
Antibiotic use: making the best of what we have. · Ampicillin. Piperacillin ... Augmented ....
91
Welcome to this SIRN symposium Antibiotic use: making the best of what we have.
-
Upload
truongkhuong -
Category
Documents
-
view
217 -
download
0
Transcript of Antibiotic use: making the best of what we have. · Ampicillin. Piperacillin ... Augmented ....
Welcome to this SIRN symposium
Antibiotic use: making the bestof what we have.
SIRN series of symposia
MRSA workshop: John Coia, Jacqui Rielly
Antibiotic use : Ysobel Gourlay, Jeff Edwards, Lesley Frew
C. difficile : Ian Poxton
Pneumococci: Tim Mitchell
Patient’s journey: missing data Fiona Skinner
Others …………………..

‘We are in a situation where infections associated with antibiotic-use and the continued emergence of strains resistant to antibiotics are not being countered by the introduction of novel therapies.
This requires debate and action.’
Programme for today
Three lectures:
The Scottish Antimicrobial Prescribing Group (SAPG) : A National Clinical Forum for Antimicrobial Stewardship
Prof Dilip Nathwani
Guess or get it right –
antimicrobial prescribing in the 21st century?
Dr Bob Masterton
Why its difficult to identify new antibacterial agents
Dr Jeff Edwards
Composite discussion led by Dr Alistair Leanord

Jeff Edwards MSc, PhD
Most of my career in big Pharma
ICI, Zeneca, AstraZeneca
Discovery scientist
Development scientist: cefotetan, ZD0870, meropenem
AstraZeneca Infection Therapy Area Team
strategy, clinical microbiology, in-licensing
Member of ECCMID and ICAAC Programme Committees

Multidrug-resistant Gram-negative infections
What is the unmet medical need?
GEORGE M. ELIOPOULOS, MD; Boston, MA.
What is currently being used?
LOUIS B. RICE, MD; Cleveland, OH.
What's in the pipeline
GEORGE TALBOT, MD; St. Davids, PA.
Why it's difficult to identify new antibacterial agents
JEFFREY R. EDWARDS, PhD; United Kingdom.
Should we rely on government intervention to encourage new solutions?
DAVID SHLAES, MD; Stonington, CT.
Multidrug-resistant Gram-negative infections
GEORGE ELIOPOULOS
spoke of LIN-R S. aureus

Multidrug-resistant Gram-negative infections
LOU RICE
‘Coming to your hospital soon –an untreatable infection’
Multidrug-resistant Gram-negative infections
GEORGE TALBOT
Produced an exhauistive list of on-going clinical studies showing that there was nothing new
Multidrug-resistant Gram-negative infections
DAVE SHLAES
Did not think Government intervention was the way forward
One company used to be 41 !
FDA threatened Bayer: provide cheap CIPRO to be stockpiled re Anthrax or watch your patents!
Why its difficult to find
new antibacterial agents
Why its difficult to find
new antibacterial agents
‘find’: discover by chance

Why its difficult to identify
new antibacterial agents
‘identify’: establish or select by consideration or analysis of the circumstances

John Bell Karen BushGraham Boulnoir Rudolph ThenPaul Newell Richard WhiteBarry MasonBob Nolan Phil Turner George Drusano
Bob Moellering
Phil Edwards Mike DudleyMike Gravestock Ron PalkMark Macielag
David LivermoreFred Tenover
Jason Oliver Al Sheldon
It is not my intention to speak only about the research process but wish to share with you some thoughts, some of which, I hope will be outside your current thinking.
You will, undoubtedly, know some of what I will say, but perhaps you didn’t realise you did!
Also, you may not agree with some of my comments and will wish to discuss. That’s just fine as I come from an environment where any time I spoke from the podium, I expected hearty challenge.
I’ll try to cover ……………….
Evolution of established antibiotic classes and their future
Reduction in choice
Comments on some recent contenders
The Pharmaceutical industry today and the increased power of the Commercial function
Making discovery-life difficult, making mistakes
How about genomics?
Discovering needed agents will be a challenge
Nympholepsy
I’ll try to cover ……………….
Evolution of established antibiotic classes and their future potential
Reduction in choice
Comments on some recent contenders
The Pharmaceutical industry today and the increased power of the Commercial function
Making life difficult, making mistakes
How about genomics?
Discovering needed agents will be a challenge
Nympholepsy: the frenzied pursuit of the unattainable

