-2 Inhibitor Overview
• Good:– Once daily, oral
– Lowers A1c .5-1% c/w placebo
– Low risk hypoglycemia
– Effect independent of insulin
– ↓ body weight by 1-4kg
– ↓ SBP by 4mmHg
• Bad:– Increased risk of
urinary/genital infections (OR 1.42 and 5.06)
– Euglycemic ketoacidosis reported
• Rare, but concerning
– Cost: $300-400/month
– Bladder/breast cancer risk
– Risk of bone loss
– Lack of long-term data
Vasilakou D et al, Annals IM 2013;159:262; Medical Letter 5/13/2013
7
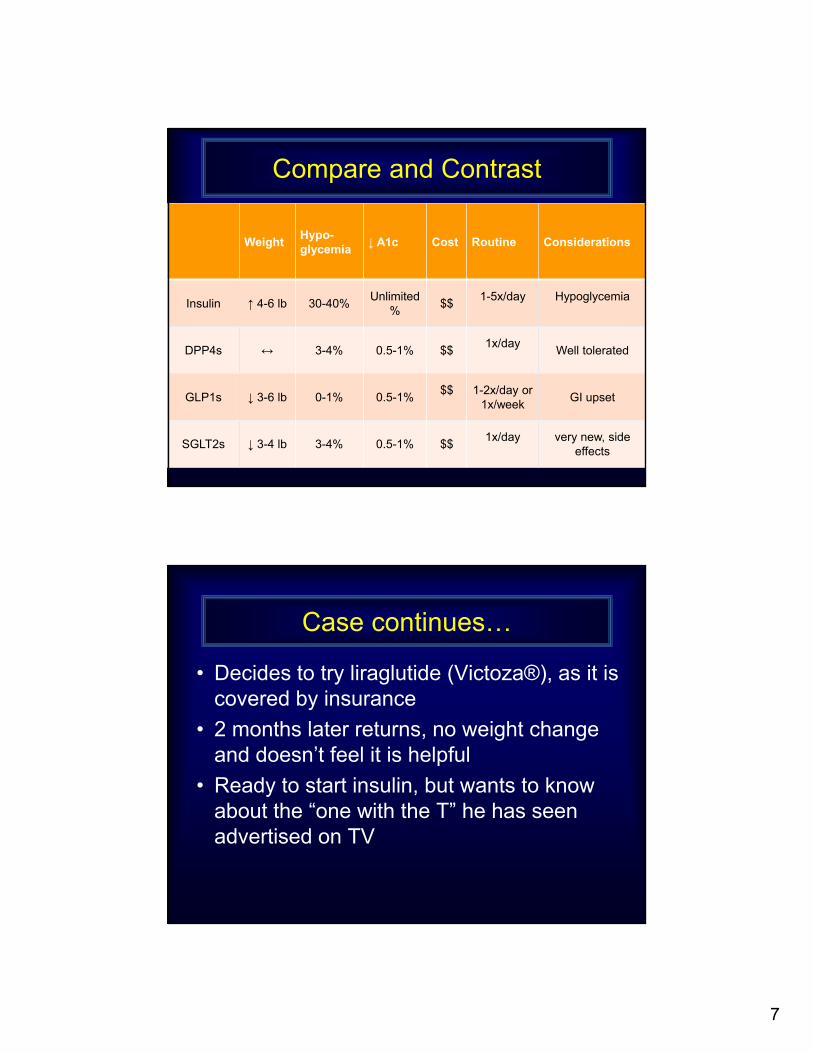
WeightHypo-glycemia
↓ A1c Cost Routine Considerations
Insulin ↑ 4-6 lb 30-40%Unlimited
%$$
1-5x/day Hypoglycemia
DPP4s ↔ 3-4% 0.5-1% $$1x/day
Well tolerated
GLP1s ↓ 3-6 lb 0-1% 0.5-1%$$ 1-2x/day or
1x/weekGI upset
SGLT2s ↓ 3-4 lb 3-4% 0.5-1% $$1x/day very new, side
effects
Compare and Contrast
Case continues…
• Decides to try liraglutide (Victoza®), as it is covered by insurance
• 2 months later returns, no weight change and doesn’t feel it is helpful
• Ready to start insulin, but wants to know about the “one with the T” he has seen advertised on TV
8
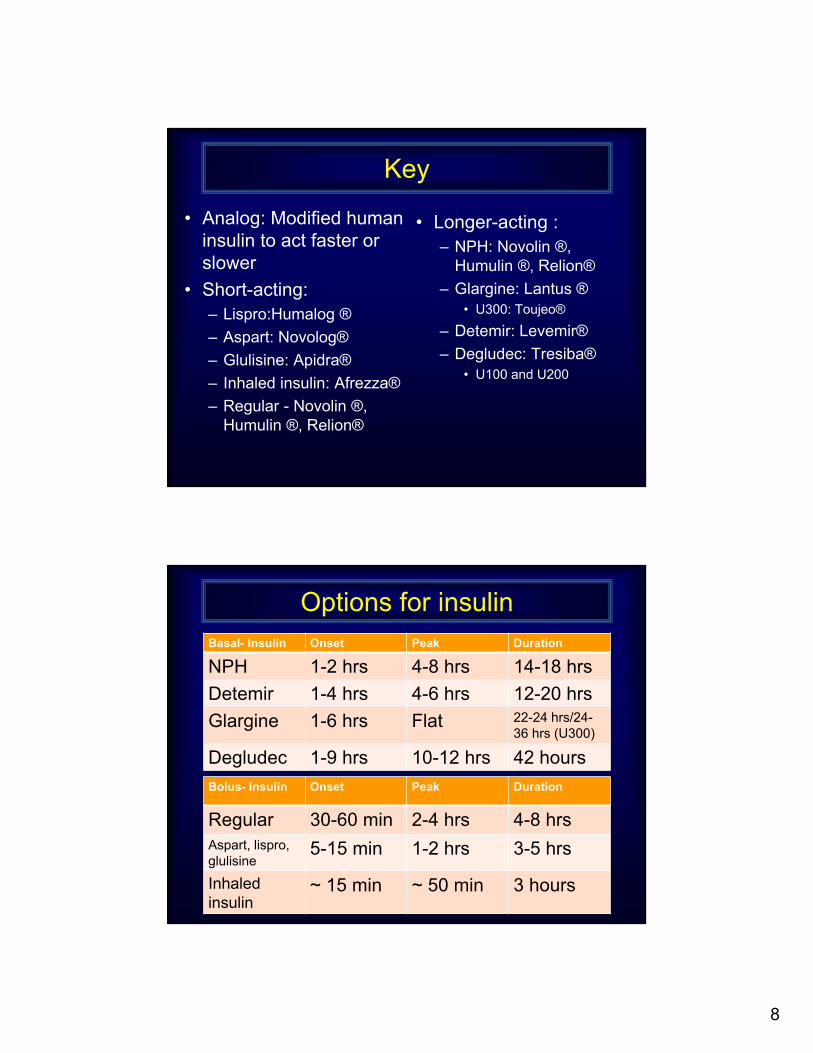
Key
• Analog: Modified human insulin to act faster or slower
