The use of fibrin sealant in burn operations
5
The use of fibrin sealant in burn operations Kevin Foster, MD, Phoeniz, Ariz The surgical technique of early excision and grafting has revolutionized the care of severe burns but can be associated with major surgical bleeding. The use of tourniquet exsanguination to prepare limbs for the procedure and the use of topical thrombin and fibrin sealants on the excised area can provide an essentially bloodless field. Even on more difficult sites like the torso and on the graft donor sites, blood loss can be reduced dramatically with the use of topical sealants. Fibrin sealants also can be employed to facilitate graft adherence and thus improve graft survival and cosmetic results. (Surgery 2007;142:S50-S54.) From the Arizona Burn Center, Phoenix, Ariz Fibrin sealants have had an important impact on 3 major problems in burn operations: intraopera- tive blood loss, graft survival, and cosmetic result. As so graphically described and illustrated in the book and movie, The English Patient, 1 before about 1980, burn patients were kept in the hospital, wait- ing for spontaneous separation of the burn eschar. Then the surgeons would do skin grafting. Around 1980, through observations that had been accumu- lating through the previous 2 decades, clinicians in the field realized that mortality for a relatively large burn was unnecessarily high. 2 Rather than waiting for the burn eschar to separate spontaneously, burn surgeons began to advocate active surgical intervention, using a process called tangential ex- cision. Ideally, this process surgically excises the dead tissue and leaves the live, functional tissue as a bed for the skin graft. Grafting is performed either immediately or after a short delay, if there is concern about the wound bed viability. Excision and grafting is one of the most significant advances in the surgical management of burn patients in the last 100 years. It resulted in much lower mortality, much lower morbidity, and much shorter length of hospital stay. 3 It also resulted in better functional and cosmetic outcomes. BLOOD LOSS The technique of tangential excision has created some interesting problems. As noted, the goal of tangential excision is to remove the nonviable and to preserve the viable tissue. The clearest sign of viable tissue is bleeding. A wound that is bleeding probably is healthy enough to support a skin graft, and the excision can stop at that point. Even using specialized excision equipment such as a Weck or Guillion knife, which are essentially razor blades with a depth guide on them, excised wounds bleed profusely. When excision is used on multiple extrem- ities and the trunk of a patient with a large total body surface area burn, the blood loss from these oozing surfaces is remarkable, even when performed in 3 or 4 surgical sessions. In addition, the skin donor sites also bleed. So the overall blood loss from full thickness burn excision and grafting procedures is a major issue in modern burn care. 4 By 1990, with a decade or more experience with this technique, the expected blood loss for tangential excision was about 0.75 mL/cm 2 excised, which meant that the average adult patient with a 25% total body surface area burn would have about 3000 cm 2 to be excised and could be expected to lose about 2200 mL, that is, four and a half units of blood. This blood loss is considerable for a relatively small operation. Another half unit of blood may be lost from the donor site, making the loss average adults half their total blood volume. Over the period of time that tangential excision has come into its own, the medical and surgical communities also have become much more aware of the risks of transfusion: Although le- Accepted for publication June 15, 2007. STATEMENT OF CONFLICT OF INTEREST: Kevin Foster, MD, reports having no conflicts of interest with the sponsor of this supplement article or the products discussed in this article. Reprint requests: Kevin Foster, MD, MBA, FACS, The Arizona Burn Center, Maricopa Medical Center, 2601 E. Roosevelt, Phoenix, AZ 85008. E-mail: [email protected]. 0039-6060/$ - see front matter © 2007 Mosby, Inc. All rights reserved. doi:10.1016/j.surg.2007.06.026 S50 SURGERY
-
Upload
kevin-foster -
Category
Documents
-
view
215 -
download
1
Transcript of The use of fibrin sealant in burn operations

The use of fibrin sealant inburn operationsKevin Foster, MD, Phoeniz, Ariz
The surgical technique of early excision and grafting has revolutionized the care of severe burns butcan be associated with major surgical bleeding. The use of tourniquet exsanguination to prepare limbsfor the procedure and the use of topical thrombin and fibrin sealants on the excised area can providean essentially bloodless field. Even on more difficult sites like the torso and on the graft donor sites,blood loss can be reduced dramatically with the use of topical sealants. Fibrin sealants also can beemployed to facilitate graft adherence and thus improve graft survival and cosmetic results.(Surgery 2007;142:S50-S54.)
