The role of carbapenems in the hospital - HTIDE · The role of carbapenems in the hospital ....
42
Matteo Bassetti, MD, PhD Infectious Diseases Division Santa Maria Misericordia University Hospital Udine, Italy The role of carbapenems in the hospital
Transcript of The role of carbapenems in the hospital - HTIDE · The role of carbapenems in the hospital ....

Matteo Bassetti, MD, PhD Infectious Diseases Division
Santa Maria Misericordia University Hospital
Udine, Italy
The role of carbapenems in the hospital
Rationale for Antibiotic Optimizaton: Balancing The Needs of Patient and Society
Inappropriate antibiotic therapy associated with higher mortality
Indiscriminate use of broad-spectrum
antibiotics driving resistance
Richards GA. Clin Microbiol Infect. 2005;11(suppl):18-S22.
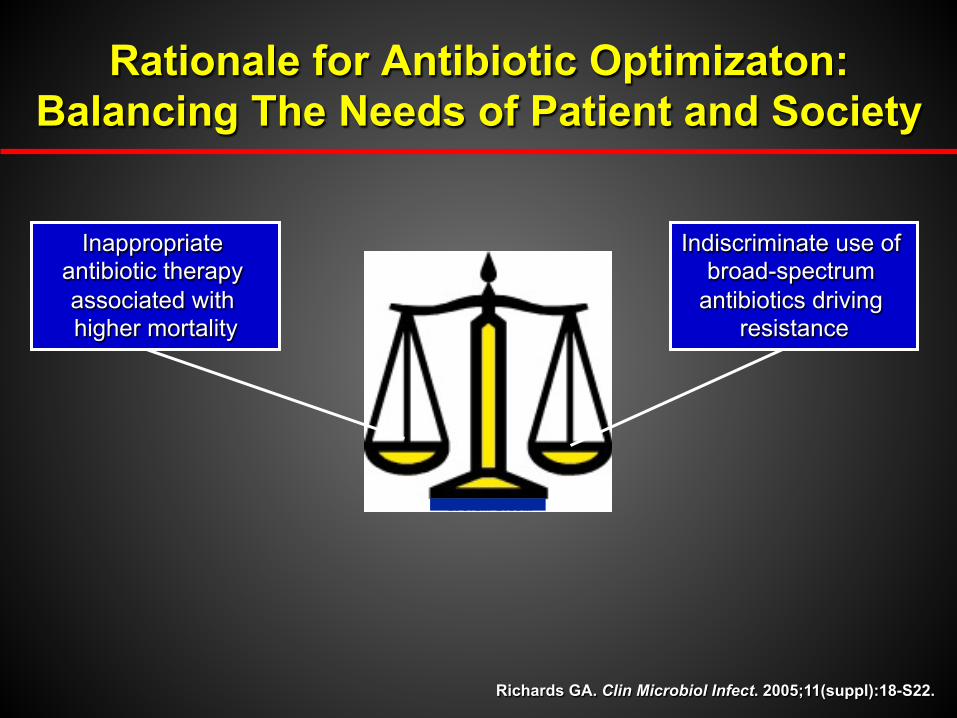
Impact of inappropriate initial empiric antibiotic selection
1. Ibrahim EH, et al. Chest. 2000; 118:146–55; 2. Valles J, et al. Chest 2003; 123:1615–24; 3. Khatib R, et al. Eur J Clin Microbiol Infect Dis 2006; 25:181–5; 4. Teixeira PJZ, et al. J Hosp Infect 2007; 65:361–7; 5. Garnacho-Montero J, et al. J Antimicrobial Chemother 2008; 61:436–41
0
10
20
30
40
50
60
70
80
Bacteraemia1 Community- acquired
bacteraemia2
S. aureus bacteremia3
Ventilator- acquired
pneumonia4
Bacteraemia in ICU patients5
Mor
talit
y (%
of p
atie
nts)
Appropriate antimicrobial treatment Inappropriate antimicrobial treatment
p < 0.001
p < 0.05
p = 0.02
p < 0.02
p < 0.001

How to be appropriate?

Optimal Empiric Therapy
h Choice1 - Patient factors including safety - Local resistance patterns (antibiogram) - Prior antimicrobial exposure
h Appropriate - All suspected pathogens susceptible to ≥1 of the
administered antibiotics
h Timely1 - In one study, patients were 2.1% more likely to die for each
30 minute delay in administration2
h Adequate dosage1 - Consistent with pK/pD parameters
1Deresinski S. Clin Infect Dis. 2007;45:S177-S183. 2Barie PS, et al. Surg Infect. 2005;6:41-54.
3. Leibovici L, et al. BMJ. 1999;318:1614-1618.
“The important decision in antibiotic treatment turns out to be the choice between present and future patients”3