• Short-acting:– Lispro:Humalog ®
– Aspart: Novolog®
– Glulisine: Apidra®
– Inhaled insulin: Afrezza®
– Regular - Novolin ®, Humulin ®, Relion®
• Longer-acting :– NPH: Novolin ®,
Humulin ®, Relion®
– Glargine: Lantus ®• U300: Toujeo®
– Detemir: Levemir®
– Degludec: Tresiba®• U100 and U200
Options for insulinBasal- Insulin Onset Peak Duration
NPH 1-2 hrs 4-8 hrs 14-18 hrs
Detemir 1-4 hrs 4-6 hrs 12-20 hrs
Glargine 1-6 hrs Flat 22-24 hrs/24-36 hrs (U300)
Degludec 1-9 hrs 10-12 hrs 42 hours
Bolus- Insulin Onset Peak Duration
Regular 30-60 min 2-4 hrs 4-8 hrsAspart, lispro, glulisine
5-15 min 1-2 hrs 3-5 hrs
Inhaled insulin
~ 15 min ~ 50 min 3 hours
9
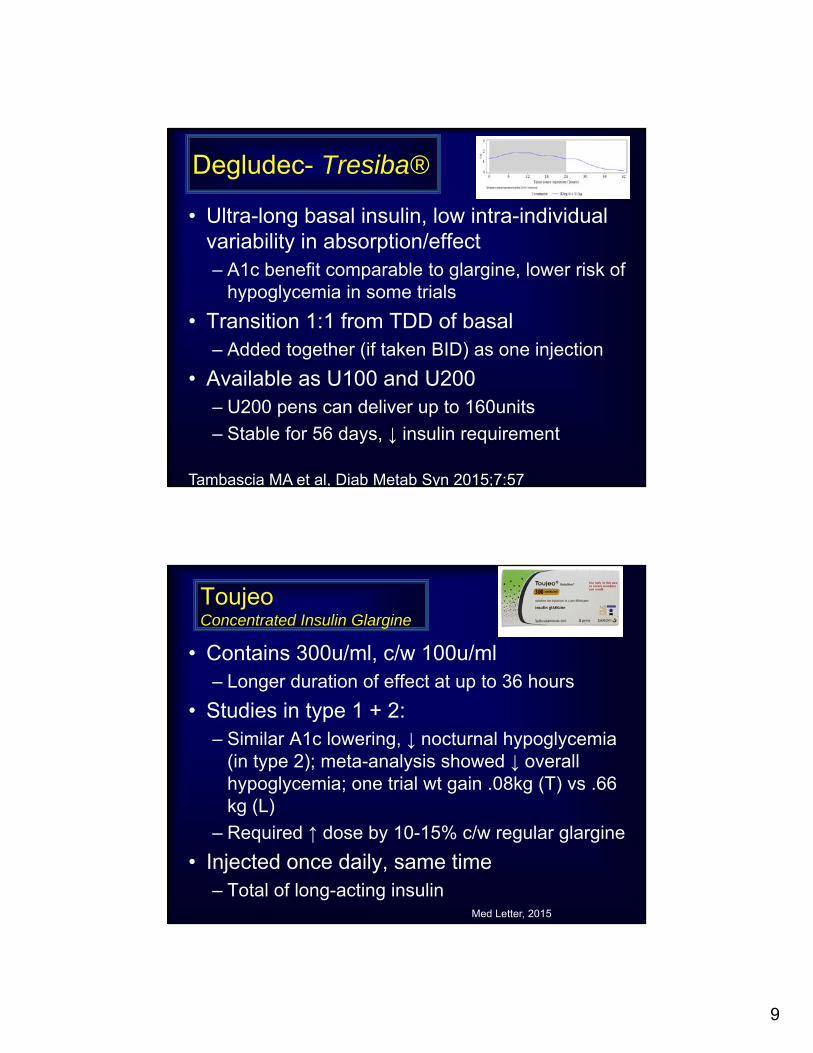
Degludec- Tresiba®
• Ultra-long basal insulin, low intra-individual variability in absorption/effect– A1c benefit comparable to glargine, lower risk of
hypoglycemia in some trials
• Transition 1:1 from TDD of basal– Added together (if taken BID) as one injection
• Available as U100 and U200– U200 pens can deliver up to 160units
– Stable for 56 days, ↓ insulin requirement
Tambascia MA et al, Diab Metab Syn 2015;7:57
ToujeoConcentrated Insulin Glargine