Also,
You will note that I will continuously make USA-related considerations
- FDA- Hospital Formulary
I do this because without the expectation of registration in the USA, the development of a new anti-bacterial will
NOT BE FINANCIALLY VIABLE.
Penicillin
Penicillin
Nalidixic acid
ErythromycinMethicillin
Vancomycin
Ampicillin
NovobiocinCarbenicillin
Lincomycin
Ticarcillin
Fusidic acid Cephalothin
Rifampacin
Cephaloradine BacitracinGentamicin + PolymyxinTetracyclinesChloramphenicol +NitrofuratoinMetronidazoleSulphanomidesTrimethoprim
β-lactams:
PenicillinMethicillinAmpicillinPiperacillin
Augmented penicillins
Cephalosporins- ceftriaxone - ceftazidime
Carbapenems-imipenem/cil-meropenem
β-lactams:
Quinolones:
Penicillin
Nalidixic acidMethicillinAmpicillin
Norfloxacin
PiperacillinCiprofloxacin
Augmented penicillins
How many other ‘floxacins ?
Cephalosporins -
ceftriaxone
- ceftazidime
Carbapenems- imipenem/cil-
meropenem

β-lactams:
Quinolones:
Others:
Penicillin
Nalidixic acid
MacrolidesMethicillin
Glycopeptides
Ampicillin Norfloxacin Lincomycin+ Piperacillin Aminoglycosides
Ciprofloxacin
PolymyxinTetracyclines
Augmented How many other Nitrofurans
penicillins ‘floxacins ?
MetronidazoleTrimethoprim
Cephalosporins - ceftriaxone - ceftazidime
Carbapenems
Linezolid-
imipenem/cil
Quin+Dalf
- meropenem Daptomycin








Are you really surprised that I defend myself by ‘resisting’ the agents you try to kill me with ?????
All bacterial infections
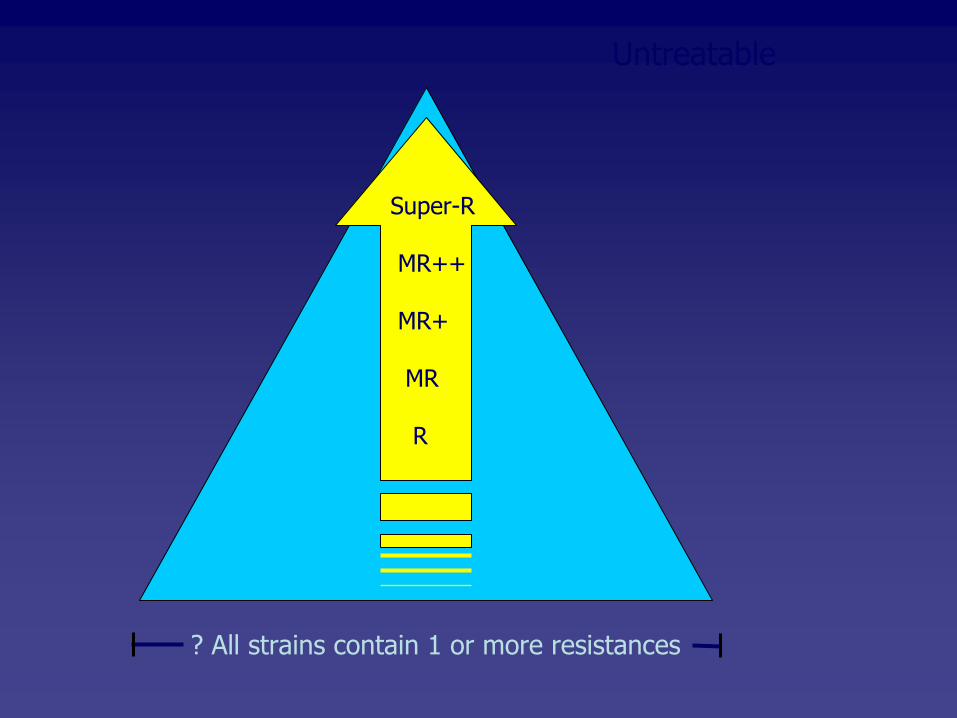
?
All strains contain 1 or more resistances
Untreatable
Super-R
MR++
MR+
MR
R

