"The role of health literacy in perceived information provision and satisfaction among women with...

of 8
-
Upload
mariette-verkissen -
Category
Documents
-
view
18 -
download
0
description
Verkissen MN, Ezendam NPM, Fransen MP, Essink-Bot ML, Aarts MJ, Nicolaije KAH, Vos MC, Husson O. The role of health literacy in perceived information provision and satisfaction among women with ovarian tumors: A study from the population-based PROFILES registry. Patient Education and Counseling, 2014; in press.
Transcript of "The role of health literacy in perceived information provision and satisfaction among women with...
-
inenF
, M
Patient Education and Counseling xxx (2014) xxxxxx
G Model
PEC-4748; No. of Pages 8
Contents lists available at ScienceDirect
Patient Education
jo ur n al h o mep ag e: w ww .e lseMarie-Louise Essink-Bot c, Mieke J. Aarts b, Kim A.H. Nicolaije a,b,M. Caroline Vos d, Olga Husson a,b
aCoRPS Center of Research on Psychology in Somatic Diseases, Department of Medical and Clinical Psychology, Tilburg University, The Netherlandsb Eindhoven Cancer Registry, Comprehensive Cancer Center South (CCCS), Eindhoven Cancer Registry, The NetherlandscDepartment of Public Health, Academic Medical Center, University of Amsterdam, The NetherlandsdDepartment of Obstetrics and Gynecology, St. Elisabeth Hospital, Tilburg, The Netherlands
1. Introduction
The provision of appropriate information is one of the mostimportant aspects of the support for cancer survivors. Appropriateinformation provision, for example about the diagnosis, treatment,long-term effects, and care services, can result in informed decisionmaking, improved treatment adherence, lower levels of distress,and higher satisfaction with care and information received [16].Nevertheless, adequate information provision remains a challenge
in the eld of cancer care. It has shown to be a common unmet needamong cancer survivors in all phases of their disease [7]. Effectiveinformation provision requires an individualized approach that istailored to the patients needs, competences, limitations, andpossible barriers to the use of health information [8]. Tailoredinformation may lead to improved outcomes, such as betteradjustment to treatment [9]. In general, patients want to beinformed about their disease and its implications, regardless ofwhether this information is positive or negative [10,11]. However,specic information needs may depend on many individualizedfactors, including education and health literacy [12,13].
Health literacy (HL) entails peoples knowledge and compe-tences to access, understand, appraise, and apply health informa-tion [14]. After a cancer diagnosis, patients are often presented
A R T I C L E I N F O
Article history:
Received 12 September 2013
Received in revised form 18 February 2014
Accepted 8 March 2014
Keywords:
Ovarian tumors
Borderline ovarian tumors
Cancer survivors
Health literacy
Information provision
Information satisfaction
A B S T R A C T
Objective: To assess the association of subjective health literacy (HL) and education with perceived
information provision and satisfaction.
Methods: Women (N = 548) diagnosed with an ovarian or borderline ovarian tumor between 2000 and
2010, registered in the Eindhoven Cancer Registry, received a questionnaire including subjective HL,
educational level, perceived information provision, and satisfaction with the information received.
Multiple linear and logistic regression analyses were performed, controlled for potential confounders.
Results: Fifty percent of the women responded (N = 275). Thirteen percent had low and 41% had medium
subjective HL. Women with low HL reported less perceived information provision about medical tests,
and were less satised with the information received compared to women with high HL. Low educated
women reported that they received more information about their disease compared to highly educated
women.
Conclusion: Low subjective HL among women with ovarian tumors is associated with less perceived
information provision about medical tests and lower information satisfaction, whereas low education is
associated with more perceived information provision about the disease.
Practice implications: HL should not be overlooked as a contributing factor to patients perceived
information provision and satisfaction. Health care providers may need training about recognizing low
HL.
2014 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author at: Comprehensive Cancer Center The Netherlands, 5600
AE Eindhoven, The Netherlands. Tel.: +31 40 2971616; fax: +31 40 2971610.
E-mail address: [email protected] (Nicole P.M. Ezendam).
http://dx.doi.org/10.1016/j.pec.2014.03.008
0738-3991/ 2014 Elsevier Ireland Ltd. All rights reserved.Health Literacy
The role of health literacy in perceivedprovision and satisfaction among womA study from the population-based PRO
Mariette N. Verkissen a,b, Nicole P.M. Ezendama,b,*Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008formation with ovarian tumors:ILES registry
irjam P. Fransen c,
and Counseling
vier . co m / loc ate /p ated u co ualth literacy in perceived information provision and satisfactionn-based PROFILES registry. Patient Educ Couns (2014), http://
-
with complex medical information regarding their disease andtreatment [15,16]. Patients with low HL are at high risk of not beingable to process the information they are provided. This puts themat risk for various negative outcomes, such as difculty under-standing the diagnosis and treatment recommendations, pooreradherence to medical advice, medication errors resulting frominability to read labels, and increased hospitalizations [1719]. HLcan be assessed using objective and subjective measures. ObjectiveHL measures assess the individuals actual skills (e.g. reading andcalculating), whereas subjective HL measures evaluate theindividuals perceived skills (e.g. asking if he or she has difcultyunderstanding health information). Education is often thought ofas a marker for HL. However, although HL and education arerelated to each other [20], they need to be understood as distinctconcepts [21,22].