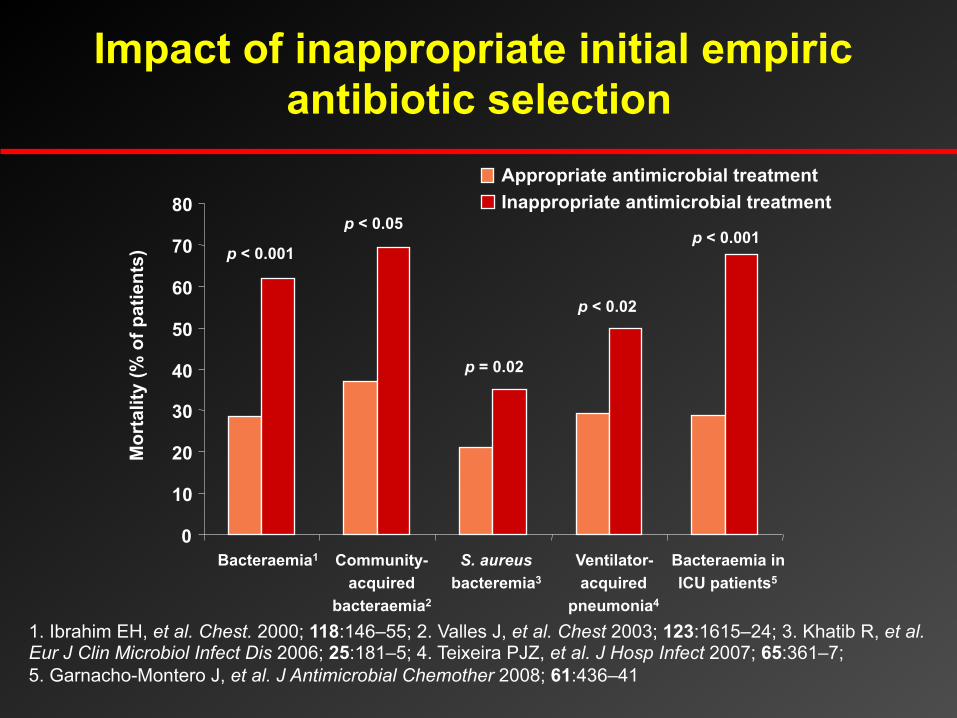
Risk factors for ESBL-producing Enterobacteriaceae isolation within 48h of hospital
Risk factor OR (95% CI) P-value Recent hospitalization a 5.69 (2.94–10.99) 0.001
Admission from another health care facility 5.61 (1.65–19.08) 0.006
Charlson comorbidity index > 4 3.80 (1.90–7.59) 0.001
Previous therapy with beta -lactams and/or fluoroquinolones b
3.68 (1.96–6.91) 0.001
History of urinary catheterization c 3.52 (1.96–6.91) 0.001
Age >70 years 3.20 (1.79–5.70) 0.001
a During the 12 months preceding index hospitalization. b Includes treatment with -lactam/-lactamase inhibitor combinations, oxyiminocephlosporins, and/or fluoroquinolones during the 3 months preceding index admission. c During the 30 days preceding index blood culture.
Tumbarello M, Bassetti M et al. Antimicrob Agents Chemother Jul 2011;55:3485–3490
Multivariate analysis
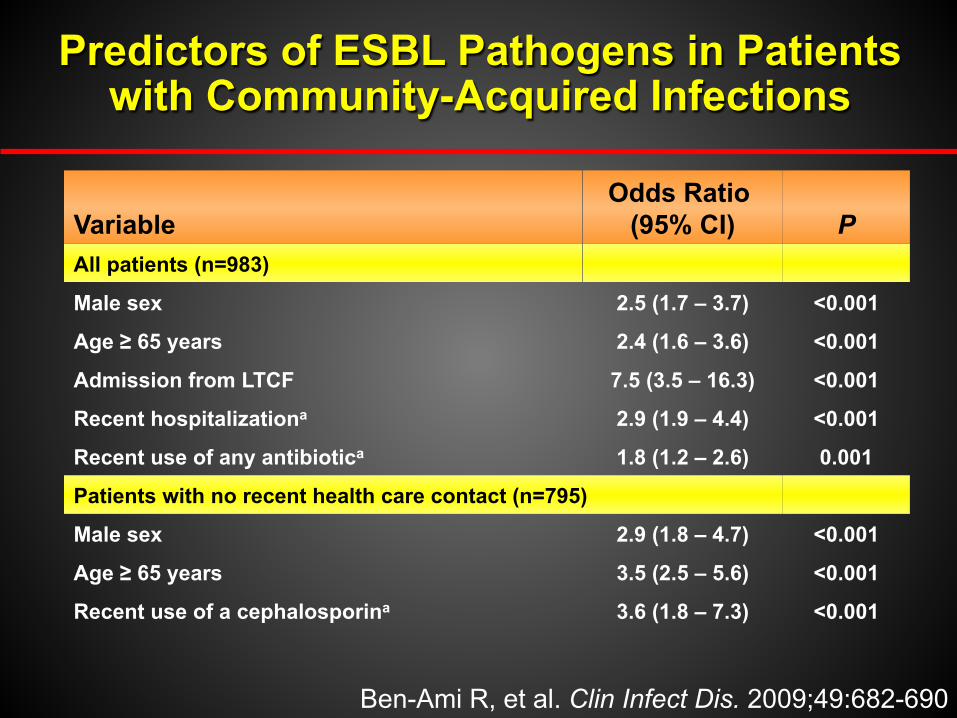
Ben-Ami R, et al. Clin Infect Dis. 2009;49:682-690
Predictors of ESBL Pathogens in Patients with Community-Acquired Infections
Variable Odds Ratio
(95% CI) P All patients (n=983)
Male sex 2.5 (1.7 – 3.7) <0.001
Age ≥ 65 years 2.4 (1.6 – 3.6) <0.001
Admission from LTCF 7.5 (3.5 – 16.3) <0.001
Recent hospitalizationa 2.9 (1.9 – 4.4) <0.001
Recent use of any antibiotica 1.8 (1.2 – 2.6) 0.001
Patients with no recent health care contact (n=795)
Male sex 2.9 (1.8 – 4.7) <0.001
Age ≥ 65 years 3.5 (2.5 – 5.6) <0.001
Recent use of a cephalosporina 3.6 (1.8 – 7.3) <0.001

ESBL-producing K. pneumoniae Bacteraemia
0 5 10 15 20 25 30
Carbapenem
Quinolone
Cephalosporin
Beta-lactaminhibitor
Survivors Non-survivors
50%
40%
36.3%
3.7%
Multivariate analysis of mortality (attributed to bacteraemia)
Carbapenem during the first 5 days : OR ( 95% CI )= 0.06 ( 0.01–0.33); p < 0.001
Paterson D et al. Clin Infect Dis 2004;39:31–37
Crude 14-day mortality (%)

Effect of initial antibiotic therapy on mortality in patients with BSI by ESBL-producing
Enterobacteriaceae
Morta
lity (
%)
Inadequate initial therapy (n=89)
Adequate initial therapy (n=97)
p<0.001
Tumbarello et al. Antimicrob Agents Chemother 2007;51:1987–1994
59,5
18,5
0 10 20 30 40 50 60 70
n=186

Effect of switching initial antimicrobial therapy on mortality
Switching after susceptibility results
p<0.001
Adequate treatment within a few hours
Morta
lity (
%)
n=75 Tumbarello et al. Antimicrob Agents Chemother 2007;51:1987–1994
52
18
0
10
20
30
40
50
60
70

21-d
ay m
orta
lity
(%)
97 ESBL-BSI patients initially treated with
potentially active agents
OR 0.14* 0.55 1.48 4.05** P =*0.01 **<0.001
Tumbarello M et al Antimicrob Agents Chemother 2007; 51:1987-1994