Untreatable
Super-R
MR++
MR+
MR
R
?
All strains contain 1 or more resistances
We have progressed through
• a new era of life-saving antibiotics• the discovery of many new series• the exploitation of these series• an era when almost all infections could be treatedwith more than one class of antibiotic.
We are now in a phase when
• many of the best classes have been exhausted or are near to exhaustion
• some older classes have been revisited• new classes are extremely uncommon• a tiny proportion of infections are untreatable• economics do not favour antibacterials and researchis contracting.
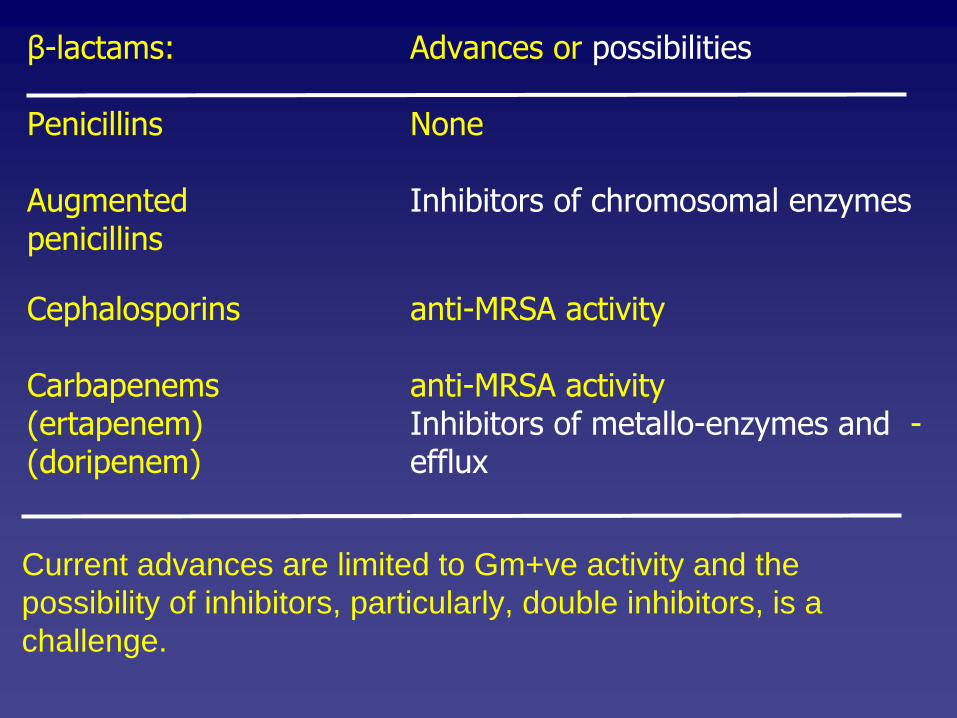
β-lactams:
Advances or possibilities
Penicillins
None
Augmented Inhibitors of chromosomal enzymes penicillins
Cephalosporins anti-MRSA activity
Carbapenems
anti-MRSA activity(ertapenem)
Inhibitors of metallo-enzymes and -
(doripenem)
efflux
Current advances are limited to Gm+ve activity and the possibility of inhibitors, particularly, double inhibitors, is a challenge.

Quinolones:
How many others and what can they deliver?
Thus far, attempts to improve properties has had two broad effects
• miscellaneous toxicities
• improved anti Gm+ve potency
Circumventing R mechanisms in Gm-ves
has not been achieved.

Others classes/types
Macrolides/ketolides
Limited advanceGlycopeptides
Exhausted
Daptomycin (lipogly…)
? Quin+dalf
More
Tetracyclines
? advance (tigecycline) Oxazolidinones
? who knows
Trimethoprim
? advance (iclaprim)
Aminoglycosides
NoneNitroimidazoles
None
Lincomycin+
NonePolymyxin NoneChloramphenicol
None
Nitrofurans
None
Cationic peptides
? safety, manufacture FAB (fatty acid biosynthesis)
Whatever the class, most of the recent advances have been directed against Gm+ves.
Most have come from known-series and even if we didn’t realize it, finding anti-Gm-ve
activity,
particularly against non-fermentors, always has been a challenge.
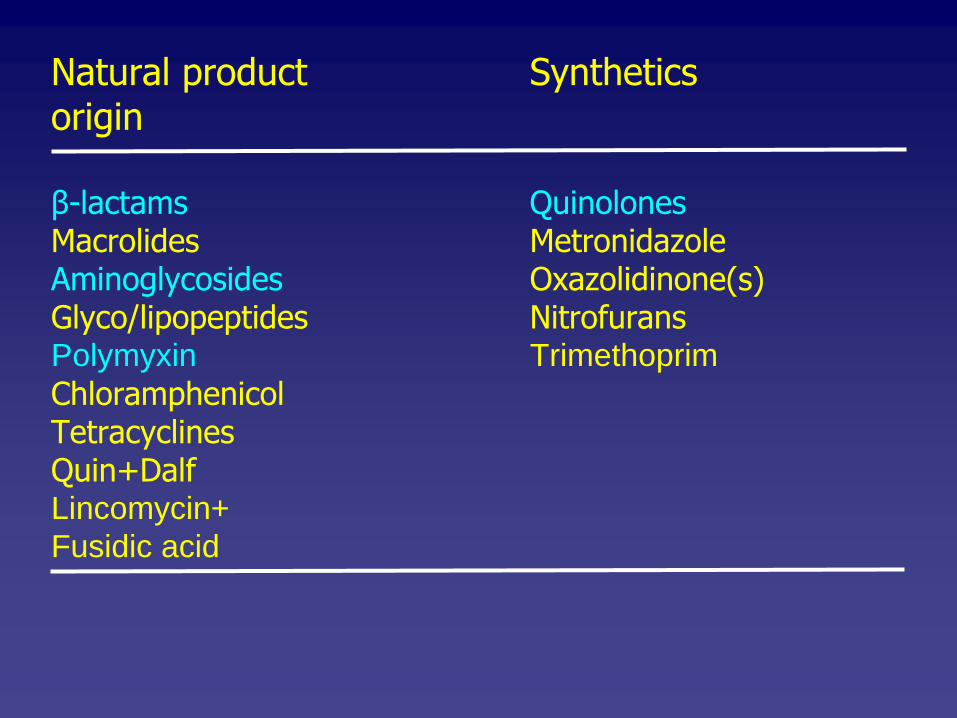
Natural product
Syntheticsorigin
β-lactams
QuinolonesMacrolides
Metronidazole
Aminoglycosides
Oxazolidinone(s)Glyco/lipopeptides
Nitrofurans
Polymyxin TrimethoprimChloramphenicolTetracyclinesQuin+DalfLincomycin+Fusidic acid