Despite the increased recognition of the importance of bothinformation provision and HL in cancer care, research on the role ofHL in information provision to cancer patients is limited. Previousstudies have examined the relation between breast cancerpatients HL and information-processing styles and preferences[23], breast cancer patients HL levels compared to the level ofwritten patient educational materials provided to them [24], and
ask few questions during consults [28,29], we hypothesized thatlower HL would be associated with less perceived informationprovision among women with ovarian tumors. In the limited timethat physicians have with their patients, they may not be able totailor the information according to their needs. We thereforehypothesized that lower HL would be associated with lesssatisfaction with the information received. Finally, based onprevious research indicating that patients with lower educationallevels generally feel less condent and are more likely to be passivein interactions with physicians [30], we hypothesized that lowereducation would also be associated with less perceived informa-tion provision and less satisfaction with the information received.
2. Methods
2.1. Setting and participants
This study is part of a population-based survey among womenwith ovarian cancer and BOT registered within the EindhovenCancer Registry (ECR). The ECR collects data of all individualsnewly diagnosed with cancer in the southern part of theNetherlands [31]. All women diagnosed with ovarian cancer or
h r
1st
11
o
n
n
da
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx2
G Model
PEC-4748; No. of Pages 8the relation between cancer patients HL and self-reportedinformation needs [22,25]. To our knowledge, however, no studieshave focused on the relation of cancer survivors HL with perceivedinformation provision and satisfaction with the informationreceived.
The present paper describes an explanatory study focusing onthe additional effect of HL over education on information provisionin a population-based sample of Dutch women with ovarian cancerand borderline (low malignant potential) ovarian tumors (BOT).Cancer of the ovary is one of the most common gynecologicmalignancies, whereas BOT are relatively uncommon. In theNetherlands, about 1300 cases of ovarian cancer and 150200cases of BOT are diagnosed annually [26,27].
The main purpose of this study was to investigate theassociation between HL and perceived level of informationprovision and information satisfaction, controlling for educationallevel. In order to distinguish between the potentially differenteffects of HL and education, we also evaluated the associationbetween educational level and perceived level of informationprovision and satisfaction. Given that patients with inadequate HLtend to be passive during physicianpatient communication and
1442 women were dia gnosed and registered witovarian ca ncer (114 7) or bord erli ne ovarian tumo(BOT) (2 95) between Ja nuary 1
st 2000 and July
2010 in 6 hospitals in the Eindhoven Cancer Registry region
719 patients were still alive on September 15th
20(454 ov arian ca ncer; 265 BOT)
Their gy necologists receiv ed an invitation letter tpermit st udy par ticipation
Addresses of 351 ovarian cancer and 202 BOTpatients were ch ecked for correctn ess
A questio nna ire was sent to the remaining ovaria
cancer (348) and BOT (2 00) patients
Patients included in the st udy: 191 (55%) ovaria
cancer and 84 (42%) BOT
Fig. 1. Flowchart of the Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008BOT between January 1, 2000 and July 1, 2010 as registered withinthe ECR were eligible for participation (N = 1442; Fig. 1). Deceasedpatients were excluded by linking the ECR with the Central Bureaufor Genealogy. Ethical approval for the study was obtained fromthe Medical Ethics Committee of St. Elisabeth Hospital, Tilburg, theNetherlands (no. 2011.129).
2.2. Data collection
Data collection took place in 2012. Along with a paperquestionnaire, patients received a letter from their specialistexplaining the survey and an informed consent form. Non-respondents were sent a reminder letter and questionnaire within2 months. Patients were asked to send the informed consent formand questionnaire back to the researchers in a pre-stampedenvelope.
The PROFILES (Patient Reported Outcomes Following Initialtreatment and Long term Evaluation of Survivorship) registry wasused to organize the data collection. PROFILES is an infrastructurefor the study of the physical and psychosocial impact of cancer andits treatment from a dynamic, growing population-based cohort of
723 patients deceased (6 93 ovarian
cancer; 30 BOT )
1 hospital declin ed (N=12 7) (74 ovarian ca ncer; 53 BOT)
Excluded: 29 ovarian ca ncer; 10 BOT (d eceased, hospitalized,
nursing home)
Addresses unkn own: 3 ov arian cancer; 2 BOT
Non-responders: 157 (45 %) ovarian
cancer; 116 (48%) BO T
ta collection process.alth literacy in perceived information provision and satisfactionn-based PROFILES registry. Patient Educ Couns (2014), http://
-
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx 3
G Model
PEC-4748; No. of Pages 8both short and long-term cancer survivors [32]. PROFILES containsa large web-based component and is linked directly to clinical datafrom the ECR. Data from the PROFILES registry are available fornon-commercial scientic research, subject to study question,privacy and condentiality restrictions, and registration (http://www.prolesregistry.nl/).