Data from SMART (Study for Monitoring Antimicrobial Resistance Trends) 2005-2007.
ESBL-Producing Gram-Negative Bacilli: A Global Problem
Hawser et al. Int J Antimicrob Agents. 2009;34:585-8.
E. coli 8.1%
K. pneumoniae 16.3%
E. coli 12.2%
K. pneumoniae 37.6%
K. oxytoca 5.3%
E. coli 34.9%
K. pneumoniae 29.8%
K. oxytoca 27.6%
E. coli 4.9%
K. pneumoniae 9.6%
E. coli 21.6%
K. pneumoniae 41.6%
Europe
Africa/Middle East
Asia/Pacific
North America
Latin America
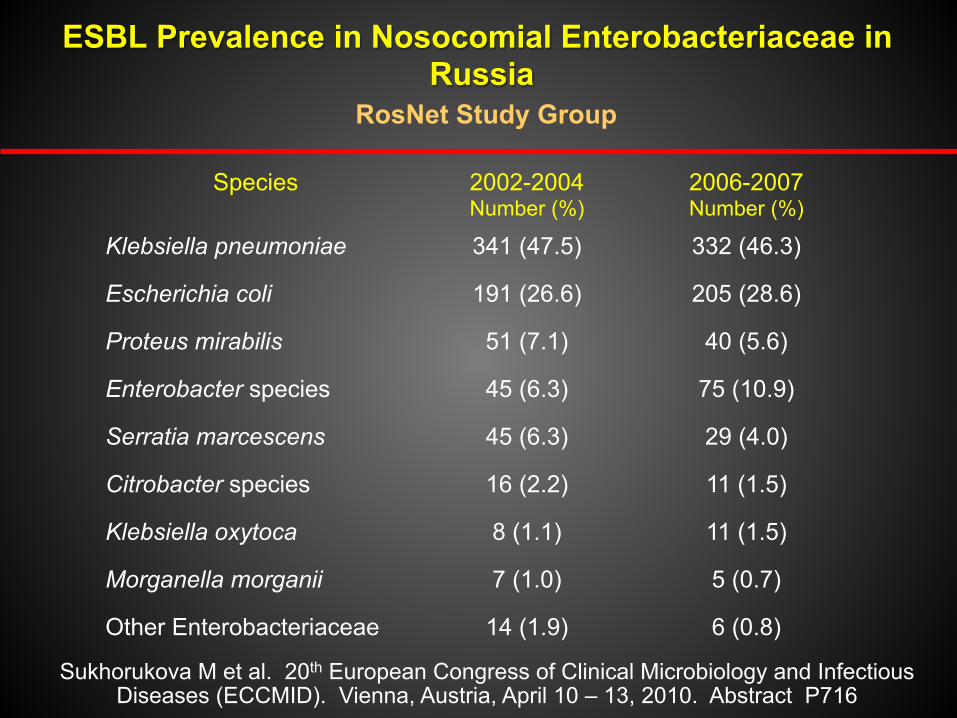
ESBL Prevalence in Nosocomial Enterobacteriaceae in Russia
RosNet Study Group
Sukhorukova M et al. 20th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID). Vienna, Austria, April 10 – 13, 2010. Abstract P716
Species 2002-2004 Number (%)
2006-2007 Number (%)
Klebsiella pneumoniae 341 (47.5) 332 (46.3)
Escherichia coli 191 (26.6) 205 (28.6)
Proteus mirabilis 51 (7.1) 40 (5.6)
Enterobacter species 45 (6.3) 75 (10.9)
Serratia marcescens 45 (6.3) 29 (4.0)
Citrobacter species 16 (2.2) 11 (1.5)
Klebsiella oxytoca 8 (1.1) 11 (1.5)
Morganella morganii 7 (1.0) 5 (0.7)
Other Enterobacteriaceae 14 (1.9) 6 (0.8)
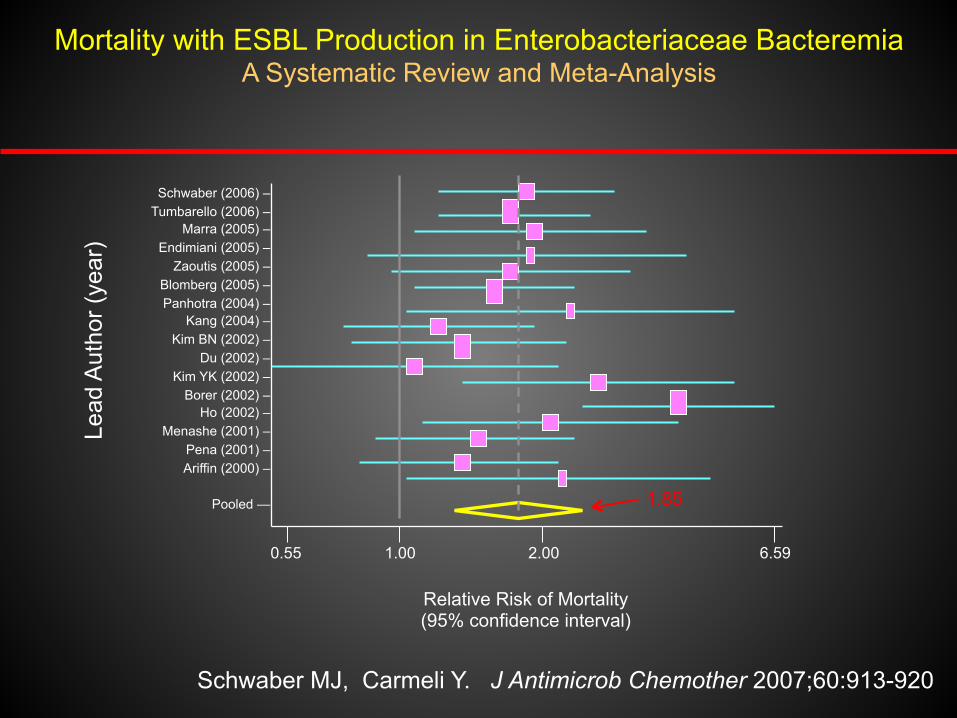
Schwaber MJ, Carmeli Y. J Antimicrob Chemother 2007;60:913-920
Mortality with ESBL Production in Enterobacteriaceae Bacteremia A Systematic Review and Meta-Analysis
Schwaber (2006) – Tumbarello (2006) –
Marra (2005) – Endimiani (2005) –
Zaoutis (2005) – Blomberg (2005) – Panhotra (2004) –
Kang (2004) – Kim BN (2002) –
Du (2002) – Kim YK (2002) –
Borer (2002) – Ho (2002) –
Menashe (2001) – Pena (2001) – Ariffin (2000) –
Pooled —
0.55 1.00 2.00 6.59
Relative Risk of Mortality (95% confidence interval)
1.85
Lead
Aut
hor (
year
)

