The Spinal Cord Honors Anatomy& Physiology for copying.
28
The Spinal Cord Honors Anatomy& Physiology for copying
-
Upload
blaise-baldwin -
Category
Documents
-
view
231 -
download
0
Transcript of The Spinal Cord Honors Anatomy& Physiology for copying.

The Spinal Cord
Honors Anatomy& Physiologyfor copying

Spinal Cord
• w/spinal nerves contain neural circuits that mediate some of your most rapid reactions to environmental changes
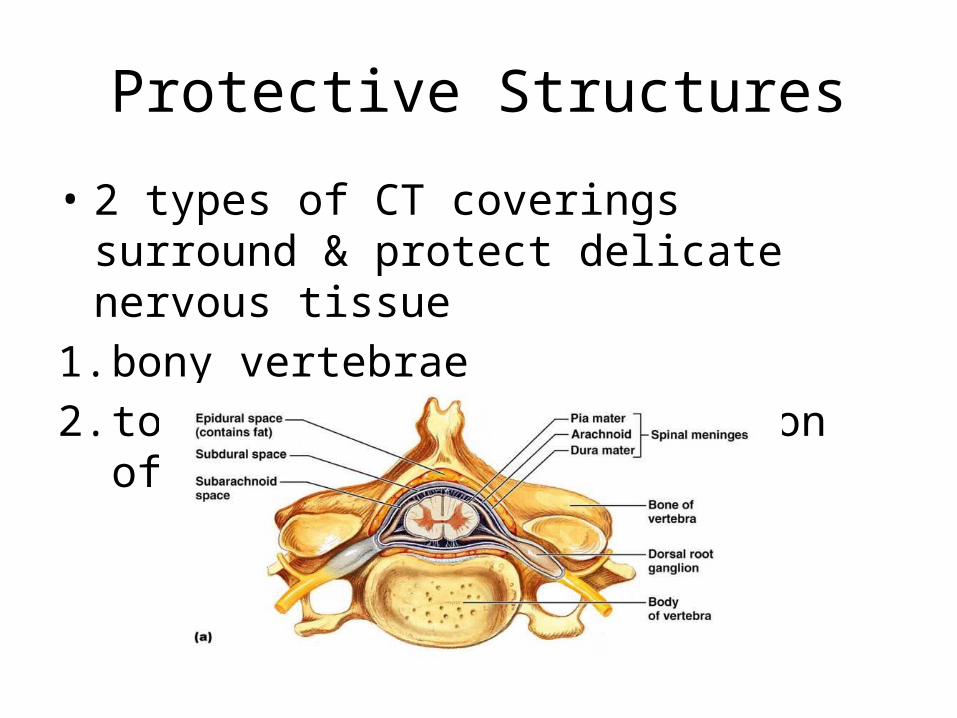
Protective Structures
• 2 types of CT coverings surround & protect delicate nervous tissue
1. bony vertebrae2. tough CT meninges, w/cushion of
CSF

Meninges
• 3 CT coverings that encircle spinal cord & brain:
• Spinal meninges covers spinal cord• Cranial meninges covers brain