2.3. Measures
2.3.1. Clinical and socio-demographic characteristics
Clinical and patient information was obtained from the ECR (i.e.,date of birth, date of diagnosis, tumor grade, and primarytreatment). Socio-economic status (SES) was determined at theneighborhood level using postal codes, combining mean house-hold income and mean value of housing, as provided by StatisticsNetherlands [33]. The questionnaire contained questions oneducational level, employment status, and marital status.
2.3.2. Subjective health literacy
A Dutch adaptation of Chews three-item Set of Brief ScreeningQuestions (SBSQ) was used to evaluate subjective HL [34]. TheAmerican version of the SBSQ has been previously validatedagainst widely used measures of health literacy (REALM and S-TOFHLA) as the reference standard [35,36] across a variety ofsettings [3739]. Previous research has suggested that a scalecombining the three items is no more effective in identifyingindividuals with inadequate HL than one single item [3537,40]. Ithas also been demonstrated that the item How condent are youlling out medical forms by yourself? (very, quite, some-what, a little and not at all) is more effective in predictinginadequate HL than the other two items [37,40]. Therefore, thissingle item was used in the analyses.
2.3.3. Perceived information provision and satisfaction
To evaluate the perceived level of and satisfaction withinformation provision, the Dutch version of the EuropeanOrganization for Research and Treatment of Cancer (EORTC)QLQ-INFO25 questionnaire, an instrument to assess the infor-mation given to cancer patients, was used [41]. Patientsresponses to the EORTC QLQ-INFO25 were collated into foursubscales: (1) perceived receipt of information about the disease(four items regarding diagnosis, spread of disease, cause(s) ofdisease and whether the disease is under control); (2) medicaltests performed in relation to the disease (three items regardingpurpose, procedures and results of tests); (3) treatment (sixitems regarding medical treatment, benets, side-effects, effectson disease symptoms, social life and sexual activity); and (4)other care services (four items regarding additional help,rehabilitations options, managing illness at home, psychologicalsupport). The question format was as follows: During yourcurrent disease or treatment, how much information did youreceive on. . .?. Additionally, the questionnaire contained asingle item regarding patients satisfaction with informationreceived (Were you satised with the amount of informationyou received?).
The response options were not at all, a little, quite a bit,and very much. After linear transformation, all scales and itemsrange in scores from 0 to 100, with higher scores indicating betterperceived information provision or higher satisfaction [3].
The EORTC QLQ-INFO25 has a good scale structure and has beeninternationally validated [41,42]. Internal consistency for all scalesand test-retest reliability have been reported to be good (a > 0.70and intraclass correlations > 0.70, respectively) [41]. Our datarevealed Cronbachs alphas of 0.80 (disease), 0.90 (medical tests),0.88 (treatment), and 0.81 (other care services) for the foursubscales.Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.0082.4. Statistical analyses
All statistical analyses were conducted using IBM SPSS Statisticsversion 19 (SPSS Inc., Chicago, IL, USA). p-Values of
-
3.2. Subjective health literacy and educational level
Thirteen percent of the women had low subjective HL; 41% hadmedium subjectiveHL.Fifteenpercenthada loweducational level;64%had a medium educational level (Table 2). HL and educational levelwere signicantly related to each other (p < 0.001). Of women withhigh HL (N = 119), 33% had a high educational level as well, and of allwomen with low HL (N = 33), 49% had a low educational level as well.
3.3. Educational level, subjective health literacy, and perceived
information provision
On average, low educated women reported a lower perceivedlevel of information provision about medical tests and treatmentcompared to highly educated women, and women with lowsubjective HL reported a lower perceived level of informationprovision about disease, medical tests, and treatment compared towomen with high HL (Table 2).
Table 1Socio-demographic and clinical characteristics of questionnaire respondents and
non-respondents.