TREATMENT OPTIONS FOR INFECTIONS DUE TO ESBL+
FIRST CHOICE SECOND CHOICE Urinary tract infection
CARBAPENEM Amoxycillin/clavulanate QUINOLONE
Ventilator-associated pneumonia
CARBAPENEM TIGECYCLINE
Bacteremia CARBAPENEM TYCECICLINE
Intra-abdominal infection
CARBAPENEM TYGECICLINE Quinolone
§ Possibility of using piperacillin-tazobactam for ESLB-producing E. coli bloodstream infections originating from the urinary tract
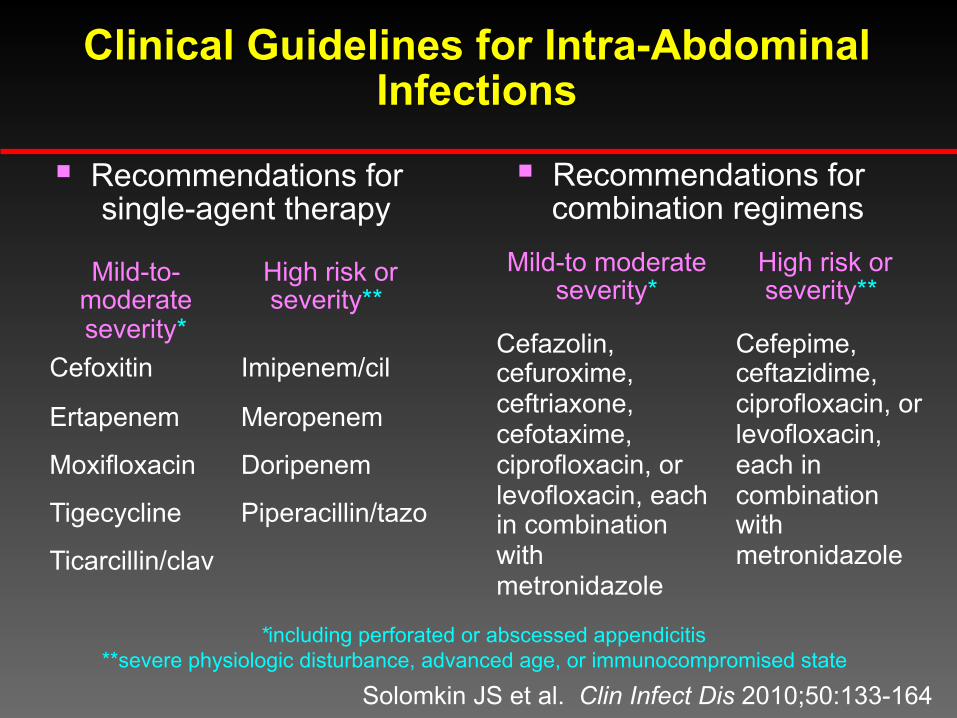
Clinical Guidelines for Intra-Abdominal Infections
Solomkin JS et al. Clin Infect Dis 2010;50:133-164
§ Recommendations for single-agent therapy
§ Recommendations for combination regimens
Mild-to moderate severity*
High risk or severity**
Cefazolin, cefuroxime, ceftriaxone, cefotaxime, ciprofloxacin, or levofloxacin, each in combination with metronidazole
Cefepime, ceftazidime, ciprofloxacin, or levofloxacin, each in combination with metronidazole
Mild-to-moderate severity*
High risk or severity**
Cefoxitin Imipenem/cil Ertapenem Meropenem Moxifloxacin Doripenem
Tigecycline Piperacillin/tazo
Ticarcillin/clav
*including perforated or abscessed appendicitis **severe physiologic disturbance, advanced age, or immunocompromised state
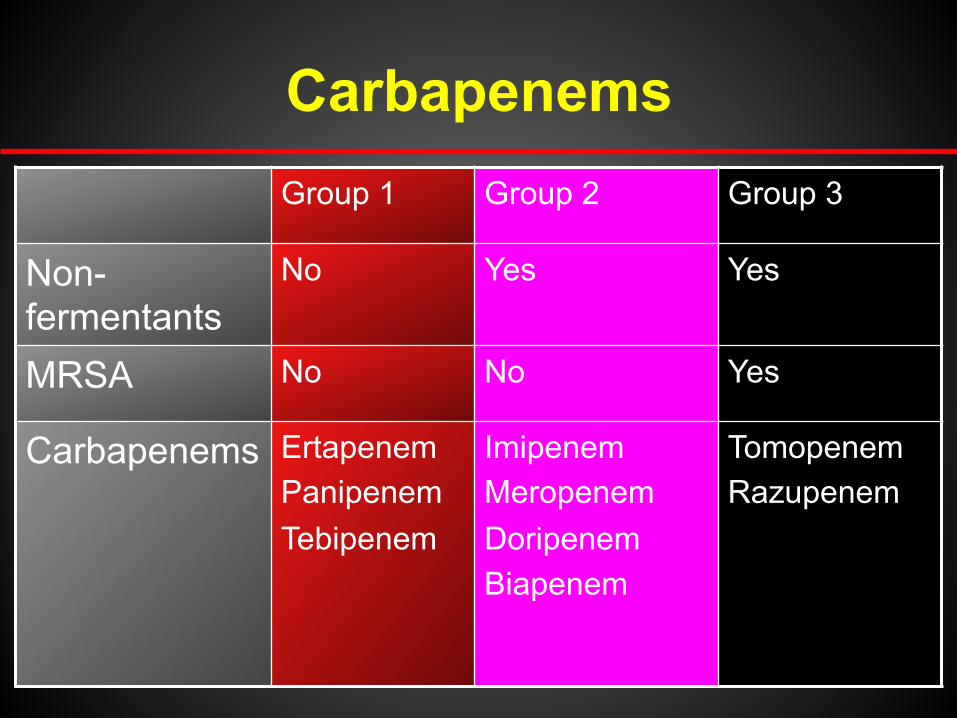
Carbapenems Group 1 Group 2 Group 3
Non-fermentants
No Yes Yes
MRSA No No Yes
Carbapenems Ertapenem Panipenem Tebipenem
Imipenem Meropenem Doripenem Biapenem
Tomopenem Razupenem

Newer carbapenems
Bassetti M et al. Curr Med Chem. 2009;16:564-75

Relative activity of Carbapenems
Gram-Positive Activity
Gram-Negative Activity
Imipenem Ertapenem
Meropenem Doripenem
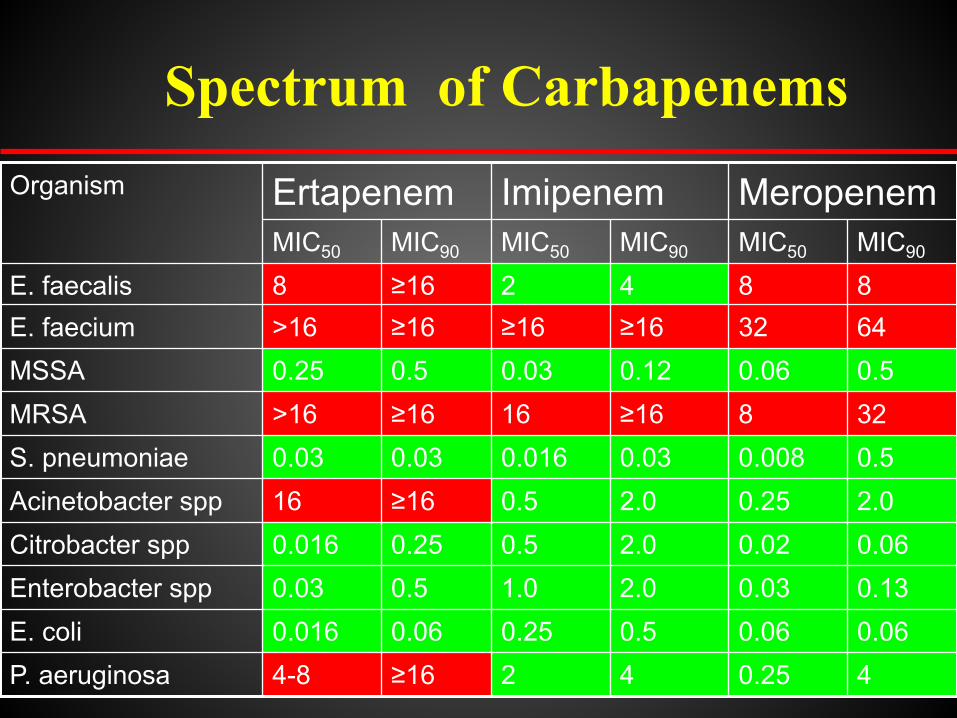
Organism Ertapenem Imipenem Meropenem MIC50 MIC90 MIC50 MIC90 MIC50 MIC90
E. faecalis 8 ≥16 2 4 8 8 E. faecium >16 ≥16 ≥16 ≥16 32 64 MSSA 0.25 0.5 0.03 0.12 0.06 0.5 MRSA >16 ≥16 16 ≥16 8 32 S. pneumoniae 0.03 0.03 0.016 0.03 0.008 0.5 Acinetobacter spp 16 ≥16 0.5 2.0 0.25 2.0 Citrobacter spp 0.016 0.25 0.5 2.0 0.02 0.06 Enterobacter spp 0.03 0.5 1.0 2.0 0.03 0.13 E. coli 0.016 0.06 0.25 0.5 0.06 0.06 P. aeruginosa 4-8 ≥16 2 4 0.25 4
Spectrum of Carbapenems