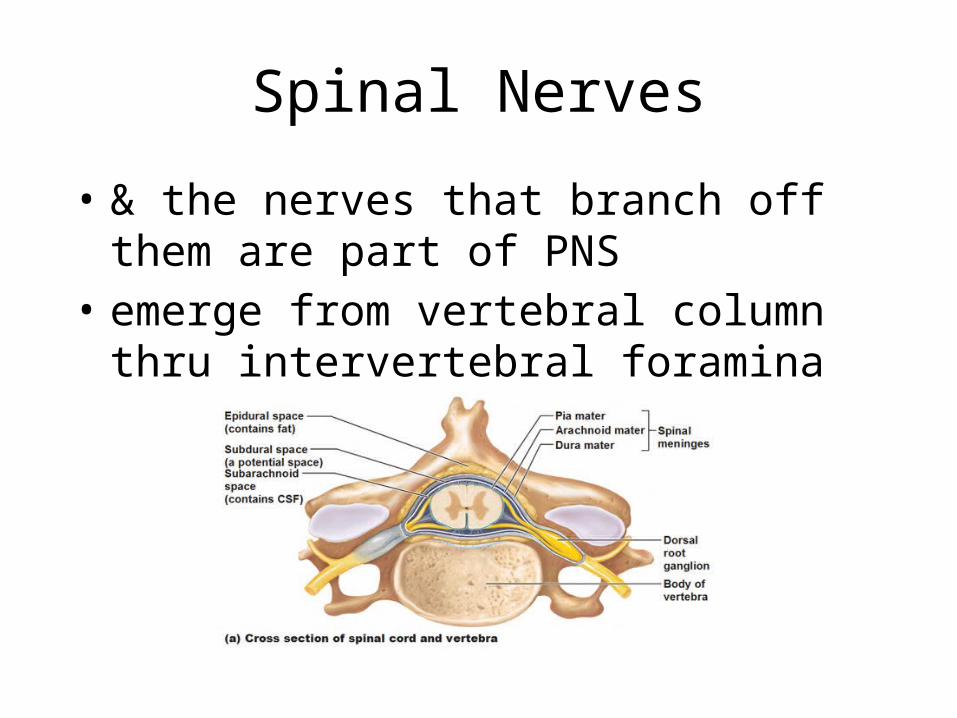
Meninges Layers: Dura Mater
• “tough mother”• most superficial layer• made of dense, irregular CT• continuous with cranial meninges• forms sac from foramen magnum S2• layer of adipose tissue between dura
mater & wall of vertebral cavity (epidural space)
Middle Meninges: Arachnoid Mater
• “spider-like”• deep to dura mater, superficial to pia
mater• contiguous with cranial arachnoid • between dura & arachnoid =
subdural space

Innermost Meninges:Pia mater
• “delicate”• thin, transparent CT• adheres to spinal cord & brain• between arachnoid & pia =
subarachnoid space
Spinal Tap
• aka lumbar puncture• long needle inserted into subarachnoid
space• adults: between L3 –L4 or L4 – L5
(inferior to lowest portion of spinal cord)
• purpose: withdraw CSF for– diagnostic purposes– insert antibiotics/contrast media for
myelography/ anesthetics/ chemotherapy

Spinal Cord
• cylindrical with flattening of its AP diameter
• adults:extends from medulla oblongata L2 vertebra
• newborns: extends to L3 or L4• elongation of spinal cord stops ~age
3-4 but growth of vertebral column continues

Spinal Cord: External View
• 2 obvious enlargements noted:– cervical enlargement• C4 – T1• serve upper limbs
– lumbar enlargement• T9- T12• serve lower limbs

Spinal Cord: External View
• conus medullaris: tapered conical structure of spinal cord below lumbar enlargement ending @ L1 – L2
• filum terminale: extension of pia mater extends inferiorly & anchors cord to coccyx
• cauda equinae: “horse tail” nerves that arise from lumbar, sacral, & coccygeal portions of spine
Spinal Nerves
• 31 pairs spinal nerves emerge thru intervertebral foramen
• 8 pair cervical nerves: C1 – C8• 12 pair thoracic nerves: T1 - T12• 5 pair lumbar nerves: L1 – L5• 5 pair sacral nerves: S1 – S5• 1 pair coccygeal nerves: Co1

Spinal Nerves
• 2 bundles of axons, called roots, connect each spinal nerve to segment of spinal cord
Spinal Cord Roots
1. posterior (dorsal) root– only sensory axons– each has dorsal root ganglion
containing cell bodies of sensory neurons
2. anterior (ventral) root– only motor axons