Respondents Non-respondents p-Value
N = 275 N = 282
N (%) N (%)
Age at time of survey (mean, SD) 62.8 (12.4) 60.9 (14.3) 0.10
Years since diagnosis (mean, SD) 6.3 (3.1) 6.4 (3.1) 0.55
Tumor type
Ovarian tumor 191 (70%) 163 (58%)
-
provision related to medical tests. We found similar trendsregarding perceived information provision about disease andtreatment, but these trends were not statistically signicant.Women with low HL were also less likely to be satised with theinformation received compared to women with high HL. Thesendings are in line with our hypotheses, and with previousresearch showing that patients with low HL were more likely toreport worse patientphysician communication in the domains ofinformation provision about disease and care processes (e.g.medical tests) [48]. Besides problems with reading, writing andnumeracy, patients with low HL may have difculty processingoral communication, assimilating new information, comprehend-ing health vocabulary and asking questions during visits with theirhealth care professional [48,49]. If health care providers lack thetime or skills necessary to help patients with low HL fullyunderstand their condition, the information provided to patientswith low HL may not correspond with their information needs.This may lead to patient dissatisfaction. Moreover, patients tend toforget a signicant amount of the information they received whenthis information is complex and emotionally charged [50], whichmay be particularly true for patients with low HL because of their
0
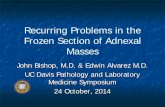
5
10
15
20
25
Informationdisease
Informationmedical tests
Information treatme nt
Information othercare services
Perc
enta
ge
Health literacy (step 3)
Educati onal lev el (st ep 2)
Confo unders (st ep 1)
*
*
Fig. 2. Explained variance (R2 (%)) of the EORTC QLQ-INFO25 perceived informationprovision subscales by the confounders tumor type, years since diagnosis, age at
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx 5
G Model
PEC-4748; No. of Pages 8Hierarchical multiple logistic regressions revealed no signi-cant association between educational level and informationsatisfaction. Compared to patients with high subjective HL, womenwith low HL were signicantly less likely to be satised with theinformation they received (OR = 0.2 (0.1; 0.6); Table 4).
4. Discussion and conclusion
4.1. Discussion
In the present study, lower subjective HL was associated withless perceived information provision about medical tests and lowerinformation satisfaction. Contrary to our hypothesis, low educa-tional level was associated with more perceived informationprovision about the disease compared to high educational level. HLand educational level explained a relatively small amount of thevariability in perceived information provision and informationsatisfaction.
time of survey, employment status and marital status (step 1); plus educational
level (step 2); plus subjective health literacy (step 3). *p < 0.05.Compared to women with high subjective HL, women withmedium and low HL scored lower on perceived information
Table 3Hierarchical multiple linear regression analyses evaluating the associations of education
High
educationaMedium education Low education Hi
HL
Information disease
Model 2 (B, 95% CI) Ref 2.3 (10.0; 5.5) 12.4 (1.1; 23.6)*Model 3 (B, 95% CI) Ref 1.5 (9.3; 6.2) 15.5 (3.8; 27.2)* Re
Information medical tests
Model 2 (B, 95% CI) Ref 5.6 (14.5; 3.4) 0.9 (13.9; 12.1) Model 3 (B, 95% CI) Ref 4.3 (13.1; 4.6) 3.4 (10.0; 16.7) Re
Information treatment
Model 2 (B, 95% CI) Ref 3.6 (12.2; 4.9) 3.7 (8.6; 16.0) Model 3 (B, 95% CI) Ref 2.8 (11.3; 5.8) 7.0 (5.8; 19.7) Re
Information other care services
Model 2 (B, 95% CI) Ref 7.0 (1.1; 15.1) 8.8 (2.8; 20.5) Model 3 (B, 95% CI) Ref 7.0 (1.2; 15.1) 9.7 (2.5; 22.0) Re
Note: Model 1 (not reported) includes tumor type, years since diagnosis, age at time of sur
education level; Model 3 includes all of Model 2 as well as subjective health literacya Educational level: high = university or higher education; medium = secondary educb HL = subjective health literacy: high = being very condent lling out medical forms;
little or not at all condent lling out medical forms* p < 0.05.
Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008poor ability to recall information provided during medicalconsultations [51].
Contrary to our hypothesis that patients with a lowereducational level would indicate that they received less informa-tion, low educated women reported that they received moreinformation about their disease compared to highly educatedwomen. Previous studies found that having a lower level ofeducation was associated with less perceived information provi-sion about medical tests and treatment [6,45,47] and with atendency to ask fewer questions during visits with a health careprovider [52]. However, a low educational level does notnecessarily implicate low learning capacity. Older women inparticular might not have had the opportunity to proceed to highereducation. Differences between the effects of HL and education onperceived information provision found in this study may thereforebe partially explained by misclassication of women in the loweducation group.
Another explanation could be that low educated women hadlower information needs and were less critical than highlyeducated women. This may have caused them to feel that theyreceived a large amount of disease-related information, while theactual amount of information was more or less equal in bothgroups. Finally, it has been suggested that low educated patients
al level and subjective health literacy with perceived level of information provision.
ghb
Medium HL Low HL R2 (%) DR2 (%) Dp-value
10.3% 4.1%
-
io
d
on
)
)
e
cy
uc
s;
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx6
G Model
PEC-4748; No. of Pages 8generally tend to report more positive health care experiencescompared to highly educated patients, which may reect areporting bias rather than a real difference [53,54].