Gram +ve
Gram -ve
Physicochemical properties required for Gram+ve and Gram-ve activity are different

ICAAC 2008 symposium
New molecules from ‘old’
classes: Is there still room for improvement?
Quinolones, oxazolidinones, tetracyclines, β-lactams
All speakers are well known academics or from established Pharma companies.
Going forward ……..

We speak about the ‘Pharmaceutical Industry’
but
• this is a composite of independent Companies, each oneserving it’s own share-holders
• as far as I know, there is no integrated approach towards finding defined anti-bacterial agents
• I would not presume to be definitive about any positionin any one Company, we will no doubt agree that infectionresearch in the Pharmaceutical Industry has reduced
• I suggest to you that there are few, if any, of the remainingCompanies, in which effort has not been focused in a mannerwhich is to the detriment of novel research
• The importance of financial return has led to a dominance of the Commercial function in decision-making processes, evenat early stages.

Some realities ……………
• we have many excellent agents
• many of today’s best agents have been used for >10 years
• any new agent must make an acceptable financial return
• the need for speed
• Regulatory requirements must be achievable
• hospital-formulary acceptance is a must for any new agent
• Proposed projects typically are assessed using
Target Product Profiles.

How is financial viability assessed?
What is a financially viable spectrum of anti- bacterial activity ?

How is financial viability assessed?
Net present value (NPV)
How much profit would be made in today’s-money
Peak-year sales
>US$ 0.5 bn

What is a financially viable spectrum of anti-bacterial activity ?
Aerobes
Anaerobes
Gram+ve
Gram-ve
Staph/strep
Enterococci
Enterobacteriaceae Non-fermenters
++ ++ + ++ + + + + + + + +
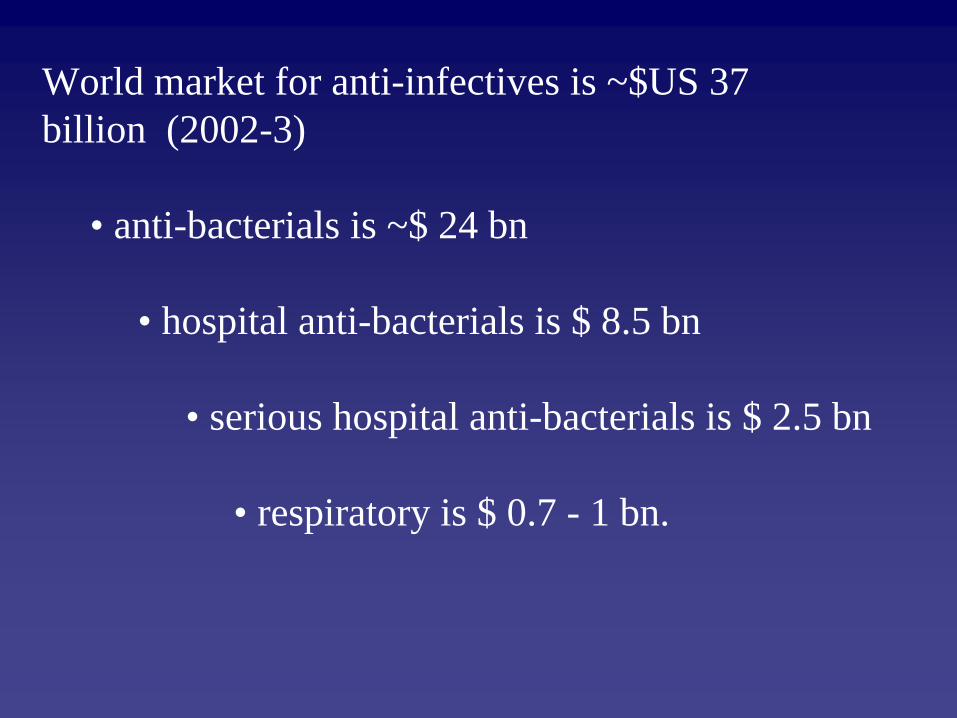
World market for anti-infectives is ~$US 37 billion (2002-3)
• anti-bacterials is ~$ 24 bn
• hospital anti-bacterials is $ 8.5 bn
• serious hospital anti-bacterials is $ 2.5 bn
• respiratory is $ 0.7 - 1 bn.