Internal Anatomy of Spinal Cord
• 2 grooves penetrate white matter & divide it in right & left sides:
1. anterior median fissure1. deeper, wider of the 2
2. posterior median sulcus1. shallower, narrow furrow
Spinal Nerves
• & the nerves that branch off them are part of PNS
• emerge from vertebral column thru intervertebral foramina
Spinal Nerves
• typically has 2 connections to spinal cord1. dorsal root (sensory)2. ventral root (motor)
• classified as “mixed”
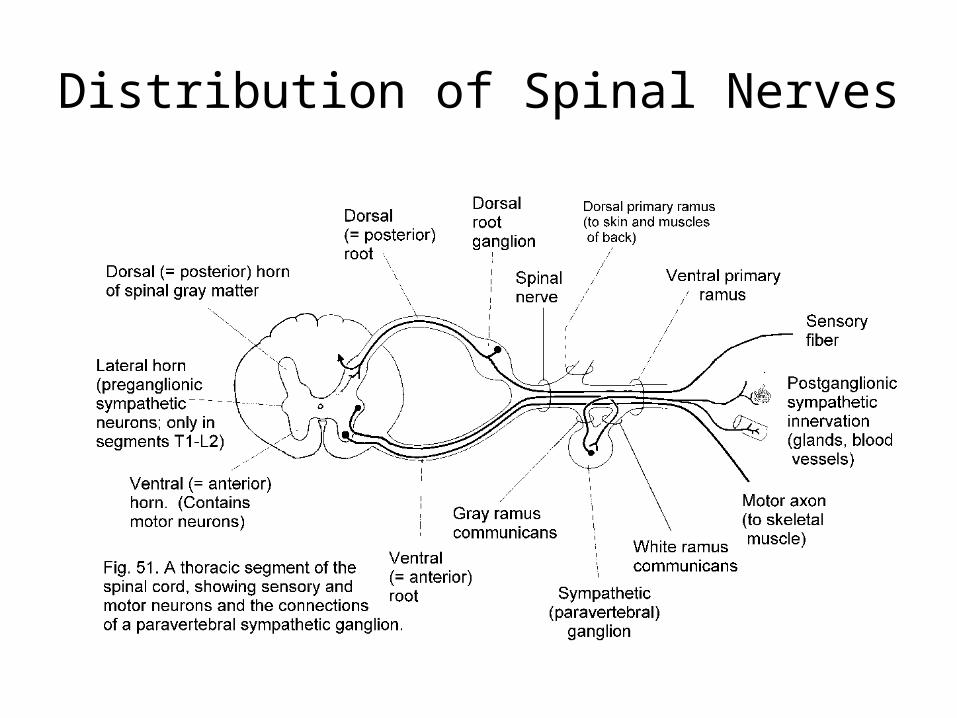
Distribution of Spinal Nerves