Subjective HL and educational level accounted for a remarkablysmall amount of the variability in the outcome variables. There areseveral factors other than subjective HL and education that mayhave had an impact on patients perceived level of informationprovision and satisfaction. We controlled for the potentialconfounders tumor type, years since diagnosis, age at time ofsurvey, employment status, and marital status. However, differ-ences in information needs may have affected the outcomes aswell. How information needs are related to HL and the outcomevariables, e.g. through mediation or as a confounding factor,remains uncertain. Another patient characteristic that might haveaffected the outcomes is coping style. Two main coping styles fordealing with cancer information have been described: monitoring(attending to) and blunting (avoiding). Patients with a monitoringstyle tend to do better when provided with more information, andpatients with a blunting style generally fare better when given lessinformation [55]. A recent study found that cancer patients with acombination of the personality traits negative affectivity and socialinhibition (the so-called Type D personality) reported that theyreceived less information about their disease, medical tests, andtreatment, and were less satised with the information receivedcompared to non-Type D patients [56]. This indicates thatpersonality could play a signicant role in cancer patientsperceived level of information provision and satisfaction. More-over, differences in actual information receipt could have directlyaffected patients perceived level of information provision andsatisfaction.
Another explanation for the small amount of variabilityexplained in the regression analyses may lie in the measurementof HL. HL was measured by asking patients perceived condence(self-efcacy) and not their actual skills in lling out medical formsby themselves [57]. As patients with low literacy skills tend tooverestimate their own abilities [58], this could have affected theprevalence rate of low HL. Future research on the relation betweenHL and information provision may be improved by addressing
Table 4Hierarchical multiple logistic regression analyses evaluating the associations of educat
unsatised (not or only a little satised with the information received; reference) an
High
educationaMedium education Low educati
Model 2 (odds ratio, 95% CI) Ref 0.5 (0.2; 1.1) 1.1 (0.4; 3.3Model 3 (odds ratio, 95% CI) Ref 0.6 (0.3; 1.2) 2.0 (0.6; 6.8
Note: Model 1 includes tumor type, years since diagnosis, age at time of survey, employm
educational level; Model 3 includes all of Model 2 as well as subjective health literaa Educational level: high = university or higher education; medium = secondary edb HL = subjective health literacy: high = being very condent lling out medical form
little or not at all condent lling out medical forms.* p < 0.01.objectively measured HL, for example by using validated versionsof the REALM (Rapid Estimate of Adult Literacy in Medicine) [59],the S-TOFHLA (Short Test of Functional Health Literacy in Adults)[60] or the NVS (Newest Vital Sign) [61]. Of these instruments, theREALM and the NVS have already been adapted and applied in theNetherlands [34]. However, it is unclear whether these generic HLmeasures cover all important skills needed for cancer survivors tond their way in cancer care. Future studies should investigatewhether a cancer-specic HL instrument is needed to measure thebroad scope of cancer-related HL.
The present study is one of the rst studies in the eld of cancercare examining the association between HL and informationprovision. However, some limitations should be considered wheninterpreting the results. One limitation concerns the relatively low
Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008response rate (50%), which increases the likelihood of selectionbias. It is also reasonable that the mean time since diagnosis of 6.3years has affected the recall of information received. We thereforecontrolled for years since diagnosis in our analyses. Furthermore,information satisfaction was measured by using only one itemwhich we dichotomized for the analyses. The test-retest reliabilityand the convergent and divergent validity of this question haveshown to be good [41], but have not been evaluated for thedichotomized item. Moreover, the question does not provideinformation as to why patients were (un)satised with theinformation they received.
The provision of information to BOT survivors may differsubstantially from the provision of information to ovarian cancersurvivors. Unlike invasive ovarian tumors, BOT rarely metastasize,are usually slow growing, and are not likely to lead to death.Furthermore, BOT generally are treated by surgery alone, becausethey are insensitive to chemotherapy. Because we expected tumortype (ovarian cancer versus BOT) to be related to informationprovision, we adjusted for tumor type in the regression analyses.For future research, it might be of interest to compare ovariancancer and BOT survivors in their information provision and itsrelationship with HL and education. This may help understand howinformation provision might differ between medical conditions.
4.2. Conclusion
Ovarian cancer and BOT survivors with low subjective HLreported that they received less information about medical testsperformed in relation to their disease, and were less likely to besatised with the information received compared to survivors withhigh subjective HL.
These associations were found after controlling for educationallevel, showing that HL is related to perceived informationprovision and satisfaction beyond the effect of education.
However, HL accounted only for a small amount of thevariability in information provision. A more objective cancer-specic measure of HL might be more appropriate to measurecancer-related HL and its association with cancer-specic infor-
nal level and subjective health literacy with information satisfaction, categorized as
satised (quite or very satised with the information received).
High HLb Medium HL Low HL 2LL D2LL Dp-value
291.7 5.1 0.08
Ref 0.9 (0.5; 1.7) 0.2 (0.1; 0.6)* 282.1 9.7
-
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx 7
G Model
PEC-4748; No. of Pages 8before they leave the consultation (the teach-back technique) toensure that patients understand what they have been told [63,64].For future research, it is important to evaluate the effectiveness ofsuch strategies in the information provision to cancer survivorswith low HL.