In vitro Activity of Antibiotics (% Susceptible) Against ESBL-Producing Organisms
Kozlov RS et al. Final report of IISP No. MK-0826 RUSLS1292, 2009
Ertapenem
h New 1-ß-methyl carbapenem licensed in 2003
h Significantly different properties from existing carbapenems
h Significantly different uses

Carbapenem properties
Ertapenem Imipenem - Cilastatin
Meropenem
Stable to renal DHP1
Yes No Yes
Metabolism Renal I: Hepatic C: Renal
Renal
Protein bound
~94% 20% <10%
Half life 4h 1h 1h

Ertapenem Human Pharmacokinetics
Bioavailability of IM Ertapenem > 90%
2 mg/L
Half-life ~ 4h
1
10
100
1000
0 2 4 6 8 10 12 14 16 18 20 22 24
Time, hr
[Tot
al E
rtape
nem
] PL (
mg/
L)
IV IM
Healthy Volunteers Single 1g dose
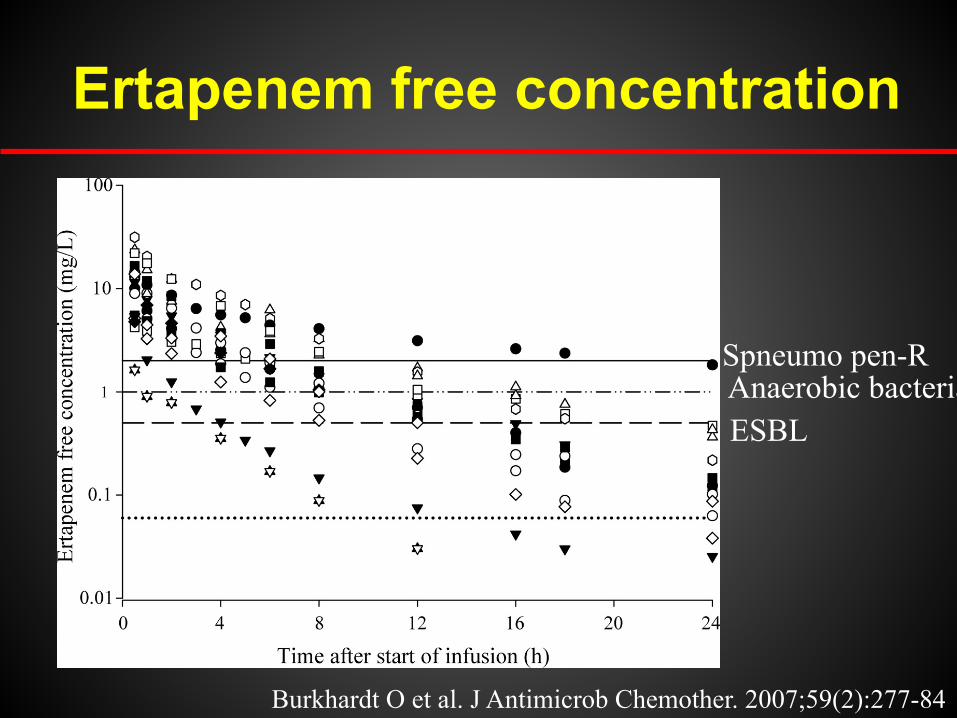
Ertapenem free concentration
ESBL
Spneumo pen-R Anaerobic bacteria
Burkhardt O et al. J Antimicrob Chemother. 2007;59(2):277-84
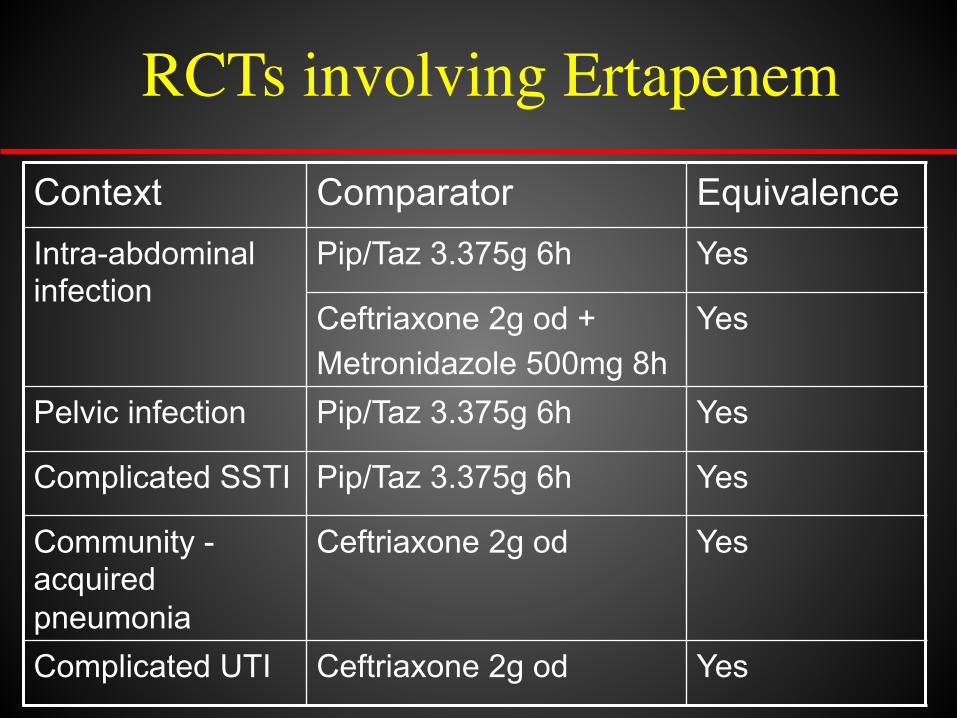
Context Comparator Equivalence Intra-abdominal infection
Pip/Taz 3.375g 6h Yes
Ceftriaxone 2g od + Metronidazole 500mg 8h
Yes
Pelvic infection Pip/Taz 3.375g 6h Yes
Complicated SSTI Pip/Taz 3.375g 6h Yes
Community -acquired pneumonia
Ceftriaxone 2g od Yes
Complicated UTI Ceftriaxone 2g od Yes
RCTs involving Ertapenem
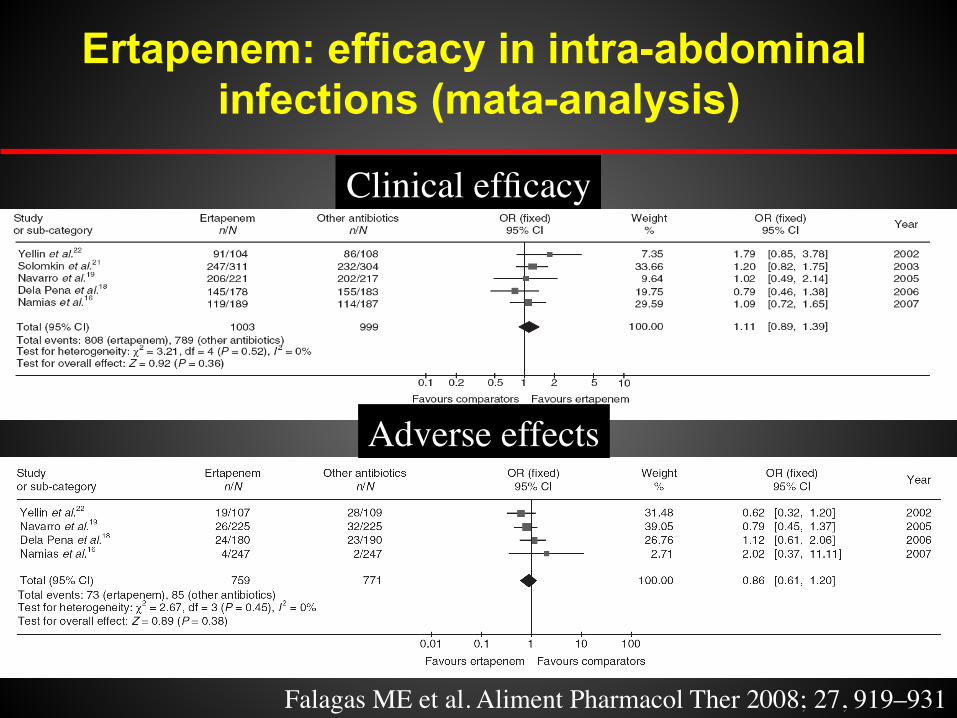
Ertapenem: efficacy in intra-abdominal infections (mata-analysis)
Clinical efficacy
Adverse effects
Falagas ME et al. Aliment Pharmacol Ther 2008; 27, 919–931
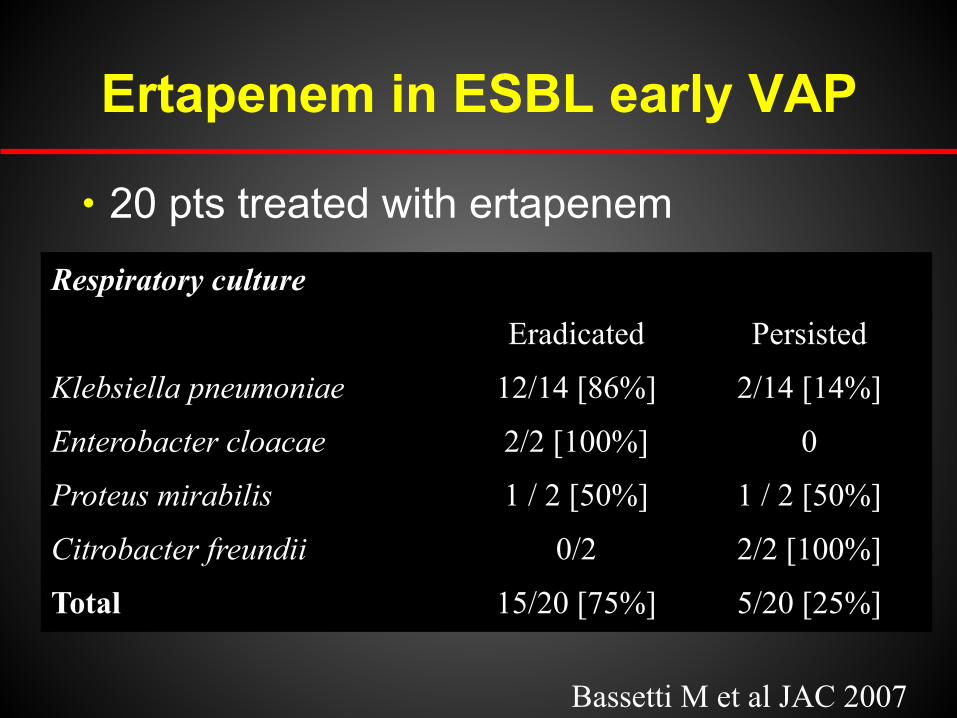
Ertapenem in ESBL early VAP
h 20 pts treated with ertapenem
Bassetti M et al JAC 2007
Respiratory culture
Eradicated Persisted
Klebsiella pneumoniae 12/14 [86%] 2/14 [14%]
Enterobacter cloacae 2/2 [100%] 0
Proteus mirabilis 1 / 2 [50%] 1 / 2 [50%]
Citrobacter freundii 0/2 2/2 [100%]
Total 15/20 [75%] 5/20 [25%]
The Primary Goal Espoused in the IDSA/SHEA Antibiotic Stewardship Guideline
§ “The primary goal of antimicrobial stewardship is to optimize clinical outcomes while minimizing unintended consequences of antimicrobial use, including toxicity, the
selection of pathogenic organisms (such as Clostridium difficile), and the emergence of
resistance.”
Dellit TH. Clin Infect Dis 2007;44:159-177