Target Product Profiles (TPPs)
• Used widely across therapeutic areas
• Compiled by scientific/medical/commercial colleagues
• Define the properties required of a new molecule to make it economically viable (worth developing)
Typically very, very challenging targets.
TPP
RTP

Broad spectrum antibacterial agent for hospital use
Registered indication: Parenteral therapy for empiric use in for moderate/severe nosocomial infections.
Customer group: Hospital specialists, ID physicians in general medical/surgical or critical care units, oncologists, haematologists and internists
Promotional claims:
Novel chemical classClinical efficacy against all Gram+ Gram-
aerobic and anaerobic pathogens Improved efficacy over contemporary therapiesPharmacodynamic properties leading to pathogen eradication Active against strains resistant to contemporary therapies Intravenous formulations given bdCompatible with other drugs and fluids given to patient groupWell tolerated
Distinguishing Attributes:
Does not cause CDADOnce daily dosing

Broad spectrum antibacterial agent for hospital use
Registered indication: Parenteral therapy for empiric use in for moderate/severe nosocomial infections.
Customer group: Hospital specialists, ID physicians in general medical/surgical or critical care units, oncologists, haematologists and internists
Promotional claims:
Novel chemical classClinical efficacy against all Gram+ Gram-
aerobic and anaerobic pathogens Improved efficacy over contemporary therapiesPharmacodynamic properties leading to pathogen eradication Active against strains resistant to contemporary therapies Intravenous formulations given bdCompatible with other drugs and fluids given to patient groupWell tolerated
Distinguishing Attributes:
Does not cause CDADOnce daily dosing

Broad spectrum antibacterial agent for hospital use
Registered indication: Parenteral therapy for empiric use in for moderate/severe nosocomial infections.
Customer group: Hospital specialists, ID physicians in general medical/surgical or critical care units, oncologists, haematologists and internists
Promotional claims:
Novel chemical classClinical efficacy against all Gram+ Gram-
aerobic and anaerobic pathogensImproved efficacy over contemporary therapiesPharmacodynamic properties leading to pathogen eradication Active against strains resistant to contemporary therapies Intravenous formulations given bdCompatible with other drugs and fluids given to patient groupWell tolerated
Distinguishing Attributes:
Does not cause CDADOnce daily dosing

Broad spectrum antibacterial agent for hospital use
Registered indication: Parenteral therapy for empiric use in for moderate/severe nosocomial infections.
Customer group: Hospital specialists, ID physicians in general medical/surgical or critical care units, oncologists, haematologists and internists
Promotional claims:
Novel chemical classClinical efficacy against all Gram+ Gram-
aerobic and anaerobic pathogens Improved efficacy over contemporary therapiesPharmacodynamic properties leading to pathogen eradicationActive against strains resistant to contemporary therapies Intravenous formulations given bdCompatible with other drugs and fluids given to patient groupWell tolerated
Distinguishing Attributes:
Does not cause CDADOnce daily dosing

Broad spectrum antibacterial agent for hospital use
Registered indication: Parenteral therapy for empiric use in for moderate/severe nosocomial infections.
Customer group: Hospital specialists, ID physicians in general medical/surgical or critical care units, oncologists, haematologists and internists
Promotional claims: A novel leanordacycline analogue Clinical efficacy against important
Gram+ Gram-
aerobic and anaerobic pathogens in indications approvedEfficacy comparable
with contemporary therapiesPharmacodynamic properties leading to pathogen eradication Active in vitro against strains resistant to contemporary therapies Intravenous formulations given bdCompatible with other drugs and fluids given to patient groupWell tolerated
Distinguishing Attributes:
Once daily dosing
Will this new analogue of an existing series be good enough to displace the current favoured analogue from formularies ???????
Laboratory activities towards a Research Target Profile
Broad spectrum antibacterial agent for hospital use
Novel chemical class Active against strains resistant to contemporary therapies
Activity against all Gram+ Gram-
aerobic and anaerobic pathogens
Pharmacodynamic properties leading to pathogen eradication Intravenous formulations given infrequently.
Laboratory activities towards a Research Target Profile
Broad spectrum antibacterial agent for hospital use
Novel chemical class (novel mode of action) Active against strains resistant to contemporary therapies
Activity against all Gram+ Gram-
aerobic and anaerobic pathogens (appropriate to the indication)
Pharmacodynamic properties leading to pathogen eradication Intravenous formulations given infrequently.