Role of funding source
The present study was supported with grant no. UVT 2010-4743 from the Dutch Cancer Society and an investment grant of theNetherlands Organization for Scientic Research (NWO #480-08-009), The Hague, the Netherlands. The funding source had noinvolvement in the study design, the collection, analysis, andinterpretation of data, the writing of the manuscript, and thedecision to submit the paper for publication.
Authors contributions
MV, NE, MF, MLE-B, MA, CV, and OH contributed to the conceptand design of the study. MF and MLE-B provided advice on HLmeasurement. NE, KN, and CV contributed to the acquisition of thedata. MV and NE analyzed the data and drafted the manuscript. Allauthors provided input into revisions of the manuscript and haveapproved the nal manuscript.
Conict of interest
None.
Acknowledgements
We would like to thank all patients and their doctors for theirparticipation in the study. In addition, we want tothank the followinghospitals for their cooperation: Amphia Hospital, Breda; CatharinaHospital, Eindhoven; St. Elisabeth Hospital, Tilburg; Jeroen BoschHospital, s Hertogenbosch; TweeSteden Hospital, Tilburg.
References
[1] Mallinger JB, Griggs JJ, Shields CG. Patient-centered care and breast cancersurvivors satisfaction with information. Patient Educ Couns 2005;57:3429.
[2] Mesters I, van den Borne B, De Boer M, Pruyn J. Measuring information needsamong cancer patients. Patient Educ Couns 2001;43:25362.
[3] Arraras JI, Kuljanic-Vlasic K, Bjordal K, Yun YH, Efcace F, Holzner B, et al.EORTC QLQ-INFO26. A questionnaire to assess information given to cancerpatients a preliminary analysis in eight countries. Psychooncology2007;16:24954.
[4] Meredith C, Symonds P, Webster L, Lamont D, Pyper E, Gillis CR, et al.Information needs of cancer patients in west Scotland: cross sectional surveyof patients views. Brit Med J 1996;313:7246.
[5] Husson O, Mols F, van de Poll-Franse LV. The relation between informationprovision and health-related quality of life, anxiety and depression amongcancer survivors: a systematic review. Ann Oncol 2011;22:76172.
[6] Nicolaije KA, Husson O, Ezendam NP, Vos MC, Kruitwagen RF, Lybeert ML, et al.Endometrial cancer survivors are unsatised with received information aboutdiagnosis, treatment and follow-up: a study from the population-based PRO-FILES registry. Patient Educ Couns 2012;88:42735.
[7] Harrison JD, Young JM, Price MA, Butow PN, Solomon MJ. What are the unmetsupportive care needs of people with cancer? A systematic review. SupportCare Cancer 2009;17:111728.
[8] Schulz PJ, Nakamoto K. Health literacy and patient empowerment in healthcommunication: the importance of separating conjoined twins. Patient EducCouns 2013;90:411.
[9] Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for informa-tion, decision-making and interpersonal behavior: evidence, models andinterventions. Patient Educ Couns 2006;61:31941.
[10] Jenkins V, Falloweld L, Saul J. Information needs of patients with cancer:results from a large study in UK cancer centres. Br J Cancer 2001;84:4851.
[11] Jefford M, Tattersall MHN. Informing and involving cancer patients in theirown care. Lancet Oncol 2002;3:62937.
[12] Mills ME, Sullivan K. The importance of information giving for patients newlydiagnosed with cancer: a review of the literature. J Clin Nurs 1999;8:63142.Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008[13] Abrahamson K, Durham M, Fox R. Managing the unmet psychological andinformation needs of patients with cancer. Patient Intell 2010;2:4552.
[14] Srensen K, van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al.Health literacy and public health: a systematic review and integration ofdenitions and models. BMC Public Health 2012;12:80.
[15] Garcia SF, Hahn EA, Jacobs EA. Addressing low literacy and health literacy inclinical oncology practice. J Support Oncol 2010;8:649.
[16] Foltz A, Sullivan J. Get real: clinical testing of patients reading abilities. CancerNurs 1998;21:1626.
[17] Baker DW, Parker RM, Williams MV, Pitkin K, Parikh NS, Coates WC, et al. Thehealth care experience of patients with low literacy. Arch Fam Med1996;5:32934.
[18] Berkman ND, Sheridan SL, Donahue KE, Halpem DJ, Crotty K. Low healthliteracy and health outcomes: an updated systematic review. Ann Intern Med2011;155:97107.
[19] Williams MV, Parker RM, Baker DW, Parikh NS, Pitkin K, Coates WC, et al.Inadequate functional health literacy among patients at two public hospitals. JAmer Med Assoc 1995;274:167782.
[20] Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR.The prevalence of limited health literacy. J Gen Intern Med 2005;20:17584.
