The role of DCB in SFA subintimal tracking lesion
29
The role of DCB in SFA subintimal tracking lesion Wei-chun Chang M.D. Wen-Lieng Lee, MD, PhD Cardiovascular Center, Taichung Veterans General Hospital, Taiwan R.O.C
Transcript of The role of DCB in SFA subintimal tracking lesion
The role of DCB in SFA subintimal tracking lesion
Wei-chun Chang M.D. Wen-Lieng Lee, MD, PhD
Cardiovascular Center, Taichung Veterans General Hospital, Taiwan R.O.C

Disclosure
Speaker name:
.................................................................................
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest

Clinical Evidence
• From literature review: IMPACT SFA 2-year outcome and LEVANT2 , DCB in FPD diastase is promising but all lesions are intra-luminal approach.
• The data about DCB effect in SFA subintimal tracking lesion is very limited.
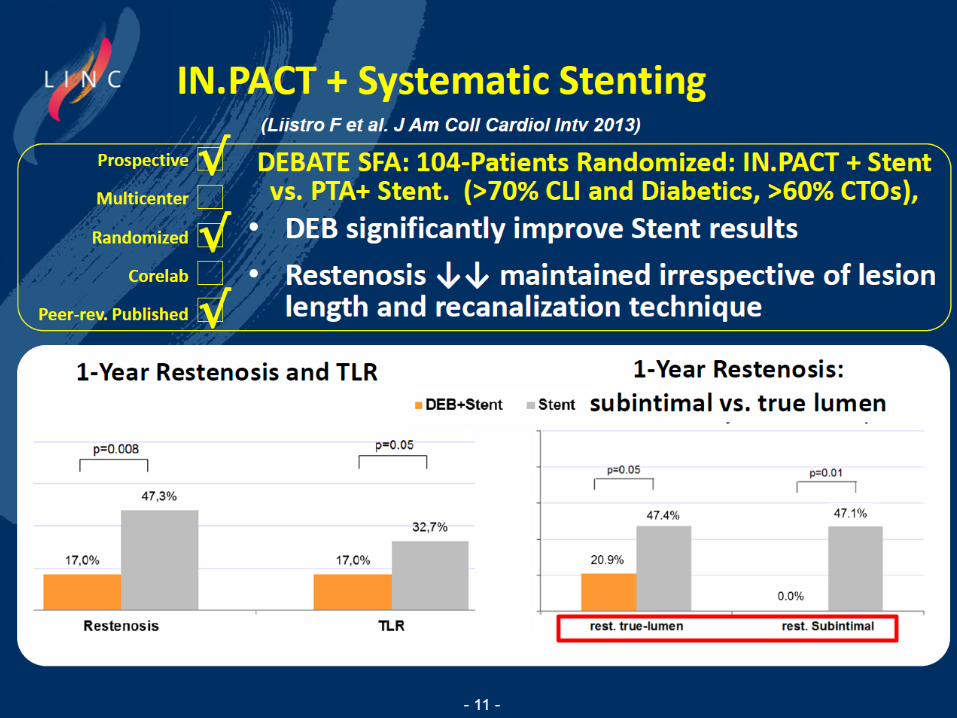
DCB Sub-intimal Potential Performance
DCBATE-SFA Randomized Trial

Drug-Eluting Balloon in Peripheral Intervention for Below the Knee Angioplasty Evaluation
(DEBATE-BTK)
Francesco Liistro et al. Circulation. 2013;128:615-621

Lesson from DEBATE-BTK trial
There should be a one-to-one ratio between the DEB and the vessel. It is not worth it to oversize the balloon with respect to the vessel diameter, because on follow-up, we could see in 3% of the cases that there is an ectatic effect from the drug delivery in the vessel.