Properties required:
Activity against:
Staphylococci
Enterobacteriaceae
additional barrier
P. aeruginosa / Acinetobacter
additional barrier / mutation
potential for efflux
Super–potency to sustain activity against penetration-mutants
? Efflux inhibition
How to approach this one?
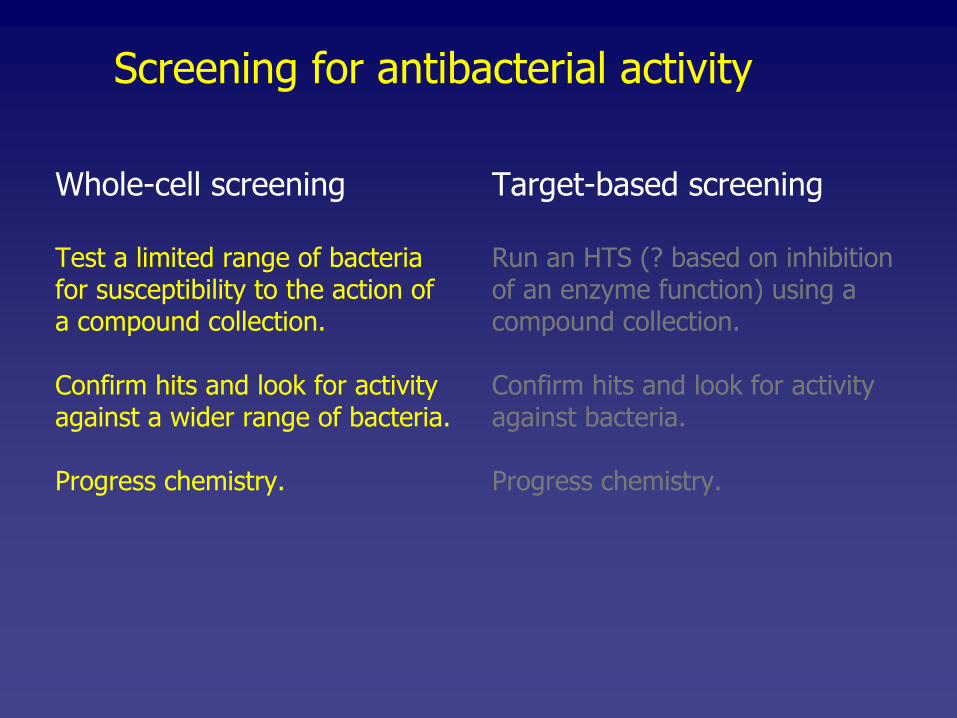
Screening for antibacterial activity
Whole-cell screening
Test a limited range of bacteriafor susceptibility to the action ofa compound collection.
Confirm hits and look for activityagainst a wider range of bacteria.
Progress chemistry.
Target-based screening
Run an HTS (? based on inhibitionof an enzyme function) using acompound collection.
Confirm hits and look for activityagainst bacteria.
Progress chemistry.
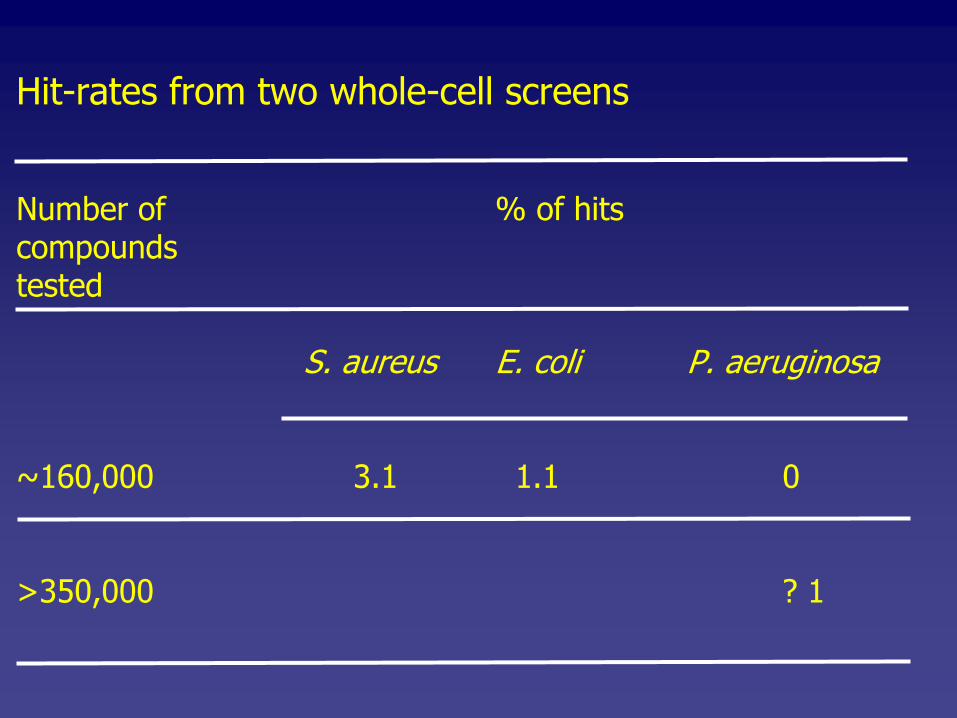
Hit-rates from two whole-cell screens
Number of % of hitscompoundstested
S. aureus E. coli
P. aeruginosa
~160,000
3.1
1.1
0
>350,000
? 1