Correlation Between Antibiotic Consumption and Resistance in P. aeruginosa
Antibiotic class !Hazard ratios! Ceftazidime !0.8!
Piperacillin !5.2!
Ciprofloxacin !9.2!
Imipenem !44!
Carmeli Y et al. Antimicrobial Agents Chemother. 1999;43:1379-1382.
Lepper PM et al. Antimicrob Agents Chemother. 2002;46:2920-2925.
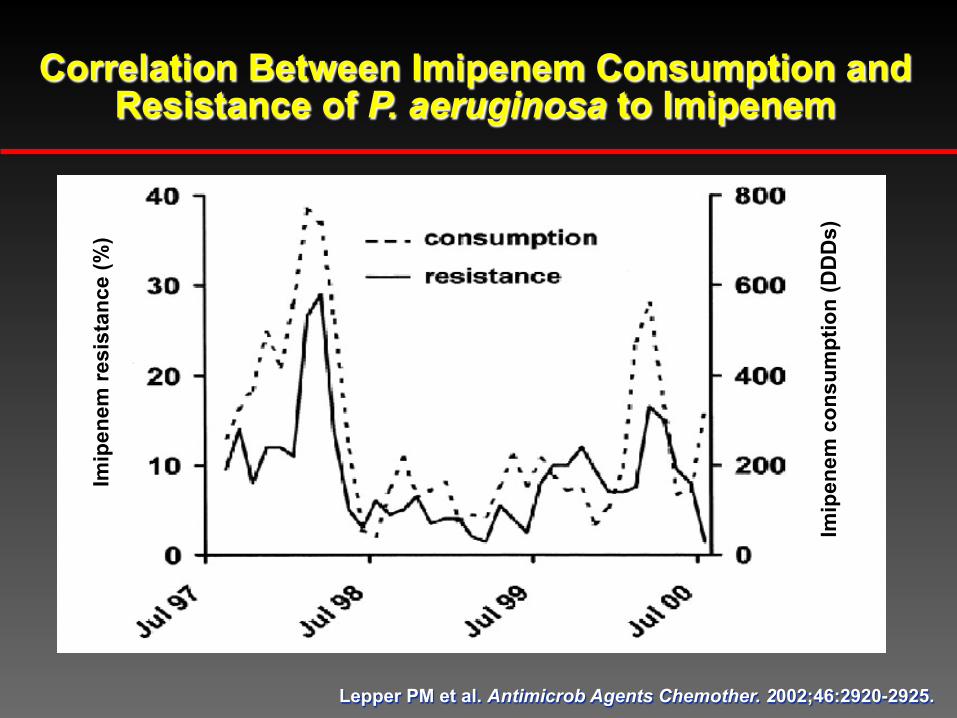
Correlation Between Imipenem Consumption and Resistance of P. aeruginosa to Imipenem
Imip
enem
resi
stan
ce (%
)
Imip
enem
con
sum
ptio
n (D
DD
s)