DCB in A Case of Femoropopliteal PAD with Subintimal Tracking EVT

Case Sharing • 21 y/o man with intermittent claudication of right
leg for months.
• PAD, Right leg post surgical thrombolectomy on April 14th, 2015, and popliteal pseudoaneurysm untreated.
• successful PTA to ATA (POBA, Export aspiration thrombectomy, local thrombolytic therapy) and PTA (POBA, Export aspiration thrombectomy, local thrombolytic therapy) on April 25th, 2015.
• Protein C/Protein S/Antithrombin-III deficiency with wafarin (INR: 1.6) and cilostazol

Case Sharing • Recurrent PAD, Right leg post successful POBA +
Impact Admiral DCB x2 of R't SFA ostial to middle long CTO with bi-directional technique; successful POBA+ Impact Admiral DCB of R't SFA-D to TP trunk CTO; successful POBA of ATA-P and Peroneal-P on Nov. 27th, 2015.
• Terminal ileum ulcer with active bleeding after EVT
• Pseudo-aneurysm of left CFA (puncture site) s/p surgical repair in Jan.18th, 2016.
• Recurrent pseudo-aneurysm of SFA –M , right after surgical repair of pseudo-aneurysm of left CFA ……

First PTA for Thromboembolism of ATA/PTA

PTA+ CDT with UK
After PTA
Before PTA
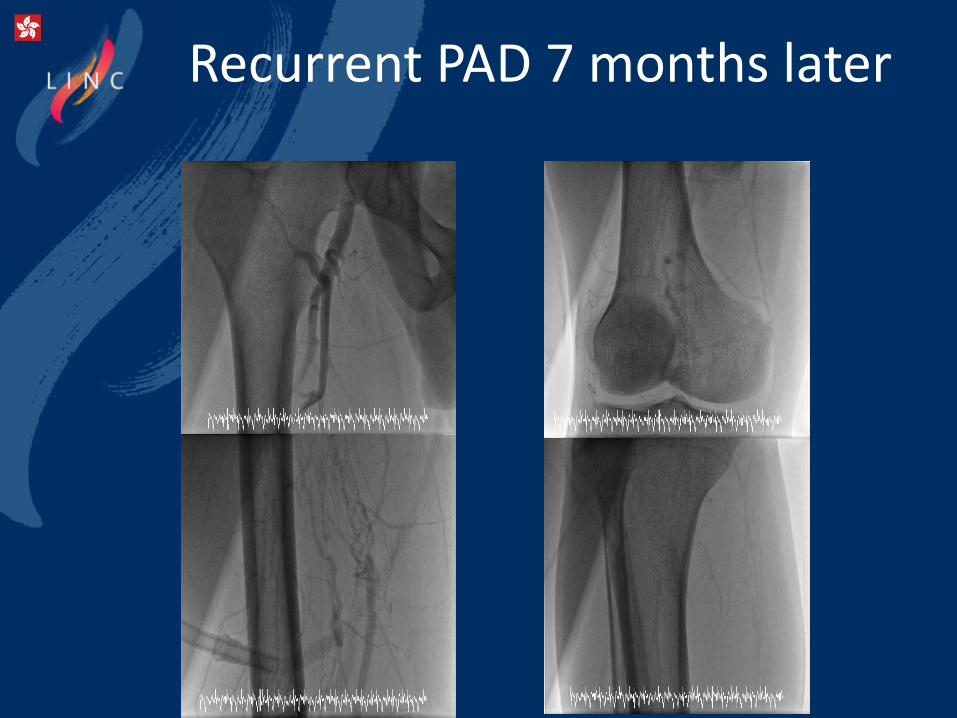
Recurrent PAD 7 months later

Cross-over EVT
Backend of control V-18 after
failed crossing with Victory 30gm Subintimal tracking with control V-18
Suppored with Pacific 4.0mmx15cm