Screening for antibacterial activity
Whole-cell screening
Test a limited range of bacteriafor susceptibility to the action ofa compound collection.
Confirm hits and look for activityagainst a wider range of bacteria.
Progress chemistry.
Target-based screening
Run an HTS (? based on inhibitionof an enzyme function) using acompound collection.
Confirm hits and look for activityagainst bacteria.
Progress chemistry.
Thus far, modern-day target-based screening has not delivered.
Why?

In my opinion, genomics was oversold and the science inadequately understood
• The expectations was that every target would lead to a new agent with a novel mechanism of action.
However ……………
• when an essential gene (potential target) is identified, many hurdles have to be overcome to allow a HTS to be run
• success from a HTS puts you at the ‘conventional’ starting point for LI and LO chemistry and biology
• as timeframes have been much longer than envisaged, this has not always been acceptable to senior management or Venture Capital providers.

Demonstration of
• essentiality
• possible identification of function
• selectivity
• spectrum
• ability to develop and assay for HTS format
• ability to produce protein or manipulate strainfor assay.
I made a scientific assessment (aka a guess), based on expected attrition rates, that it would take ~ 49 essential genes to have one progressed towards development.
I made a scientific assessment (aka a guess), based on expected attrition rates, that it would take ~ 49 essential gene to have one progressed towards development.
One other colleague was insistent it was 42
I have made a scientific assessment (aka a guess) that it would take ~ 49 essential gene to have one progressed towards the clinic.
One other colleague was insistent it was 42
This is perhaps she was called Jacqui Smith or had read The Hitchers Guide to the Galaxy!
In my opinion, genomics was oversold and the science inadequately understood
• The expectations was that every target would lead to a new agent with a novel mechanism of action.
However ……………
• when an essential gene (potential target) is identified, many hurdles have to be overcome to allow a HTS to be run
• success from a HTS puts you at the ‘conventional’ starting point for LI and LO chemistry and biology
• as timeframes have been much longer than envisaged, this has not always been acceptable to senior management or Venture Capital providers.

Screening for antibacterial activity
Whole-cell screening
Test a limited range of bacteriafor susceptibility to the action ofa compound collection.
Confirm hits and look for activityagainst a wider range of bacteria.
Progress chemistry.
Target-based screening
Run an HTS (? based on inhibitionof an enzyme function) using acompound collection.
Confirm hits and look for activityagainst bacteria.
Progress chemistry.
Compound libraries (or collections)Company libraries are basically a collection of all molecules made by the Chemists working in all therapeutic areas.
Those used in the good-old-bad-old days had a natural product component.
Over the years, optimised molecules in these collections have become bigger etc and do not represent good starting points for new chemistry.
Perhaps because of the potential difficulties of ‘rediscovery’
and time
in optimising activity, natural products have been less studied.
Therefore, we may question the suitability of such a compound-set even for whole-cell screening.
Hits found in an HTS require much more chemistry and thus start-
molecules should be small and of low lipophylicity to allow chemists the opportunity to design-in the required features.