Risk Factors for Imipenem-Resistant P. aeruginosa
h A total of 779 isolated resulting in an incidence of 5.6 cases per 1,000 patient admissions (with an average % resistance of 21.6%)
h Associated with a high incidence of imipenem-resistant P. aeruginosa by univariate analysis - Group 2 carbapenems (P <0.0001) - Aminoglycosides (P = 0.034) - Penicillins (P = 0.05)
h Group 1 carbapenems not associated with imipenem-resistant P. aeruginosa (P = 0.2)
Carmeli Y et al. Diagn Microbiol Infect Dis 2011;70:367–372
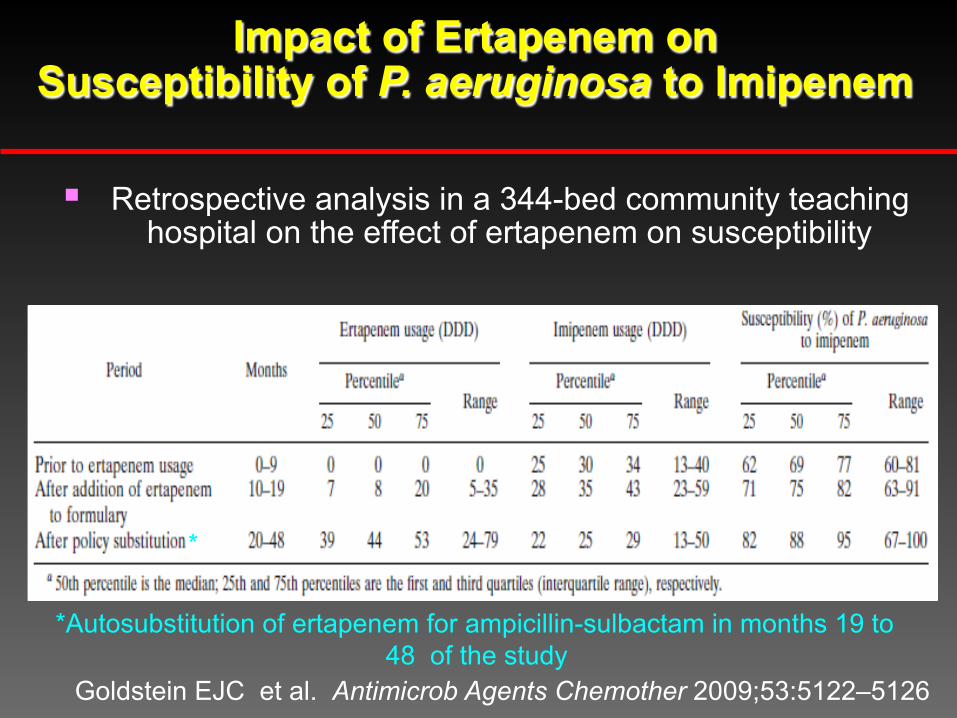
Impact of Ertapenem on Susceptibility of P. aeruginosa to Imipenem
Goldstein EJC et al. Antimicrob Agents Chemother 2009;53:5122–5126
*
*Autosubstitution of ertapenem for ampicillin-sulbactam in months 19 to 48 of the study
§ Retrospective analysis in a 344-bed community teaching hospital on the effect of ertapenem on susceptibility

*Nicolau DP et al. Int J Antimicrob Agents 2012;39:11-15
§ Suggestion that ertapenem best used as either empirical or directed therapy for infections due to aerobic gram-negative and mixed anaerobic bacteria where coverage of non-fermentative gram-negatives including Pseudomonas is not typically necessary or desirable • Suspected infections due to ESBL-producing bacteria • Polymicrobial complicated intra-abdominal infections
where the probability of Pseudomonas is unlikely based on the medication history, clinical course, and demographics of the patient
§ Potential role in de-escalation or step-down therapy from carbapenems when possible, with therapy being changed as necessary once culture data become available
An Example of Optimizing Antibiotic Use Through an ASP: Carbapenem Stewardship*

Carbapenems in VAP
Soo Hoo GW et al. Chest 2005;128:2778-87
h ICU carbapenem-based regimen
h After D3 therapy based on susceptibility results
h Better empirical cover (81 vs 46%; p<0.01)