Retrograde Puncture of D-SFA

Angio of SFA after POBA
a
BC-assisted hemostasis

Pop to TP trunk CTO
Subintimal tracking with V-18

EVT in BTK
Victory 30gm in Peroneal artery RegaliaXS in ATA with Crusade support
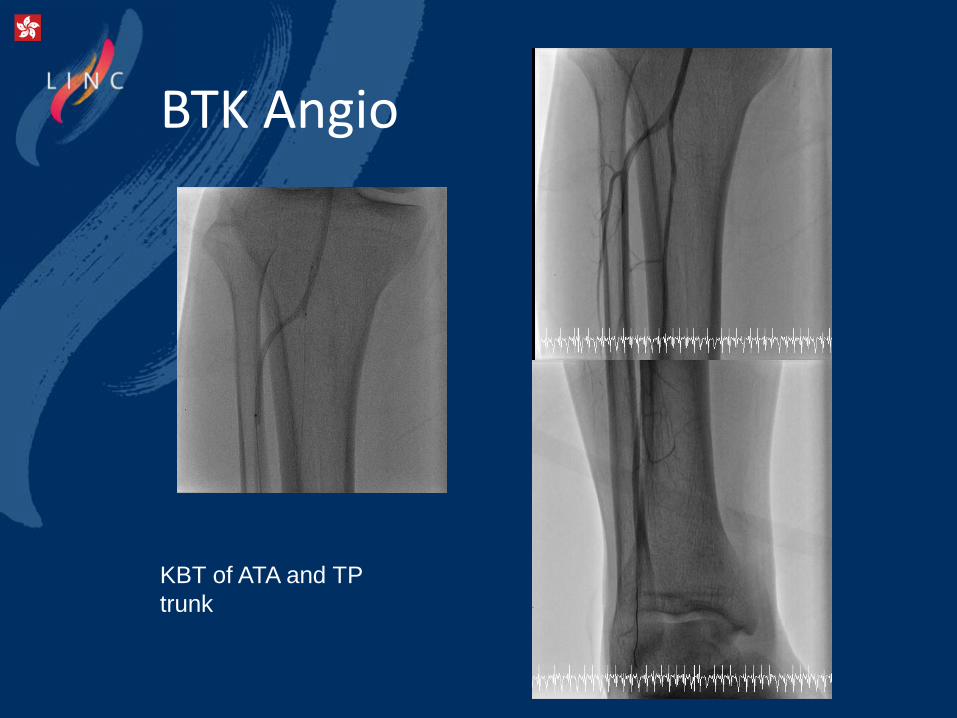
BTK Angio
KBT of ATA and TP
trunk

Final Angio
Three Impact Admiral DCB: SFA-ostium to Popliteal artery
But…. Massive GI bleeding with Terminal ileal Uncer (Hb:12>6) A Pseudo-aneurysm of left CFA
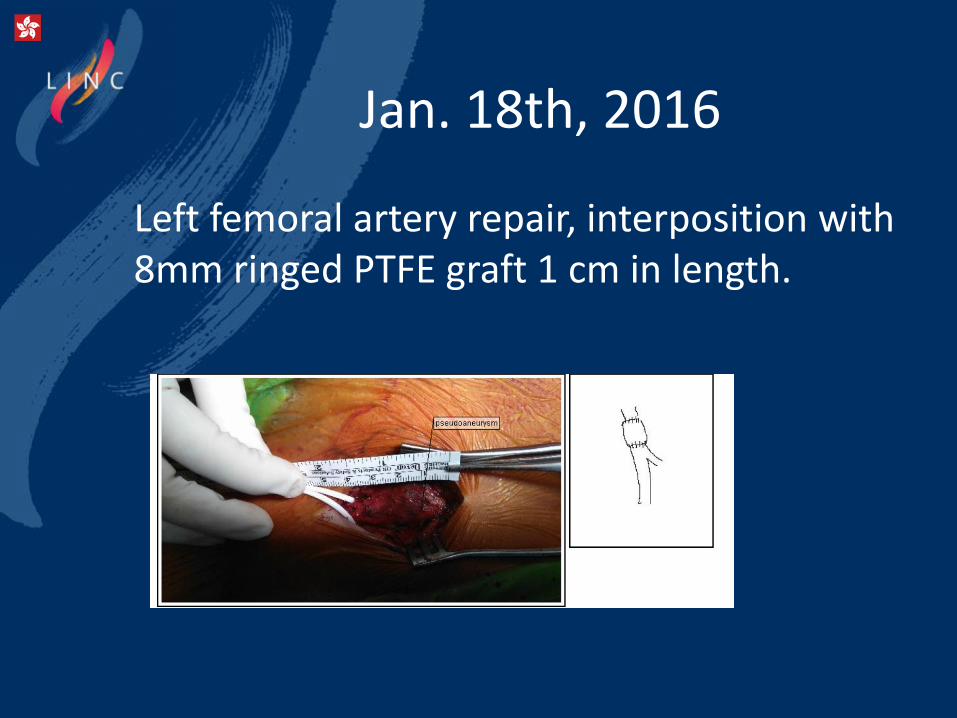
Jan. 18th, 2016
Left femoral artery repair, interposition with 8mm ringed PTFE graft 1 cm in length.