Spinal Nerve Plexuses
• a network of nerves (or veins, or lymphatic vessels)
Cervical Plexus
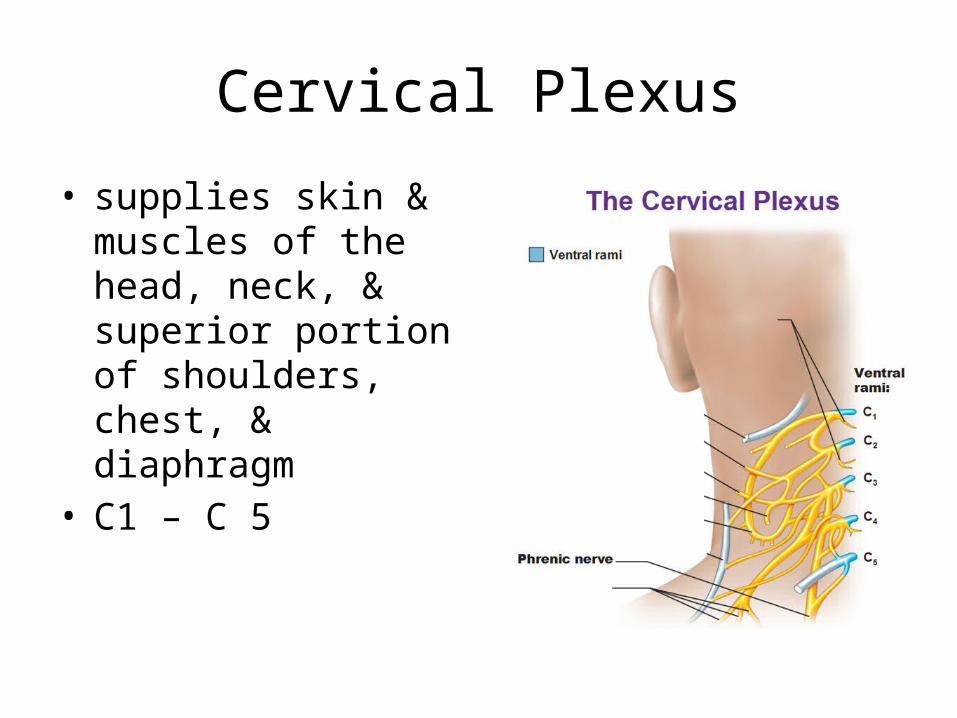
• supplies skin & muscles of the head, neck, & superior portion of shoulders, chest, & diaphragm
• C1 – C 5
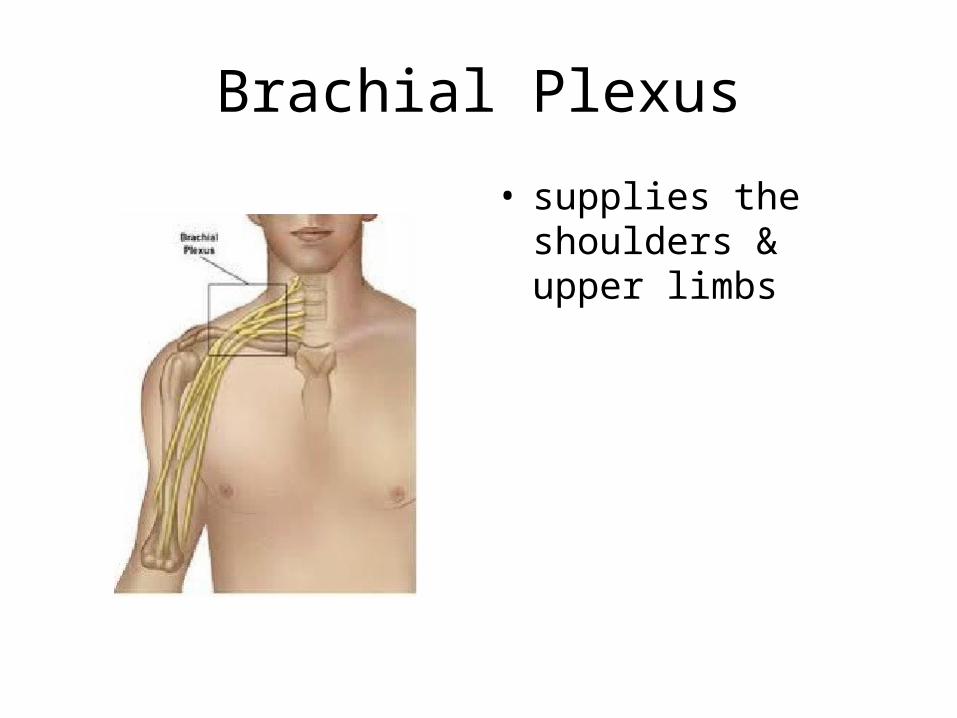
Brachial Plexus
• supplies the shoulders & upper limbs