• Contains 300u/ml, c/w 100u/ml – Longer duration of effect at up to 36 hours
• Studies in type 1 + 2:– Similar A1c lowering, ↓ nocturnal hypoglycemia
(in type 2); meta-analysis showed ↓ overall hypoglycemia; one trial wt gain .08kg (T) vs .66 kg (L)
– Required ↑ dose by 10-15% c/w regular glargine
• Injected once daily, same time– Total of long-acting insulin
Med Letter, 2015
10
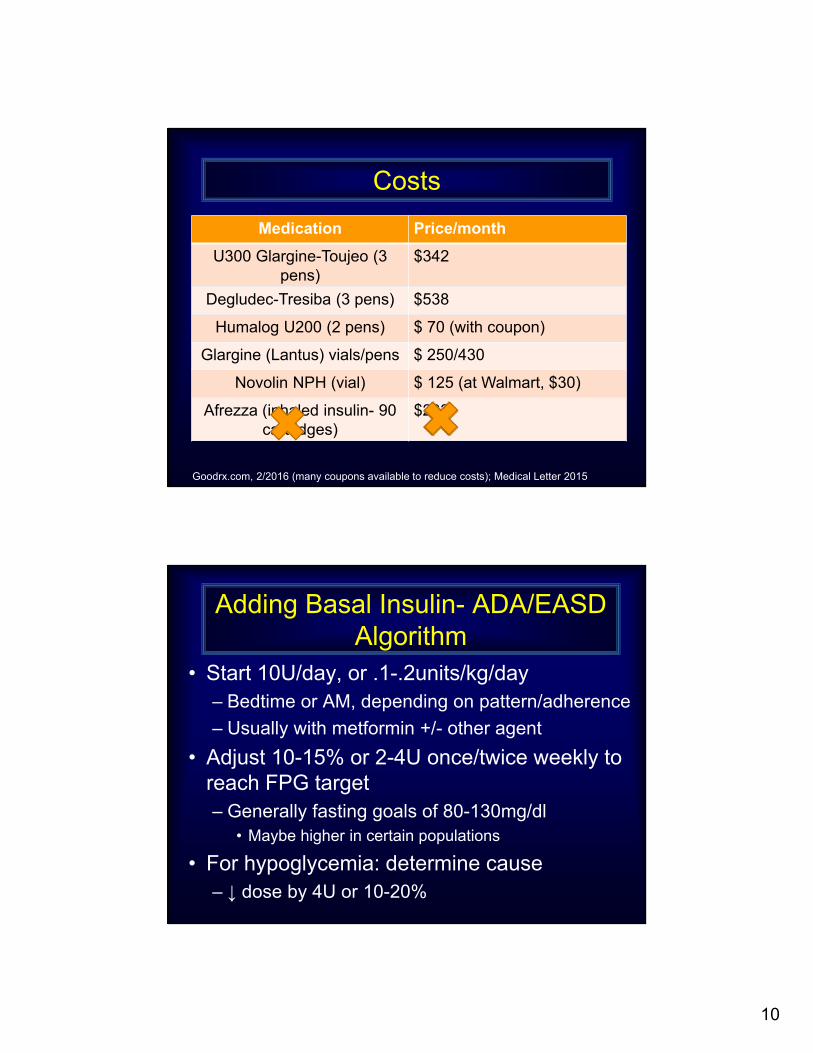
Costs
Goodrx.com, 2/2016 (many coupons available to reduce costs); Medical Letter 2015
Medication Price/month
U300 Glargine-Toujeo (3 pens)
$342
Degludec-Tresiba (3 pens) $538
Humalog U200 (2 pens) $ 70 (with coupon)
Glargine (Lantus) vials/pens $ 250/430
Novolin NPH (vial) $ 125 (at Walmart, $30)
Afrezza (inhaled insulin- 90 cartridges)
$233
Adding Basal Insulin- ADA/EASD Algorithm
• Start 10U/day, or .1-.2units/kg/day– Bedtime or AM, depending on pattern/adherence
– Usually with metformin +/- other agent
• Adjust 10-15% or 2-4U once/twice weekly to reach FPG target– Generally fasting goals of 80-130mg/dl
• Maybe higher in certain populations
• For hypoglycemia: determine cause– ↓ dose by 4U or 10-20%

11
Back to Case
AM Noon Dinner Hs
134 213 168 224
125 151 184 245
161 143 232 212
152 175 215 286
143 121 186 312
- Started on glargine 15units hs, titrated up to 45units- A1c dropped to 8.2%- Largest meal tends to be dinner, but not always- Since starting insulin has gained 8#
When to add bolus?
• Basal should be 50% of total daily dose (TDD)– Estimate based on TDD
1-2u/kg/day
– Generally consider if using> 60-70unts per day basal, or considering splitting glargine
– A1c above goal
– Start with largest meal

12
Alternatives to consider
• When you need to add to basal insulin:– GLP-1 or SGLT2 medications
• Effective to control BG + weight loss + ↓ hypoglycemia
• Consider as alternative to meal insulin– Comparison of basal+ bolus TID or albiglutide showed
comparable A1c lowering, wt loss with GLP1 and more hypoglycemia with bolus insulin (Rosenstock et al, Diab Care 2014)
– TZD also an option• ↑ fluid retention, weight gain when used with insulin
Case continued
• Gets started on pre-dinner lispro (humalog®), and occasionally pre-lunch if eating out
• Taking 10-12units with those meals, BG has improved
• Went to the pharmacy to pick up prescriptions and price has gone up dramatically
• Are there any less costly options for insulin?