From the Arizona Burn Center, Phoenix, Ariz
Fibrin sealants have had an important impact on3 major problems in burn operations: intraopera-tive blood loss, graft survival, and cosmetic result.As so graphically described and illustrated in thebook and movie, The English Patient,1 before about1980, burn patients were kept in the hospital, wait-ing for spontaneous separation of the burn eschar.Then the surgeons would do skin grafting. Around1980, through observations that had been accumu-lating through the previous 2 decades, clinicians inthe field realized that mortality for a relatively largeburn was unnecessarily high.2 Rather than waitingfor the burn eschar to separate spontaneously,burn surgeons began to advocate active surgicalintervention, using a process called tangential ex-cision. Ideally, this process surgically excises thedead tissue and leaves the live, functional tissue asa bed for the skin graft. Grafting is performedeither immediately or after a short delay, if there isconcern about the wound bed viability. Excisionand grafting is one of the most significant advancesin the surgical management of burn patients in thelast 100 years. It resulted in much lower mortality,much lower morbidity, and much shorter length of
Accepted for publication June 15, 2007.
STATEMENT OF CONFLICT OF INTEREST: Kevin Foster,MD, reports having no conflicts of interest with the sponsor ofthis supplement article or the products discussed in this article.
Reprint requests: Kevin Foster, MD, MBA, FACS, The ArizonaBurn Center, Maricopa Medical Center, 2601 E. Roosevelt,Phoenix, AZ 85008. E-mail: [email protected].
0039-6060/$ - see front matter
© 2007 Mosby, Inc. All rights reserved.
doi:10.1016/j.surg.2007.06.026
S50 SURGERY
hospital stay.3 It also resulted in better functionaland cosmetic outcomes.
BLOOD LOSSThe technique of tangential excision has created
some interesting problems. As noted, the goal oftangential excision is to remove the nonviable andto preserve the viable tissue. The clearest sign ofviable tissue is bleeding. A wound that is bleedingprobably is healthy enough to support a skin graft,and the excision can stop at that point. Even usingspecialized excision equipment such as a Weck orGuillion knife, which are essentially razor bladeswith a depth guide on them, excised wounds bleedprofusely. When excision is used on multiple extrem-ities and the trunk of a patient with a large total bodysurface area burn, the blood loss from these oozingsurfaces is remarkable, even when performed in 3or 4 surgical sessions. In addition, the skin donorsites also bleed. So the overall blood loss from fullthickness burn excision and grafting procedures isa major issue in modern burn care.4
By 1990, with a decade or more experience withthis technique, the expected blood loss for tangentialexcision was about 0.75 mL/cm2 excised, whichmeant that the average adult patient with a 25% totalbody surface area burn would have about 3000 cm2 tobe excised and could be expected to lose about 2200mL, that is, four and a half units of blood. This bloodloss is considerable for a relatively small operation.Another half unit of blood may be lost from thedonor site, making the loss average adults half theirtotal blood volume. Over the period of time thattangential excision has come into its own, the medicaland surgical communities also have become much
more aware of the risks of transfusion: Although le-
Surgery Foster S51Volume 142, Number 4S
thal outcomes from individual units are rare—1 in10,000 to 1 in 100,000 reported to the Phoenix BloodBank—the more units transfused, the more likely theadverse outcome.5
Hemorrhage control now is a major focus of sur-gical technique with burns.6-8 The procedure must beperformed rapidly. A skilled burn surgeon may notbe able to tie a laparoscopic knot in less than 3 min,but the surgeon can excise a 20% burn in about 5min. The classic way to care for burn patients surgi-cally is to excise the burn and place nonadherentdressings soaked in warm epinephrine solution(10-20 mg/L) on the open areas of excised burn. Theepinephrine provides some hemostasis by capillarycontraction. This process works fairly well but takestime and a fair amount of blood is lost in the interim.More recently, the addition of thrombin at about10,000 units/L to the solution enhances hemostasisby facilitating activation of the clotting cascade.
Tourniquet exsanguination is a useful physicaltechnique for extremities. It involves the applicationof an inflatable tourniquet, exsanguination of theextremity by wrapping, and then inflation of the tour-niquet. The excision is then performed, the dress-ings is soaked in epinephrine, thrombin are placedon the wound, and the tourniquet is deflated. Al-though this procedure reduces blood loss, it doesnot eliminate it and blood loss still is substantial.Another technique used less now than in the past issubcutaneous clysis or subeschar clysis. It involvesinjecting a solution of epinephrine, thrombin, andsterile saline under the burn before excision.9 Epi-nephrine and thrombin provide some vasoconstric-tion and topical hemostasis during the excision and
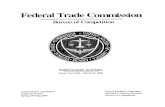
Fig 1. Sheet graft. Sheet grafts taken from unaffected sitesof the donor’s skin tend to have a more natural look thanthe mesh graft; however, they tend to be more delicate, andin extensive burns, the donor generally does not haveenough skin available to cover the burned areas.
help limit blood loss, but the procedure is not
ideal. It can interfere with the appearance of thewound and often results in the excision of moretissue than necessary. It also takes a long time. Inpediatric and elderly patients, it can result in sig-nificantly excess fluid loads.