[21] Shaw SJ, Huebner C, Armin J, Orzech K, Vivian J. The role of culture in healthliteracy and chronic disease screening and management. J Immigr MinorHealth 2009;11:4607.
[22] Matsuyama RK, Wilson-Genderson M, Kuhn L, Moghanaki D, Vachhani H,Paasche-Orlow M. Education level, not health literacy, associated with infor-mation needs for patients with cancer. Patient Educ Couns 2011;85:22936.
[23] Lillie SE, Brewer NT, ONeill SC, Morrill EF, Dees EC, Carey LA, et al. Retentionand use of breast cancer recurrence risk information from genomic tests: therole of health literacy. Cancer Epidemiol Biomarkers Prev 2007;16:24955.
[24] Cox N, Bowmer C, Ring A. Health literacy and the provision of information towomen with breast cancer. Clin Oncol 2011;23:2237.
[25] Douma KF, Koning CCE, Zandbelt LC, de Haes HC, Smets EM. Do patientsinformation needs decrease over the course of radiotherapy. Support CareCancer 2012;20:216776.
[26] Netherlands Cancer Registry. http://www.cijfersoverkanker.nl [accessed25.07.13].
[27] Borderline ovariumtumoren. Landelijke richtlijn met regionale toevoegingen,Versie: 1.5 [accessed 25.07.13].
[28] Arthur SA, Geiser HR, Arriola KR, Kripalani S. Health literacy and control in themedical encounter: a mixed-methods analysis. J Natl Med Assoc2009;101:67783.
[29] Katz MG, Jacobson TA, Veledar E, Kripalani S. Patient literacy and question-asking behavior during the medical encounter: a mixed-methods analysis. JGen Intern Med 2007;22:7826.
[30] Rademakers J, Delnoij D, Nijman J, de Boer D. Educational inequalities inpatient-centred care: patients preferences and experiences. BMC Health ServRes 2012;12.
[31] Janssen-Heijnen MLG, Louwman WJ, van de Poll-Franse LV, Coebergh JWW.Results of 50 years cancer registry in the South of the Netherlands: 19552004. Eindhoven: Eindhoven Cancer Registry; 2005 [in Dutch].
[32] Van de Poll-Franse LV, Horevoorts N, van Eenbergen M, Denollet J, Roukema JA,Aaronson NK, et al. The Patient Reported Outcomes Following Initial treatmentand Long term Evaluation of Survivorship registry: scope, rationale and designof an infrastructure for the study of physical and psychosocial outcomes incancer survivorship cohorts. Eur J Cancer 2011;47:218894.
[33] Van Duijn C, Keij I. Sociaal-economische status indicator op postcodeniveau.Maandstatistiek van de Bevolking 2002;50:325.
[34] Fransen MP, van Schaik TM, Twickler TB, Essink-Bot ML. Applicability ofinternationally available health literacy measures in the Netherlands. J HealthCommun 2011;16:13449.
[35] Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients withinadequate health literacy. Fam Med 2004;36:58894.
[36] Chew LD, Grifn JM, Partin MR, Noorbaloochi S, Grill JP, Snyder A, et al.Validation of screening questions for limited health literacy in a large VAoutpatient population. J Gen Intern Med 2008;23:5616.
[37] Wallace LS, Rogers ES, Roskos SE, Holiday DB, Weiss BD. Brief report: screeningitems to identify patients with limited health literacy skills. J Gen Intern Med2006;21:8747.
[38] Wallace LS, Cassada DC, Rogers ES, Freeman MB, Grandas OH, Stevens SL, et al.Can screening items identify surgery patients at risk of limited health literacy.J Surg Res 2007;140:20813.
[39] Sarkar U, Piette JD, Gonzales R, Lessler D, Chew LD, Reilly B, et al. Preferencesfor self-management support: ndings from a survey of diabetes patients insafety-net health systems. Patient Educ Couns 2008;70:10210.
[40] Powers BJ, Trinh JV, Bosworth HB. Can this patient read and understandwritten health information. J Amer Med Assoc 2010;304:7684.
[41] Arraras JI, Greimel E, Sezer O, Chie WC, Bergenmar M, Costantini A, et al. Aninternational validation study of the EORTC QLQ-INFO25 questionnaire: aninstrument to assess the information given to cancer patients. Eur J Cancer2010;46:272638.
[42] Singer S, Engelberg PM, Weissog G, Kuhnt R, Ernst J. Construct validity of theEORTC quality of life questionnaire information module. Qual Life Res2013;22:1239.
[43] Fayers PM, Bjordal K, Groenvold M, Curran D, Bottomley A. The EORTC QLQ-C30 Scoring Manual. 3rd ed. Brussels: European Organisation for Research andTreatment of Cancer; 2001.alth literacy in perceived information provision and satisfactionn-based PROFILES registry. Patient Educ Couns (2014), http://
-
[44] Babyak MA. What you see may not be what you get: a brief, nontechnicalintroduction to overtting in regression-type models. Psychosom Med2004;66:41121.