Jan. 24th, 2016

Viabahn 7mmx10cm surgical cutdown via R’t CFA
on Feb. 4th, 2016
Progressive enlargement of pseudoaneurysm (2.1cm 4.7cm)

Hospital Course
• Possible Behcet's disease with GI and vascular involvement.
• Skin biopsy of erythema nodosum of right leg: favored vasculitis
• Ileocecal ulcer: four
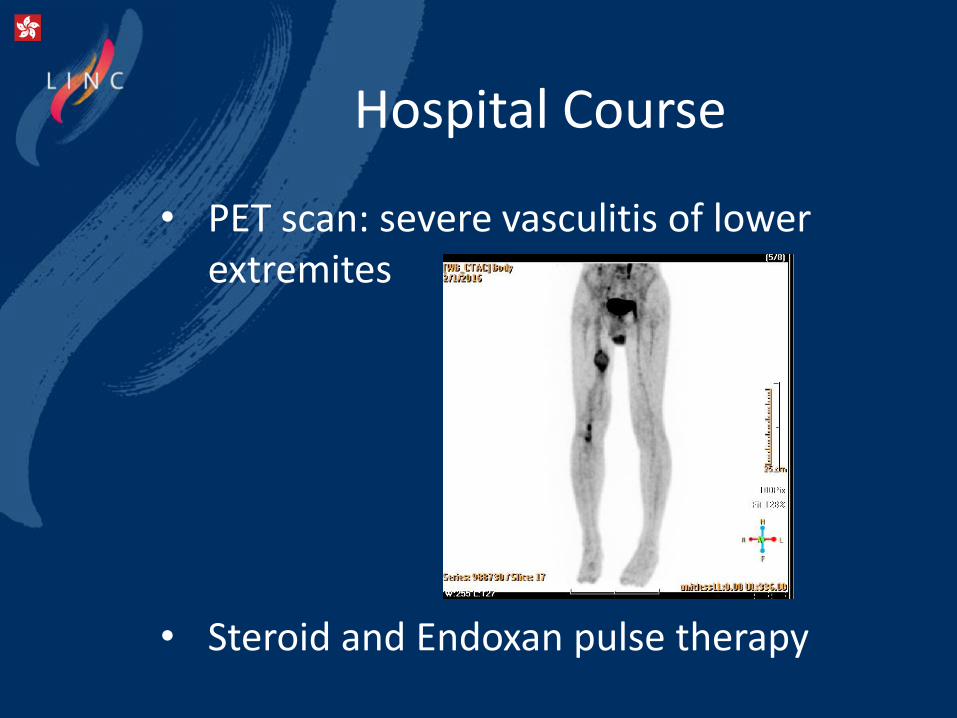
Hospital Course
• PET scan: severe vasculitis of lower extremites
• Steroid and Endoxan pulse therapy
Discussion
• From DEBATE SFA trial, DCB effect is positive irrespective of the recanalization approach (true lumen vs. subintimal) and no arterial aneurysm due to DCB was reported.
• The Global SFA Registry of LUTONIX DCB: Preliminary safety information from the 437 patients enrolled indicates that the most frequent SAEs are pseudoaneurysm (0.7%, 3/437) and Occlusion/Closure (0.7%, 3/437).

Conclusion
• We reported a rare case of young PAOD treated with subintimal approach and DCB, but multiple pseudoaneurysm developed after procedure. The location of pseudoaneurysm is not related to DCB . Finally, vascular Behcet’s disease is diagnosed and we treated the complication by hybrid procedure with surgical repair/Viabahn stenting. The main strategy of treatment is medication of immunosupressants.

Thank You for Attention!

The role of DCB in SFA subintimal tracking lesion
Wei-chun Chang M.D. Wen-Lieng Lee, MD, PhD
Cardiovascular Center, Taichung Veterans General Hospital, Taiwan R.O.C