Molecular weight
500
Lipo
phili
city
(cl
ogP
/ lo
gD)
5
Lipinski: rule of 5
ClogP <5M wt <500n of H bond donor <5n of H bond acceptor <10

Molecular weight
500
Lipo
phili
city
(cl
ogP/
logD
)
5
300
3
Thus, I suspect that we do not have sufficient collections rich in new, appropriately designed entries
and
natural products do not have adequate prominence.

ICAAC 2008 symposium
The role of medicinal chemistry in antimicrobial drug discovery:
How can we improve our libraries?
Are natural products still a viable source?
Crystals, chemicals and creativity ………..
Finding a new compound to satisfy this TPP will be exceptionally difficult.
Do we need to find a compound (? exquisitely potent) with all the properties?
Do we first need to find an efflux inhibitor, if one with a sufficient efflux-spectrum can be found, and include it with all early MIC tests to ultimately form part of a combination therapy?
Big challenge …………………
Finding a new compound to satisfy this TPP will be exceptionally difficult.
Do we need to find a compound (? exquisitely potent) with all the properties?
Do we first need to find an efflux inhibitor, if one with a sufficient efflux-spectrum can be found, and include it with all early MIC tests to ultimately form part of a combination therapy?
Big challenge …………………
How about a real big challenge and think about in vivo targets which go beyond the in vitro paradigms.

ICAAC 2008 symposium
New approaches circumventing classical drug targets:
Virulence factors …………………
Targeting transposition as an anti-virulence approach …..
A novel anti-Gm+ve antibiotic class acting on a non-essential target.
Speakers from academia or biotech.

Concluding commentsWhy is it now difficult to identify the new antibacterial agents
that we really need?
Over the years we have had many new agents introduced which havetaken care of bugs-of-the day; many of these are additional molecules from know series. These series are mostly exhausted.
We have expended a disproportionate effort on these series.
Compound collections are often inappropriate. This is now appreciated
Compounds with a novel mode of action are as common as hens teeth.
Infection-discovery research is much reduced, too heavily controlled by commercial considerations and too heavily influenced by non-research staff.
TPPs are now seen to ‘aspirational’
as opposed to absolute requirements.
If all of that sounds depressing or defeatest, I personally still have great hopes for biochemically-
or target-based programmes. Smaller Biotechs are active in this area and may provide big pharma with franchise-sustainers.

If all else fails, adopt the John Travolta / Mr Micawber last-resort-algorithm:
Keep’em stayin’
alive whilst hoping something will turn up.
Discussion time

Category
Name
Strength
Weakness
Dosing
β-lactam
c’penem
Doripenemβ-lactam
c’penem
tomopenem
MRSA
long t halfRO-4908463
β-lactam
ceph
ceftobiprole
MRSA
Gm negβ-lactam
ceph
ceftaroline
MRSA
Gm negβ-lactam
penem
faropenem
P.aeruginasa
PO
glycopeptide
Oritavancin
MRSA VRE
liver tox
lipo
Dalbavancin
MRSA
VRElipo
Telavancin
MRSA wide
VRE
qolipo
Ramoplanin
C. diff
PO
Macrolide/ketalide
cethromycin
telith
issue
PO
Trimethoprim
Iclaprim
?TPR-R staph
QTc
Misc
OPT80 PAR101 C. diffDifimicin
Misc
Tolevamer
C. diff
toxin binder
PO
Topical
Pleuromutalin
FDA ??

Compound libraries (or collections)
Company libraries are basically a collection of all molecules made by the Chemists working in all therapeutic areas.
Those used in the good-old-bad-old days had a natural product component.
Over the years, optimised molecules in these collections have become bigger etc and these do not represent good starting points for new chemistry. Perhaps because of the potential difficulties and time in optimising activity, natural products have been less studied.
Therefore, we may question the suitability of such a compound-set even for whole-cell screening.
Hits found in an HTS will require much more chemistry and thus start-molecules should be small and of low lypophylicity
to
allow chemists the opportunity to design-in the required features

Thus, I suspect that we do not have sufficient collections rich in new, appropriately designed entries
and
natural products do not have adequate prominence.

Finding a new compound to satisfy this TPP will be exceptionally difficult.
Do we need to find a compound (? exquisitely potent) with all the properties?
Do we first need to find an efflux inhibitor, if one with a sufficient efflux-spectrum can be found, and include it with all early MIC tests to ultimately form part of a combination therapy?
Big challenge …………………

What is a financially viable spectrum of anti-bacterial activity ?
Aerobes
Anaerobes
Gram+ve
Gram-ve
Staph/strep
Enterococci
Enterobacteriaceae Non-fermentors
++
++
++ ++ + ++ + + + + + + + +
Strains resistant to current agents are susceptible

Introducing ……………………………….
SIRNocycline (SUREKILL tm
)
The latest and most exciting analogue in the Leanordacycline series


