ENGRAFTMENTDescribed here are some of the major reasons why
skin grafts fail. If the bed was not excised adequatelyand dead tissue remains under the graft, the graft willnot adhere. It will not revascularize, and it will fail.New grafts also are particularly susceptible to shearforces. If the patient gets up and walks, if the dressingslips, or if the patient rolls over in bed, sufficient shearforce can be generated to lift the graft off of thewound bed. Fluid collections, seromas, and hemato-mas can form under the graft and, in essence, float itoff. Particularly given a nidus of dead tissue or collec-tions of fluid, infections can destroy a wound bed andnascent revascularization. Burn patients have tremen-dous metabolic needs; inadequate nutrition may in-hibit and result in graft failure.
COSMETIC RESULTSIn burn operations, skin grafts are generally di-
vided into 2 general types, sheet grafts (Fig 1) andmesh grafts (Fig 2). A sheet graft is skin taken as isfrom the donor site. It is laid onto the excised
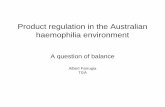
Fig 2. Mesh graft. Mesh grafts can cover a much largersurface area than sheet grafts; however, they tend to scarand should be avoided in highly visible areas.
wound and secured into place. Patients with large,

S52 Foster SurgeryOctober 2007
percent body-surface-area burns will not have suffi-cient normal healthy skin to provide extensivesheet grafts. In this circumstance, available skin canbe meshed and expanded in a variety of ways tocover much larger surface areas than the originalsheet. Unfortunately, mesh grafts scar and contractmuch more than sheet grafts. They were used ex-tensively, even for relatively small burns, whichshould be considered inexcusable in current prac-tice. Mesh grafts should be avoided entirely inhighly visible areas or areas where significant scarcontraction will cause problems with sensation ormobility. Wherever a mesh graft is placed, the cli-nician must remember that the grid pattern ofmesh graft healing is permanent (Fig 3).
In general, therefore, sheet grafts are prefera-ble. Less contraction occurs, color tends to be bet-ter, and no meshed pattern of scarring exists.However, sheet grafts are somewhat more sensitivethan mesh grafts; they tend not to take as well.Suturing or stapling of sheet grafts—that is, in-troduction of any unnecessary defects in thesheet, any potential interference with microcir-culation—should be avoided. Fluid also collectsmore readily under sheet grafts, so they are more
Fig 3. Results of a mesh graft. Mesh grafts leave a per-manent grid pattern on the healed graft.
vulnerable to loss by that means. They also are
more subject to shear forces, so they must bedressed and managed more carefully. Any noveltechniques that improve survival of sheet grafts aregoing to improve overall cosmetic results.
TISSUE SEALANT IN BURN SURGERY:HEMOSTASIS
Burn surgeons always are looking for new ways tolimit intraoperative blood loss and improve autograftsurvival and enhance cosmetic results. Fibrin sealantswere introduced into burn care and burn operationsabout 15 years ago for hemostasis and for graft ad-herence.10,11 Used in an excision procedure withtourniquet exsanguinations, fibrin sealants can resultin a truly bloodless field.12,13 The tourniquet isplaced, the extremity is exsanguinated by pressure asdescribed, and then the tourniquet is inflated to 200-250 mm Hg. The burn is excised, leaving an essen-tially bloodless wound, and fibrin sealant is sprayedover the open wound. After a pause of several min-utes to allow the fibrin sealant to set up, the epineph-rine/thrombin-soaked Telfa pads are placed on thewound. Placed too soon, the pads will adhere andmay require excision to remove them. Once the Telfapads are appropriately placed, they are secured gentlywith Ace wrap (BD, Franklin Lakes, NJ), and thetourniquet is deflated. At that point, the skin graftscan be harvested from the donor sites and prepared.After about 10 min, the epinephrine-soaked Telfapads are removed from the excised area. The woundis completely dry, completely excised, and ready forskin grafting.