[45] Oerlemans S, Husson O, Mols F, Poortmans P, Roerdink H, Daniels LA, et al.Perceived information provision and satisfaction among lymphoma and mul-tiple myeloma survivorsresults from a Dutch population-based study. AnnHematol 2012;91:158795.
[46] Husson O, Thong MS, Mols F, Oerlemans S, Kaptein AA, van de Poll-Franse LV.Illness perceptions in cancer survivors: what is the role of informationprovision. Psychooncology 2013;22:4908.
[47] Husson O, Holterhues C, Mols F, Nijsten T, van de Poll-Franse LV. Melanomasurvivors are dissatised with perceived information about their diagnosis,treatment and follow-up care. Br J Dermatol 2010;163:87981.
[48] Schillinger D, Bindman A, Wang F, Stewart A, Piette J. Functional health literacyand the quality of physicianpatient communication among diabetes patients.Patient Educ Couns 2004;52:31523.
[49] Williams MV, Davis T, Parker RM, Weiss BD. The role of health literacy inpatientphysician communication. Fam Med 2002;34:3839.
[50] Siminoff LA, Ravdin P, Colabianchi N, Sturm CM. Doctorpatient communica-tion patterns in breast cancer adjuvant therapy discussions. Health Expect2000;3:2636.
[51] McCarthy DM, Waite KR, Curtis LM, Engel KG, Baker DW, Wolf MS. What didthe doctor say? Health literacy and recall of medical instructions. Med Care2012;50:27782.
[52] Derman U, Serbest P. Cancer patients awareness of disease and satisfactionwith services: the inuence of their general education level. J Cancer Educ1993;8:1414.
[53] Damman OC, Stubbe JH, Hendriks M, Arah OA, Spreeuwenberg P, Delnoij DM,et al. Using multilevel modeling to assess case-mix adjusters in consumerexperience surveys in health care. Med Care 2009;47:496503.
[54] OMalley AJ, Zaslavsky AM, Elliott MN, Zaborski L, Cleary PD. Case-mixadjustment of the CAHPS1 Hospital Survey. Health Serv Res2005;40:216281.
[55] Miller SM. Monitoring versus blunting styles of coping with cancer inuencethe information patients want and need about their disease: implications forcancer screening and management. Cancer 1995;76:16777.
[56] Husson O, Denollet J, Oerlemans S, Mols F. Satisfaction with informationprovision in cancer patients and the moderating effect of Type D personality.Psychooncology 2013;22:212432.
[57] Ishikawa H, Yano E. Patient health literacy and participation in the health-careprocess. Health Expect 2008;11:11322.
[58] Cornett S. Assessing and addressing health literacy. Online J Issues Nurs2009;14.
[59] Davis TC, Crouch MA, Long SW, Jackson RH, Bates P, George RB, et al. Rapidassessment of literacy levels of adult primary care patients. Fam Med1991;23:4335.
[60] Baker DW, Williams MV, Parker RM, Gazmararian JA, Nurss J. Development of abrief test to measure functional health literacy. Patient Educ Couns1999;38:3342.
[61] Weiss BD, Mays MZ, Martz W, Castro KM, DeWalt DA, Pignone MP, et al. Quickassessment of literacy in primary care: the Newest Vital Sign. Ann Fam Med2005;3:51422.
[62] Kelly PA, Haidet P. Physician overestimation of patient literacy: apotential source of health care disparities. Patient Educ Couns2007;66:11922.
[63] Schillinger D, Piette J, Grumbach K, Wang F, Wilson C, Daher C, et al. Closing theloop: physician communication with diabetic patients who have low healthliteracy. Arch Intern Med 2003;163:8390.
[64] Davis TC, Williams MV, Marin E, Parker RM, Glass J. Health literacy and cancercommunication. CA Cancer J Clin 2002;52:13449.
M.N. Verkissen et al. / Patient Education and Counseling xxx (2014) xxxxxx8
G Model
PEC-4748; No. of Pages 8Please cite this article in press as: Verkissen MN, et al. The role of heamong women with ovarian tumors: A study from the populatiodx.doi.org/10.1016/j.pec.2014.03.008alth literacy in perceived information provision and satisfactionn-based PROFILES registry. Patient Educ Couns (2014), http://
The role of health literacy in perceived information provision and satisfaction among women with ovarian tumors: A study from the population-based PROFILES registryIntroductionMethodsSetting and participantsData collectionMeasuresClinical and socio-demographic characteristicsSubjective health literacyPerceived information provision and satisfaction
Statistical analyses
ResultsPatient characteristicsSubjective health literacy and educational levelEducational level, subjective health literacy, and perceived information provisionEducational level, subjective health literacy, and information satisfaction
Discussion and conclusionDiscussionConclusionPractice implications
Role of funding sourceAuthors contributionsConflict of interestAcknowledgementsReferences