Lumbar Plexus
• supplies anterolateral abd wall, external genitals, part of lower limb
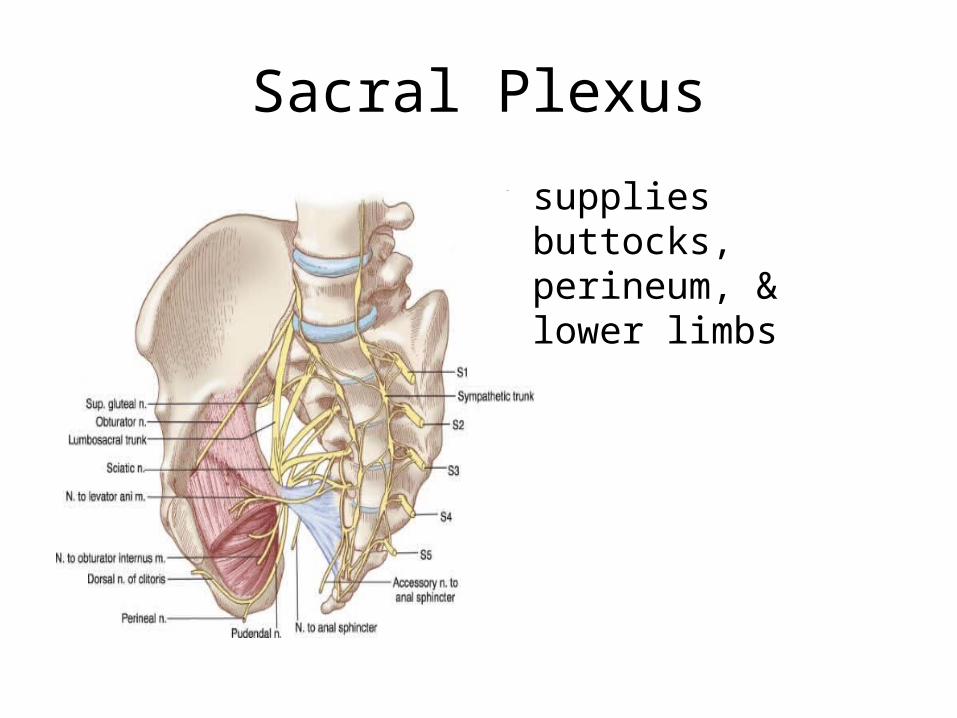
Sacral Plexus
• supplies buttocks, perineum, & lower limbs

Dermatomes
• cutaneous area developed from one embryonic spinal cord segment & receiving most of its sensory innervation from one spinal nerve
• knowing which spinal cord segments supply each dermatome makes it possible to locate damaged regions of the spinal cord
Spinal Cord Injuries
• most due to trauma– cervical, lower thoracic, upper lumbar
most common regions involved
• paralysis – depends on location, extent of damage–monoplegia: 1 limb– paraplegia: both lower limbs– hemiplegia: upper limb, trunk, lower
limb on 1 side of body– quadriplegia: all 4 limbs & trunk

Extent Muscle Paralysis
• C1 – C3: no function neck down, requires ventilator to breathe
• C4 – C5: diaphragm, allows breathing• C6 – C7: some arm, chest, allows breathing,
moving wheelchair• T1 – T3: intact arm function• T4 – T9: control of trunk above umbilicus• T10 – L1: most thigh muscles, walk w/long
leg braces• L1 – L2: most leg muscles, walk w/short leg
braces

Shingles
• acute infection of PNS • caused by herpes zoster (chicken
pox)• virus stays in posterior root ganglion– becomes reactivated normally immune
system will prevent it from spreading– reactivated virus can overcome
weakened immune system leaves ganglion travels down sensory neurons supplying skin

Medical Terminology• meningitis: inflammation of
meminges due to infection, bacterial (worse) or viral, vaccine protests against some bacterial causes: headache, N/V, fever, stiff neck
• neuralgia: pain along a sensory nerve, trigeminal neuralgia
• neuritis: inflammation of 1 or several nerves
• paresthesis: abnormal sensation