The Sepsis Timebomb - WordPress.com · The Sepsis Timebomb James Wigfull ... Shock to effective...
43
The Sepsis Timebomb James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals
Transcript of The Sepsis Timebomb - WordPress.com · The Sepsis Timebomb James Wigfull ... Shock to effective...

The Sepsis Timebomb
James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals

Relationship of SIRS, Sepsis and Infection
The ACCP/SCCM consensus Conference Committee, Chest 1992;101:1644-55.
INFECTION
SEPSIS
SIRS
BURNS
OTHER
TRAUMA
BACTEREMIA
FUNGEMIA
PARASITEMIA
VIREMIA
OTHER
PANCREATITIS
POST-PUMP SYNDROME

Sepsis and mortality
Vallés et al. Chest 2003;123:1615–1624

Time
Antiinflammatory
(endogenous)
CARS
SIRS RECOVERY
Organ Injury
van der Poll T, van Deventer SJH. Infect Dis Clin N Am
Infection
Antimicrobials
Sepsis and Septic Shock: An
Intensivist’s Immunologic View

Microbial load
Inflammatory response
Toxic burden
Cellular dysfunction/tissue injury
TIME
Sepsis and Septic Shock: An ID View
Shock Threshold

“An Injury Paradigm of Sepsis and Septic Shock” Prof A Kumar, University of Manitoba
Microbial load
Inflammatory response
Toxic burden
Cellular dysfunction/tissue injury
TIME
Antimicrobial
therapy
Shock
Threshold

“An Injury Paradigm of Sepsis and Septic Shock” Prof A Kumar, University of Manitoba
Microbial load
Inflammatory response
Toxic burden
Cellular dysfunction/tissue injury
TIME
earlier
antimicrobial
therapy
Shock
Threshold

“An Injury Paradigm of Sepsis and Septic Shock” Prof A Kumar, University of Manitoba
Microbial load
Inflammatory response
Toxic burden
Cellular dysfunction/tissue injury
TIME
Antimicrobial
therapy
+
Source control
Shock
Threshold

Kumar et al. CCM. 2006:34:1589-96.
Cumulative Initiation of Effective Antimicrobial Therapy and Survival in Septic Shock
time from hypotension onset (hrs)
fraction o
f to
tal patients
0.0
0.2
0.4
0.6
0.8
1.0 survival fraction
cumulative antibiotic initiation

Kumar et al, CCM. 2006:34:1589-96.
Mortality Risk with Increasing Delays in Initiation of Effective Antimicrobial Therapy
Time (hrs)
Od
ds R
atio
of D
ea
th
(95
% C
on
fid
en
ce
In
terv
al)
1
10
100

Comparison with other time dependent interventions
Not recognized early Easy diagnosis
Insidious onset Clear onset
Often develops on wards Presents to A&E
NNT
Severe sepsis 6-8 Septic shock
NNT
MI 30 CVA 30-40 Trauma 30

Door to balloon time and mortality in AMI
Adapted from Cannon et al. JAMA 2000; 283: 2941-7.

Door to balloon time and mortality in AMI
0-2h >2-3h >3-4h >4-6h >6-12h >12h
"Preventable deaths" 0 282 1350 1555 1384 204
0
200
400
600
800
1000
1200
1400
1600
"P
reven
tab
le" d
eath
s p
er
year
By getting door-to-balloon times of <2h for ALL STEMI patients,
we would save 4775 lives per year.
Adapted from Cannon et al. JAMA 2000; 283: 2941-7.

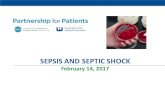
Shock to effective antibiotic time and mortality in septic shock
Adapted from Kumar et al. Crit Care Med 2006; 34: 1589-96.
0-2h >2-3h >3-4h >4-6h >6-12h >12h
%Mortality 26.7 36.1 36.6 46.8 62.3 83.1
% of patients 26.8 9.0 7.8 12.8 18.8 24.9
0
10
20
30
40
50
60
70
80
90 P
erc
en
tag
e o
f p
ati
en
ts

0-2h >2-3h >3-4h >4-6h >6-12h >12h
"Preventable" Deaths 0 1093 1000 3318 8710 18239
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
"P
reven
tab
le" d
ea
ths p
er
year
Shock to effective antibiotic time and mortality in septic shock
Adapted from Kumar et al. Crit Care Med 2006; 34: 1589-96.
By getting shock-to-antibiotic times of <2h for ALL septic shock patients,
we would save 32,360 lives per year.