Excision and grafting on the torso are more diffi-cult because tourniquet exsanguination is not an op-tion. Under those circumstances, a sequentialexcision is performed, which is an extremely unpleas-ant, bloody operation. Since the advent of fibrinsealants, however, although the procedure is notsimple, it can be performed such that it limitsblood loss. A much larger knife is used, allowinglarge swaths to be removed in a few quick swipes,followed by rapid application of fibrin sealant. Aswith the extremity procedure, there is an intervalof a few minutes while the sealant sets, then theepinephrine-soaked Telfa pads are applied andthe team moves on to the next area. The result isa sequential procedure, excising and achievinghemostasis stepwise across the burn area until thegraft bed is satisfactory. Of course, the nature ofburn operations can be horrifying. But fibrinsealants have brought to this field the ability notonly to do this operation with considerably in-creased safety but also with success. The ArizonaBurn Center in Phoenix admitted over 800 burn
patients in 2006, most of whom underwent 1 or
Surgery Foster S53Volume 142, Number 4S
more operations. Most of these patients will havebeen treated with Tisseal (Immuno, Vienna, Aus-tria) or another fibrin sealant in almost everyoperation. Blood loss and the rate of transfusionshave both plummeted over the years as a result.
TISSUE SEALANTS IN BURN OPERATIONS:ADHERENCE
As noted, thrombin has become a mainstay inburn operations in many centers. For hemostasis, theusual concentration of the solution is 500 units/mL.Only about 1/100 of that concentration, 4 to 5 units/mL, is needed to support adherence. With the re-duced concentration, the fibrin sealant does not setup as quickly, giving the surgical team a couple min-utes to manipulate a skin graft on the wound beforethe thrombin starts to become sticky. Full-strengthfibrin sealant sets up immediately and therefore isdifficult to use as an adhering mechanism. The moredilute thrombin solution allows a little extra timebetween placement of the graft and when the throm-bin begins to adhere. The graft is oriented appropri-ately on the prepared wound site and tacked downwith a couple of sutures, and then it is folded back toexpose the wound surface. The wound surface issprayed with sealant (Fig 4), and the graft is flappedback down over it and secured lightly. In the past,securing usually was done with a few sutures. Thegrafting described here generally is finished with afew steri-strips, with or without a few absorbable su-tures, depending on the situation. Then the wound
Fig 4. Graft adherence. After the graft is positioned onthe prepared wound, it is tacked down with a few suturesand then folded back to expose the wound surface. Thewound surface is sprayed with sealant; a dilute thrombinsolution allows a little extra time between placement ofthe graft and when the thrombin begins to adhere. Thegraft is flapped back down over the wound and securedlightly, generally with a few steri-strips, with or without afew absorbable sutures.
is dressed.
A study conducted at our center several years agodemonstrated that the use of fibrin sealant versusstaples for stabilizing and securing sheet grafts essen-tially are equivalent from the surgeon’s point of viewin the operating room (Foster, unpublished data).Postoperatively, however, patients much prefer thefibrin sealant over the staples (Fig. 5, A and B). Thestaples pull uncomfortably when the person moves,and removing them is painful.
PROBLEMS IN THE USE OF TISSUESEALANTS IN BURN OPERATIONS
Early experience with fibrin sealants in burn oper-ations was probably not dissimilar to its early use invascular operations: The biggest problem was learn-
Fig 5. Results of fibrin sealant versus staples. The pa-tient’s wound pictured here is sealed with both fibrinsealant (patch A) and staples (patch B). On postopera-tive day 0 (A), the staples are apparent on the top edgeof patch B. By postoperative day 21 (B), not much dif-ference is found in the results of the 2 methods. The 2techniques for stabilizing and securing sheet grafts areequivalent in terms of operative time and cosmetic ap-pearance. Patients prefer the fibrin sealant, however,because staples pull on the skin during movement andhurt when they are removed.
ing to mix the 2 components of the sealant in a

S54 Foster SurgeryOctober 2007
correct and timely manner, which requires trainingand practice. The delivery systems always have beenmildly problematic.14 The dual tube delivery systemsare awkward and tend to clog. The new delivery sys-tems are better, but they still must be handled withcare.15 The scrub nurse or technicians often hadproblems drawing up the sealant from the circulatingnurse, and in the past, it was not unusual for thesurgeon to have to scrub out and prepare the sealant.As with any procedure only performed occasionally, 1or 2 cases per week, the learning curve was both flatand bumpy. The issue develops as to whether thesealant should be managed by the pharmacy at anygiven center; however, it is unusual to have well-coordinated protocols between the pharmacy and thesurgical suite, and most surgeons prefer to managesealant use directly.