When to Expect P. aeruginosa
h Retrospective analysis from 4 hospitals - 151 patients and 152 controls
h P. aeruginosa caused 6.8% of 4,114 episodes of Gram-negative bacteremia
h Risk factors: severe immunodeficiency, OR: age >90, antimicrobials within 30 days, presence of central venous catheter or a urinary device - If ≥2 had over 25% risk for P. aeruginosa
V Schechner et al, CID 48:580-6, 2009
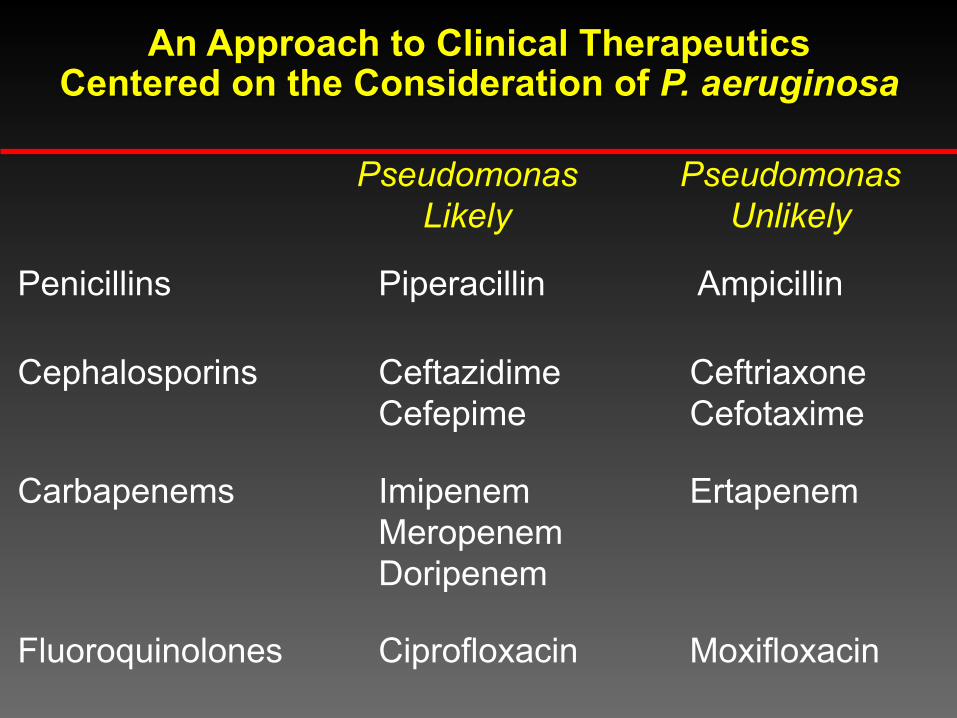
An Approach to Clinical Therapeutics Centered on the Consideration of P. aeruginosa
Pseudomonas Likely
Pseudomonas Unlikely
Penicillins Piperacillin Ampicillin
Cephalosporins Ceftazidime Cefepime
Ceftriaxone Cefotaxime
Carbapenems Imipenem Meropenem Doripenem
Ertapenem
Fluoroquinolones Ciprofloxacin Moxifloxacin
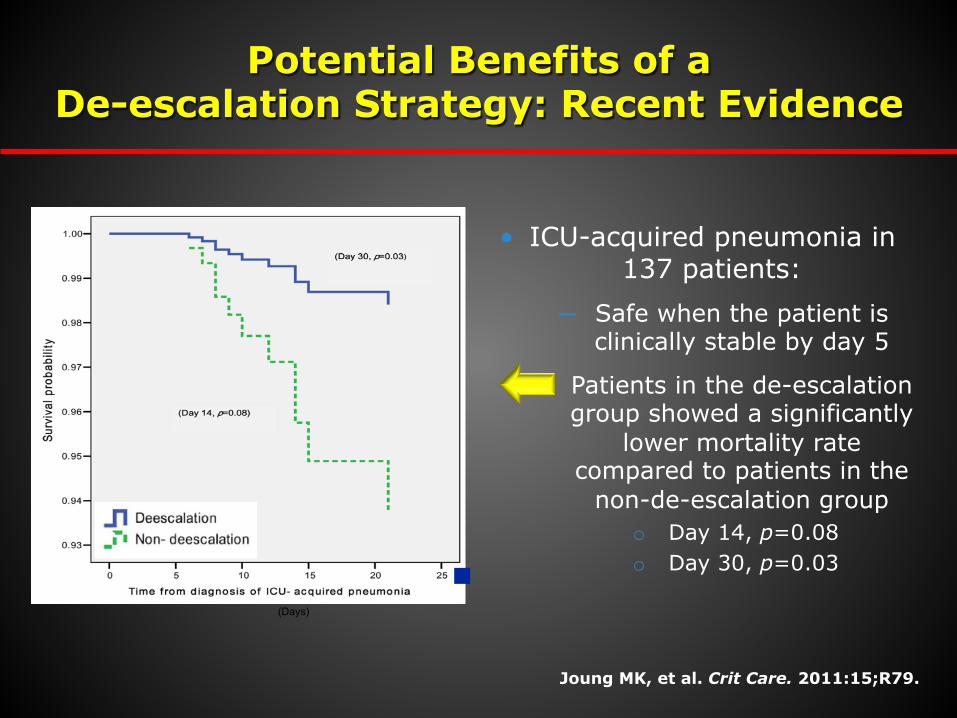
Potential Benefits of a De-escalation Strategy: Recent Evidence
• ICU-acquired pneumonia in 137 patients:
─ Safe when the patient is clinically stable by day 5
─ Patients in the de-escalation group showed a significantly
lower mortality rate compared to patients in the
non-de-escalation group o Day 14, p=0.08 o Day 30, p=0.03
(Days)
Joung MK, et al. Crit Care. 2011:15;R79.

De-escalation in the ICU: A Retrospective Study
• All consecutive patients treated with empiric therapy in the ICU for ≥72 hours over a period of 16 months
─ 116 patients with 133 infections
─ All infections were examined, not just VAP
─ De-escalation in 60 (45%) of cases
• De-escalation therapy was associated with a significant reduction of recurrent infection
• 15% vs. 5% (p = 0.02)
• De-escalation had no effect on mortality
Morel J, et al. Crit Care. 2010:14;R225.

Potential Benefits of a De-escalation Strategy
• A reduction in overall antimicrobial costs
• Beneficial impacts on the antimicrobial resistance
profile of the institution
• Decreased antibiotic-related adverse events
– Superinfection with resistant bacteria
– Clostridium difficile
• No alteration in treatment outcomes
Masterton RG. Crit Care Clin. 2011:27;149-162.
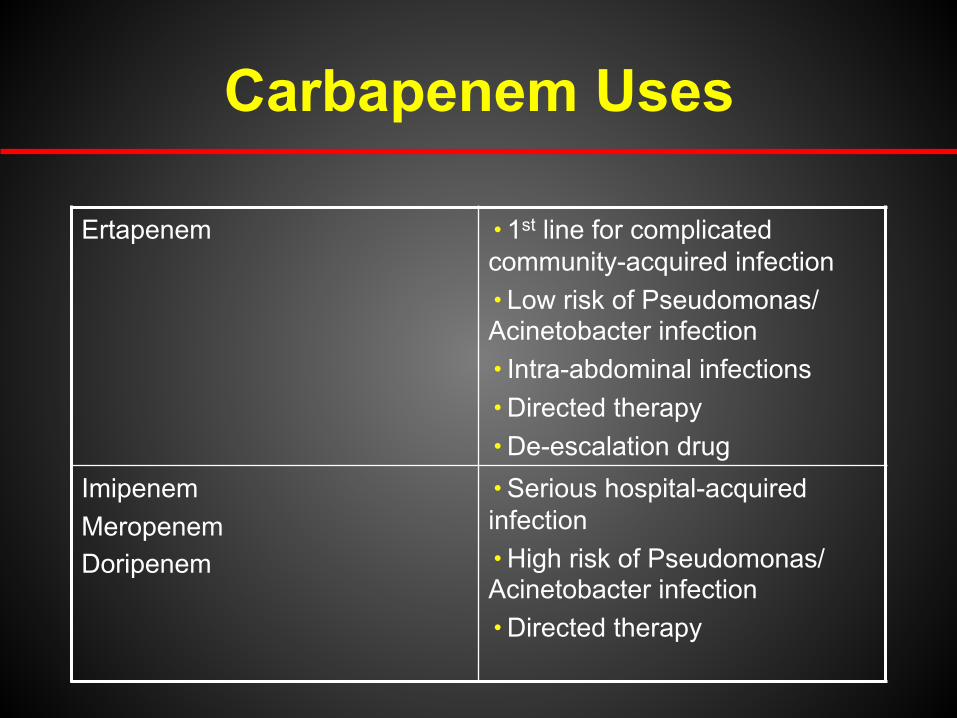
Carbapenem Uses
Ertapenem h 1st line for complicated community-acquired infection h Low risk of Pseudomonas/ Acinetobacter infection h Intra-abdominal infections h Directed therapy h De-escalation drug
Imipenem Meropenem Doripenem
h Serious hospital-acquired infection h High risk of Pseudomonas/ Acinetobacter infection h Directed therapy