83 72
50 35 26
18
Ab’s given

Effect of Failure to Implement Source Control if Required
0
20
40
60
80
100
Source Control
Implemented
Source Control Not
Implemented
% total patients
% survival

Cumulative Source Control Implementation and
Survival in Septic Shock
time from hypotension onset (hrs)
fraction o
f to
tal patients
0.0
0.2
0.4
0.6
0.8
1.0 survival fraction cumulative source control implementation

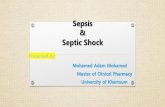
Source Control/Antimicrobial Interaction and Survival in Septic Shock
Antimicrobial Initiation Post-Shock
< 3 h 3-6 h
Source
Control
Initiation
Post-Shock
< 6 h
> 24 h
92%
(n=75)
70.3%
(n=37)
80.0%
(n=60)
46.0%
(n=50)
44.4%
(n=63)
13.0%
(n=100)
19.0%
(n=94)
36.0%
(n=25)
69.0%
(n=29)
> 6 h
6-24 h

83
83
78
78
72
72
60
Ab’s given Source control
22 30
46%

0
1
2
3
4
5
6
7
8
9
A B C D E F
A: SHEWS 2 to SpR review
B: SpR review to Antibiotics
C: CT booking to scan
D: CTscan to report
E: Scan to theatre booking
F: Booking to arrival
Audit of Event timing from SHEWS 2 to theatre for
the deteriorating colorectal patient at NGH from
October 2009 to March 2010
hours

0
5
10
15
20
25
Survivors Non-
survivors
Total time fromtrigger to theatre
Audit of Event timing from SHEWS 2 to theatre for
the deteriorating colorectal patient at NGH from
October 2009 to March 2010

Resulting in 25000 deaths
100 000 will develop significant complications
170 000 patients per year in the UK receive higher risk emergency general surgery
The Size Of The Problem

Number of ITU beds by country
0 5 10 15 20 25 30
Germany
Belgium
Croatia
USA
Canada
France
Netherlands
Spain
Australia
New Zealand
China
UK
Series1 Series2
█ ITU beds per 100000 population
█ ITU beds per 100 acute hospital beds



Key recommendations



Key recommendations

Key recommendations

Key recommendations


Key recommendations



The National Emergency
Laparotomy Audit
Dave Murray
National Clinical Lead
www.nela.org.uk [email protected]

Audit against standards

–Patient Pathway:
•Clear diagnostic and monitoring plans
•Adoption of escalation strategy with early involvement of senior staff
•Timing of diagnostic tests / timing of surgery • Adequate emergency theatre access with appropriate prioritisation
• Post-operative location
• Risk of death estimated and documented:
• prior to surgery to ensure adjustments made in urgency of care and seniority of staff involved
• at end of surgery to determine optimal location for post-operative care
•Key Recommendations: Delivery of Care

Key Recommendations: Individualised care •High risk patients
–≥10% 30d mortality
–Two consultants in theatre (surgeon and anaesthetist)
–Post-op Critical Care Unit
–‘Elderly’ patients
– Specialist input pre- and post-op
– Nutrition

The role of Outcome Measures in
improving quality of care
• 30-day mortality
• Risk adjusted via P-POSSUM
• Unplanned
‒ return to theatre
‒ escalation of care
‒ 30-day readmission

The role of Process Measures in
improving quality of care
• Admission to first dose of antibiotics
• Time from decision to theatre
• Pre-op CT scan
• Objective assessment of risk of death
• High risk patients directly admitted to critical care post-op
• Key Standards of Care relate to patient’s predicted risk of death

Conclusions
With the onset of shock – the mortality clock starts ticking!
Timely delivery of appropriate antibiotics is everybody’s responsibility – deal with it if it hasn’t already happened
Source control – the mortality clock does not wait for a convenient theatre slot