The cost of fibrin sealants is considerable; how-ever, so is the cost of blood, which is expensive inmore than just a monetary way. In our institution,operative time has dropped dramatically as has blooduse. The use of staples and suture materials also hasdecreased. Less time is spent waiting for hemostasis.In addition, the anecdotal experience in our group isthat graft loss also has decreased. Less wound care isrequired; staples do not need to be removed; nordoes a 4-year-old with a 20% total body-surface-areaburn with a graft require conscious sedation to re-move staples, which was common in the past. Lengthof hospital stay has decreased, and again as an anec-dotal observation from our institution, the need foradditional operations seems to have decreased. Over-all, the net cost is decreased costs, and our experienceis not unique.16
CASE SELECTIONThe best cases for fibrin sealants as hemostatic
agents are early excision of a large burn or an extrem-ity burn. Fibrin sealants are useful as fixation agentsin virtually all cases, but they definitely should beconsidered if a sheet graft is planned or if the graftsite involves crucial areas, particularly cosmeticallyimportant areas like the face or the hands where anydegree of graft loss results in unacceptable cosmeticdeformity. Fibrin sealants also offer critical advan-tages in pediatric cases, particularly in the reducedneed for postoperative wound care. For those forwhom blood transfusion is unacceptable, the employ-ment of fibrin sealants to reduce blood loss can liter-ally make the difference between life and death.
CONCLUSIONThe most remarkable thing that fibrin sealants
have done for burn operations is markedly decreased
blood loss. The use of fibrin sealants has taken bloodloss in burn operations from massive to virtually nonefor extremity burns. In addition, their use has de-creased operative time and resulted in better graftadherence and graft take and in less complicatedpostoperative care. The latter is especially true andespecially important for pediatric patients. Finally,cosmetic results are improved. Problems with theiruse include the persistent complexity of preparationand application, which is even more of a problem forpeople who use the currently available fibrin sealantsrelatively rarely. Those who use them more frequentlyhave worked out solutions for their particular needs,and for them, the advantages to fibrin sealant usenow far outweigh the problems. These products areexpensive in themselves, but their use contributesto overall decreases in the cost of burn care, bothfinancially and in terms of morbidity.
REFERENCES1. Ondaatje M. The English patient. London: Bloomsbury
Publishing Ltd.; 1992.2. Heimbach DM, Engrav LH, Marvin JA. Advances in burn
care. West J Med 1981;134:274-9.3. Gray DT, Pine RW, Harnar TJ, Marvin JA, Engrav LH,
Heimbach DM. Early surgical excision versus conventionaltherapy in patients with 20 to 40 percent burns. A compar-ative study. Am J Surg 1982;144:76-80.
4. Monafo WW, Bessey PQ. Benefits and limitations of burnwound excision. World J Surg 1992;16:37-42.
5. Palmieri TL, Caruso DM, Foster KN, Cairns BA, Peck MD,Gamelli RL, et al. Effect of blood transfusion on outcomeafter major burn injury: a multicenter study. Crit Care Med2006;34:1602-7.
6. Palmieri TL, Greenhalgh DG. Blood transfusion in burns:what do we do? J Burn Care Rehabil 2004;25:71-5.
7. Sheridan RL, Szyfelbein SK. Trends in blood conservationin burn care. Burns 2001;27:272-6.
8. Niemi T, Svartling N, Syrjala M, sko-Seljavaara S, Rosenberg P.Haemostatic disturbances in burned patients during early exci-sion and skin grafting. Blood Coagul Fibrinolysis 1998;9:19-28.
9. Beausang E, Orr D, Shah M, Dunn KW, Davenport PJ.Subcutaneous adrenaline infiltration in paediatric burn sur-gery. Br J Plast Surg 1999;52:480-1.
10. Spotnitz WD, Dalton MS, Baker JW, Nolan SP. Successfuluse of fibrin glue during 2 years of surgery at a universitymedical center. Am Surg 1989;55:166-8.
11. Ofodile FA, Sadana MK. The role of topical thrombin inskin grafting. J Natl Med Assoc 1991;83:416-8.
12. Losee JE, Fox I, Hua LB, Cladis FP, Serletti JM. Transfusion-free pediatric burn surgery: techniques and strategies. AnnPlast Surg 2005;54:165-71.
13. Cartotto R, Musgrave MA, Beveridge M, Fish J, Gomez M. Mini-mizing blood loss in burn surgery. J Trauma 2000;49:1034-9.
14. Spotnitz WD. Commercial fibrin sealants in surgical care.Am J Surg 2001;182:8S-14.
15. Jackson MR. New and potential uses of fibrin sealants as anadjunct to surgical hemostasis. Am J Surg 2001;182:36S-9.
16. McGill V, Kowal-Vern A, Lee M, Greenhalgh D, Gomperts E,Bray G, et al. Use of fibrin sealant in thermal injury. J Burn
Care Rehabil 1997;18:429-34.