13
Don’t Overlook NPH and Regular
• Among privately insured adults + DM2– 19% using analogs in 2000, c/w 96% in 2010
– From 2001 → 2015, lispro vials increased from $35 → $234, human insulin $20 → $131
• LOTS of marketing with insulin analogs– Emphasizing more physiologic, less
hypoglycemia
• No difference in A1c, no data on outcomes or complications
Tylee T, Hirsch I, JAMA 2015
Trials that Compare Basal Initiation
• Treat to Target- NPH vs glargine 1
– Equivalent A1c achieved with less nocturnal hypoglycemia in those using glargine
• Comparison of NPH and detemir 2
– Equivalent A1c achieved with less hypoglycemia (47%) and slightly less wt gain with detemir
• Degludec vs Glargine 3
– No difference in A1c, less nocturnal hypoglycemia with degludec
1-Riddle MC, Diab Care 2003;26:3080; 2- Hermansen K, Diab Care 2006;29:1269;3- Garber et al, Lancet 2012;379:1498
14
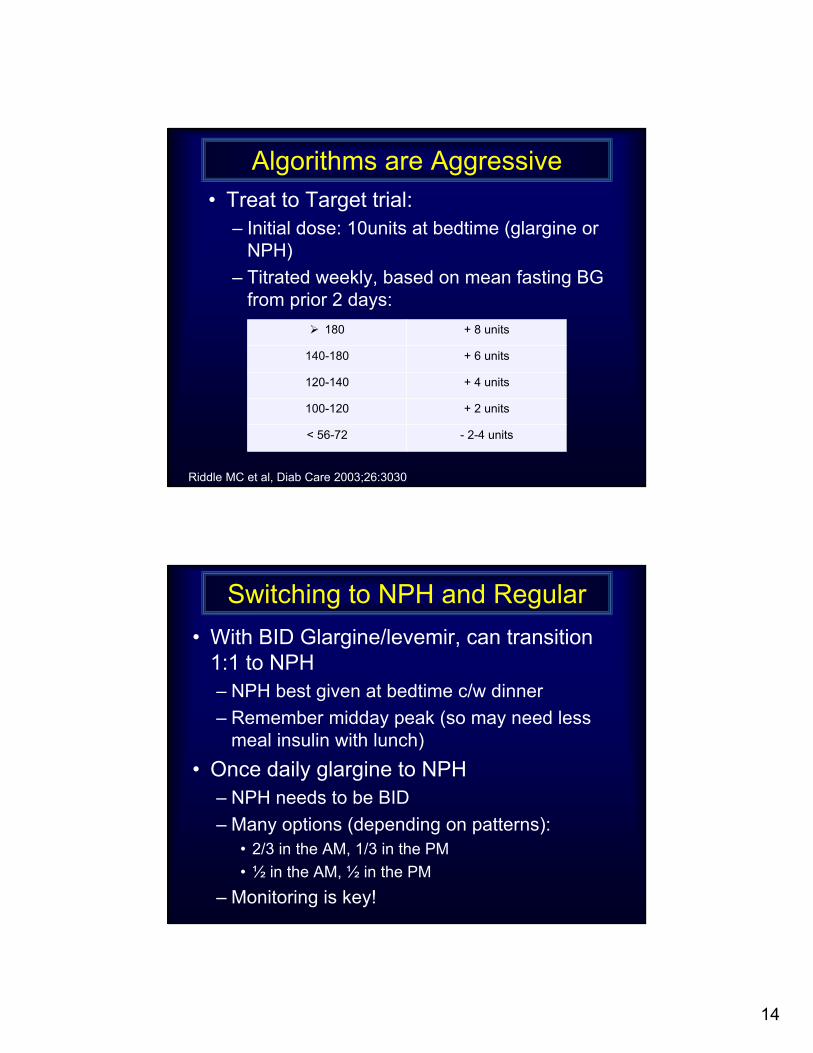
Algorithms are Aggressive
Riddle MC et al, Diab Care 2003;26:3030
• Treat to Target trial:– Initial dose: 10units at bedtime (glargine or
NPH)
– Titrated weekly, based on mean fasting BG from prior 2 days:
180 + 8 units
140-180 + 6 units
120-140 + 4 units
100-120 + 2 units
< 56-72 - 2-4 units
Switching to NPH and Regular
• With BID Glargine/levemir, can transition 1:1 to NPH– NPH best given at bedtime c/w dinner
– Remember midday peak (so may need less meal insulin with lunch)
• Once daily glargine to NPH– NPH needs to be BID
– Many options (depending on patterns):• 2/3 in the AM, 1/3 in the PM
• ½ in the AM, ½ in the PM
– Monitoring is key!

15
Mealtime insulin
• When switching to Regular insulin (Novolin ®, Humulin ®, Relion®) from analog (Lispro:Humalog®, Aspart: Novolog®, Glulisine: Apidra®)
• Same dose as analog insulin, given with meals
• Given 30 minutes before eating ??– Study of 100pts given regular at time of eating vs 20 min
prior
» No difference in A1c and much higher satisfaction when taken with meal (Muller N, Diabetes Care 2013;36:1865)
• Consider referral to teach how to mix insulin (reduce injection frequency)
Conclusions
• DM is complicated
• Newer isn’t necessarily better– But lots of direct-to-consumer marketing,
so good to have some familiarity
• Cost an ongoing challenge
• More people have diabetes but:– Management is improving
– Fewer complications
16
THE END


















